S KIN C ANCER Amy Stinson ENT Resident Affinity Medical Center.
33
SKIN CANCER Amy Stinson ENT Resident Affinity Medical Center
-
Upload
rosalind-moore -
Category
Documents
-
view
215 -
download
0
Transcript of S KIN C ANCER Amy Stinson ENT Resident Affinity Medical Center.

SKIN CANCERAmy Stinson
ENT Resident
Affinity Medical Center

SKIN CANCER
Most common human malignancy US: >1,300,000 cases annually 2,000 deaths annually (non-melanoma) Most common location – sun exposed areas
of head and neck Basal Cell accounts for 90% (baileys) Squamous cell next most common, then
melanoma Pearls: What is the reported ratio of BCC to
SCC in the US? 4:1
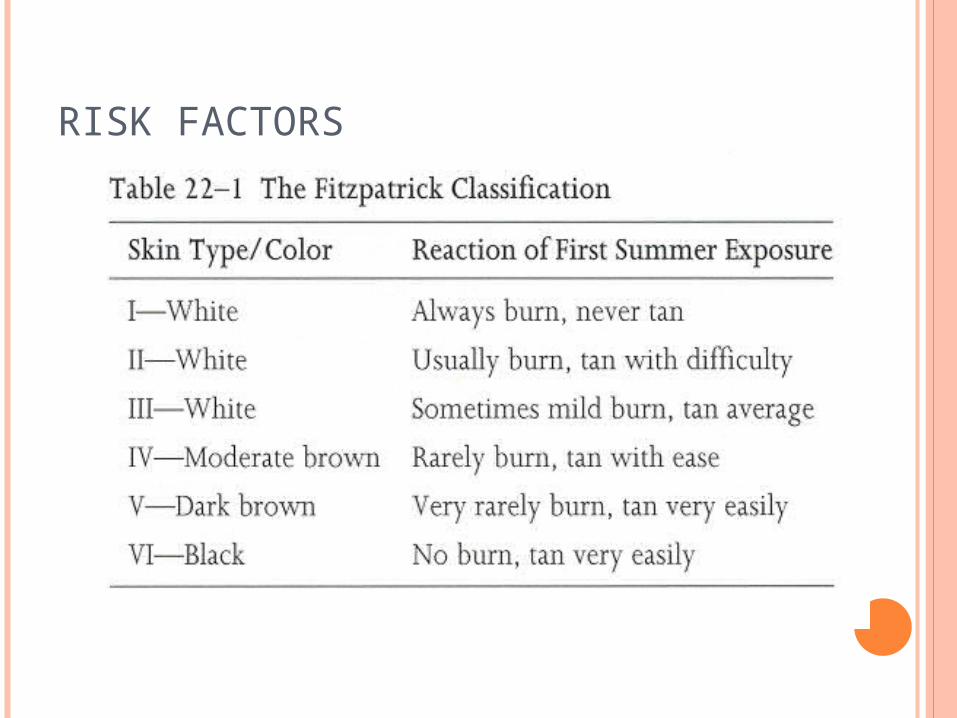
SKIN CANCER RISK FACTORS Age > 60 UV light exposure
Pearls: specifically UV B (280-320nm) Specific Traits: fair complexion, blue/green eyes,
light hair, inability to tan, celctic ancestry Hx of multiple or severe sunburns Tanning bed use
Mainly UV A – UV A synergistically augments UV B response
Arsenic exposure Chronic radiodermatits (pearls) Immunosuppression (pearls) Trauma: burns, ulcers or scars
Pearls: Marjolin Ulcer
RISK FACTORS

RISK FACTORS
Genetic disorders (Pearls) Basal Cell-Nevoid Syndrome (Grolin’s)
Aut Dom, multiple BCC, odontogenic keratocysts, rib abnormailties, palmar/plantar pits, calcification of falx cerebri
Xeroderma pigmentosa Albinism Epidermisdysplastic verruciformis Epidermolysis bullosa dystrophica Dyskeratosis congenital

NORMAL SKIN

NORMAL SKIN
5 layers of epidermis from superficial to deep (Pearls) Stratum Corneum Stratum Lucidum Stratum Granulosum Stratum Spinosum Stratum Basale
Pneumonic: Come, Let’s Get Sun
Burned

BASAL CELL Slowly growing malignancy
of the epidermis Extends peripherally
without vertical invasion Rarely metastasizes Cells appear histologically
similar to basal cells of epidermis (small dark blue cells with little cytoplasm)
BCC – clefting, lack of intracellular bridges, nuclear pallisading, peritumoral lucunae

Basal Cell
Growth pattern (pearls) Follows the path of least resistance Typically along embryonic fusion planes Susceptible areas:
Inner canthus Philtrum Mid - Lower chin Nasolabial groove Periauricular area Retroauricular sulcus

BASAL CELL Clinical subtypes (pearls)
Nodular – Most Common Pearly, telangiectatic papule, central ulceration, rolled
border Superficial
Rare in H & N, scaly, waxy, indurated, irregular More common on extremeties and trunk
Pigmented/Cystic Similar to nodular type, more pigmented resembling
melanoma or benign nevus Morpheaform
Common on face, flat or depressed, indurated, aggressive with high rate of recurrence, worst prognosis, can resemble scar
Keratotic aggressive

BASAL CELL
NodularSuperficial
Pigmented

BASAL CELL
MorpheaformPost - excision

BASAL CELL
Management Avoid excess sun – sunblock Careful follow-up for recurrence
Pearls: After having one (BCC or SCC) what are the chances of developing another within 5 yrs?
50% Curettage with Electrodisiccation Cryosurgery Scalpel excision – need 5 mm margins Radiation therapy – poor operative candidates Mohs – for high risk areas, morpheaform 1/3 of incompletely excised BCC will recur

SQUAMOUS CELL
More aggressive Higher recurrence rates Vertical extension 1-4% metastatic potential
Scar/chronic inflam > de novo > from AK Signs:
Erythematous, hyperkeratotic, opaque nodule, ulcerative, granular base, bleeds easily
SCC that arise in sun exposed areas have better prognosis than those arising de novo

SQUAMOUS CELL
Histopath Keratin pearls Broder Classification
1 – well differentiated 4 – poorly differentiated
Types: Adenoid Bowenoid Verrucus – mc in oral mucosa Spindle-pleomorphic – least common Generic – from actinic change

SQUAMOUS CELL
Premalignant Lesions Actinic Keratosis
Most common Sun exposed skin Less than 1 cm Chance of progression – 20% Erythematous patch with scale Can have cutaneous horn
Pearls: Most common premalignant lesion of H & N? AK

TYPICAL AK
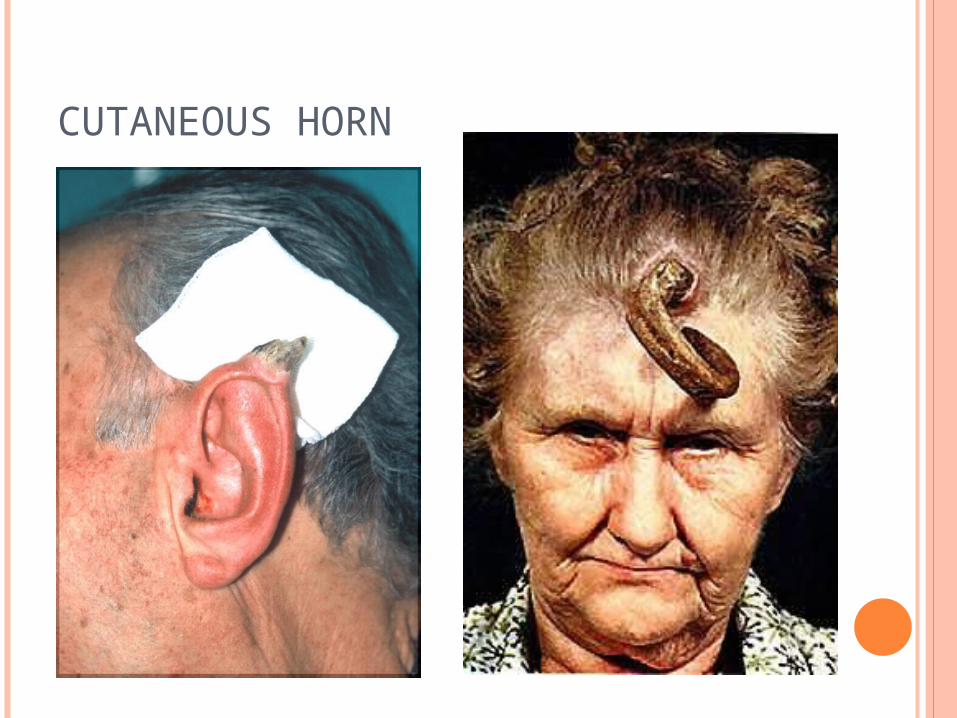
CUTANEOUS HORN

SQUAMOUS CELL
Premalignant Lesions Bowen Disease
Pearls: Squamous cell carcinoma in situ of the skin Full thickness dysplasia of epidermis Well circumscribed Common with hx of arsenic exposure
Keratoacanthoma (pearls) Benign, usually self limited Common in older males 2-6 mo hx of rapid growth – usually on nose Central area of ulceration – volcano-like Spontaneous involution

KERATOACANTHOMA
SQUAMOUS CELL The following are features of high-risk SCC:
Size Width greater than 2 cm Depth greater than 4 mm
Location Ear Lip
Histologic features Perineural invasion Lymphovascular invasion Poorly differentiated grade
Recurrence Immunosuppression
MANAGEMENT
Initial evaluation involves Assessment of location Punch or excisional biopsy Staging

AJCC CLASSIFICATION TNM staging system for NMSC Primary tumor (T)
TX - Primary tumor cannot be assessed. T0 - No evidence of primary tumor Tis - Carcinoma in situ T1 - Tumor 2 cm or less T2 - Tumor larger than 2 cm but smaller than 5 cm T3 - Tumor larger than 5 cm T4 - Tumor invades deep extradermal structures (bone, muscle,
cartilage). Regional lymph nodes (N)
NX - Regional lymph nodes cannot be assessed. N0 - No regional lymph node metastasis N1 - Regional lymph node metastases
Distant metastasis (M) MX - Distant metastasis cannot be assessed. M0 - No distant metastasis M1 - Distant metastasis

MANAGEMENT - CRYOSURGERY
Cryogen such as liquid Nitrogen to kill tumor cells
Typical temperature of -50°C . Tissue-sparing, but leave open wound Hypopigmentation and scarring may result Limited to favorable small lesions with well-
defined borders

MANAGEMENT – RADIATION THERAPY
Used extensively in the past, now sparingly High cure rate (95%) Does not allow surgical staging Protracted treatment course, and expensive Radiodermatitis, delayed carcinogenesis Currently reserved for poor operative
candidates, adjuvant in high risk malignancy

PHOTODYNAMIC THERAPY Photosensitizing drug (porphyrin, 5-ALA)
applied topically, orally or parenterally and localizes into tumor cells
Drug is activated by exposure to light (laser) Efficacy is low (45%) Side effects include local edema, erythema,
blistering, ulceration Used as palliation

MANAGEMENT - EXCISIONAL SURGERY Most often used by surgeons, esp for larger
lesions Can be with cold steel or laser Can allow reconstruction in the same sitting Frozen sections decrease recurrence rate Can be time consuming and inconvenient If more than 1/3 of a cosmetic facial unit is
excised, better cosmesis with removal of entire unit
Success rate 93-95%

MANAGEMENT – EXCISIONAL SURGERY
MOHS SURGERY - INDICATIONS Recurrent skin cancer Skin cancer in “high risk anatomic areas” and
cosmetically important areas Histologically aggressive skin cancer Large skin cancers Skin cancer with ill-defined clinical margins Irradiated skin Dermatofibrosarcoma Protuberans Selected mucosal squamous cell cancers

LYMPHATIC DISSECTION No hard and fast rules
governing lymphatic dissection in N0 Necks
Elective Parotidectomy for deeply invasive tumors of the periauricular region
Large SCCA (>2cm), recurrent SCCA, Marjolin’s ulcer, perineural invasion may require regional lymphadenectomy
Prophylactic neck when SCC >4 cm with deep invasion arising on cheek, neck, scalp

RARE CUTANEOUS MALIGNANCIES
Merkel’s Cell Carcinoma Tumor arising from pluripotential
basal cells within or around hair cells (pearls)
Poorly differentiated histology High rate of recurrence and
lymph node metastasis requires excisional surgery with adjuvant radiation and treatment of lymphatic drainage in most cases
NO neck should be treated Solitary erythematous to deep
purple plaque or nodule of up to several centimeters in size
RARE CUTANEOUS MALIGNANCIES
Dermatofibrosarcoma Protuberans Arises in dermis, spreads deeply Large indurated plaque with firm irregular flesh
colored nodules Mohs is treatment of choice
Pilomatrix Carcinoma Arises from Pilomatricoma, a benign tumor of
hair matrix origin Aggressive wide local excision is treatment

THE END
Questions?