3.-Enfermedad Celiaca

of 86
-
Upload
marcos-abraham-gonzalez-esteban -
Category
Documents
-
view
225 -
download
0
Transcript of 3.-Enfermedad Celiaca
-
7/31/2019 3.-Enfermedad Celiaca
1/86
Issue date: May 2009
NICE clinical guideline 86Developed by the Centre for Clinical Practice at NICE
Coeliac diseaseRecognition and assessment of coeliacdisease
-
7/31/2019 3.-Enfermedad Celiaca
2/86
NICE clinical guideline 86Coeliac disease: recognition and assessment of coeliac disease
Ordering information
You can download the following documents from www.nice.org.uk/CG86 The full guideline (this document) all the recommendations, details of how
they were developed, and reviews of the evidence they were based on.
A quick reference guide a summary of the recommendations forhealthcare professionals.
Understanding NICE guidance a summary for patients and carers.
For printed copies of the quick reference guide or Understanding NICEguidance, phone NICE publications on 0845 003 7783 or [email protected] and quote:
N1859 (quick reference guide)
N1860 (Understanding NICE guidance).
NICE clinical guidelines are recommendations about the treatment and care ofpeople with specific diseases and conditions in the NHS in England andWales.
This guidance represents the view of NICE, which was arrived at after carefulconsideration of the evidence available. Healthcare professionals areexpected to take it fully into account when exercising their clinical judgement.
However, the guidance does not override the individual responsibility ofhealthcare professionals to make decisions appropriate to the circumstancesof the individual patient, in consultation with the patient and/or guardian orcarer, and informed by the summary of product characteristics of any drugsthey are considering.
Implementation of this guidance is the responsibility of local commissionersand/or providers. Commissioners and providers are reminded that it is theirresponsibility to implement the guidance, in their local context, in light of theirduties to avoid unlawful discrimination and to have regard to promotingequality of opportunity. Nothing in this guidance should be interpreted in a way
that would be inconsistent with compliance with those duties.
National Institute for Health and Clinical Excellence
MidCity Place71 High HolbornLondon WC1V 6NA
www.nice.org.uk
National Institute for Health and Clinical Excellence, 2009. All rights reserved. This materialmay be freely reproduced for educational and not-for-profit purposes. No reproduction by orfor commercial organisations, or for commercial purposes, is allowed without the express
written permission of NICE.
-
7/31/2019 3.-Enfermedad Celiaca
3/86
NICE clinical guideline 86 Coeliac disease 3
Contents
Disclaimer ....................................................................................................... 4Foreword ........................................................................................................ 5Patient-centred care ...................................................................................... 71 Summary .................................................................................................. 9
1.1 Recommendations ............................................................................. 91.2 Care pathway .................................................................................. 141.3 Overview .......................................................................................... 18
2 Evidence review .................................................................................... 202.1 Introduction ...................................................................................... 202.2 Prevalence of coeliac disease ......................................................... 212.3 The possible long-term consequences of undiagnosed coeliac
disease ........................................................................................... 232.4 Signs and symptoms of coeliac disease and coexisting conditions
with coeliac disease ......................................................................... 262.5 Serological tests in the diagnostic process for coeliac disease ....... 372.6 Research recommendations ............................................................ 59
3 References, glossary and abbreviations ............................................. 613.1 References ...................................................................................... 613.2 Glossary .......................................................................................... 713.3 Abbreviations ................................................................................... 74
4 Methods.................................................................................................. 744.1 Aim and scope of the guideline ........................................................ 744.2 Development methods ..................................................................... 74
5
Contributors ........................................................................................... 79
5.1 The Guideline Development Group ................................................. 795.2 Declarations ..................................................................................... 86
The appendices are available as separate files.
Appendix 6.1 Scope
Appendix 6.2 Key clinical questions and protocols
Appendix 6.3 ROC curves and forest plots
Appendix 6.4 Search strategiesAppendix 6.5 Health economics evidence and evidence tables
Appendix 6.6 Evidence tables
-
7/31/2019 3.-Enfermedad Celiaca
4/86
NICE clinical guideline 86 Coeliac disease 4
Disclaimer
NICE clinical guidelines are recommendations about the treatment and care of
people with specific diseases and conditions in the NHS in England and
Wales.
This guidance represents the view of NICE, which was arrived at after careful
consideration of the evidence available. Healthcare professionals are
expected to take it fully into account when exercising their clinical judgement.
However, the guidance does not override the individual responsibility of
healthcare professionals to make decisions appropriate to the circumstances
of the individual patient, in consultation with the patient and/or guardian or
carer, and informed by the summary of product characteristics of any drugs
they are considering.
Implementation of this guidance is the responsibility of local commissioners
and/or providers. Commissioners and providers are reminded that it is their
responsibility to implement the guidance, in their local context, in light of their
duties to avoid unlawful discrimination and to have regard to promoting
equality of opportunity. Nothing in this guidance should be interpreted in a way
that would be inconsistent with compliance with those duties.
-
7/31/2019 3.-Enfermedad Celiaca
5/86
NICE clinical guideline 86 Coeliac disease 5
Foreword
Coeliac disease is believed to be present in up to 1 in 100 of the population
although only about 1015% of people with the condition are clinically
diagnosed. Many of the remainder may be well, but a significant minority will
have chronic problems such as lethargy, gastrointestinal symptoms, or the
effects of anaemia. These result in chronic ill health and often extensive
medical investigation without a definite diagnosis.
Because coeliac disease can be very effectively treated with a gluten-free diet
it is important to identify people with the undiagnosed disease so as to provide
satisfactory individual treatment and also to improve the overall health of the
community.
To improve the recognition of coeliac disease and to increase the number of
people diagnosed with the condition, the Department of Health asked NICE to
produce a short clinical guideline about how the disease should be recognised
and which people should be assessed for the disease.
The Guideline Development Group (GDG) comprised experts in both adult
and paediatric gastroenterology from primary and secondary care, dietitians,
patient members and a clinical immunologist. It was supported by the NICE
Short Clinical Guidelines Technical Team.
The GDG considered systematically identified and reviewed evidence
concerning the recognition of coeliac disease. A new health economic model
was also developed to consider the cost effectiveness of serological tests for
coeliac disease.
The guideline gives recommendations about the clinical signs, symptoms and
types of presentation or conditions that should alert practitioners to consider
the presence of coeliac disease, and suggests a scheme of investigation to
follow when making the diagnosis. It is expected that implementation of the
guideline recommendations will lead to many new cases being diagnosed and
much ill health being alleviated.
-
7/31/2019 3.-Enfermedad Celiaca
6/86
NICE clinical guideline 86 Coeliac disease 6
The GDG hopes that this guideline will be sufficiently clear and non-
contentious that its implementation will be routine both in secondary care and
in primary care, where most patients with coeliac disease will present.
Professor Peter D Howdle
Chair, Guideline Development Group
-
7/31/2019 3.-Enfermedad Celiaca
7/86
NICE clinical guideline 86 Coeliac disease 7
Patient-centred care
This guideline offers best practice advice on the recognition and assessment
of coeliac disease and the care of children and adults who are undergoing the
diagnostic process for coeliac disease.
This diagnostic process should take into account patients needs and
preferences. People with symptoms and/or signs suggestive of coeliac
disease should have the opportunity to make informed decisions, in
partnership with their healthcare professionals. If patients do not have the
capacity to make decisions, healthcare professionals should follow the
Department of Health (2001) guidelines Reference guide to consent for
examination or treatment (available from www.dh.gov.uk). Healthcare
professionals should also follow a code of practice accompanying the Mental
Capacity Act (summary available from www.publicguardian.gov.uk).
If the patient is under 16, healthcare professionals should follow guidelines in
Seeking consent: working with children (available from www.dh.gov.uk).
Good communication between healthcare professionals and patients is
essential. It should be supported by evidence-based written information
tailored to the patients needs. Diagnosis, treatment and care, and the
information patients are given about it, should be culturally appropriate. It
should also be accessible to people with additional needs such as physical,
sensory or learning disabilities, and to people who do not speak or read
English.
If the patient agrees, families and carers should have the opportunity to be
involved in decisions about diagnosis, treatment and care.
Families and carers should also be given the information and support they
need.
Care of young people in transition between paediatric and adult services
should be planned and managed according to the best practice guidance
-
7/31/2019 3.-Enfermedad Celiaca
8/86
NICE clinical guideline 86 Coeliac disease 8
described in Transition: getting it right for young people (available from
www.dh.gov.uk).
Adult and paediatric healthcare teams should work jointly to provide
assessment and services to young people with coeliac disease. Diagnosis
and management should be reviewed throughout the transition process, and
there should be clarity about who is the lead clinician to ensure continuity of
care.
-
7/31/2019 3.-Enfermedad Celiaca
9/86
NICE clinical guideline 86 Coeliac disease 9
1 Summary
1.1 Recommendations
When to offer testing
1.1.1 Offer serological testing for coeliac disease to children and adults
with any of the following signs and symptoms:
chronic or intermittent diarrhoea
failure to thrive or faltering growth (in children)
persistent or unexplained gastrointestinal symptoms includingnausea and vomiting
prolonged fatigue (tired all the time)
recurrent abdominal pain, cramping or distension
sudden or unexpected weight loss
unexplained iron-deficiency anaemia, or other unspecified
anaemia.
1.1.2 Offer serological testing for coeliac disease to children and adults
with:
any of the following conditions:
autoimmune thyroid disease
dermatitis herpetiformis
irritable bowel syndrome
type 1 diabetes
or
first-degree relatives (parents, siblings or children) with coeliac
disease.
-
7/31/2019 3.-Enfermedad Celiaca
10/86
NICE clinical guideline 86 Coeliac disease 10
1.1.3 Consider offering serological testing for coeliac disease to children
and adults with any of the following:
Addison's disease
amenorrhoea
aphthous stomatitis (mouth ulcers)
autoimmune liver conditions
autoimmune myocarditis
chronic thrombocytopenia purpura
dental enamel defects
depression or bipolar disorder
Downs syndrome
epilepsy
low-trauma fracture
lymphoma
metabolic bone disease (such as rickets or osteomalacia)
microscopic colitis
persistent or unexplained constipation
persistently raised liver enzymes with unknown cause
polyneuropathy
recurrent miscarriage
reduced bone mineral density
sarcoidosis
Sjgren's syndrome
Turner syndrome
unexplained alopecia
unexplained subfertility.
Dietary considerations before testing for coeliac disease
1.1.4 Do not use serological testing for coeliac disease in infants before
gluten has been introduced to the diet.
1.1.5 Inform people (and their parents or carers, as appropriate) that any
testing for coeliac disease is accurate only if the person continues
-
7/31/2019 3.-Enfermedad Celiaca
11/86
NICE clinical guideline 86 Coeliac disease 11
to follow a gluten-containing diet during the diagnostic process
(serological tests and biopsy if required).
1.1.6 Inform people that they should not start a gluten-free diet until
diagnosis is confirmed by intestinal biopsy, even if a self-test or
other serological test is positive.
1.1.7 Inform people that when they are following a normal diet
(containing gluten) they should eat some gluten (for example,
bread, chapattis, pasta, biscuits, or cakes) in more than one meal
every day for a minimum of 6 weeks before testing; however, it is
not possible to say exactly how much gluten they should eat.
1.1.8 If a person is reluctant or unable to reintroduce gluten into their diet
before testing:
refer them to a gastrointestinal specialist and
inform them that it may be difficult to confirm a diagnosis of
coeliac disease on intestinal biopsy, and that this may have
implications for the prescribing of gluten-free foods.
Other information before serological testing
1.1.9 Inform people who are considering, or have undertaken, self-testing
for coeliac disease (and their parents or carers) that any result from
self-testing needs to be discussed with a healthcare professional
and confirmed by laboratory-based tests.
1.1.10 Before seeking consent to take blood for serological tests, explain:
what coeliac disease is
that serological tests do not diagnose coeliac disease, but
indicate whether further testing is needed
the implications of a positive test (including referral for intestinal
biopsy and implications for other family members)
the implications of a negative test (that coeliac disease is
unlikely but it could be present or could arise in the future).
-
7/31/2019 3.-Enfermedad Celiaca
12/86
NICE clinical guideline 86 Coeliac disease 12
1.1.11 Inform people and their parents or carers that a delayed diagnosis
of coeliac disease, or undiagnosed coeliac disease, can result in:
continuing ill health
long-term complications, including osteoporosis and increased
fracture risk, unfavourable pregnancy outcomes and a modest
increased risk of intestinal malignancy
growth failure, delayed puberty and dental problems (in
children).
Serological tests
1.1.12 All tests should be undertaken in laboratories with clinical pathologyaccreditation (CPA).
1.1.13 Do not use immunoglobulin G (IgG) or immunoglobulin A (IgA)
anti-gliadin antibody (AGA) tests in the diagnosis of coeliac
disease.
1.1.14 Do not use of self-tests and/or point-of-care tests for coeliac
disease as a substitute for laboratory-based testing.
1.1.15 When clinicians request serology, laboratories should:
use IgA tissue transglutaminase (tTGA) as the first choice test
use IgA endomysial antibodies (EMA) testing if the result of the
tTGA test is equivocal
check for IgA deficiency if the serology is negative1
use IgG tTGA and/or IgG EMA serological tests for people withconfirmed IgA deficiency
communicate the results clearly in terms of values, interpretation
and recommended action.
1.1.16 Do not use human leukocyte antigen (HLA) DQ2/DQ8 testing in the
initial diagnosis of coeliac disease. (However, its high negative
1Investigation for IgA deficiency should be done if the laboratory detects a low or very low
optical density on IgA tTGA test or low background on IgA EMA test.
-
7/31/2019 3.-Enfermedad Celiaca
13/86
NICE clinical guideline 86 Coeliac disease 13
predictive value may be of use to gastrointestinal specialists in
specific clinical situations.)
After serological testing
1.1.17 Offer referral to a gastrointestinal specialist for intestinal biopsy to
confirm or exclude coeliac disease to people with positive
serological results from any tTGA or EMA test.
1.1.18 If serology tests are negative but coeliac disease is still clinically
suspected, offer referral to a gastrointestinal specialist for further
assessment.
-
7/31/2019 3.-Enfermedad Celiaca
14/86
1.2 Care pathway
Does the person have any of the signs, symptomsor conditions listed in box A or box B?
Yes
No
Is the person on a gluten-containing diet?
Is the person willing/able toreintroduce gluten to theirdiet?
Yes
No
Recognitionanassessmen
t
No
Important: Do not use serological testing for coeliac disease in infants before gluten has been introduced to the diet
Offer serological testing if the person has any of thesigns, symptoms or conditions in box AConsider offering serological testing if the personhas any of the conditions in box B
Person is unlikely to needtesting for coeliac disease atthis point, unless there is acontinuing medical problemor clinical suspicion
Refer them to agastrointestinalspecialist and informthem that it may bedifficult to confirm adiagnosis of coeliacdisease on intestinalbiopsy, and that thismay have implicationsfor their ability to accessprescribed gluten-freefoods
-
7/31/2019 3.-Enfermedad Celiaca
15/86
Dietary considerations before serological testing
Inform people (and their parents or carers as appropriate)that:
testing (serology and biopsy if required) is accurateonly if they follow a gluten-containing diet
when following a gluten-containing diet they should eatsome gluten in more than one meal every day for atleast 6 weeks before testing
they should not start a gluten-free diet until diagnosis isconfirmed by intestinal biopsy (even if a self-test orother serological test is positive)
Other information before serological testing
Inform people who are considering, or who have undertaken, self-testing forcoeliac disease that any result from self-testing needs to be discussed with ahealthcare professional and confirmed by laboratory-based tests.
Before seeking consent to take blood for serological tests, explain:
what coeliac disease is
that serological tests do not diagnose coeliac disease, but indicate whetherfurther testing is needed
the implications of a positive test (including referral for intestinal biopsy andimplications for other family members)
the implications of a negative test (that coeliac disease is unlikely but itcould be present or arise in the future).
Inform people (and their parents or carers as appropriate) that a delayeddiagnosis of coeliac disease, or undiagnosed coeliac disease, can result in:
continuing ill health
long-term complications, including osteoporosis and increased fracture risk,unfavourable pregnancy outcomes and a modest increased risk of intestinalmalignancy
growth failure, delayed puberty and dental problems (in children).
Information
needs
-
7/31/2019 3.-Enfermedad Celiaca
16/86
Serologytestinga
ndafter
Use serological testing for IgA tissuetransglutaminase (tTGA) as a first-choice test
Use IgA endomysial antibodies (EMA) testing ifthe result of the tTGA test is equivocal
Negativeresult
Check for IgAdeficiency
a
Offer IgG tTGA testsand/or IgG EMA tests
Positiveresult
Negative resultbut continuing
clinical suspicion
Positive result
Positive result Negative resultbut continuing
clinical suspicion
Negativeresult, no
furtherreason tosuspectcoeliacdisease
aInvestigation for IgA deficiency should be done if the laboratory
detects a low or very low optical density on IgA tTGA test or lowbackground on IgA EMA test.
Important:
All tests should be undertaken in laboratories with clinical pathology accreditation (CPA) Do not use IgA or IgG anti-gliadin antibody (AGA) tests in the diagnosis of coeliac disease Do not use HLA DQ2/DQ8 testing in the initial diagnosis of coeliac disease (However, its high negative
predictive value may be of use to gastrointestinal specialists in specific clinical situations)
Do not use self-tests and/or point of care tests for coeliac disease as a substitute for laboratory-basedtesting
Unlikely to have coeliacdiseaseNo need to repeat tests
Refer to a gastrointestinalspecialist for intestinal biopsy toconfirm or exclude coeliacdisease
-
7/31/2019 3.-Enfermedad Celiaca
17/86
Signs, symptoms and conditions associated with coeliac disease
Box A. Offer serological testing to children and adults with any of thefollowing signs, symptoms and conditions
Signs and symptoms Conditions
Chronic or intermittent diarrhoea
Failure to thrive or faltering growth (in
children)
Persistent or unexplained gastrointestinal
symptoms including nausea and vomiting
Prolonged fatigue (tired all the time)
Recurrent abdominal pain, cramping or
distension
Sudden or unexpected weight loss
Unexplained iron-deficiency anaemia, or
other unspecified anaemia
Autoimmune thyroid disease
Dermatitis herpetiformis
Irritable bowel syndrome
Type 1 diabetes
First-degree relatives (parents, siblings or
children) with coeliac disease
Box B. Consider offering serological testing to children and adults withany of the following
Addison's disease
amenorrhoea
aphthous stomatitis (mouth ulcers)
autoimmune liver conditions
autoimmune myocarditis
chronic thrombocytopenia purpura
dental enamel defects
depression or bipolar disorder
Downs syndrome
epilepsy
low-trauma fracture
lymphoma
metabolic bone disease (such asrickets or osteomalacia)
microscopic colitis
persistent or unexplainedconstipation
persistently raised liver enzymes withunknown cause
polyneuropathy
recurrent miscarriage
reduced bone mineral density
sarcoidosis
Sjgren's syndrome
Turner syndrome unexplained alopecia
unexplained subfertility.
-
7/31/2019 3.-Enfermedad Celiaca
18/86
Nice clinical guideline 86 Coeliac disease 18
1.3 Overview
1.3.1 Coeliac disease: recognition and assessment
Coeliac disease is a state of heightened immunological response to ingestedgluten in genetically susceptible people. Gluten is a protein that is present in
wheat, barley and rye. Historically, coeliac disease was believed to be
uncommon; however, population-based studies have identified that it is more
common than previously thought.
Coeliac disease has traditionally been associated with mainly gastrointestinal
symptoms (such as diarrhoea, abdominal pain, bloating, constipation and
indigestion), because chronic inflammation of the small intestine is a feature of
the immune response to gluten. However, non-gastrointestinal features of
coeliac disease have been increasingly recognised in people presenting with
the disease. Some people with coeliac disease have no obvious symptoms.
Coeliac disease is considered to be more prevalent in people with
autoimmune conditions such as type 1 diabetes or autoimmune thyroid
disease, and in first-degree relatives of people with coeliac disease.
Coeliac disease can be diagnosed at any age (after the introduction of gluten-
containing foods to the infant weaning diet), and presents in both children and
adults.
Because of the disparate nature of its signs and symptoms, and the historical
belief that it is not a common disease, there is concern that coeliac disease
often goes unrecognised and consequently is underdiagnosed. As a result,
people may present to primary and secondary care on many occasions and
with a range of symptoms before diagnosis. Delayed diagnosis is a concern
because the symptoms of coeliac disease remain untreated and because of
the possible long-term effects of undiagnosed coeliac disease.
There is also some uncertainty about which of the serological tests are most
suitable for use in the diagnostic process for coeliac disease. Small intestinal
biopsy is used as the reference standard for the diagnosis of coeliac disease.
-
7/31/2019 3.-Enfermedad Celiaca
19/86
Nice clinical guideline 86 Coeliac disease 19
Although there is ongoing debate about the possibility of diagnosis without the
need for an intestinal biopsy, it is accepted that currently it is needed for a
definitive diagnosis.
This short clinical guideline aims to improve the care of children and adults
with undiagnosed coeliac disease by making evidence-based
recommendations about its recognition, and about using serological testing to
direct referral for definitive diagnosis by intestinal biopsy.
This guideline uses the best available clinical-effectiveness and cost-
effectiveness evidence, which is analysed and discussed by the GDG to
develop recommendations. The GDG considered the signs and symptoms,
conditions likely to coexist with coeliac disease, the role of serological testing
in the diagnostic process up to referral for small intestinal biopsy, and the
information needs of patients and carers throughout this process.
1.3.2 The NICE short clinical guideline programme
Coeliac disease: recognition and assessment' (NICE clinical guideline 86) is a
NICE short clinical guideline. For a full explanation of the NICE guideline
development process, see The guidelines manual (2009) (available from
www.nice.org.uk/guidelinesmanual).
1.3.3 Using this guideline
This document is intended to be relevant to healthcare professionals in
primary and secondary care. The target population is adults and children with
symptoms and/or signs that suggest coeliac disease.
This is the full version of the guideline. It is available from
www.nice.org.uk/CG86. Printed summary versions of this guideline are
available: Understanding NICE guidance (a version for patients and carers)
and a quick reference guide (for healthcare professionals). These are also
available fromwww.nice.org.uk/CG86.
http://www.nice.org.uk/guidelinesmanualhttp://www.nice.org.uk/guidelinesmanualhttp://www.nice.org.uk/CG86http://www.nice.org.uk/CG86http://www.nice.org.uk/CG86http://www.nice.org.uk/CG86http://www.nice.org.uk/CG86http://www.nice.org.uk/CG86http://www.nice.org.uk/CG86http://www.nice.org.uk/guidelinesmanual -
7/31/2019 3.-Enfermedad Celiaca
20/86
Nice clinical guideline 86 Coeliac disease 20
1.3.4 Using recommendations and supporting evidence
For each clinical question the GDG was presented with a summary of the
clinical evidence, and economic evidence if appropriate, derived from the
studies reviewed and appraised. The GDG based the guidelinerecommendations on this information. The link between the evidence and the
view of the GDG in making each recommendation is made explicit in the
'Evidence to recommendations' sections (2.2.3, 2.3.4 and 2.4.5).
2 Evidence review
2.1 Introduction
The clinical-effectiveness and cost-effectiveness evidence that was used in
the development of this guideline is summarised in this section. Further details
about the cost-effectiveness evidence, including details of the economic
model, are given in appendix 6.5; details about the clinical evidence are given
in the tables in appendix 6.6.
The aim of this guideline is to improve the recognition and assessment of
coeliac disease in children and adults; it considers the diagnostic pathway upto referral for intestinal biopsy. Small intestinal biopsy is the reference
standard used throughout this guideline; the studies included are those in
which coeliac disease was confirmed by intestinal biopsy. In 2004 the Agency
for Healthcare Research and Quality (AHRQ) published an evidence
report/technology assessment on coeliac disease. The report included a
series of systematic reviews using clearly defined methods; these reviews
have been included when appropriate to the scope of this guideline. TheAHRQ report, assessed as a well-conducted systematic review, is considered
as high-quality evidence (details of the evidence grading system can be found
in The guidelines manual [2009], available fromwww.nice.org.uk). Other
studies included in this guideline have been mainly cohort-based studies,
notably for the evidence of serological test accuracy. Casecontrol studies
have also been included when appropriate. Both the cohort and casecontrol
studies have limitations resulting from study design, and as such are regarded
as level + evidence. Case series, case reports and studies with small
http://www.nice.org.uk/http://www.nice.org.uk/http://www.nice.org.uk/http://www.nice.org.uk/ -
7/31/2019 3.-Enfermedad Celiaca
21/86
Nice clinical guideline 86 Coeliac disease 21
numbers (less than 50 participants) have not been included. When both signs
and symptoms and coexisting conditions have been listed in this guideline
they have been listed alphabetically.
2.2 Prevalence of coeliac disease
2.2.1 Evidence review
The prevalence of coeliac disease has historically been difficult to determine
because in many cases people with coeliac disease do not have specific signs
and symptoms. Difficulties in recognising coeliac disease have resulted in its
prevalence being considerably underestimated.
A search was carried out to identify large population-based studies giving data
on the prevalence of coeliac disease; these are reviewed below.
Overall prevalence of coeliac disease
The AHRQ report (2004) includes studies that considered the prevalence of
coeliac disease in north America and western Europe up to and including
2003. The evidence below includes the AHRQ report with additional relevant
large population-based studies in north America and western Europe from
2003 onwards and studies in other geographical areas from 1990. The AHRQ
report found a prevalence of coeliac disease in children by biopsy of 0.5 to
1.6% (six studies) and by serology of 0.3 to 1.9% (eight studies); in adults the
prevalence by biopsy was 0.07 to1.9% (15 studies) and by serology was 0.2
to 2.7% (22 studies). The three UK-based studies in the AHRQ report are all
of adults, and identify a prevalence of coeliac disease by biopsy of 1.0% and
by serology of 0.8 to 1.9%.
The Avon Longitudinal Study of Parents and Children (a population-based
cohort study) used IgA EMA to investigate children aged 7.5 years and
reported that 1% (54 out of 5470) were serologically positive for coeliac
disease. This study also showed that IgA EMA positive rates were higher in
girls than in boys, odds ratio (OR) 2.12 (95% confidence interval [CI] 1.20 to
3.75) (Bingley et al. 2004).
-
7/31/2019 3.-Enfermedad Celiaca
22/86
Nice clinical guideline 86 Coeliac disease 22
Additional international studies in adults used data which was available from
large samples such as people donating blood (Bdioui et al. 2006; Melo et al.
2006; Oliveria et al. 2007; Pereira et al. 2006; Shahbazkha et al. 2003) and
people attending for prenuptial medical checks (Gomez et al. 2001). A further
study used random sampling from a national register (Roka et al. 2007).
These studies found a prevalence of coeliac disease in adults of 0.14 to
0.86%.
Additional international studies in children used data on children younger than
3 years (Castano et al. 2004), samples from an existing public health register
(Korponay-Szabo et al. 1999) and random sampling of school children (Ben
Hariz et al. 2007; Ertekin et al. 2005). These studies identified a prevalence of
coeliac disease in children of 0.64 to 1.17%.
The AHRQ report (2004) also included studies on the prevalence of coeliac
disease in both children and adults in whom coeliac disease was suspected.
These studies were mainly situated in referral centres and the prevalence of
coeliac disease varied widely: in children it was 1.1 to 4.0% with EMA
serology, 4.6 to 17.0% with biopsy; in adults it was 1.5% with EMA serology,
11.6 to 50.0% with biopsy.
Prevalence in first-degree relatives
The AHRQ report (2004) included studies that considered the prevalence of
coeliac disease in first-degree relatives of people who had had a diagnosis of
coeliac disease. These studies showed a prevalence of 2.8 to 17.2% with
serology (five studies) and 5.6 to 44.1% with biopsy (12 studies). The three
studies completed in the UK all reported a prevalence found using biopsy, andreported a prevalence in first-degree relatives of 5.6 to 22.5%.
Three additional studies were included (Fraser et al. 2006; Biagi et al. 2008;
Szaflaraka-Sczepanik et al. 2001). These reported a prevalence of coeliac
disease in first-degree relatives of 2 to 17.7%. The study by Fraser et al. was
in the UK and reported a prevalence of 5.5%.
-
7/31/2019 3.-Enfermedad Celiaca
23/86
Nice clinical guideline 86 Coeliac disease 23
2.2.2 Evidence statements
In national studies in the UK, the prevalence of coeliac disease ranges
between 0.8% and 1.9%. This is broadly similar to other international studies.
Among first-degree relatives of people with coeliac disease, the majority of
studies report a prevalence of coeliac disease between 4.5% and 12%.
There is limited evidence that the prevalence of coeliac disease is twice as
high in females as in males.
2.3 The possible long-term consequences of
undiagnosed coeliac disease
2.3.1 Evidence review
The review considered only the possible long-term consequences of
undiagnosed coeliac disease, and therefore did not include any studies that
considered people with diagnosed coeliac disease. It did not include
consideration of any long-term consequences of coeliac disease that may
affect coexisting conditions such as type 1 diabetes. The included studies
looked at undiagnosed coeliac disease or where other possible long-term
consequences had been noted as present at the point of diagnosis. It should
be noted that these possible long-term consequences are associations and
the studies are not considered to provide evidence of a causal relationship. In
all but one of the included studies coeliac disease had been confirmed by
biopsy; the other study included pregnant women and intestinal biopsy was
not considered ethical in those near to delivery (Greco et al. 2004). Overall
evidence was identified in three areas: pregnancy outcomes, fracture risk and
malignancy.
Pregnancy outcomes
An Italian study of 5055 women admitted to obstetric and gynaecological
wards (Greco et al. 2004) identified no pregnancy outcomes for which there
was a significant difference between women with and without coeliac disease.
Outcomes included risk of spontaneous abortion, premature delivery, low birth
weight and intrauterine growth retardation (IUGR).
-
7/31/2019 3.-Enfermedad Celiaca
24/86
Nice clinical guideline 86 Coeliac disease 24
A Swedish study analysed data on people from a national inpatient register
who had a hospital-based discharge record of coeliac disease (Ludvigsson et
al. 2005). It included 929 women whose coeliac disease had not been
diagnosed when they gave birth, and 2,822,805 women without coeliac
disease. There were significant differences between outcomes in the two
groups of women. IUGR was reported in 5.5% of mothers with undiagnosed
coeliac disease, and in 3.1% of mothers without coeliac disease (adjusted
odds ratio [OR] 1.62, 95% confidence interval [CI] 1.22 to 2.15, p = 0.001).
The equivalent figures for low-birth-weight were 7.0% and 3.4% (adjusted OR
2.13, 95% CI 1.66 to 2.75, p < 0.001); for very-low-birth-weight 1.2% and
0.5% (adjusted OR 2.45, 95% CI 1.35 to 4.43, p = 0.003); for preterm birth
8.0% and 5.0% (adjusted OR 1.71, 95% CI 1.35 to 2.17, p < 0.001); and for
caesarean section 3.4% and 2.3% (adjusted OR 1.82, 95% CI 1.27 to 2.60,
p = 0.001). No significant difference was found between the groups for very
preterm birth (before 30 weeks) or for babies with low Apgar scores (less
than 7).
Fracture risk
A second Swedish study using the national inpatient register (Ludvigsson etal. 2007) considered hip fractures (14,187 in patients with coeliac disease;
68,852 in patients without coeliac disease) and any fractures (13,724 in
patients with coeliac disease; 65,627 in patients without coeliac disease). The
estimated association of coeliac disease and prior fractures showed an
increased risk of diagnosis with coeliac disease after hip fracture (OR 2.0,
95% CI 1.6 to 2.5, p < 0.001) and after any fracture (OR 1.6, 95% CI 1.5 to
1.8, p < 0.001). This study also identified significantly higher rates of hip
fractures in people with undiagnosed coeliac disease compared with those
with diagnosed coeliac disease. This increased risk was seen throughout the
time period from 10 years to 0.01 years before diagnosis of coeliac disease.
A Danish study used the national patient discharge register to consider
fracture risk in people with coeliac disease (Vestergaard et al. 2002). This
study identified no increase in fracture risk before diagnosis of coeliac disease
compared with matched controls for skull and jaw fractures, spine, rib and
-
7/31/2019 3.-Enfermedad Celiaca
25/86
Nice clinical guideline 86 Coeliac disease 25
pelvis fractures, upper arm fractures, forearm fractures, Colles fractures,
hand and finger fractures, hip and femur fractures, fractured neck of femur,
lower leg fractures, foot fractures and osteoporosis.
Malignancy
A US study considered the standardised mortality ratio (SMR) of observed to
expected rates for cancers that were diagnosed before or simultaneously with
coeliac disease diagnosis (Green et al. 2003). Although numbers were small,
this study identified significant SMRs for non-Hodgkins lymphoma (4
observed cases compared with 0.7 expected, SMR 5.3, 95% CI 2.3 to 13,
p < 0.001), small bowel cancer (3 vs. 0.1, SMR 45, 95% CI 34 to 61,
p < 0.001), oesophageal cancer (3 vs. 0.2, SMR 16, 95% CI 9.7 to 26,
p < 0.001) and melanoma (4 vs. 0.8, SMR 5, 95% CI 2.1 to 12, p < 0.001). It
did not identify a significant difference SMR for colon cancer, breast cancer
and total cancers.
An Italian study considered the impact of delayed diagnosis of coeliac disease
on cancer risk using a standardised incidence ratio (SIR) of observed
compared with expected cases in 1968 adults with diagnosed coeliac disease
(Silano et al. 2007). In this study 55 people were diagnosed with cancer
before or simultaneously with coeliac disease diagnosis, compared with
42.1 expected cases (SIR 1.3, 95% CI 1.0 to 1.7). Although numbers involved
were small, this study identified 20 observed cases compared with
4.2 expected of non-Hodgkin's lymphoma (SIR 4.7, 95% CI 2.9 to 7.3), for
colon cancer 7 compared with 6.2 (SIR 1.1, 95%CI 0.68 to 1.56), for small
bowel cancer 5 compared with 0.19 (SIR 25, 95% CI 8.5 to 51.4) and for
Hodgkins lymphoma 4 compared with 0.4 (SIR 10, 95% CI 2.7 to 25). A lower
risk was identified for breast cancer in people with newly diagnosed coeliac
disease (3 vs. 14, SIR 0.2, 95% CI 0.04 to 0.62).
2.3.2 Evidence statements
There is evidence that undiagnosed maternal coeliac disease has a negative
effect on intrauterine growth and birth weight, and is associated with
increased preterm birth and caesarean section rates.
-
7/31/2019 3.-Enfermedad Celiaca
26/86
Nice clinical guideline 86 Coeliac disease 26
Evidence suggests an association between undiagnosed coeliac disease and
an increased risk of fractures.
Undiagnosed coeliac disease is associated with an increased risk of non-
Hodgkins and Hodgkins lymphoma and small bowel cancer, but overall rates
are low.
2.3.3 Linking evidence to recommendations
The GDG discussed the evidence, agreed the evidence statements relating to
the possible effects of long-term undiagnosed coeliac disease, and developed
recommendations. This discussion is summarised here:
The GDG agreed the need to include information about the risk of long-
term complications of undiagnosed coeliac disease. It noted that although
there is an increased risk of the specific cancers with undiagnosed coeliac
disease, the overall risk of developing these cancers is low.
The GDG discussed the different possible long-term effects in children and
adults and agreed an additional recommendation for children specifying
growth failure, delayed puberty and dental complications.
2.4 Signs and symptoms of coeliac disease and
coexisting conditions with coeliac disease
2.4.1 Evidence review signs and symptoms
Recognition and assessment of coeliac disease can be difficult because of the
variety of presenting signs and symptoms.
The AHRQ report considered the prevalence of coeliac disease in adults with
iron-deficiency anaemia and in adults with low bone-mineral density. Eight
studies from the AHRQ report with 50 or more participants were included;
these were all in adults with biopsy-proven coeliac disease. The prevalence of
coeliac disease in people with iron-deficiency anaemia ranged from 2.3 to
15%. Four studies from the AHRQ report considered people with low bone
mineral density; these studies identified a prevalence of coeliac disease
ranging from 0 to 3%.
-
7/31/2019 3.-Enfermedad Celiaca
27/86
Nice clinical guideline 86 Coeliac disease 27
Further papers included in this review considered people with coeliac disease
at the point of it being diagnosed and the features that they presented with.
(Those reported in table 1 are where 5% or more of participants had the
presenting feature.)
Table 1 Presenting features of people with coeliac disease
Feature People withthe feature
Adults/children Studies
Iron-deficiencyanaemia
39.3%
25%
11.7%
adults and children
adults
adults and children
Bottaro 1999
Brandimarte 2002
Emami 2008
Other or unspecifiedanaemia
16%
3 to19%
3.0 to 12.7%
23.3%
adults and children
children
adults
older adults
Dickey 1997
Garampazzi 2007
Rampertab 2006
Vilppula 2008
Anorexia 7.8 %
25.6 to 35.1%
adults and children
children
Bottaro 1999
Bottaro 1993
Weight loss 43.6 to 59.6%
6%
15.6%
16.7%
children
adults and children
adults
older adults
Bottaro 1993
Dickey 1997
Hopper 2008
Vilppula 2008
Abdominal
distension/bloating
28.4 to 35.8%
10%20 to 39%
children
adults and childrenchildren
Bottaro 1993
Emami 2008Garampazzi 2007
Abdominal pain 12%
8.2%
11 to 21%
adults and children
adults and children
children
Dickey 1997
Emami 2008
Garampazzi 2007
Abdominalpain/distension/flatulence
31.7% older adults Vilppula 2008
Vomiting 26.1 to 32.5% children Bottaro 1993
Flatulence 5.4% adults and children Emami 2008
Diarrhoea 70.2 to 75.2%
51%
13.1%
12 to 60%
42.9%
37.2 to 91.3%
25%
children
adults and children
adults and children
children
adults
adults
older adults
Bottaro 1993
Dickey 1997
Emami 2008
Garampazzi 2007
Hopper 2008
Rampertab 2006
Vippula 2008
Short stature/growthfailure
19.2%
20.2 to 30.8%
adults and children
children
Bottaro 1999
Bottaro 1993
Irritability 10.3 to 13.9% children Bottaro 1993Alopecia 10% adults Brandimarte 2002
-
7/31/2019 3.-Enfermedad Celiaca
28/86
Nice clinical guideline 86 Coeliac disease 28
Feature People withthe feature
Adults/children Studies
Osteoporosis 6% adults Brandimarte 2002
Recurrent aphthousstomatitis
6% adults Brandimarte 2002
Amenorrhoea/recurrent abortion
6% adults Brandimarte 2002
Hypertransaminase-aemia
6% adults Brandimarte 2002
Abnormal liverbiochemistry
5% adults and children Dickey 1997
Chronic fatigue 7%
8.3%
adults and children
older adults
Dickey 1997
Vilppula 2008
Failure to thrive 48 to 89% children Garampazzi 2007
Constipation 4 to 12% children Garampazzi 2007
Irregular bowel habits 4 to 12% children Garampazzi 2007
Three further studies considered a specific symptom or presentation and the
percentage of those presenting with it who also had coeliac disease:
Karnam et al. (2004) considered adults who were undergoing endoscopy
for iron-deficiency anaemia and found 3 of 105 people (2.9%) had coeliac
disease.
Imanzadeh et al. (2005) considered children with small bowel type chronic
diarrhoea and found that 54 of 825 people (8.96%) had coeliac disease.
Sanders et al. (2005) considered adults with acute abdominal pain and
found that 9 of 300 people (3%) had coeliac disease. In people with non-
specific abdominal pain 10.5% had coeliac disease.
Some people presenting with the features of coeliac disease in the studiessummarised in table 1 had a coexisting condition at the point of diagnosis of
coeliac disease:
dermatitis herpetiformis 10%, Brandimarte 2002 (adults); 1%, Dickey
1997 (adults and children)
irritable bowel syndrome 20.2%, Emami 2008 (adults and children)
liver disorder 0.85%, Emami 2008 (adults and children)
rheumatological disorder 0.28%, Emami 2008 (adults and children)
-
7/31/2019 3.-Enfermedad Celiaca
29/86
Nice clinical guideline 86 Coeliac disease 29
Crohns disease 0.57%, Emami 2008 (adults and children)
bone disease 0 to15%, Rampertab 2006 (adults)
malignancy 5 to 21.7%, Rampertab 2006 (adults).
2.4.2 Evidence review coexisting conditions
The studies included for this review considered coexisting conditions
associated with coeliac disease up to and including the point of it being
diagnosed. Studies that considered subsequent development of conditions in
people who had been diagnosed with coeliac disease were excluded. The
relationship between the coexisting conditions and coeliac disease here is not
considered to be causal; the aim was to examine whether people with certain
conditions have a higher rate of coeliac disease than the general population.
Papers in which there was a substantial discrepancy between numbers of
people who had serological tests and numbers of people who had biopsies
were excluded, because of the possibility that results could be biased if not all
those with positive serology had a biopsy.
Type 1 diabetes
The AHRQ report included papers on the prevalence of coeliac disease inpeople with type 1 diabetes; 21 of these studies (people with coeliac disease
proven by biopsy; each had 50 or more participants) were included here.
These studies identified a prevalence of coeliac disease in people with type 1
diabetes of 1.4 to 8.2% in children, 0.3 to 11.3% in adults and 1.7 to 5.7% in
combined child and adult studies. Two additional papers also considered
people with type 1 diabetes: one in children reported that 6.6% had coeliac
disease (Salardi et al. 2008) and one in adults reported that 6.4% had coeliac
disease (Picarelli et al. 2005).
Other conditions
Papers were included that considered cohorts of people with specified other
conditions who were tested for coeliac disease (see table 2).
-
7/31/2019 3.-Enfermedad Celiaca
30/86
Nice clinical guideline 86 Coeliac disease 30
Table 2 Coexisting conditions and coeliac disease
Condition Study participants Participants withcoeliac disease
Study authorand year
Arthritis 160 adults with rheumatoidarthritis
0.63% Francis 2002
62 children with juvenilechronic arthritis
1.5% George 1996
119 children with juvenilechronic arthritis
2.5% Lepore 1996
Autoimmunethyroid
136 adults withautoimmune thyroiditis
2.9% Guliter 2007
152 adults withautoimmune thyroiddisease
3.29% Sategna-Guidetti 1998
Down
syndrome
1453 children and adults 4 (0.3%), adjusted risk
ratio 4.7 (95% CI 1.3to 12.2)
Goldacre 2004
1110 children, 92 adults 55 (4.6%) Bonamico 2001
Epilepsy 255 children and adults 2 (0.8%) Pratesi 2003
177 adults 1:44 (2.3%) Cronin 1998
Inflammatoryboweldisease
354 adults (173 Crohnsdisease, 154 ulcerativecolitis, 27 other conditions)
0.85% Leeds 2007
Irritable bowelsyndrome
300 adults OR 7 (95% CI 1.7 to28.0)
Sanders 2001
Liver disease 624 adults with chronichepatitis C
0% Thevenot 2007
738 children and adultswith chronic liver disease
1:185 (0.45%) Germenis 2005
57 adults with primarybiliary cirrhosis
7% Dickey 1997
Lymphoidmalignancy
298 adults 0.67% Farre 2004
Myocarditis 187 adults withautoimmune myocarditis
4.4% (p < 0.003 vs.control group)
Frustaci 2002
Sjgren'ssyndrome
111 adults 4.54% Szodoray 2004
Subfertility 99 women 3.03%(p = 0.037unexplained infertilityvs. control group)
Meloni 1999
150 women 2.7% all unexplainedinfertility (p = 0.06 vs.control group)
Collin 1996
Turnersyndrome
389 children and adults 25 (6.4%) Bonamico 2002
-
7/31/2019 3.-Enfermedad Celiaca
31/86
Nice clinical guideline 86 Coeliac disease 31
One study was also included that identified the existing conditions of people at
the point of diagnosis of coeliac disease (Collin et al. 1994). Also included
were studies in which logistical regression had been used to investigate
coeliac disease that developed following a prior history of a coexisting
condition (see table 3).
Table 3 Coexisting conditions and coeliac disease
Study group:peoplewith newlydiagnosed coeliacdisease
Coexisting conditions
335 adults (335control group)
(figures are givenfor study groupfirst, control groupsecond)
(Collin 1994)
Endocrine disorders: 12% (study group) vs. 4.2% (control group),p = 0.0003
insulin dependent diabetes 18 (5.4%) vs. 5 (1.5%),p = 0.0094
autoimmune thyroid 18 (5.4%) vs. 9 (2.7%)
Connective tissue disorder: 7.2% vs. 2.7%, p = 0.011
Sjgren's syndrome 11 (3.3%) vs. 1 (0.3%), p = 0.0059
rheumatoid arthritis 6 (1.8%) vs. 7 (2.1%)
Pulmonary disorders:
asthma 9 vs. 12
sarcoidosis 5 vs. 0
Neurological disorders: epileptic seizures 5 vs. 3
dementia 5 vs. 1
Liver diseases: 4 vs. 0
14,349 adults andchildren (69,998control)(Ludvigsson 2007a)
Increased risk of coeliac disease in those with prior sarcoidosisOR 3.58, 95% CI 1.98 to 6.45, p < 0.001
14,371 adults andchildren (70,096control)
(Ludvigsson 2007b)
Increased risk of coeliac disease in those with priorpolyneuropathy OR 5.4, 95% CI 3.6 to 8.2, p < 0.001
Other neurological diseases were not associated withsubsequent coeliac disease
13,776 adults andchildren (66,815control)(Ludvigsson 2007c)
Increased risk of coeliac disease in those with history of mooddisorder:
prior depression OR 2.3, 95% CI 2.0 to 2.8, p < 0.001
prior bipolar disorder OR 1.7, 95% CI 1.2 to 2.3, p = 0.001
-
7/31/2019 3.-Enfermedad Celiaca
32/86
Nice clinical guideline 86 Coeliac disease 32
Study group:peoplewith newlydiagnosed coeliacdisease
Coexisting conditions
13,818 adults and
children (66,584control)(Ludvigsson 2007d)
Increased risk of coeliac disease in those with history of liver
disorder: acute hepatitis OR 4.98, 95% CI 1.59 to 12.06, p = 0.004
chronic hepatitis OR 5.79, 95% CI 3.13 to 10.70,p < 0.001
primary sclerosing cholangitis OR 4.42, 95% CI 2.38 to8.24, p < 0.001
fatty liver OR 5.83, 95% CI 1.96 to 17.36, p < 0.002
ascites OR 5.00, 95% CI 2.08 to 12.01, p < 0.001
liver failure, extended OR 5.88, 95% CI 4.05 to 8.54,p < 0.001
liver failure, restricted OR 8.33, 95% CI 1.99 to 34.87,p < 0.004
liver cirrhosis/fibrosis OR 5.83, 95% CI 3.86 to 8.81,p < 0.001
primary biliary cirrhosis OR 15.00, 95 %CI 4.84 to 46.51,p < 0.001
hepatomegaly OR 2.00 (95% CI 0.39 to 10.31) notsignificant
14,335 children andadults (69,888
control)(Ludvigsson 2007e)
Increased risk of coeliac disease in those with prior tuberculosis:
OR 2.5, 95% CI 1.75 to 3.55, p < 0.001
15,533 children andadults (14,491inpatient referencecontrols)(Ludvigsson 2008)
Increased risk of coeliac disease in those with prior sepsis
OR 2.2, 95% CI 1.7 to 3.0, p < 0.001
14,366 children andadults (70,095control)
(Elfstrm 2007)
Increased risk of coeliac disease in those with prior Addison'sdisease OR 8.6, 95% CI 3.4 to 21.8
14,347 adults andchildren (69,967control) (Olen2008)
Increased risk of coeliac disease in those with history ofthrombocytopenia purpura OR 2.96, 95% CI 1.60 to 5.50, p= 0.001; and those with prior chronic thrombocytopenia purpuraOR 6.00, 95% CI 1.83 to 19.66, p = 0.003
2.4.3 Evidence statements
In children and adults, coeliac disease can present with a broad range of
signs and symptoms. The most frequent are:
abdominal pain, cramping or distension
chronic or intermittent diarrhoea
-
7/31/2019 3.-Enfermedad Celiaca
33/86
Nice clinical guideline 86 Coeliac disease 33
failure to thrive or faltering growth in children
fatigue
iron-deficiency anaemia
nausea or vomiting weight loss.
The following findings may also be present when coeliac disease is
diagnosed:
abnormal liver biochemistry
alopecia
amenorrhoea
aphthous stomatitis (mouth ulcers)
constipation
dermatitis herpetiformis
epilepsy
microscopic colitis
osteoporosis
recurrent abortion
type 1 diabetes.
There is good evidence that coeliac disease has an increased prevalence in
people with:
autoimmune thyroid disease (up to 7%)
irritable bowel syndrome (up to 7%)
type 1 diabetes (210%).
There is some evidence that coeliac disease has an increased prevalence in
people with:
autoimmune myocarditis
chronic thrombocytopenic purpura
depression/bipolar disorder
Downs syndrome
-
7/31/2019 3.-Enfermedad Celiaca
34/86
Nice clinical guideline 86 Coeliac disease 34
epilepsy
liver conditions
lymphoid malignancy
polyneuropathy Sjgren's syndrome
sarcoidosis
Turner syndrome
unexplained subfertility.
2.4.4 Linking evidence to recommendations
The GDG discussed the evidence and agreed the evidence statements
relating to the signs and symptoms of coeliac disease and the coexisting
conditions, and developed recommendations. This discussion is summarised
here:
The GDG agreed that there were certain signs and symptoms and
coexisting conditions (as well as the known risk factor of being a first-
degree relative of a person with coeliac disease) that are sufficiently
associated with coeliac disease that people with them should be offered
serological testing, and developed recommendations to reflect this. The
GDG discussed the historic division of symptoms into gastrointestinal and
non-gastrointestinal and concluded that it would be more beneficial to
identify the overall signs and symptoms for which testing would be
recommended. The GDG further discussed the non-specific nature of many
of the signs and symptoms and consequently added 'unexplained' and
'chronic' to the description of some signs and symptoms to ensure thatpeople who may have coeliac disease are identified.
The GDG agreed a list of further signs, symptoms and coexisting
conditions for which they wanted to raise awareness of the link with coeliac
disease. Therefore recommendations were developed that identified where
offering serological testing for coeliac disease should be considered.
The GDG discussed weight loss as a feature of coeliac disease and noted
that, although weight loss can be a symptom of coeliac disease, thetraditional view of a patient with coeliac disease being underweight is no
-
7/31/2019 3.-Enfermedad Celiaca
35/86
Nice clinical guideline 86 Coeliac disease 35
longer true and that patients may present underweight, at a normal weight
or overweight.
Recommendation 1.1.1
Offer serological testing for coeliac disease to children and adults with any of
the following signs and symptoms:
chronic or intermittent diarrhoea
failure to thrive or faltering growth (in children)
persistent or unexplained gastrointestinal symptoms including nausea and
vomiting
prolonged fatigue (tired all the time) recurrent abdominal pain, cramping or distension
sudden or unexpected weight loss
unexplained iron-deficiency anaemia, or other unspecified anaemia.
Recommendation 1.1.2
Offer serological testing for coeliac disease to children and adults with:
any of the following conditions: autoimmune thyroid disease
dermatitis herpetiformis
irritable bowel syndrome
type 1 diabetes
or
first-degree relatives (parents, siblings or children) with coeliac disease.
-
7/31/2019 3.-Enfermedad Celiaca
36/86
Nice clinical guideline 86 Coeliac disease 36
Recommendation 1.1.3
Consider offering serological testing for coeliac disease to children and adults
with any of the following:
Addison's disease
amenorrhoea
aphthous stomatitis (mouth ulcers)
autoimmune liver conditions
autoimmune myocarditis
chronic thrombocytopenia purpura
dental enamel defects
depression or bipolar disorder
Downs syndrome
epilepsy
low-trauma fracture
lymphoma
metabolic bone disease (such as rickets or osteomalacia)
microscopic colitis
persistent or unexplained constipation
persistently raised liver enzymes with unknown cause
polyneuropathy
recurrent miscarriage
reduced bone mineral density
sarcoidosis
Sjgren's syndrome
Turner syndrome
unexplained alopecia
unexplained subfertility.
Recommendation 1.1.4
Do not use serological testing for coeliac disease in infants before gluten has
been introduced to the diet.
-
7/31/2019 3.-Enfermedad Celiaca
37/86
Nice clinical guideline 86 Coeliac disease 37
2.5 Serological tests in the diagnostic process for coeliac
disease
2.5.1 Evidence review information for patients before testing
The search strategy was designed to identify any studies that relate
specifically to the information needs and support of patients and parents or
carers before the diagnosis of coeliac disease. No studies were identified.
2.5.2 Evidence review serological tests
This review incorporated studies that included a blood sample drawn from
children or adults suspected of having coeliac disease. This suspicion may
have been based on clinical symptoms, an existing condition (such as type 1
diabetes) or having a first-degree relative with coeliac disease. The included
studies were mainly cohort studies, which provided the best quality evidence.
The data were synthesised and are presented in the form of forest plots and
receiver operating characteristic (ROC) curves (see appendix 6.3). Summary
statistics have not been included because the studies were not considered
homogenous, the methodology for the meta-analysis of diagnostic studies is
not clear and expert opinion in this area varies. Within the studies different kits
and different cut-off values were used for the analysis2
IgA AGA
. Further differences
between studies were different or incompletely reported biopsy strategies,
possible variability between laboratories or operators, the use of different
samples or studies taking place in several different countries.
The serological tests considered for this review were:
IgG AGA
IgA EMA
IgG EMA
IgA tTGA
IgG tTGA.
2If studies used different cut-off levels, the data used were that of the manufacturers
recommended cut-off levels.
-
7/31/2019 3.-Enfermedad Celiaca
38/86
Nice clinical guideline 86 Coeliac disease 38
Table 4 summarises the studies, total participants, test methods (enzyme-
linked immunosorbent assay [ELISA] or diffusion in gel [DIG]) and substrate
used for EMA (human umbilical cord [HU] or monkey oesophagus [ME]) and
for tTGA (human recombinant [HR] or guinea pig [GP]) in the included studies.
Table 4 Summary of serological test studies
Serologicaltest
Number ofstudiesincludingthis test
Totalparticipants
Methods
IgA AGA 31 5600 24 used ELISA, 5 used DIG-ELISA, 1used immunohistochemistry, 1 usedimmunofluorescence
IgG AGA 25 4820 20 used ELISA, 3 used DIG-ELISA, 1used immunohistochemistry, 1 usedimmunofluorescence
IgA EMA ME 21 5265 18 used immunofluorescence, 2 usedELISA, 1 used DIG-ELISA, 1 unknown
IgA EMA HU 3 264 3 used immunofluorescence
IgG EMA ME 1 89 1 used immunofluorescence
IgA tTGA GP 8 946 8 used ELISA
IgA tTGA HR 11 3853 9 used ELISA, 1 used radiobindingassay, 1 unknown
IgG tTGA GP 1 111 1 used ELISA
IgG tTGA HR 1 254 1 unknown
IgA deficiency
People with IgA deficiency will have a false negative result if IgA-based
serological tests are used in the diagnosis of coeliac disease. It has been
suggested that there has been inadequate evaluation of IgA deficiency while
testing for coeliac disease, which has resulted in the underdiagnosis of both
(McGowan et al. 2008). Therefore, this guideline also considered the use of
IgA-deficiency testing and IgG-based serological testing in the diagnostic
process for coeliac disease.
Included studies
All studies considered people with suspected coeliac disease who had one of
the included serological tests and had coeliac disease confirmed by biopsy.
There were 29 studies included from the AHRQ (2004) report, 18 in children
-
7/31/2019 3.-Enfermedad Celiaca
39/86
Nice clinical guideline 86 Coeliac disease 39
(Altuntas et al. 1998; Artan et al. 1998; Ascher et al. 1996; Bahia et al. 2001;
Bode et al. 1993; Chan et al. 2001; Chartrand et al. 1997; Chirdo et al. 1999;
Iltanen et al. 1999; Kumar et al. 1989; Lindberg et al. 1985; Lindquist et al.
1994; Maki et al. 1991; Meini et al. 1996; Poddar et al. 2002; Rich et al. 1990;
Russo et al. 1999; Wolters et al. 2002), seven in adults (Bardela et al. 2001;
Bode et al. 1994; Carroccio et al. 2002; Kaukinen et al. 2000; McMillan et al.
1991; Valdimarss et al. 1996; Vogelsang et al. 1995) and four in children and
adults (Carroccio et al. 2002; Gonczi et al. 1991; Tesei et al. 2003; Troncone
et al. 1999). A further 14 studies were identified from the search, four in
children (Del Rosario et al. 1998; Liu et al. 2003 and 2005; Viola et al. 2004),
six in adults (Abrams et al. 2006; Hopper et al. 2008; Johnston et al. 2003;
Kocna et al. 2002; Niveloni et al. 2007; Reeves et al. 2006) and four in
children and adults (Carroccio et al. 2006; Dickey et al. 1997; Emami et al.
2008; Rostami et al. 1999). The largest of the additional studies was based in
the UK and included a cohort of 2000 adults, 77 of whom were diagnosed with
coeliac disease, and included data on IgA/IgG AGA, IgA tTGA and IgA EMA
with biopsy (Hopper et al. 2008).
-
7/31/2019 3.-Enfermedad Celiaca
40/86
Nice clinical guideline 86 Coeliac disease 40
Table 5 Sensitivity/specificity of serological tests for coeliac disease
Serologicaltest
Studies Sensitivity Specificity
IgA AGA 31 studies (5600participants)
18 child studies
10 adult studies
3 child/adult studies
Range 23 to100%
(adults 46 to 100%)(children 23 to100%)
Range 45 to100%
(adults 45 to 100%)(children 51 to 99%)
IgG AGA 25 studies (4830participants)
15 child studies
8 adult studies
2 child/adult studies
Range 46 to 100%
(adults 22 to 100%)
(children 71 to100%)
Range 77 to 99%
(adults 41 to 97%)
(children 38 to 99%)
IgA EMA 23 studies (5529
participants)10 child studies
9 adult studies
4 child/adult studies
Range 68 to 100%
(adults 68 to 100%)(children 46 to100%)
Range 89 to 100%
(adults 94 to 100%)(children 77 to 100%)
IgG EMA 1 adult study (89participants)
Sensitivity 39% Specificity 98%
IgA tTGA 19 studies (4799participants)
6 child studies
9 adult studies
4 child/adult studies
Range 38 to 100%
(adults 71 to 100%)
(children 89 to100%)
Range 25 to 100%
(adults 65 to 100%)
(children 25 to 100%)
IgG tTGA 2 studies (365participants)
1 adult study
1 child/adult study
Sensitivity 23 to85%
Specificity 89 to 98%
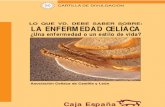
The overall efficacy of the IgA AGA, IgA EMA and IgA tTGA serological tests
was summarised in forest plots and ROC curves (see appendix 6.3). The
ROC curves below show the overall results for the IgA AGA, tTGA and EMA
tests. They show a lower level of accuracy for the IgA AGA than the other
tests, with both IgA EMA and IgA tTGA identified as having high levels of both
sensitivity and specificity. For AGA the IgA serological tests results appeared
to show higher sensitivity and specificity than the IgG tests. For IgG tTGA and
IgG EMA there were insufficient data available to draw reasonable
conclusions.
-
7/31/2019 3.-Enfermedad Celiaca
41/86
Nice clinical guideline 86 Coeliac disease 41
L eg endIg A AGAIg A EMAIg A tTG
00 .10 .20 .30.40.50.60.70.80 .910
0 .1
0 .2
0 .3
0 .4
0 .5
0 .6
0 .7
0 .8
0 .9
1
S pe cific ity
Se nsit ivit y
Figure 1 IgA overall results for anti-gliadin antibodies, anti-endomysialantibodies and anti tissue transglutaminase antibodies
Combined and sequence testsA small number of papers considered the sensitivity and specificity of test
combinations or sequencing of tests. One large UK study in adults (Hopper et
al. 2008) considered the use of IgA tTGA and EMA. This study identified
improvements in positive predictive value (PPV) and some small differences
in sensitivity, specificity and negative predictive value (NPV) if both tests were
used, either in a two-step process or simultaneously, compared with if tests
were completed individually.
A second UK-based paper (Johnston et al. 2003), also in adults, considered
the results if either IgA tTGA or EMA were positive. Positive results for either
test gave a lower PPV than was found with each test individually, and a higher
NPV than IgA tTGA.
A paper from the Czech Republic (Kocna et al. 2002) considered a two-step
screening algorithm and identified IgA/IgG AGA to be the least accurate
-
7/31/2019 3.-Enfermedad Celiaca
42/86
Nice clinical guideline 86 Coeliac disease 42
first-step marker if it is followed by biopsy, with IgA EMA the most accurate
first-step marker if it is followed by IgA tTGA.
Three studies in the AHRQ report considered the use of IgA/IgG AGA
together or each individually; they did not find the combination results to be
notably different from the individual tests.
Human leukocyte antigen tests
Coeliac disease has a genetic association with certain types of type II human
leukocyte antigens (HLA); HLA DQ2 is found in 95% of people with coeliac
disease and HLA DQ8 in most of the remaining 5%. No studies identified by
the searches considered the sensitivity and specificity of the HLA DQ2 and
DQ8 tests in coeliac disease. The AHRQ report identified papers that
considered the prevalence of HLA DQ2 and DQ8 in a population of people
with coeliac disease, but these studies were not designed to determine the
diagnostic utility of HLA DQ2 or DQ8. Three studies in the AHRQ report were
completed in people with biopsy-proven coeliac disease; these had sensitivity
results of 87 to 90% and specificity of 70 to 81%.
AgeROC curve analysis categorising studies into those with child participants,
those with adult participants and those with mixed (child and adult)
participants reflected the overall analysis, with both IgA EMA and IgA tTGA
(there is insufficient evidence for IgG in either test to plot on the curves)
showing considerably higher levels of sensitivity and specificity than IgA or
IgG AGA.
One study (Viola 2004) also considered IgA AGA, IgA EMA and IgA tTGA
results in children 2 years and younger and those older than 2 years. It found
similar results in both age categories for IgA tTGA and for IgA EMA.
-
7/31/2019 3.-Enfermedad Celiaca
43/86
Nice clinical guideline 86 Coeliac disease 43
Subgroups
The search for this question was designed to identify studies in which there
was evidence that the serological tests for coeliac disease performed in any
way differently from the general population. The only areas in which studies
were identified were liver disease and IgA deficiency.
Liver disease: one study of 105 participants who had primary biliary
cirrhosis reported a specificity range for IgA tTGA of 82.5 to 97.1% and
95.1 to 100% for IgG tTGA (Bizzaro et al. 2006). The authors noted that
with almost all the antibody concentrations IgA tTGA was close to the cut-
off level, and that positive results were inconsistent between the test kits.
They identified a concern about the false-positive rate with IgA tTGA testing
in people with primary biliary cirrhosis, although only six participants had
biopsies.
IgA deficiency: one paper was identified that considered the use of IgG
AGA and IgG tTGA tests in 126 children with IgA deficiency (Lenhardt et al.
2004). Eleven were diagnosed with coeliac disease: all were IgG tTGA
positive and five were also IgG AGA positive, this suggests that IgG tTGA
is more accurate than IgG AGA in children with IgA deficiency.
Newer tests
Deamidated gliadin
Two papers were included that considered the use of deamidated gliadin
peptide (DGP)-based assays as a diagnostic tool for coeliac disease. The first
paper considered the use of IgA and IgG antibodies to synthetic DGP and
tTGA in 176 children (Agardh et al. 2007) and found 119 (68%) with coeliac
disease.
-
7/31/2019 3.-Enfermedad Celiaca
44/86
Nice clinical guideline 86 Coeliac disease 44
Table 6 Sensitivity and specificity results for deamidated gliadin (Agardhet al. 2007)
Antibody Sensitivity Specificity PPV NPV
IgA/G DGP/tTGA 100% 94.7% 97.5% 100%
IgA/G DGP 97.5% 98.2% 99.1% 94.9%IgA DGP 90.8% 94.7% 97.3% 83.1%
IgG DGP 95.0% 98.2% 99.1% 90.3%
IgA tTGA 96.6% 100% 100% 93.4%
IgG tTGA 12.6% 100% 100% 35.4%
The second study considered 141 adults and used IgA tTGA and IgA/IgG
DGP; 60 were diagnosed with coeliac disease (Niveloni et al. 2007).
Table 7 Sensitivity and specificity results for deamidated gliadin(Niveloni et al. 2007)
Antibody Sensitivity Specificity PPV NPV
IgA DGP 98.3% 93.8% 92.2% 98.7%
IgG DGP 96.7% 100% 100% 97.6%
IgA + IgG DGP 98.3% 98.8% 98.3% 79.6%
IgA tTGA 95.0% 97.5% 96.6% 96.3%
IgA DGP + tTGA 100% 97.5% 96.7% 100%
IgG DPG + IgA tTGA 100% 97.5% 96.7% 100%
IgA+IgG DGP + tTGA 100% 96.3% 95.2% 100%
Results for both of these studies using deamidated gliadin peptide showed
sensitivity and specificity values similar to those found with tTGA.
-
7/31/2019 3.-Enfermedad Celiaca
45/86
Nice clinical guideline 86 Coeliac disease 45
Immunochromatographic sticks
One paper was included that considered the use of immunochromatographic
sticks3
IgA/G tTGA (tTG stick): children sensitivity 97%, specificity 98%; adults
sensitivity 83%, specificity 100%
for tissue transglutaminase and antigliadin antibody screening in 286
children and 49 adults (Ferre-Lopez et al. 2004); 142 (51%) children and 30
(61%) adults were diagnosed with coeliac disease. Sensitivity and specificity
results for immunochromatographic sticks were broadly similar to those from
the ELISA method:
IgA tTGA (tTG-AGA stick): children sensitivity 96%, specificity 98%; adults
sensitivity 80%, specificity 100%
IgA AGA (tTG-AGA stick): children sensitivity 89%, specificity 96%; adults
sensitivity 83%, specificity 100%
IgA tTGA + AGA (stick, one test): children sensitivity 99%, specificity 95%;
adults sensitivity 86%, specificity 100%.
2.5.3 Evidence statements
The IgA tTGA and IgA EMA serological tests show high levels of sensitivityand specificity in the diagnostic process for coeliac disease.
Gliadin antibody serological tests show lower levels of sensitivity and
specificity than tTGA and EMA.
Based on limited clinical evidence, combination testing with IgA tTGA and IgA
EMA does not appear to substantially to improve accuracy in the diagnostic
process.
There is limited evidence that IgA tTGA yields more false positive results in
people with liver disease than in the general population.
Serological tests have comparable accuracy in children and in adults.
Newer tests for deamidated gliadin may be useful but require further
evaluation.
3Can be used for self-test or point of care testing.
-
7/31/2019 3.-Enfermedad Celiaca
46/86
Nice clinical guideline 86 Coeliac disease 46
Limited evidence suggests that point-of-care tests and self tests may be
accurate but require further evaluation.
HLA DQ2 or DQ8 is present in approximately 25% of the UK population so a
positive test has no predictive value, but a negative test can exclude a
diagnosis of coeliac disease.
2.5.4 Health economics
Published health economics material
A literature review was conducted to identify evidence on the cost-
effectiveness of serological tests for coeliac disease.
Several potentially useful studies were identified (Atkinson et al. 1997;
Dretzke et al. 2004; Dorn et al. 2007; Harewood and Murray 2001; Hopper et
al. 2008; Mein and Ladabaum et al. 2004; Shamir et al. 2006; Spiegel et al.
2004; Swigonski et al. 2008; Yagil et al. 2005). The studies by Atkinson et al.
(1997) and Harewood and Murray (2001) were cost-minimisation studies that
compared serological test strategies with biopsy for diagnosing coeliac
disease. Dorn et al. (2007), Hopper et al. (2008) and Yagil et al. (2005) used
cost-effectiveness analysis to examine the costs and diagnostic accuracy of
serological tests for coeliac disease. Dorn et al. (2007) also examined the cost
effectiveness of HLA testing. Mein and Ladabaum (2004) and Spiegel et
al. (2004) examined the cost effectiveness of testing people with irritable
bowel syndrome for coeliac disease. Shamir et al. (2006) examined a
population screening approach in the adult population and Swigonski et al.
(2008) examined the cost effectiveness of screening for coeliac disease in
children with Downs syndrome, with the specific aim of preventing lymphoma.
None of the 10 papers examining the cost effectiveness of serological tests for
coeliac disease was considered directly applicable to this guideline. However,
one UK study (Dretzke et al. 2004) examined serological tests and used
quality-adjusted life-years (QALYs) as an outcome measure, so was reviewed
in detail for this guideline. The remaining papers were used to explore
previous approaches to modelling serological test strategies and to inform the
structure of the model but were not quality-assessed or reviewed in detail for
-
7/31/2019 3.-Enfermedad Celiaca
47/86
Nice clinical guideline 86 Coeliac disease 47
this guideline because they did not include health-related quality-of-life
outcomes and/or were not based in the UK.
A full data extraction form for Dretzke et al. (2004) is available in appendix 6.5
and the techniques from that study (2004) have been examined alongside
careful consideration of the modelling methods used by the other studies
identified in the review.
Summary of Dretzke et al. (2004)
Dretzke et al. (2004) is a full health technology assessment (HTA) of
autoantibody testing in children with newly diagnosed type 1 diabetes. It
includes an economic model to quantify the costs and benefits of screening
for coeliac disease at the time of diagnosis of diabetes. The assessment took
place because of the variation in practice of screening for autoantibodies
associated with coeliac disease in this population.
Six possible screening strategies were compared:
no screening
biopsy of all children
single autoantibody test confirmed by biopsy in those testing positive
combination of autoantibody tests confirmed by biopsy in those testing
positive
single autoantibody test without confirmatory biopsy
combination of autoantibody tests without confirmatory biopsy.
The authors were clear that not all of these strategies are used in current
clinical practice, although all strategies were included for completeness. The
analysis took an NHS perspective, with costs and outcomes modelled over a
lifetime.
The prevalence of undiagnosed coeliac disease in children with diabetes was
estimated from the literature. The effectiveness estimates for the serological
tests were taken from the authors systematic review outlined in the report.
The tests considered were IgA AGA, IgG AGA, IgA EMA, IgA ARA and IgA
tTGA. Other tests were excluded because too few studies were found. The
-
7/31/2019 3.-Enfermedad Celiaca
48/86
Nice clinical guideline 86 Coeliac disease 48
values used in the model were taken from the summary ROC curves
presented in the clinical section of Dretzke et al. (2004) for each test at the
point at which sensitivity and specificity were equal. This is called the Q point.
For combination tests the authors assumed that the results of the tests were
independent and clearly set out the method of calculating sensitivity and
specificity for combination strategies. Adherence to a gluten-free diet was
included in the model, as was the proportion of patients who would have
received a later diagnosis through normal clinical routes if they had not been
previously picked up by screening. The delay to diagnosis for these patients
was included, with associated costs and utilities for undiagnosed coeliac
disease. The authors assumed that the delay to diagnosis was 5 years in the
base case.
Utility estimates (quality of life weights) and assumptions were informed by
existing literature. Studies on quality of life of treated and untreated coeliac
disease were searched and reviewed. Utilities could not be derived directly
from the studies identified. Estimates of the utility of treated and untreated
coeliac disease, and of the disutility of endoscopy, biopsy and gluten-free diet
were derived from the literature and assumptions.
Costs were estimated for serological tests, endoscopy and biopsy, and gluten-
free diet. Personal communication was used to evaluate the costs of the
serological tests; this is likely to be because of the absence of a national tariff
for diagnostic tests (such as the British National Formulary for drug prices).
All strategies were compared with a no-screening strategy. The lowest cost
per QALY gained was for a positive IgA EMA with confirmatory biopsy, with anincremental cost-effectiveness ratio of 12,250 per QALY gained compared
with no screening. The least cost-effective strategies were those using IgG
AGA tests alone or in combination with other autoantibody tests. The authors
reported that the results were sensitive to the disutility of being on a gluten-
free diet, the cost of gluten-free diet, the differences in utilities between health
states and the reduction in life expectancy as a result of coeliac disease.
-
7/31/2019 3.-Enfermedad Celiaca
49/86
Nice clinical guideline 86 Coeliac disease 49
An important limitation of this study is that the authors do not present the
costs and QALYs separately in the results section. This makes it difficult to
determine whether costs or QALYs have the most influence on the
incremental cost-effectiveness ratio. Limitations of the individual input
parameters are discussed throughout the methods section, but the discussion
does not address limitations of the overall model.
De novo economic model
In summary, there is evidence on the cost effectiveness of serological tests for
various patient populations and country settings; however, there is a lack of
evidence for the cost effectiveness of serological tests for the patient
population of direct relevance to this guideline.
Because of the lack of published economic evidence that fully addresses the
cost effectiveness of serological testing in the decision-making context of this
guideline, the GDG requested the development of a de novo model. Any cost-
effectiveness analysis carried out should also examine the costs and
consequences of the outcomes of diagnosis. Although it is outside the scope
of this guideline to make recommendations on the treatment or management
of coeliac disease, the economic evaluation considers the costs and benefits
of current standard practice after diagnosis of coeliac disease. This allows us
to include the long-term consequences of testing, along with the costs and
consequences of incorrect diagnosis.
A model was developed to estimate the cost effectiveness of serological test
strategies for detecting coeliac disease in patients presenting with signs and
symptoms. The model was built and analysed using TreeAge Pro 2007 Suite(TreeAge software) and adopted a lifetime horizon. Several test strategies
were examined and compared with a no-test strategy (see table 8). The
structure of the decision tree was agreed with the GDG and was also informed
by previous cost-effectiveness studies. Patients accrued costs and utilities
depending on their pathway through the model. At the end of the decision
tree, patients entered a Markov model with states reflecting their eventual
diagnosis (that is, diagnosed as having coeliac disease, no diagnosis of
-
7/31/2019 3.-Enfermedad Celiaca
50/86
Nice clinical guideline 86 Coeliac disease 50
coeliac disease or undiagnosed coeliac disease) and picked up costs and
utilities linked with these states until death.
Serological tests examined in the model were the IgA tTGA and the IgA EMA
tests. These were analysed alone and in combination. In all cases, tests were
followed by biopsy to confirm positive results. Strategies with separate IgA
deficiency testing were also included. For completeness a no-test strategy
and a biopsy-only strategy wer