Pathology of Cholestasis
4
a oogy o oes ass Cholestasis Bile f ormation Bile flow Definition Histopathologic Clinical Bile within elements of liver Associated with secondary cell injury Substances normally excreted into bile are retained Causes of Cholestasis Hepatocellular Type Obstructive Type Hepatocellula r dysfunc tion Intra-hepatic obstruction (small bile duct) Extra-hepatic obstruction (large bile duct) Hepatitis Alcoholic liver disease Primary biliary cirrhosis -1 antitrypsin deficiency Inborn errors of bile acid synthesis Drug induced cholestasis Progressive familial intrahepatic cholestasis Stones in common bile duct Pancreatic tumour Biliary atresia Choledocal cyst Cholelithiasis Primary sclerosing choleangitis Alagille syndrome Pregnancy Sensitivity of bile ducts to estrogen Cholestasis y Often develops during 2 nd , 3 rd trimesters of pregnancy y 2 nd most common cause of jaundice during pregnancy y Generalized itching (pruritus gravidarum) (only symptom experienced) y Run in families y Symptoms disappear within 2-4 weeks after babys birth May reappear if pregnant again y Birth control pills (symptoms disappear after women stop using) Neonatal Jaundice Physiological Pathological Phase 1 Term infants y Jaundice lasts for 5 days y Bilirubin Perterm infants y Jaundice lasts for a week y Bilirubin Phase 2 Bilirubin decline for 2 weeks Preterm infants y Last more than 1 month Babies who receive exclusive breast feeding y Last more than 1 month Clinical jaundice appearing in 1 st 24h Bilirubin Hyperbilirubinemia Bile Duct Normal Biliary Obstruction Bile Secretion Normal Abnormal Cholestasis Retention of bile salts Results in injury to biological membranes throughout body Liver (most affected) Retention of hydrophobic bile salts (results in their incorporation into membranes) Alter membrane fluidity, function Bile salt injure hepatocyte membranes (important amplifier of cholestasis) Retention of secondary cholesta tic bile acids (eg. l ithocholi c acid) Results in further membrane injury Retention of cholesterol Cholesterol content of membranes Fluidity Impair function of integral membrane proteins Further retention of damaging substances Accelerated membrane injury, dysfunction Generalized failure of excretory mechanism for bile
Transcript of Pathology of Cholestasis

8/6/2019 Pathology of Cholestasis
http://slidepdf.com/reader/full/pathology-of-cholestasis 1/3
a o ogy o o es as s
Cholestasis
Bile formation
Bile flow
Definition
Histopathologic Clinical
Bile within elements of liver
Associated with secondary cell injury
Substances normally excreted into
bile are retained
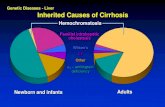
Causes of Cholestasis
Hepatocellular Type Obstructive Type
Hepatocellular dysfunction Intra-hepatic obstruction
(small bile duct)Extra-hepatic obstruction
(large bile duct)
Hepatitis
Alcoholic liver disease
Primary biliary cirrhosis
-1 antitrypsin deficiency
Inborn errors of bile acid synthesis
Drug induced cholestasis
Progressive familial intrahepatic
cholestasis
Stones in common bile duct
Pancreatic tumour
Biliary atresia
Choledocal cyst
Cholelithiasis
Primary sclerosing choleangitis
Alagille syndrome
Pregnancy
Sensitivity of bile ducts to estrogen
Cholestasis
y Often develops during 2nd
, 3rd
trimesters of pregnancy
y 2nd
most common cause of jaundice during pregnancy
y Generalized itching (pruritus gravidarum) (only symptom experienced)
y Run in families
y Symptoms disappear within 2-4 weeks after babys birth
May reappear if pregnant again
y Birth control pills (symptoms disappear after women stop using)
Neonatal Jaundice
Physiological Pathological
Phase 1
Term infants
y Jaundice lasts for 5 days
y Bilirubin
Perterm infants
y Jaundice lasts for a week
y Bilirubin
Phase 2
Bilirubin decline for 2 weeksPreterm infants
y Last more than 1 month
Babies who receive exclusive breast
feeding
y Last more than 1 month
Clinical jaundice appearing in 1st
24h
Bilirubin
Hyperbilirubinemia
Bile Duct
Normal Biliary Obstruction
Bile Secretion
Normal
Abnormal
Cholestasis
Retention of bile salts
Results in injury to biological membranes throughout body
Liver (most affected)
Retention of hydrophobic bile salts
(results in their incorporation into membranes)
Alter membrane fluidity, function
Bile salt injure hepatocyte membranes
(important amplifier of cholestasis)
Retention of secondary cholestatic bile acids (eg. l ithocholic acid)
Results in further membrane injury
Retention of cholesterol
Cholesterol content of membranes
Fluidity
Impair function of integral membrane proteins
Further retention of damaging substances
Accelerated membrane injury, dysfunction
Generalized failure of excretory mechanism for bile

8/6/2019 Pathology of Cholestasis
http://slidepdf.com/reader/full/pathology-of-cholestasis 2/3
Clinical Features
Jaundice
y Absent in partial obstruction
y Yellowish discoloration of skin
y Excess bilirubin
y > 2.0 2.5 mg/dl
y Disturbance in bilirubin production, clearance
Pruritus (bile acids)
Cholesterol deposits on skin
Laboratory Features
Dark urine
Conjugated bilirubin
Bile acids
Cholesterol
Serum Alkaline phosphatase
Transaminases
Morphology
Normal
Bile pigments within hepatocytes, canaliculi
Hepatocytes larger
Apoptosis
Mild Bile Duct Proliferation
Portal fibrosis

8/6/2019 Pathology of Cholestasis
http://slidepdf.com/reader/full/pathology-of-cholestasis 3/3
Specific Cholestatic Disorders
Large Bile Ducts Small Bile Ducts Hepato-cellular
Acute Acute biliary
obstruction
Acute cholangit is Pure cholestasis
Drug injury Drug injury
Compound
cholestasis
Chronic Chronic biliary
obstruction
Primary biliary
cirrhosis
Drug injury
Progressive familia l
cholestasisPrimary sclerosing
cholangitis
Primary sclerosing
cholangitis
Biliary Obstruction
Mechanical blockage of
y Large intrahepatic bile ducty Extra hepatic duct
Can lead to bacterial cholangitis, sepsis
Causes
Morphology
Extrahepatic biliary atresia
Inflammation with stricture of hepatic, common bile ducts
Cholestasis with intrahepatic bile duct proliferation, fibrosis, cirrhosis
Extrahepatic biliary atresia
Brown-green bile plugs
Bile duct proliferation
Extensive fibrosis
Morphology (cont.)
Primary Biliary Cirrhosis(Rare autoimmune disease)
Destruction of bile ductules (within triads of liver)
Cholestasis
Acute Chronic
Hepatocyte injury
Degeneration
Inflammatory cell infiltration
(acute inflammation)
Repair
Restoration of normal architecture
Foamy changes of hepatocytes
Focal destruction of parenchyma
Unrelieved obstruction
y Portal tract fibrosis
y End stage cirrhosis
Cirrhosis
End stage of liver disease
Bridging fibrous septae
Disruption of entire architecture of liverParenchymal nodules
y Micronodular (nodules < 3mm) Alcoholic
y Macronodular (nodules > 3mm) Hepatitis C infection
Macronodular Cirrhosis
Morphology
Regenerative nodules of hepatocytes
Surrounded by fibrous connective tissue (bridges between portal tracts)
Bile plugs
Diagnosis
Biliary Obstruction Intrahepatic Cholestasis
Clinical
Radiological
Clinical
Radiological
Liver biopsy