Dyspepsia 1
23
Functional Dyspepsia Functional Dyspepsia Yehudith Assouline- Yehudith Assouline- Dayan, MD Dayan, MD
Transcript of Dyspepsia 1

Functional DyspepsiaFunctional Dyspepsia
Yehudith Assouline-Dayan, MDYehudith Assouline-Dayan, MD

Functional Dyspepsia
Definition
Incidence
Pathophysiology
Management

Functional Dyspepsia (FD) is a clinical syndrome characterized by
• Chronic or recurrent upper abdominal pain or discomfort
• in the absence of underlying organ disease that can explain the symptoms

Rome IIIB. Functional Gastroduodenal Disorders
B1 Functional Dyspepsia
• B1a: postprandial distress syndrome (PDS)
• B1b: epigastric pain syndrome (EPS)
B2 Belching disorders
• B2a: Aerophagia
• B2b: Unspecific excessive belching B3 Nausea and vomiting disorders B4 Rumination syndrome

B1 Functional Dyspepsia Must Include one or more of the following:
• Bothersome postprandial fullness
• Early satiation
• Epigastric pain/ burning
AND• No evidence of structural disease
At the last 3 months and onset at least 6 months prior to diagnosis

Incidence Dyspepsia is common, and affects about ¼
individuals in the community
About 25% of symptomatic people eventually present to their primary-care physician
About 10% of these are referred because of refractory symptoms and unhelpful diagnostic tests

Pathophysiology of FGID
Abnormal motility Visceral hypersensitivity Psychosocial factors Mucosal inflammation Altered bacterial flora Disturbed brain–gut interactions

FD-Pathophysiological Mechanisms

GI motor abnormalities in FD
Delayed gastric emptying
Impaired gastric meal distribution
Impaired gastric accommodation
Abnormal fundic phasic contractions
Disturbed antroduodenal motility
Abnormal duodenogastric refluxes

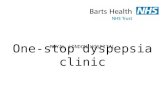
The mechanism and associated symptoms in FD

Prevalence of gastroduodenal dysmotility and relation with symptoms in FD patients
Mizuta Y, J of Gastroenterology, 2006

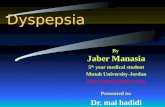
Algorithm for the management of uninvestigated dyspepsia

Initial management strategies for dyspepsia- Review, 2007

Early investigation vs acid suppression
Effectiveness: no difference in 1,125 pts
Fewer dyspepsia-related and other sick leave days with early investigation
Higher patient satisfaction with early investigation

HP test and treat vs endoscopy
No difference in outcome

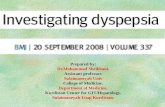
Efficacy of PPI in FD
Moayyedi P, Gastroenterology, 2004

Eradication of HP NUD 21 RCTs
10% relative risk reduction in the HP eradication group compared with placebo
NNTs =14
HP eradication has a small but statistically significant effect in HP positive NUD
Moayyedi P, Cochrane Database Syst Rev 2006

Antidepressants Limited data
No RCTs
One study:
• Good response to SSRI (depressive FD pts)
• No change in EGG

Pharmacotherapy Metoclopramide- standard of care in the US: SE,
efficacy is poorly documented
Cisapride- restricted in the US, not superior to placebo in 512 pts
Domperidone- not FDA proved in the US, poor evidence

Pharmacotherapy
Tegaserod- accelerates gastric emptying in some but not all studies, efficacy in FD not established
Sumatriptan- 5-HT1- receptor agonist
Buspirone (anti anxiety)- potential eficacy

Modulation of pain pathways
Psychological treatments: A meta-analysis -insufficient evidence for a benefit
Potential benefit (methodologic problems)• Applied relaxation therapy
• Psychodynamic psychotherapy
Antidepressants- no RCTs

Hypnotherapy
Calvert EL, Gastroenterology, 2002

Difficult-to-treat dyspeptic patient HP infection was excluded or eradicated
No response to acid suppression therapy
Antidepressants and psychological therapies might be useful
TLC = Patient education and support remain key to the logical management these patients