SURGERY ULCERATION AND ITS COMPLICATIONS · tional forms maymimic ulcer dyspepsia, make it unsafe...
14
SURGERY AND OF PEPTIC ULCERATION ITS COMPLICATIONS BY NORMAN C. TANNER, M.D., F.R.C.S . The three Lettsomian Lectures delivered at the Medical Society of London on February I5, 24 and March I, I954- (They will be published in this and the next two numbers of the journal.) Part I LECTURE ONE Gastric and Duodenal Ulceration. Operative Methods. Results of Operation I am greatly honoured by your invitation to me to deliver the lectures in memory of John Coakley Lettsom. It is only nine years since my distinguished pre- decessor, Sir Gordon Gordon-Taylor, delivered the Lettsomian Lecture on the subject of haemor- rhage from peptic ulcer (Gordon-Taylor, 1945). I shall have little of value to add to his words on this aspect except to record diminished mortality figures, largely as a result of the policies he then advocated to us. I shall discuss the subject widely and can therefore only touch lightly on certain aspects, though I shall prod more heavily in certain places where it may do good. Selection for Surgery Twenty to thirty years ago there was more dis- agreement among clinicians on the selection of 'cases for surgical treatment. In those days the physician tended to find it one of his functions to save the patient from the surgeon. The patient who arrived at the surgical outpatients' clinic with an ulcer sometimes found that his only course of medical treatment was a packet of alkaline powder to take while awaiting admission for operation! Nowadays the position has changed. The physician is almost more ready than the surgeon to advocate surgical interference. There are even a few hybrids like Dr. F. Avery Jones and myself who have both medically and surgically treated patients under their care and do, I believe, have equal pleasure in recording successful results by either method. The causes of this new outlook are many. The gastroscope has proved a common bond of interest between physicians and surgeons. It has shown to the surgeon how readily the acute gastric ulcer can heal and how even the chronic ulcer begins to heal when the patient is rested in bed. It has shown to the physician the very or- ganic and destructive nature of the ulcerative lesion and demonstrated the persistence of many chronic ulcers long after the symptoms have dis- appeared. The increasing use of surgical methods is founded on solid grounds. The first is that short of enforcing a state of invalidism on the patient there is no medical means of preventing relapse of ulceration. The second is the increasing efficiency of operations for peptic ulcer in relieving pain, in preventing ulcer recurrence and in avoiding side effects of the operations. The diminishing opera- tive mortalities and morbidities are also a major encouragement for surgery. The last but very effective cause of the increasing use of surgery is a rising demand for surgery from the laity who have come to discover its possibilities. Principles of Selection for Surgery In the selection of cases for operation certain general principles can be established. The first is that the subjective success of an operation varies directly with the.amount of pain which the patient has previously suffered, though there are occasional exceptions to this. It will be found that there is less satisfaction with the operation among those who have had an emergency operation, e.g. to arrest gastro-duodenal bleeding, than among those operated on for chronic pain, though it cannot be disputed that nevertheless both operations have succeeded in their object, the one to avoid death from bleeding, the other to cure chronic ulcer pain. The next principle is that the patient who gets good relief from bed rest and medical treatment is the one who is most certain to get relief from surgical treatment. One should be somewhat Protected by copyright. on 23 March 2019 by guest. http://pmj.bmj.com/ Postgrad Med J: first published as 10.1136/pgmj.30.347.448 on 1 September 1954. Downloaded from
Transcript of SURGERY ULCERATION AND ITS COMPLICATIONS · tional forms maymimic ulcer dyspepsia, make it unsafe...

SURGERYAND
OF PEPTIC ULCERATIONITS COMPLICATIONS
BY NORMAN C. TANNER, M.D., F.R.C.S .The three Lettsomian Lectures delivered at the Medical Society of London on February I5, 24 and
March I, I954-
(They will be published in this and the next two numbers of the journal.)
Part I
LECTURE ONEGastric and Duodenal Ulceration. OperativeMethods. Results of Operation
I am greatly honoured by your invitation to meto deliver the lectures in memory of John CoakleyLettsom.
It is only nine years since my distinguished pre-decessor, Sir Gordon Gordon-Taylor, deliveredthe Lettsomian Lecture on the subject of haemor-rhage from peptic ulcer (Gordon-Taylor, 1945).I shall have little of value to add to his words onthis aspect except to record diminished mortalityfigures, largely as a result of the policies he thenadvocated to us. I shall discuss the subjectwidely and can therefore only touch lightly oncertain aspects, though I shall prod more heavilyin certain places where it may do good.
Selection for SurgeryTwenty to thirty years ago there was more dis-
agreement among clinicians on the selection of'cases for surgical treatment. In those days thephysician tended to find it one of his functions tosave the patient from the surgeon. The patientwho arrived at the surgical outpatients' clinic withan ulcer sometimes found that his only course ofmedical treatment was a packet of alkaline powderto take while awaiting admission for operation!Nowadays the position has changed. Thephysician is almost more ready than the surgeon toadvocate surgical interference. There are even afew hybrids like Dr. F. Avery Jones and myselfwho have both medically and surgically treatedpatients under their care and do, I believe, haveequal pleasure in recording successful results byeither method. The causes of this new outlookare many. The gastroscope has proved a commonbond of interest between physicians and surgeons.It has shown to the surgeon how readily the acute
gastric ulcer can heal and how even the chroniculcer begins to heal when the patient is rested inbed. It has shown to the physician the very or-ganic and destructive nature of the ulcerativelesion and demonstrated the persistence of manychronic ulcers long after the symptoms have dis-appeared.The increasing use of surgical methods is
founded on solid grounds. The first is that shortof enforcing a state of invalidism on the patientthere is no medical means of preventing relapse ofulceration. The second is the increasing efficiencyof operations for peptic ulcer in relieving pain, inpreventing ulcer recurrence and in avoiding sideeffects of the operations. The diminishing opera-tive mortalities and morbidities are also a majorencouragement for surgery. The last but veryeffective cause of the increasing use of surgery isa rising demand for surgery from the laity whohave come to discover its possibilities.
Principles of Selection for SurgeryIn the selection of cases for operation certain
general principles can be established. The first isthat the subjective success of an operation variesdirectly with the.amount of pain which the patienthas previously suffered, though there are occasionalexceptions to this. It will be found that there isless satisfaction with the operation among thosewho have had an emergency operation, e.g. toarrest gastro-duodenal bleeding, than among thoseoperated on for chronic pain, though it cannot bedisputed that nevertheless both operations havesucceeded in their object, the one to avoid deathfrom bleeding, the other to cure chronic ulcer pain.The next principle is that the patient who gets
good relief from bed rest and medical treatment isthe one who is most certain to get relief fromsurgical treatment. One should be somewhat
Protected by copyright.
on 23 March 2019 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.30.347.448 on 1 S
eptember 1954. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
wary of the case who gets no relief from medicaltreatment unless the ulcer is a penetrating one.Periodical remission of symptoms and relief ofpain from bed rest are typical features of pepticulceration.and if they are missing the possibilityof an incorrect diagnosis or of an excessive func-tional overlay should be considered.Young patients, being intolerant of ill health,
are often anxious for surgery prematurely and tendto regard the operation as the removal of an un-pleasant aching foreign body and do not realizethat it entails an alteration in their gastric physi-ology. Nevertheless, well-selected young subjectsdo extremely well after gastrectomy.
P.y. T., aged 25, was admitted under my care in194I. He gave a history of duodenal type ofdyspepsia since childhood and of an unsuccessfuloperation for duodenal uilcer, I believe a pyloro-plasty, at the age of I3. I carried out a partialgastrectomy for a chronic penetrating duodenalulcer. His subsequent progress was excellent, hegained weight and is now a muscular and well-nourished man. At any rate his progress satisfiedhis family, for in 1943 his 34 year old brother(T.T.) came for a gastrectomy for a stomal ulcerfollowing a gastro-jejunostomy performed when hewas aged 2., and in I95I his remaining twobrothers, M.T., ~aged 36, and P.T., aged 38, bothrequested and had partial gastrectomies -for severeduodenal ulceration. All the four young men hadhistories of ulceration dating from childhood orteens and made careful observation of theirbrother's progress before submitting themselvesfor surgery!
Middle-aged men with heavy family and socialresponsibilities are sometimes debarred from sur-gery because it is believed that their nervous tem-perament may invite failure. It is my impressionthat many such patients become emotionally morestable when a major cause of their anxiety, namelythe ulcer, is removed.
Elderly patients not infrequently decide to retirefrom work on account of their persistent ulcersymptoms, believing that freed from responsibilityand daily toil the ulcer will heal. If the diagnosisof chronic ulceration is correct, most such patientsare disappointed in their hopes and find that theyare unable to enjoy their retirement without thehelp of surgery.
The Diagnosis of Peptic UlcerationThree years ago Dr. Cochrane Shanks told us
something of the radiological diagnosis of pepticulceration (Shanks, 1952). X-ray examination ofthe passage of an opaque meal remains the secondmost important means of diagnosis. I would givethe first place to the clinical history. The symp-toms of peptic ulceration tend to follow certain
well-marked patterns with occasional difficult vari-ants such as the penetrating ulcer in which thefood-pain relationship is lost, the ulcer at thecardiac end of the stomach which may produce anangina-like pain or the posterior duodenal ulcerwhich may cause only an intractable backache untila melaena discloses the intestinal origin of the pain.However, the fact that certain other forms ofdyspepsia, for example that due to simple ormalignant tumours or to gastritis, and some func-tional forms may mimic ulcer dyspepsia, make itunsafe to operate merely on a clinical diagnosis.A difficulty arises when a patient with typical
ulcer symptoms is reported to have normal appear-ances on X-ray examination. Repetition of theX-ray after a short period of bed rest may enablethe radiologist to demonstrate scarring moreclearly. In this type of case a gastric analysis ishelpful. If the patient has duodenal ulcer-likesymptoms, the X-ray is negative and the fractionaltest meal reveals a high acidity, then I think it wiseto treat the patient as a duodenal ulcer. If anulcer-like dyspepsia is found with a negative X-rayand an achlorhydria on test meal examination, thenit is well to add a gastroscopic examination, whenan atrophic gastritis or even an ulcer or carcinomamay, at times be found. The ' false positive' inradiology is also disconcerting and on several oc-casions I have found the test meal of help. Forexample, a deformity believed to be due to duo-denal ulceration may be associated with hypo-acidity or anacidity. Such conflicting findingsindicate the need for gastroscopy, particularly ifthere is blood in the gastric content. On gastro-scopy in such cases I have found a carcinoma, oftenfundic or diffusely infiltrative, on several oc-casions. An atrophic gastritis may be present and,if so, one can be sure that the duodenal deformityis either a false finding or it is the healed scar of anulcer from which the patient suffered earlier inlife. This latter combination is important becausegastric resection may not relieve the symptoms ofatrophic gastritis. I have seen three patients whohad a gastrectomy because of the. laparotomy find-ings of a duodenal scar-but who in fact had longsince ceased to suffer from the duodenal ulcer,because with the passage of the years they haddeveloped gastric atrophy and hypoacidity, andall three were disappointed by the post-operativepersistence of their symptoms. One must evenbe guarded as to the symptomatic prognosis ofactive gastric ulceration when it is associated withachlorhydria and atrophic gastritis. The majoritywill have symptomatic relief but in some, pre-sumably those whose symptoms were due to thegastritis rather than to the ulcer, dyspeptic symp-toms of varying severity may continue.
In a clinic such as ours in S.W. London where
S-eptember 1954450P
rotected by copyright. on 23 M
arch 2019 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.347.448 on 1 Septem
ber 1954. Dow
nloaded from

TANNER: Surgery of Peptic Ulceration and Its Complications
there are about three gastric ulcers to every fiveduodenal ulcers treated and where more than ahalf of the cases of haematemesis have a gastriclesion, we find gastroscopy of great value in diag-nosis. A successful -gastroscopy is usually morereliable than an exploratory laporotomy in the de-tection of the smaller gastric ulcers. On gastro-scopy I have occasionally discovered gastric polypsor gastric diverticula, and many times foundgastric ulcers in patients who had previously hadnegative gastric findings at laparotomy. It is themost reliable means of differentiation betweensimple ulcer and carcinoma, apart perhaps fromlaparotomy. It is frequently quoted in the NorthAmerican literature that some io per cent. of ulcersresected in the belief that they are innocent, are infact malignant. With the aid of pre-operativegastroscopy we find well under i per cent. of suchresected ulcers to be malignant on histological orfollow-up investigation. It is reported that acarcinoma may appear to heal for a time on X-rayexamination. In a series of between i,ooo and2,000 gastroscopic examinations of gastric ulcersI have never found a gastric ulcer apparently healand later turn out to be malignant. Therefore Iplace considerable value on pre-operative visualiza-tion of a gastric ulcer. In cases of doubt atlaparotomy I have usually found it safe to trustmy pre-operative gastroscopic diagnosis. The dis-advantage of gastroscopy is the need for veryextensive training and an experience of manyhundreds of examinations bef6re one is able tointerpret the findings.
Peptic Ulceration and the Gastric MucosaPerhaps it is opportune at this stage to make
some remarks on the relation between the gastro-scopic appearances of the gastric mucosa and pepticulceration. Duodenal ulceration is usually associ-ated with a raised gastric acidity, an increasedvolume of basal day and night secretion, and avigorous secretory response to stimulation byappetite or by food. On gastroscopy, as HaroldRodgers has pointed out, it is usual to find thenormal mucosal pattern, the areae gastricae, to bewell marked and the folds well developed. Onenever finds widespread atrophic changes in thepresence of an active duodenal ulcer. In cases ofgastric ulceration the mucosa is occasionally welldeveloped, but much more often it is thinner thannormal. Not infrequently the areae gastricae areflattened and unrecognisable, with stippled con-gestion of the mucosa, or even atrophic changes,making it possible to see intramucosal andsubmucosal blood vessels. In these cases thegastric acidity is depressed below normal, or theremay be achlorhydria. Thus it appears that gastriculcer frequently arises in a diseased or degenerate
FIG. I.-With the high secretion of gastric juice, aduodenal ulcer may appear. When the mucosa de-generates, the duodenal ulcer tends to heal and agastric ulcer may appear. (Note-This illustra-tion has also appeared in the Edin. med. J7., I95I,58, 288.)
mucosa, and the acid-peptic factor is much lessimportant.My impression (Fig. i) is that the duodenal
ulcer appears in subjects with a healthy gastricmucosa which possibly under some nervousinfluence is capable of excessive secretion, causingulceration of the duodenal mucosa. With theonset of gastritis or degenerative atrophic changes,and there is on the average a tendency for thegastric acidity to fall with advancing years, thepowers of excessive secretion diminish and aduodenal ulcer will tend to heal This gastritictendency leads to a decrease in the resistance ofthe gastric mucosa, so that despite the lowerederosive power of the gastric juice, it mav breakdown to produce a gastric ulcer much as the skinulcerates in a case of varicose eczema, with theminimum of trauma.That this is the sequence of events is supported
by the fact that gastric ulceration tends to appearon the average some ten years later in life thanduodenal ulcer.
It is also supported by a finding that has.frequently interested me at operation in caseswhere there is evidence of coincident gastric andduodenal ulceration. In go per cent. of suchcases, it is found that the gastric ulcer is active, butthe duodenal is inactive or is a healed scar. In thecases when the duodenal ulcer is active it is oftenfound that the gastric ulcer is an early or subacute
September I954 451P
rotected by copyright. on 23 M
arch 2019 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.347.448 on 1 Septem
ber 1954. Dow
nloaded from

POSTGRADUATE MEDICAL JOURNAL
one, suggesting that when the two are combined,the gastric ulcer is waxing, the duodenal waning.About one quarter of my gastric ulcer cases are
found to have a duodenal scar or ulcer. The ageof onset of symptoms in the combined group issimilar to that of the age of onset of duodenalulceration. The age at operation is more similarto the age at operation of gastric ulcer cases.
Age of onset of symptomsAge at operation
D.U.and
D.U. G.U. G.U... 32.2 32.7 40.8*- 42.6 49.4 47.6
This small point also suggests that duodenalulceration was the first event and gastric ulcera-tion a later event in cases of combined ulceration.
Further evidence of the difference in the erosivepowers of the gastric juice is given by the vastexperience we have from the performance ofgastro-jejunal anastomoses. If a hundred gastro-jejunostomies are done for duodenal ulcer, abouta half will get jejunal ulceration. If a hundred aredone for gastric ulceration, the gastric ulcer maypersist but the jejunum will rarely ulcerate.Similarly, the jejunal ulceration rate after gas-trectomy for duodenal ulcer is usually 2-3 percent., but only a small fraction of i per cent. afterthe same type of gastrectomy done for gastriculcer.
I think that if the erosive powers of the gastricjuice are diminished in gastric ulcer cases, then itis reasonable to assume that the gastric mucosa insuch patients has a diminished resistance toulceration.These points are I think important and help to
guide us in our selection of operations for thevarious forms of peptic ulcer.
Operative Methods in Dealing with PepticUlcerA great many ingenious operations have been
described, carried out and finally discarded, in thetreatment of peptic ulceration. Some ten yearsago, in my armchair, I discovered-or if I studythe literature hard enough, I shall probably findthat I re-discovered a form of gastro-jejunostomythat seemed less likely to lead to stomal ulceration.I decided that a likely cause of stomal ulcerationwas that as the gastro-jejunal stoma was placed inthe most dependent part of the body of thestomach, not only was the adjacent jejunumconstantly bathed in the resting gastric juice, butthe susceptible jejunal mucosa was sutured to acidsecreting gastric mucosa. It occured to me that astoma immediately proximal to the pylorus wouldbe in less contact with the resting intercibal juiceand as the secretion of the pyloric mucosa is
weakly alkaline, the jejunal mucosa would beadjacent to alkali secreting gastric mucosa. Icarried out some twelve of these operations inI943, which I called juxta-pyloric gastro-jejunos-tomy. At a follow-up some three years later, Ifound the operation extremely satisfactory, thoughtwo or three were requiring alkaline powders fromtime to time. Fortunately I decided to wait longerbefore generally advocating the operation. Whatis the position todav-some ten years later ?
GASTRO-JEJUNOSTOMY FOR DUODENAL ULCEROperations 1943-44. Follow-up 1954
JuxtaPyloric Orthodox
Operation OperationNo. of operations .. .. I 19Followed-up, ten years ..5Recurrent Proved 2.7 8Stomal ** 2l1Ulceration Clinical diag- j 8
nosis .. 3J iJWellDied (not of ulcer)
40
43
I need hardly emphasize the grave risks inaccepting new operations based only on theoreticalconsiderations, without the test of time.
I believe it is safe to say that the orthodoxoperation for gastric or duodenal ulcer is a partialgastrectomy, with vagotomy still under trial. Theshort circulating operations, the local excisions andplastic operations have been discarded, apart fromtheir occasional use as a temporary expedient, as apalliation in feeble or aged persons, or as anaccessory to vagal resection. A wide pyloroplastyis sometimes of help in a senile starved personwith a stenosed duodenal ulcer. A gastro-jeju-nostomy is also justifiable for aged or decrepitpersons with intractable ulcer pain. It will usuallycure the duodenal ulcer, though age and decrepi-tude may not protect the patient against stomalulceration, and one can only hope that the stomalulcer will be less troublesome than was theduodenal ulcer.
Partial gastrectomy for gastric and duodenalulceration is a well-tried operation and has main-tained its prestige despite much criticism. Mylate senior registrar, Mr. Colin Craig, now con-sultant surgeon at Lowestoft, and a physiciancolleague, Dr. Chippendale, recently made* anextremely critical follow-up of 6II consecutive,elective and emergency partial gastrectomies forulcer, carried out at St. James's Hospital (271 forgastric ulcer, 246 for duodenal ulcer, 89 for gastricand duodenal ulcer, 5 unclassified). Follow-upby personal interview between three and six yearsafter operation disclosed that 89 per cent. of thepatients were completely satisfied by the operationand had had to make no change in their normal
September 1954452P
rotected by copyright. on 23 M
arch 2019 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.347.448 on 1 Septem
ber 1954. Dow
nloaded from

TANNER: Surgery of Peptic Ulceration and Its Complications
habits of life. None of the gastric ulcer cases haddeveloped further ulcer trouble, though five of the244 patients with duodenal ulcer (2 per cent.) haddeveloped stomal ulceration. It has been suggestedthat stomal ulceration can be almost eliminated ifonly 5-6 cm. of stomach is preserved. I wouldagree that such is probable, but it would be anentirely ridiculous price to pay. We know thatthe three-quarter or so gastrectomy generallycarried out makes no very profound change in thepatients' general health or longevity. Such ex-treme resections however are likely, like totalgastrectomy, to produce an appreciable number ofcases of macrocytic anaemia as well as manymicrocytic ones. Now that we have another verypromising weapon, namely vagotomy, in the treat-ment of stomal ulcer, there is even less need toperform these drastic resections for the sake ofthe 2-3 per cent who are going to develop a stomalulcer.Of late years, with the great increase in the
numbers of the gastrectomized population, con-siderable interest and some alarm has been arousedby the incidence of certain symptoms appearingafter meals, notably epigastric discomfort withsweating, flushing, palpitations, sometimes fatigueand at times accompanied by biliary regurgitation,or diarrhoea. These have been grouped togetheras the early post cibal symptoms or ' dumpingsymptoms '-a term which Dr. Cochrane Shanksin his Lettsomian Lecture suggested 'should bedumped.'
In view of our very great ignorance of themechanism, prevention and treatment of thesesymptoms, I considered that it would be helpfulto try and discover which form of gastrectomy wasleast prone to develop these symptoms. Mimprissand Burt (I948) have reported a similar investi-gation. Therefore the period 1946-49 was dividedinto two. During the first part, all gastrectomiesfor duodenal or duodenal plus gastric ulcer wereperformed by an antecolic gastro-jejunal anasto-mosis, the jejunum running from lesser to greatercurve, with a valve on the lesser curve half of thestomach, and an afferent loop 9 to I5 in. in length.During the second period, similar anastomoseswere made with a much shorter loop, but thestomach was drawn through the transverse meso-colon-a retrocolic anastomosis. During the wholeperiod, many of the gastric ulcers were treated bythe Billroth I (PNan) form of gastrectomy (recon-struction by gastro-duodenal anastomosis).
Craig and Chippendale classified the resultsunder the following categories.Category I. Free of all gastric symptoms.
II. Fullness after meals.III. The early post-cibal syndrome-with
mild symptoms, a satisfied patient
and no interference with normalhabits.
IV. The early post-cibal syndrome-withseveral symptoms necessitating restafter meals and causing interferencewith normal work.
V. The late post-cibal syndrome.VI. Recurrent ulceration.VII. Deficiency syndromes; including loss
of weight, anaemia, vitamin de-ficiencies.
VIII. Miscellaneous.The following Table gives the results so far as
early post cibal symptoms are concerned:
Cases Billroth ITotal assessed . . 95Category I .. 51
(53 *7%),, II .. 22
(23.2%)III . . II
( I . 6%)IV .. 4
(5 *4%)
AntecolicPolya245146
(59.6%)50
(20.4%)29
(ii. 8%)8
(3 *3 %)
RetrocolicPolyai6877
(45.8%>37
(22%)33
(I9. 6%)'3
(7-7%)
I was surprised to find that the retrocolic gastro-jejunal type came out somewhat the worse asregards both the mild and severe types of postcibal symptoms. It should be added that Craigand Chippendale found that our Billroth I patientswhile having a similar incidence of dumping tothe antecolic valved gastro-jejunal operation, hadgenerally milder symptoms.The antecolic Polya and the Billroth I opera-
tions thus proving the more satisfactory, we havesince used them more frequently.We found, however, a grave drawback to these
long looped antecolic operations. Cases of acuteafferent loop obstruction occured in a few of ourown patients and other surgeons told me of acuteobstruction of the long afferent jejunal loop as earlyas five days, and as late as seven years after theoperation. It is true that any form of gastrectomymay be followed by obstruction or internalherniation, but such mishaps are rare. Oneloop obstruction occurred in the series of I68retrocolic gastrectomies, (Fig. 2) two years afteroperation. The efferent loop of jejunum haspassed through an opening bounded by the shortafferent jejunal loop and meso-colon, and wassuccessfully reduced by my then Registrar, Mr. E.Murray. The afferent loop obstruction typical ofthe long looped antecolic operation was very fullyinvestigated by my late Senior Registrar, Mr.Derek Teasdale, and it has also been described byQuinn W. F. and Gifford J. H. (I950). It may beillustrated by the following history.
A.E., a female, aged 47 in I947 had a haemate-a
September 1954 453.P
rotected by copyright. on 23 M
arch 2019 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.347.448 on 1 Septem
ber 1954. Dow
nloaded from

September 1954 TANNER: Surgery ofjPeptic Ulceration and Its Complications 455
: I.
I .%t %
:::I %
I I* '
EFFERENT LOOP OBSTRUCTION- RETROCOLIC ANASTOMOSIS.
FIG. 2.-Obstruction of efferent jejunal loop followingretrocolic partial gastrectomy.
/Rs
LONG AFFERENT LOOP OBSTRUCTION.FIG. 3.-Obstruction of long afferent loop behind its
own mesentery following. antecolic.. partial gastrec'tomy.
(11I'll I)
SAFE ANTECOLIC LOOPS.
N1't-
FIG. 4.-Moynihan type ofgastrectomy (above) and shortloop antecolic ' efferent to greater curve ' gastrec-tomy (below). These appear to be free from therisk of afferent loop obstruction.
mesis and three weeks later was subjected togastrectomy at a London Hospital. She was wellfor nearly four years, when she developed severeperi-umbilical pain radiating to the back, tem-porary collapse and slight vomiting. She wasadmitted to St. James' Hospital four days later.On examination she was apyrexial, pale and thin.There was a midline epigastric operation scar anda sausage-shaped mass under the left costal margin.The haemoglobin was 46 per cent. and urinarydiastatic index raised to 8oo units (Normal 33)4After transfusion she was operated on by Mr.Teasdale. A little free fluid escaped on openingthe abdomen. There was an antecolic gastrectomywith afferent jejunum joined to the lesser curve.The duodenum and gall-bladder were tensely dis-tended and the afferent jejunal loop similarly dis-tended lay behind and to the left of the efferentloop (Fig. 3). Attempts to reduce this loop wereunsuccessful- and so after aspiration ofnmuch biliary
C2
Protected by copyright.
on 23 March 2019 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.30.347.448 on 1 S
eptember 1954. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
fluid from it, the efferent and afferent loops wereshort circuited. This afferent loop was found tobe I8 in. long. The post-operative course wassmooth and on discharge her urinary diastase was20 units.
Altogether four such cases were seen at St.James', in one of which the afferent loop was sodistended that it ruptured and led to death. Oneor two cases were suspected of slight obstructionafter operation, but subsided after turning the
patient on the right side and elevating the foot ofthe bed. These cases were enough to make usabandon the antecolic long loop efferent to greatercurve (E.G.) operation, despite its greater freedomfrom 'dumping' symptoms. Gastro-duodenalanastomosis was a satisfactory alternative ingastric ulcer cases but we were averse to using thevery unhealthy duodenum in duodenal ulcer cases.It seemed to us that the gastro-jejunal possibilitieswere either (Fig. 4): (i) Moynihan (efferent-
FiGs. 5 and 6.-The author's technique for performing gastrectomy with a valve in non crushing(Lane's) clamps.
456 September 1954
7W.2"NOWN.-Al,_~ , 100b.- if &#"%*aI mus
Protected by copyright.
on 23 March 2019 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.30.347.448 on 1 S
eptember 1954. D
ownloaded from

TANNER: Surgery of Peptic Ulceration and Its Complications
jejunum to lesser curve) (E.L.) operation, or, (2)Short loop antecolic efferent loop to greater curve(E.G.) anastomosis.We decided on the latter and since 195I nearly
half the gastrectomies have been of this type. Ihave personally performed just under two hundredand about three hundred of this type have beencarried out by my ' team' without any furtherafferent loop or other mechanical troubles. Theafferent loop is made only 4 in to 5 in. long andmay seem tense to the observer at the time ofanastomosis, but when it lies in the abdomen it isfree of tension.A description of my present mode of per-
formance of the antecolic operation may be ofinterest. After duodenal division and closure,and mobilization of the stomach, the stomach andjejunum are placed in Lane clamps, with a four tofive inch afferent jejunal loop. After uniting thetwo with a Lembert (Figs. 5 and 6) stitch a Payrclamp is placed half to two-thirds of the wayacross the lesser curve side of the stomach, thisbeing the part which is to be closed. I think itunreal to measure the future stoma in inches insuch an elastic organ as the stomach, and so Ileave a stoma between a third and a half of thestomach diameter. After removal of the stomachthe lesser curve half is closed with a sewingmachine stitch. I used fine silk for this during thewar but had to abandon this practice, for mycolleague, Mr. Desmond, and I had some six casesof mild haematemesis up to a year after operationdue to extrusion into the stomach of one of the
FIG. 7. -Gastroscopic view of silk knot partially ex-truded into stomach after gastrectomy. (Note.-This illustration was also shown in the Edin. med. J3.article.)
knots, with retention of the second knot in thestomach wall (Fig. 7). The diagnosis wasevident on gastroscopic examination when theknot could be seen hanging from what was a stitchabscess cavity and which bled, presumably whenit underwent peptic digestion. In two cases wehad to remove the silk at a second operation andthe suspected state of affairs was confirmed. In athird case I was able to introduce a flexibleforceps into the stomach through a rubber channelmade in the side of a Hermon Taylor gastroscope,and grasp and pull out the stitch, whereupon therewas no more trouble (Fig 8). The lesson is, ofcourse, to use continuous catgut or interruptednon-absorbable stitches when suturing gastrictissues. We use the former.To continue with the gastrectomy. After uniting
the open end of the stomach to an opening in thejejunum, the gastrectomy is completed by simplycontinuing the Lembert stitch round the anteriorsurface of stomach and jejunum, taking deep bitesover the closed part of the stomach to produce avalvular effect. This is, I believe, simpler thanthe orthodox Hofmeister valve and is more likelyto have a valvular action. I have made the valvein this fashion since I94I and there has been noleak or other anxiety connected with it, so it iscertainly safe.The main difficulty in the operation for duodenal
ulcer concerns safe duodenal closure. It so hap-pens that I have never had a leak and certainly nomortality, or so far as I know, morbidity fromduodenal leakage, and so it may be helpful to makea few remarks on our methods of closure. Thefirst point is that we never hurry and are preparedto spend as much time over duodenal closure asover the rest of the operation. The second pointis that although we usually find it advisable todissect just past the ulcer in order to get a conicalstump to invaginate, we never mind where theduodenum is closed so long as it is closed safely.We never dissect well past the ulcer simply inorder to give the pathologist a good specimen.The appearance of the ulcer at operation is thebest evidence of the duodenal pathology. Goodspecimens of duodenal ulcer are best obtained fromthe post-mortem room.The third point is that in dissecting distal to the
ulcer, where sharp dissection is always necessary,we keep close to the duodenal wall. When clamp-ing vessels, bands or omenta, we clamp so closeto the duodenum that one cannot put on a secondforceps and so it is necessary to cut between theduodenum and forceps. When there is a largecompletely penetrating ulcer, I find it helpful toput one finger in the duodenum and shave theduodenum off the pancreas, keeping the scalpelclose to the finger.
S-eptember I954 457P
rotected by copyright. on 23 M
arch 2019 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.347.448 on 1 Septem
ber 1954. Dow
nloaded from

POSTGRADUATE MEDICAL JOURNAL
FIG. 8.-Type of flexible forceps usedstomach.
The fourth point is to operate with the ulcerquiescent whenever possible. To allow this objectwe insist on giving the patient a few days inhospital prior to operation. The consequent lackof acute inflammation will enable one to transectthe duodenum close to, and in difficult cases eventhrough the ulcer, and the fibrotic duodenum atthe ulcer edge will be found to hold sutures well.
Point number five is that we never cut, cauterize,or insert needles into healthy pancreatic tissue forfear that leakage of pancreatic juice may occur.When it is difficult to invaginate the duodenalstump, I do not hesitate to put interrupted non-absorbable sutures between the healthy lateralduodenal wall and the fibrotic ulcer crater edgein the pancreas.The sixth very important point is that there
must be no obstruction of the afferent loop of thegastro-jejunal anastomosis-for this could lead tostump rupture. So far as my own technique isconcerned this reinforces our decision to abandon
to extract the silk knot from the
the long antecolic afferent loop in favour of a 4 to5 in. one.
Finally, if there is anything short of perfectionin the closure of the stump, a small drainage tubeshould be placed down to it. I have only oncenoticed any intestinal discharge from this tube,about i ml. of mucus per day, three weeks after adifficult post-pyloric, pre-ulcer closure; neverthe-less it is a wise precaution.What of the patient in whom duodenal closure
appears to be too hazardous to attempt? In suchcases there are three alternatives.
i. Gastro-jejunostomy, preferably combinedwith vagotomy.
2. Two-stage gastrectomy. Stage one is pre-pyloric closure of the duodenum across the antrum,removal of the lower two-thirds of the body of thestomach followed by gastro-jejunal anastomosis.The second stage, carried out six week-s lat1ewhen all ulcer activity will have died down, is to
excise the antrum.
458 ,Sebtember I 954P
rotected by copyright. on 23 M
arch 2019 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.347.448 on 1 Septem
ber 1954. Dow
nloaded from
TANNER: Surgery of Peptic Ulceration and Its Complications
GASTRIC ULCER PLUS DUODENAL ULCERSTENOSING COMMON DUCT.
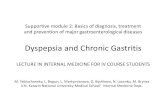
PARTIAL GASTRECTOMY.FIG. 9.-Final disposition after dealing with a case of
gastric ulcer associated with a duodenal ulcer whichhad stenosed the common bile duct.
3. Pre-pyloric closure of the duodenum, re-moving the antral mucous membrane and thenmaking a high partial gastrectomy. Follow-upstudies have shown no difference in the late pro-gress of this form of gastrectomy from those withduodenal closure distal to the ulcer. A criticismof this method is the difficulty in controllingbleeding while separating the mucosa from themuscular coat of the antrum. It is necessary toleave branches of the right gastric and right gastro-epiploic arteries to the pyloric antrum intact, forthe only other good blood supply coming to theantrum from the duodenal side lies in the sub-mucosa, and this is destroyed in removing themucosa. The application of arterial clamps on theright gastric and right gastro-epiploic vessels makeslittle difference to the bleeding and putting a non-crushing clamp across the duodenum in cases ofpenetrating duodenal ulcer is very hazardous, thusthere is no alternative to slow and careful ligationof the submucosal vessels during the stripping ofthe seromuscularis from the mucous membrane.A rare difficulty arises in the case where a duo-
denal ulcer has stenosed the common bile duct.Perhaps recital of our management of a compli-cated case of this type will be of interest: L. J.,female, aged 64, first came to St. James' Hospitalin 1938, when she had a cholecyst-gastrostomyfor jaundice due to involvement of the commonbile duct by a duodenal ulcer. She had a thirty
year history of duodenal dyspepsia, but in I949a gastric ulcer arose and gave increasingly severepain and vomiting. Gastroscopy confirmed thepresence of a high chronic gastric ulcer. In I953,I operated on her and found a high gastric ulcer,a narrowed duodenum, stenosed common ductand a healthy cholecyst-gastric anastomosis. Wedismantled the anastomosis of stomach and gall-bladder, transected the duodenum just beyond thepylorus but proximal to the stenosed area. Theduodenum was closed by uniting the fundus ofthe gall-bladder to it, and after partial gastrectomya gastro-jejunal anastomosis was made. (Fig. 9.)As the gastro-duodenal (Billroth I) form of
reconstruction proved very satisfactory in ourfollow-up, we use it for most of our gastric ulcercases, where the duodenum is healthy, or duodenalulceration is inactive. There has been a suggestionthat stomal ulceration is commoner after the Bill-roth I operation, but as stomal ulceration isextremely rare after gastric ulcer resection, this isno objection.
I would like to make a few remarks concerninggastrectomy for gastric ulcer. In order to avoida narrow stoma, it is wise to use at least half thegastric diameter for it, no matter how narrow theduodenum may be. The duodenal circumferencecan always be increased by an anterior incision,extending distally from its cut end.A great deal of ingenuity can be used in con-
structing the new stomach when the gastric ulceris found in awkward situations.When the ulcer is high and on the posterior
wall; in our experience the commonest situationin women (25 per cent.) and the situation inio per cent of the male cases, then I use whatwe call the rotation gastrectomy (Tanner, 1952).The curvatures and the ulcer region are dissectedfree, and then the ulcer is grasped with the leftfingers. (Fig. io.) A Payr or Stevenson clamp isplaced over half the gastric diameter on the oppo-site side to the ulcer, that is the anterior wall,lower down on the stomach, and this is to be thenew stoma. (Fig. ii.) After cutting across thestomach below this clamp a second curved crushingclamp is made to arch over the ulcer, and then thestomach with a tongue-shaped extension of theposterior wall containing the ulcer, is removed.The cut edges contained in the crushing clamp areunited with two layers of suture and the part inthe Payr or Stevenson clamp is anastomosedend to end to the duodenum. The rotation of thestomach if anything makes the stoma lie morenormally, despite the fact that the gastric side ofthe stoma is made almost entirely of anteriorgastric wall. (Fig. 12.)We see many very high gastric ulcers within a
centimetre or two of the cardiac orifice. We have
September I954 46IP
rotected by copyright. on 23 M
arch 2019 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.347.448 on 1 Septem
ber 1954. Dow
nloaded from

462 POSTGRADUATE MEDICAL JOURNAL September I954
S ;ar :j}:: s}, :.j: oB'W.-.:' .:::i .. ^: : }:: 538>. }:ES e llB;'se . !:::Bx. . .. ' i:s : :;':: .w ';1S:S : BiF.:: : 31d. . .. S: :- . MBE2 :. : :3 . ^: .: a.E| $, ', 5. X ivuB^':-e .} :.X. .. .:: :.:'>BS :i'0fi'S:> < 0 82 yeB ; mK SiS .: q>. :' ' ': ' d; SEiBY : BBis ., .e8ffi.v-.'i ...... S7«'3 ffi ' r ::: ......... .. ' :.' : :i:, ....... :S¢B 3.N,-,.D . L: .: Y:' : . .::::: M *E. 3E ::. ::- .. X } } :eS :}EBB:SSF-. J IIL. : .; .................. . : :.gY: : .. : .:i . S: : :::H. .:3z .: : s ': :::: .. G :.::.o :.}, .X.e: %.,^,. :.* LsM 3. .Ns i :.. v !1 .- .......... : i- ... j;.,..:wi. - -] . -11| m0: ......... >!: 1 -1t .: 7 ..
.................i::3.' :^:.i.' ........... :}^:.}e-- .e ................. : .. ......... ...
........ 011 Xil i::. :o ',3
FIG. IO.-' Rotation gastrectomy.' The clamp is placed across the stomachbelow ulcer level, after the stomach has been rotated.
POSTERsOR |
N1'N8 LES16ER CURVE
ULC I
A TERsOR
OCOZ.uou*\4vFIG. iI.-Diagrammatic representation of the ' rota-
tion gastrectomy ' for high posterior gastric ulcer.(Note.-This illustration was also shown in Ann.Roy. Coll. Surg., 1952, 10, 45.)
never practised gastrectomy below the ulcer,although we have resected below a high healedgastric scar on two occasions. No matter howhigh a gastric ulcer may be, we never find itnecessary to use a transthoracic approach. Re-moval of the xiphoid process and sternotomy mayhelp the abdominal approach at times. We havenever found it necessary to perform total gastrec-tomy for a gastric ulcer. We avoid total resectionby fashioning a stomach out of the greater curveside of the fundus and then removing a longupward extension of the lesser curve to just excisethe ulcer edges-an extended Pauchet operation.(Fig. I3.) Several arguments may be used againstcutting close to the ulcer, but I do so for thefollowing reasons:
i. By preliminary gastroscopic observation ofthe ulcer and the further information gained atlaparotomy, it is extremely rare to mistake acarcinoma for an innocent ulcer, not more thanone in a hundred gastric ulcer resections.
2. For many years I have cut close to high
Protected by copyright.
on 23 March 2019 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.30.347.448 on 1 S
eptember 1954. D
ownloaded from

September 1954 TANNER: Surgery of Peptic Ulceration and Its Complications 463
-~ ~~~I.sSi. ...l. ...uZ
...........
....
FIG. I2.-Final appearance after ' rotation ' Billroth I gastrectomy.
ulcers-through thick fibrous submucous coats-and these cases heal well, appear healthy gastro-scopically and eventually do as well as any other.Some difficulty may arise when the resection
goes up.to or into the oesophagus. Normally weclose the incision which surrounded the ulcer areain two layers and finish the case with a gastro-duodenal anastomosis. If, however, the upperend reaches the oesophagus, the incision is closedin one layer (if very thick, two layers) withoutinversion. The cut end of the stomach is thenanastomosed to a jejunal loop and the afferentloop of jejunum is brought up over the lessercurvature suture line as high as the oesophagus,in order to reinforce the single line of sutures.(Fig. 14.) This, if done carefully, makes it abso-lutely safe. Some temporary dysphagia mayfollow, but so long as at least half of the oeso-phageal circumference was intact, the dysphagiadisappears in time.
FIG. 13.-Form of gastrectomy for high lesser curvegastric ulcer. (Also illustrated in Edin. med. J7.article.)
,.I1, L "
.
Protected by copyright.
on 23 March 2019 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.30.347.448 on 1 S
eptember 1954. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
FIG. I4.-Form of reconstruction for ulcer which abutson or invades the oesophagus. (Note.-Illustra-tion also in Edin. med. J7.)
Very high resections for gastric ulcer may benecessary on three types of occasion.
i. When the blood supply to the stomach isdamaged.
G.T., aged 5I, gave a history of gastric ulcerationand repeated haematemesis. An attempt at gas-trectomy failed in October I952, apparently be-cause the ulcer was high and penetrating. Haema-temesis was repeated twice and so in January 1953,the stomach was approached by a thoraco-abdo-minal incision. Again the operation was abandonedafter the spleen had been removed and the fundusmobilized. Haematemesis recurred, and so in May1953 she was transferred to St. James' Hospital,when at gastroscopy a deep penetrating innocentulcer was found just below oesophagus level. Wereopened the abdominal incision. The pyloricend of the stomach was first mobilized, whichnaturally entailed division of the right gastric andright gastro-epiploic arteries. The spleen hadbeen removed by the previous operator so that thevasa brevia and left gastro-epiploic had beendivided. The last artery to the stomach, the leftgastric artery, had been completely destroyed bythe ulcer. In such a case a high resection was
necessary because practically the only blood supplywas that which came through the oesophagus.However a useful remnant of greater curve waspreserved and united to the duodenal stump,making a Billroth I form of gastrectomy (Fig. I5).The patient made good progress.
2. The high hour glass stomach.If stenosis of the stomach due to gastric ulcerationoccurs very high up, then transection above thescarred area is usually the most satisfactory pro-cedure. I have used sleeve resection to avoid tooextreme a resection, but this procedure is ofdoubtful prognosis. Some will ulcerate on thescar and stenose again, and the functional resultsometimes leaves much to be desired, perhaps asa result of the division of so many vagus fibres tothe lower stomach.
3. The high ulcer on the greater curvature.Similar considerations apply to the rare cases ofgreater curve simple ulcer in the upper stomach.
Operative MortalityLet us consider next the operative mortality.
Operative mortalities have fallen a good deal inalmost all classes of operation of late years, and itis our duty to keep a careful watch on this figure,particularly when dealing with non-malignantconditions. New methods become fashionablefrom time to time, such as the various forms ofgastric replacement operation. Used indiscrimi-nately these methods will raise the ulcer-gastrec-tomy mortality, and therefore I believe that theyshould be reserved for the occasional case wherean orthodox gastrectomy has proved unsatisfactory.There are two conditions, however, when a tenderregard for the gastrectomy mortality must beabandoned.
I. In considering the mortality of resectionfor cancer. Here the main object is to extirpatethe tumour radically, and too careful attentionto the immediate mortality figures may lead thesurgeon to carry out an inadequate operation.
2. In cases of massive haematemesis andmelaena. In some cases, death is almost certainunless a hazardous gastrectomy is performed ona near moribund patient. At such times thesurgeon's aim must be at the goal of a low mortalityfor haematemesis, and it is not the time to thinkin terms of a low mortality for any particularoperation.
Therefore in considering the mortalitv of gas-trectomy, it clarifies the position if we consider itunder various headings according to the lesiontreated, and consider emergency resections separ-ately. Taking my personal operative mortalitiessince 1941, when the sulphonamide drugs whichwere potent against pneumonia first came intowider use, the figures are as follows:
S-eptember 1954464P
rotected by copyright. on 23 M
arch 2019 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.347.448 on 1 Septem
ber 1954. Dow
nloaded from

September 1954 TANNER: Surgery of Peptic Ulceration and Its Complications 465
..p7xL ..:..
}..::.: :... .'.'..: .::i:.:::
FIG. IS.-Post-operative X-ray of a Billroth I anastomosis in a patient who hadhad all the gastric arteries divided except those coming through theoesophagus.
Mortalities for gastrectomy for peptic ulcer(excluding operations primarily for acute bleeding,perforation or for gastro-colic fistula) (I941-53).
Cases Deaths MortalityDuodenal ulcer * 531 7 I .3Gastric ulcer .. 637 9 1.4Stomal ulcer following
gastro-jejunostomy.. 107 I . O
T have not available our general hospital mor-tality figures, including operations by colleaguesand registrars, but I know that they would bemuch the same.(The second and third lectures of this series
will be published in the next two numbers of thisjournal.)
Protected by copyright.
on 23 March 2019 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.30.347.448 on 1 S
eptember 1954. D
ownloaded from