Spontaneous Fragmentation of Indwelling Ureteral …...Ahmed R, Elshal Ahmed, Shokeir Ahmed A....
2
Cite this article: Shapiro M, Deters L (2016) Spontaneous Fragmentation of Indwelling Ureteral Stent after Three Decades. J Clin Nephrol Res 3(3): 1038. Central Journal of Clinical Nephrology and Research *Corresponding author Michael Shapiro, University of Washington School of Medicine, 925 Cherry, St. Apt. 304 Seattle, WA 98104, USA, Tel: 206-200-4092; Email: Submitted: 08 March 2016 Accepted: 28 March 2016 Published: 28 March 2016 ISSN: 2379-0652 Copyright © 2016 Shapiro et al. OPEN ACCESS Clinical Image Spontaneous Fragmentation of Indwelling Ureteral Stent after Three Decades Michael Shapiro 1 * and Levi Deters 2 1 University of Washington School of Medicine, USA 2 Spokane Urology, USA A 54 year-old gentleman with a medical history of nephrolithiasis presents with lower abdominal pain and gross hematuria. Thirty years ago the patient was diagnosed and treated for a right ureteropelvic junction obstruction, and a stent was placed at this time with a plan for repair with pyeloplasty. The patient was lost to follow-up and failed to have the temporary stent removed. Upon evaluation a CT scan revealed fragmentation of the stent within the right ureter and formation of a right staghorn stone with a greater than 6 cm stone burden and significant right parenchymal thinning, as well as a left renal stone of approximately 1.5 cm and an 8 cm bladder calculus. Within both the renal pelvis and the bladder there also appeared to be stent remnants. Ureteral stents are routinely used in the treatment of conditions such as nephrolithiasis and ureteral strictures or in this case to temporize an ureteropelvic junction obstruction until it can be repaired, usually with a pyeloplasty. Although designed to be temporary, patients are often lost to follow-up, and the indwelling stents can become encrusted. Patients with encrusted stents often present with flank pain with costovertebral angle tenderness, as well as hematuria, dysuria, and even stenturia [1]. Stent encrustation can lead to complications such as infection, hematuria, decreased renal function, and massive stone formation [2]. Rarely, if stents continue to encrust, spontaneous fragmentation can occur, with a staghorn stone forming in the renal pelvis and a large stone forming in the bladder around the distal end of the stent [3]. In order to prevent retained stents, patients are educated about the temporary nature of the stent, and often a stent registry is kept by the urologist’s office to help track patients with indwelling stents. Several methods are currently being pursued to prevent stent encrustation. These include coating stents with various glycosaminoglycans to reduce crystal growth and aggregation, as well as using oxalate- degrading enzyme coatings to break-down encrustation as it occurs [4]. Currently there are many options for management of patients with large renal and bladder stone burdens, which traditionally utilize both a transurethral and percutaneous approach, with a percutaneous nephrolithotomy and cystolithalopaxy respectively. Quantifying stone burden Figure 1 KUB showing retained fractured stent with significant renal and bladder stone burden. Figure 2 (A)–Radiogram of renal portion of retained stent with staghorn stone formation. (B) – CT of renal portion of retained stent with staghorn stone formation. through width of encrustation multiplied by length along stent may have prognostic significance, with a stone burden of over 40cm 2 generally regarded as severe and requiring a multimodal approach [4]. A recent study [5] confirms that even with severe stone burden, endoscopic management is possible, avoiding the morbidity of open surgery. Of note, the patient in this report
Transcript of Spontaneous Fragmentation of Indwelling Ureteral …...Ahmed R, Elshal Ahmed, Shokeir Ahmed A....

Cite this article: Shapiro M, Deters L (2016) Spontaneous Fragmentation of Indwelling Ureteral Stent after Three Decades. J Clin Nephrol Res 3(3): 1038.
CentralBringing Excellence in Open Access
Journal of Clinical Nephrology and Research
*Corresponding authorMichael Shapiro, University of Washington School of Medicine, 925 Cherry, St. Apt. 304 Seattle, WA 98104, USA, Tel: 206-200-4092; Email:
Submitted: 08 March 2016
Accepted: 28 March 2016
Published: 28 March 2016
ISSN: 2379-0652
Copyright© 2016 Shapiro et al.
OPEN ACCESS
Clinical Image
Spontaneous Fragmentation of Indwelling Ureteral Stent after Three DecadesMichael Shapiro1* and Levi Deters2
1University of Washington School of Medicine, USA2Spokane Urology, USA
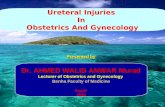
A 54 year-old gentleman with a medical history of nephrolithiasis presents with lower abdominal pain and gross hematuria. Thirty years ago the patient was diagnosed and treated for a right ureteropelvic junction obstruction, and a stent was placed at this time with a plan for repair with pyeloplasty. The patient was lost to follow-up and failed to have the temporary stent removed. Upon evaluation a CT scan revealed fragmentation of the stent within the right ureter and formation of a right staghorn stone with a greater than 6 cm stone burden and significant right parenchymal thinning, as well as a left renal stone of approximately 1.5 cm and an 8 cm bladder calculus. Within both the renal pelvis and the bladder there also appeared to be stent remnants.
Ureteral stents are routinely used in the treatment of conditions such as nephrolithiasis and ureteral strictures or in this case to temporize an ureteropelvic junction obstruction until it can be repaired, usually with a pyeloplasty. Although designed to be temporary, patients are often lost to follow-up, and the indwelling stents can become encrusted. Patients with encrusted stents often present with flank pain with costovertebral angle tenderness, as well as hematuria, dysuria, and even stenturia [1]. Stent encrustation can lead to complications such as infection, hematuria, decreased renal function, and massive stone formation [2]. Rarely, if stents continue to encrust, spontaneous fragmentation can occur, with a staghorn stone forming in the renal pelvis and a large stone forming in the bladder around the distal end of the stent [3]. In order to prevent retained stents, patients are educated about the temporary nature of the stent, and often a stent registry is kept by the urologist’s office to help track patients with indwelling stents. Several methods are currently being pursued to prevent stent encrustation. These include coating stents with various glycosaminoglycans to reduce crystal growth and aggregation, as well as using oxalate-degrading enzyme coatings to break-down encrustation as it occurs [4].
Currently there are many options for management of patients with large renal and bladder stone burdens, which traditionally utilize both a transurethral and percutaneous approach, with a percutaneous nephrolithotomy and cystolithalopaxy respectively. Quantifying stone burden
Figure 1 KUB showing retained fractured stent with significant renal and bladder stone burden.
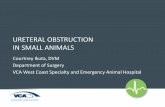
Figure 2 (A)–Radiogram of renal portion of retained stent with staghorn stone formation. (B) – CT of renal portion of retained stent with staghorn stone formation.
through width of encrustation multiplied by length along stent may have prognostic significance, with a stone burden of over 40cm2 generally regarded as severe and requiring a multimodal approach [4]. A recent study [5] confirms that even with severe stone burden, endoscopic management is possible, avoiding the morbidity of open surgery. Of note, the patient in this report

CentralBringing Excellence in Open Access
Shapiro et al. (2016)Email:
J Clin Nephrol Res 3(3): 1038 (2016) 2/2
Shapiro M, Deters L (2016) Spontaneous Fragmentation of Indwelling Ureteral Stent after Three Decades. J Clin Nephrol Res 3(3): 1038.
Cite this article
still defers intervention. We believe this case report illustrates an interesting natural course of a stent retained for over three decades with spontaneous fragmentation.
REFERENCES1. Chua Michael E, Morales Marcelino L. “Spontaneous Fracture of
Indwelling Polyurethane Ureteral Stents: A Case Series and Review of Literature.” Can Urol Assoc J. 2012; 6: 386–392.
2. Zahran Mohamed H, Harraz Ahmed M, Taha Diaa-Eldin, EL-Nahas Ahmed R, Elshal Ahmed, Shokeir Ahmed A. “Studying the Morbidity and Renal Function Outcome of Missed Internal Ureteral Stents: A Matched Pair Analysis.” Journal of Endourology. 2015; 29: 1070-1075.
3. Papo J, Waizbard E, Merimsky E. Spontaneous breakage of a double pigtail stent and bladder stone formation. J Urol (Paris). 1986; 92: 617-619.
4. Vanderbrink Brian A, Rastinehad Ardeshir R, OstMichael C, Smith Arthur D. J Endourol. 2008; 22: 905-912.
5. Whetstone Joseph L, Smaldone Marc C, Gibbons Erin P, Jackman Stephen V. “Complete ureteral stent encrustation managed with serial nephroscopy and laser lithotripsy.” Urology. 2007; 69: 576.
Figure 3 (A) – Radiogram of retained bladder stent with stone formation. (B) – CT of retained bladder stent with stone formation.