WHAT IS NEW IN BILE DUCT CANCER IN THE LAST 12 MONTHS?€¦ · WHAT IS NEW IN BILE DUCT CANCER IN...
40
WHAT IS NEW IN BILE DUCT CANCER IN THE LAST 12 MONTHS? Juan W Valle University of Manchester / The Christie Manchester, UK 21 June 2018
Transcript of WHAT IS NEW IN BILE DUCT CANCER IN THE LAST 12 MONTHS?€¦ · WHAT IS NEW IN BILE DUCT CANCER IN...

WHAT IS NEW IN BILE DUCT CANCER IN THE LAST 12 MONTHS?Juan W ValleUniversity of Manchester / The ChristieManchester, UK21 June 2018

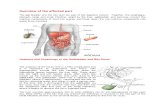
1 Bañales et al Nat Rev Gastroenterol Hepatol 2016;13;261, 2 Hundall & Schaffer Clin Epidemiol 2014 6;99
Cholangiocarcinoma1 Gallbladder cancer2
BILIARY TRACT CANCER | A GLOBAL CHALLENGE

Adjuvant Phase III BCAT study
Advanced disease Phase III FUGA-BT study Randomised phase II: addition of MEKi (BIL-MEK) New promising agents/combinations
Understanding biology and actionable sub-groups International Cancer Genome Consortium Single target and multiple target studies
NEW DATA IN THE PAST 12 MONTHS

ADJUVANTResectable disease

BCAT | BILE DUCT CANCER ADJUVANT TRIAL
Ebata et al Br J Surg 2018; 105: 192–202
Extrahepatic CCA (perihilar and distal CCA)≤10 weeks post-opAge ≥20PS 0-1
225 patients recruited from 48 Japanese hospitals
1o endpoint | OS2o endpoints | RFS, subgroup analysis, toxicity
observation
gemcitabine [6 cycles]
1 : 1
Stratification:R0 vs. R1N0 vs. N1PrimaryCentre
HR 0.85Power 80%Two-sided-α 5%N=300 for 189 eventsInterim analysis (200 patients)

BCAT | BILE DUCT CANCER ADJUVANT TRIAL
Relapse-free survival Overall survival (1o endpoint)
HR 1.01 (95%CI 0.70-1.45; p=0.964)HR 0.93 (95%CI 0.66-1.32; p=0.693)
No subgroup benefitted (N0/1; R0/1)5YS better than anticipated (50% vs 30%)

ADJUVANT CHEMOTHERAPY | RANDOMISED TRIALS
1. Ebata et al Br J Surg 2018; 2. Edeline et al (ASCO-GI) J Clin Oncol 2017;35:suppl 4S: abstr 225; updated ESMO 2017 LBA29; 3. Primrose et al (ASCO 2017) J Clin Oncol 35 (15) 4006
BCAT1
• RFS: HR=0.93 [0.66-1.32], p=0.693• OS: HR= 1.01 [0.70-1.45], p=0.964
BILCAP3
• RFS: HR=0.93 [0.66-1.32], p=0.693• OS: HR= 0.81 [0.63-1.04], p=0.097• OS: HR 0.70 [0.55-0.91], p=0.007*
* pre-planned sensitivity analysis
PRODIGE 122
• RFS: HR=0.88 [0.62-1.25], p=0.47*• OS: HR= 1.08 [0.70-1.66], p=0.74
*co-primary endpoint: QoL

BilCap study | improved overall survival in per-protocol analysis*
*Benefit seen in per-protocol analysis population onlyBenefit seen following sensitivity analysis (LN status, disease grade, gender): HR 0.70 (95% CI 0.55-0.91) p=0.007
ADJUVANT CHEMOTHERAPY RCTs
Primrose et al ASCO 2017; J Clin Oncol 35, suppl; abstr 4006

ADJUVANT CHEMOTHERAPY | SUMMARY OF RANDOMISED TRIALS
Study [clinicaltrials.gov ID]
N Population Arms vs. Status
PRODIGE12 | France[NCT01313377]
190 Cholangio & GB Observation GemOx No benefit
BilCap | UK[NCT00363584]
360 Cholangio & GB Observation Capecitabine Improved survival**pre-specified sensitivity analysis
BCAT| Japan[UMIN000000820]
300 EH-Cholangio Observation Gemcitabine No benefit
ASCOT| Japan[UMIN000011688] JCOG1202
350440 Cholangio & GB Observation S1 Recruiting
ACTICCA-1 | Germany[NCT02170090]
781 Cholangio & GB ObservationCapecitabine CisGem Design revised

DIFFERENCES IN STUDY POPULATIONBCAT1 PRODIGE2 BILCAP3
iCCA (%) - 44 19hCCA (%) 45 8 29dCCA (%) 55 28 35GBC (%) - 20 18
1. Ebata et al Br J Surg 2018; 2. Edeline et al (ASCO-GI) J Clin Oncol 2017;35:suppl 4S: abstr 225; updated ESMO 2017 LBA29; 3. Primrose et al (ASCO 2017) J Clin Oncol 35 (15) 4006

DIFFERENCES IN STUDY POPULATIONBCAT1 PRODIGE2 BILCAP3
iCCA (%) - 44 19hCCA (%) 45 8 29dCCA (%) 55 28 35GBC (%) - 20 18N0 / N1 (%) 65 / 35 63 / 37 47 / 47
(6% unknown)
R0 / R1 (%) 89 / 11 87 / 13 62 / 38
1. Ebata et al Br J Surg 2018; 2. Edeline et al (ASCO-GI) J Clin Oncol 2017;35:suppl 4S: abstr 225; updated ESMO 2017 LBA29; 3. Primrose et al (ASCO 2017) J Clin Oncol 35 (15) 4006

DIFFERENCES IN STUDY POPULATIONBCAT1 PRODIGE2 BILCAP3
iCCA (%) - 44 19hCCA (%) 45 8 29dCCA (%) 55 28 35GBC (%) - 20 18N0 / N1 (%) 65 / 35 63 / 37 47 / 47
(6% unknown)
R0 / R1 (%) 89 / 11 87 / 13 62 / 38Experimental arm 62.3 75.8 52.7Control arm (mo) 63.8 50.8 36.1
1. Ebata et al Br J Surg 2018; 2. Edeline et al (ASCO-GI) J Clin Oncol 2017;35:suppl 4S: abstr 225; updated ESMO 2017 LBA29; 3. Primrose et al (ASCO 2017) J Clin Oncol 35 (15) 4006

Phase II, multi-centre• EHCC or GBCA after radical resection, pT2-4 or N1 or R1
• Gem-Cap (4 cycles, q3w), then CRT 45Gy/25 fractions to LN bed and 54-59 Gy tumour boost + capecitabine as sensitizer
• 79 eligible patients− R0 (n= 54); R1 (n=25)− EHCC 68%; GBCA, 32%− 86% completed, acceptable toxicity− 2-year DFS 52% (met threshold of activity)
Ben-Josef et al J Clin Oncol 2015;33(24)2617
SWOG 0809 STUDY
Inclusion of radiotherapy question – in R1 disease

ADVANCEDNon-resectable and metastatic

1. Valle et al Ann Oncol 2016;27(suppl5):v28-v37; 2. Valle 2010 New Eng J Med
ESMO GUIDELINES1

In Japan: cisplatin & gemcitabine (CisGem) improves survival (over Gem alone)
• BT-22 (n=84): OS 11.2 months 1
• Meta-analysis with ABC-02 (n=493) OS 11.6 months 2
JCOG0805 trial3 (randomized phase II selection study of gemcitabine plus S-1 (GS) vs. S-1):
• GS had improved 1YS 52.90% vs. 40.00%
• Acceptable toxicity profile
• OS 12.5 months
1 Okusaka 2010 Br J Cancer, 2 Valle 2014 Ann Oncol; 3Morizane Cancer Sci 2013;104: 1211–1216
CIS-GEM | ONLY THE “FIRST STEP” ON THE LADDER

Randomized phase III study of gemcitabine plus S-1 combination therapy versus gemcitabine plus cisplatin combination therapy in advanced biliary tract cancer (JCOG1113)
Hepatobiliary and Pancreatic Oncology Group of Japan Clinical Oncology Group (JCOG), Japan
Presented By Makoto Ueno, MD
FUGA-BT
Morizane et al ASCO-GI 2018: abstr 205; Ueno et al ASCO 2018 abstr 4014
GEM:1000 mg/m2 d1, 8 + CDDP: 25 mg/m2
d1, 8; repeated every 3 wks
Cisplatin was administered up to 16 times (total 400 mg/m2), thereafter GEM monotherapy was continued
GEM+CDDP GEM+S1GEM:1000 mg/m2 d1, 8 + S-1: 60, 80, 100 mg/body/day d1-14; repeated every 3 wks
Adjustment factors• Primary tumor (GB vs. others)• History of primary tumor resection (yes/no)• Institution
Recurrent/Unresectable biliary tract cancer (IHBD, EHBD, GB, AV)
Randomisation

Primary analysis| Overall survival
Hepatobiliary and Pancreatic Oncology Group of Japan Clinical Oncology Group (JCOG), Japan
FUGA-BT
GCN=175
GSN=179
%1 year OS(95% CI)
58.3%(50.6%-65.2%)
59.2%(51.6%-66.0%)
Median OS(95% CI)
13.4 months(12.4-15.5)
15.1 months(12.2-16.4)
HR✝): 0.945, 90% CI 0.777-1.149p for non-inferiority = 0.0459 < 0.05
Morizane et al ASCO-GI 2018: abstr 205; Ueno et al ASCO 2018 abstr 4014

Exploratory subgroup analysis
Hepatobiliary and Pancreatic Oncology Group of Japan Clinical Oncology Group (JCOG), Japan
FUGA-BT
Morizane et al ASCO-GI 2018: abstr 205; Ueno et al ASCO 2018 abstr 4014

GC/GS• Primary endpoint
Median OS: 13.4 /15.1 months HR 0.945 (90% CI: 0.777-1.149), p=0.0459
• Secondary endpoint Median PFS: 5.8 / 6.8 months RR: 32.4 / 29.8% AE: Both regimens are tolerable Clinically significant AE: 35.1 / 29.9% SAE: TRD 3 / 0 %Planned dose: GEM:75.7% / CDDP:76.7%
GEM:76.2% / S-1:75.3%• Hydration GC require, GS not require GS convenient
GS betterGC better
GS betterGS better
Primary Metnon-inferiority demonstrated
Comparable
Comparable
FUGA-BT
Gem-S1 is non-inferior to Cis/Gem in Japanese patients
Authors’Summary
Morizane et al ASCO-GI 2018: abstr 205; Ueno et al ASCO 2018 abstr 4014

BIL-MEK STUDY | BACKGROUND
BTC frequently demonstrates upregulation of RAS/RAF/MEK/ERK pathway
Selumetinib (ARRY-142886, AZD6244) is an oral inhibitor of MEK1/2
Selumetinib exhibited synergistic preclinical activity with gemcitabine (used sequentially)
A phase II trial of selumetinib in advanced BTC demonstrated safety at a dose of 100mg BID, with 12% response rate1
A phase 1b study of CisGem with selumetinib recommended a phase 2 dose of 75mg BID (ABC-04) 2
1. Bekai-Saab, et al. JCO 2011; 2. Bridgewater, et al. BMC Cancer 2016

BIL-MEK STUDY | SCHEMA
**Selumetinib dose was reduced from 75 mg to 50 mg BID March 2016 by protocol amendment
Doherty et al ASCO 2018

Arm AContinuous Selumetinib + CisGem
Arm BSequential Selumetinib + CisGem
Arm CCisGem Alone
Median change at 10 wk-12.4%
ORR 35.7%
Median change at 10 wk-15%
ORR 33.3%
Median change at 10 wk-11.6%
ORR 29.4%
Kruskal-Wallis p=0.73
% c
hang
e in
mea
sura
ble
tum
or a
t 10
wee
ks
* Denotes patients non-evaluable due to lack of 10 week study imaging
Primary Endpoint: Median % change in measurable disease at 10 weeks
BIL-MEK STUDY | EFFICACY
Doherty et al ASCO 2018

Secondary Endpoints: PFS, OS
BIL-MEK STUDY | EFFICACY
Doherty et al ASCO 2018

1 Blagden et al J Clin Oncol 33, 2015 (suppl; abstr 2547); 2 ClinicalTrials.gov | NCT02351765
first-in-class nucleotide analogue hENT1 independent transportno metabolism by cytidine deaminase (reduced toxic metabolites) achieves higher intracellular levels of dFdCTP than gemcitabine1
Phase IB study | acelarin and cisplatin in BTChENT1, human equilibrative nucleoside transporter-1; CDA,
cytidine deaminase; dCK, deoxycytidine kinase; dFdC,
gemcitabine; dFdU, ifluorodeoxyuridine
DEVELOPMENTS IN CHEMOTHERAPYAcelarin
Acelarin | ABC-08 study2

1 ClinicalTrials.gov | NCT02351765; 2 McNamara et al ASCO-GI 2018 (abstr TPS544)
DEVELOPMENTS IN CHEMOTHERAPYABC-081
NUC-1031 at 625 mg/m2 + cisplatin at 25 mg/m2 is an attractive and effective combination for treatment of patients with advanced/metastatic biliary tract cancer

Gem/Cis/nab-paclitaxel1
[NCT02392637]USA (MDA and Mayo)Single-arm, phase II; n=61
GCN regimen
1Shroff et al ASCO 2017 J Clin Oncol 35, 2017 (suppl; abstr 4018); 2 Shroff et al ASCO-GI 2018 (abstr 350)
Schedule | gemcitabine 800mg/m2 + cisplatin 25 mg/m2 + nab-paclitaxel 100 mg/m2 ; D1,8 q21d
Promising early data1
- median PFS (1o endpoint): 11.8 months- response rate: 28.8%- median OS: 18.8 months
DEVELOPMENTS IN CHEMOTHERAPY
Updated analysis2
- median PFS: 11.4 months (95% CI: 6.1-16.1)- response rate: 39%.- median OS: 19.2 months (95%CI: 13.6-NA) Phase III study
planned (vs. CisGem)

UNDERSTANDING BIOLOGY AND ACTIONABLE SUB-GROUPS

IMPROVING OUR UNDERSTANDING OF THE GENETIC ENVIRONMENT OF BTC
Intrahepatic cholangiocarcinoma CCA has a different profile to extrahepatic CCA or GBC 1,2
Opisthorchis viverrini (liver-fluke)*-associated CCA (TP53 mutations) is different from non-liver fluke associated CCA (BAP1, IDH1 and IDH2 mutations)3
Inflammatory subclass is different from proliferative subclass4
Table adapted from 1
1Ross (ASCO GI) J Clin Oncol 33, 2015 (suppl 3; abstr 231); 2Borger 2011 Oncologist 17(1):72; 3Chan-on 2013 Nat Genet 45(12):1474; 4Sia 2015 Nat Commun 6:6087

Up to 70% of IH-CCA patients have an actionable mutation1
IDH-1 mutations and FGFR fusion rearrangements have emerged as potential therapeutic targets
IMPROVING OUR UNDERSTANDING OF THE GENETIC ENVIRONMENT OF BTC
1 Sia 2015 Nat Commun 6:6087

IMPROVING OUR UNDERSTANDING OF THE GENETIC ENVIRONMENT OF BTC
1 Jasakul et al Cancer Discov 2017;7(10); 1116–35

IMPROVING OUR UNDERSTANDING OF THE GENETIC ENVIRONMENT OF BTC
1 Jasakul et al Cancer Discov 2017;7(10); 1116–35

IDH-1 MUTATION IS DRUGGABLE
Phase I study: cholangiocarcinoma (CCA), chondrosarcoma, glioma, others [NCT02073994]
CCA cohort1: n=73 [dose escalation (n=24); dose-expansion 500 mg QD (n=49)]
No DLTs; drug-related AEs: fatigue, nausea, diarrhoea, vomiting
Activity: median PFS 3.8 months6-month PFS: 38.5%12-month PFS: 20.7%RR 5% (4 PRs)OS data not mature
1 Lowery et al ASCO 2017 J Clin Oncol 35, 2017 (suppl; abstr 4015); 2 Lowery et al ASCO2017 J Clin Oncol 35 (suppl; abstr TPS4142)
AG-120 is a first-in-class, potent, oral inhibitor of the mutant IDH1 enzyme
n=186
2:1R
AG-120n=124
Placebon=62
Cross-over to AG-120
on disease progression
Phase III study, second-line, placebo-controlled (ClarIDHy) [NCT02989857]

FGFR AS A POTENTIAL TARGET IN INTRAHEPATIC CHOLANGIOCARCINOMA
Fibroblast Growth Factor Receptor
Turner & Gross 2010 Nat Rev Cancer

BJG398 Phase II trial
Javle et al J Clin Oncol 2017 [Nov 28, Epub ahead of print]
BGJ398 125 mg dailyDays 1-21, every 28 days
Treatment until disease progression, unacceptable toxicity, withdrawal of informed consent, or death
Key inclusion criteria• Advanced or metastatic CC• FGFR2 fusion or other genetic alterations in FGFR• Progression following prior cytotoxic therapy
Primary endpoint | RR (RECIST v1.1)Secondary endpoints | PFS, OS, best overall response (BOR), disease control rate (DCR), safety, and pharmacokinetics.
• 47 patients treated
• Majority of patients had ≥2 prior therapies and 11% had at ≥ 4 prior regimens
• FGFR2 fusions/rearrangements were present in 38 patients
• Other FGFR genetic alterations were present in 9 patients;− FGFR2 mutations (n=3) − FGFR2 amplifications (n=4) − FGFR3 amplifications (n=2)
TARGETING FGFR IN THE CLINIC

BJG398 Phase II trialMedian duration of exposure was 188 days (6.2 months)
**All 8 patients with a partial response had an FGFR2 fusion**
Javle et al J Clin Oncol 2017 [Nov 28, Epub ahead of print]
TARGETING FGFR IN THE CLINIC

MOSCATO study | 1035 patients≥1 prior systemic treatmentECOG PS 0-1At least one tumour site accessible to biopsy
Multiple high-throughputmolecular analysis BTC n=43 Evaluable n=34 Druggable alteration n=23 Treated n=18
Verlingue et al Eur J Cancer 2017;87:122e130
MOSCATO STUDY
ORR 33%DCR 88%Median OS 17 mo vs. 5 mo, [HR 0.29; 95% CI, 0.11-0.76; p< 0.008).

Valle et al Cancer Discovery Cancer Discov; 2017;7(9); 943–62.
TARGETS UNDER EVALUATION

Adjuvant Phase III BCAT study – no benefit from adjuvant gemcitabine
Advanced disease Phase III FUGA-BT study – gem/S1 a new option for Japanese patients Randomised phase II (BIL-MEK) – no benefit from adding selumetinib to CisGem New promising agents/combinations – acelarin; gem/nab-pac/cisplatin (early days)
Understanding biology and actionable sub-groups International Cancer Genome Consortium – improved understanding of landscape Single target and multiple target studies – exciting times ahead: targeted therapies,
umbrella studies
NEW DATA IN THE PAST 12 MONTHS | SUMMARY

THANK YOU