CMT FACTS I - Charcot-Marie-Tooth · PDF fileRoviding information on Charcot-Marie-Tooth...
16
CMT FACTS I ISBN # 1-56806483-X A CMTA Special Report Vol. 1, No. 1 -- - Roviding information on Charcot-Marie-ToothDisorders (aka. Peroneal Muscular Atrophy or Hereditary Motor Sensory Neuropathy), the most common in- herited neuropathy. Published by the Charcot-Marie-Tooth Association. Contents 01993, CMTA. All rights reserved. CMT ... ....... is the most common inherited neuropathy, affecting approximately 125,000 Americans. ....... is also known as peroneal muscular atrophy and hereditary motor sensory neuropathy ....... is slowly progressive, causing deterioration of peripheral newes which control sensory information and muscle function of the fodlower leg and handfoream. ....... causes degeneration of peroneal muscles (located on the front of the leg below the knee). :......causes foot-drop waking gait, foot bone abnormalities, high arches and hammer toes, problems with balance, problems with hand function, occasional lower leg and forearm muscle cramping, loss of some normal reflexes, oc- casional partial sight andlor hearing loss problems, respiratory problems. Scoliosis (curvature of the spine) is some- times present. ....... does not affect life expectancy. .... ... has no effective treatment, although physical therapy, occupational therapy and moderate physical activity are beneficial. ....... is sometimes surgically treated. ....... is usually inherited in an autosornal dominant pattern ....... may become worse if certain neurotoxic drugs are taken. ....... can vary greatly in severity, even within the same family. ....... can, in rare instances, cause severe disability. ....... is the focus of significant genetic research, bringing us closer to answering the CMT enigma. ABOUT THE CMTA: The Charcot-Marie-Tooth Association (CMTA) was founded in 1983 to provide a focal point for those involved with CMT- patients, families, medical professionals, research scientists and others. The CMTA educates by pub- lishing a quarterly newsletter, sponsoringpatient andprofessional conferences, and serving as an information source about CMT. It also coordinates support groups, provides physician referrals, does patient advocacy and works closely with the research conimunip. To join the CMTA, complete the form on the back cover. The Charcot-Marie-Tooth Asso- ciation is a tax-exempt, not-for-projt corporation. This material is presented for educationalpurposes only and is not meant to either diagnose or prescribe. While there is no substitute for profes- sional medical care for Charcot-Marie- Tooth Disorders, these briefs oger current medical opinion that the reader may use to aid and supplement a doc- tor's treatment.
Transcript of CMT FACTS I - Charcot-Marie-Tooth · PDF fileRoviding information on Charcot-Marie-Tooth...

CMT FACTS I ISBN # 1-56806483-X
A CMTA Special Report
Vol. 1, No. 1 -- -
Roviding information on Charcot-Marie-Tooth Disorders (aka. Peroneal Muscular Atrophy or Hereditary Motor Sensory Neuropathy), the most common in- herited neuropathy. Published by the Charcot-Marie-Tooth Association. Contents 01993, CMTA. All rights reserved.
CMT ... ....... is the most common inherited neuropathy, affecting approximately 125,000 Americans.
....... is also known as peroneal muscular atrophy and hereditary motor sensory neuropathy
....... is slowly progressive, causing deterioration of peripheral newes which control sensory information and muscle function of the fodlower leg and handfoream.
....... causes degeneration of peroneal muscles (located on the front of the leg below the knee).
:......causes foot-drop waking gait, foot bone abnormalities, high arches and hammer toes, problems with balance, problems with hand function, occasional lower leg and forearm muscle cramping, loss of some normal reflexes, oc- casional partial sight andlor hearing loss problems, respiratory problems. Scoliosis (curvature of the spine) is some- times present.
....... does not affect life expectancy.
.... ... has no effective treatment, although physical therapy, occupational therapy and moderate physical activity are beneficial.
....... is sometimes surgically treated.
....... is usually inherited in an autosornal dominant pattern
....... may become worse if certain neurotoxic drugs are taken.
....... can vary greatly in severity, even within the same family.
....... can, in rare instances, cause severe disability.
....... is the focus of significant genetic research, bringing us closer to answering the CMT enigma.
ABOUT THE CMTA: The Charcot-Marie-Tooth Association (CMTA) was founded in 1983 to provide a focal point for those involved with CMT- patients, families, medical professionals, research scientists and others. The CMTA educates by pub- lishing a quarterly newsletter, sponsoringpatient andprofessional conferences, and serving as an information source about CMT. It also coordinates support groups, provides physician referrals, does patient advocacy and works closely with the research conimunip. To join the CMTA, complete the form on the back cover. The Charcot-Marie-Tooth Asso- ciation is a tax-exempt, not-for-projt corporation. This material is presented for educational purposes only and is not meant to either diagnose or prescribe. While there is no substitute for profes- sional medical care for Charcot-Marie- Tooth Disorders, these briefs oger current medical opinion that the reader may use to aid and supplement a doc- tor's treatment.

Professionals Facts about C harcot-Marie-Tooth Disorders
Following is a list of professionals yo1 may encounter or to whom you may b referred during the course of CM' management and treatment. W thought it might be helpful to explaii exactly what each is and does.
Neurologist- A medical doctor spe cializing in neurology, the study of dis orders of the nervous system.
Orthopedist- A medical doctor spe cializing in orthoped~cs, the surgical o manipulative treatment of disorders o the skeletal system and associated mo tor organs.
Orthotist- A person who fabricate: braces on an individual basis.
Pbysiatrist- A medical doctor trainec in physical medicine and rehabilita tion.
Podiatrist- A medical doctor special king in the study and treatment of foo ailments.
Pedortbist- A practitioner who pro vides care to the patient by fitting or. thopedic shoes and devices, ix consultation with physicians.
Occupational Tberapist- An OTR, o: registered occupational therapist, has 2
ninimum of a bachelors degree anc us passed registering examinations gelshe incorporates exercises, splint. .ng andlor adaptive utensils to help im. )rove hand function and to enable the ~atient to be as self-sufficient as possi. ~ le .
Physical Therapist- A physical them list will set specific therapeutic exer- ;ises to help maintain and improve nuscle function. Physical therapy is he treatment of disease and injury by nechanical means, such as manipula. ion, massage and exercise, sometimes 11so using heat, light and water. A reg- stered physical therapist has a mini- num of a bachelors degree and has &wed registering examinations.
Charcot-Marie-Tooth (CMT) is an in- herited disorder primarily affecting the peripheral nerves. The muscles of the exuemities- the feet, lower legs and hands, foreanns- are secondarily af- fected and become thin and weak. As the most common inherited neuropathy, it is found in 112,500 people, or at least 125,000 affected people in the U.S.A.
The Name The name, Charcot-Marie-Tooth, is de- rived from the three doctors who de- scribed the disorder in the 1880's. The disorder is also known as hereditary mo- tor sensory neuropathy and peroneal muscular atrophy. The name covers a variety of disorders with similar appear- ances, but the two common varieties are known as Type I and Type 11. In Type I, or hypertrophic CMT, patients have thickened nerves and abnormal fatty covering (myelin) on the nelve fibers. In Type II, or neuronal CMT, the axon or central part of the nerve (as opposed to the myelin, or nerve covering) deterio- rates.
Life &in and intellectual ability are usu- ally unaffected. Perhaps because of the challenges the disorder presents to pa- tients, they often attain substantial skills and professional success. Walking diffi- culties and foot deformities produce the most sigdicant disabilities. Fractures and sprains ofthe ankle and lower leg are not uncommon. The legs can become very thin and are called "stork legs". However, rarely do patients need crutches. In rare cases patients are con- fined to a wheelchair. Hands are some- times affected with a major symptom being a predisposition for the hand to fold in on itself and assume a claw-like position. Some patients may require splints and other aids for activities of daily living such as writing, button fas- tening, turning door knobs, etc. Some patients experience sensory loss in the hands and feet with numbness, burning, and tingling present. Chronic fatigue and weakness can be a problem. Rarely will patients develop central nervous system, eye, ear, respiratory, bladder or bowel problems.
CMT symptoms can become more se- vere during pregnancy, but this is r a ~ . Symptoms usually subside after the birth of the baby. Regardless, any rapid in- crease in the severity of CMT symptoms would warrant further medical evalu- ation for possible other causes.
Age of Onset The first symptoms of CMT commonly occur during childhood and early adult- hood. Early features in young children are problems with walking, toe-walking and foot deformities. Statistically, the other most common ages of diagnosis are in the thirties and fifties.
CMT Inheritance The most common inheritance pattern for CMT is the dominant pattern. This means if one parent has the disorder that each of hisher children have a 50% chance of inheriting CMT. This variety of CMT affects males and females. There is an X-linked CMT and the in- heritance is like that of hemophilia. Fe- males carry the gene on the X chromosome but are usually not af- fected. However, if the male child inher- its the affected X chromosome, he will have CMT. There is a much m r inheri- tance pattem called recessive inheritance where both parents must have a CMT recessive gene. Usually these parents are unaffected, but the child who inherits a recessive gene from each of his parents can be quite severely afflicted. In gen- eral, the recessive forms of CMT are more severe than the dominant forms. (CMT inheritance and genetics are dis- cussed in detail later in this publication.)
CMT has sometimes been called the "mystery disease" because of the great variability of symptoms from patient to patient and even within the same family. Within a family there can be members with very slight symptoms and other family members who require surgery, bracing, aidsand even wheelchairs. Ge- netic counselors can assist you in under- standing the inheritance of this disorder. There are diagnostic and prenatal tests available for Type IA CMT.
(continued on next page)
CMT Facts, page 2

Genetics of Charcot-Marie-Tooth by Dr. Judith Willner and Ms. Felice Yahr
This article is taken from a letter to the mother of a newly diagnosed CMTchild. At the time of the child's diagnosis u p propriate testing was done on family members. The child's mother, grand- mother, great-grandmother and two ma- ternal aunts were also diagnosed as CMTpatients. Dr. Willner is apediatri- cian in the Division ofMedical Genetics at Mt. Sinai Medical Center, New York Cify and Mrs. Yahr, now retired, was a genetic counselor at Mt. Sinai Medical Center.
Charcot-Marie-Tooth disorder is a dis- ease that affects the peripheral newes. There are two forms of CMT which may appear quite similar clinically, since both may cause weakness of the leg and foot
a d foot deformities. In one form there is a loss of a substance called myelin Mye- lin, which forms the sheaths surrounding the newes, is necessary for normal newe conduction. This rate of conduction is measured by an electromyogram (EMG). Thus with myelin loss, conduc- tion velocity is slower. This lowered ve- locity, as revealed by an EMG, differentiates this form of CMT from the second form. This form is called Type I or hypertrophic CMT.
In the second form, while some newes may be lost, there is no delay in the speed with which nerve impulses are con- ducted along the existing nerves. This form of CMT is called Type II or neuro- nal .
Both you and your mother show reduced conduction velocity. This permits diag- nosis of the demyelinating form of CMT (Type I), and also tells us that in your family Ch4T is inherited in a dominant fashion That is, inheritance of only one gene from one parent can cause the dis- order to appear.
There is a recessively inherited form of the disease; in this case, an individual would have to inherit two genes, one from each parent, to have the disease. There is also an X-linked form of CMT where the CMT gene is located on the X chromosome. In that form the female carries the gene but does not have CMT.
(continued on page 4)
CMT Facts (cont 'dj-ompg. 2)
Diagnosis Diagnosis is made by clinical evaluation (with appropriate testing), exclusion of metabolic problems, and evaluation of several family members, especially par- ents. Informative diagnostic procedures include electromyography (EMG) and nerve conduction velocities (NVC). Nerve conduction velocities measure the rate at which nerve impulses are trans- mitted across the newe. Sometimes, a p parently unaffected family members are included in these NVC studies and will show lowered conduction rates. This procedure is non-invasive and is likened to a strong tingling sensation with j ump ing of the muscles. The EMG is per- formed by the physician with a very small needle electrode which is inserted into various muscles and helps deter- mine the degree of muscle damage or deterioration. This procedure also helps the physician confirm that the patient's
symptoms are in fact due to CMT rather than another neuromuscular disorder. This procedure is semi-invasive with a small needle being used. Appropriate blood and urine testing is done as well as any necessary x-rays. For Type 1A Ch4T a diagnostic blood test is available. Some CMT children do have cuwature of the spine (scoliosis). Occasionally, more complex testingsuchas newe biopsy and spinal tap will be done, but not usually.
Treatment Treatment is available, however the pos- sibility of a cure awaits the discovery of the underlying cause(s) of CMT disor- ders. The discoverey for the CMT gene for Type IA CMT (about 70% of CMT cases) means that now the researcher can begin to unravel the mystery of this dis- order. Once the abnormal or missing bio- chemical substances are known and understood, then cures and therapies be- come possible. For now the CMT patient
has available to h i n h r physical ther- apy, occupational therapy, orthopedic surgery, appropriate bracing and splint- ing, supportive footwear, and the counsel of the physician familiar with CMT. Cer- tainly, this last is of vital importance as the Ch4T patient can develop symptoms unique to this disorder, but unrecognized by the uninformed physician. The CMT patient should be an aggressive con- sumer of modem medicine and work in partnership with hidher physician and therapists.
0
CMT Facts, page 3

Genetics (cont m o m page 3) (However, some carriers may have very mild or sub-clinical signs of CMT.) [Note: Sex of the individual is deter- mined by the X & Y chromosomes. Fe- males have two X chromosomes; males have one X and one Y chromo- some.] That female carrier has a 50% chance of passing the CMT gene to a son and he will have the disorder. This fe- male carrier also has a 50% chance of passing the CMT gene to a daughter and that daughter would be a carrier also. This CMT genetic pattern is similar to the inheritance of hemophilia.
By way of review, genes are the units of heredity. They are so small that they are invisible by any modem means of exarni- nation. Hundreds of genes together, al- ways in a specific sequence, make up the structures known as chromosomes, which are present in every cell. With the exception of sperm and egg cells, all normal body cells have 23 pairs of chro- mosomes or a total of 46. When an egg and sperm come together at conception, they form a new individual who will have 46 chromosomes in all cells.
Every individual has many thousands of genes, each of which directs the cell to make a specific enzyme or other protein. Genes themselves are made of a sub- stance which is capable of changing or mutating. Thus, among the vast number of genes present in all of us, a few in each individual are likely to have changed, with the result that they are unable to direct the production of (or code for) a normal protein Each person is esti- mated to have h e to eight such abnor- mal genes. The one which causes CMT probably should contain information for making a protein which is necessary for proper newe function
When a single abnormal or mutant gene in an individual causes the clinical pic- ture of the disease as in your family, the disorder is said to be dominantly inher- ited. One parent carries a mutant gene for a dominant disorder and each child that individual has will have a 50% chance of inheriting the gene and therefore the dis- order. It is true that sometimes a child will be born with such a disease when neither parent carries the mutant gene. In such a case the first mutation of that gene occurred spontaneously in the egg or sperm that form that individual. In such a situation the parents are not at increased risk to have another similarly
affected child, but the affected child will parent has (paired with the abnormal re- have a 50% chance to pass the mutant cessive gene) protects them from having gene on to each of h i s h r children. We the disorder. This is the case with the do not believe this the case in your fam- pure recessive form of Ch4T inheritance. ily, since we have found evidence of the The inheritance of X-linked CMT we gene in you and your mother. discussed earlier.
Dominant disorders can vary widely in Although a biochemeical defect (that is, terms of the severity of the symptoms. a lowered level of a particular enzyme or This is called expressivity. In some indi- other protein) almost certainly exists in viduals therecan be severe clinical prob- carriers of the recessive gene, no test has lems while other affected members of the yet been devised to identify the carrier
state. Recessively inherited CMT is gen- erallv a more severe disorder than the
"In some families carrying this (CMT)
gene, the only visible sign of the disorder may be a high arch."
family may have hardly noticeable or even unnoticeable symptoms. For exam- ple, in dominantly inherited deafness there may be a severely deaf child with a parent who has a very small hearing loss detectable only on a sophisticated audiogram. The parent may be unaware of this small loss. Therefore, in some of these dominantly inherited disorders while the gene is inherited, the severity of the symptoms may vary widely.
CMT is one of these. While the gene seems highly penetrant (that is an iradi- vidual who carries it is likely to show some recognizable symptoms), the level of expressivity (degree of severity) is often low. In some families canying this gene, the only visible sign of the disorder may be a high arch In other families the severity varies and probably depends on whether other "modifier" genes were in- herited along with the abnormal gene itself. The degree of severity of the dis- order is therefore impossible to predict.
Since your daughter manifested symp toms earlier than you it is possible that she may not have received the modifiers that you have. When she herself has chil- dren eachchild will have a 50-50 chance of receiving the gene. Again the severity of the symptoms in a child with the gene will depend on the number of modifiers also inherited, some of which could come from the child's father.
For your information, it was mentioned that in the recessive form of CMT the parents of an affected individual appear to be completely normal and are normal by EMG. The normal gene that each
doknant form. It has an earlier age of onset and the symptoms progress much faster.
You were also told that while CMT is a progressive disease it usually progresses very slowly. Sometimes the condition appears so stable that it is misdiagnosed as polio. The very slow rate of progres- sion of the symptoms in your mother is likely to be a familial characteristic of the disorder. Although this cannot be predicted with certainty, the same rate can reasonably be expected in your case as well as your daughter's. Your EMG showed that the rate of conduction of the sensory nerves was 35% below the nor- mal mean and that of the motor Ewes was 33% slowed. Latency (the time elapsed from conduction of the impulse to your muscle contraction) was 5 0 4 W below the normal mean Yet your deficit is minimal and is unlikely to be apparent until you are much older. Like your mother, you may begin to experience some slight difficulty in later years.
The 50% chance in each future preg- nancy for a child with CMT was dis- cussed with you. It was also mentioned to you, as a matter of information, that every couple regardless of age or health, has a 2%, or 1 in 50, chance to have a child witha major congenital problem of some kind. Your 50% risk of a CMT child would be in addition to this general figure. We hope all of this is clear.
Editor 's note: Since this article was writ- ten, the CMT gene located on chromo- some 17 has been identi'ed. Thisgene is responsible for Type U CMT which is about 70% of all CMT cares. It is a dominantlydnherite Jform of CMT. As of this printing work continues on locating the CMT genes on the X chromosome, chronrosome 1 and other unknown loca- tions.
n
CMT Facts, page 4

CMT Children: Advice and Information A leading pediatric neurologist discusses the issues.
Dr. Harold B. Marks was inter- viewed at the AIfLed I, dupont Institute by the CMTA. Dr. Marks, who is Direc- tor of Neurology at the Institute, has substmtial experience diagnosing and treating the CMT child. The Aped I. duPont Institute is a multi-specialty hos- pital for infants, children and adoles- cents located in Wilmington, Delaware.
Dr. Marks, let us suppose that there is a CMT parent who has normal parents and siblings, would it be possible for the CMT parent to have a CMT child?
Yes, it ispossible, and there are three d~fferent situations to explain this. Our first considerations would be a parent who inherited hisher disease as an autosomal recessive disorder. In this case the parent would not pass the disor- der to hisher children unless he marries a CMTpatient or CMT carrier. This is very unlikely except when he/she marries a relative. The secondpossibility is that the CMTparent has uutosomal dominant W and he/she represents a first gen- eration mutation. Hidher children would have a one in two chance of hav- ing CMT. The third possibility is that CMT has been present in the family, but totally undiagnosed. Aubsomal domi- nant disorders like CMT have very vary ing degrees of severity even within the same family. Again, the odds are one in two a child would be CMT. Another con- sideration would be sex-linked inherited CMT. g the CMT parent is male and inherited his disease as sex-linked, his children would be disease j e e , but his daughters would be carriers. Those daughters would have a one in four chance of having a male child with CMT.
What are the early warning signs of CMT in children?
From the results o f a study we did here the overwhelming majority ofpa- tients (93.8%) had a foot deformity. The most common of these deformities was pes caws (high arches, 84.6%)followed by claw-toes (39.5%) and varus foot (turned-in foot, 25.4%).
What is the most commonage for parents to seek help for a child and a diagnosis to be made?
Again from the study we did here, the median age of onset of CMT was 5.3 years +/-4.2 years with a range of age from 0 to 12.4 years of age. Almost all patients (80.9%) had symptoms of CMT before age 10. It was interesting to note that 60.5% of the patients were males compared to 39.5%females.
Would a one year old CMT baby walk normally?
Mostly they will, but as the disease progresses they develop high arches and foot deformities. Occmionally, babies with CMT are persistent toe walkers. However, there are other causes of toe walking. If there is a family history of CMTI would do nerve conduction stud- ies and EMG 's.
Can nerve conduction studies be done on a full age range of patients?
Yes, but I usually wait until a child is 2 years of age and'then do an EMG.
By EMG, you mean you are testing the electrical function of muscle tissue?
Yes, as opposed to nerve conduction studies, which test the peripheral nerve fibers.
When you do an EMG on a CMT patient what do you learn? How do they differ from a normal person?
With CMT, EMG's demonstrate changes in muscle electrical activity which is due to decreasednervefirnction. These changes are both acute and chronic.
With a child do you usually do both an EMG and a nerve conduction study?
Yes.
How do you get the cooperation of a young child?
It is a matter of experience. I do not do EMG 's but rather use very experi- enced physicians who do them fie- quently. We have three physicians here who do EMG 's.
Do you sedate a child? No, it is not necessary. We try to get
the child's cooperation. It is not ideal to do an EMG at a very young age. Since CMT is not a treatable disease, in the
child with afamily history of W when diagnosis is not wantedfor genetic coun- seling, we wait until the child is older. Also, ifthe child shows an unusualfear ofneedles we will wait until the childcan understand the reasonsfor testing.
When you do EMG's and nerve conduc- tion studies on a child, are there needle electrodes involved?
In an EMG there are needle elec- trodes; for the nerve conduction test there are surface electrodes.
It sounds as if it is important to relate to the child.
Yes, it is very important, and I stress to the parents that there is minimal or no risk to the child. Once the test is finished there are no after effects.
How long does the test take? Usually 30 minutes.
Lf a child had been diagnosed as having CMT, is there any way of predicting the severity of the disease?
It is my impression that children with the demyelihating form of CMT (HSMN I) are overall a little more severely in- volved than the aronal form (HSMN II). Others have reported in adults a corre- lation between age ofonset of .rymptoms and severity of disease. In children this does not seem to consistently correlate. Finally, others have reported the spo- radic or autosomal recessive forms of CMT to be more severe than the autoso- ma1 dominant.
Does the clinical history of the parent affect the degree of disability of the child?
No, there doesn 4 seem to be a way to predict that, As I said before, autosomal dominant disorders have varying de- grees ofseverity even within the same family.
At what point do you think that a CMT child is a candidate for orthopedic refer- ral?
We see patients here in a clinic set- ting. The clinic is attended by an ortho- pedist and me. Dr. Richard Bowen, the orthopedist, also continually monitors
(continued on next page)
CMT Facts, page 5

CMT Kids (contldfi.ompg. 5)
the child Initially, we tend to put the children in AFO's (leg braces). As the disease progresses, they may go on to surgery, but this decision is made by Dr. Bowen and the parents.
I know Dr. Bowen prefers to wait until age 12-13 to operate. Is the decisionever made to operate earlier?
Yes. There are two indications for surgery. They are ankle instability re- sulting in repetitive ligaments injury which is not helped by non surgical means such as AFO 's and progressive pes caws deformity (high arches) which limits walking ability or causespain.
What percentage of Ch4T children here are referred for surgery?
I would estimate less than 10%
What determines ifa child needs AFO's? Ifthe child is twisting hidher ankles
frequently, or ifhelshe has a lot ofpain in the ankles and arches and it alfects hisher walking, we then recommend AFO 's. If all hehhe has is ankle weak- ness or high arches alone, I don 't recom- mend theA FO. I try to wait until the child will clearly benefitfrom the AFO before Iprescribe it. As you know, the A FO may cause disuse weakness. In addition, i f children don't clearly benefit from AFO 's they will refuse to wear them.
Do children outgrow braces? They usually last 1-2 years.
Do the children here come through the MDA clinic? (Editor's note: MDA is the Muscular Dystrophy Association, an or- ganization that is independent of the Ch4TA.)
About one-tenth ofthem do and the others are privately referred. Almost aN our CMT referrals are from orthopedic surgeons.
If a child needs leg braces does the MDA cover the cost?
Yes, MDA helps provide for their purchase and reasonable repair. Once a W c h i l d comes here I enroll the child with the MDA. Helshe then has the choice of being followed at our MDA sponsored clinic, and i f the child needs orthopedic aids such as braces, a wheel- chair, crutches, etc. JULIA will helppro- vide for their purchase.
( CLINICAL FINDINGS OF CHILDREN WITH CMT
Family HIatory
I Oecreaaed Ref k m a
What about exercise and the CMT child? I encourage them to be as active as
possible, but I discourage them Porn participating in contact sports. How- ever, I do not prohibit them Porn doing so. II have one patient who loves to play football andhe has continued toplay. As for exercises, I initially send new pa- tients with moderate to severe weakness to see a physical therapist for strength- ening exercises. If I see a signijicant hand weakness, I send them to an occu- pational therapist. The therapists give them exercises to do at home, and the patient is re-evaluatedperiodically, usu- ally every 3-6 months.
Do you see CMT children a$ having a balance problem that limits them in sports?
No, I haven 't had a patient complain of this. In fact, I know of two CMT pa- tients who are skiers. I know ofno study showing therapy helps, but lfeel keeping the muscles stretched so they do not de- velop contractures and maintaining and improving muscle strength must benejt children.
Is there anything you tell the childm not to do?
No, not really except for the contact sports warning. I try to have the children live as normally as possible.
I know you have seen a child who is mentally retarded and has CMT.
Yes, but Ifeel she has two common diseases, having cerebral palsy and mental retardation as well as CMT. I have tested her for several other disor- ders that involve both the central nerv- ous system and the peripheral nerves, but they have all been negative. Her brother, also a CMTpatient, has normal intelligence.
In other words, you feel there is no cor- relation between Ch4T and mental retar- dation
No, in fact most children I see with CMT are very bright. These children tend to focus their potential in academic areas rather than motor areas.
Have you referred any children to special education programs'?
No, most CMT children don't have this need.
Should parents confer with the child's primary teacher and explain the disabil- ity?
In a few CMT children with hand weakness it is very d?fficultfor them to copy schoolwork or take notes. For these children I have asked the teachers that they be allowed to tape lectures and other class work. Additionally, I encour- age these children to learn to use a work processor (if they have a computer at home) in order to M e their assignments. In gym it is different. Activities such as running and rope climbing would be dif- ficult and should be explained to the
CMT Facts, page 6

Physical Therapy and Rehabilitation of the CMT Patient Conservative Management of the Functional Manifestations of Charcot-Marie-Tooth Disease
We are extremely pleased to be able to reprint a condensed version ofthis chap ter pom the recently published book, Charcot-Marie-Tooth Disorders: Pathophysiology, Molecular Genetics, and Therapy, 01990 Alan R. Liss, Inc. reprinted bypermission ofJohn Wiley & Sons, Inc. We are able to do this because ofthe cooperation ofthe publisher and the author Dr. Carol Oatis. An expert on gaitproblems, she teaches physical ther- apy at Beaver College, Glenside, PA. Dr. Oatis has spoken at several GMTA pa- tient andprofessional conferences. Some ofthe materialpresented is ofa technical nature, but we believe everyone will benefit from reading this article.
Charcot -Marie-Tooth (CMT) disease lperoneal muscular atro~hv) is a deeen- (continued on next page)
erative disorder of the peripheral nervous system leading to a progressive weaken- ing of the peripheral muscles of the upper and lower extremities. The disease gen- erally involves the most distal muscles first and then progresses in a proximal direction. It is a progressive disease but is generally considered not fatal and there is no known cure (Gilroy and Meyer, 1979). Unfortunately, however, patients are often told that there also is no treatment. Yet, treatment to alter the physiological course of the disease should not be confused with treatment directed toward relieving the functional deterioration which accompanies the progressive weakness. The purpose of this article is to present the conservative treatments which can be utilized to mini-
mize the manifestations of CMT and to optimize the function in patients with CMT. Of course, surgery is also a poten- tial option which is addressed in a sepa- rate article.
The goals of conservative management are to: 1. maintain function 2. insure safety 3. maintain comfort 4. protect the weakened joints 5. conserve energy.
These goals can be met by maximizing muscle strength and endurance, mini- mizing deformities, and by the use of orthotic devices (braces) to compensate for weaknesses or deformities, and adap
CMT Kids teacher. However, no parent has ever asked me aboutgym class. Gym teachers should not have unreasonable expecta- tionsfor the CMT child.
Are pediatricians as a group trained to recognize the CMT child?
No, there is a needfor education in this area. CMT is a relatively common problem. In the ten years I have been here I have seen 200 - 300 cases.
Are you aware of CMT children having chronic pain?
Yes, but it is not common. Some chil- dren complain ofintermittent back pain, calf pain, thigh pain, and pain of the arches. This is more severe at night. I wouldguess 5-1 0% ofthe children have pain. With these children Isend them to a physical therapist for stretching exer- cises.
Do you give drugs to children for chronic pain?
'No, but most children do not have severe pain. YIhad apatient with severe pain, then I would consider medication.
What is your philosophy about labeling the CMT child as disabled?
Although I recognize that children with CMT have limitations, I fie1 that they should lead as normal a life as pos- sible. Their areas ofstrength should be identified and i f physically able they
should be encouraged to participate in activities that interest them. As I said before, I know peisons with CMT who ski, run in marathons, and play high school football. Furthermore, I know CMT adults who are physicians, scien- tists, attorneys, and truck drivers.
If the child is wearing leg braces, can helshe participate in sports?
Yes, they can. To summarize, I en- courage the child to be as normal as possible, I want the child to look upon himself as normal, not crippled. CMT patients go into all professions. At- though, I do warn the children about choosing heavy labor occupations. As the disease progresses, some things would become drflcult to do as the mus- cles weaken. For instance, a CMT pa- tient should not become a bricklayer.
Then you would not encourage a musical CMT child to become a professional mu- sician.
No, I would not ifthe child is inter- ested in playing an instrument that re- quires great manual dexterity and was interested in a performance career. However, for the rrrusicallyg~j?ed child I would certainly encourage their talents to be expressed in composing, teaching, conducting, or wherever hidher inter- ests lie. Furthermore, I would alwqvs encourage them in their nrusic for an avocation. What 1 do not want isfor the
CMTchild to have to re-train in mid-life because of their disease. I also warn CMTpatients about working with neuro- toxic chemicals. In- there is an ab- normality ofthe nerve and the nerve is very limited in its abilily to withstand chemical as well as physical trauma.
You are referring to industrial solvents? Yes, the patient should ask hidher
place of employment about toxins and consult with hidher doctor about them. Physical trauma is another factor. Some people have to wear heaypacks or belts which would subject them to physical trauma. Prolonged standing would also be very diflcult.
As a final question, what about scoliosis in children?
Yes, scoliosis ispresent in about 40% of the CMT patients seen here at A.I. duPontInstitute. About 15% oDur CMT patients have come to us because of scoliosis and subsequently the CMT di- agnosis was made. From our study 43.2% ofthe CMTchildren had scoliosis while an equal portion did not, leaving 13.6%for whom the information was not available. This would suggest that the true percentage for scoliosis is closer to 50%. The scoliosis was not usually se- vere and did not generally require sur- gery. However, 10- 15% of CMT scoliosis patients may require surgery.
CMT Facts, page 7

Rehabilitation ( c o n ~ l d ~ o m p g 7, strengthening and conditioning exer- Exercises are projpssed by increasing cises. the resistance used in the exercise or by
tive equipment to make activities of daily living easier. How each of these treat- ments is carried out is discussed in detail in the following sections.
Maximizing Muscle Strength CMT is a degenerative disease and there are no means presently available to pre- dict the course of the disease. Some pa- tients may progress to diffuse and profound weakness while others may re- main minimally involved. Therefore strengthening exercises will have vary- ing degrees of success. In some patients the exercises may serve only to retard the
--
"...even neurologically involved muscles can
be strengthened."
rate of weakening while other patients may see a real, measurable increase in strength. Yet both effects will be valu- able in enabling the patient to remain functional.
If a muscle is able to contract it is theo- retically capable of increasing its strength of contraction (Brooks and Fa- hey, 1985). Thus, ifa patient can activate any of the motor units of an involved muscle, that patient has the potential for increased strength Research studies s u p port the concept that even neurologically involved muscles can be strengthened. Therefore, people with CMT may be able to improve function or at least mini- mize the loss of function through appro- priate strengthening exercises.
Even the muscles not involved by the disease should be exercised. Because of the nature of the disease many patients with CMT discontinue vigomus physical activity and become more and more sed- entary. This lifestyle results in pmgres- sive weakness in n o d muscles and generalized deconditioning. However, compensation for the weakness associ- ated with CMT requires additional physical exertion. Strengthening the nor- mal muscles in the feet will help the patient tolemte the increased stresses a p plied in quiet standing and in gait due to weaknesses in other muscles. Function will be improved dramatically by estab- lishing a generalized program of
Some authors have suggested that neurologically impaired muscles may be injured by resistance exercises (Johnson a d Braddon, 197 1). However, the stud- ies referred to above denied any sign of damage to the exercised muscles (McCartney, et al, 1988 and DeLateur ad Giaconi, 1979). Excessive resistance ad excessive fatigue have been shown to result in injuries to normal muscles. So similar results are possible but are not inevitable in nemlogically weakened muscles. Admittedly, the loads and repe- titions sufficient to cause injury are likely to be decreased in the abnormal muscles. Thus while there may be no unique deleterious effect of strengthen- ing exercises in patients with CMT, re- sistance exercise must be carried out cautiously to avoid the damaging effects of overtraining, because injury to an al- ready weakened muscle can f;rther com- promise its performance. A progmm for strengthening must be directed toward improving the function of the weakened muscles and maximizing the strength in the uninvolved muscles. Even small in- creases in strength of the impaired mus- cles can result in a significant improvement in function Patients have reported an increased tolerance for hand- writing after only one month of hand exercises. One patient reported that he was unable to write a single-page letter without resting his hand to relieve cramping. One month following the in- auguration of an exercise program, he stated that he was able to complete two or three pages without discomfort. An- other patient reported that prior to begin- ning exercise, she had difficulty walking her dog because of ankle and knee insta- bility. A program of stretching and strengthening exercises for the lower ex- tremities allowed her to increase her tol- erance to ambulation. In fact, she resumed walking a round of nine holes of golf. Neitherof these patients returned to normal strength However, their func- tion was markedly improved in a rela- tively short period of time.
An appropriate exercise program must also be based on an understanding of the patient's individual level of function. Thus each patient should undergo a com- plete evaluation by a physical therapist to establish a level of exe~ise for each muscle group which will result in strengthening without injury.
increasing the number of repetitions. Re- sistance for foot and ankle exercises can be progressed from lifting only the weight of the Limb to lifting the limb and a weight attached to it. Another conven- ient method for increasing exercises is the use of rubber strips meraband: Fit- ness Wholesale, Inc., 800-537-5512], which the patient can use to tie the limbs together, making it harder to pull apart. Resistance for the intrinsic muscles of the hand can be applied by exercise putty [Exercise Putty: Smith and Nephew RO- lyan, Inc,, 800-72244421. It must be noted that strengthening exercises must be carried out with careful precision It is quite easy to substitute a strong muscle forthe weakened one and thus not obtain the desired effect. Careful guidance by the physical therapist is essential for o p timal results.
Resistance should increase the diffculty of the exercise without causing pain or making it impossible to complete the exercise correctly. Repetitions shouldbe increased in small increments to avoid excessive fatigue. For example, a patient may be able to do an exercise and repeat it four times. Perhaps that patient can increase the repetitions to two sets of five in the next week or so taking care to avoid excessive fatigue. Fatigue is ex- cessive if it results in pain or leaves the patient too tired to resume normal activ- ity. Repetitions can be increased gradu- ally from ten to a maximum of three sets of ten. When the patient is ready to in- crease resistance the number of repeti- tions should be decreased then gradually increased again to avoid injury to the muscle.
Electrical stimulation has been em- ployed by some clinicians for muscle strengthening. Muscles and nerves can be stimulated by external electricity to elicit a muscle contraction This hasbeen shown to result in strengthening when the electricity is strong enough to elicit a visible contraction. This technique was not shown to be more beneficial than voluntary exercise in normal subjects (Currier an Mann, 1983). Further study is required before the usefulness of elec- trical stimulation in patients with CMT can be determined. However, dener- vated muscles require more electricity to produce a stimulated contraction. Pa- tients with intact sensation may not tol- erate the discomfort associated with this
CMT Facts, page 8

increased intensity. Thus for most pa- tients a program of voluntary exercise remains the most reasonable approach to ixreasing strength.
In most cases, the patient can cany out this strengthening program at home, re- quiring only occasional visits to the physical therapist to modify the program based on any functional changes secon- dary to the disease. Periodic reevalu- ations will also allow close monitoring of the progression of the disease.
Maximizing Endurance Mention should also be made of the gen- eralited conditioning program empha- sizing aerobic conditioning. Aerobic exercises are designed to increase the heart rate and sustain that increased rate for approximately thirty minutes. The "target heart rate" for aerobic exercise is usually a rate (220 minus age). Simple activities like walking have been shown to require more energy to accomplish when the subject has a weakness or lim- ited movement (Winter, 1978). There- fore, walking a city block is generally more fatiguing for a patient with Ch4T than for a normal subject. However, the sedentary lifestyle of most Ch4T patients also contributes to ~ i g ~ c a n t decondi- tioning. So not only is the patient gener- ally required to spend more energy to accomplish a task, he is often less capa- ble of expending that energy. Thus the Ch4T patient will benefit from improved conditioning. However, such condition- ing exercises must accommodate the pa- tient's weakness. For example, walking may be too stressful, so swimming or the use of a stationary bicycle may be more suitable. The benefits of such exercise include those accrued by normal sub- jects, such as decreased risk of heart dis- ease, decreased body fat, lowered resting blood pressure and increased sense of well4eing. However, the most obvious benefit to a patient with Ch4T is in- creased muscular and cardiovascular en- durance, enabling that person to take a more active role in everyday life. It should be noted that because aerobic ex- ercise involves elevation of the normal heart rate, there are some risks involved. Therefore, no patient should undertake such a program without appropriate medical supervision.
Minimizing Deformities The characteristic deformities seen in patients with CMT result from an imbal- ance between the weakened muscles and
the unopposed pull of their antagonists. For example, the dorsiflexor muscles of the feet are often weakened before the plantarflexor muscles which oppose them. As the dorsiflexors become weak, the plantarflexors pull and become tight. The resulting "plantarflexion contrac- ture" makes it for the patient to stand with his/her feet flat on the floor. The patient usually reports that he feels as though he will fall backwards or that hdshe is only comfortable in shoes with hgher heels.
The disadvantage of such deformities are many. First, the deformity often results in abnormal pressure on the foot, and consequently, in pain The resulting ab-
"Careful guidance by the physical therapist
is essential for optimal results."
normal weight bearing may also put an excessive strain on theotherjoints. In the case of a plantarflexion contracture, the '
deformity often results in a backward pull on the lower leg and a hyperexten- sion pull at the knee.
Appropriate stretching exercises are use- ful in minimizing, if not completely avoiding, such deformities. However, as in strengthening exercises, specificity in the stretches is essential. First, the mus- cle imbalance must be identified since stretching the weaker muscle may in- crease the imbalance. The stretch also must be performed carefully to insure that the stretch is applied to the intended muscle. So again stretching should be taught by aphysical therapist who knows how to isolate individual muscles for stretching and for strengthening.
Orthotic Devices When muscle weakness progresses to such an extent that the patient is unable to walk normally or is frequently falling, it is time to consider orthotic devices to support the weakened limb. The most common device of this sort is the ankle- foot orthosis (AFO) to support the weak- ened ankle. When the dorsiflexor muscles are weak, the patient has culty lifting the foot away from the floor when stepping forward during walking. The patient has a tendency to trip over the dangling foot. To prevent stubbing
the toes and a potential fall, the patient will bend his hip and knee excessively as he swings his leg forward. This exces- sive movement causes increased energy expenditure. An AFO supports the foot and thus decreases the chance of tripping and the increased energy expenditure. The most common such device is a light weight plastic brace molded to the foot and worn inside the shoe. This device can also support the foot in the presence of weak plantarflexors. The disadvantage of the molded AFO is that it is hard and occasionally causes discomfort particu- larly in the sensitive foot.
Metal upright braces also provide sup port for a weakened foot. However, these braces are considerably heavier and should be used only when the patient cannot tolerate the molded AFOs. There are other variations of orthoses to sup port the weakened foot. The appropriate device should be determined by the pa- tient, the physical therapist, the physi- cian, and the orthotist, based on the patient's individual needs.
Orthoses are also useful in accommodat- ing foot deformities. In particular, foot orthoses are devices which fit in the shoe and cover the sole of the foot without crossing the ankle. Thus, they may in- crease foot comfort, but they do not pro- vide ankle stability. These devices are usually prescribed and made by podia- trists or physical therapists. It should be noted that some of the modifications of the foot orthoses can be incorporated, to a certain extent, in the ankle-foot or- thoses to provide stability and inc~ease comfort.
Adaptive Equipment Adaptive equipment is equipment spe- cially altered to improve its utility for patients with musculoskeletal patholo- gies. For example, enlarged grips can be used on table flatware to improve the patient's hold on the device. Enlarged handles can also be used to improve the grip on pens and pencils. Special devices are available to make tasks in the kitchen easier. Others provide ease of dressing. There are countless devices on the mar- ket today designed to make activities of daily living easier. Much of this equip ment is available through catalogues.
(Continued on next page)
CMT Facts, puge 9

CMT Foot- Surgical Options An Overview
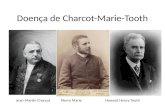
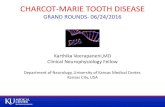
Problems with the feet are often the ear- liest symptoms of Charcot-Marie-Tooth disorder. Beginning as curled toes and high arches, CMT foot problems usually progress. There are three foot deform- ities typical of CMT, all of which may be present to some degree. These include the cavus foot, the varus heel and claw toes. They usually begin as flexible de- formities and progress to fixed deform- ities. These foot deformities are caused by growth of bone during a state of mus- cle imbalance. The progression of the deformities can be seen in Figures 1 - 3.
The cams foot, also called pes cavus or high arches, results from a muscle imbal- ance between the extrinsic and intrinsic muscles of the foot. The plantar fascia (soft tissue on the sole of the foot) and the plantar ligaments (tissue connecting the bones of the feet) tighten, somewhat like a rubberband, pulling the ends of the foot closer together. This results in the high m h .
Heel varus, also referred to as hindfoot varus, is a condition in which the heel
Fig. 1 The normal foot
turns in. When viewed from behind it appears that the person is walking on the outside edge of the foot. Heel varus cre- ates instability and balance problems.
Claw toes, or hammer toes, is acondition where the toes cock up. Initially claw toes are seen during walking due to mus- cle imbalance. Later, this condition be- comes rigid and the toes stay cocked. Claw toes cause initation to the top of the toes as they rub against the shoe. This condition also makes it dficult to find shoes that fit properly.
In addition to these three deformities,
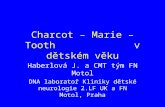
bottoms of the feet and the feet become somewhat rigid. Ankles may become weak and unstable and the "forefoot equinus" (footdmp) may set i n Foot drop results from the wasting of the peroneal muscles ( located on the outside of the leg below the knee) and is the cause of high steppage gait.
Surgery's aim is to enable the CMT pa- tient to walk with the entire lower sur- face of the foot on the ground (plantigrade), to decrease pain, to im-
U $#c!$Q d
Fig. 2 Intermediate CMT Foot- Note cocked toes, high arch, tight- ened plantar fascia
painful callouses often develop on the
Rehabilitation (contilfi.om pg. 9)
In particularly involved cases or for spe- cific needs, occupational therapists can evaluate patients and make recommen- dations for adaptive equipment. Such de- vices can make a marked difference in the quality of life for patients with CMT. Patients with CMT should seek a con- sultation with an occupational therapist to see if any adaptive equipment would be helpful.
Adaptive eating utensils
Editor's note: Seep. l3for addresses & phone numbers for gadget catalogues.
Sunznmry While there is no known treatment to alter the physiological degeneration characteristic of Charcot Marie Tooth disease, there is treatment available to minimize the manifestations of the dis- ease. Physical and occupational therapy provide programs utilizing exercises and orthotic and adaptive equipmeht to maxi- mize strength and endurance, minimize deformities and to improve function. These approaches can help the patient with CMT to consewe energy, function safely, and minimize the discomfort as- sociated with contractures. By doing so,
the patient can significantly improve the quality of life and remain hopeful with the realization that he is taking an active part in the treatment of his disease.
- Carol A. Oatis, P. T., Ph.D.
Bibliography available upon request.
Jointhefight 1 against CMT !
See the back cover for
complete details.
CMT Facts, page 10

prove balance and agility, and to halt progression of the deformity.
The Assessment The progressive nature of CMT makes early assessment and long-term treat- ment planning prudent. A carefid evalu- ation of the foot is the first step. Distinguishing between fixed and flex- ible components of each deformity is essential to the proper management of CMT and formulation of an individual- ized treatment plan
Options I f the assessment concludes that surgexy is indicated, things become more com- plicated. Several types of surgexy may be performed on the Ch4T foot depending on the level of involvement. Tendon transfers, lengthenings and sometimes tenotomy (surgical division of a tendon) may be used to eliminate deforming forces (to slow or stop progression of the deformity) and to balance the foot. Osteotomies (surgical division or sec- tioning of bones) and arthrodesis (fusing joints) are often necessary to correct alignment and to alleviate symptoms, es- pecially in the case of rigid or fured de- formities.
The three foot deformities and respective surgical options will be discussed sepa- rately, but the foot is treated as a whole and surgeries, if necessary, are often done at the same time. Specific surgical procedures will not be discussed in detail in this article.
Cavus Foot Where there is no bony deformity, the goal is to release the tightened tissues ad ligaments to relax the bottom of the foot and the cock up tendencies of the toes. Surgical procedures include plantar fasciotomy/fasciotomies, also called plantar release.
When bony deformities are present, some formof osteotomy (removal or cut- ting of bone) may be performed. Essen- tially these remove a section or wedge of bone, then "close" the foot to reposition the foot to plantigrade (walking with the entire bottom of the foot on the floor.) Surgical procedures may include "clos- ing wedge greenstick dorsal proximal metatarsal osteotomies", "closed wedge dorsal osteotomy", "the Japas-V-tarsal osteotomy", the "Cole osteotomy" and the "tarsometatarsal truncated wedge osteotomy". A variety of muscle trans-
fers in various combinations (such as moving the long peroneal muscle to the short; or moving the posterior tibialis to the dorsum of the foot) may also be done to eliminate the deforming force and im- prove the position of the foot.
Varus Heel If the heel is flexible, cormtion of the cavus component should correct the flex- ible varus heel.
Fig. 3 Advanced CMT Foot- Foot drop, rigid deformities
If the varus heel is rigid, an osteotomy may be performed on the heel bones. A wedge of bone is removed from the heel bone to correct it to the straight position. Technically (ad with more details) this is a Dwyer osteotomy, closing lateral wedge osteotomy of the calcaneus, or hindfoot osteotomy . Claw Toes I f the claw toes are still flexible and have not become rigid, cavus correction should fu the claw toes.
Surgical procedures to fix rigid claw toes include transferring the tendons con- nected to the toes to the bones of the foot, fusing interphalangeal joints (the ones in the middle of the toes) and fusing bones. Procedures include the Jones procedm, modified Jones transfer and the Gird- lestone-Taylor Transfer.
Triple Arthrodesis Triple Arthrodesis is a procedure which stabilizes the hind foot by fusing three joints. There are several types of triple arthmdeses; the conditionof the foot dic- tates which might be appropriate. The basic triple arthrodesis involves fusing three joints in the hind foot (the ta- lonavicular joint, the subtalar joint ad the calcanocuboid joint). This eliminates side-to-side movement of the foot, but the ankle joint is still free so you retain up and down movement of the foot. In the Pantaylor Triple Arthrodesis, the an- kle joint is also fused. The Lambrinudi Triple Arthrodesis "tricks" the ankle into
thinking that the foot is completely flexed, or pointing down when it has been surgically moved to a position par- allel with the ground/floor. The ankle can still move the foot up but not down.
A triple arthrodesis is not done before the foot stops growing- usually age 12 in girls and age 14 in boys. The goal is to prevent progression of the deformity. There is some controversy over whether or not triple arthrodesis offers better long-term stability than combined mid- foot and hind-foot osteotornies.
Summary The progression of the development of the cavus foot needs to be closely moni- tored. By identming progressive pes caws in the early stages before rigid deformities have occurred, muscle-bal- ancingprocedures may suffice. Once de- formities have become rigid, surgery becomes even more complex. Most sur- geries will require casts for at least six weeks, followed by several months of frequent elevation of the leg ad foot to control swelling.
CMT is a progressive disorder. Follow- ing foot surgery it is recommended that the patient receive intensive physical therapy under the guidance of a therapist well versed in the Ch4T foot. This is especially imperative following muscle balancing operations, tissue release, ten- don transfers and muscle lenghthening operations.
Corditions are dynamic- ever changing. In situations where a second opinion is required, it is not unusual for the opin- ions to conflict. Surgery may not solve all problems, and there is always the potential for deterioration of the foot cor- rection with time. However, when indi- cated, foot surgery can drastically improve the quality of life for the CMT patient.
Jennifer Schoonmaker Hitt
Our thanks to Dr. Bruce Sangeonan for his review of this article.
Bibliography available upon request.
CMT Facts, page 11

The CMT Hand
This article was written @om a dis- cussion between the CMTA and Janies Hunter, M.D.. Dr. Hunter is head of the Hand Clinic in Philadelphia, PA and a hand surgeon of international repute. He is a Professor of Orfhopaedic Surgery at Thomas Jefferson University, Philadel- phia, Pa. During the interview Dr. Hunter discussed hand treatment o p tions for CMTpatients. The CMTpatient is not@equently referred to handpro fes- sionals which i s unfortunate a s Dr. Hunter feels that much can be done to maintain and improve the quality of life of the CMT patient. Dr. Hunter stressed that early assessment and inter- cock-UD mlint vention are vital to preserve and main- tain hand function. The cooperative assessment by a hand therapist and a hand surgeon, who are also experienced in treating peripheral neuropathies, can be the beginning of a program to fore- stall deformities.The problems with the CMT hand usually develop gradually with weakness a primary symptom. This is a result of atrophy of thejine intrinsic muscles of the hand resulting in the "claw" hand a n d m thumb. There is a loss of coordination and tasks become dl@cult.
The Assessment Initially, several procedures are per- 'formed which give the physician and therapist a baseline of the hand's func- tional ability. These include an evalu- ation of the hand's work capacity; a sensibility assessment, which is not re- lated to sensation but rather to how the brain is perceiving sensation; complete muscle assessment determining what muscles are at what level of function; and an identification ofjoint deformities. Dr. Hunter again stressed the importance of early assessment by noting that if the patient is adapting to muscle loss improperly additional harm can be done to other structures not directly involved. Moreover, with early interven- tion the patient is taught to protect and preserve hisher hand function Finally, he noted that much knowledge has been gained within the last twenty years about peripheral neuropathies with many re- sulting new hand therapies.
. s Treatment Inilal treatment might begin with any number of splinting procedures depend- ing upon the individual's muscle loss and the tasks heishe needs or wants to per- form. The splints could be day andlor night splints, even splints for a specific activity. Splints can include dynamic splints which move with the joint or pas- sive splints which are stationary. The patient is studied for a period of time and is then evaluated. If splinting has helped, the patient might be a candidate for inter- nal splinting which is a surgical proce- dure. After surgery the patient no longer needs the external splint which is dis- carded.
Surgical Procedures The tendon transfer results in an internal splint.(Tendons are tissue that connect muscle to bone.) The surgeon transfers tendons from one location in the hand to another in order to maintain a specific function Often, tendons are transferred from a strong muscle to a weak muscle and perform a different job than pre- viously. The tendon transfer can be done on the thumb to restore the pinch be- tween the thumb and another finger. There are other operations that can be done, among them the capsulo desis. This involves fascia and tendon furing across the joint and allows partial joint function to be retained. The procedure is a way of blocking a joint from extreme motions, but allows some motion. This is good for the palsied hand. It can set the stage for tendon transfer, sometimes giv- ing back function the patient has lost.
The surgeon's goal is to return prehen- sion (grasping) with power and stability. Particularly, surgery can restore strength so that the thumb and index or middle finger come together with strength to produce a grip with more power than the "claw" grip. A capsulo desis is done on the middle joint of a finger to allow this. Dr. Hunter pointed out that patients with polio, cerebral palsy, and accidental in- juries are also helped with these proce- dures. Occasionally joints require fusing (arthrodesis) because another joint will benefit. These decisions are only made after careful study of the patient. Briefly to recount, capsulo desis is done to per- mit joint motion, arthrodesis to restrict joint motion, and tendon transfers to con- trol the wrist and thumb and to enhance prehension The recovery period varies with each procedure and is highly indi- vidual. Post surgery therapy is vital to recovery and that therapy must be done by a qualified hand therapist. Dr. Hunter will not operate unless the patient agrees to the post-operative therapy.
The Wrist Dr. Hunter discussed the failing wrist and fusion (arthrodesis). If the wrist is failing and needs fusing it comes after splinting and long study. The wrist may be splinted in several different positions to see which position is the most effec- tive and the patient is the judge. The physician can do individual finger splint- ing to further determine what is most helpful to the patient. Selective splinting gives information about what is effective for the patient and if surgery will help.
Other Options Ifa patient rejects surgery, the physician has the information to selectively splint the hand for optimum function Dr. Hunter encourages patients to talk with other patients who have experienced hand surgery and therapy. Patients do get into fvred habits and refuse treat- ment. Sometimes the mind set of the patient precludes any therapy. Occa- sionally, the family is reluctant to allow therapy for a child. They are not looking ahead to the time when that child must perform adult functions and be self-sup- porting. Dr. Hunter compared CMT with the position of rheumatoid arthritis
CMT Facts, page 12

several years ago. At that time rheuma- toid aahritis patients were not sent to hand therapists for treatment. The result- ing problems of the arthritic hand stemmed, not from the disease process which was long gone, but from the ne- glect of the unprotected deformed joints. Over time daily living tasks performed without protective splinting tear the joints apart The loss of muscle causes the ligaments to stretch and then joints sag and new deformities result. As the joints wear out there is a loss of balance in the hand. Today, the arthritic patient is seen fitquedy by the hand surgeon for his/her expert care. The surgeon quali- fied to treat the hand has been trained in orthopedic techniques, micro-surgery and plastic surgical techniques. Some hand surgeons have received their initial training in orthopedic surgery and others in plastic surgery. They then go on to specialize in surgery of the hand and upper extremities. Additionally, and
Muscle Balance
necessary for the CMT patient, some have gone on for further study of periph- eral neuropathies.
Carpal Tunnel Syndrome The CMTA has been informed by neu- rologists that CMT patients should be wary of carpal tunnel syndrome surgery since the CMT disease process can mimic that syndrome. When asked that question Dr. Hunter agreed that carpal tunnel did present a diagnostic problem. A differential diagnosis must be made to determine if the problem stems from car- pal tunnel syndrome or CMT. Nerve conduction studies would be an essential part of the very thorough neumlogical work-up necessary to make an accurate diagnosis.
In conclusion Dr. Hunter stressed that CMT is a progressive disease that fre- quently reaches a plateau. When the dis- ease is at a plateau, the unchecked and untreated deformity continues to pro-
gress. This deformity progression can be forestalled and perhaps halted with early assessment and intervention by the hand therapy team of surgeon and therapist. However, assessment at any time can certainly be of benefit and is an option that every Ch4T patient should consider. Treatment started now might enable the patient to perform tasks in later years that would be impossible without h cam
Referral Sources To find a qualified hand surgeon in your m a contact the American Society for Surgery of the Hand, 3025 South Parker Road, Suite 65, Aurora, CO80014; (303) 755-4588.
0
Muscle Imbalance
The CMT Hand The Intrinsic minus hand (claw hand) has lost function of both the lumbricals and the intemssei muscles. Imbalance of the pull of Extensor digitorurn communis causes hyperextension of the MP joints and flexion of the IP joints. When this condition exists, the classic picture of the claw appears. The distal transverse arch is flattened completely which, in turn, renders the thumb useless except for the lateral grasp. (From the Manual of Management of the Quadriplegic Upper Extremity, by Maude Malick, OTR, 1978, Harma~ille Rehabilitation Center.)
CMT Facts, p q e I3

OCCUPATIONAL THERAPY AND THE CMT PATIENT
This article was written j?om a dis- cussion between the CMTA and Joanne Cassidy, M.Ed., O T R L Ms Cassidy is a Registered Ocupational Therapist, Chief of Occupational Therapy at Thomas JeJerson Hospital in Philadel- phia, PA, and teaches at Thomas JeJer- son University.
How does occupational therapy (OT) re- late to the CMT patient?
The occupational therapist should have a vital role in the care of the CMT patient. The initial visit would be a thor- ough hand evaluation. We would look at the hand and see how to increase hand finction. This can be done by an exercise program and/or a splinting program de- signed to support structures, to substi- tute motion, or regain range of motion. The OT is also concerned with direct functional application in daily living ac- tivities. Everyday things like buttons, eating utensils and zippers can be prob- lemsfor the patient. We also mod;& ath- letic equipment such as golf clubs and tennis racquets. The key philosophy of the OT is that the work of daily living is an integralpart ofthe rehabilitationpro- gram of the patient. In other words, be- ing able to care for your own daily needs is therapy in itse f j When treating trauma patients, early on we have the patient care for him/herselJ: In chronic illnesses we slowly introduce adaptive measures to allow the patient to remain inde- pendent.
What do you assess on the patient's first visit?
A standard basic evaluation includes current hand function, documented grip strength, range of motion, and notation o u x e d defirmities and weakness. We also discuss current vocational interests, hobbies and daily living tasks. We work very closely with PT's who are more involved with the patient's overallphysi- cal motion. We also must consider the patient's whole body range of motion. I read the PT's evaluation as part o f n y assessnrent process.
Who refers CMT patients to you? Primarily neurologists but sonre-
times our referrals are jFom orthopedic
night splint
surgeons. Here at Jegerson we get refer- ralsj?om many diflerent sources. Since Jegerson is such a diverse place we are called in from a variety oJsources.
What is splinting? Splinting is a way of supporting a
structure. For some splints we use a low temperature, light weight plastic, warm- ing it in water and then molding it to the patient's hand for a specific purpose. This material is very versatile and we use it for many applications. For example, an eaJy splint to do is a wrist cock-up splint. It is done to stabilize a weak wrist, and gives the jngers more power. Most of the muscles for the jngers run j?om the arm across the wrist. They lose power going across the dropped wrist. In the claw hand there is a hyperextension of the MP joints and ajlexion (cocking- up) of thejngers (see diagrams on p. 13). This corresponds to the hammer toes of the foot. Splints can be made for a spe- cijc activity or for general purpose use. Splints are madejiom a variety ofmate- rials. Elastic straps can be used which allow a range of motion. The splints are highly customized and adapted to the patient's needs and usage. Some splints are for resting night time use and some are taskspecijc. A thumb splint could be used to keep the thumb out, to allow pinching with the indexjnger.
What is the age range of patients you have treated?
Most of my patients have been in their 40's and 50 's. They were adapting to daily living and work related tasks. I have treated one teen-age patient who was a high schoolgolfer. He was a mem- ber of the school golf team, and we adapted golf clubs for him.
What are some adaptive devices that are used in a home setting?
A common tool is the button hook to aid in buttoning. Buttoning requires the thumb and indexjnger, andfor some this is very diflcult. The button hook goes through the buttonhole and grabs the button. It is then pulled through the but- tonhole by wrist or shoulder action. An- other tool is a long handled shoe horn. This aids the patient who wears AFO 's and other adaptive footwear. Elastic shoe laces, which don't need tying, and velcro are two great adaptations for shoes. Sock donners assist the patient in putting on socks.
Where can the patient purchase these and other gadgets?
When a patient is evaluated, most of the gadgets are available here. There are several medical supply catalogs that sell directly to the patient. (See p. 15)
What about eiercise? If the nerve has some activity, then
the muscle can be exercised. The claw hand is a hand out ofbalance. One group ofmuscles is stronger and overpowers a weaker group ofmuscles, and this dis-
CMT Facts, page 14

torts the appearance andfitnction of the hand. With specijic activities we work to maintain and increase strength in the weaker muscle group to maintain bal- ance of the hand. For exercise we use puttiesanda wide range ofrubber bands to exercise h e hand using very specijic motions. These are very simple tools and very efective. The exercises and activi- ties can be done in idle and spare time.
What would be a long term therapy pro- gram for a CMT patient?
It is very specijic to the individual depending on hisher disease and life- style. In an exercise program there should be a regular routine to maintain muscle strength. A couple of short daily sessions are better than one long session. This lessens the chance of over fatiguing an already weakened muscle. If cramp ing andpain lasts longer than 1/2-1 hour after exercising the muscle has been over exercised. With weak muscles we begin with a light rubber band and only a few repetitions. Itellpeople to use the rubber band when watching TC.: talking on the phone etc. Putty can be used similarly.
What training does an OT receive? There are two drgerent approaches.
The jrst is a four year program with a six month internship which gives a de- gree in occupational therapy. Also a stu- dent may be a college graduate in a relatedjeld and then goes through an 18-24 month certificate program. In ad- dition, there is a six month internship. Students fiom both courses must pass a national certifiing examination. Suc- cessfirl completion of this registers the OT and he/she then is an OTR Also, most states have a license requirement, and it varies from state to state. More- over, there is a two year program to be a certijied OT assistant. They work un- der the supervision of an OTR, and carry outprescribedservices. Of course, there are also advanced degree programs in OT.
What are the cost ranges for OT serv- ices?
They are very variable with the aver- age being $75.00/hour with a range of $50.00-1 00.OO/hour depending on loca- tion. Major centers are usually higher. Insurance reimbursement for OT serv- ices is poor. In-hospital services are gen- erally covered but outpatient care is usually not covered. Unfortunately, most
insurance plans do not cover chronic conditions. Medicare and some state programs cover OT services. Private coverage variesfi.om state to state and plan to plan. Our national organization has reimbursement for OT'sas apriorily item. Some states have a mandatory law requiring reimbursement for OT serv- ices prescribed by a physician. This is what the national organization is work- ing to establish in all states.
How can a patient find a hand facility? The patient should call hisher local
hospital and ask for the OT department. If there is none ask for the PT department and they will make a referral.
adaptive hair brush
Gadgets Catalogs Following is a list of catalog suppliers of "adaptive equipmentw- gadgets!
* ABLEWARE A Division Of Maddak, Inc. Pequannock, NJ 07440- 1993
* COMFORTABLY YOURS 61 West Hunter Avenue Maywood, NJ 07607-1005 201/368-0400
* BRUCEMEDIC4 L SUPPLY 41 1 Waverly Oaks Rd. Waltharn, M A 02154 8001225-8446
* EMIICHMENTS, INC. P. 0. Box 579, 145 Tower Dr. Hinsdale, IL 60521 800/343-9742
* INDEPENDENT LIVING AIDS Plainview, NY 11 803 8OO/262-782 7
GLOSSARY
The following glossary is intended to help the reader understand the iuti- cles in this publication. The deftni- tions are rather general, and no attempt was made to give complex anatomical explanations.
ADL's - Aids to daily living
Ataxia - inability to perform coordi- nated muscular movements
Caws Foot - foot with a vexy high arch
CMT - Hypertrophic - peripheral nerve fibers are thickened, myelin sheath breaks down.
CMT - Neuronal - the axon or cc* tml part of the nerve cell deteriorates
Hypotonia - dimumition or loss of muscle tone, consequently muscles may be stretched beyond their mr- ma1 limits.
Muscular atrophy - wasting of the muscles due to diseased or injured nerves
Muscular dystrophy - wasting of the muscle due to a defect in the muscle itself
Myelin sheath -fatty outer covering of a nerve fiber
Palsy - a condition marked by loss of power to feel or to control movement in any part of the body
Peroneal muscle - group of muscles below the knee on the outside of the leg going from just below the knee to the ankle. These muscles raise the Foot during walking.
Tendon - tissue which connects muscles to bones
CMT Facts, page 15

i I want to be in touch with the CMTA! i
Name:
; Address:
i Phone Number
! Tell us about purse@ 0 CMT Patient
CMT Family Member
Medical Professional
O other
Join the fight against CMT!
i Enclosed is my gi) o$
$35 Member
$ other
Please make check payable to The CWA Your contribution is tax deductible.
If you would like a copy of this publication, "CMT Facts I", please i check here and enclose a check or money order payable to The CMTA i for $3.00 to cover printing and majling costs.
i Mail completed form to:
The CMTA, 601 Chestnut Parkway, Chester, PA 1901 3 . .
Certain Drugs Toxic to the Peripheral Nervous System
h
MEDICAL \ ALERT This is a list of neurotoxic drugs which could be harmful to the
CMT patient. Adriamycin Alcohol Amiodarone Chloramphenicol Cis-platinum Dapsone Diphenylhydantoin [Dilantin) Disulfiram (Antabuse) Glutethimide (Doriden) Gold Hydralazine (Apresoline) soniazid (INH) Mega Dose of Vitamin A Mega Dose of Vitamin D Metronidazole (Flagyl) Uitrofurantoin :Furadantin, Macrodantin) Uitrous Oxide :chronic repeated inhalation) Penicillin ;Large IV doses only) Perhexiline (Pexid) Pyridoxine (Vitamin B6) Jincristine
Before taking any medication pleiue discuss it fully with your h t o r for ~ossible side effects.
L Join the CMTA! Return the above form and receive our Charcot-Marie-Tooth Association quarterly newsletter, CMTA Report. 2700 Chestnut Parkway This will put you in touchwith the CMT chester, PA ,9013 community and keep you informed of 1-800-606-CMTA current CMT research, treatment innova- tions, support group meetings, CMT conferences and provide you with other helpful information. The CMTA has published a sequel to this publication which is entitled CMT Fads II. The CMTA also has medical lectures on VCR tape which were made at past CMT patientlfamily conferences. For infonna- tion about ordering these resources con- tact the CMTA.
CMT Facts, page 16