OPEN COMMON BILE DUCT EXPLORATION
51
CBD EXPLORATION DR.MATHISEKARAN.T
description
open CBD Exploration -a powerpoint presentation
Transcript of OPEN COMMON BILE DUCT EXPLORATION
CBD EXPLORATION
DR.MATHISEKARAN.T
Early years: Open CBD exploration & Introduction of endoscopic sphincterotomy
• 1889, 1st CBD exploration by Ludwig Courvoisier, a Swiss surgeon – Kocherization of duodenum and short longitudinal
choledochotomy– Stones removed with palpation, irrigation with flexible
catheters, forceps, – Completion with T-tube drainage– For many years, this was the standard treatment for
cholecystocholedocholithiasis
• 1970s, endoscopic sphincterotomy (ES)– Gained wide acceptance as good, less invasive,
effective alternative– In patients with CBD stones who have previously
undergone cholecystectomy, ES is the method of choice
OPERATIVE TECHNIQUES
TYPES:
Right subcostal
Midline
Transverse (cosmetic advantage)
Surgeon stands on right side in subcostal and transverse incision
Left side in midline incision
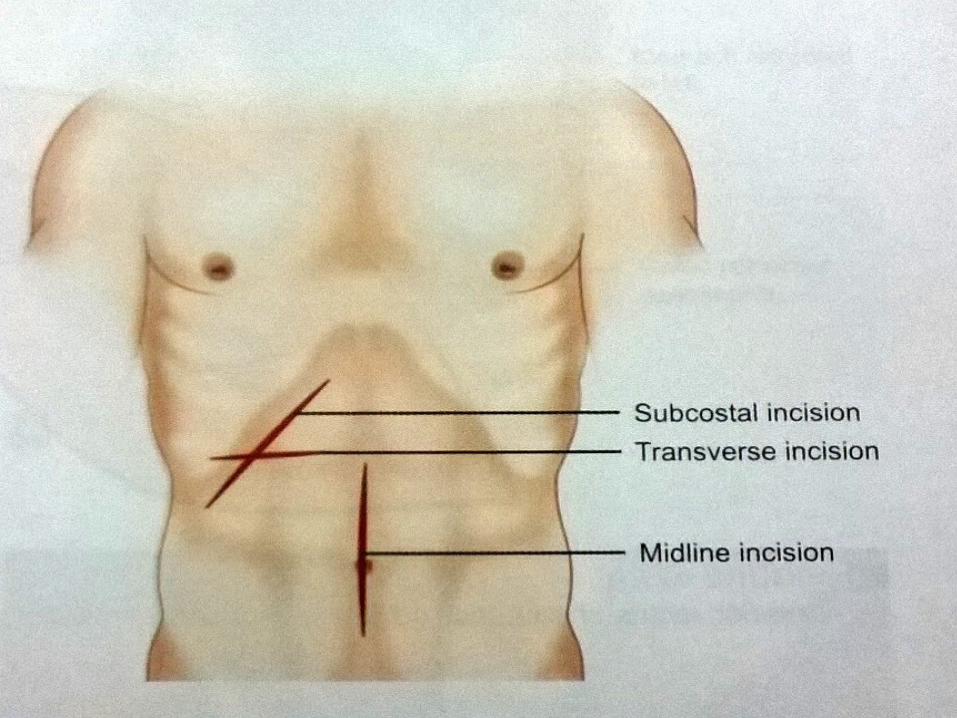
Subcostal incision
4cm below and parallel to the right costal margin and usually extends from close to the midline to tip of ninth costal cartilage.
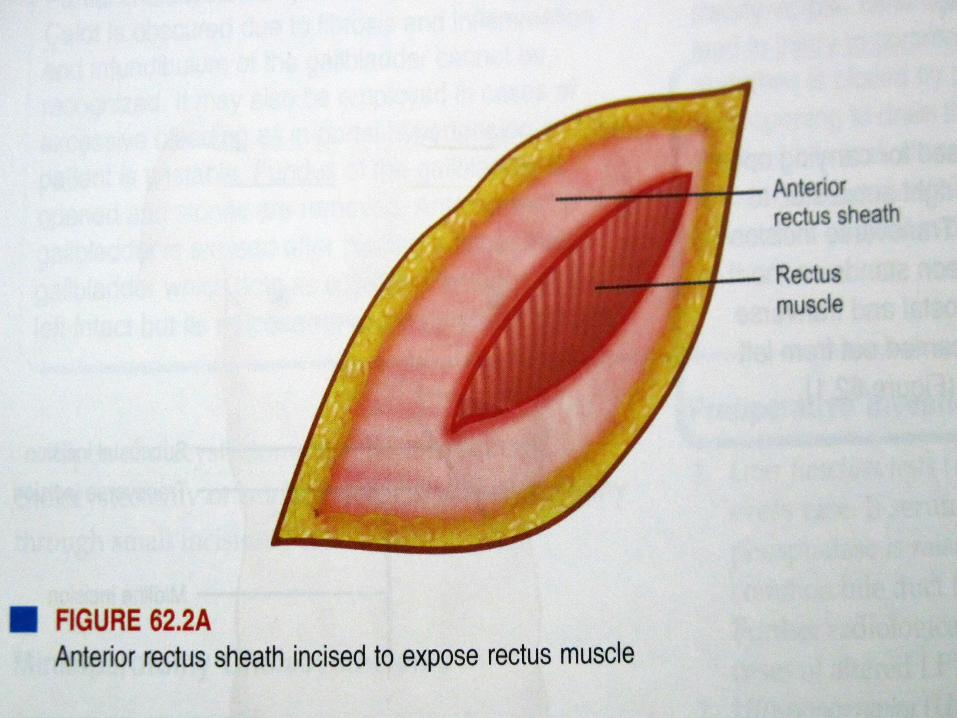
Once skin and subcutaneous tissue incised, anterior rectus sheath and muscle is divided with a diathermy
Robert’s or Mayo’s forceps can be passed behind the muscle to coagulation or ligation of vessels
Subcostal incision
Peritoneum is next opened with a knife between forceps.
Incision can be lengthened with scissors or diathermy.
Muscle layers can be divided laterally with diathermy taking care to avoid damaging the ninth intercostal nerve.

EXPLORATION
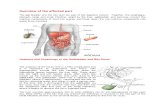
• ATTENTION: To rule out unsuspected pathology – Esophageal hiatus– Stomach– Duodenum– Liver – Gall bladder– Small bowel and colon
SURGICAL INSIGHT
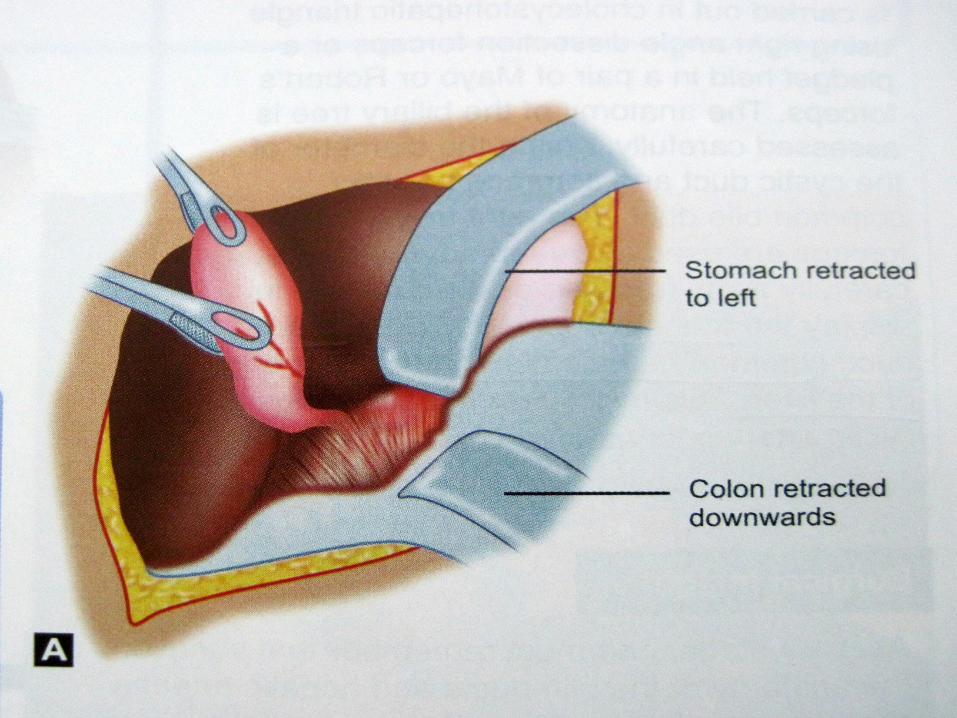
• Two moist packs inserted – First pack retracts the colon downwards – Second pack to retract duodenum,stomach
and free edges of lesser omentum to left.
Deaver’s retracter to retract liver upwards after placing a pack between retracter and liver.

SURGICAL INSIGHT
• The right hand is passed between liver and diaphragm to break the vaccuum and introduce air liver descends into wound
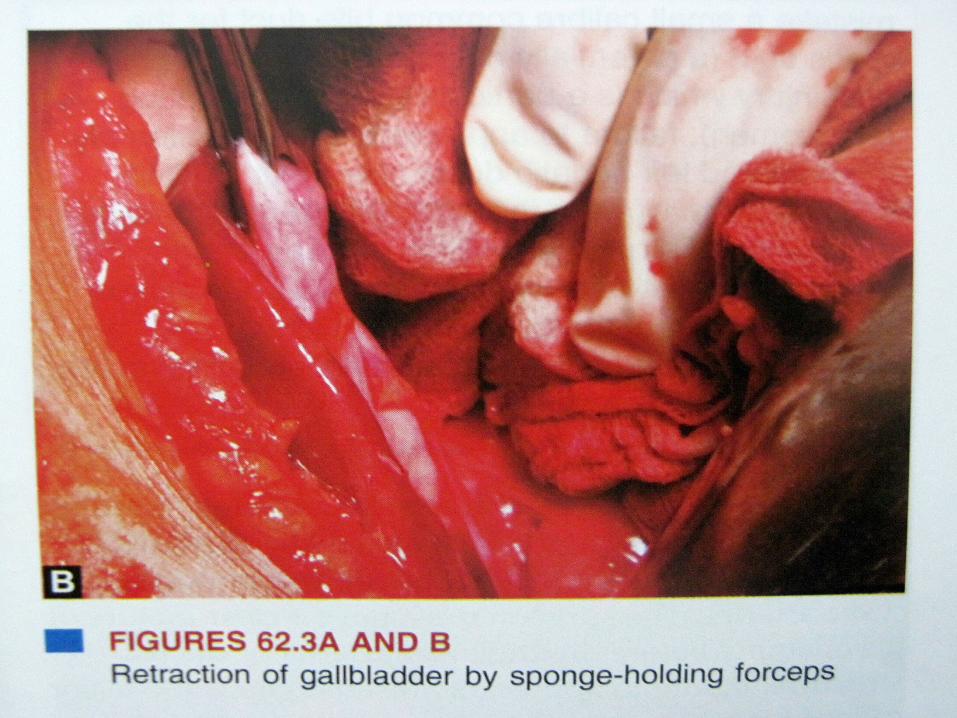
• Gall bladder is grasped with two pairs of sponge –holding forcepsone pair to fundussecond to Hartmann’s pouch
• Gallbladder is retracted downwards and laterally
• Adherent structure dissected with scissors carefully to avoid damage to hepatic flexure or colon or duodenum.
SURGICAL INSIGHT
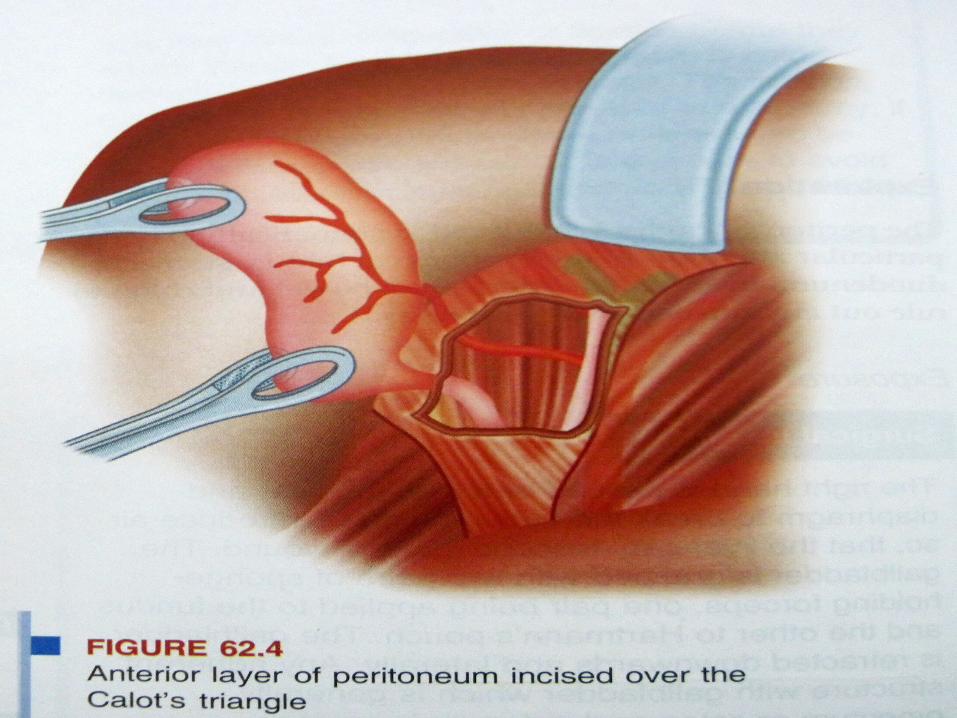
• The anterior layer of peritoneum overlying hepatoduodenal lig is incised near the region of neck of gallbladder using dissecting scissors
• Dissection is carried out in cholecystohepatic triangle right angled dissection forceps/pledget held in a pair of Mayo or Robert’s forceps
• Anatomy of biliary tree is assessed for cystic/hepatic and CBD diameter
SURGICAL INSIGHT
• A right angled dissection forceps is used to sweep adventitial tissues away from cystic duct
• Callot’s triangle is visualized which brings the cystic artery in view.
• One must remember the variations in biliary anatomy
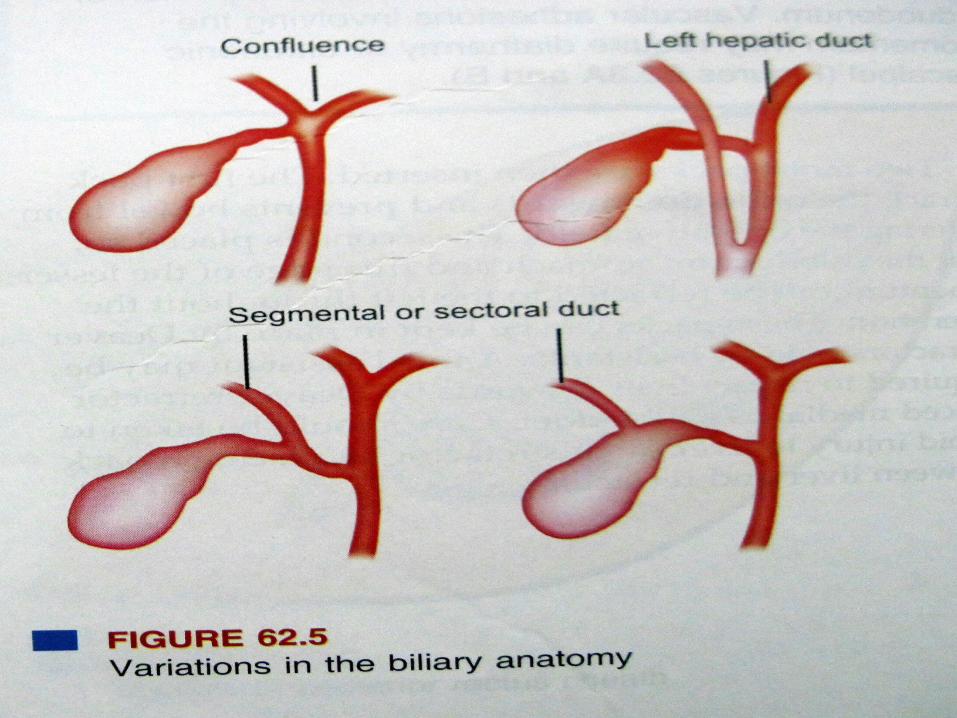
PITFALLS• Mistake a small caliber CBD for cystic duct• Failure to appreciate a low junction of right and
left hepatic ducts• The junction of RT and LT hepatic duct may be
mistaken for the junction of cystic and common hepatic duct
• Failure to appreciate that the cystic duct is absent or very short.
• Right hepatic artery swings far to the right before giving of short cystic artery or multiple cystic artery
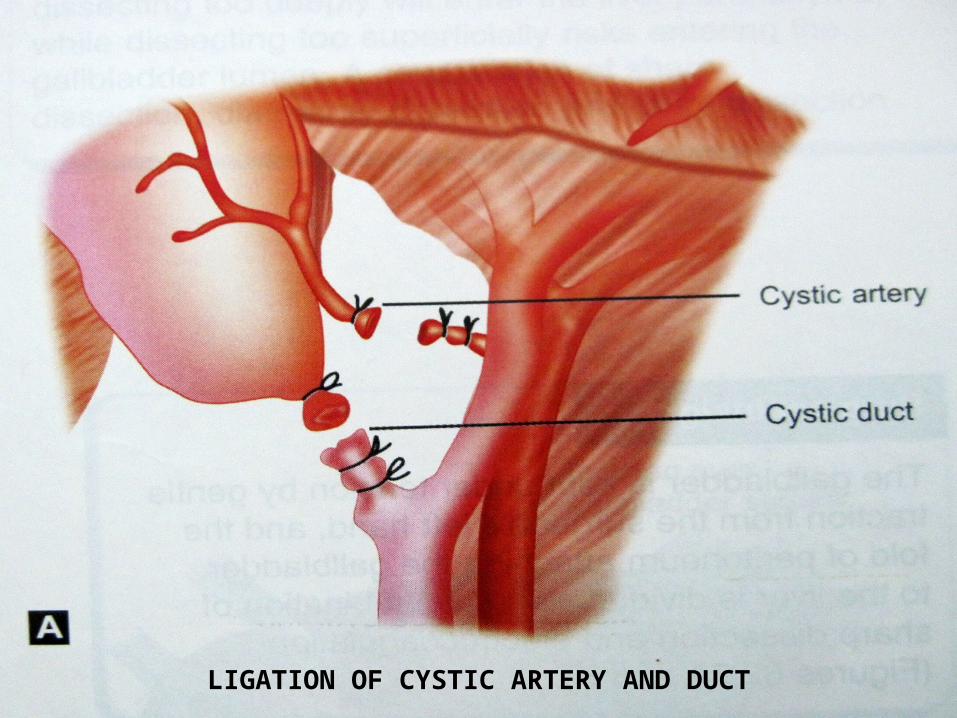
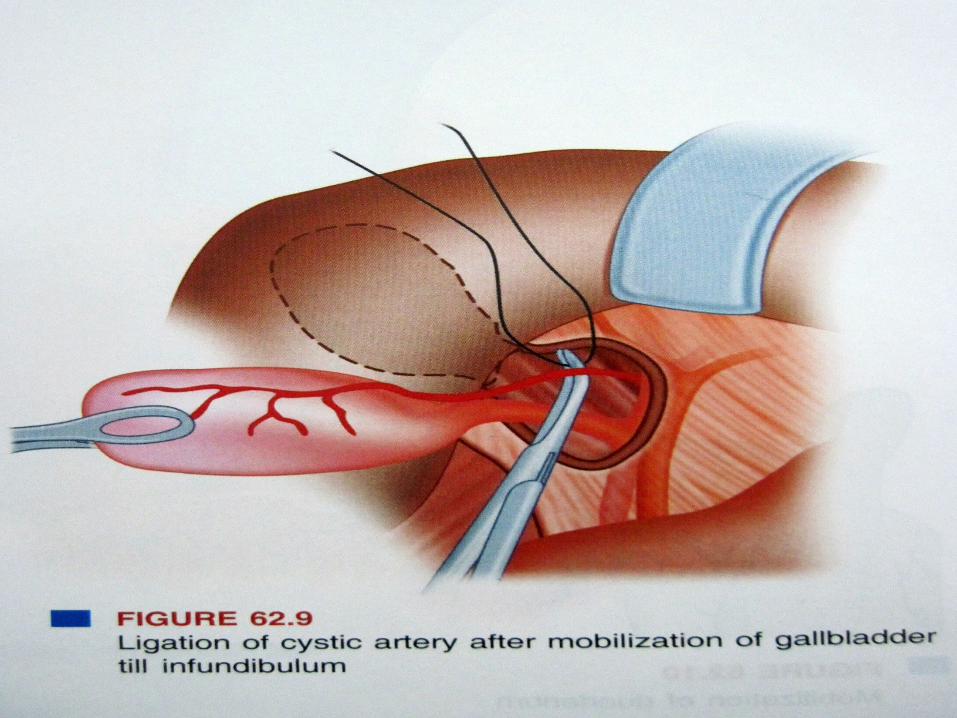
LIGATION OF CYSTIC ARTERY AND DUCT
SURGICAL INSIGHT
• Cystic duct securely tied with polyglactin or silk suture.
• Two suture on CBD side and one on gallbladder side
• The cystic artery also doubly ligated and both sturctures are divided.
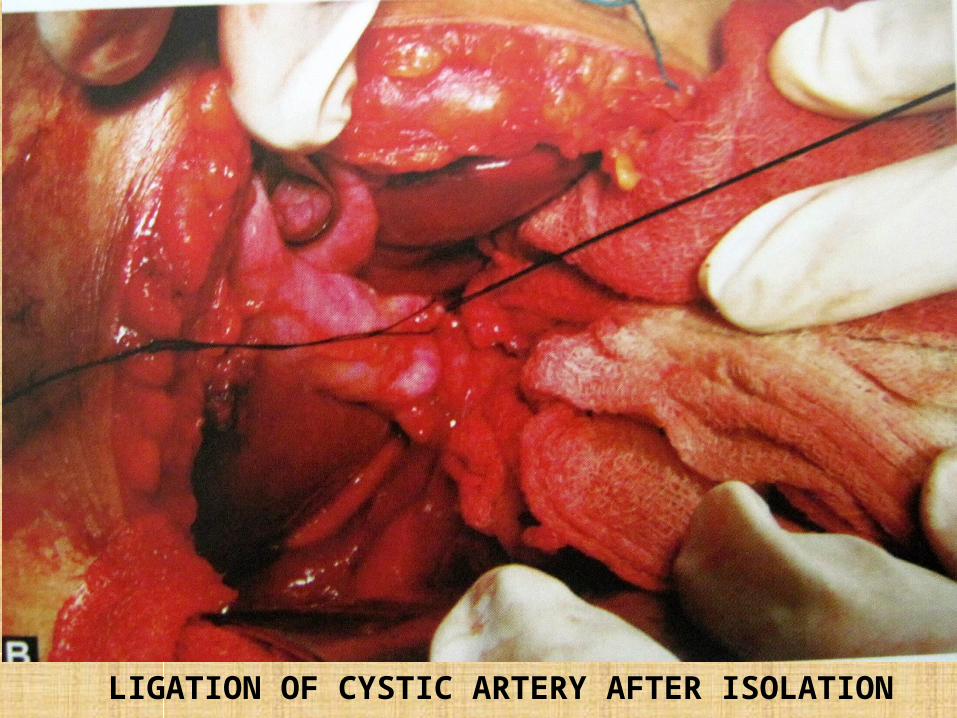
LIGATION OF CYSTIC ARTERY AFTER ISOLATION
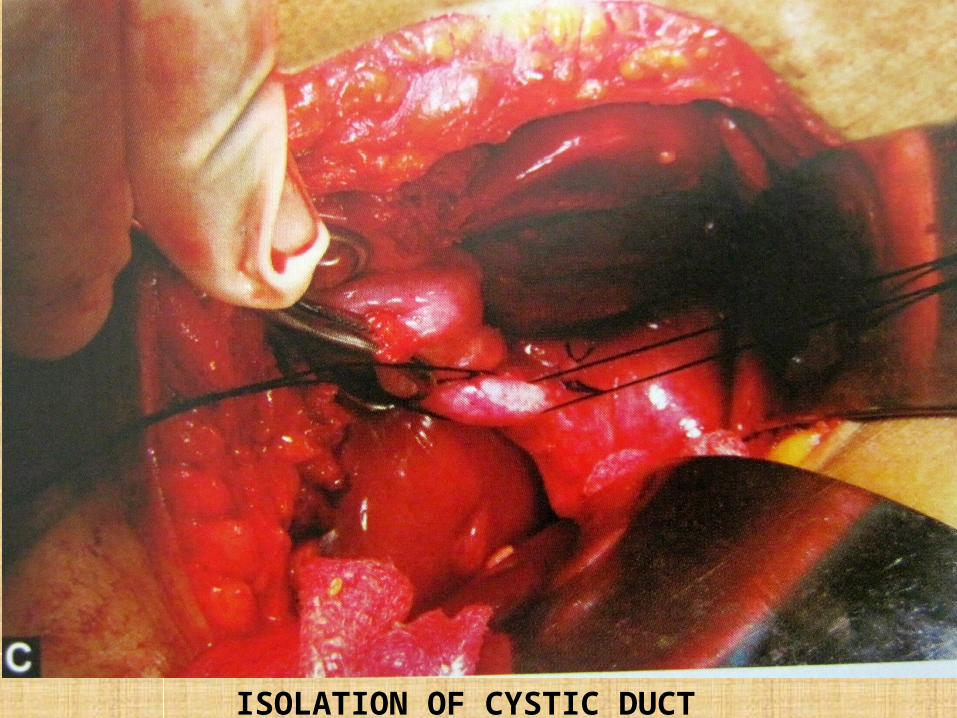
ISOLATION OF CYSTIC DUCT
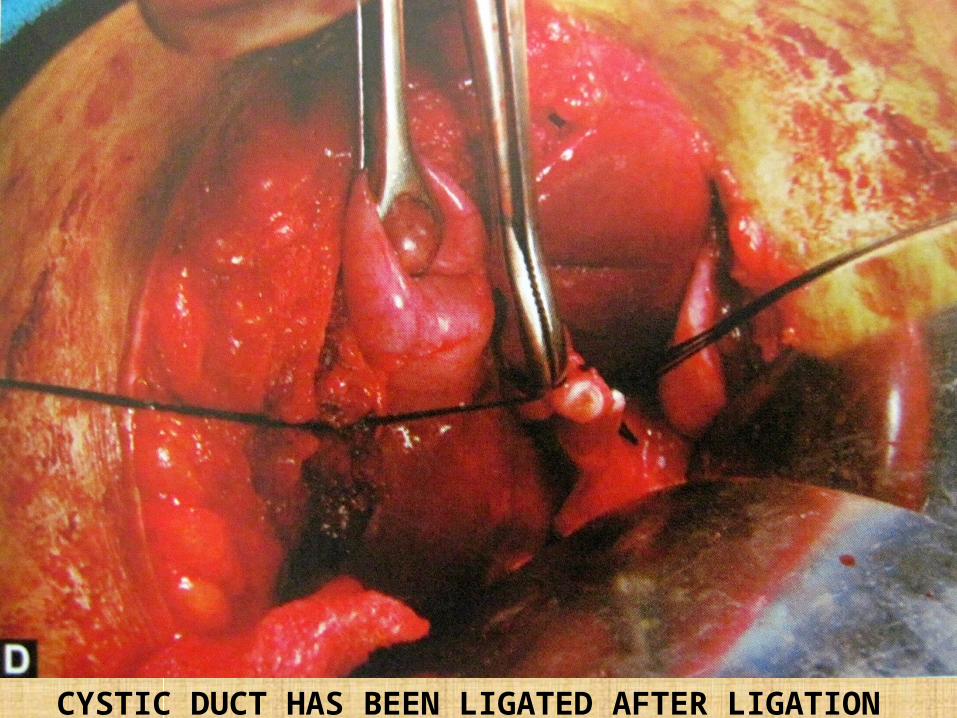
CYSTIC DUCT HAS BEEN LIGATED AFTER LIGATION
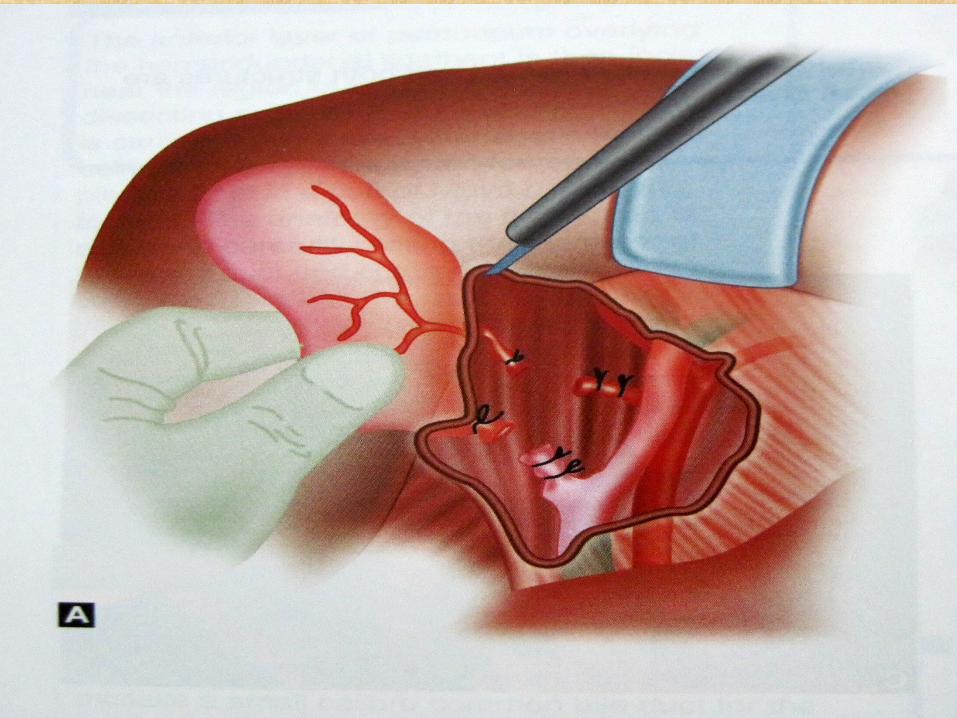
SURGICAL INSIGHT
• Gallbladder is kept under tension by gentle traction by surgeons left hand
• Fold of peritoneum attaching the gallbladder to the liver is divided using sharp dissection and coagulation.
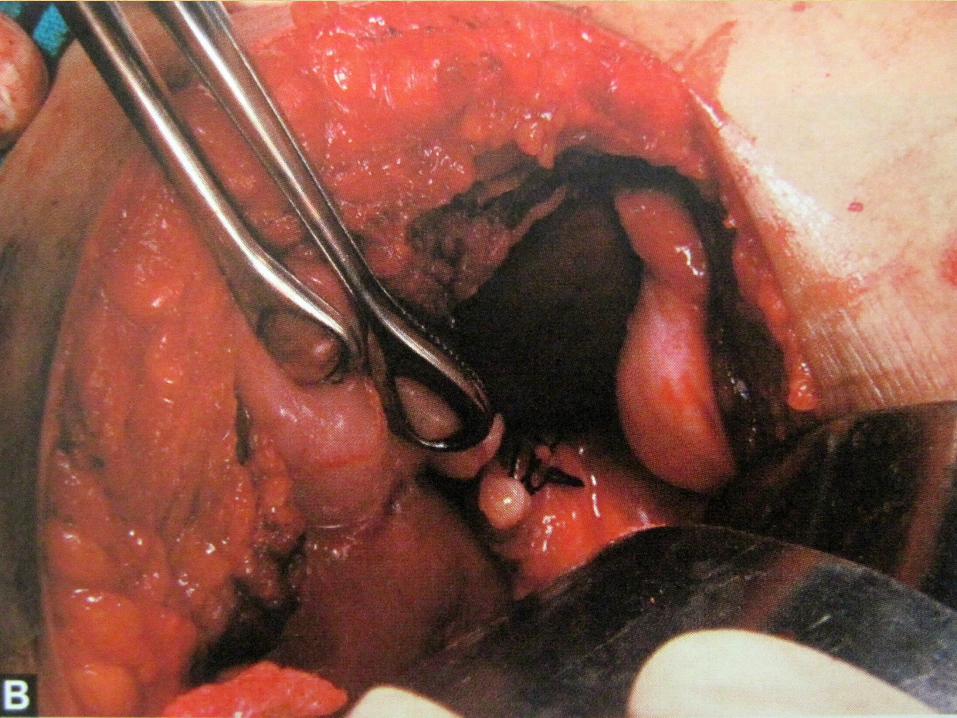
SURGICAL INSIGHT
FUNDUS FIRST METHOD:
Particularly when inflammation or adhesion formation makes it difficult to display CBD,cystic duct and artery.
It is important to establish the correct plane between the gallbladder and its bed
TOO DEEP TOO SUPERFICIAL
MAY ENTER LIVER PARENCHYMA
MAY ENTER GB LUMEN
SURGICAL INSIGHT
• Care must be taken as the dissection approached main biliary tree and when displaying cystic duct and artery
• Safer to leave a small over-sewen cuff of Hartmann’s pouch rather than to attempt hazardous dissection to free an adherent gallbladder and cystic duct form common hepatic duct
• Partial cholecystectomycirrhosis and portal hypertension

SURGICAL INSIGHT
• A small swab placed in gallbladder to control oozing.
• Any small bleeding vessels are coagulated
• Further bleeding may require placement of swabs or packs for 3-5 minsstill bleeding under-running of bleeding points with fine absorbable suture may be needed.
SURGICAL INSIGHT
• Hemostasis is achieved RT upper quadrant is lavaged with warm saline and removed
• A drain(redivac) is usually kept if there is anxieties about hemostasis.
• Incision is closed using a mass suture technique.skin is closed.
EXPLORATION OF CBD
Decision to explore CBD rests on
-demonstration of stones on preoperative MRCP
-operative cholangiogram
-palpation
SURGICAL INSIGHT
• The second part of the duodenum is mobilized by division of lateral leaf of its peritoneal covering (KOCHER MANEUVER).
• This allows the surgeon’s hand to pass behind the duodenum and head of pancreas to palpate the lower CBD.
• The anterior surface of the CBD is then cleared of its peritoneal covering.
• It is needled to get a bile specimen for bacteriological examination.

SURGICAL INSIGHT
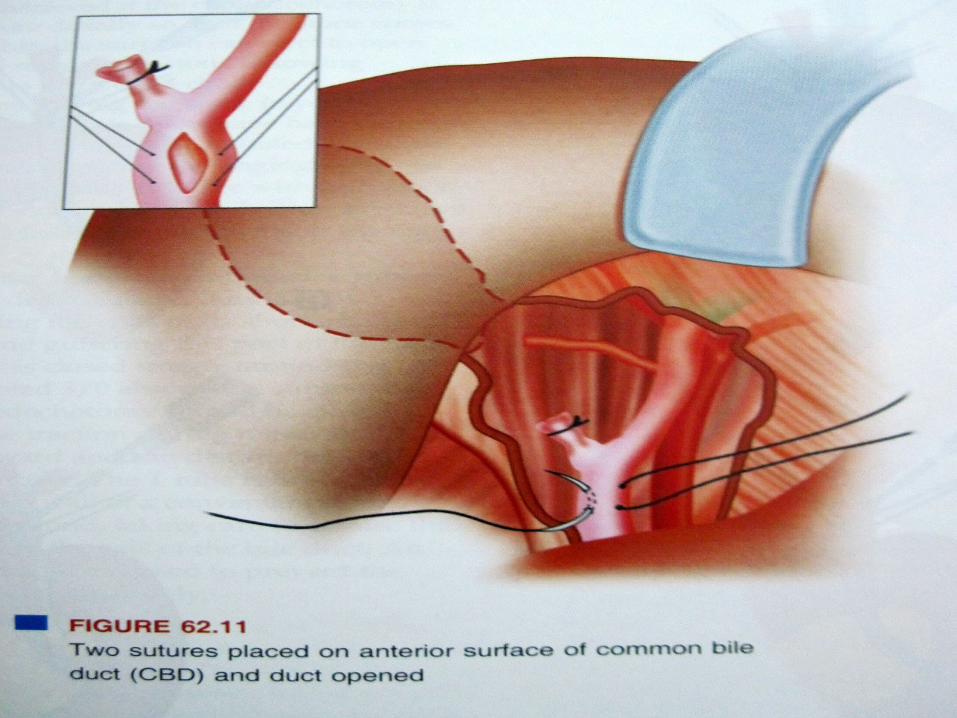
• The layer of peritoneum over CBD is incised to expose anterior surface
• The duct is incised between stay sutures using a 15 size blade longitudinally
• Incision is enlarged using angled dissection scissors
• Size of incision is dictated by stone size,usually 15-20mm long
CAUTION:# Extending the incision upwards may damage the
hepatic arterial tree.# The right hepatic artery loops in front of the bile duct# Extending incision downwards may injure numerous
small veins to duodenum
SURGICAL INSIGHT
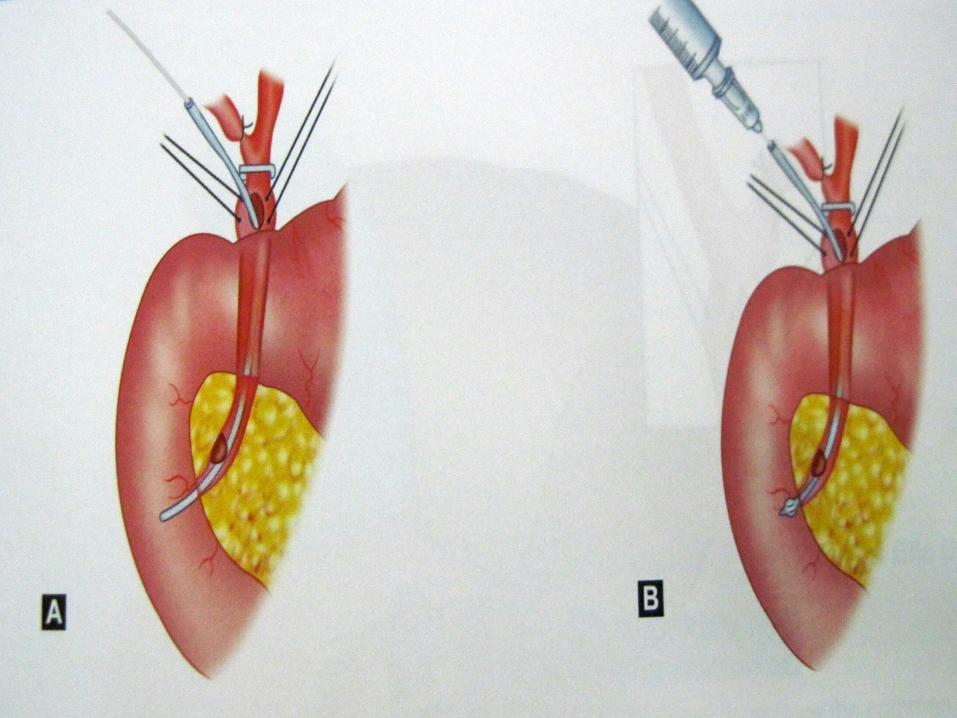
• A fine catheter is inserted into bile ductwarm saline is used to flush out any stone or debris.
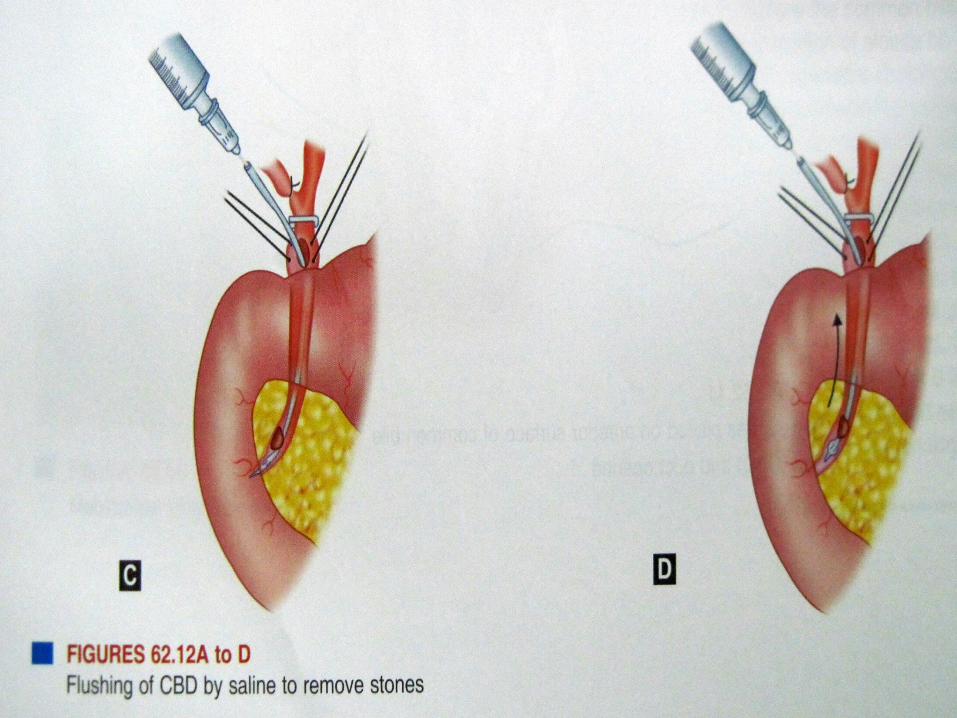
SURGICAL INSIGHT
• A flexible choledochoscope offers the ideal method of inspecting the billiary tree from within.
• Passed till ampulla and upwards till eight and left hepatic duct.
• Residual stones are flushed using warm saline or by biliary Fogarty balloon catheter.
PROCEDURE
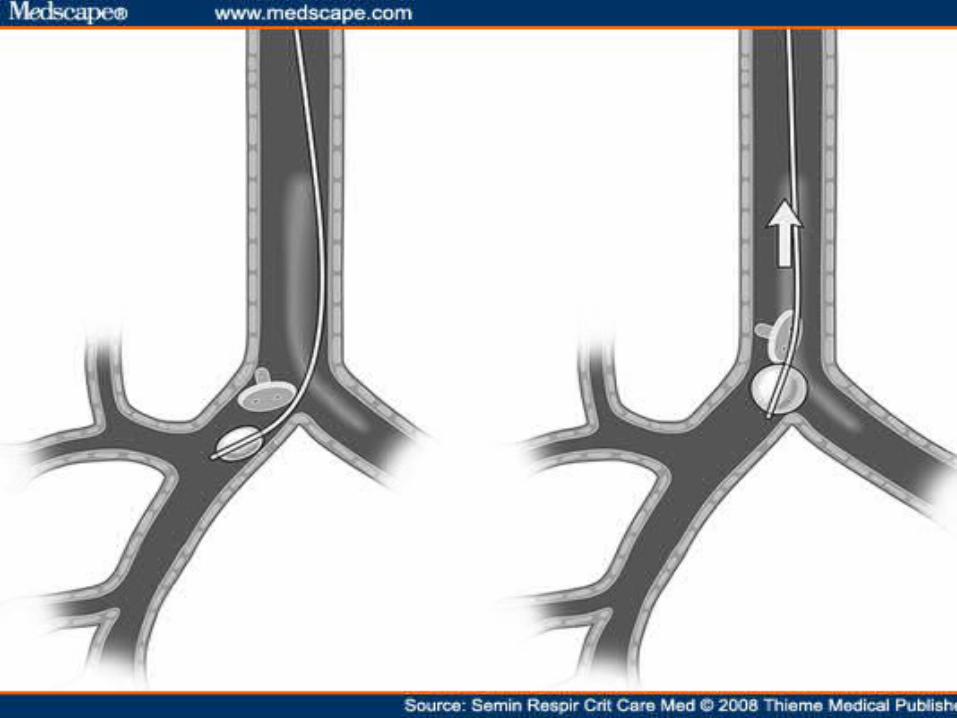
• The catheter is passed into duodenum and balloon is carefully inflated
• Gently withdrawn allowing balloon to deflate as it passes through papilla of Vater and sphincter of Oddi without undue force
• Above the sphincter region the balloon is reinflated
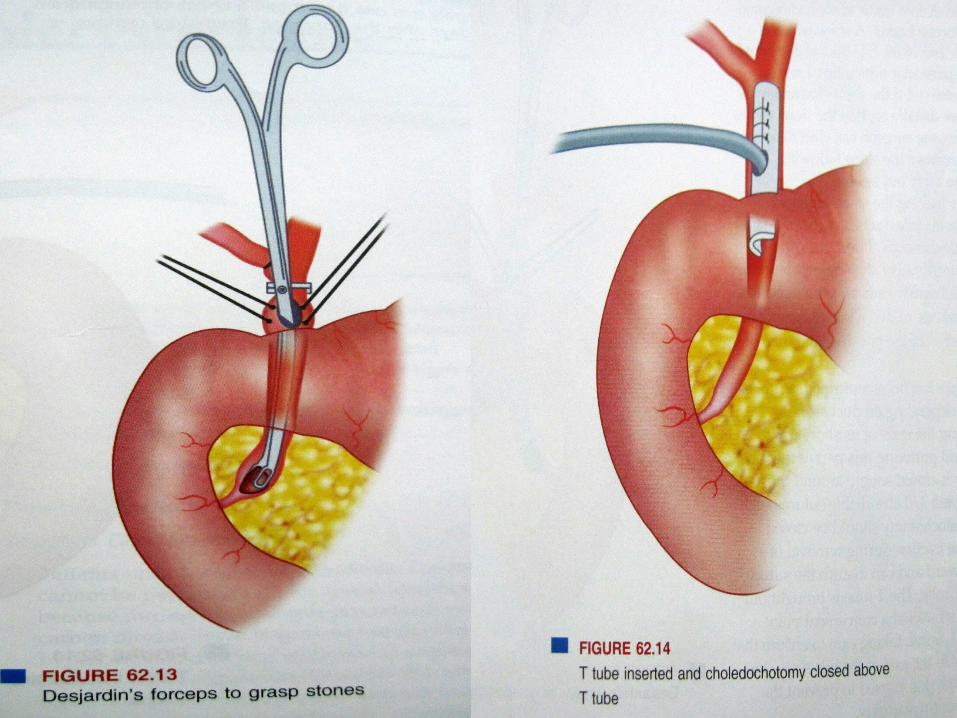
• Stones are seen in choledochotomy and withdrawn from the duct.
• Similar manner is employed for the upper reaches of biliary tree
SURGICAL INSIGHT
SURGICAL INSIGHT
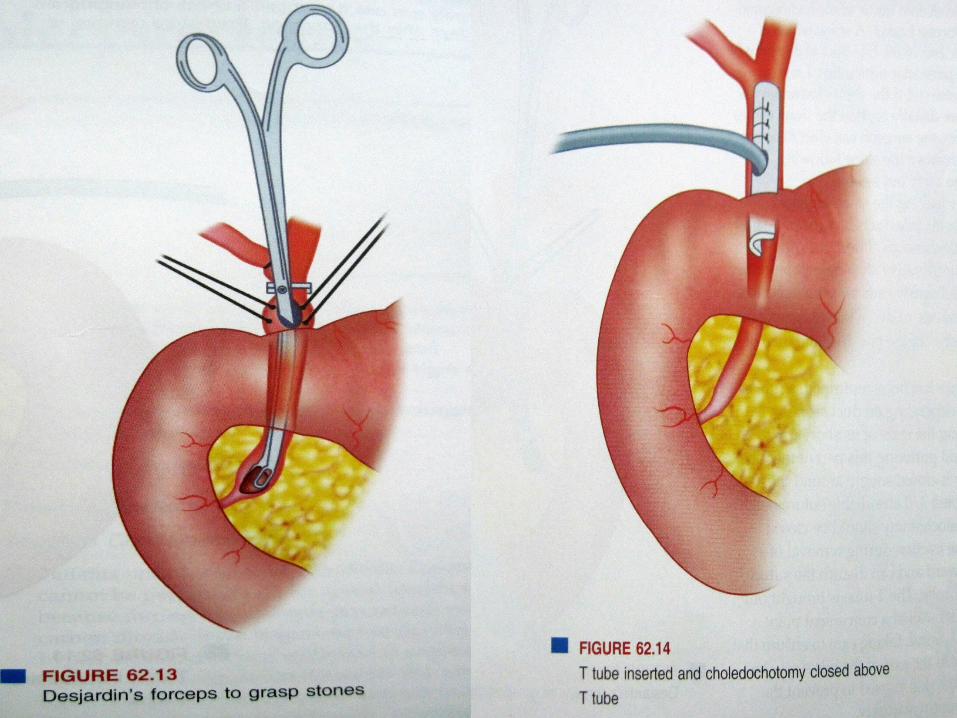
• If these measures fail, DESJARDIN’S forceps can be inserted into duct systemto grasp any visible stones.
• Repeated attempts to grasp stones “blindly” may damage the duct and should be avoided.
SURGICAL INSIGHT
• The stones which can’t be removed can be removed using dormia basket
• As the scope is pulled back, the common duct should be inspected.
• A stone trapped at lower end of bile duct can be retrieved if choledochotomy is extended a little more distally.
• The surgeon can elect to open duodenum and remove the stone following sphincterotomy
SURGICAL INSIGHT
• Can also carryout choledochoduodenostomy leaving the stone in place.
• Once duct clearance has been confirmed, choose a T tube of appropriate size.
• If the duct is large and multiple stones have been obtained, use at least a No. 14 French T tube.
• Tube is inserted after trimming ends of its short arm to an appropriate length and guttered.
• The choledochotomy is closed snugly around the T-tube using interrupted 3/0 absorbable suture.
SURGICAL INSIGHT
• Choledochostomy should be closed above T tube.
• T tube is brought out through the abdominal wall at a convenient point away from the main wound.
• T tube has to run perpendicular to the axis of the bile duct.
• Anchoring suture to the skin is used to prevent the Ttube from premature falling.
SURGICAL INSIGHT
• Some surgeons do not insert a T tube after exploring the bile duct.
• Many surgeons prefer a T tube and obtain a check cholangiogram 5-7 days after the operation.
• Premature removal of tube may allow biliary leakage and biliary peritonitis(7-10 days).
• Few other surgeons close the common bile duct after putting a biliary stent inside which is removed endoscopically 8 weeks later.
SURGICAL INSIGHT
POSTOPERATIVE CARE:
-patients maintained in IVF for first 12 hours.
-oral intake after 1st postoperative day and clinical condition of patient.
-early mobilization.
-after uneventful elective cholecystectomy,many patients are ready for discharge from hospital within a few days