hypothalamus , pituitary and adrenal glands
137
THE ENDOCRINE SYSTEM By : Rijaa A .
-
Upload
rijaa -
Category
Health & Medicine
-
view
48 -
download
6
Transcript of hypothalamus , pituitary and adrenal glands
THE ENDOCRINE SYSTEM
By : Rijaa A.
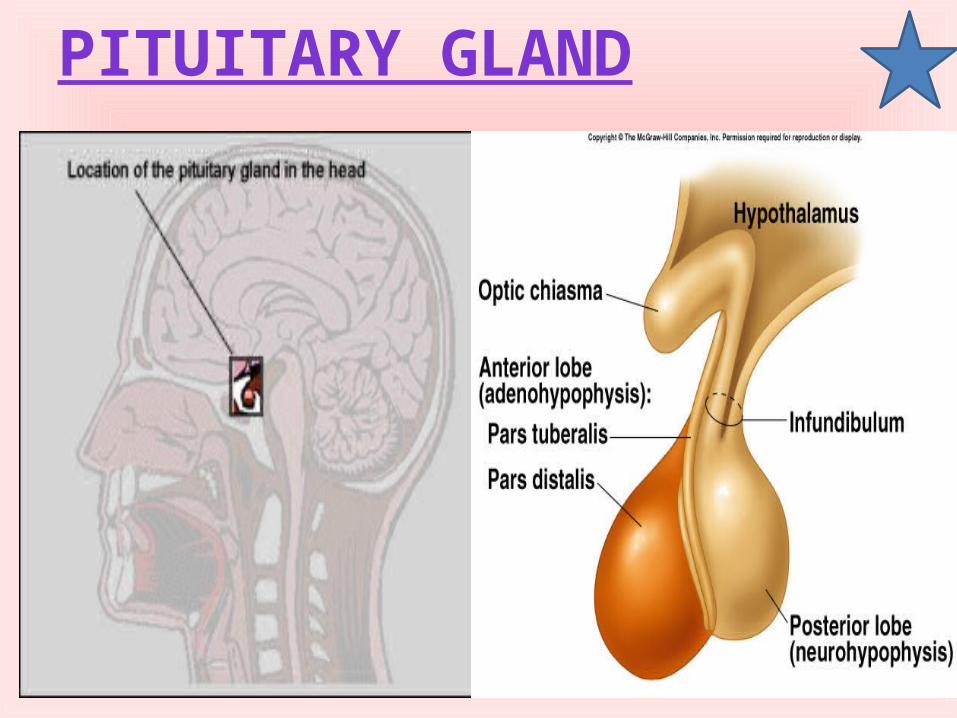
PITUITARY GLAND
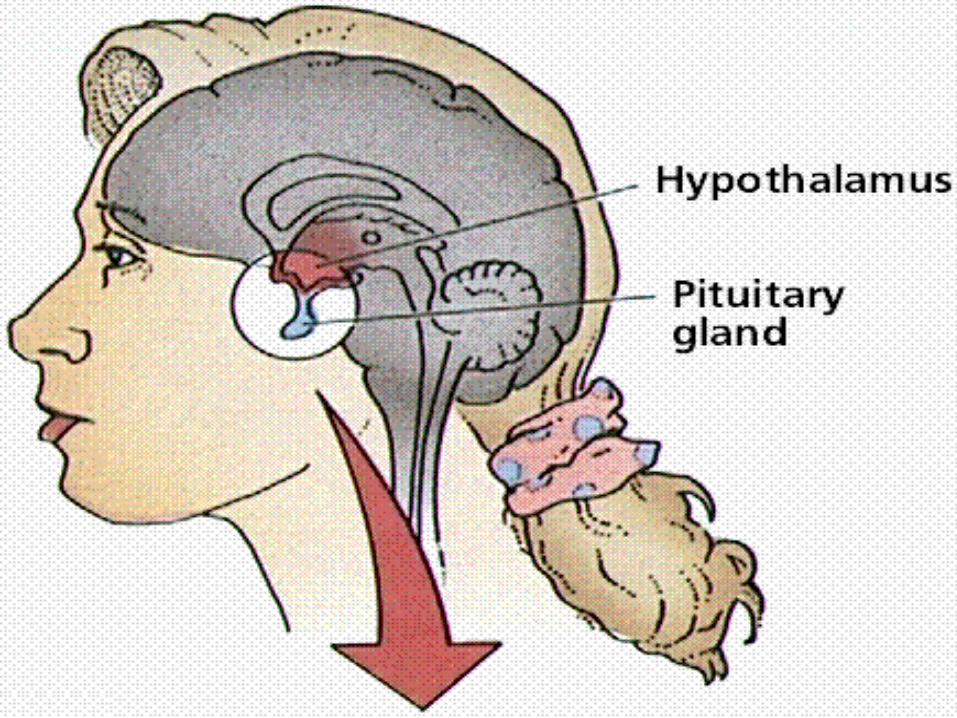
• Difintion :• The pituitary is an endocrine
(hormone-producing) gland that sits just beneath the base of the brain, behind the bridge of the nose.
• It is very small – only about the size of a pea , and weighing 0.5 grams .
• It is very important as it takes messages from the brain (via a gland called the hypothalamus) and uses these messages to produce hormones that affect many parts of the body, including stimulating all the other hormone-producing glands to produce their own hormones. For this reason it is often referred to as the ‘master gland’.
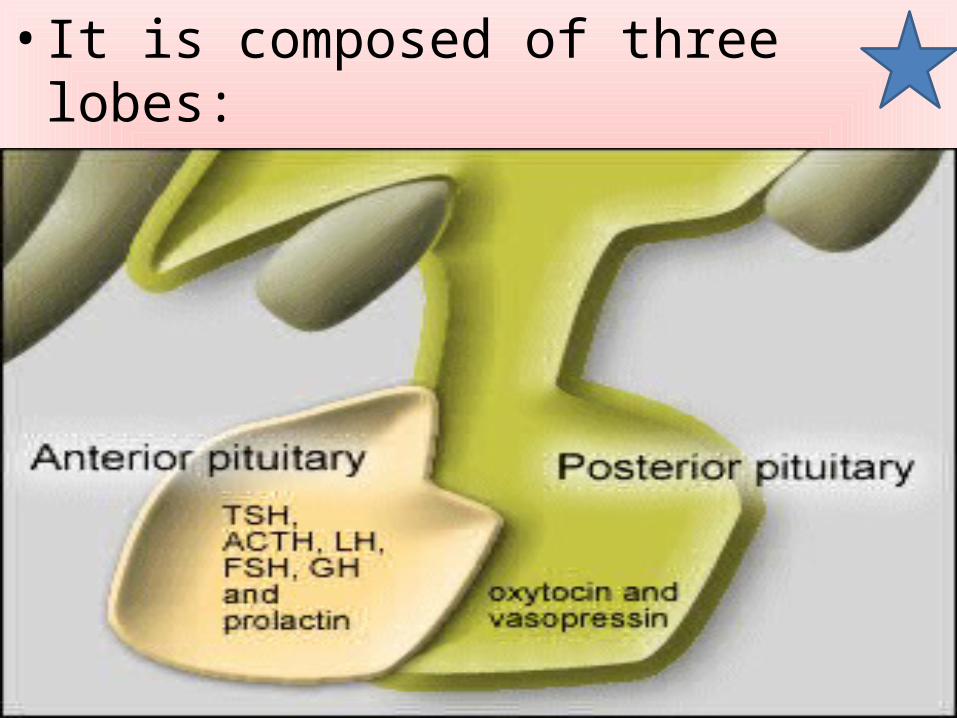
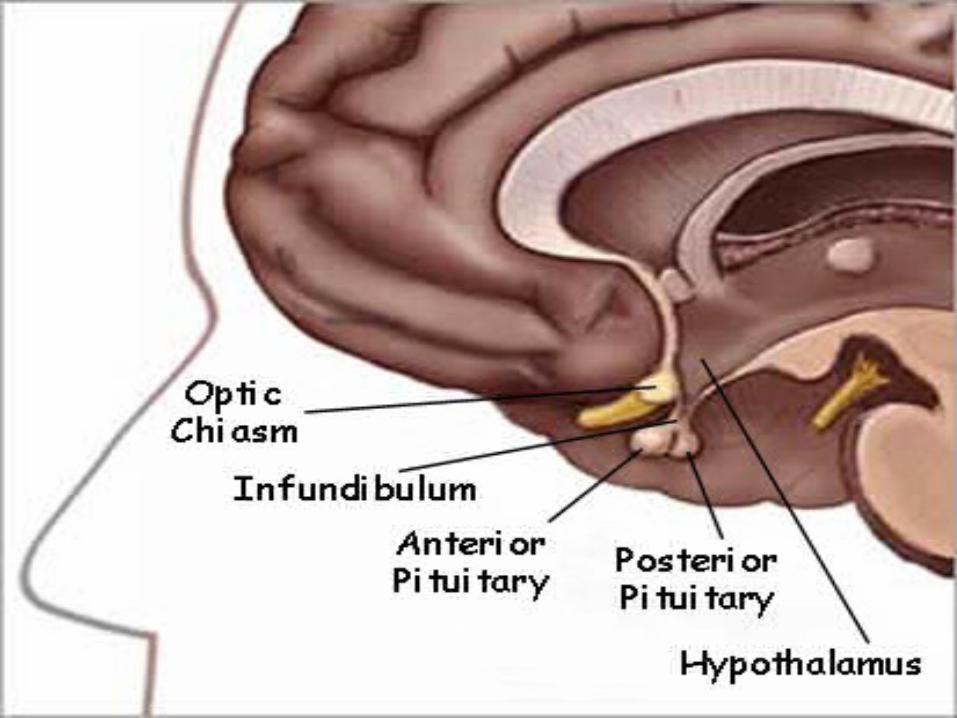
• It is composed of three lobes:• anterior, intermediate, and posterior.
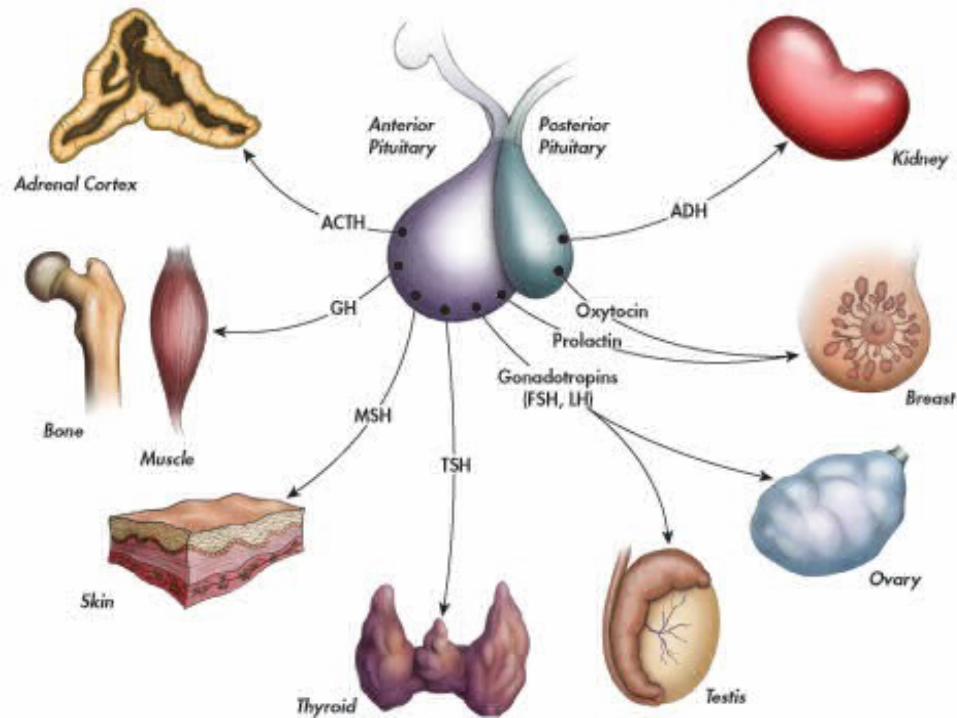
Hormones secreted• The anterior pituitary • synthesizes and secretes the following important
endocrine hormones. All releasing hormones (-RH) referred to, can also be referred to as releasing factors (-RF ) .
• 1-Somatotrophins:• Human growth hormone (HGH), also referred to as
'growth hormone' (GH) , and also as somatotropin, is released under the influence of hypothalamic growth hormone-releasing hormone(GHRH), and is inhibited by hypothalamic somatostatin
• 2- Thyrotrophins:• Thyroid-stimulating hormone (TSH), is
released under the influence of hypothalamic thyrotropin-releasing hormone (TRH) and is inhibited by somatostatin.
• 3 - Corticotropins:
Adrenocorticotropic hormone (ACTH), and Beta-endorphin are released under the influence of hypothalamic corticotropin-releasing hormone (CRH).
• 4 - Lactotrophins:• Prolactin (PRL), whose release is
inconsistently stimulated by hypothalamic TRH, oxytocin, vasopressin, and inhibited by hypothalamic dopamine.
• 5 - Gonadotropins:• Luteinizing hormone (also referred to as
'Lutropin' or 'LH').• Follicle-stimulating hormone (FSH), both
released under influence of Gonadotropin-Releasing Hormone (GnRH)
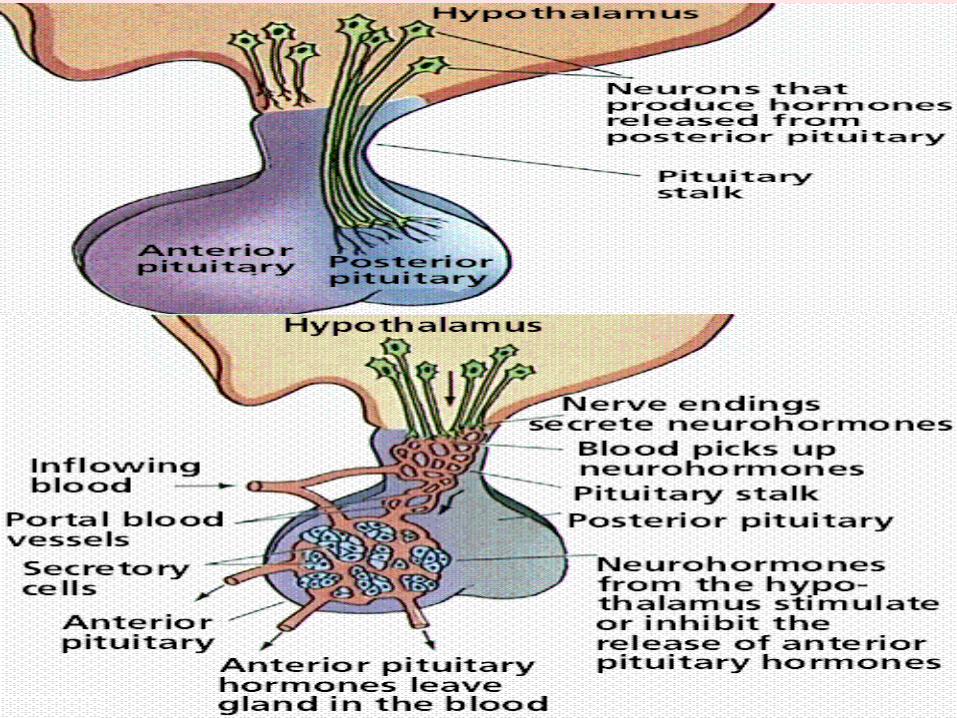
• These hormones are released from the anterior pituitary under the influence of the hypothalamus. Hypothalamic hormones are secreted to the anterior lobe by way of a special capillary system .
• The Posterior pituitary• The posterior pituitary stores and secretes
(not synthesize) the following important endocrine hormones:
1 - Antidiuretic hormone (ADH, also known as vasopressin and arginine vasopressin AVP).
2 – Oxytocin .
Functions
• Hormones secreted from the pituitary gland help control the following body processes:
• Growth• Blood pressure• Some aspects of pregnancy and childbirth
including stimulation of uterine contractions during childbirth
• Breast milk production
• Sex organ functions in both males and females• Thyroid gland function .• The conversion of food into energy
(metabolism) .• Water and osmolarity regulation in the body .• Water balance via the control of reabsorption
of water by the kidneys .• Temperature regulation .• Pain relief .
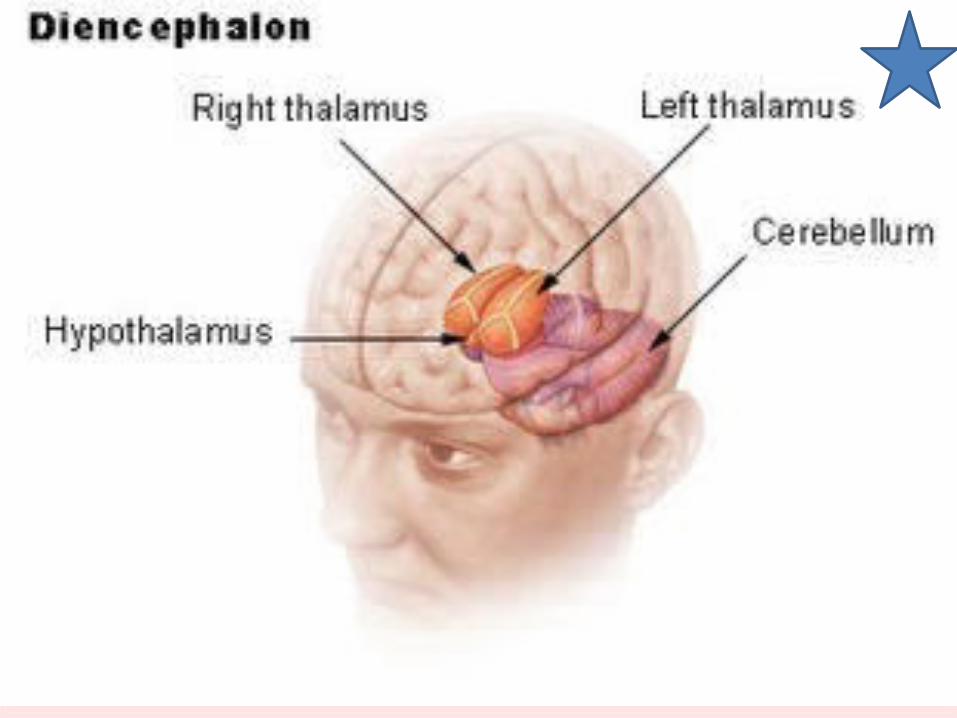
Hypothalamus
• is a portion of the brain that contains a number of small nuclei with a variety of functions. One of the most important functions of the hypothalamus is to link the nervous system to the endocrine system via the pituitary gland (hypophysis).
The hypothalamus controls• Body temperature.• Hunger.• Important aspects of parenting and
attachment behaviors.• Thirst. • Fatigue. • Sleep. • And circadian rhythms.
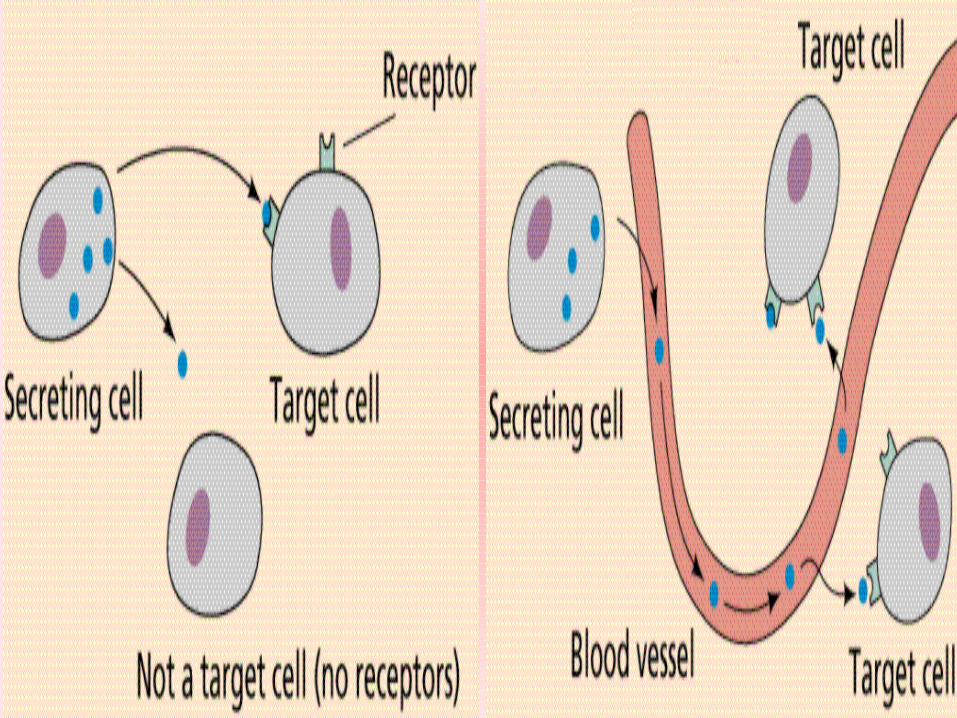
Hormones• Hormones are chemical
messengers that are secreted directly into the blood, which carries them to organs and tissues of the body to exert their functions. Hormones are secreted from the endocrine glands in the body.
• The glands are ductless, so hormones are secreted directly into the blood stream rather than by way of ducts.
Hormonal Regulation• Regulating hormones means controlling
how much hormones are made and released from cells.
• Hormones secretion is regulated through the hypothalamus and pituitary which regulate their own secretion through negative feedback inhibition.
• Negative feedback occurs when the rate of the process decreases as the concentration of the product increases.
• Negative feedback leads to hormone production switching on and off, creating pulses of hormone secretion. This means that blood hormone levels rise and fall cyclically, within a relatively narrow normal range.
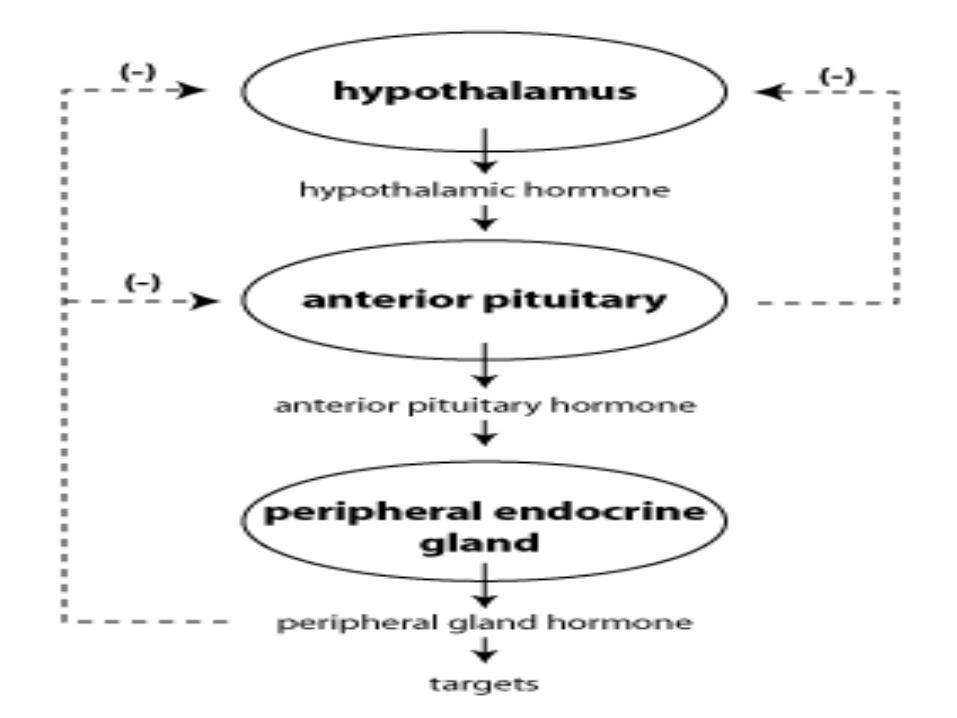
• What this means is that a hormone from a peripheral gland, binds to its receptor on cells in the hypothalamus and pituitary, and has the effect of inhibiting secretion of tropic hormones.
• The usefulness of negative feedback inhibition is that it results in "hormonal homeostasis", that is the maintenance of hormone levels within a particular appropriate physiological range.
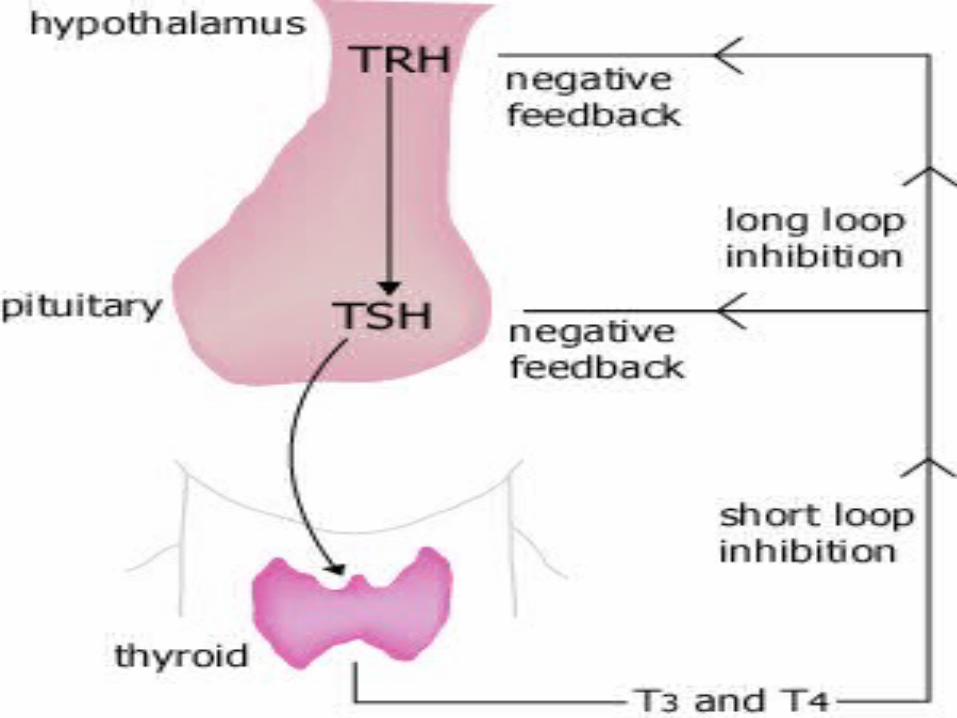
• An example of negative feedback in the endocrine system can be seen in the regulation of thyroid hormones.
• It starts with the brain's hypothalamus, which produces thyroid releasing hormone (TRH).
• This hormone moves to the nearby pituitary gland, causing production of thyroid stimulating hormone (TSH), which is then released into the blood stream.
• On reaching the thyroid, TSH stimulates the cells there to now secrete thyroid hormones.
• When the level of thyroid hormones in the blood reaches an upper threshold, the cells in the hypothalamus that make and secrete TRH are affected.
• The result is that TRH, then TSH, and finally thyroid hormone levels fall.
• Once the level of thyroid hormones in the blood falls below a lower threshold point, negative feedback ends.
•
• ( In negative feedback, the hormone's effect makes a gland stop making hormones ) .
Positive feedback • occurs when the rate of a process
increases as the concentration of the product decreases.
• In positive feedback the opposite happens. The effect of the hormone tells the gland to make even more hormones.
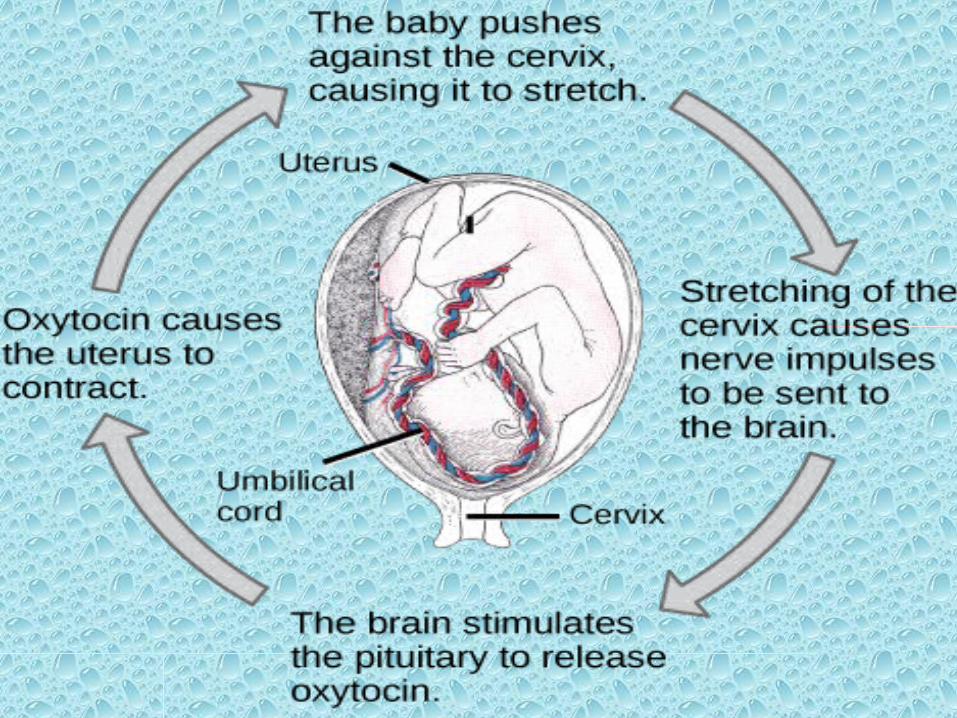
• One example of a biological positive feedback loop is the onset of contractions in childbirth.
• When a contraction occurs, the hormone oxytocin is released into the body, which stimulates further contractions.
• This results in contractions increasing in amplitude and frequency.
• Childbirth contractions stop when the baby is out of the mother's body.

Adrenal gland
رجاء \ الكيمياويه اعدادعبود
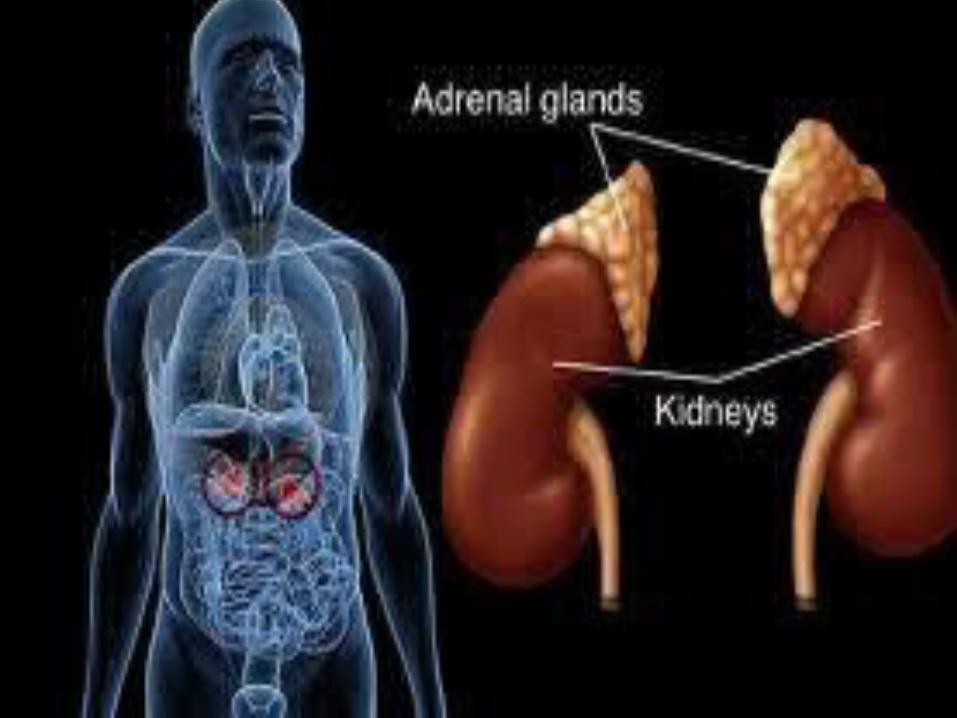
Adrenal gland• Difintion :
are endocrine glands that sit at the top of the kidneys; the right adrenal gland is triangular shaped, while the left adrenal gland is semilunar shaped. They secretes hormones directly into the bloodstream.
• Anatomy and physiology
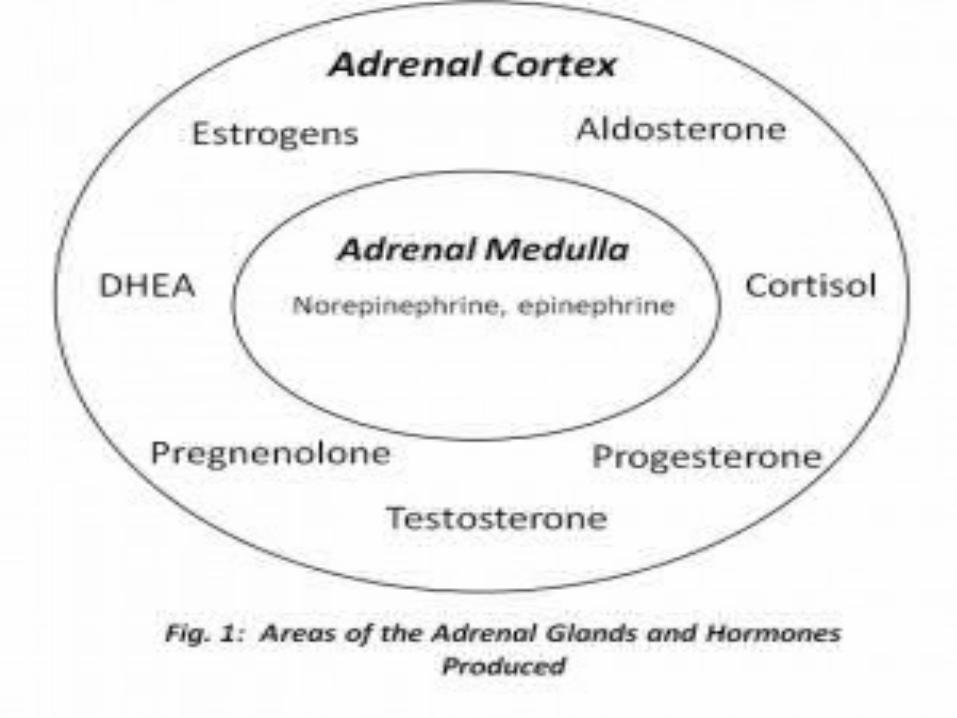
• An adrenal gland is made of two parts:
1- Adrenal cortex ,The outer region which is regulated by neuroendocrine hormones secreted from the pituitary gland which are under the control of the hypothalamus.
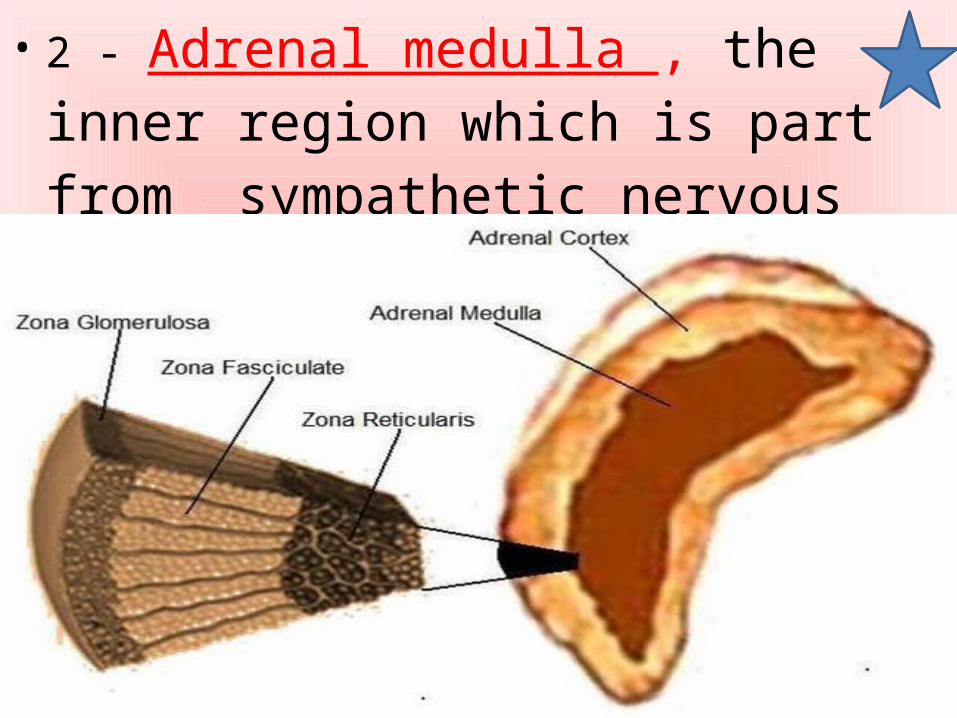
• 2 - Adrenal medulla , the inner region which is part from sympathetic nervous system .
• adrenal cortex
• The adrenal cortex is responsible for creating three different types of hormones:
• A- mineralocorticoids which save sodium in the body.
• B- glucocorticoids which increase blood glucose levels.
• C- and gonadocorticoids which regulate sex hormones such as estrogen.
• Death would result if the adrenal cortex were to stop functioning as it controls metabolic processes that are essential to life.
• The adrenal cortex include three zones, or layers ,each zone produce and secrete distinct hormones:
1- Zona glomerulosa (outer) is the main site for production and secretion of mineralocorticoid mainly aldosterone . 2- Zona fasciculate ( middle ) ,responsible for producing glucocorticoids mainly cortisol .
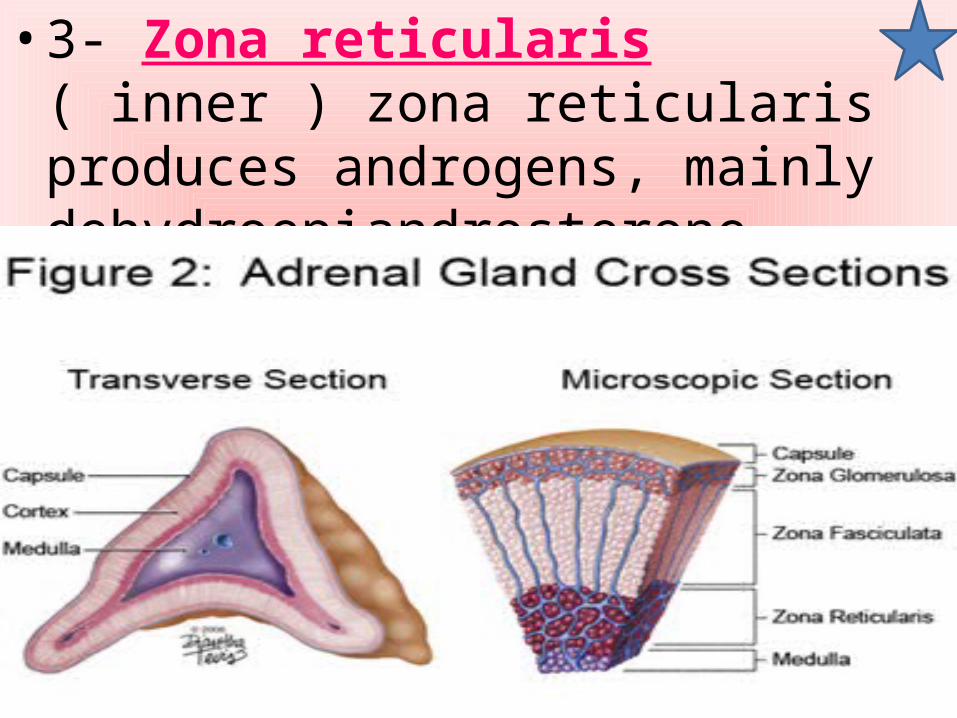
• 3- Zona reticularis ( inner ) zona reticularis produces androgens, mainly dehydroepiandrosterone (DHEA) .
Glucocorticoids•Cortisol • Is the main glucocorticoid under normal
conditions it is also Called “the stress hormone,” .
• When you faced a threat — your hypothalamus, sets off an alarm system in your body.
• Through a combination of nerve and hormonal signals, this system induce your adrenal glands, to release a surge of hormones, including adrenaline and cortisol.
• Adrenaline increases your heart rate, elevates your blood pressure and increase energy supplies.
• Cortisol, the primary stress hormone, increases sugars (glucose) in the bloodstream.
• Enhances your brain's use of glucose . • And increases the availability of
substances that repair tissues .
• The body's stress-response system is usually self-limiting. Once the threat has passed, hormone levels return to normal.
• As adrenaline and cortisol levels drop, your heart rate and blood pressure return to baseline levels, and other systems resume their regular activities.
Function of Cortisol• cortisol influences, regulates or modulates
many of the changes that occur in the body in response to stress including :
1 - Blood sugar (glucose) levels.plays an important role in (glycogenolysis ), the breaking down of glycogen to glucose-1-phosphate and glucose, in liver and muscle tissue.
2 - Fat, and protein metabolism to maintain blood glucose (gluconeogenesis) .3 - It reduces protein uptake (those proteins are used in gluconeogenesis) by the muscles. So, if cortisol is around for long periods of time, it can lead to a reduction in lean muscle mass.
4 - Immune responses .5 - Anti-inflammatory actions (Has anti-inflammatory properties, reducing histamine secretion ) .6 - Blood pressure (Increases blood pressure by increasing the sensitivity of the vasculature to epinephrine and norepinephrine; in the absence of cortisol, widespread vasodilation occurs ) .
7 - Heart and blood vessel tone and contraction .8 - Central nervous system activation .9 - Cortisol also reduces calcium absorption in the intestine so it reduces bone formation .10 - It acts as antidiuretic hormone, controlling one-half of intestinal diuresis .11 -There are potential links between cortisol, appetite, and obesity.
12 - Additionally, cortisol enhances the activity of other hormones including glucagon and catecholamines.
Patterns• Cortisol levels normally fluctuate
throughout the day and night in a circadian rhythm that peaks at about 8 AM and reaches it lowest around lowest levels are at about midnight.
• They drop very low in the evening and during the early phase of sleep. But if you sleep during the day and are up at night, this pattern may be reversed.
• If you do not have this daily change (diurnal rhythm) in cortisol levels, you may have overactive adrenal glands. This condition is called Cushing's syndrome.
• While it is vital to health for the adrenals to secret more cortisol in response to stress, it is also very important that bodily functions and cortisol levels return to normal following a stressful event.
• Unfortunately, in our current high-stress culture, the stress response is activated so often that the body does not always have a chance to return to normal.*
• This can lead to health problems resulting from too much circulating cortisol and/or from too little cortisol if the adrenal glands become chronically fatigued (adrenal fatigue).
Binding• Most serum cortisol (all but about 4%) is
bound to proteins, including corticosteroid binding globulin (CBG) and serum albumin. Free cortisol passes easily through cellular membranes, where they bind intracellular cortisol receptors . The "free" is biologically active.
• Free cortisol is excreted into the urine and is present in the saliva.
• The test measures the amount of cortisol in the blood, urine, or saliva.
• Small increases of cortisol have some positive effects:
1 - A quick burst of energy for survival reasons .2 – increases memory functions .3 - A burst of increased immunity .4 - Lower sensitivity to pain .5 -Helps maintain homeostasis in the body
• Higher and more prolonged levels of cortisol in the bloodstream (like those associated with chronic stress) have been shown to have negative effects, such as:
1 - Impaired cognitive performance .2 - Suppressed thyroid function .3 - Blood sugar imbalances such as hyperglycemia .4 - Decreased bone density .
5 - Decrease in muscle tissue .6 - Higher blood pressure .7 - Lowered immunity and inflammatory responses in the body, slowed wound healing, and other health consequences .
8 - Increased abdominal fat, which is associated with a greater amount of health problems than fat deposited in other areas of the body. Some of the health problems associated with increased stomach fat are heart attacks, strokes, the development of metabolic syndrome, higher levels of “bad” cholesterol (LDL) and lower levels of “good” cholesterol (HDL), which can lead to other health problems!
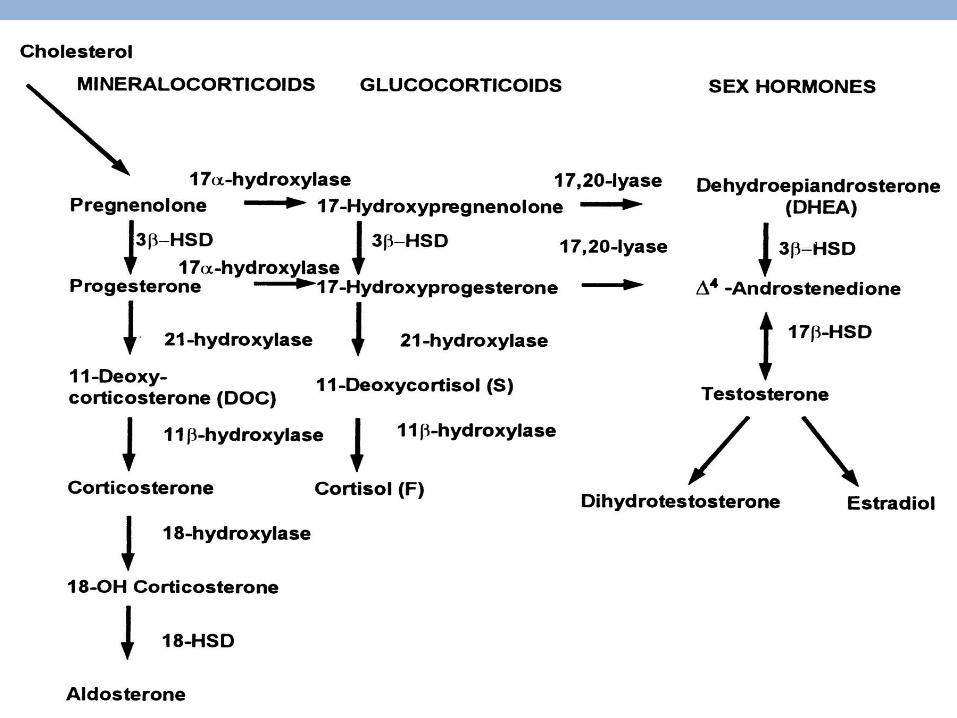
Biosynthesis and Regulation• Cortisol is synthesized from cholesterol ,
Synthesis takes place in zona fasciculata of the adrenal cortex .
• The synthesis of cortisol in the adrenal gland is stimulated by the anterior lobe of the pituitary gland with adrenocorticotropic hormone (ACTH) .
• ACTH production is in turn stimulated by corticotropin-releasing hormone (CRH), which is released by the hypothalamus.
Disorders of cortisol production • Disorders of cortisol production , whether ( increased or decreased ) will cause :• Anxiety .• Depression .• Digestive problems .• Heart disease .• Sleep problems .• Weight gain .• Memory and concentration impairment .
• Hypercortisolism: Excessive levels of cortisol in the blood.
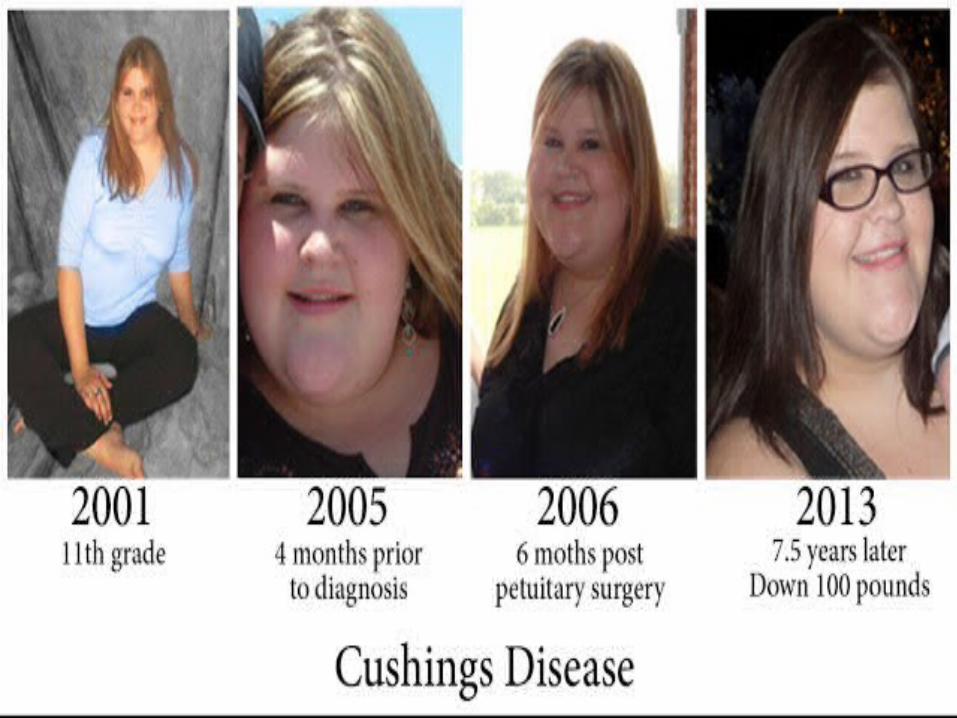
• Cushing's syndrome
• Is a group of signs and symptoms caused by abnormally high levels of cortisol (hypercortisolism).
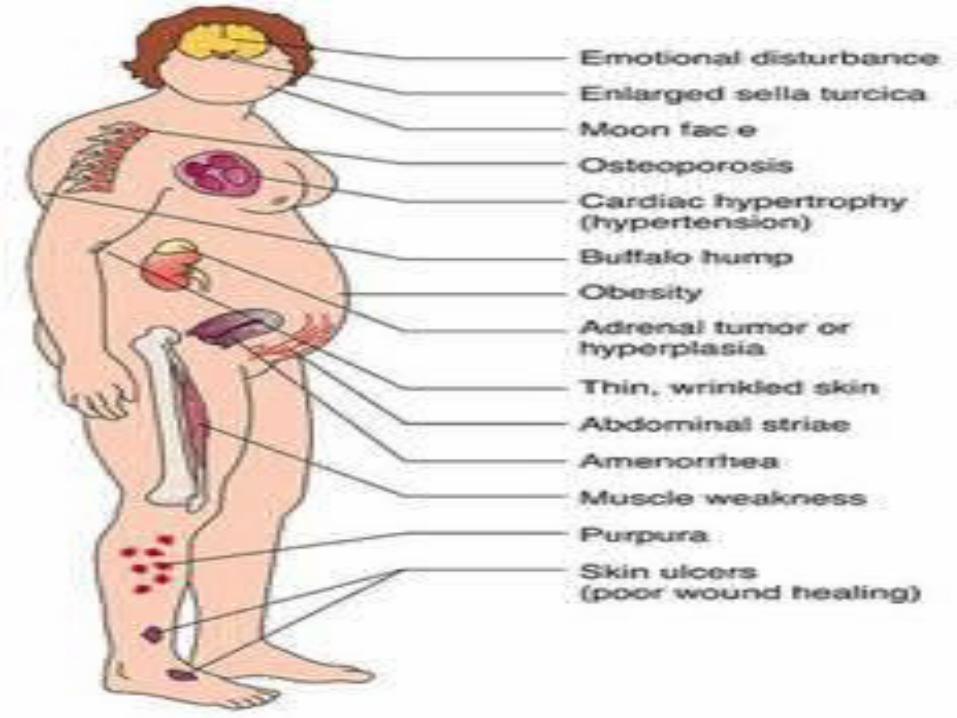
• SIGNS AND SYMPTOMS• Signs and symptoms associated with
Cushing syndrome vary but frequently include:
• Obesity in the trunk (central obesity) with thinner arms and legs .
• A large rounded face (moon face) .• Increased fat in the neck and shoulder
area .
• Thirst and excessive urination .• Visual problems .• Increased susceptibility to infections .• Thin, fragile skin that bruises easily and
heals slowly .• Pinkish streaks that look like stretch
marks on the abdomen, thighs, and buttocks .
• Muscle weakness .
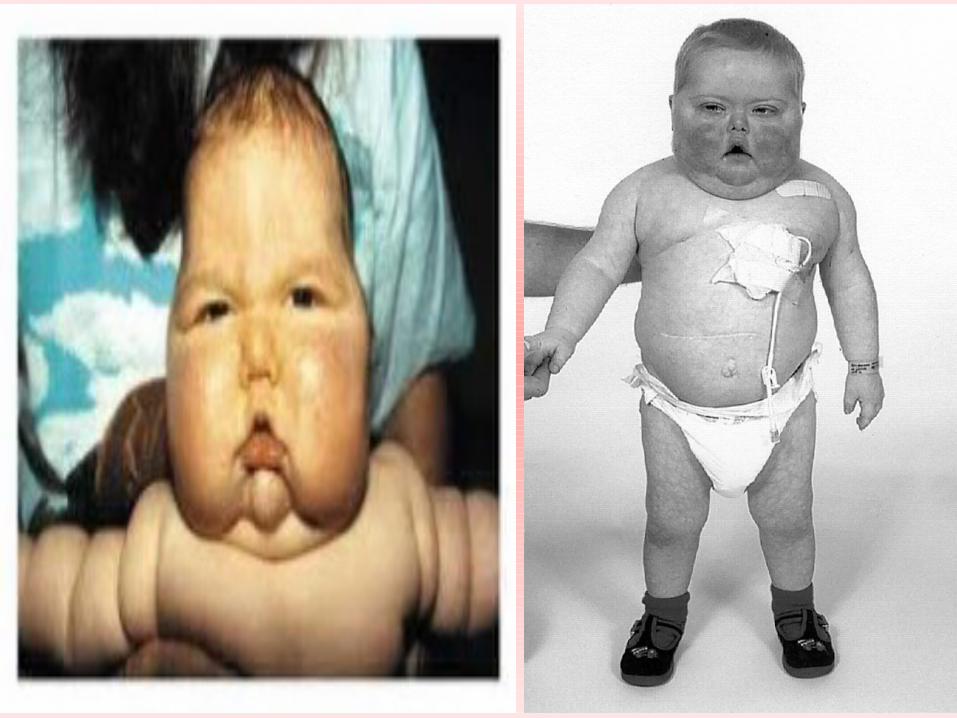
• Decreased endurance .• Osteoporosis .• High blood pressure .• Increased blood sugar .• Headaches, backaches .• Children with Cushing syndrome tend to
be obese, develop slowly, and may remain short.
• Women may have excess hair on their face and chest and menstrual irregularities.
Common causes of Cushing syndrome 1 - Prolonged glucocorticoid therapy (iatrogenic Cushing syndrome) -- a result of taking glucocorticoids-steroid hormones that are chemically similar to natural cortisol, such as anti-inflammatory medications like prednisone prescribed for asthma, rheumatoid arthritis, lupus, and other inflammatory diseases, or after an organ transplant to suppress the immune system and prevent organ rejection.
2 - Cushing disease -- caused by a pituitary gland that produces too much of the hormone ACTH, which then signals the adrenal glands to produce cortisol. • It is caused by a pituitary tumor
(adenoma) that secretes ACTH.3 - An adrenal gland tumor or adrenal hyperplasia can cause the adrenal gland to overproduce cortisol.
4 - A tumor in another part of the body such as the pancreas, lung, or thyroid can produce ACTH (called "ectopic" ACTH production because it is produced somewhere other than the pituitary gland).
Fcats about Cushing syndrome• Cushing syndrome can affect anyone, but
it is most frequently seen in adults between the ages of 20 to 50 years .
• It is 3 times more common in women than men.
• It is estimated that there are two new cases per million people each year.
• LABORATORY TESTS• No single laboratory test is ideal to
diagnose Cushing syndrome and more than one is often used. Since cortisol levels change over the course of a day, a single cortisol result from a blood sample drawn at most times of the day is of little value.
• Testing for Cushing syndrome is typically done in two stages. Initial tests are used to verify that there is excess cortisol present. The second set of tests is used to determine the cause of the increased cortisol: pituitary, adrenal, or other.
• Initial tests to diagnosis Cushing syndrome
• The three most common tests are : 1 - Measurement of midnight plasma cortisol or late-night salivary cortisol . 2 - 24-hour urinary free cortisol test . 3 - The dexamethasone suppression screening test .

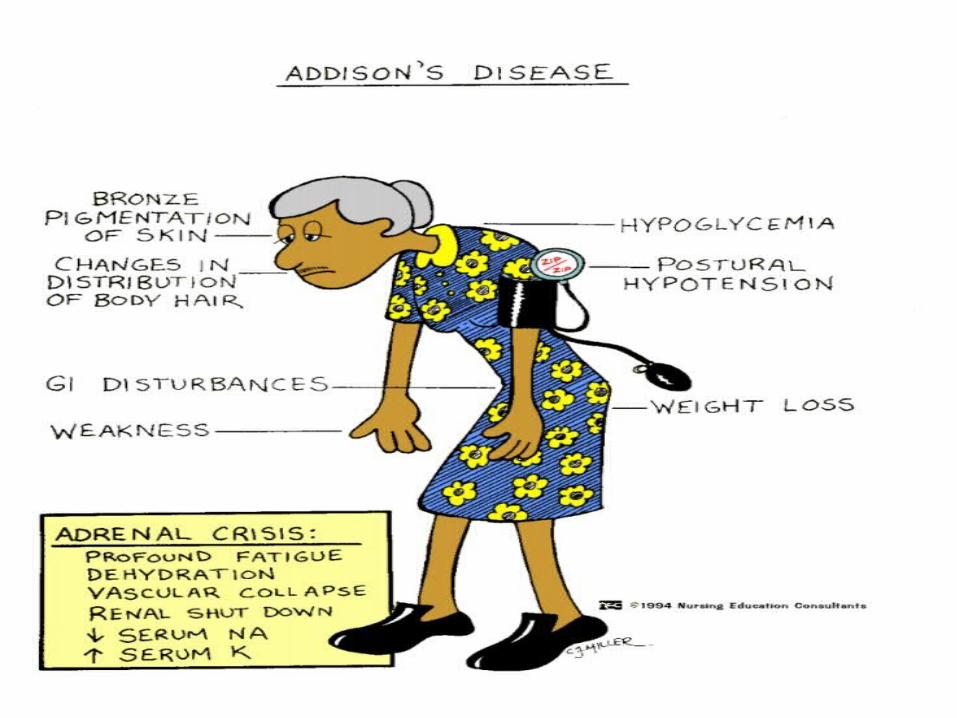
CORTISOL UNDER PRODUCTION• Adrenal Insufficiency and Addison Disease
( HYPOCORTISOLISM )• They are hormonal or endocrine
disorders caused by the body not producing enough of the adrenal hormones cortisol and aldosterone.
• There are two different types of adrenal insufficiency and they depend on whether pituitary gland or adrenal dysfunction underlies hormone deficiencies,they are :
1 - Underactive or damaged adrenal glands cause Addison disease, also known as primary adrenal insufficiency.• They affect cortisol and aldosterone
amounts.
2 - Decrease in the production of the pituitary hormone ACTH is at the root of secondary adrenal insufficiency. • If there is insufficient ACTH, due to
pituitary damage, a pituitary tumor, or some other cause, then cortisol production is not stimulated.
• Secondary adrenal insufficiency can also arise when corticosteroid therapy (such as prednisone, which may be given to relieve inflammation ) ,These treatments suppress natural cortisol production and it can take several weeks or months for normal production to resume.
• Fcats about Cortisol under production• Addison disease is found in people of all
ages and affects both males and females equally.
• Symptoms of insufficiency may not arise until about 80% to 90% of the adrenal cortex has been destroyed.
SIGNS AND SYMPTOMS May include:• Low blood pressure .• Hyponatremia, with Addison disease .• Hypoglycemia .• Hyperkalemia .• Abdominal pain .• Decreased body hair .
• Dehydration, with Addison disease .• Diarrhea or constipation .• Dizziness and fainting .• Fatigue or extreme weakness .• Hyperpigmentation, with Addison disease
- dark spot of skin, especially in the folds of the skin; sometime black freckles on the forehead and face .
• Salt craving, with Addison disease .
• Changes in blood pressure or heart rate .• Muscle weakness .• Vomiting .• Weight loss .
LABORATORY TESTS1 - Cortisol.2 – ACTH .3 – Aldosterone .4 - Electrolytes .

Mineralocorticoid• They are a class of steroid hormones
characterized by their influence on salt and water balances.
• These hormones were involved in the retention of sodium .
• Acutely critical for maintenance of life .�• The primary mineralocorticoid is �
aldosterone.
• Loss of mineralocorticoid activity • Elevated concentration of potassium in �
extracellular fluid . • High urinary excretion of sodium .�• Decreased concentration of sodium in �
extracellular fluid .• Decreased volume of extracellular fluid �
and blood .• Decline of cardiac output and shock .�
• Good news• � All those symptoms can largely be prevented
by .• replacement of salts and mineralocorticoids .
• ALDOSTERONE• Is a steroid hormone produced from
cholesterol by the outer section (zona glomerulosa) of the adrenal cortex in the adrenal gland .
• It plays a central role in the regulation of blood pressure mainly by acting on the distal tubules and collecting ducts of the nephron.
• TRANSPORT• 20% bound to cortisol-binding protein .�• 40% albumin-bound .�• 40% free .�• METABOLISM• Half-life 20 min .�• Liver .�• Free hormone filtered by kidneys .�
• FUNCTION• Increased resorption of sodium, sodium
loss in urine is decreased under aldosterone stimulation.
• Increasing reabsorption of ions and water in the kidney.
• Secretion of potassium.• Increased water retention.• Increased blood pressure.
• THE CELLULAR MECHANISM OF ACTION• Aldosterone stimulates transcription of
the gene encoding the sodium-potassium ATPase, leading to increased numbers of "sodium pumps" in the membranes of tubular cells.
• Aldosterone also stimulates a sodium channel which facilitates uptake of sodium from the tubular lumen.
• Aldosterone has also effects on sweat glands, salivary glands and the colon which are essentially identical to those seen in the distal tubule of the kidney.
• The major net effect is again to conserve body sodium by stimulating its resorption or, in the case of the colon, absorption from the intestinal lumen.
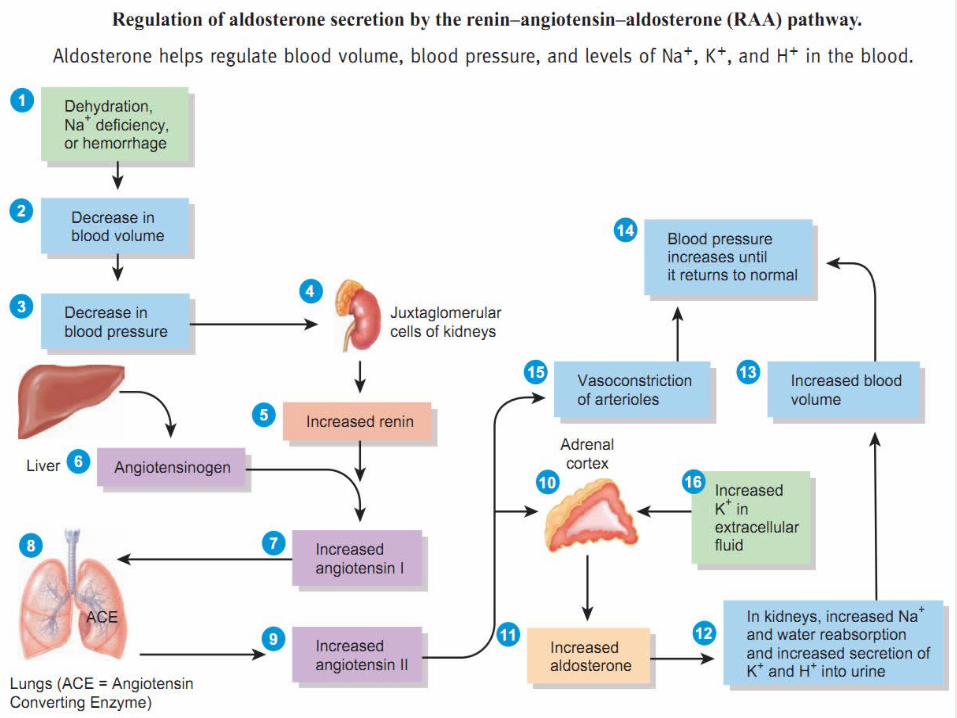
• Control of aldosterone release from the adrenal cortex
1 -The role of the renin-angiotensin system 2 - The plasma concentration of potassium
�3 - ACTH .
� 4 - Atrial Natriuretic Peptide( suppress aldosterone ).
• PATHOPHYSIOLOGY Hyperaldosteronism ( aldosterone
overproduction ) 1 - Primary aldosteronism, also known as ( Conn syndrome )(Conn syndrome) is caused by the overproduction of aldosterone usually by a benign tumor of one of the glands.
• By overactivity of both glands called bilateral adrenal hyperplasia.
• Or for unknown reasons (idiopathic).• Rarely, it is caused by a cancerous
(malignant) adrenal tumor .
The high aldosterone level will CAUSE:increases reabsorption of sodium (salt) .loss of potassium by the kidneys. an electrolyte imbalance .
• Signs and symptoms include • High blood pressure.• Headache. • And muscle weakness, espeically if
potassium levels are very low.Lower than normal blood potassium
(hypokalemia) in someone with hypertension suggests the need to look for aldosteronism.
• In Conn syndrome, aldosterone is produced despite low renin levels.
• Sometimes, to determine whether only one or both adrenal glands are affected, blood may be taken from both of the adrenal veins and testing is done to determine whether there is a difference in the amount of aldosterone (and sometimes cortisol) produced by each of the adrenal glands.
2 - SECONDARY ALDOSTERONISM
which is more common than primary aldosteronism, is caused by anything that leads to excess aldosterone, other than a disorder of the adrenal glands.• It could be caused by any condition that• decreases blood flow to the kidneys.• decreases blood pressure.• or lowers sodium levels.
• Congestive heart failure . • liver Cirrhosis . • Kidney disease .• And toxemia of pregnancy
(preeclampsia) . In these conditions, the cause of aldosteronism is usually obvious .
• The most important cause of seconary aldosteronism is narrowing of the blood vessels that supply the kidney, termed (renal artery stenosis ).
• This causes high blood pressure due to high renin and aldosterone .
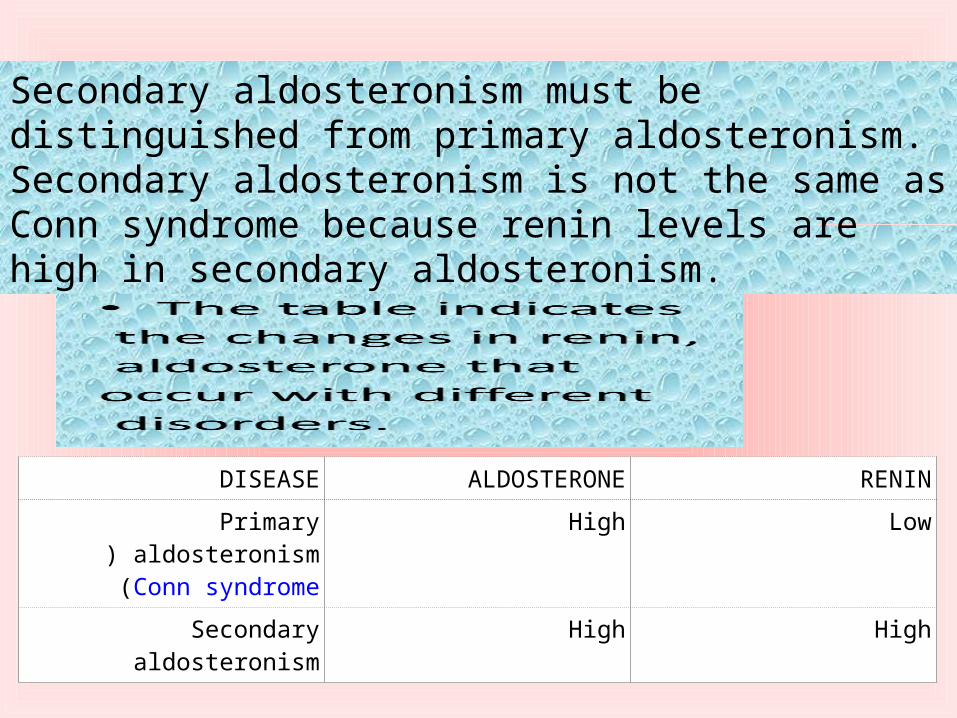
DISEASE ALDOSTERONE RENIN
Primary aldosteronism( Conn syndrome)
High Low
Secondary aldosteronism High High
Secondary aldosteronism must be distinguished from primary aldosteronism. Secondary aldosteronism is not the same as Conn syndrome because renin levels are high in secondary aldosteronism.
• ALDOSTERONE EXCESS• Na+ retention → hypernatremia → EC volume↑↑ �
→BP↑↑• K+ depletion → hypokalemia → damages kidneys �
and also muscle weakness• H+ depletion → alkalosis → plasma Ca++↓ →�muscle cramp
Hypoaldosteronism (Low aldosterone)Usually occurs as part of adrenal
insufficiency; it causes Dehydration. low blood pressure. low blood sodium level. And a high potassium level.
• Is there anything else I should know?• The amount of salt in your diet and
medications, such as over-the-counter pain relievers of the non-steroid class, diuretics, beta blockers, steroids, angiotensin-converting enzyme (ACE) inhibitors, and oral contraceptives can affect the test results. Some of these drugs are used to treat high blood pressure.
• Stress, exercise, and pregnancy can also affect the test results.
• Coffee, tea or cola can affect the 24-hour urine sample test .
• The body's position .• Both aldosterone and renin levels are
highest in the morning and vary throughout the day.
• Aldosterone levels become very low with severe illness, so testing should not be done at times when someone is very ill.
ADRENAL MEDULLA
catecholaminesEpinephrine (adrenaline), and norepinephrine (noradrenaline)
• It is part of the adrenal gland. • It is located at the center of the gland,
being surrounded by the adrenal cortex.• It is consisting of cells that secrete
epinephrine (adrenaline), norepinephrine (noradrenaline), and a small amount of dopamine in response to stimulation by the central nervous system .
• FunctionAdrenal medulla Is the principal site of
the conversion of the amino acid tyrosine into the catecholamines .
The hormone release In response to stressors such as exercise or danger.
medullary cells release catecholamines into the blood in a 15:3 ratio of adrenaline to noradrenaline.
Release of catecholamines is stimulated by nerve impulses, and receptors for catecholamines are widely distributed throughout the body.
Effects of adrenaline and noradrenaline include
# Increased heart rate and blood pressure. #Blood vessel constriction in the skin and gastrointestinal tract.
# Smooth muscle (bronchiole and capillary) dilation. # And increased metabolism, all of which are characteristic of the fight-or-flight response.
• SYNTHESIS OF CATECHOLAMINES Synthesis of catecholamines begins with the amino acid Tyrosine------Dihydroxyphenylalanine------Dopamin----Norepinephrine -------Epinephrine .
• The human adrenal medulla produces and releases about 80% epinephrine and 20% norepinephrine, with a small amount of dopamine.
• While the adrenergic neurons are responsible for the majority of norepinephrine production, the adrenal is the source of essentially all of the epinephrine produced in the body .
• DIRECT EFFECTS OF EPINEPHRINE ON ENERGY METABOLISM
• Epinephrine (and to some extent norepinephrine) has effects in all of the major tissues involved in energy metabolism.
• 1 - In the liver, these hormones stimulate glycogen and lipid breakdown.
• 2 - Epinephrine also stimulates gluconeogenesis.
• The combination of the effects is a large increase in glucose availability, which can lead to hyperglycemia in cases of prolonged stimulation.
• 3 - In skeletal muscle, epinephrine also stimulates glycogen breakdown .
• The effect of epinephrine in muscle is a preparation for the requirement of exercise – without exercise, the increase in glycolysis in muscle is fairly limited.
• 4 - In adipose tissue, epinephrine stimulates lipolysis by increasing the activity of hormone-sensitive lipase.
INDIRECT EFFECTS OF EPINEPHRINE ON METABOLISM
Epinephrine and norepinephrine decrease pancreatic production of insulin . This reduction of insulin secretion may also protectthe pancreas from exhaustion in conditions of chronic stress, by reducing the necessity for insulin production to compete with production of adrenal hormones.
• This is potentially important, because, unlike the adrenal, which responds to increased requirement for its hormones by increasing its ability to produce those hormones, the pancreas has only a limited capacity for increasing insulin secretion rates.
• Adrenal Medulla abnormalities• There are no direct clinical consequences
of adrenal medullary insufficiency.• An adrenal disorder patient’s requires
supplementation with glucocorticoids and mineralocorticoids, but suffers no apparent ill effects from lack of epinephrine.
• The reason for this is unknown.
• It is possible that norepinephrine release from the sympathetic nervous system yields sufficient circulating catecholamine to maintain normal functioning.
• Alternatively, other systems have somewhat similar effects, especially on glucose homeostasis, and these other systems may compensate for lack of epinephrine.
METABOLISM• Most of the metabolism of the
catecholamines occurs in the liver, which contains a number of enzymes.
• Uncontrolled excessively high levels of catecholamines are usually the result of a relatively rare tumor of the chromaffin cells called a pheochromocytoma.
• These tumors may occur in the adrenal.• A pheochromocytoma may release
catecholamines continually .
•