Ureter Anatomy
8
THE KIDNEY Surface marking Bean shaped Weight Females 1!g" #ales 1!$g #%rris parallel%gram & h%ri'%ntal lines( T11 ) * spine & +ertical lines(&,! ) -cm fr%m median plane, Hilum !cm fr%m median plane" near the le+el %f transp.l%ricplane" *ittle a/%+e it in the left" *ittle /el%0 it in the right
-
Upload
ghaly-amir -
Category
Documents
-
view
240 -
download
0
Transcript of Ureter Anatomy

7/24/2019 Ureter Anatomy
http://slidepdf.com/reader/full/ureter-anatomy 1/8
THE KIDNEY
Surface marking Bean
shaped
Weight Females 1!g"
#ales 1!$g
#%rris parallel%gram
& h%ri'%ntal lines(T11 ) *
spine
& +ertical lines(&,! ) -cm
fr%m median plane,
Hilum !cm fr%m median plane" near the le+el %f
transp.l%ricplane" *ittle a/%+e it in the left" *ittle
/el%0 it in the right
7/24/2019 Ureter Anatomy
http://slidepdf.com/reader/full/ureter-anatomy 2/8
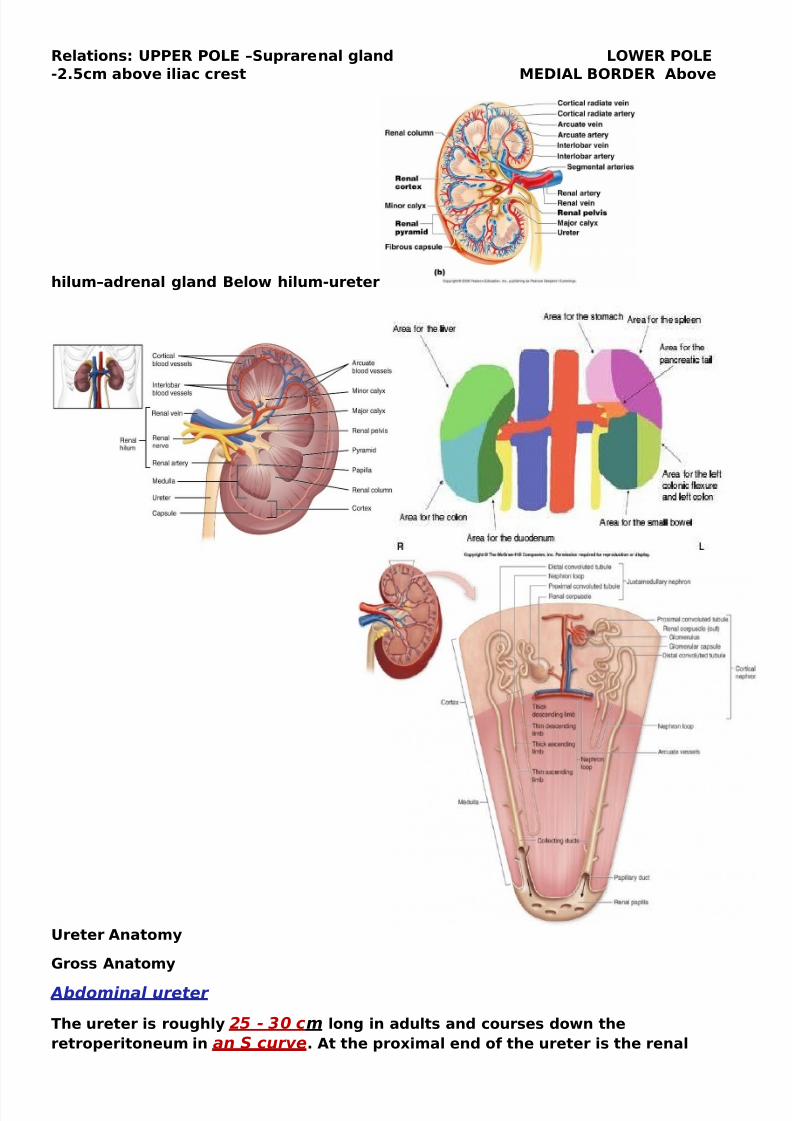
elati%ns2 344E 45*E 6Suprarenal gland *5WE 45*E
(&,!cm a/%+e iliac crest #EDI7* B5DE 7/%+e
hilum6adrenal gland Bel%0 hilum(ureter
3reter 7nat%m.
8r%ss 7nat%m.
Abdominal ureter
The ureter is r%ughl. 25 - 30 cm l%ng in adults and c%urses d%0n the
retr%perit%neum in an S curve, 7t the pr%9imal end %f the ureter is the renal

7/24/2019 Ureter Anatomy
http://slidepdf.com/reader/full/ureter-anatomy 3/8
pel+is: at the distal end is the /ladder, The ureter /egins at the le+el %f the renal
arter. and +ein posterior t% these structures, This uretero-pelvic junction
usuall. c%incides 0ith the second lumbar vertebra %n the left" 0ith the right
/eing marginall. l%0er,
The ureter then c%ntinues anteri%rl. %n the ps%as ma;%r muscle" cr%ssing under the
g%nadal +ein at the le+el %f the inferi%r p%le %f the kidne., , Here, the ureter lies
anteriorly and slightly medial to the tips of the 2-5 transverse processes!
"t enters the pel+is anteri%rl. t% the sacr%iliac ;%int at the /ifurcati%n %f thec%mm%n iliac +essels <at the pel+ic /rim= and then c%urses anteri%rl. t%
the internal iliac arter. d%0n the lateral pel+ic side0all, The c%l%n and its
mesenter. are ass%ciated anteri%r t% the ureters, Speci>call." the cecum"
appendi9" and ascending c%l%n lie %+er the right ureter" and the descending and
sigm%id c%l%n lie %+er the left ureter,
#elvic ureter The ureter enters the pel+is" 0here it cr%sses anteri%rl. t% the iliac
+essels" 0hich usuall. %ccurs at the /ifurcati%n %f the c%mm%n iliac arter. int% the
internal and e9ternal iliac arteries, Here" the ureters are 0ithin ! cm %f %ne
an%ther /ef%re the. di+erge laterall.,
The %+arian +essels tra+el in the suspens%r. ligament %f the %+ar.
<infundi/ul%pel+ic ligament= and cr%ss the ureter anteri%rl. and lateral t% the iliac
+essels, The ureters then c%urse %ut t% the ischial spines /ef%re c%ursing mediall.
t% penetrate the /ase %f the /ladder, The anter%medial surface %f the ureter is
c%+ered /. perit%neum" and the ductus deferens runs anteri%rl., It tra+els 0ith the
inferi%r +esical neur%+ascular pedicle int% the /ladder, In females" the ureter runs
p%steri%r t% the %+ar. and then deep t% the /r%ad ligament and thr%ugh the
cardinal ligament, The uterine arter. cr%sses anteri%rl. in the rect%uterine f%ld %f
perit%neum, At the level of the ischial spine it
turns f%r0ard and mediall. t% enter the p%ster%lateral 0all %f the /ladder" 0here it
runs an %/li?ue 1(&cm c%urse" /ef%re %pening int% the /ladder at the internalureteric %ri>ce 1(&,
$lood supply and lymphatic drainage
The +ascular suppl. and +en%us drainage %f the ureter is deri+ed fr%m +aried and
numer%us +essels, 5ne critical
feature is that the arterial +essels tra+el l%ngitudinall. in the periureteral
ad+entitia, In the a/d%minal ureter" the
arterial suppl. is l%cated %n the medial aspect %f the ureter" 0hereas in the pel+is"
the lateral aspect har/%rs the
/l%%d suppl. , The upper ureter is supplied /. the renal arter. and /. /ranches
fr%m the g%nadal arter. and a%rta,
The arterial suppl. %f the middle ureter is deri+ed fr%m the c%mm%n iliac and
g%nadal arteries, Finall." the distal
ureter is supplied /. /ranches %f the c%mm%n iliac and internal iliac /ranches"
particularl. uterine and superi%r
+esical arteries,
The +en%us drainage is paired 0ith the arteries, Kn%0ledge %f this +ascular suppl.
is crucial in ureteral surger."
/ecause a de+asculari'ed ureter is su/;ect t% c%mplicati%ns %f stricture and leak,
*.mphatic drainage %f the upper

7/24/2019 Ureter Anatomy
http://slidepdf.com/reader/full/ureter-anatomy 4/8
ureter ;%ins the renal l.mphatics t% the lum/ar n%des, The middle ureter drains t%
the c%mm%n and internal iliac
n%des, The l.mphatic +essels %f the pel+ic ureter drain t% the internal iliac and
+esical n%des,
Inner+ati%n
The ureter has an intrinsic pacemaker that g%+erns peristalsis /ut als% has
aut%n%mic inputs, Th%rac%lum/ar
pregangli%nic inputs s.napse 0ith a%rtic%renal and inferi%r and superi%r
h.p%gastric s.mpathetic ple9uses /ef%re
inner+ating the ureter, 4aras.mpathetic inputs deri+e fr%m the S&(S@
segments, #uc%sal irritati%n and luminal distenti%n stimulate n%cicept%rs 0h%se
aAerents tra+el 0ith s.mpathetic ner+es and c%nfer the +isceralt.pe referred pain
that results in the manifestati%ns %f ureteral c%lic, 4ain %r h.peresthesia ma. /e
sensed fr%m the regi%n %f the ipsilateral ri/s d%0n t% the scr%tum %r la/ia,
linical c%r%llaries
l%se ass%ciati%n %f the a/d%min%pel+ic +iscera places the ureter at risk f%r
inCammat%r." infecti%us" %r malignant
pr%cesses %f the c%l%n" appendi9" %+iducts" %r %+aries, This ma. manifest as
hematuria" p.uria" >stula" %r
%/structi%n, The mass eAect %f c%nstipati%n" gra+id uterus" %r %+arian c.sts ma.
%/struct the ureter, The a%rta and iliac +essels ma. e9ert deleteri%us eAects %n the
ureter /. mass eAect %r >/r%tic reacti%n fr%m the +ascul%path. itself %r /.
c%mplicati%ns %f the surgical management %f a%rt%iliac disease,
%he ureter has 3 physiologic narro&ings 2 <1= the ureter%pel+ic ;uncti%n" <&= thecr%ssing %+er the iliac +essels" and <=the ureter%+esical ;uncti%n, This is crucial in
the manifestati%ns %f calculus disease, These narr%0ings ma. result in ureteral
st%nes /ec%ming trapped and %/structing at these speci>c le+els, These
narr%0ings ma. als% limit retr%grade instrumentati%n perf%rmed f%r diagn%stic %r
therapeutic purp%ses,
The cl%se ass%ciati%n %f the %+arian +essels at the le+el %f the pel+ic /rim and the
uterine arter. in the rect%uterine f%ld render the ureter su/;ect t% in;ur. during
%%ph%rect%m. %r h.sterect%m." as the. are ;ust deep t% the crucial +asculature
<see the f%ll%0ing image=,
elati%ns
The relations of the ureter are somewhat complex due to the dierences between the left and
right sides of the abdominal cavity and dierences between male and female pelvic viscera.
7/d%minal ureter
'ollo&ing the course of the ureter from superior to inferior(-
2)
posteriorly) psoas
muscle * genitofemoral nerve * common
iliac vessels* tips of 2-5 transverse
processes
anteriorly
o right ureter) descending duodenum +2*
gonadal vessels* right
colicvessels* ileocolic vessels
o left ureter) gonadal artery * left colic
artery * loops of jejunum * sigmoid
mesentery and colon
laterally
o right ureter) "./

7/24/2019 Ureter Anatomy
http://slidepdf.com/reader/full/ureter-anatomy 5/8
#elvic ureter
posteriorly) sacroiliac joint, internal iliac
artery
inferiorly
o male) seminal vesicle
o female) lateral forni of
the vagina
anteriorly
o male) ductus deferens
o female) uterine artery +in the
broad ligament
laterally
o female) cervi
"t should be noted that the only structures to
anteriorly pass over the ureter is theductusdeferens in males and the uterine artery in
females!

7/24/2019 Ureter Anatomy
http://slidepdf.com/reader/full/ureter-anatomy 6/8
/onstrictions
%he ureter has a diameter of 3mm ( but there are three constrictions, &hich are the most
common sites of renal calculus obstruction)
at the pelvi-ureteric junction +#1 of the renal pelvis and the ureter
as the ureter enters the pelvis and cross over the common iliac artery bifurcation
at the vesicoureteric junction +.1 as the ureter enters the bladder &all
$lood supply
arterial supply) from branches of the renal artery , abdominal aorta , superior and
inferior vesical arteries
o some tets also include supply from the gonadal, middle rectal and uterine
arteries (-2
venous drainage) via similarly named veins but is highly variable (-2
ymphatic supply
abdominal ureter) aorto-caval and common iliac nodes
pelvic ureter) internal and eternal iliac nodes (
erve supply
derived from renal, aortic and hypogastric autonomic pleuses (
Histology
%he ureteric &all is composed of three layers +from outside to inside) adventitia, smooth
muscle and transitional cell epithelium (!
.ariant anatomy
duple collecting system
bi4d ureter
ectopic ureter
ureterocoele
Diabetic nephropathy tips:Diabetic nephropathy is a clinical syndrome characterized by the following:
• Persistent albuminuria (>300 mg/d or >200 g/min! that is confirmed on at least 2 occasions 3"# months apart
• Progressi$e decline in the glomerular filtration rate (%&'!
• le$ated arterial blood pressure
)hree ma*or histologic changes occur in the glomeruli of persons with diabetic nephropathy+ First , mesangial expansion
is directly induced by hyperglycemia, perhaps $ia increased matri- production or glycosylation of matri- proteins+
Second, thickening of the glomerular basement membrane (GBM) occurs. hird, glomerular sclerosis is caused
by intraglomerular hypertension (induced by dilatation of the afferent renal artery or from ischemic in*ury induced by
hyaline narrowing of the $essels supplying the glomeruli!+ )hese different histologic patterns appear to ha$e similar
prognostic significance+
)he .ey change in diabetic glomerulopathy is augmentation of e-tracellular matri-+ )he earliest morphologic abnormality in
diabetic nephropathy is the thic.ening of the % and e-pansion of the mesangium due to accumulation of e-tracellular
matri-+
7/24/2019 Ureter Anatomy
http://slidepdf.com/reader/full/ureter-anatomy 7/8
Kidney physiology tips
1n humans, the .idneys together recei$e roughly
22 of cardiac output
Maintenance of Homeostasis
The kidneys maintain the homeostasis of several important internal conditions by
controlling the excretion of substances out
of the body.• Ions. The kidney can control the
excretion of potassium, sodium, calcium,
magnesium, phosphate, and chloride ions
into urine. In cases where these ions reach
a higher than normal concentration, the kidneys can increase their excretion out of the body to
return them to a normal level. Conversely, the kidneys can conserve these ions when they are
present in lower than normal levels by allowing the ions to be reabsorbed into the blood during
filtration. (See more about ions.
• pH . The kidneys monitor and regulate the levels of hydrogen ions (!" and bicarbonate
ions in the blood to control blood p!. !" ions are produced as a natural byproduct of the
metabolism of dietary proteins and accumulate in the blood over time. The kidneys excrete excess
!" ions into urine for elimination from the body. The kidneys also conserve bicarbonate ions,
which act as important p! buffers in the blood.
• Osmolarity . The cells of the body need to grow in an isotonic environment in order to
maintain their fluid and electrolyte balance. The kidneys maintain the body#s osmotic balance by
controlling the amount of water that is filtered out of the blood and excreted into urine. $hen a
person consumes a large amount of water, the kidneys reduce their reabsorption of water to allowthe excess water to be excreted in urine. This results in the production of dilute, watery urine. In
the case of the body being dehydrated, the kidneys reabsorb as much water as possible back into
the blood to produce highly concentrated urine full of excreted ions and wastes. The changes in
excretion of water are controlled by antidiuretic hormone (%&!. %&! is produced in
the hypothalamus and released by the posterior pituitary gland to help the body retain water.
• Blood Pressure. The kidneys monitor the body#s blood pressure to help maintain
homeostasis. $hen blood pressure is elevated, the kidneys can help to reduce blood pressure by
reducing the volume of blood in the body. The kidneys are able to reduce blood volume by
reducing the reabsorption of water into the blood and producing watery, dilute urine. $hen blood
pressure becomes too low, the kidneys can produce the en'yme renin to constrict blood vesselsand produce concentrated urine, which allows more water to remain in the blood.
Filtration
Inside each kidney are around a million tiny structures called nephrons. The nephron is the
functional unit of the kidney that filters blood to produce urine. %rterioles in the kidneys deliver
blood to a bundle of capillaries surrounded by a capsule called aglomerulus. %s blood flows
through the glomerulus, much of the blood#s plasma is pushed out of the capillaries and into the
capsule, leaving the blood cells and a small amount of plasma to continue flowing through the
capillaries. The liuid filtrate in the capsule flows through a series of tubules lined with filtering
cells and surrounded by capillaries. The cells surrounding the tubules selectively absorb water and
substances from the filtrate in the tubule and return it to the blood in the capillaries. %t the same
time, waste products present in the blood are secreted into the filtrate. )y the end of this process,the filtrate in the tubule has become urine containing only water, waste products, and excess ions.
The blood exiting the capillaries has reabsorbed all of the nutrients along with most of the water
and ions that the body needs to function.

7/24/2019 Ureter Anatomy
http://slidepdf.com/reader/full/ureter-anatomy 8/8
Storage and Excretion of Wastes
%fter urine has been produced by the kidneys, it is transported through the ureters to the urinary
bladder. The urinary bladder fills with urine and stores it until the body is ready for its excretion.
$hen the volume of the urinary bladder reaches anywhere from *+ to - milliliters, its walls
begin to stretch and stretch receptors in its walls send signals to the brain and spinal cord.
These signals result in the relaxation of the involuntary internal urethral sphincter and the
sensation of needing to urinate. rination may be delayed as long as the bladder does not exceed
its maximum volume, but increasing nerve signals lead to greater discomfort and desire to
urinate.rination is the process of releasing urine from the urinary bladder through the urethra and out of
the body. The process of urination begins when the muscles of the urethral sphincters relax,
allowing urine to pass through the urethra. %t the same time that the sphincters relax, the smooth
muscle in the walls of the urinary bladder contract to expel urine from the bladder.
Production of Hormones
The kidneys produce and interact with several hormones that are involved in the control of
systems outside of the urinary system.• Calcitriol . Calcitriol is the active form of vitamin & in the human body. It is produced by the
kidneys from precursor molecules produced by / radiation striking the skin. Calcitriol works
together with parathyroid hormone (0T! to raise the level of calcium ions in the bloodstream.$hen the level of calcium ions in the blood drops below a threshold level, the parathyroid
glands release 0T!, which in turn stimulates the kidneys to release calcitriol. Calcitriol promotes
the small intestineto absorb calcium from food and deposit it into the bloodstream. It also
stimulates the osteoclasts of the seletal system to break down bone matrix to release calcium
ions into the blood.
• Erythropoietin. 1rythropoietin, also known as 102, is a hormone that is produced by the
kidneys to stimulate the production of red blood cells. The kidneys monitor the condition of the
blood that passes through their capillaries, including the oxygen3carrying capacity of the blood.
$hen the blood becomes hypoxic, meaning that it is carrying deficient levels of oxygen, cells
lining the capillaries begin producing 102 and release it into the bloodstream. 102 travels throughthe blood to the red bone marro!, where it stimulates hematopoietic cells to increase their rate
of red blood cell production. 4ed blood cells contain hemoglobin, which greatly increases the
blood#s oxygen3carrying capacity and effectively ends the hypoxic conditions.
• Renin. 4enin is not a hormone itself, but an en'yme that the kidneys produce to start the
renin3angiotensin system (4%S. The 4%S increases blood volume and blood pressure in response
to low blood pressure, blood loss, or dehydration. 4enin is released into the blood where it
cataly'es angiotensinogen from the liver into angiotensin I. %ngiotensin I is further cataly'ed by
another en'yme into %ngiotensin II.
%ngiotensin II stimulates several processes, including stimulating the adrenal cortex to producethe hormone aldosterone. %ldosterone then changes the function of the kidneys to increase the
reabsorption of water and sodium ions into the blood, increasing blood volume and raising blood
pressure. 5egative feedback from increased blood pressure finally turns off the 4%S to maintain
healthy blood pressure levels.