Let’s move to the Adrenal Glands
55
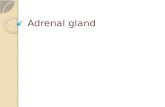
Let’s move to the Adrenal Glands In this space, please draw an adrenal gland…. Where does it live, what is its shape? Does it communicate with the kidney? Did you include the inner and outer part of the adrenal gland?
description
Let’s move to the Adrenal Glands. In this space, please draw an adrenal gland…. Where does it live, what is its shape? Does it communicate with the kidney? Did you include the inner and outer part of the adrenal gland?. Lots of Group Activities so let’s get into our groups. Group 1: - PowerPoint PPT Presentation
Transcript of Let’s move to the Adrenal Glands

Let’s move to the Adrenal GlandsIn this space, please draw an adrenal gland….
Where does it live, what is its shape? Does it communicate with the kidney?Did you include the inner and outer part of the adrenal gland?

Lots of Group Activities so let’s get into our groupsGroup 1:Group 2:Group 3:Group 4:Group 5:Group 6:

Now come up with a Name of your Group
Group 1:Group 2:Group 3:Group 4:Group 5:Group 6:

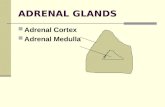
What are the 2 parts of the Adrenal Gland???Inner part is the _________
________
What does the inner part secrete or release?
_____________________ ______________________

What are the 2 parts of the Adrenal Gland???Outer part is the _________
________
What does the outer part secrete or release?
_____________________ _____________________ ______________________

Sugar….Salt….and Sex

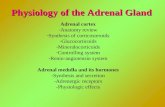
Let’s go with the Adrenal Cortex first…..3 Hormone types:
Glucocorticoids (Cortisol)Mineralocorticoids (Aldosterone)Androgens (Testosterone)
Or………..Sugar, Salt and Sex
Activity: Giving you 10 minutes, get in your group and create a jingle, song or rap about these 3 types of hormones…..

Disorder #1 Cushing’s Disease We are nurses taking care of a patient with Cushing’s Syndrome
What is Cushing’s syndrome?Too much _______________What is a synthetic form of
cortisol that you have probably administered in clinical to your patients?
Syndrome vs Disease………..

Too much Cortisol….What do you remember
about cortisol or side effects of glucocorticoids?
Write down here what you remember…..

Do you need to look up cortisol?Consult with your team and
combine what you all know about cortisol?
Record data here:______________________________________________

Cushing’s Syndrome vs Cushing’s DiseaseSyndrome is iatrogenically
induced, how?________________________Cushing’s disease could be caused
by a tumor causing too much cortisol release.
Where could the tumor be located?1. ________________ 2._____________3. ___________________

Textbook Pic of Cushing’s Syndrome/Disease

Can we live without glucocorticoids or cortisol?
What does cortisol do in our body?
CHO (carbohydrate) metabolism
Fatty acid mobilizationProtein catabolism
Ding ding

Function of Cortisol or Glucocorticoids:***CHO MetabolismWhat happens when we break down
carbohydrates?Increase in amount of glucose formedIncrease in amount of glucose
released
Therefore a major complication is_______________________

Function of Cortisol:*****Fat metabolismWhat happens when we mobilize
fatty acids somewhere unusual?
Therefore we see some classic body image changes in our patient-name these here:
________________________________________________

Re Group for a POC ActivityDevelop a plan of care for a
patient with Cushing’s Disease
What are the priorities?
What can the nurse expect to see in this patient?

Function of Cortisol:****Protein breakdown or catabolismWhat happens in Cushing’s
syndrome with protein breakdown, how does this look in our patients?
________________________________________________________

Re Group for a POC ActivityDevelop a plan of care for a
patient with Cushing’s Disease
What kind of things can the nurse call the physician about in preventing complications in this patient? SBAR ideas?

Clinical reasoning….If glucocorticoids have a
mineralocorticoid like effect, what would we see in our patients?

Too much Aldosterone or Hyperaldosteronism
Excessive retention of Na and H2O
Excessive excreting of K+
So what would we see in clinical in our patients?
______________________________________________

Still in the Adrenal Cortex…now 2nd major group of hormonesMineralocorticoids or
Aldosterone
You know this…what does aldosterone do?
What stimulates its’ release?

Still in the Adrenal Cortex…now 3rd major group of hormonesAndrogens or Testosterone
What happens if females have too much testosterone?
_______________________________________

What diagnostic tests could help diagnose Cushing’s Disease?Serum cortisol levelsSerum ACTH levelsCT scan of abdomen or
adrenalsMRI of brain to detect if
pituitary adenoma24 hour urine for cortisol

Normal Cortisol Levels

What would we expect to see in Cushing’s, what would the graph look like?Try to draw here
So in summary, what effects the release of cortisol?
________________________
What would the serum levels of cortisol be at 8am vs 8pm?
________________________

Collaborative Management of Cushing’s DiseaseNeed to know what first?????_____________________________
Open adrenalectomy or laparoscopic adrenalectomy if tumor or cancer of
adrenal glandWhat if it is an ectopic tumor releasing
too much ACTH? How would this be managed or treated? __________________________
What other surgery could be necessary?______________________________________

Medications-Cushing’s DiseaseMitotane (Lysodren) which
suppresses cortisol production if surgery not an option
Ketoconazole (Nizoral) inhibits cortisol synthesis
Activity: Look up doses and routes of these medications and list as would be on the MAR

Medications-Cushing’s DiseaseMitotane (Lysodren)
Ketoconazole (Nizoral)
Why would these be called a “medical adrenalectomy”

Write a detail nurse’s note on the appearance of the client’s skin or “Prednisone skin”

Prednisone skin documentationSkin is fragile, thin and has
decreased elasticity. Multiple areas on all 4 extremities of dark purple bruises.

What assessment findings would you document?

What does Cortisol do to the immune system?
What would you have in your POC?
________________________________________________________________________________________

Cushing’s Disease-During

Cushing’s Disease-After Treatment

Now the innermost part of Adrenal GlandWhat is it called?_________________________What does it release?1.___________________2.___________________What “response” does it trigger?____________________________

Ok let’s summarize, how to collaboratively intervene in patient with Cushing’s disease/syndrome?

Disorder #2 HyperaldosteronismToo much aldosterone secretionWhat does aldosterone do?___________________________________________________Usually caused by a tumor on
Adrenal cortex

Clinical Manifestations: HyperaldosteronismHeadache due to Na and H2O
retentionHTN due to Na and H2O retentionK+ excretion which leads to
________ muscle weakness, fatigue cardiac dysrhythmias usually no edema

Diagnostic Tests: Hyperaldosteronism urinary K+
plasma aldosterone levels with low
plasma renin levels---WHY?
CT scan will reveal adenoma of adrenal
gland EKG changes

Collaborative Management of HyperaldosteronismLow sodium dietK+ sparing diuretic such as
aldactone…How will this help perfectly???___________________________Calcium channel blockers to treat
the elevated blood pressureAdrenalectomy

Disorder #3 Addison’s DiseaseWhich famous President had
Addison’s Disease?

What is Addison’s DiseaseToo little of Sugar, Salt, and Sex
glucocorticoids
mineralocorticoids
androgens

Not enough Cortisol? POC priorities________________________________________________________________________________________________

Not enough Aldosterone…..POC priorities__________________________________________________________________Salt craving—why?Not enough Androgens…what
could be a priority?______________________

Diagnostic Studies-Addison’s DiseaseSerum cortisol levels or
Urine cortisol high or lowHypo or hyper kalemic?Serum glucose levels or
Serum aldosterone levels high or low?
EKG peaked T waves due to hyperkalemia

In summary…Low bpF & E imbalancesHypoglycemicHyponatremiaHyperkalemiaNausea and VomitingDehydrationAnxiety, irritable

Addisonian Crisis or Acute Adrenal CrisisSevere hypotensionTachycardiaSevere nausea and vomitingHypovolemic shockHypoglycemiaHyponatremiaHyperkalemia

Emergency Treatment-Addisonian Crisis or Adrenal Crisis
Rapid infusion of IV fluids (D5NS)Frequent VS and I & OMay need to administer
vasopressors to bring up blood pressure
Solucortef IVP until enough glucocorticoid on board

Collaborative ManagementAddison’s DiseaseOral glucocorticoids 2/3 dose in am 1/3 dose in pmDOC is Cortate poOral mineralocorticoidFlorinef 0.1mg poLifelong hormone replacementStress management

Patient Teaching-Addison’s –ding dingSalt additives for excess heat or humidityDaily glucocorticoid replacement Daily mineralocorticoid replacementList of all medsMedical identification device in wallet, or
in the form of a bracelet or necklaceConditions requiring larger dose of
hormones (surgery, trauma, happy stress) IM glucocorticoid administration by patient
(100mg hydrocortisone kit)

Disorder #4 Pheochromocytoma-in the Adrenal MedullaRare, benign tumor of the
adrenal medulla
Oh no, what are we going to see a hyper secretion of???
______________________________________

Clinical ManifestationsHallmark is hypertension-200/150 or >NE and Epinepherine released
sporadicallyDeep breathingProfound sweating due to peripheral
vasoconstrictionPounding HRHeadacheVisual disturbances“Spells” or paroxysmal attacks
◦Triggers can be from bladder distension, exposure to cold, emotional distress

Pheochromocytoma-Diagnostic StudiesIncrease serum NE and
Epinepherine levelsIncrease in urine metabolites of
NE and EpinepherineCT scan of adrenal gland(s)MRI of adrenal gland(s)

Collaborative Management-PheochromocytomaAdrenergic Blocker1. Minipress to decrease bpBeta blocker1. Inderal to decrease HR and bp and
force of contraction also helps reduce anxiety
Monitor vs Adrenalectomy-usually laporoscopic If having episode, elevate HOB and
complete bedrest

During surgery….and post opPotent vasodilator Regitine or
Nipride administered due to manipulation of tumor in the medulla and surge of NE and Epi
BP may be elevated initially, but can bottom out post operatively, why?
If not a surgical candidate, then drug Demser (drug which inhibits catecholamine synthesis) is given