
1-s2.0-0735109795005986-main
6
1264 JACC Vol. 27, No. 5 April 1996:1264-9 In Vitro Flow Experiments for Determination of Optimal Geometry of Total avopulmonary onnection for Surgical Repair of hildren With Functional Single Ventricle SHIVA SHARMA, MD, FACC, SEAN GOUDY, BS,* PETER WALKER, PHD,* SAMIR PANCHAL, MS,* ANN ENSLEY, BS,* KIRK KANTER, MD,t VINCENT TAM, MD, ~ DEREK FYFE, MD, PHD, AJIT YOGANATHAN, PHD* Atlanta, Georgia Objectives. This study sought to evaluate the effect of offsetting cavopulmonary connections at varying pulmonary flow ratios to determine the optimal geometry of the connection. Background. Previous investigators have demonstrated energy conservation within the streamlined contours of the total cavo- pulmonary connection compared with that of the atriopulmonary connection. However their surgical design of connecting the two cavae directly opposite each other may result in high energy losses. Others have introduced a unidirectional connection with some advantages but with concerns about the formation of arteriovenous malformation in the lung excluded from hepatic venous return. Thus an optimal surgical design has not been determined. Methods. In the present models the caval connections were offset through a range of 0.0 to 2.0 diameters by 0.5 superior cava diameter increments. Flow ratios were fixed for superior and inferior cavae and varied for right and left pulmonary arteries as 70:30 60:40 50:50 40:60 and 30:70 to stimulate varying lung resistance. Pressure measurements and flow visualization were done at steady flows of 2 4 and 6 liters/rain to simulate rest and exercise. Results. Our data show that the energy losses at the 0.0- diameter offset were double the losses of the 1.0 and 1.5 diameters which had minimal energy losses. This result was attributable to chaotic patterns seen on flow visualization in the 0.0-diameter offset. Energy savings were more evident at the 50:50 right/left pulmonary artery ratio. Energy losses increased with increased total flow rates. Conclusions. The results strongly suggest the incorporation of caval offsets in future total cavopulmonary connections. J Am CoU Cardiol 1996;27:1264-9 The history of surgical management of patients with a func- tional single ventricle has been characterized by modifications, many of which were done to reduce complications and improve the functional outcome of children (1-3). O ne of the major modifications followed the pioneering work of de Leval et al. (4), who demonstrated that pulsatile valveless cavities like the right atrium and venous connections at sharp angles contrib- uted to energy losses. Concomitantly they developed the total cavopulmonary connection with anastomosis of the inferior and superior cava directly opposite each other on the right pulmonary artery (i.e., with zero offset of cavae from each other). A subsequent study (5) comparing the traditional Fontan atriopulmonary connection with the total cavopulmo- nary connection dem onstrated lower systemic venous pres- From the Children's Heart Center, Emory University School of Medicine; *Cardiovascular Fluid Mechanics Laboratory, Georgia Institute of Technology, School of Chemical Engineering; and tEgleston Children's Hospital at Emory University, Atlanta, Georgia. Sean Goudy was supported by a National Science Foundation Fellowship, Washington, D.C. Manuscript received June 22, 1995; revised manuscript received November 10, 1995, accepted Novem ber 22, 1995. Address for correspondence: Dr. Shiva Sharma, The Children's Heart Center, 2040 Ridgewood Drive NE, Atlanta, Georgia 30322. sures and a lower incidence of atrial arrhythmia in the latter group of patients. The total cavopulmonary connection con- cept was extended further by Laks et al. (6) by development of the unidirectional cavopulmonary connection in which the superior vena cava and inferior vena cava were connected exclusively to the left and right pulmonary arteries, respec- tively, with creation of a fenestration in the inferior channel. The theoretic advantages of this modification were that it provided even lower inferior vena caval pressures and obliga- tory superior vena caval flow to the left lung. It also matched the relatively higher inferior vena caval flow to the larger volume of the right lung. Despite these improvements, concerns remain about both these designs. In the zero-offset design, dissipative energy losses are believed to be high at the site of collision of the caval flows. In the unidirectional connection, hepatic venous blood is completely excluded from the left lung by design. Srivastava et al. (7) reported the developm ent of pulmonary arteriovenous malformation in the lung sequestered from hepatic venous blood in their patients with cavopulmonary connections, un- derscoring the need for hepatic venous perfusion to both lungs. Furtherm ore, the unidirectional design does not allow for variations in pulmonary resistance to adjust pulmonary blood ©1996 by the Am erican College of Cardiology 0735-1097/96/ 15.00 Published by Elsevier Science Inc. SSD I 0735-1097(95)00598-6
-
Upload
diana-brihan -
Category
Documents
-
view
216 -
download
0
Transcript of 1-s2.0-0735109795005986-main

7/24/2019 1-s2.0-0735109795005986-main
http://slidepdf.com/reader/full/1-s20-0735109795005986-main 1/6
1264
JACC Vol . 27, No. 5
Apr i l 1996:1264-9
I n V i t r o F l o w E x p e r i m e n t s f o r D e t e r m i n a t i o n o f O p t i m a l G e o m e t r y o f
To ta l a v o pulm o na ry o nn ec t io n fo r Surg ica l Re pa ir o f h i ldren
W i t h F u n c t i o n a l S i n g l e V e n t r i c l e
S H I V A S H A R M A , M D , F A C C , S E A N G O U D Y , B S ,* P E T E R W A L K E R , P H D ,*
S A M I R P A N C H A L , M S , * A N N E N S L E Y , B S ,* K I R K K A N T E R , M D , t V I N C E N T T A M , M D , ~
D E R E K F Y F E , M D , P H D , A J I T Y O G A N A T H A N , P H D *
Atlanta, Georgia
Objectives.
This s tudy sou ght to eva luate the e f fec t o f o ff se tt ing
c a v o p u l m o n a r y c o n n e c t i o n s a t v a r y i n g p u l m o n a r y f l o w r a t i o s t o
d e t e r m i n e t h e o p t i m a l g e o m e t r y o f t h e c o n n e c t io n .
Background.
P r e v i o u s i n v e s t ig a t o r s h a v e d e m o n s t r a t e d e n e r g y
c o n s e r v a t i o n w i t h i n t h e s t r e a m l i n e d c o n t o u r s o f t h e t o t a l c a v o -
p u l m o n a r y c o n n e c t io n c o m p a r e d w i t h t h a t o f t h e a t r i o p u l m o n a r y
c o n n e c t i o n . H o w e v er t h e i r s u r g i c a l d e s i g n o f c o n n e c ti n g t h e t w o
c a v a e d i r e c t l y o p p o s i t e e a c h o t h e r m a y r e s u l t i n h i g h e n e r g y
l o s s e s . O t h e r s h a v e i n t r o d u c e d a u n i d i r e c t i o n a l c o n n e c t i o n w i t h
s o m e a d v a n t a g e s b u t w i t h c o n c e r n s a b o u t t h e f o r m a t i o n o f
a r t e r i o v e n o u s m a l f o r m a t i o n i n t h e l u n g e x c l u d e d f r o m h e p a t i c
v e n o u s r e tu r n . T h u s a n o p t i m a l s u rg i ca l d e s i g n h a s n o t b e e n
d e t e r m i n e d .
M ethods.
I n t h e p r e s e n t m o d e l s t h e c a va l c o n n e c t i o n s w e r e
of fse t through a range o f 0 .0 to 2 .0 d iameters by 0 .5 super ior cava
d i a m e t e r i n c r e m e n t s . F l o w r a t i o s w e r e f i x e d f o r s u p e r i o r a n d
in fer ior cavae and var ied for right and le f t pu lmo nary ar teries as
70:30 60:40 50:50 40:60 and 30:70 to s t imu la te vary ing lung
r e s i s ta n c e . P r e s s u r e m e a s u r e m e n t s a n d f l o w v i s u a l i z a t io n w e r e
don e a t s teady f lows o f 2 4 and 6 l i ters /ra in to s imula te res t and
exercise.
Results.
O u r d a t a s h o w t h a t t h e e n e r g y l o s s e s a t t h e 0 . 0 -
d i a m e t e r o f f se t w e r e d o u b l e t h e l o s s e s o f t h e 1 . 0 a n d 1 .5 d i a m e t e r s
w h i c h h a d m i n i m a l e n e r g y l o s s e s . T h i s r e s u l t w a s a t tr i bu t ab l e t o
c h a o t i c p a t t e r n s s e e n o n f l o w v i s u a l i z a t i o n i n t h e 0 . 0 - d i a m e t e r
of fse t . Energy sav ings were more ev ident a t the 50 :50 r ight / le f t
p u l m o n a r y a r t e ry r a ti o . E n e r g y l o s s e s i n c r e a s e d w i t h i n c r e a s e d
total f low rates.
Conclusions.
The resu l t s s trong ly sugges t the incorporat ion o f
cava l o ff se ts in fu ture to ta l cavopulm onary connect ion s .
J
Am CoU Car dio l 1996;27:1264-9
Th e h i s to ry o f su rg i ca l m a n a g e m e n t o f p a t ie n t s w i th a fu n c -
t iona l s ing le ventr ic le has bee n ch arac te r ized by modifica tions,
m a n y o f w h ic h w e r e d o n e t o r e d u c e c o m p l ic a t io n s a n d i m p r o v e
th e fu n c t io n a l o u t c o m e o f c h i l d re n (1 -3 ) . O n e o f t h e m a jo r
m o d i f i c a t i o n s fo l l o w e d th e p io n e e r in g w o rk o f d e Le v a l e t a l .
(4) , who demonst ra ted tha t pu lsa t i le va lve less cavi t ies l ike the
r ig h t a t r i u m a n d v e n o u s c o n n e c t io n s a t sh a rp a n g l e s c o n t r i b -
u t e d t o e n e rg y l osses . Co n c o m i t a n t ly t h e y d e v e lo p e d th e t o t a l
c a v o p u lm o n a ry c o n n e c t io n w i th a n a s to m o s i s o f t h e i n fe r io r
a n d su p e r io r c a v a d i r e c t l y o p p o s i t e e a c h o th e r o n t h e r i g h t
p u lm o n a ry a r t e ry ( i . e . , w i th z e ro o f f se t o f c a v a e f ro m e a c h
o th e r ) . A su b se q u e n t s t u d y (5 ) c o m p a r in g t h e t r a d i t i o n a l
Fo n ta n a t r i o p u lm o n a ry c o n n e c t io n w i th t h e t o t a l c a v o p u lm o -
n a ry c o n n e c t io n d e m o n s t r a t e d l o w e r sy s t em ic v e n o u s p re s -
From the Chi ldren 's Hear t Cente r , Emory Univer s i ty School of Medic ine ;
*Cardiovascula r F lu id Mechanics Labora tory, Geo rgia Ins t itute of Technology,
School of Chemica l Engineer ing; and tEgles ton Chi ldren 's Hospi ta l a t Emory
University, Atlanta, Georgia. Sean Goudy was supported by a National Science
Founda t ion Fe l lowship, Washington, D.C.
Manuscr ipt r ece ived Jun e 22, 1995; revised manuscr ipt r ece ived N ovember
10, 1995, accepted No vem ber 22, 1995.
Address for cor respondence : Dr . Shiva Sharma, The Chi ldren 's Hear t
Cente r , 204 0 Ridgewood Dr ive NE, At lanta , Georgia 30322.
su re s a n d a l o w e r i n c id e n c e o f a t r i a l a r rh y th m ia i n t h e l a t t e r
g ro u p o f p a t i e n t s. Th e t o t a l c a v o p u lm o n a ry c o n n e c t io n c o n -
c e p t w a s e x t e n d e d fu r th e r b y La k s e t a l. (6 ) b y d e v e lo p m e n t o f
th e u n id i r e c t i o n a l c a v o p u lm o n a ry c o n n e c t io n i n w h ic h t h e
su p e r io r v e n a c a v a a n d i n fe r io r v e n a c a v a w e re c o n n e c t e d
exc lusive ly to the le f t and r igh t pu lmonary a r te r ies , respec-
t ive ly , wi th c rea t ion of a fenest ra t ion in the infe r ior channe l .
Th e t h e o re t i c a d v a n ta g e s o f th i s m o d i f i c a t i o n w e re t h a t i t
p ro v id e d e v e n l o w e r i n fe r io r v e n a c a v a l p re ssu re s a n d o b l ig a -
to ry su p e r io r v e n a c a va l f lo w to t h e l e f t l u ng . I t a l so m a tc h e d
the re la t ive ly h igher in fe r ior vena cava l f low to the la rger
volume of the r igh t lung .
D e s p i t e t h e s e i m p r o v e m e n t s , c o n c e r n s r e m a i n a b o u t b o t h
these designs. In th e ze ro-offse t design , d iss ipat ive energ y
losses a re be l ieved to b e h igh a t th e s i te of co l li s ion of the cava l
f lo w s . In t h e u n id i r e c ti o n a l c o n n e c t io n , h e p a t i c v e n o u s b lo o d i s
comple te ly exc luded f rom the le f t lung by design . Sr ivastava e t
a l. (7) r e p o r t e d t h e d e v e lo p m e n t o f p u lm o n a ry a r t e r i o v e n o u s
m a l fo rm a t io n i n t h e l u n g se q u e s t e re d f ro m h e p a t i c v e n o u s
b lo o d in t h e i r p a t i e n t s w i th c a v o p u lm o n a ry c o n n e c t io n s , u n -
d e r sc o r in g t h e n e e d fo r h e p a t i c v e n o u s p e r fu s io n t o b o th l u n g s .
Fu r th e rm o re , t h e u n id i r e c ti o n a l d e s ig n d o e s n o t a l l o w fo r
v a r i a t i o n s i n p u lm o n a ry r e s i s t a n c e t o a d ju s t p u lm o n a ry b lo o d
©1996 by the Am er ican Col lege of Cardiology 0735-1097/96/ 15.00
Published by Elsevier Science Inc. SSD I 0735-1097(95)00598-6

7/24/2019 1-s2.0-0735109795005986-main
http://slidepdf.com/reader/full/1-s20-0735109795005986-main 2/6
J A C C V o l. 2 7, N o . 5 S H A R M A E T A L . 265
A p r il 1 9 9 6 :1 2 64 -9 E X P E R I M E N T S F O R F O N T A N O P E R A T I O N O P T I M I Z A T I O N
1 3 . 5 m m
- ml.-Im -
v c
mm TI RP ~ ~ LP mrn
~ I V C
1 3 . 5 m m
Figure 1. Schematicof 1.0-diameter offset model showing dimensions
used. IVC = inferior vena cava; LPA = left pulmo nary artery; RPA =
right pulmon ary artery; SVC = superior ven a cava.
f low between the two lungs. T here fore , whi le a l lowing for
ci rculatory mixing of sys temic venou s re turn, w e s tudied the
effects of varying caval offsets at various right and left pulmo-
nary ar tery f low rat ios (varying pulmonary res is tance) to
de te rmine the op t ima l combina t ion for min imiz ing ene rgy
losses.
e t h o d s
Dete rmin at ion of glass m odel s izes. To obtain real is t ic
s izes of the inferior and su perior vena cavae and r igh t and lef t
pu lmon ary a r t er i e s, an 8-yea r o ld boy wi th a Fontan ope ra t ion
underwent magne t i c re sonance imaging MRI)with a Philips
Medical Sys tems ACS 1.5-tes la scanner. The magnet ic reso-
nance images were then t ra nsferre d to an ISG al legro graphics
works ta t ion for image s egmenta t ion and th ree -d imens iona l
recons t ruc tion . F rom the com pute r recons t ruc t ion , t he s izes o f
in fe r io r and supe r ior vena cavae and r igh t and l e f t pu lmon ary
arter ies were measured.
Exper imen ta l sys tem and condi t ions . F igure 1 represen t s
the configurat ion and dimensions of the 19-ram (1.0-diameter
offset ) mo del th at was ma de of cus tom -crafted Pyrex glass. A11
in le t and ou t l e t duc ts had an inne r d i amete r o f 13 .5 mm and
were -15 cm long. Five models were cons tructed with offsets
of 0.0 mm (0.0-diameter offset ) , 8 mm (0.5-diameter offset ) ,
19 mm (1.0-diameter offset ), 25 m m (1.5-diameter offset ) and
30 m m (2.0-diameter offset ) . f f s e t was defined as the horizo n-
ta l dis tance between the caval midpoints (Fig. 1) . A 2-ram
diame te r ho le was dr il l ed in to each in l e t and ou t l e t condu i t t o
measure the di fferent ia l s ta t ic pressure decrease within the
mode l s . The ho les were used to inse r t f l a t - t i pped me ta l
ca the te rs tha t were connec ted to a p res sure t ransduce r . The
flow rat ios for the superior and inferior cavae were f ixed a t
40:60, respectively, which was used to reflect the higher
superior vena caval f low seen in infants and young chi ldren
(8,9) . The f low rat ios to the r ight and lef t pulmonary ar ter ies
we re var ied as follows: 30:70 , 40:60, 50:50, 60:40 and 70:30.
Pressure measurements were carr ied out a t 2, 4, and 6 l i ters /
min. An aqueo us solut ion of glycerin wi th a me an (+_SD)
kinematic viscosity of 3.5 _+ 0.1 centistokes was used to
repr odu ce the kinem at ic viscosi ty of bloo d. T he viscosi ty was
measured a t a l l s tages of data col lect ion to ensure that i t
r ema ined cons tan t.
By maintaining a cons tant head different ia l between the
supply and dump tanks , s teady f low was produced. We used
three ro t am ete rs to measure the f low: one m easured the to t a l
f low; anothe r mea sured in ferior caval f low; the las t meas ured
the h ighe r f low of e i the r the r igh t o r l e f t pu lmonary a r t ery . A
mul t ip le - range DP 15TL Va l idyne pres sure t ransduce r w i th a
no . 24 d iaphragm was used to m easure the pres sure dec rease
across each mod el , using the inferior vena caval inle t as the
re fe rence po in t fo r each measurem ent . We co l l ec ted da ta for
10 s and averag ed these data to ge t a s ingle mean value for the
s ta t ic pressure decrease .
Flow visualization. To visualize flow through the glass
mod els , neutra l ly buo yant spherical 100-p,m Am berl i te part i -
c les wer e adde d to th e water/glycerin solut ion and i l lum inated
with whi te l ight . The experimental f low condi t ions were the
same as those desc r ibed for p res sure measurement s . The
mot ion of the pa r t i c l e s a s they t rave led th rough the mode l s was
recorded wi th a v ideo camera . F low pa th l ines were ob ta ined
by black-and-white pho tograp hy of the mod els using a 35-mm
cam era with 400-ASA speed f i lm with a shu t ter speed o f 1/15
and 1/30 s .
Data analys is . Afte r col lect ing s ta t ic pressure (Pi,s) a t each
of the condui t measurem ent por t s and the a s soc ia t ed vo lumet -
r ic flow (Qi) , the d ata we re analyzed to calculate the veloci ty
(u) through each of the condui ts and the power losses associ-
a t ed w i th each to t a l cavopulmonary connec t ion conf igura t ion .
Using the veloci ty data and de ns i ty data (p) , the dyna mic
pres sure (Pi,ke) was ca lculate d as follows:
P i , k e =
1/2pu2.
Next , us ing the Bernoui l l i equat ion, both the ra te of kinet ic
energy losses (Eke,loss) and the ra te of p otent ia l energy losses
(Es,loss) w ere calculated:
Es,lo~.,= (Qiv~ P¢c~+Q~c Psvc.s)-(Q,v. P~pa,s+Qlm Plp~.s),
E k e ,, o s s = ( Q i v c . P i v c , k e + Q s v c . P s v c , k e ) - ( Q r p a . P r p a , k e + Q l p a . P t p a , k e ) .
Final ly, summing the separate contr ibut ions of the power
losses (rate of en ergy losses), th e tot al po we r losses (EtotaUoss)
were calculated as fol lows:
Eto ta l , los s = Eke , los s + Es , loss .
A fte r calculating the to tal pow er losses for all cases studied, we
ident i f ied the na dir of the po wer losses a t 2 l i ters /min and used
that q uant i ty as the refere nce value. Th e refere nce value (Xref)
was then u sed to calculate the re la t ive percen t change of a l l the
cases studied:
Change = ( X i - X r e f ) / X r e f X 1 0 0 ° ~ .
7/24/2019 1-s2.0-0735109795005986-main
http://slidepdf.com/reader/full/1-s20-0735109795005986-main 3/6
1 2 6 6 SHA RM A T AL. JACC Vol. 27, No. 5
EXPERIMENTS FOR FONTAN OPERATIONOPTIMIZATION April 1996:1264-9
o
o~
( 3 .
2 . 5
2
1.5
1
0 . 5
0
-0 . 5
--.~ 0.0 Diam eter Of fset KE) I
X 0.0 Diame ter Of fset PE)
.0 D iame ter Of fset PE)
1.0 D iame ter Of fset KE)
I ~ 0 .0 D iame ter Of fset Tota l)
[ • 1.0 Diam eter Offset Total )
, , ; , I , , i i I i i , , [ , , , ¢ I , , , , I , , , , I
7 0 / 3 0 6 0 / 4 0 5 0 / 5 0 4 0 / 6 0 3 0 / 7 0
Flow Split RPNLPA)
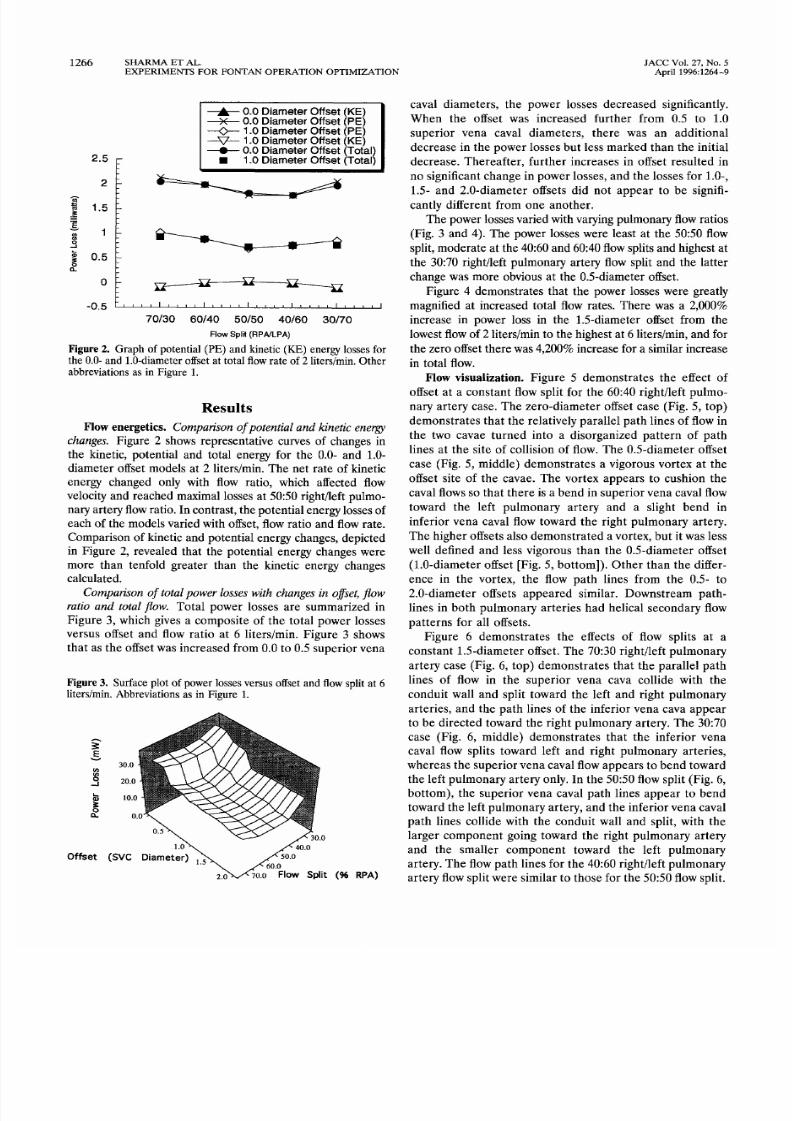
Figure
2. Graph of poten tial (PE) and kine tic (KE) energy osses for
the 0.0- and 1.0-diameteroffsetat total flow ate o f 2 liters/min. Other
abbreviations as in Figu re 1.
R e s u l t s
Flow energet ics Com parison o f potent ial an d k inetic energy
changes .
Figure 2 shows representative curves of changes in
the kinetic, po tentia l and tota l energy for the 0.0- and 1.0-
diameter offset models at 2 liters/min. The net rate of kinetic
energy changed only with flow ratio, which affected flow
velocity and reached maximal losses at 50:50 right/left pulmo-
nary ar tery f low ratio. In con trast , the po tentia l energy losses of
each of the models var ied w ith offset, f low ratio and f low rate .
Com parison of kinetic and poten tia l energy changes, d epicted
in Figure 2, revealed that the p otentia l energy changes were
more than tenfold greater than the kinetic energy changes
calculated.
C om par i son o f t o t a l pow er l os se s w i t h changes i n o f f se t f l ow
rat io and total f low.
Tota l power losses a re summar ized in
Figure 3, which gives a composite of the tota l power losses
versus offset and f low ratio a t 6 l i ters/min. Figure 3 shows
tha t a s the of f se t was inc reased f rom 0 .0 to 0 .5 supe r ior vena
Figure
3. Surfaceplot o f po wer losses versus offsetand flowsplit at 6
liters/rain. Abbreviations as in Figu re 1.
E
30.0
20.0
10.
0
s v c
ffset
i t ( R P A )
caval diameters, the power losses decreased signif icantly.
Wh en the of f se t was inc reased fur the r f rom 0 .5 to 1 .0
super ior vena cava l d iamete r s , the re was an addi t iona l
dec rease in the pow er losses bu t le ss marked than the in i t ia l
dec rease . Therea f te r , fur the r inc reases in of f set r e su l ted in
no sign if icant change in powe r losses, and the losses for 1.0-,
1.5- and 2.0-diameter offsets did not appear to be signif i-
can t ly d i ffe ren t f rom o ne anothe r .
The power losses var ied with varying pulm onary f low ratios
(Fig. 3 and 4). The power losses were least at the 50:50 flow
split, mo dera te at th e 40:60 and 60:40 flow splits and highes t at
the 30:70 r ight/ left pulmonary ar tery f low spli t and the la t ter
chang e was more obvious at th e 0.5-diameter offset.
Figure 4 demonstra tes that the power losses were greatly
magnif ied a t increased tota l f low rates. There w as a 2,000
increase in power loss in the 1.5-diameter offset from the
lowest flow of 2 liters/min to the h ighest at 6 liters/rain, and for
the zero offset there was 4,200 increase fo r a similar increase
in total flow.
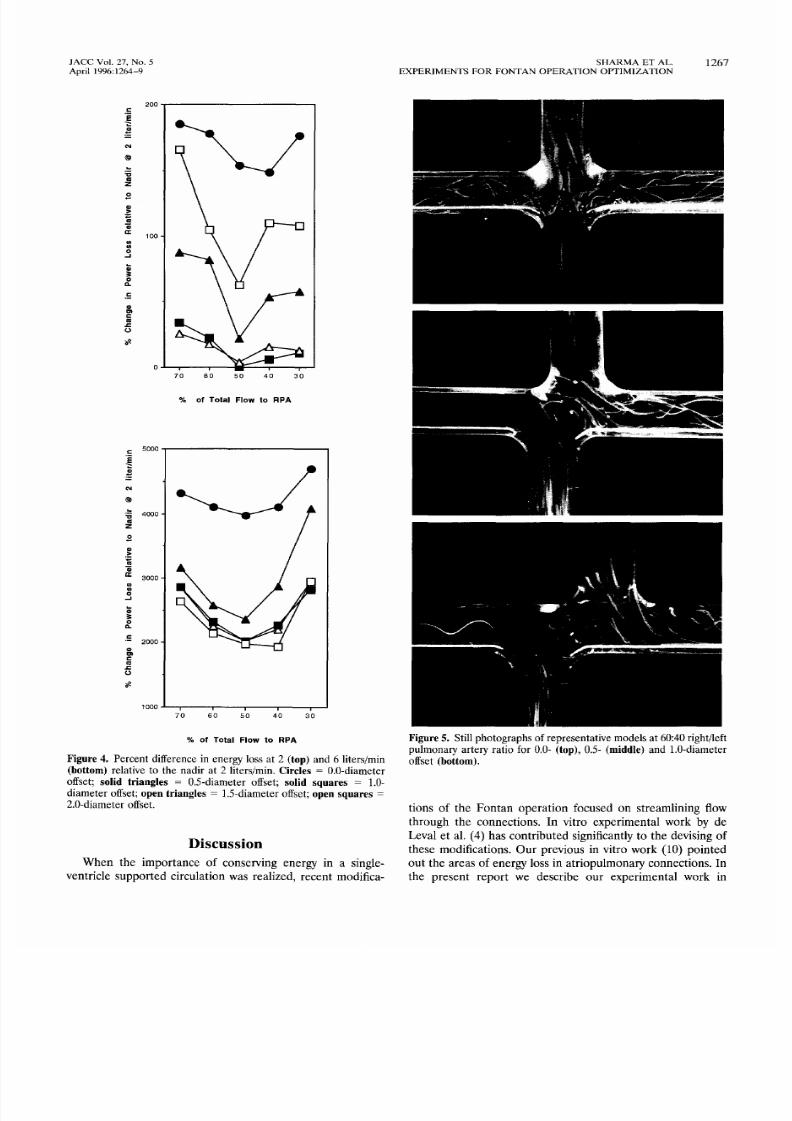
F low visua l iza t ion . F igure 5 demonst ra te s the e f fec t o f
offset a t a co nstan t f low spli t for the 60:40 r ight/ lef t pulmo -
nary ar tery case . The ze ro-d iam eter offset case (Fig. 5, top)
dem onst ra te s tha t the re la tive ly pa ra l le l pa th l ines of flow in
the two cavae turned in to a d isorganized pa t te rn of pa th
lines a t the si te of coll ision of f low. The 0.5-diameter offset
case (Fig. 5, middle) demonstra tes a vigorous vortex a t the
of f se t s i te of the cavae . The vor tex appea rs to cushion the
caval flows so that there is a ben d in sup erior vena caval f low
toward the le f t pu lmonary a r te ry and a s l igh t bend in
infe r ior vena cava l flow toward the r igh t pu lm onary a r te ry .
The h ighe r of f se ts a lso dem onst ra ted a vor tex , bu t i t was le ss
we l l de f ined and le ss v igorous than the 0 .5-d iamete r of f se t
(1.0-diameter offset [Fig. 5, bottom]) . Other than the differ-
ence in the vor tex , the f low pa th l ines f rom the 0 .5- to
2 .0-d iamete r of f se ts appea red s imi la r . Downst ream pa th-
l ines in bo th pu lmon ary a r te r ie s ha d he l ica l secondary flow
patterns for all offsets.
Figure 6 demonstra tes the effects of f low spli ts a t a
cons tan t 1 .5-d iamete r of fse t. The 70:30 r igh t / le f t pu lmonary
a r te ry case (Fig. 6 , top) dem onst ra te s tha t the pa ra l le l pa th
l ines of f low in the supe r ior vena cava co l l ide wi th the
condui t wa l l and sp l i t toward the le f t and r igh t pu lmonary
a r te rie s , and the pa th l ines of the infe r ior vena cava appea r
to be d i rec ted toward the r igh t pu lmo nary a r tery . The 30:70
case (F ig . 6 , middle ) demonst ra te s tha t the infe r ior vena
cava l f low sp l i t s toward le f t and r igh t pu lmonary a r te r ie s ,
whereas the supe r ior vena cava l f low appea rs to b end toward
the lef t pulm on ary ar tery only. In the 50:50 flow split (Fig. 6,
bo t tom) , the supe r ior vena cava l pa th l ines appea r to bend
toward the le f t pu lmona ry a r tery , and th e infe r ior vena cava l
pa th l ines co l lide wi th the c ondui t wa l l and sp li t, w i th the
la rge r component go ing toward the r igh t pu lmonary a r te ry
a n d t h e sma l l e r c o mp o n e n t t o w a r d t h e l e f t p u lmo n a r y
a r te ry . The f low pa th l ines for the 40:60 r igh t / le f t pu lmon ary
artery f low spli t were similar to thos e for t he 50:50 f low split .
7/24/2019 1-s2.0-0735109795005986-main
http://slidepdf.com/reader/full/1-s20-0735109795005986-main 4/6
J A C C V o l . 2 7 N o . 5 S H A R M A E T A L . 267
A p r il 1 9 9 6 :1 2 6 4 -9 E X P E R I M E N T S F O R F O N T A N O P E R A T I O N O P T I M I Z A T I O N
_=
E
o
@
Z
o
a r
3
_=
2 0 0
1 0 0
7 0 8 0 5 0 4 0 3 0
o f T o t a l
Flow to FIPA
0 o o l z
=
Z~~0 4 ]
3 0 0 0
t
2
,=
f_,
1 0 0 0
7JO 6 5 0 4 0 3 0
o f T o t a l F l o w t o R P
Figu re 4. Percent difference in energy loss at 2 top) and 6 liters/min
bottom) relative to the nadir at 2 liters/min. Circles = 0.0-diameter
offset; s o l id t r ian g les = 0.5-diameter offset; solid squares = 1.0-
diameter o ffset;op e n t r ian g les = ] .5-diameter offset; o p e n s q u a r e s =
2.0-diameter offset.
i s c u s s i o n
W h e n t h e i m p o r t a n c e o f c o n s e r v i n g e n e r g y i n a s i n g l e -
v e n t r i c le s u p p o r t e d c i r c u l at i o n w a s r e a l i ze d , r e c e n t m o d i f i c a -
Figure 5. Still photographs o f representative m odels at 60:40 r ight/lef t
pulm onary ar tery ratio for 0.0- top) , 0.5- middle) and 1.0-diameter
offset bottom).
t i o n s o f t h e F o n t a n o p e r a t i o n f o c u s e d o n s t r e a m l i n i n g f l o w
t h r o u g h t h e c o n n e c t i o n s . I n v i t r o e x p e r i m e n t a l w o r k b y d e
Le v a l e t a l. 4 ) h a s c o n t r ib u te d s ig n i f i c a n t ly to th e d e v i s in g o f
t h e s e m o d i f i ca t i o n s . O u r p r e v i o u s in v i t r o w o r k 1 0 ) p o i n t e d
o u t t h e a r e a s o f e n e r g y lo s s i n a t r i o p u l m o n a r y c o n n e c t i o n s . I n
t h e p r e s e n t r e p o r t w e d e s c r i b e o u r e x p e r i m e n t a l w o r k i n

7/24/2019 1-s2.0-0735109795005986-main
http://slidepdf.com/reader/full/1-s20-0735109795005986-main 5/6
1 2 6 8 S H A R M A E T A L . J A C C V o l . 2 7 N o . 5
E X P E R I M E N T S F O R F O N T A N O P E R A T I O N O P T I M I Z A T I O N A p r il 1 9 9 6: 1 26 4 -9
Figure 6. Still photographs of representative right/left pulmon ary
artery flow sp lits at fixed 1.5-diameter offset: 70:30 flow split (top),
30:70 flow split (m iddle) and 50:50 flow split (bottom).
determining the optimal geometry of tota l cavopulmonary
connection that would keep en ergy losses to a m inimum. The
study utilized patient-de rived sizes of glass mo dels an d realistic
f low rates found in children. T he quanti ta t ive portion of ou r
wo rk was sup ported by extensive flow visualization studies.
Relat ion between f low energetics and f low vi sual izat ion
E f f e c t o f o f f s e t
The present s tudy demonst ra ted tha t the
introduction of caval offsets significantly reduced energy con-
sumption within the connections. At the 0.0-diameter offset,
f low visualization demonstra ted that the high energy losses
meas ured were du e to intensely disorganized f low patterns and
secon dary flows. A t th e 0.5-diameter offset, energy losses were
-4 0 lower tha n tha t at the 0.0-diameter offset at 6 liters/min.
This finding is confirmed by the flow visualization, which
revealed that the vortex at the site of the anastomosis at the
0.5-diameter offset effectively cushio ned th e collision o f the
converging caval flows and redu ced th eir interacti on and, thus,
power losses (Fig. 5, top and middle) . Further , a t the 1.0- and
1.5-diameter offset, the energ y losses were -5 0 lower tha n
that at the 0.0-offset at 6 liters/min (Fig. 3). We believe that
significantly lower ene rgy losses were m easu red in the 1.0- and
1.5-diameter offsets because o f furthe r reduc tion in caval flow
interaction. This interaction was stronger for th e 0.5-diameter
case a nd m anifested as a mo re vigorous centra l vortex than the
vortices a t the high er offsets. Fo r this reason, th e 0.5-diameter
offset was n ot as efficient in minimizing energy losses as the 1.0-
or 1.5-diameter offsets.
E f f e c t o f f l o w s p l i t
In addit ion to determining the effect of
offset on p ow er losses, the presen t stud y evalu ated the effect of
variable pulm ona ry flow ratio a nd its effects on pow er losses.
Our results show that the power losses associated with the
respective offsets were lowest when the pulmonary resistance
was equ ally distr ibuted ( i .e ., 50 :50 pulmonary f low ratio, as
explained in the Appendix). In addition, our results show that
at a pulm ona ry resistance equivalent to a 60 :40 and 40:60
right/ left pulmo nary ar tery f low ratio, power losses were com-
parably low for a given model and tota l f low rate a nd were a lso
nearly symmetric (Fig. 4). These experimental results are
consistent with theory (see Appendix).
Surgical applications.
O f f s e t
Although preliminary, our
study has potential surgical applications. The study separated
the caval offsets with th e least energ y losses (1 .0 and 1.5
diame ter) f rom those with re la tively low (0.5 and 2.0 diam eter)
and high losses (0.0 diam eter). These results imply that futu re
surgical designs should definitely have an offset and that the
1.0- or 1.5-diameter offset wou ld be m ore desirable. H owever,
our surgeons (V.T., K.K.) believe that anatomic space con-
straints in som e situations m ay allow a maximal offset of only
0.5 mm in diameter. Our results show that in these situations,
energ y losses would be also lower tha n a t the 0.0-offset case.
P u l m o n a r y f l o w r a t i o
The optimal offsets were found to
main ta in low losses through a rang e o f pulmo nary f low ratios,
with the n adir a t the 50:50 f low ratio. The impo rtance of this
f inding l ies in the fact that m any postoperative patients with a
tota l cavopulmonary connection develop a te lectasis , dia-
phragm paralysis or pleural effusions, which can lead to an
alteration in pulmonary resistance. Because of the bidirec-
t ional option of f low in our proposed design, pulmonary
redistribution can occur without significant energy losses.
T o t a l f lo w
The present experiments w ere don e a t varying
tota l f low rates to simulate the rest and activity cardiac o utpu t

7/24/2019 1-s2.0-0735109795005986-main
http://slidepdf.com/reader/full/1-s20-0735109795005986-main 6/6
JACC Vol. 27, No. 5 SHARM A ET AL. 1269
April 1996:1264-9 EXPERIM ENTS FOR FONTA N OPERAT ION OPTIMIZATIO N
seen in children. Although the differences between the best
and w orst cases for en ergy loss were significant, they were still
relatively sm all at low flow rates of 2 liters/rain. W hen the flow
rate w as increased to 6 liters/rain, these differences increased
20-fold, underscoring the need for offset.
Mixing The experimental models, by vir tue of not being
unidirectional, enab led m ixing of caval flows. In the 30:70,
40:60 and 50:50 f ight/ lef t pulmonary ar tery f low splits , there
was clear visualization of inferior caval flow toward both the
r ight and lef t pulmonary ar ter ies. In the other models, the
central vortex app eared to facilitate mixing. The im portan ce of
mixing l ies in the provision o f hepatic venous blood to both
lungs. It was convincingly dem on strate d by Srivastava et al. 7)
that exclusion of hepatic venous blood from a lung can result
in the deve lopment of pu lmon ary a rte r iovenous ma lformat ion
in that lung. The factors in hepatic venous blood th at prevent
this complication have not been isola ted and therefore cann ot
be quantified. Nevertheless, future surgical designs should
allow at least some mixing to occur, and our experiments
suggest that this mixing can occur at most flow splits and
offsets.
Conclusions. Th e presen t study investigated the effect of
caval offset and varying pulmo nary vascular resistance and
cardiac output on the energy losses associa ted with the tota l
cavopulmo nary connection. These effects were then re la ted to
flow visualization. Fr om these investigations o ur results indi-
cate that an offset should be incorporated into future tota l
cavopulmonary c onn ection designs, and th e ideal offset shou ld
be 1.0 to 1.5 mm in diameter . These offsets consume the least
amount: of en ergy whe n vascular resistance is equally distrib-
uted between both lungs. Furthermore, increases in cardiac
outp ut are associated with increased energy consum ption. Our
future work will investigate the effect of both curvature and
pulsatility on the energy losses associated with the total
cavopulm onary connection.
We acknowledge he secretarial help of Ellen Troutman and Leigh Swisher, The
Children's Heart Center, Atlanta, Georgia.
ppendix
Theoret ical A nalys is
I t can be shown by the Po iseu i l le and Bernou i l l i equa t ions tha t ou r
exper imen ta l re su l t s a re cons is ten t wi th p rev ious ly accep ted theor ies .
The Po iseu i l le equa t ion re la tes the change in s ta t ic p ressu re to the
vo lumetr ic f low ra te :
Q =/3 • APs,
where ]3 = pd4/(128t, AL); APs = change in s ta t ic p ressu re ; d =
d iamete r ; /z = v iscos i ty ; and AL = change in leng th ' , Q = vo lumetr ic
flow rate'. .
F igure 2 o f ou r resu l t s shows the change in k ine t ic and po ten t ia l
energy losses ve rsus f low ra t io fo r severa l rep resen ta t ive cu rves .
M o r e o v e r , F i g u r e 2 s h o w s t h a t t h e m a g n i t u d e o f t h e k i n e t i c p o w e r
l o s s e s a r e m u c h s m a l l e r t h a n t h e m a g n i t u d e o f t h e p o t e n t i a l p o w e r
losses . The k ine t ic and po ten t ia l power losses a re the change in the
dynamic and s ta t ic p ressu res , re spec t ive ly , mul t ip l ied by the vo lum etr ic
f low ra te :
P s , l o s s =
Q x A P s ,
P k e , l o s s =
Q
× A P k e
I f we assum e tha t the dy namic p ressu re i s much sm al le r than th e s ta t ic
p ressu re te rms , we can make the assumpt ion tha t the change in to ta l
p ressu re i s approx imate ly equa l to the change in s ta t ic p ressu re .
AP = APk~ + AP ~,
A P t o t a I -~
AP~.
Fur the rmo re , i f the change in s ta t ic p ressu re i s approx imate ly equa l to
the to ta l p ressu re , we can subs t i tu te the s ta t ic p ressu re in to the
Bernou i l l i equa t ion fo r the change in to ta l p ressu re :
AE = Q
X A P t o t a l ,
AE ~ Q x AP~,
whe re E = to ta l power . F ina l ly , i f we so lve the Po iseu i l le equa t ion fo r
the change in s ta t ic p ressu re and subs t i tu te the resu l tan t equa t ion in to
the Bernou i l l i equa t ion fo r the change in s ta t ic p ressu re , the resu l tan t
equa t ion revea ls tha t the change in power losses a re p ropor t iona l to
t h e s q u a r e o f t h e v o l u m e t r i c f l ow r a t e :
aPs = (l/H) • Q, aXE
~ Q 2 / ~ .
In our sys tem we se t the inpu t energy by se t t ing the inpu t f low ra te fo r
a g iven to ta l f low ( i. e. , the super io r and in fe r io r vena cava l f low ra tes
a re se t a t 40 and 60 o f the to ta l f low, respec t ive ly ) . F ina l ly , u s ing
the p rev ious t runca ted equa t ion , when the energy losses assoc ia ted
wi th eac h o f the respec t ive o f fse ts a re ca lcu la ted , the 50 :50 f low ra t io
consumes le ss energy regard less o f the o f f se t o f the mode ls .
e f e r e n c e s
l. Fon tan F, Baudet E. Surgical repair of tricuspid atresia. Thorax 1971;26:
240-8.
2. Gale AW , Danielson DC, McGoon D C, M air DD. M odified operation for
univentricular heart and complicated congenital lesions. J Thorac C ardio-
vasc Surg 1979;78:831-8.
3. K reutzer G, Galindez E, Bon o H, de Palma C, Laura JP. An operation for
the correc tion of tricuspid atresia . J T horac C ardiovasc Surg 1973;66:613-21.
4. de Leval MR , Kilner P, Gew illigM, B ull C. Total cavopulmonary connec-
tion: a logical alternative to atfiopulmonary connection for com plex Fontan
operations. J Tho rac C ardiovasc Surg 1988;96:682-95.
5. Pearl JM , Laks H, Stein DG, D rinkwater DC, George BL, Williams RG.
Total cavopulmonary anastomosis versus conventional modified Fontan
procedure. A nn Thorac S urg 1991;52:180-96.
6. Laks H, Ardehali A, G rant PW, et al. Modificationof the Fontan procedure:
superior vena cav a to left p ulmonary artery connection and inferior vena
cava to right pulmonary artery connection with adjustable atrial septal
defect. Circula tion 1995;91:2943-7.
7. Srivastava D, Preminger T, Lock JE, et al. Hepatic venous blood and the
developmen t of pulmonary arteriovenous malformations in congenital heart
disease. Circu lation 1995;92:1217-22.
8. G ross GJ, Jonas RA, Castaneda AR, H anley FL, M ayer JE, Bridges ND.
Maturational and hemody namic factors predictive of increased cyanosis
after bidirectionalcavopulmonaryanastom osis. Am J Cardio11994;74:705-9.
9. Salim MA, Di Sessa TG, Reed CM, Ko rones SB, Alpert BS. The contribu-
tion of superior vena cava l flow to total cardiac output in infants: an
echo-Dopp ler study. Clin R es 1992;17:234-41.
10. Kim YH , Walker PG, Fontaine AA , et al. Hemodynam ics of the Fontan
conne ction: an in-v itro study. J B iom ech 1995;117:423-9.


















