FISIOLOGI GINJAL
56
Unit 1 - Objective 1 F I S I O L O G I HEWAN II
-
Upload
alpharose-dotorg -
Category
Documents
-
view
227 -
download
1
Transcript of FISIOLOGI GINJAL

Unit 1 - Objective 1
F I S I O L O G I HEWAN II

Unit 1 - Objective 1
YANG DIPELAJARI
EKSKRESI---GINJAL + KULIT THERMOREGULASI ENDOKRINOLOGI OTOT REPRODUKSI SARAF

Unit 1 - Objective 1
Pustaka : Guyton, Fisiologi manusia dan
mekanisme penyakit Ganong, Review Fisiologi Kedokteran

Unit 1 - Objective 1
EKSKRESI? SEKRESI?

Unit 1 - Objective 1
GINJALFungsi umum ginjal : mengatur volume cairan badan, tek. osmotik dan
keseimbangan elektrolit pengaturan keseimbangan asam basa pengeluaran zat2 yg tidak berguna ; urea, uric acid penyimpanan substansi energi yg menguntungkan :
glukosa, asam amino detoksifikasi

Unit 1 - Objective 1
fungsi endokrin : eritropoetin,renin (??) Pelepasan prostaglandin
menyebabkan pembuluh darah ginjal berdilatasi yang berperan dalam pengaturan aliran darah ke ginjal

Unit 1 - Objective 1
Aktivasi vitamin D Vitamin D dibuat di kulit , dirubah menjadi vit D3 oleh
ginjal Vit D3 membantu homeostasis dengan meningkatkan
absorbsi kalsium dari tractus digestivus
Sekresi H+ dan reabsorbsi HCO3-
Eliminasi ion hidrogen yangberlebihan dan conserves zat buffer spt bikarbonat shg dpt mengontrol pH cairan tubuh

Unit 1 - Objective 1
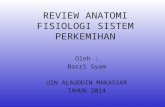
Anatomi ginjal
Capsule
Renal VeinRenal ArteryCortex
Pyramid
PapillaCalyx
Pelvis
Ureter
Column
Medulla
Nephron

Unit 1 - Objective 1
Fungsi utama ginjal :
Membuat urin, meliputi : ekskresi sisa metabolisme reabsorbsi zat yg msh bermanfaat----Atur
kadar komponen cairan tubuh -----(homeostasis)

Unit 1 - Objective 1
Sistem Urinaria
Renal arteryKidney
Ureter
Urinary Bladder
Renal Vein
For sphincters, see nex slide

Unit 1 - Objective 1
SISTEM URINARIA
Internal urethral sphincterExternal Urethral Sphincter
Male Sphincters
Female Sphincters

Unit 1 - Objective 1
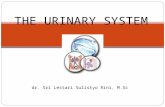
Anatomi faali ginjalterdiri dari nefron : glomerulus tubulus kontortus proximalis ansa henle tubulus kontortus distalis bbrp nefron bermuara pd tub. kolektivus----duktus
kolektivus

Unit 1 - Objective 1
NEFRON
Efferent arteriole
Afferent arteriole
Bowman’s capsule
Collecting duct
Proximal convoluted tubuleGlomerulus
Peritubular capillaries
Vasa recta
Decending limb of loop of Henle
Ascending limb of loop of Henle
Distal convoluted tubule
Unit 1 - Objective 4

Unit 1 - Objective 1
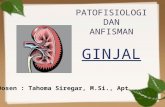
Glomerulus diameter ±200 mikron luas permukaan filtrasi kapiler 1,5 m2 tdr anyaman kapiler diselubungi kantong buntu spt
mangkok ----kapsula bowman permeablitas kapiler tinggi, membrana basalis kapiler
berpori2. arteriola afferen-----anyaman (rete) kapiler---arteriola
efferen scr fungsional hanya dpt dilewati zat diameter < 8 nm pembuatan urin dimulai dlm kapiler glomerulus-----
mjd ultra Filtrat

Unit 1 - Objective 1
Glomerulus
Afferent Arteriole
Efferent Arteriole
Bowman’s Capsule
Proximal Convoluted Tubule
Glomerulus

Unit 1 - Objective 1
Tubulus konvulatus proksimalis panjang 14 mm, diameter 55 mikron epitel kuboid simplek mpy “brush border” ---mikrovilli banyak mgdg mitokondria (energi utk transpor aktif) Reabsorbsi filtrat : sodium (65%), water (65%),
bicarbonate (90%), chloride (50%), glucose (nearly 100%!), etc
Sekresi obat, sampah dan ion hidrogen
Unit 1 - Objective 4

Unit 1 - Objective 1
Ansa henle sel epitel sangat tipis pori2 luas, permeabilitas besar ada 2 bagian---masuk medula dsbt
pars descendent, meninggalkan medula pars ascendent---ke korteks---mendekati glomerulus---nampak padat berinti dsbt makula densa-----ke tub. distalis

Unit 1 - Objective 1
Afferent Arteriole
Efferent Arteriole
DCT
Macula Densa Cells
Granular Juxtaglomerular (JG) Cells
PCT
Bowman’s Capsule

Unit 1 - Objective 1
Tubulus kontortus distalis di korteks tdk py makula densa bermuara pd tub. kolektivus banyak mitokondria di membran basalis

Unit 1 - Objective 1
Pembentukan urin Urin : larutan encer mgdg limbah hasil
metabolisme berasal drdarah. Warna kuning---urokrom
Proses pembentukan urin A. filtrasi glomeruli B. reabsorbsi tubulus C. sekresi tubulus

Unit 1 - Objective 1
Filtrasi Glomeruli darah dlm kapiler glomeruli dipisahkan dr
cairan filtrat glomeruli dlm kapsula bowman oleh filter yg tdr dr 3 lapisan
1. endotelium kapiler 2. Podocyt 3. epitel pars visceralis kapsula bowman (py
celah diameter 25 nm)

Unit 1 - Objective 1
Mekanisme Filtrasi Glomerular
Bowman’s Capsule
Glomerulus
Fenestrated Capillary
Podocyte with Basement Membrane

Unit 1 - Objective 1
Aliran darah ginjal(RBF = renal blood flow)
25% dr curah jantung (1200 ml/menit)
Proses filtrasi glomerulus tjd krn adanya: 1. tek. Hidrostatik drh di kapiler glomerulus (pB) 2. tek. Hidrostatik dalam kapsula bowman (pC) 3. tek. Kolloid osmotik protein plasma (pCo)

Unit 1 - Objective 1
Gaya Netto
(Effective Filtration Pressure/EFP)
EFP = PB-PC-PCo
EFP = 55-15 -30
= 10 mmHg

Unit 1 - Objective 1
Laju Filtrasi Glomerulus (GFR= Glomerulus Filtration Rate) jumlah filtrat yang disaring dari plasma dlm
satu menit mis. GFR 125 ml/mnt---tiap jam 7,5 liter
filtrat---tiap hari 180 liter filtrat Padahal produksi urin ± 1 liter / hari----artinya
99% filtrat direabsorbsi kembali

Unit 1 - Objective 1
Tekanan hidrostatik kapiler glomeruli berubah2 tergantung:
vasokontriksi a. afferent—tek. drh glomerulus<< tek. Filtrasi effektif<<
vasokontriksi a. effrent----tek. drh. glomerulus>>tek. Filtrasi effektif>>
vasodilatasi a. afferent----tek. drh glomerulus>> tek. Filtrasi efektif>>
vasodilatasi a. efferent----tek. drh glomerulus << tek. Filtrasi glomerulus <<

Unit 1 - Objective 1
Faktor2 yg mempengaruhi GFR
1. Perubahan tekanan hidrostatik dalam kapiler glomeruli
olah raga berat---tek, drh umum meningkat---vasokonstriksi a. aferent (rangsangan sy. Simpatik)-----GFR turun----urin sedikit
-minum kopi---kafein sebabkan vasodilatasi a. afferent---GFR naik---urin banyak

Unit 1 - Objective 1
2. Perubahan tekanan hidrostatik kapsula Bowman
obstruksi jalan kencing (mis. : batu ginjal/parasit)---tek. hidrostatik kaps. Bowman meningkat----GFR turun

Unit 1 - Objective 1
3. Perubahan tekanan kolloid osmotik plasma
Dehidrasi (minum<<, diare/muntah)---GFR turun
Hiperproteinemia---tek. koloid osmotik plasma meningkat----GFR turun

Unit 1 - Objective 1
4. Perubahan permeabilitas membran glomeruli
Penyakit ginjal (mis. : radang)---kapiler glomeruli permeable---protein plasma ikut masuk---proteinuria/albuminuria

Unit 1 - Objective 1
5. perubahan luas filtrasi penyakit ginjal + nephrectomy parsial---
rusak glomeruli----luas area berkurang----GFR turun

Unit 1 - Objective 1
Mekanisme perpindahan air dan
NaCl
Unit 1 - Objective 7
?
?
?
?

Unit 1 - Objective 1
Persentase cairan filtrat glomerulus yg direabsorbsi dlm tiap segmen tubulus sbb. :
% Tub. proximalis 65 Lenkung Henle 15 Tub. distalis 10 Duktus kolektivus 9,3 Mengalir sbg urin 0,7

Unit 1 - Objective 1
Reabsorbsi air dipengaruhi hormon antidiuretic hormon
(ADH=vasopresin)---hipofisis posterior pembebasan diatur oleh osmoreseptor fungsi meningkatkan permeabilitas tub. thd air----
meningkatkan reabsorbsi air darah encer (mis.banyak minum)---kadar ADH turun----
reabsorbsi air berkurang—urin banyak darah pekat---- (mis. : ???) kadar ADH naik----reabsorbsi
air bertambah----urin sedikit gangguan produksi ADH---produksi air banyak---
diabetes insipidus tekanan osmotik dr isi tubulus---pengaruhi jumlah air yg
diambil-->>garam, gula (diabetes mellitus)

Unit 1 - Objective 1
Reabsorbsi Glukosa absorbsi scr transport aktif kemampuan reabsorbsi glukosa oleh sel2 tub. terbatas nilai ambang ginjal= batas kemampuan sel2 tub.
reabsorbsi glukosa scr sempurna contoh : kadar gula nomal mns 60-100mg/100cc jika
kadar glukosa drh 180 mg/100cc( diabetes mellitus)-----sisanya
(80 mg/ 100cc)dibuang bersama urin----glikosuria

Unit 1 - Objective 1
Fungsi Juxtaglomerular Apparatus• Memelihara tekanan darah• Jika tekanan darah turun, sel granular JG akan
melepaskan renin Renin
• angiotensinogen angiotensinogen I ACE(angiotensin converting enzime)
angiotensinogen I angitensinogen II
vasokonstriktor
tekanan darah
Unit 1 - Objective 6Granular juxtaglomerular cell

Unit 1 - Objective 1
Angiotensin II jg menstimuli pelepasan aldosteron dr adrenal korteks
Aldosteron menstimuli tub. Konvul. Distalis utk mengabsorbsi NaCl
Reabsorbsi garam menyebabkan air akan berpindah ke darah, meningkatkan volume shingga meningkatkan tekanan darah.
Unit 1 - Objective 6

Unit 1 - Objective 1
makula densa cells akan memonitor kandungan garam dalam darah
Jika kandungan garam terlalu tinggi , makula densa sel akan menghambat sel granular dan menekan pelepasan renin
Unit 1 - Objective 6
Makula densa

Unit 1 - Objective 1
Penekanan renin beraksi sbagi mekanisme feedback negatif yg mencegah peningkatan angiotensin II, aldosteron dan tekanan darah
Unit 1 - Objective 6

Unit 1 - Objective 1
The Counter Current Mechanism We will begin our discussion of the counter current mechanism with the ascending limb of the loop of Henle (ALLH). This portion of the nephron reabsorbs chloride by active transport. As chloride moves from the filtrate it pulls along sodium into the interstitium of the medulla. The medulla then becomes very hyperosmotic
Unit 1 - Objective 7

Unit 1 - Objective 1
The Counter Current MechanismAs salt (NaCl) leaves the ALLH, the osmolarity of the fluid decreases from 1,200 to 100 milliosmoles/L (mOSM/L). This happens because the ALLH is impermeable to water. The net effect of this activity is to remove salt from the kidney filtrate and transfer it into the medulla where it can be saved for use by the body.
Unit 1 - Objective 7

Unit 1 - Objective 1
The Counter Current MechanismThe accumulated salt in the interstitium of the medulla acts as an osmotic force which can be used to “draw” and conserve water from other parts of the nephron: the decending limb of the Loop of Henle (DLLH) and the collecting duct. The DLLH is a thin passive segment that is permeable to water, but, impermeable to salt.
Unit 1 - Objective 7

Unit 1 - Objective 1
The Counter Current MechanismAs the DLLH gives up water to the medullary interstitium, the osmolarity of the fluid changes from 300 to 1,200 mOSM/L. The net effect of this process is to conserve water for the body. Thus, the loop of Henle actively transfers salt back into the kidney which can be used to save water osmotically. A remarkable process!
Unit 1 - Objective 7

Unit 1 - Objective 1
The Counter Current MechanismThe hyperosmotic interstitium of the medulla will also “pull” and conserve water from the collecting duct, but, on a variable basis depending on the availibility of ADH. As water moves from the collecting duct, urea will follow. Thus, as water is conserved at this level, a certain amount of urea is also conserved. The urea contributes to the high osmolarity of the medulla
Unit 1 - Objective 7

Unit 1 - Objective 1
The Counter Current MechanismThe availibility of Antidiurectic Hormone (ADH) is determined by dehydration and thirst. Under these conditions, the hypothalamus makes extra ADH and stores it in the posterior pituitary where it can be released. The increased release of ADH causes the “water pores” of of the collecting duct to open and allow water to move from the urine to the medulla.
Unit 1 - Objective 7

Unit 1 - Objective 1
The Counter Current MechanismAs water leaves the collecting duct, the urine becomes progressively more concentrate. The osmolarity of the collecting duct fluid will increase from about 150-300 to 1,200 mOsm/l. under these conditions. If ADH is not present, water is not conserved and is lost as part of a dilute urine (100 mOsm/l).
Unit 1 - Objective 7

Unit 1 - Objective 1
The Counter Current MechanismThe vasa recta is made up of a group of capillary like vessels and is freely permeable to salt and water. The vessels of the vasa recta roughly flow counter to the loop of Henle and acts as a counter current exchanger. As blood flows through the vasa recta it picks up water and leaves behind salt. Thus, the vasa recta returns conserved water back to the body and leaves the salt which maintains the hyperosmotic medulla.
Unit 1 - Objective 7

Unit 1 - Objective 1
Objective 8If the kidneys filter 16 grams of NaCl per day and then reabsorb 14 grams of NaCl per day, then 2 grams of NaCl would be excreted or eliminated by the kidneys per day as part of the urine.
Amount Excreted = Amount Filtered - Amount Reabsorbed
2 g NaCl/day = 16 g NaCl/day - 14 g NaCl/day
Unit 1 - Objective 8

Unit 1 - Objective 1
Objective 8Examine the following and find the missing value: Amount Excreted = Amount Filtered - Amount Reabsorbed
1) ? = 100 g of glucose - 100 g of glucose
2) 100 g of glucose = ? - 300 g of glucose
3) 100 g of glucose = 400 g of glucose - ?
Answers: (1)equals zero; (2) equals 400; (3) equals 300
Unit 1 - Objective 8

Unit 1 - Objective 1
Plasma Clearance
Plasma clearance is defined as the amount of plasma that is cleared or “cleansed” of a particular substance in one minute. The kidneys will carry out this clearance process through the use of filtration, reabsorption and secretion.
Unit 1 - Objective 9

Unit 1 - Objective 1
Plasma ClearanceFiltration will directly affect clearance. As filtration increases, more material will be removed from the blood plasma. Reabsorption will indirectly affect clearance. As reabsorption increases, less material will be removed from the blood plasma. Secretion will directly affect clearance. As secretion increases, more material will be removed from blood plasma.
Unit 1 - Objective 9

Unit 1 - Objective 1
Plasma Clearance
The formula used to calculate plasma clearance is: C = V x U/P
C = plasma clearance rate in ml/min
V = urine production rate in ml/min
U = the concentration of a substance in the urine in mg/ml
P = the concentration of a substance in the plasma in mg/ml
As you track the units in the equation, you will notice that mg/ml cancel out, leaving ml/min.
Unit 1 - Objective 9

Unit 1 - Objective 1
Plasma Clearance
Let us practice calculating plasma clearance using the clearance equation. In all your calculations, assume that the urine production rate (V) is 2 ml/min. Let’s start with the substance inulin (not insulin!). If after a dose of inulin, your urine has 30 mg/ml and your plasma has 0.5 mg/ml of this substance, what is the inulin clearance rate? If you got 120ml/min, you are correct!
Unit 1 - Objective 9

Unit 1 - Objective 1
Plasma Clearance
If you did not get 120ml/min, look at the following calculation and recheck your work.
120 ml/min = 2 ml/min x 30 mg/ml/ 0.5 mg/ml
Unit 1 - Objective 9

Unit 1 - Objective 1
Plasma ClearanceTest your ability to conduct further calculations by calculating the clearance rate for the following substances:Substance Urine concentration Plasma concentration
Urea 7.0 mg/ml 0.2 mg/ml
Glucose 0.0 mg/ml 1.0 mg/ml
Penicillin 298 mg/ml 0.7 mg/ml
Remember that the urine production rate (2ml/min) will be the same for all of the above calculations. The clearance rate for each of the above substances will be: Urea = 70 ml/min; Glucose = 0 ml/min; Penicillin = 851 ml/min. Were you able to get the right answers? If not, go back and restudy the clearance process.
Unit 1 - Objective 9

Unit 1 - Objective 1
Dialysis Therapy
Dialysis is a process that artificially removes metabolic wastes from the blood in order to compensate for kidney (renal) failure. Kidney failure results in the rapid accumulation of nitrogen waste (urea, etc.) which leads to azotemia. Uremia and ion disturbances can also occur. This condition can cause acidosis, labored breathing, convulsions, coma and death.
Unit 1 - Objective 11