SURGERY OF PEPTIC ULCERATION AND ITS COMPLICATIONS fileoperation, as a form of functional dyspepsia,...
10
523 SURGERY OF PEPTIC ULCERATION AND ITS COMPLICATIONS NORMAN C. TANNER, M.D., F.R.C.S. ! Part HI Post-Gastrectomy Conditions Early post cibal symptoms. I have little to add to the vast amount which has been written on the aetiology of early post cibal symptoms or 'dumping '-that is symptoms of epigastric discomfort, sweating, flushing, palpitation and fatigue, sometimes biliary vomiting, appearing usually shortly after a meal, particularly a heavy meal in patients who have had a gastrectomy. I would, however, suggest that many of the symptoms are merely an exaggeration of the normal physiological response to over-eating. The reaction naturally comes sooner in the gastrectomized, because the capacity for taking food is reduced. Similar symptoms are occas- ionally encountered in persons who have had no operation, as a form of functional dyspepsia, and they may occur in persons who suddenly take a large meal after many hours or days of frugal meals. In prophylaxis, I commend the practice of explanation before the onset of symptoms. The sudden onset of flushing and palpitation during convalescence, shocks the patient and undermines his confidence and leads to ap- prehension and anxiety. If the patient has been told to expect these symptoms, and reassured that they will progressively diminish and that they do not imply the development of heart or other new trouble-then they are accepted calmly and are minimized rather than exaggerated. In treatment, the patient should be advised to resume normal meals as early as possible in order to hasten the time when the organism becomes adjusted to the new state of affairs. A period of recumbency should be taken if the symptoms occur, and the tea-time meal-the time when dumping is usually first complained of, should be made a small, dry, high protein, high fat meal-e.g., boiled egg, bread and butter with minimal fluid, or abandoned altogether. Certain cases are severe enough to require further surgical help. Surgery for post cibal symptoms should not; be undertaken less than a year from operation, for the symptoms usually abate with time and they may diminish even as late as after the third or fourth post-operative years. Flushing and palpitations rarely persist and the symptoms most likely to continue are biliary vomiting, which is not always post-prandial, inability to take certain articles of diet with comfort, notably milk or egg, and post-prandial diarrhoea. We have used six surgical procedures for persistent symptoms. i. Vagotomy. This was done several years ago in the belief that some of the symptoms might have been due to stimulation of vagus nerve endings in the suture line. This operation has produced no benefit in any case (eight altogether). 2. Short circuiting the afferent and efferent jejunal loops. This is done in the belief that discomfort is due to stasis of bile in the afferent jejunal loop, this belief being supported by the relief often obtained when bile is vomited. As the short circuit reduces the volume of biliary fluid entering the stomach and so increases the risk of stomal ulceration, we usually add a vagotomy. In the earlier four cases a two to three inch long stoma was made, but latterly in two cases we have used Steinberg's pantaloon operation, that is removing the whole spur between efferent and afferent loops right up to the stomach (Fig i6). This operation does diminish biliarv vomiting and tlhree of the cases were improved. None were made worse by it. 3. Conversion to a Roux type of stoma. In the Macarthur Lectures which I had the honour to deliver in Edinburgh in 1951, I mentioned the great benefit to be obtained by conversion to a Roux type of anastomosis when there was severe biliary regurgitation following end in side oesophago-jejunostomy after total gastrectomy (Tanner, I 95I). I mentioned a simple method of affecting this (Fig. I7). A similar easy method is avaailable following partial gastrectomy,? 1;ut I pointed out that there was a great risk of stomal group.bmj.com on July 8, 2017 - Published by http://pmj.bmj.com/ Downloaded from
Transcript of SURGERY OF PEPTIC ULCERATION AND ITS COMPLICATIONS fileoperation, as a form of functional dyspepsia,...
523
SURGERY OF PEPTIC ULCERATIONAND ITS COMPLICATIONS
NORMAN C. TANNER, M.D., F.R.C.S. !
Part HI
Post-Gastrectomy ConditionsEarly post cibal symptoms. I have little to add
to the vast amount which has been written on theaetiology of early post cibal symptoms or'dumping '-that is symptoms of epigastricdiscomfort, sweating, flushing, palpitation andfatigue, sometimes biliary vomiting, appearingusually shortly after a meal, particularly a heavymeal in patients who have had a gastrectomy. Iwould, however, suggest that many of thesymptoms are merely an exaggeration of thenormal physiological response to over-eating.The reaction naturally comes sooner in thegastrectomized, because the capacity for takingfood is reduced. Similar symptoms are occas-ionally encountered in persons who have had nooperation, as a form of functional dyspepsia, andthey may occur in persons who suddenly take alarge meal after many hours or days of frugalmeals. In prophylaxis, I commend the practiceof explanation before the onset of symptoms.The sudden onset of flushing and palpitationduring convalescence, shocks the patient andundermines his confidence and leads to ap-prehension and anxiety. If the patient has beentold to expect these symptoms, and reassured thatthey will progressively diminish and that theydo not imply the development of heart or othernew trouble-then they are accepted calmly andare minimized rather than exaggerated.
In treatment, the patient should be advised toresume normal meals as early as possible inorder to hasten the time when the organismbecomes adjusted to the new state of affairs. Aperiod of recumbency should be taken if thesymptoms occur, and the tea-time meal-thetime when dumping is usually first complained of,should be made a small, dry, high protein, high fatmeal-e.g., boiled egg, bread and butter withminimal fluid, or abandoned altogether.
Certain cases are severe enough to requirefurther surgical help. Surgery for post cibalsymptoms should not; be undertaken less than a
year from operation, for the symptoms usuallyabate with time and they may diminish even as lateas after the third or fourth post-operative years.Flushing and palpitations rarely persist and thesymptoms most likely to continue are biliaryvomiting, which is not always post-prandial,inability to take certain articles of diet withcomfort, notably milk or egg, and post-prandialdiarrhoea.We have used six surgical procedures for
persistent symptoms.i. Vagotomy. This was done several years ago
in the belief that some of the symptoms mighthave been due to stimulation of vagus nerveendings in the suture line. This operation hasproduced no benefit in any case (eight altogether).
2. Short circuiting the afferent and efferentjejunal loops. This is done in the belief thatdiscomfort is due to stasis of bile in the afferentjejunal loop, this belief being supported by therelief often obtained when bile is vomited. As theshort circuit reduces the volume of biliary fluidentering the stomach and so increases the risk ofstomal ulceration, we usually add a vagotomy.In the earlier four cases a two to three inch longstoma was made, but latterly in two cases we haveused Steinberg's pantaloon operation, that isremoving the whole spur between efferent andafferent loops right up to the stomach (Fig i6).This operation does diminish biliarv vomitingand tlhree of the cases were improved. None weremade worse by it.
3. Conversion to a Roux type of stoma. In theMacarthur Lectures which I had the honour todeliver in Edinburgh in 1951, I mentioned thegreat benefit to be obtained by conversion to aRoux type of anastomosis when there was severebiliary regurgitation following end in sideoesophago-jejunostomy after total gastrectomy(Tanner, I95I). I mentioned a simple method ofaffecting this (Fig. I7). A similar easy method isavaailable following partial gastrectomy,? 1;ut Ipointed out that there was a great risk of stomal
group.bmj.com on July 8, 2017 - Published by http://pmj.bmj.com/Downloaded from

524 POSTGRADUATE MEDICAL JOURNAL October 1954
A
B I
C
D
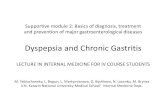
FiG. l6.-Operations designed to correct dumpingsymptoms. B-Conversion to a gastro-duodenalanastomosis. C-Jejuno-jejunostomy. D-The'Pantaloon ' operation.
-1 -ass:IsStfirp4
$J||E 1.
-
..-. q. . ...f f !i.
- i l . ss
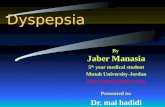
FIG. 17.-Simple methods of conversion of (i) total or(2) partial gastrectomy to a Roux form of anasto-mosis. (Note.-This diagram was also shown inEdin. med. J3. article.)
ulceration following and that it must be combinedwith vagotomy or a very high partial gastrectomymade. In a partial gastrectomy which I con-verted to a Roux form combined with vagotomyin 1950, there was no benefit, and I have sinceconverted him to a Billroth I type of anastomosis.My colleague, Mr. Andrew Desmond, did twoothers and there is a suspicion of stomal ulcera-tion in both.
4. Capper and Butler (1951) suggest thatdumping symptoms are due to drag on theoesophagus and lesser curve of the stomach by theweight of the filled stomach and adjacent jejunum,and suggest stitching up the gastric stump to theleft gastric pedicle and to the gastrosplenicomentum, both as a means of prophylaxis and oftreatment. We used it nine 'times in prophylaxis,and three times in treatment. One of the latterhad temporary relief but relapsed after fourmonths, and two had no relief at all. (Veryadequate suspension was later confirmed at afurther operation in two cases.) The prophylacticsuspension was added in nine cases. Five haveno dumping, two have developed mild post cibalsymptoms (one with biliary vomiting), one hasfullness after meals and attacks of diarrhoea and
group.bmj.com on July 8, 2017 - Published by http://pmj.bmj.com/Downloaded from

October 1954 TANNER: Surgery of Peptic Ulceration and its Complications 525
CONVERSION TO BILLROTH I FOR DUMPINGNo. followed-up, three month to four years .. .. .. 21Very satisfactory .. .. .. .. .. .. .. 10Much improved .. .. .. .. .. .. .. 5Improved .. .. .. 3I.S.Q . .. .. .. .. .. .. .. 3Worse .. . . . . . . .
one has late hypoglycaemic-like attacks. Thesesymptoms will probably be transitory, but onthe whole, judging by this very small series thereis no great improvement
5. Although we found the gastro-duodenalform of anastomosis after gastrectomy to lead tonearly as many cases of dumping as the gastro-jejunal anastomosis, they seemed to be less severeforms. Consequently, since 1948 we have triedthe effect of conversion from gastro-jejunal to agastro-duodenal anastomosis in some 26 cases.There was an operative death in a man withmitral stenosis, and one patient died since returning to his home from pulmonary tuberculosis,from which he was known to have sufferedpreviously. Three have less than three monthsfollow up, leaving 21 -cases carried out betweenthree months and four years ago.The three patients not improved by conversion
to a Billroth I anastomosis included one who hadpreviously had a Roux operation, and one patientwho was at first remarkably well, now has con-siderable financial and domestic troubles andrelapsed.
This method can be quite dramatic in its goodeffects. It relieves biliary vomiting and diminishesor abolishes diarrhoea. Some patients who wereunable to take milk or egg can now take it withcomfort. It is our only present reasonably satis-factory solution to the problem.
6. The last method of treatment is by jejunalor colonic replacement of the stomach. We usedthe jejunal method with considerable doubt andtrepidation in three cases. In two the conversionwas carried out for cases of dumping associatedwith a gastro-jejunal stoma. The operation itselfis delightfully simple. Both cases had immediaterelief of their symptoms and one remains verywell at eight months and has gained eleven poundsin weight. The second began to get severe ulcerpain within six weeks and gastroscopy four monthsafter operation showed extensive jejunal ulcera-tion. At re-operation the replacing loop ofjejunum was extensively ulcerated, and so it wasremoved and a Billroth I form of anastomosismade instead. The patient still remains free ofhis dumping symptoms and this helps to confirmmy belief that the major benefit of jejunal andprobably of colonic replacement is the re-directionof gastric chyme through the duodenum. Therisk of stomal ulceration is less with colonic
replacement, probably because the reverse peri-stalsis of the colonic loop carries duodenal juicesinto the stomach. Moroney (i -)has mentionedthis point. The jejunal loop might be safer if putin reverse! A third case was one of ' inability totake big meals and loss of weight,' in a womanaged 47. She had already had a high Billroth Ianastomosis for gastric ulceration, and this seemedas suitable a case as any for enlarging the stomachby the insertion of a jejunal loop between thestomach and duodenum. She made a goodrecovery but her symptoms remain quite un-changed.
This small but interesting series of three casesshows that jejunal replacement is easy to do butdangerous in view of the risk of post-operativeulceration. I believe its main benefit is that itreturns the gastric chyme through the duodenumagain. This can be done more simply by con-version to a Billroth I operation.To sum up. I am not of the opinion that the
earlv post-cibal or dumping symptoms are suffi-ciently frequent or severe enough to cause alarm.They can, however, be disturbing in a certainsmall group of cases. The severity of the dis-turbance can be minimized by warning the patientthat these attacks are likely to arise for a limitedspace of time. In our own series we found theattacks less common after the gastro-duodenal andantecolic gastro-jejunal anastomosis, and so wefavour these operations on that account. If theattacks do develop, it is reasonable to reassure thepatient, for the severity of the attacks diminisheswith time.
Further surgery should on no account take placeless than a year after operation, because o£ -thetendency of the symptoms to abate.
Before operating a second tiune for post-cibal.symptoms there is one piece of advice I wouldgive most earnestly, and it is this. Look up thefirst notes of the patient-read the letter sent byhis doctor when he first came. This may be arevelation. There is an all too facile tendency toattribute to a gastrectomy all the ills that subse-quently befall the patient. In two of my very worstso-called post-gastrectomy dumping cases, I studiedthe earliest symptoms and found that the fatigue,and bloating after meals, palpitations and feelingsof weakness were all complained of prior- to thegastrectomy-in addition to the ulcer symptomsand only the ulcer symptoms had been cured by
group.bmj.com on July 8, 2017 - Published by http://pmj.bmj.com/Downloaded from

5z6 ,,.POSTGRADUATE MEDICAL. JQURNAL October I954
OPERATIONS FOR 'DUMPING SYMPTOMSOperation No. Results
I. Vagotomy .. .. .. .. .. .. .. 4 -All failed2. Jejuno-jejunostomy:
(a) Alone .. .. .. .. .. 2 i cured, I I.S.Q.(b) P'us vag(otomy .. .. .. .. .. .. 2 2 failed(c) Pantaloon operation .. .. .. .. .. 2 I cured, i improved
3. Roux conversion (2 plus vagotomy) .. .. .. 3 i well but anaemia,I stomal ulcer, II.S.Q.
4. Capper suspension .. .. .. .. .. 3 All failed5. Conversion to Billroth I .. .. .. .. 26 See below.6. Jejunal transplant after Billroth I .. .. .. .. I Failed
the gastric resection. Needless to say, technicalvariations in the operation will not relieve suchpatients. Furthermore, two of my old gastrec-tomy patients who developed carcinomas were fora time returned to us as cases of post-cibal symp-toms. Carcinoma of other organs than the stomachshould be considered when old gastrectomy caseslose weight severely or become suddenly anaemic.Of course it is possible for carcinoma to developin the gastric stump, for B. F. Swynnerton andN. C. Tanner (I953) record that four patients outof 254 developed cancer in the gastric remnantbletween five and twelve years after gastrectomyfor simple gastric ulcer.Now if it is found that the dumping symptoms
are truly consequent on the gastric resection, andparticularly if much biliary vomiting or weightloss is complained of, then further surgery can beconsidered. The procedure we have found mostsatisfactory is conversion of a gastro jejunal into agastro-duodenal anastomosis. If the dumpingpersists after a Billroth I form of anastomosis, thenno surgery is advisable unless it can be shown thatthere is recurrent ulceration, stomal obstruction ora mechanical defect.
Anaemia Following GastrectomyIt is well known that iron deficiency anaemia
is common in patients with achlorhydria and wecannot expect to reduce the gastric acidity radicallywithout getting diminution of the powers of ironabsorption. My friend, Mr. Harold Burge of theWest London Hospital has surveyed large numbersof our cases and his own and finds that there is atendency for the blood haemoglobin percentage tofall with each year following partial gastrectomy.He has kindly placed this Table at my disposal.
* GASTRECTOMY FOR SIMPLE PEPTIC ULCERMale Cases
(50 cases examined in each year)Years after Gastrectomy
I 2 34 5 6.Igb. below: % % % O/<r ) %*85% X2 12 22 32 j38.585% 6 8 IO 20 26 367% - 2 6 4 14 I8 24.70% 0 00 4 6 i8
In all these cases the anaemia was microcyticand responded to iron therapy, though it wouldgradually relapse if iron was discontinued. Mr.Burge made similar careful examination of a groupof female cases and found the same trend, thoughas might be expected, it was more exaggerated,e.g., at the end of five years 84 per cent. had ahaemoglobin below 85 per cent.We advise our gastrectomized patients to take
iron-containing foods and warn them of thesymptoms of iron deficiency anaemia. In thefollow-up of 6ii of our gastrectomy patients byCraig and Chippendale, I2 were suffering from, orhad been treated for a microcytic anaemia, anincidence which was not significantly greater thanthat among patients without operation.
I have seen only one macrocytic anaemiafollowing one of our gastrectomies.. This was apatient who had had a total gastrectomy, splen-ectomv and hemi-pancreatectomy for carcinoma.He was very well and had a blood count withinnormal limits for six years after operation and thenquite suddenly became anaemic, and the anaemiawas found to be a macrocytic one.
Weight Loss following GastrectomyThe cases of weight loss following gastrectomy.
usually result from diminished intake of foodrather than any deficiency of fat digestion. (Brainand Stammers (I95i).) Thus the comfortablepatient usually maintains or gains weight, but ifthere is some post-prandial fullness, dumping,biliary regurgitation, pain or stenosis from stomalulceration, then intake is restricted and the weightmay fall., The treatment of weight loss is to treatany of these causative lesions and to encouragethe intake of a high calorie diet. In our afore-mentioned series of 6i i gastrectomies it was foundthat compared with their best or normal weight,244 (53 per cent.) had gained weight, i6o (34 percent.) had lost up to one stone and 6o (I3 percent.) were more than a stone under weight. Theantecolic valved gastro-jejunal type of operationgave the greatest gain of weight, but there was nota great deal of difference in the three -groups.(57.8 per cent. antecolic ' Polya,' 50o pdr cent.
group.bmj.com on July 8, 2017 - Published by http://pmj.bmj.com/Downloaded from
October 1954 TANNER: Surgery of Peptic Ulceration and its Complications 527
Billroth I and 46 per cent. retrocolic ' Polva'gained or maintained weight.)
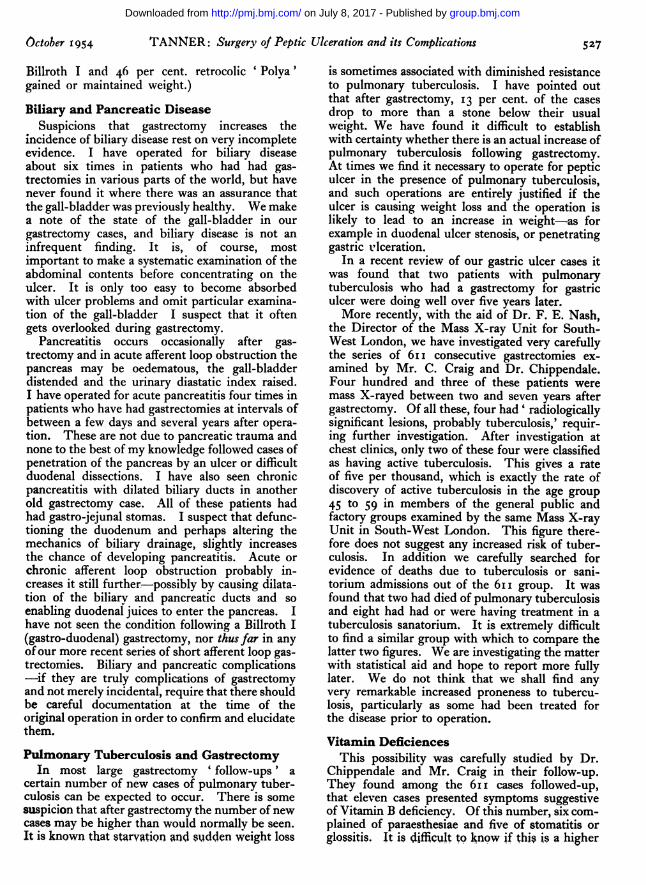
Biliary and Pancreatic DiseaseSuspicions that gastrectomy increases the
incidence of biliary disease rest on very incompleteevidence. I have operated for biliary diseaseabout six times in patients who had had gas-trectomies in various parts of the world, but havenever found it where there was an assurance thatthe gall-bladder was previously healthy. We makea note of the state of the gall-bladder in ourgastrectomy cases, and biliarv disease is not aninfrequent finding. It is, of course, mostimportant to make a systematic examination of theabdominal contents before concentrating on theulcer. It is only too easy to become absorbedwith ulcer problems and omit particular examina-tion of the gall-bladder I suspect that it oftengets overlooked during gastrectomy.
Pancreatitis occurs occasionally after gas-trectomy and in acute afferent loop obstruction thepancreas may be oedematous, the gall-bladderdistended and the urinary diastatic index raised.I have operated for acute pancreatitis four times inpatients who have had gastrectomies at intervals ofbetween a few days and several years after opera-tion. These are not due to pancreatic trauma andnone to the best of my knowledge followed cases ofpenetration of the pancreas by an ulcer or difficultduodenal dissections. I have also seen chronicpancreatitis with dilated biliary ducts in anotherold gastrectomy case. All of these patients hadhad gastro-jejunal stomas. I suspect that defunc-tioning the duodenum and perhaps altering themechanics of biliary drainage, slightly increasesthe chance of developing pancreatitis. Acute orchronic afferent loop obstruction probably in-creases it still further;-possibly by causing dilata-tion of the biliarv and pancreatic ducts and soenabling duodenal juices to enter the pancreas. Ihave not seen the condition following a Billroth I(gastro-duodenal) gastrectomy, nor thus far in anyofour more recent series of short afferent loop gas-trectomies. Biliary and pancreatic complications-if they are truly complications of gastrectomyand not merely incidental, require that there shouldbe careful documentation at the time of theoriginal operation in order to confirm and elucidatethem.
Pulmonary Tuberculosis and GastrectomyIn most large gastrectomy ' follow-ups ' a
certain number of new cases of pulmonary tuber-culosis can be expected to occur. There is somesuspicion that after gastrectomy the number of newcases may be higher than would normally be seen.It is known that starvatiQn and sudden weight loss
is sometimes associated with diminished resistanceto pulmonary tuberculosis. I have pointed outthat after gastrectomy, 13 per cent. of the casesdrop to more than a stone below their usualweight. We have found it difficult to establishwith certainty whether there is an actual increase ofpulmonary tuberculosis following gastrectomy.At times we find it necessary to operate for pepticulcer in the presence of pulmonary tuberculosis,and such operations are entirely justified if theulcer is causing weight loss and the operation islikely to lead to an increase in weight-as forexample in duodenal ulcer stenosis, or penetratinggastric ulceration.
In a recent review of our gastric ulcer cases itwas found that two patients with pulmonarytuberculosis who had a gastrectomy for gastriculcer were doing well over five years later.More recently, with the aid of Dr. F. E. Nash,
the Director of the Mass X-ray Unit for South-West London, we have investigated very carefullythe series of 6II consecutive gastrectomies ex-amined by Mr. C. Craig and Dr. Chippendale.Four hundred and three of these patients weremass X-rayed between two and seven years aftergastrectomy. Of all these, four had' radiologicallysignificant lesions, probably tuberculosis,' requir-ing further investigation. After investigation atchest clinics, only two of these four were classifiedas having active tuberculosis. This gives a rateof five per thousand, which is exactly the rate ofdiscovery of active tuberculosis in the age group45 to 59 in members of the general public andfactory groups examined by the same Mass X-rayUnit in South-West London. This figure there-fore does not suggest any increased risk of tuber-culosis. In addition we carefully searched forevidence of deaths due to tuberculosis or sani-torium admissions out of the 6ii group. It wasfound that two had died of pulmonary tuberculosisand eight had had or were having treatment in atuberculosis sanatorium. It is extremely difficultto find a similar group with which to compare thelatter two figures. We are investigating the matterwith statistical aid and hope to report more fullylater. We do not think that we shall find anyvery remarkable increased proneness to tubercu-losis, particularly as some had been treated forthe disease prior to operation.
Vitamin DeficiencesThis possibility was carefully studied by Dr.
Chippendale and Mr. Craig in their follow-up.They found among the 6i i cases followed-up,that eleven cases presented symptoms suggestiveof Vitamin B deficiency. Of this number, six com-plained of paraesthesiae and five of stomatitis orglossitis. It is difficult to know if this is a higher
group.bmj.com on July 8, 2017 - Published by http://pmj.bmj.com/Downloaded from

528 POSTGRADUATE MEDICAL JOURNAL October 1954
A
B
-II
| Ei|g1-lwl
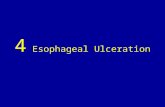
FIG. i8.-The Heineke-Mikulicz py-loroplasty. A-The deformity dueto duodenal ulceration, note thediverticula between pylorus andthe ulcer scar. B-A longitudinalincision through pylorus and scaris pulled out transversely. C-Theincision is sutured transversely.
CI
group.bmj.com on July 8, 2017 - Published by http://pmj.bmj.com/Downloaded from

October I954 TANNER: Surgery of Peptic Ulceration and its Complications 529
number than might be expected in an examina-tion of 515 people in these age groups. Thefinding is to my mind on a par with that of theiron deficiency anaemia. In order to cure theulcer we have lowered the hydrochloric acid con-centration in the stomach. We know that in thepresence of hypoacidity, iron and vitamin absorp-tion may be impaired. It is, therefore, not sur-prising that a small percentage of these cases willget iron or Vitamin B deficiency. It is wise, Ithink, to advise the gastrectomized patient to takea slight excess of iron and Vitamin B in the diet,in order to compensate for this deficiency. It isfortunate that the deficiency can be so readilyovercome.
Vagotomy for Duodenal UlcerI mentioned in my first lecture that vagotomy
is still under trial in the treatment of duodenalulceration. In I943 I carried out two or threepartial vagotomies combined with fundusectomy,but it did not appear to be verv effective. In 1947being convinced that complete vagal section hadgreat potentialities for benefit to the ulcer patient,we felt it our duty to try to assess the operationas rapidly and as scientifically as possible. Inorder to be sure that anv beneficial effects were infact due to the vagotomy, we decided to use purevagotomy without accessory operations in a fairlyunselected series of duodenal ulcer cases. In caseswhere there was gross duodenal stenosis, correc-tion of the mechanical defect was imperative andso we added a Heineke Mikulicz pyloroplasty inthese cases (Fig. i8a, b and c). Our previousexperiences of simple pyloroplasty for duodenalulcer were enough to persuade us that it was nota curative operation and that any beneficial resultsfrom the combination could be safely attributedto the vagotomy.
Following this programme we soon came intotrouble, for although those who needed a pyloro-plasty did well on the whole, some of those whosimply had a vagotomy suffered greatly fromgastric retention, foul sulphurous belching andsome had diarrhoea. This led to a good deal ofpersonal discomfort and domestic upset to thepatients, and it is well known that many surgeonsabandoned the vagotomy operation altogether onthis account. It appeared to us, however, thatthis condition which is also seen in cases ofobstructive oesophageal or gastric cancer, was dueto the combination of hypoacidity with gastricstatis. In a way it revealed the effectivity ofvagotomy. We decided that one of these factors,obviously the stasis, must be overcome. Con-sequently, in I948 we decided that we mustabandon simple vagotomy, and thereafter we addeda pyloroplasty in all cases, for we found to our
surprise that this simple procedure greatly ex-pedited gastric evacuation, even in those withoutthe slightest duodenal narrowing. This removedmost of the trouble. A Finney type of pyloro-plasty was necessary in two children whose de-formity was considered to be too extreme for theHeineke Mikulicz operation. We used gastro-jejunostomy in a few cases where the duodenumwas extensively damaged, though we avoided it asa routine, because although it may well eventuallyprove to be the most satisfactory addition tovagotomy, it would have clouded the issue as itis itself curative of the duodenal ulcer.
Technique of VagotomyThe results of vagotomy depend on a scrupulous
technique. The transthoracic approach is un-suitable because the nature of the lesion cannotbe confirmed, and the so-called drainage operation,the pyloroplasty, cannot be added. We use a highabdominal approach, sometimes removing thexiphisternum and then reflect the left lobe of theliver to the right, after dividing the left triangularligament. The oesophagus is exposed by a trans-verse incision through the two distinct layers overit, the peritoneum and the phreno-oesophagealligament. In order to steady the oesophagus it isusual to put a tractor tape round it. I gave upthis practice because I feared it might increase theliability to cardiospasm and because it obscuresthe lower vagal branches. Instead I pass a rubberband through the lesser omentum into, and thenthrough the roof of the lesser sac over the fundusof the stomach to the left of the oesophagus(Fig. I9). On drawing this down the branches ofthe anterior vagus nerve to the body and lessercurve of the stomach and to the liver can be easilydissected and the branch of the posterior vagusto the coeliac artery can be readily palpated. Thenerves are cuit well down on the stomach afterthey have divided into branches, and also as highas can be reached through the oesophageal hiatus.After carefully searching for any accessory vagusfibres, the opening in the phreno-oesophagealligament is closed to prevent subsequent hiatusherniation. Following this the pyloroplasty iscarried out.
Like many others we made several earlyfollows-up which showed reasonably satisfactoryresults, but the results were confusing because ofthe number of recent cases. I really do not thinkwe should draw conclusions on anything less thana five year follow-up, and that is why, when I amasked ' What is the place of vagotomy in thetreatment of duodenal ulcer ? ' I have to answerthat I do not know. However, the reply to thequestion is slowly emerging. On the fifthanniversary of their operation, all our vagotomy
group.bmj.com on July 8, 2017 - Published by http://pmj.bmj.com/Downloaded from

POSTGRADUATE MEDICAL JOURNAL October 1954
m..........
FIG. I9.-The author's method of traction over the gastric fundus-whichallows good exposure of the branches of the vagus nerve.
cases come to the hospital for careful assessment byDr. Brian Swynnerton, our Weir ResearchAssistant. The results to date or prior to anysecondary operation, containing as they do mainlyour early pure vagotomy cases, do little more thanconfirm our dissatisfaction with that operation.(The Visick classification is used.)
TABLE I
Simple Vagotomy for Duodenal Ulcer(No secondary operations)
Number of cases .. .. .. ..55Died since (not of ulcer) .. .. 2Very satisfactory .. .. .. .. 19 35.8%Minor symptoms not controlled by care
(IIIs) . 5 9.4%Unsatisfactory (IIIu) ,,29 54.7%
The causes of the poor results were as follows:
TABLE IA
Gastric retention 19Active recurrent duodenal ulceration 4Ulcer-type pain, scar only at later operation 4Later gastric ulcerMiscellaneous I
NOTE.-Of the 29 unsatisfactory cases, 27 have hadsubsequent operations (1I3 pyloroplasty, 7 gastro-jejunostomy and i i partial gastrectomy).
The final state of the 53 surviving simplevagotomies with their various drainage and re-section operations is as follows:
group.bmj.com on July 8, 2017 - Published by http://pmj.bmj.com/Downloaded from
October I 954 TANNER: Surgery of Peptic Ulceration and its Complications 531
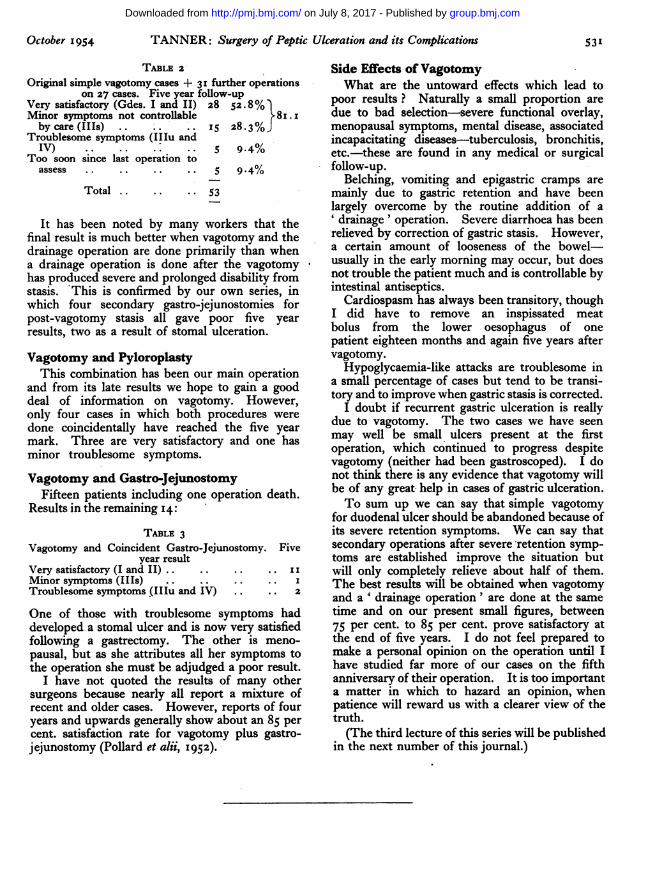
TABLE 2
Original simple vagotomy cases + 3' further operationson 27 cases. Five year follow-up
Very satisfactory (Gdes. I and II) 28 52.8%Minor symptoms not controllable 8i.Iby care (IIIs) .. .. .. IS 28.3%J
Troublesome symptoms (IIIu andIV) * .* . 5 9.4%
Too soon since last operation toassess . .. .. .. 5 9.4%
Total .. .. .. 53
It has been noted by many workers that thefinal result is much better when vagotomy and thedrainage operation are done primarily than whena drainage operation is done after the vagotomyhas produced severe and prolonged disability fromstasis. This is confirmed by our own series, inwhich four secondary gastro-jejunostomies forpost-vagotomy stasis all gave poor five yearresults, two as a result of stomal ulceration.
Vagotomy and PyloroplastyThis combination has been our main operation
and from its late results we hope to gain a gooddeal of information on vagotomy. However,only four cases in which both procedures weredone coincidentally have reached the five yearmark. Three are very satisfactory and one hasminor troublesome symptoms.
Vagotomy and Gastro-JejunostomyFifteen patients including one operation death.
Results in the remaining I4:TABLE 3
Vagotomy and Coincident Gastro-Jejunostomy. Fiveyear result
Very satisfactory (I and II) .. .. .. .. IIMinor symptoms (IIIs) .. .. .. .. ITroublesome symptoms (IIIu and IV) .. .. 2
One of those with troublesome symptoms haddeveloped, a stomal ulcer and is now very satisfiedfollowing a gastrectomy. The other is meno-pausal, but as she attributes all her symptoms tothe operation she must be adjudged a poor result.
I have not quoted the results of many othersurgeons because nearly all report a mixture ofrecent and older cases. However, reports of fouryears and upwards generally show about an 85 percent. satisfaction rate for vagotomy plus gastro-jejunostomy (Pollard et alii, 1952).
Side Effects ofVagotomyWhat are the untoward effects which lead to
poor results ? Naturally a small proportion aredue to bad selection-severe functional overlay,menopausal symptoms, mental disease, associatedincapacitating diseases-tuberculosis, bronchitis,etc.-these are found in any medical or surgicalfollow-up.
Belching, vomiting and epigastric cramps aremainly due to gastric retention and have beenlargely overcome by the routine addition of a' drainage ' operation. Severe diarrhoea has beenrelieved by correction of gastric stasis. However,a certain amount of looseness of the bowel-usually in the early morning may occur, but doesnot trouble the patient much and is controllable byintestinal antiseptics.
Cardiospasm has always been transitory, thoughI did have to remove an inspissated meatbolus from the lower oesophagus of onepatient eighteen months and again five years aftervagotomy.
Hypoglycaemia-like attacks are troublesome ina small percentage of cases but tend to be transi-tory and to improve when gastric stasis is corrected.
I doubt if recurrent gastric ulceration is reallydue to vagotomy. The two cases we have seenmay well be small ulcers present at the firstoperation, which continued to progress despitevagotomy (neither had been gastroscoped). I donot think there is any evidence that vagotomy willbe of any great help in cases of gastric ulceration.To sum up we can say that simple vagotomy
for duodenal ulcer should be abandoned because ofits severe retention symptoms. We can say thatsecondary operations after severe -retention symp-toms are established improve the situation butwill only completely relieve about half of them.The best results will be obtained when vagotomyand a ' drainage operation' are done at the sametime and on our present small figures, between75 per cent. to 85 per cent. prove satisfactory atthe end of five years. I do not feel prepared tomake a personal opinion on the operation until Ihave studied far more of our cases on the fifthanniversary of their operation. It is too importanta matter in which to hazard an opinion, whenpatience will reward us with a clearer view of thetruth.(The third lecture of this series will be published
in the next number of this journal.)
group.bmj.com on July 8, 2017 - Published by http://pmj.bmj.com/Downloaded from

and its Complications: Part IISurgery of Peptic Ulceration
Norman C. Tanner
doi: 10.1136/pgmj.30.348.5231954 30: 523-531 Postgrad Med J
nhttp://pmj.bmj.com/content/30/348/523.citatioat: Updated information and services can be found
These include:
serviceEmail alerting
corner of the online article. this article. Sign up in the box at the top right Receive free email alerts when new articles cite
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on July 8, 2017 - Published by http://pmj.bmj.com/Downloaded from