Peptic Ulcer Disease and Dyspepsia - UCSF · PDF filePeptic Ulcer Disease and Dyspepsia ......
45
Peptic Ulcer Disease and Peptic Ulcer Disease and Dyspepsia Dyspepsia John M. Inadomi, MD John M. Inadomi, MD Professor of Medicine Professor of Medicine UCSF UCSF Chief, Clinical Gastroenterology Chief, Clinical Gastroenterology San Francisco General Hospital San Francisco General Hospital
Transcript of Peptic Ulcer Disease and Dyspepsia - UCSF · PDF filePeptic Ulcer Disease and Dyspepsia ......

Peptic Ulcer Disease and Peptic Ulcer Disease and DyspepsiaDyspepsia
John M. Inadomi, MDJohn M. Inadomi, MDProfessor of MedicineProfessor of Medicine
UCSFUCSFChief, Clinical GastroenterologyChief, Clinical GastroenterologySan Francisco General HospitalSan Francisco General Hospital

Case HistoryCase History
49 y/o woman complains of several 49 y/o woman complains of several months of intermittent epigastric months of intermittent epigastric discomfort made worse with mealsdiscomfort made worse with meals–– She has associated nausea, bloating and early She has associated nausea, bloating and early
satiety but denies weight losssatiety but denies weight lossQuestions:Questions:–– What is the difference between dyspepsia and What is the difference between dyspepsia and
functional dyspepsia?functional dyspepsia?–– Where is Rome and what does it have to do Where is Rome and what does it have to do
this this case?this this case?



Rome Consensus GroupRome Consensus Group
Description of group processDescription of group process–– Meeting since 1988 to address functional GI Meeting since 1988 to address functional GI
disorders disorders –– Chair, coordinating committee, working Chair, coordinating committee, working
committeescommittees–– Functional esophageal, gastroduodenal, Functional esophageal, gastroduodenal,
bowel, bowel, pancreaticobiliarypancreaticobiliary, , anorectalanorectal, and , and childhood disorderschildhood disorders
–– Design of treatment trials; basic science; Design of treatment trials; basic science; physiology:motility/sensation; psychosocialphysiology:motility/sensation; psychosocial

Rome Dyspepsia Definition:Rome Dyspepsia Definition:Rome II: Rome II: ““Dyspepsia refers to pain or Dyspepsia refers to pain or
discomfort centered in the upper discomfort centered in the upper abdomen.abdomen.””
Rome III: Rome III: ““Dyspepsia refers to postprandial Dyspepsia refers to postprandial fullness, early satiation, or epigastric pain or fullness, early satiation, or epigastric pain or burningburning””
Note: patients with primarily heartburn or acid Note: patients with primarily heartburn or acid regurgitation are excludedregurgitation are excluded

More DefinitionsMore Definitions
•• Pain: subjective, unpleasant sensationPain: subjective, unpleasant sensation•• Discomfort: subjective, unpleasant sensation Discomfort: subjective, unpleasant sensation
that is not interpreted as pain by patientthat is not interpreted as pain by patient•• Early satiety: feeling that stomach is overfilled Early satiety: feeling that stomach is overfilled
soon after starting to eat so that meal cannot soon after starting to eat so that meal cannot be finishedbe finished
•• Bloating: tightness located in upper abdomenBloating: tightness located in upper abdomen•• Nausea: queasiness or sick sensationNausea: queasiness or sick sensation•• Retching: heaving as if to vomit but no gastric Retching: heaving as if to vomit but no gastric
contents are forced upcontents are forced up

DyspepsiaDyspepsiaEpidemiologyEpidemiology
Prevalence Prevalence 25%25%–– U.S. and Western countriesU.S. and Western countries
Incidence Incidence 1%1%–– Resolution of symptoms in similar number Resolution of symptoms in similar number
therefore prevalence constanttherefore prevalence constant
BurdenBurden–– 22--5% of all family practice consultations are 5% of all family practice consultations are
for dyspepsiafor dyspepsia

What Comprises the Differential What Comprises the Differential Diagnosis of Dyspepsia?Diagnosis of Dyspepsia?

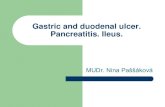
Differential Diagnosis of DyspepsiaDifferential Diagnosis of Dyspepsia
50%
10%
20%
1%
19%
Functional Dyspepsia Peptic Ulcer GERD Cancer Other

Dyspepsia: Dyspepsia: ““OtherOther””
Medications Medications BiliaryBiliaryPancreaticPancreaticCeliac diseaseCeliac diseaseLactose intoleranceLactose intoleranceGastroparesisGastroparesisIBSIBSChronic mesenteric ischemiaChronic mesenteric ischemiaOther Other ““othersothers””–– EosinophilicEosinophilic gastritis, Crohngastritis, Crohn’’s disease, s disease, sarcoidosissarcoidosis, ,
metabolic (metabolic (hypercalcemiahypercalcemia, heavy metals), , heavy metals), hepatomahepatoma, , steatohepatitis steatohepatitis

What would increase your What would increase your suspicion of cancer?suspicion of cancer?
““AlarmAlarm”” features: warrant immediate features: warrant immediate evaluationevaluation–– Age Age >> 4545--50 w/new onset50 w/new onset–– DysphagiaDysphagia–– Weight lossWeight loss–– Symptoms of GI bleeding, overt or occultSymptoms of GI bleeding, overt or occult–– Iron deficiency anemiaIron deficiency anemia–– Family history of gastric cancerFamily history of gastric cancer

Value of Alarm SymptomsValue of Alarm Symptoms
Prevalence of alarm symptoms among dyspeptic Prevalence of alarm symptoms among dyspeptic patients referred for EGDpatients referred for EGD–– 3333--61%61%
Sensitivity Sensitivity 00--100%100%–– Negative predictive value Negative predictive value >97%>97%
SpecificitySpecificity 1616--98%98%–– Positive predictive valuePositive predictive value <11%<11%
Presence of alarm symptoms does not correlate Presence of alarm symptoms does not correlate with presence of structural diseasewith presence of structural disease
AGA Technical Review 2005

Rome III Functional DyspepsiaRome III Functional Dyspepsia
One or more ofOne or more of::–– Bothersome postprandial fullnessBothersome postprandial fullness–– Early satiationEarly satiation–– Epigastric painEpigastric pain–– Epigastric burningEpigastric burningANDAND
No evidence of structural disease (including at No evidence of structural disease (including at upper endoscopy) that is likely to explain the upper endoscopy) that is likely to explain the symptomssymptoms

Functional Dyspepsia SubgroupsFunctional Dyspepsia Subgroups
Postprandial Distress Syndrome (PDS)Postprandial Distress Syndrome (PDS)Either symptomEither symptom–– Bothersome postprandial fullness, occurring after Bothersome postprandial fullness, occurring after
ordinary sized meals at least several times per weekordinary sized meals at least several times per week–– Early satiation that prevents finishing a regular meal Early satiation that prevents finishing a regular meal
at least several times per weekat least several times per week
–– Symptoms for the last 3 months with onset at least 6 Symptoms for the last 3 months with onset at least 6 months before diagnosismonths before diagnosis

Functional Dyspepsia SubgroupsFunctional Dyspepsia Subgroups
Epigastric Pain Syndrome (EPS)Epigastric Pain Syndrome (EPS)–– Pain or burning localized to the Pain or burning localized to the epigastriumepigastrium of at least of at least
moderate severity at least once per weekmoderate severity at least once per week–– The pain is intermittentThe pain is intermittent–– Not generalized or localized to other abdominal or Not generalized or localized to other abdominal or
chest regionschest regions–– Not relieved by defecation of passage of flatusNot relieved by defecation of passage of flatus–– Not fulfilling criteria for gallbladder and sphincter of Not fulfilling criteria for gallbladder and sphincter of
Oddi disordersOddi disorders
–– Symptoms for the last 3 months with onset at least 6 Symptoms for the last 3 months with onset at least 6 months before diagnosismonths before diagnosis

This patient has no warning symptoms or This patient has no warning symptoms or signs. What do you want to do next?signs. What do you want to do next?
Upper endoscopyUpper endoscopyTest for Test for H. pyloriH. pylori–– If positive, eradicateIf positive, eradicate
Empirical antiEmpirical anti--secretory trial (4secretory trial (4--8 weeks)8 weeks)Other testsOther tests–– Ultrasound, CT scan, Gastric emptying, ERCP, Ultrasound, CT scan, Gastric emptying, ERCP,
EGG, functional MR imagingEGG, functional MR imaging

Yield of Other TestsYield of Other Tests
Gastric emptyingGastric emptying–– 2525--40% positive40% positive–– Usually fails to alter managementUsually fails to alter management
UltrasonographyUltrasonography–– 11--3% yield3% yield–– Gallstones are usually incidentalGallstones are usually incidental

Management Trials (1)Management Trials (1)
Test forTest for H. pyloriH. pylori, EGD for positives, EGD for positives–– 3 RCTs3 RCTs–– No benefit over empirical acid suppressionNo benefit over empirical acid suppression–– More expensiveMore expensive
Empiric Empiric H. pyloriH. pylori eradicationeradication–– Not tested in U.S.Not tested in U.S.–– Needs high prevalence to be feasibleNeeds high prevalence to be feasible
Neither strategy reasonable in U.S.Neither strategy reasonable in U.S.

Management Trials (2)Management Trials (2)
Early EGD vs. empiric acid suppressionEarly EGD vs. empiric acid suppression–– 5 prospective trials5 prospective trials–– No clear benefit from EGD despite greater costsNo clear benefit from EGD despite greater costs
Early EGDEarly EGD vs. vs. H. pyloriH. pylori test & treat test & treat –– EGD cured 4% (95% C.I. 1EGD cured 4% (95% C.I. 1--8%) more 8%) more
dyspepsia, but at substantial cost increase dyspepsia, but at substantial cost increase ($7000 per dyspepsia cure)($7000 per dyspepsia cure)

Management Trials (3)Management Trials (3)
Empiric acid suppression vs. placeboEmpiric acid suppression vs. placebo–– PPI therapy more effective in symptom reliefPPI therapy more effective in symptom relief–– Symptom odds 0.65 (95% CI .55Symptom odds 0.65 (95% CI .55--.78).78)–– PPI more effective against heartburn than PPI more effective against heartburn than
epigastric painepigastric painH. pyloriH. pylori T&T vs. empiric acid suppressionT&T vs. empiric acid suppression–– H. pyloriH. pylori T&T more effective in some trialsT&T more effective in some trials–– Equivalent costsEquivalent costs–– Data heterogeneousData heterogeneous

Uninvestigated DyspepsiaUninvestigated DyspepsiaManagement TrialsManagement Trials
SummarySummary
Empirical PPI > H2RA or placeboEmpirical PPI > H2RA or placeboH. pyloriH. pylori test & treat > empirical PPItest & treat > empirical PPIEarly EGD Early EGD –– Equivalent to empiric PPIEquivalent to empiric PPI–– Minor advantage over Minor advantage over H. pyloriH. pylori test & treattest & treat–– Greatly increased costsGreatly increased costs

Factors Affecting Optimal StrategyFactors Affecting Optimal StrategyPrevalencePrevalence–– H. pyloriH. pylori–– PUDPUD
Response of FDResponse of FD–– PPIPPI–– H. pyloriH. pylori eradicationeradication
Recurrence rate Recurrence rate –– FD after empirical therapyFD after empirical therapy
Cost of EGDCost of EGDValue of negative EGDValue of negative EGDMedicalMedical--legal impact of missing gastric cancerlegal impact of missing gastric cancer

Value of Negative EndoscopyValue of Negative Endoscopy
StudiesStudies–– Prompt EGD vs. empiric H2RAPrompt EGD vs. empiric H2RA
Satisfaction improved in EGD subjectsSatisfaction improved in EGD subjects
–– Open access EGDOpen access EGDDyspepsia consultations decreased 57%Dyspepsia consultations decreased 57%
–– Cohort study of EGDCohort study of EGDHealth preoccupation and illness fear improvedHealth preoccupation and illness fear improved
Bytzer. Lancet 1994; Hungin. Br J Gen Pract 1994; Quadri. APT 2003

Potential Benefits of Empirical PPIPotential Benefits of Empirical PPI
Treats PUDTreats PUD > 90 %> 90 %Treats atypical GERDTreats atypical GERD 50 50 –– 80 %80 %Treats FDTreats FD 30 30 –– 50 %50 %Reflects current practice in primary careReflects current practice in primary care““Acid testAcid test””: non: non--response predicts probable FDresponse predicts probable FD

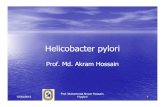
Uninvestigated DyspepsiaUninvestigated Dyspepsia
Spiegel B, Ofman J. Gastroenterology 2002
$2535
$1996
$2078
$2124
Hp Test & Treat
PPI TrialHp T&T
EGD
EGD
PPI trial
EGD
EGD
CostSymptom Free Patient

Uninvestigated DyspepsiaUninvestigated Dyspepsia
Spiegel B, Ofman J. Gastroenterology 2002
$2535
$1996
$2078
$2124
Hp Test & Treat
PPI TrialHp T&T
EGD
EGD
PPI trial
EGD
EGD
CostSymptom Free Patient

Which nonWhich non--invasive Hp test?invasive Hp test?
Rapid Rapid ““near patientnear patient””ELISA serologic testsELISA serologic testsUrea breath testUrea breath testStool antigen testsStool antigen tests

TestTest Sensitivity Specificity Cost
Near patient testNear patient test 71 %71 % 88 %88 % $6$6ELISAELISA 85 %85 % 79 %79 % $30$30UBTUBT 97 %97 % 95 %95 % $60$60--200200Stool antigen assayStool antigen assay 93 %93 % 93 %93 % $60$60
NonNon--invasive Hp testsinvasive Hp tests

Despite my recommendations, you Despite my recommendations, you perform EGDperform EGD
EGD is normalEGD is normalManagement options:Management options:–– Test for Test for H. pylori H. pylori at time of EGDat time of EGD–– Acid suppressionAcid suppression–– Further testingFurther testing
Abdominal CTAbdominal CTUSUSGastric emptyingGastric emptying
–– ReassuranceReassurance

Tests for Hp at EndoscopyTests for Hp at Endoscopy
SensitivitySensitivity SpecificitySpecificity CommentsComments
Rapid Rapid ureaseurease testtest 8080--95 %95 % 9595--100 %100 % Inexpensive; < 24 h;Inexpensive; < 24 h;Reduced w/ PPI, bleedReduced w/ PPI, bleed
HistologyHistology 9090--95 %95 % 9595––98 %98 % Expensive; 48 h;Expensive; 48 h;GiemsaGiemsa > H&E> H&E
CultureCulture variesvaries 100 %100 % Expensive; tedious;Expensive; tedious;antibiotic sensitivityantibiotic sensitivity

Hp Testing PreHp Testing Pre-- and Postand Post--TreatmentTreatment
Methods:Methods:–– 345 patients with duodenal ulcers345 patients with duodenal ulcers–– EGD at 0, 8 weeks (4 weeks after EGD at 0, 8 weeks (4 weeks after H. pyloriH. pylori treatment)treatment)–– Histology: 2 Histology: 2 antralantral, 2 body biopsies, 2 body biopsies–– RUT: 1 RUT: 1 antralantral biopsybiopsy–– Culture: 1 Culture: 1 antralantral, 1 body biopsy, 1 body biopsy
Gold standardGold standard–– Hp Hp ““positivepositive”” = positive RUT plus positive histology or culture= positive RUT plus positive histology or culture
Laine, GI Endoscopy 2000Laine, GI Endoscopy 2000

PrePre-- and Postand Post--Therapy YieldTherapy Yield
PrePre--TherapyTherapy PostPost--TherapyTherapyAntralAntral histologyhistology 98 %98 % 81 %81 %Body histologyBody histology 98 %98 % 81 %81 %AntralAntral/body histology/body histology 100 %100 % 85 %85 %AntralAntral cultureculture 85 %85 % 64 %64 %Body cultureBody culture 86 %86 % 68 %68 %AntralAntral/body culture/body culture 88 %88 % 68 %68 %AntralAntral CLO + histologyCLO + histology 92 %92 %AntralAntral CLO + CLO + antralantral/body /body histohisto 96 %96 %
Caveats: Caveats: Duodenal ulcer, 1 central pathologist (experienced) using Duodenal ulcer, 1 central pathologist (experienced) using GentaGentastain, In stain, In antrumantrum and body, 1 biopsy as good as two (2and body, 1 biopsy as good as two (2--3 % difference)3 % difference)

RecommendationsRecommendationsDr. McQuaidDr. McQuaid
3 biopsies: 3 biopsies: –– 2 2 antrumantrum
Histology, especially if GU or postHistology, especially if GU or post--therapytherapyRUTRUT
–– 1 body1 bodyHistologyHistology
–– If rapid If rapid ureaseurease test positive, dontest positive, don’’t send histology!t send histology!

Functional DyspepsiaFunctional Dyspepsia
The patient undergoes EGD which is normal. The patient undergoes EGD which is normal. •• Biopsies taken for H. pyloriBiopsies taken for H. pylori
•• RUT is negative. RUT is negative. •• Histology is negativeHistology is negative
Diagnosis of Functional DyspepsiaDiagnosis of Functional Dyspepsia
Now what? Now what?

Functional DyspepsiaFunctional DyspepsiaTherapiesTherapies
Acid suppressionAcid suppressionH. pyloriH. pylori eradicationeradicationProkineticProkinetic agentsagents–– CisaprideCisapride–– TegaserodTegaserod
AntidepressantsAntidepressants–– TricyclicTricyclic–– SSRISSRI
Psychological therapyPsychological therapy

Functional DyspepsiaFunctional DyspepsiaAcid SuppressionAcid Suppression
H2RAH2RA–– 11 trials, significant heterogeneity11 trials, significant heterogeneity–– Unable to determine efficacyUnable to determine efficacy
PPIPPI–– 8 trials8 trials–– PPI superior to placeboPPI superior to placebo
Symptom RR 0.86 (95% C.I. 0.78Symptom RR 0.86 (95% C.I. 0.78--0.95)0.95)
AGA Technical Review. Gastro 2005

Functional DyspepsiaFunctional DyspepsiaH. pyloriH. pylori EradicationEradication
13 trials in 3180 subjects with FD13 trials in 3180 subjects with FDEradication superior to placeboEradication superior to placebo–– Symptom RR 0.91 (95% C.I. 0.87Symptom RR 0.91 (95% C.I. 0.87--0.96)0.96)–– NNT 17 (95% C.I. 11NNT 17 (95% C.I. 11--33)33)
AGA Technical Review. Gastro 2005

ProkineticProkinetic AgentsAgents
14 studies of 1053 subjects14 studies of 1053 subjects–– Significant reduction in dyspepsiaSignificant reduction in dyspepsia–– RR 0.52 (95% C.I. 0.37RR 0.52 (95% C.I. 0.37--0.73)0.73)–– All but one study evaluated All but one study evaluated cisapridecisaprideTegaserodTegaserod–– 2 RCT, placebo controlled trials (N=>2600)2 RCT, placebo controlled trials (N=>2600)–– Significant benefit over placebo in Significant benefit over placebo in ½½ studiesstudies–– % days with satisfactory relief of symptoms% days with satisfactory relief of symptoms
32.2%; 31.9% tegaserod32.2%; 31.9% tegaserod26.6%; 29.4% placebo (p=0.0002; 0.06)26.6%; 29.4% placebo (p=0.0002; 0.06)
AGA Technical Review. Gastro 2005; Talley. Am J Gastro 2006

AntiAnti--DepressantsDepressants
MetaMeta--analysisanalysis–– More effective than placeboMore effective than placebo–– NNT 3 (95% C.I. 2NNT 3 (95% C.I. 2--7)7)
AmitriptylineAmitriptyline–– Single doubleSingle double--blind placebo controlled blind placebo controlled
crossover studycrossover study–– 50mg QHS vs. placebo50mg QHS vs. placebo–– RR symptoms 0.4 (95% CI RR symptoms 0.4 (95% CI 0.110.11--1.211.21))
AGA Technical Review. Gastro 2005

Psychological TherapyPsychological Therapy
4 trials4 trials–– Applied relaxationApplied relaxation–– Psychodynamic psychotherapyPsychodynamic psychotherapy–– Cognitive therapyCognitive therapy–– HypnotherapyHypnotherapyImprovement in dyspepsia symptoms Improvement in dyspepsia symptoms scores over placeboscores over placebo–– Unable to synthesize dataUnable to synthesize data–– Insufficient evidenceInsufficient evidence
AGA Technical Review. Gastro 2005

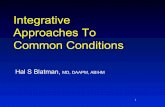
Uninvestigated DyspepsiaUninvestigated Dyspepsia
UninvestigatedDyspepsia
Heartburn or Acid Regurgitation NSAID Exclude GERD
or NSAID
Acid Suppression D/C NSAID, switch,or add PPI NEXT!

UninvestigatedDyspepsia
Age >55 orAlarm symptoms
Age ≤55No alarm symptoms
EGD Test for H. pylori
positiveEradicate H. pylori
negativePPI trial (4-6 weeks)
FailPPI trial (4-6 weeks)
Reassurancereassess
Consider EGD

Investigated DyspepsiaInvestigated Dyspepsia
EGD
Structural Disease Normal EGDFunctional Dyspepsia
Treat Underlying Disease
H. pylori test (RUT/Histology)
PositiveH. pylori therapy
NegativeAlternative therapies

Functional DyspepsiaFunctional DyspepsiaManagementManagement
ReassuranceReassurance–– Realistic goalsRealistic goals–– Cognitive therapy (symptom diary)Cognitive therapy (symptom diary)–– Waxing and waning symptomsWaxing and waning symptoms
Medical therapyMedical therapy–– Acid suppressionAcid suppression–– H. pyloriH. pylori eradicationeradication–– ProkineticProkinetic agentsagents–– AntidepressantsAntidepressants
Psychological therapyPsychological therapy