
Endoscopic management of common bile duct stones
24
Endoscopic management of common bile duct stones Shannon Acker August 1, 2011
Transcript of Endoscopic management of common bile duct stones

Endoscopic management of common bile duct
stonesShannon AckerAugust 1, 2011

Gallstones occur in 15% of population
10-50% cause symptoms within 10-20 yrs
10-18% of patients who have cholecystectomy for gallstones have common bile duct (CBD) stones
Natural history of CBD stones is not known, complications appear to be more frequent and severe than with asymptomatic stones
Martin DJ, et al. Surgical versus endoscopic treatment of bile duct stones. Cochrane Database Syst Rev 2006;CD003327.

Evolution of CBDS management
1889 - first surgical exploration of the CBD by Swiss Surgeon Ludwig Courvoisier via incision in the CBD
1960s - Mazzariello, an Argentinean surgeon, introduced non operative instrument extraction of retained CBDS via T-tubes
1970s -Gastroenterologists from Germany and Japan introduced endoscopic sphincterotomy for retained CBDS
Memon MA, et al. Laparoscopic common bile duct exploration: the past, the present, and the future. The Amer J of Surg 2000:179.

Evolution of CBDS management
In the era of open cholecystectomy, intraoperative cholangiography was performed routinely
Surgical CBD stone extraction was the recommended treatment option
Open CBD exploration results in: lower primary treatment failure fewer additional procedures fewer average number of procedures required per
patient lower mortalitywhen compared to ERCP Martin DJ, et al. Surgical versus endoscopic
treatment of bile duct stones. Cochrane Database Syst Rev 2006;CD003327.

Evolution of Cholecystectomy
Laparoscopic cholecystectomy introduced in 1985 by Erich Muhe -Germany
Advantages of laparoscopy: shorter
hospitalizations quicker return to work decreased
complications less postoperative
pain
Kroh M, Chand B. Choledocholithiasis, endoscopic retrograde cholangiopancreatography, and laparoscopic common bile duct exploration. Surg Clin N Am 88(2008)1019-31.

CBDS in the era of laparoscopic cholecystectomy Advances in
endoscopic stone clearance techniques Endoscopic
sphincterotomy Endoscopic
baskets, balloons, lithotripsy devices
Advances in laparoscopy Improved experience
and instrumentation Transcystic stone
removal Laparoscopic
choledochotomy with stone clearance
Transcystic stenting followed by post operative ERCPKroh M, Chand B. Choledocholithiasis, endoscopic retrograde
cholangiopancreatography, and laparoscopic common bile duct exploration. Surg Clin N Am 88(2008)1019-31.

Current Debate

Advantages of Endoscopic Treatment of CBD StonesOptimal for elderly and high risk
patientsPrimary treatment for acute
cholangitis and gallstone pancreatitis
Option as single therapy for common bile duct stones

Acute Cholangitis 82 patients with severe acute cholangitis due
to choledocholithiasis randomly assigned to undergo surgical decompression of the biliary tract or endoscopic biliary drainage
Lai ECS, at al. Endoscopic biliary drainage for severe acute cholangitis. NEJM 1992; 326:24.

Acute Cholangitis Review of 94 pts admitted with acute
cholangitis: 82 had CBD stones, 71 underwent
decompression28 surgically, 43 ES
Endoscopic sphincterotomy (ES) associated with lower 30 day mortality
Of 43 pts undergoing ES23 had gallbladder left in situ; 2 of 23 required
future cholecystectomy
Endoscopic biliary drainage is associated with a significantly reduced mortality and morbidity rate
Lai ECS, at al. Endoscopic biliary drainage for severe acute cholangitis. NEJM 1992; 326:24. Leese T, Neoptolomos JP, Baker AR (1985) Cholangitis and the impact of endoscopic sphincterotomy. Gut 26:A553.

Patients with mild or severe pancreatitis who underwent emergency ERCP Decreased rates of biliary sepsis (0/97 vs 12/98
patients) Decreased rate of hospital morality (5 patients vs
9 patients)
Fan ST, et al .NEJM 1993(328)4.Cuschieri A, et al. Surg Endosc (1999)13:952-57.
“It is generally agreed that the two-stage approach (ERCP with endoscopic stone extraction followed by laparoscopic cholecystectomy) is indicated in poor-risk patients, including those with established cholangitis or severe pancreatitis.” Cuschieri 1999
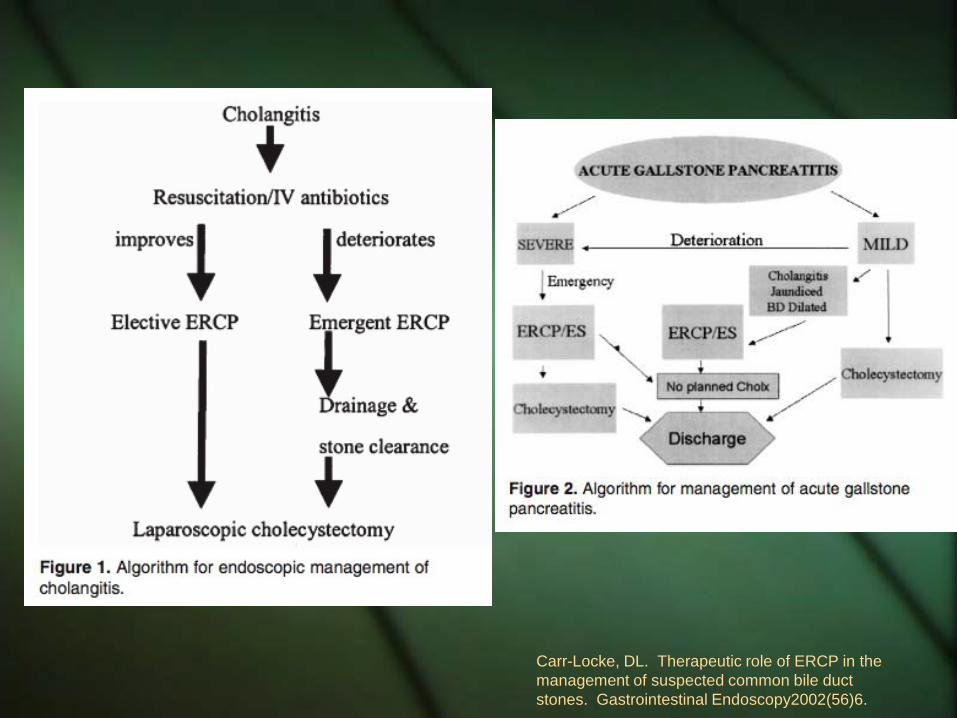
Carr-Locke, DL. Therapeutic role of ERCP in the management of suspected common bile duct stones. Gastrointestinal Endoscopy2002(56)6.

Targarona EM, et al. Randomied trial of endoscopic sphincterotomy with gallbladder left in situ versus open surgery for common bile duct calculi in high risk patients. The Lancet. 1996(347).

Endoscopic Sphincterotomy as Single Therapy
71 patients with both CBDS and gallbladder stones in whom endoscopic clearance of bile duct stones was achieved 3 pts underwent cholecystectomy within 1
week (acute cholecystitis) 42 pts - cholecystectomy was
recommended (based on specialist preference)
26 pts - wait and see strategy recommended5 pts underwent cholecystectomy with no worse
surgical outcomeKeulemans YCA, et al. Current management of the gallbladder after endoscopic sphincterotomy for common bile duct stones. Gastrointestinal Endoscopy 1997(46)6.

Endoscopic Sphincterotomy as Single Therapy
83 pts with CBDS enrolled in RCT of endoscopic sphincterotomy and stone removal vs surgery alone
5 year follow up7/39 ES pts underwent
cholecystectomy (6 for symptoms, 1 for cholecystitis)
2/39 ES pts died of gallbladder cancer Hammarstrom LE, et al. Long-term follow-up of a
prospective randomized study of endoscopic versus surgical treatment of bile duct calculi in patients with gallbladder in situ. Br J Surg 1995;82(11)1516-21.

Endoscopic and surgical treatment of bile duct
calculi in middle-aged and elderly patients with gallbladder in situ are equally effective in the
long term -Hammarstrom
1995
Indications for Endoscopic Treatment of CBDS
Acute cholangitisGallstone pancreatitisElderly and high risk patients

Quality of Data Only two proscpective RCTs comparing
endoscopic to surgical treatment of common bile duct stones discovered intraoperatively
Numerous exclusion criteria: acute pancreatitis, acute cholangitis, anatomy precluding ERCP, ASA status 3-4, need for a drainage procedure of the CBD
Phillips EH, at al. Treatment of common bile duct stones discovered during cholecystectomy. J Gastrointest Surg (2008)12:624-28.

Surgeon Experience Over past 30 years: Number of cholecystectomies increased from
400,000 to 750,000 per year Rate of CBDE dropped from 20% to 2%
Only 15,000 CBDEs performed each year Published data comes from centers of
excellence No data on outcomes of procedures
performed by less experienced surgeons Number of CBDEs reported by finishing chief
surgery residents: 10 in 1990 (all open) 1.5 open and 0.8 laparoscopic in 2008
Phillips EH, at al. Treatment of common bile duct stones discovered during cholecystectomy. J Gastrointest Surg (2008)12:624-28.

Survey of 68 general surgeons practicing in rural USOnly 45% reported that they perform
LCBDE 75% reported that ERCP was preferred
approach to a patient with choledocholithiasis
Reasons for not performing LCBDE58% - time24% - equipment6% - lack of good GI backup3% - reimbursement1.5% - increased morbidity1.5% - lack of skill
Bingener J, Schwesinger WH. Management of common bile duct stones in a rural area of the US: Results of a survey. Surg Endosc (2006)20:577-79.

Application of LCBDE Data Taylor 2007 - Australia Campbell-Lloyd 2008 - Australia Poole 1997 - UK O’Neill 2008 - Australia Tang 2006 - Hong Kong Sgourakis 2002 - Greece Tinoco 2008 - Brazil Cuschieri 1999 - UK, Italy, Spain, Australia, Portugal,
The Netherlands Clayton 2006 - New Zealand, Greece Suc 1998 - France Neoptolemos 1987 - UK Tranter 2002 - UK Nathanson 2005 - Australia Rhodes 1998 - UK Gurusamy 2001 - UK

There are several approaches (to the management of CBDS) and
current data does not suggest clear superiority of any one approach; decisions regarding treatment are most appropriately made based on surgeon preference as well as the
availability of equipment and skilled personnel. (Level I, Grade A)
-SAGES Recommendations
Guidelines for the clnical application of laparoscopic biliary tract surgery: Practice/Clinical Guidelines published on 01/2010.

ConclusisonsEndoscpic management of CBDS: Optimal for elderly and high risk
patients Primary treatment for acute cholangitis
and gallstone pancreatitis Option as single therapy for common
bile duct stonesNo data to support use of LCBDE in US

Taylor CJ, Kong J, Ghusn M, White S, Crampton N, Layani L. Laparoscopic bile duct exploration: results of 160 consecutive cases with 2-year follow up. ANZ J Surg 2007;77:440-5
Campbell-Lloyd AJ, Martin DJ, Martin IJ. Long-term outcomes after laparoscopic bile duct exploration: a 5-year follow up of 150 consecutive patients. ANZ J Surg 2008;78:492-4.
Poole G, Waldron B, Shimi SM, Cuschieri A. Laparoscopic common bile duct exploration after failed endoscopic stone extraction. Endoscopy 1997 Sep:29(7):609-13.
O'Neill CJ, Gillies DM, Gani JS. Choledocholithiasis: overdiagnosed endoscopically and undertreated laparoscopically. ANZ J Surg 2008;78:487-91.
Tang CN, Tsui KK, Ha JP, Siu WT, Li MK. Laparoscopic exploration of the common bile duct: 10-year experience of 174 patients from a single centre. Hong Kong Med J 2006;12:191-6.
Sgourakis G, Karaliotas K. Laparsocopic common bile duct exploration and cholecystectomy versus endoscopic stone extraction and laparoscopic cholecystectomy for choledocholithiasis. A prospective randomized study. Minerva Chir 2002 Aug;57(4)467-74.
Tinoco R, Tinoco A, El-Kadre L, Peres L, Sueth D. Laparoscopic common bile duct exploration. Ann Surg 2008;247:674-9.
Cuschieri A, et al. EAES multicenter proscpecitve randomized trial comparing two-stage vs single-stage management of patients with gallstone disease and ductal calculi. Surg Endosc (1999)13:952-57.
Clayton ES, Connor S, Alexakis N, Leandros E. Meta-analysis of endoscopy and surgery versus surgery alone for common bile duct stones with the gallbladder in situ. Br J Surg 2006;93:1185-91.
Suc B, et al. Surgery vs Endocsopy as primary treatment in symptomatic patients with suspected common bile duet stones: a multicenter randomized trial. Arch Surg, 1998;133:702-708.
Neoptolemos JP, Carr-Locke DL, Fossard DP. Prospective randomized study of preoperative endoscopic sphincterotomy versus surgery alone for common bile duct stones. British Medical Journal 1987Feb:294.
Tranter SE, Thompson MH> Comparison of endoscopic sphinctertomy and laparoscpic exploration of the common bile duct. British Journal of Surgery 2002(89)1495-1504.
Nathanson LK, et al. Postoperative ERCP versus laparoscopic choledochotomy for clearance of selected bile duct calculi: a randomized trial. Ann Surg 2005;242:188-192.
Rhodes M, et al. Randomised trial of laparoscopic exploration of common bile duct versus postoperative endoscopic retrograde cholangiography for common bile duct stones. Lancet 1998;351:159-61.
Gursamy K, et al. Systematic review and meta-analysis of inraoperative versus preoperative endosocpic sphincterotomy in patients with galldbldder and suspected common bile duct stones. British Journal of Surgery 2001;98:908-916.















![Endoscopic management of common bile duct stones: European ... · dence of gallstone formation of 0.60% per year [13]. According to a large Swedish registry [14], the prevalence of](https://static.fdocuments.net/doc/165x107/5e22403e4a0c0855ec03f978/endoscopic-management-of-common-bile-duct-stones-european-dence-of-gallstone.jpg)

