Nonverbal Communication Skill Practiced by Cardiologists...
16
Volume-01 Issue-08 August-2019 ISSN: 2663-0931(Print) ISSN: 2663-2594(online) International Journal of Interdisciplinary Current Advanced Research www.ijicar.in © IJICAR 2019, All Rights Reserved 6 | Page Nonverbal Communication Skill Practiced by Cardiologists at National Heart Institute, Malaysia *1 Vimala Govindaraju * 1 Faculty of Languages and Communication,University Malaysia Sarawak Note: * Indicates corresponding author ARTICLE DETAILS ABSTRACT Article History: Received Date: 14/08/2019 Revised Date: 18/08/2019 Accepted Date: 26/8/2019 e-First: 28/08/2019 Communication perceived as significant process that supports doctors convey the health care information to patients. The purpose of this research is to study nonverbal communication skills practiced by cardiologists to communicate with patients. Qualitative method thru phenomenological approach was applied to conduct in-depth interviews and observations with 8 cardiologists who participated as informants in the study at the National Heart Institute, Kuala Lumpur Malaysia. The data were transcribed verbatim and analyzed using ATLAS.ti 7 to code the key themes, sub-themes and inter-relationships. The research outcomes showed the nonverbal communication skills such as touch, body language and gesture, eye contact and tone of voice were essential elements used by the cardiologists during they consulting with their patients. The results suggested that doctors can be provided professional training to improve their nonverbal communication skills while consulting with patients. The nonverbal communication skill training can help the cardiologists effectively deliver health care service to their patients. Keywords Communication, nonverbal, tone, touch, body language, eye contact. * Corresponding Author (Vimala Govindaraju) 1. Introduction The Malaysian health care system is an efficient and widespread public and private network of health care delivery organizations where doctors are responsible for sharing their medical knowledge, clinical skills, and communication skills with their patients. However, there are many challenges to communicating effectively with patients, including the use of effective Nonverbal communication skills. Nonverbal communication skills are essential for building rapport between doctors and patients, encouraging patient information sharing, and evaluating patients’ responses to information and treatments provided. This study examines how cardiologists use Nonverbal communication skills when interacting with heart patients during consultations at the National Heart Institute (IJN). The IJN is one of the institutes within the Malaysian health care system that provides advanced treatment in cardiac services. Cardiologists at IJN are among the most skillful medical specialists in Malaysia who are capable to treat the most complicated cardiac disease cases. This study examined how the cardiologists at IJN used Nonverbal communication skills to interact effectively with their patients. The research objective in this study is to identify the specific nonverbal communication skills practiced by cardiologists at IJN. This study also focused on the uses of Nonverbal communication by cardiologists to deliver good care. For example, how do cardiologists respond to patients’ Nonverbal cues, and how do they use Nonverbal skills to demonstrate trust. The study examined how the effective use of Nonverbal communication skills by cardiologists can lead to positive health outcomes and enhance patients’ satisfaction. 2. Doctor-Patient Nonverbal Communication Communication between doctor-patient is primary element in the health care perspective. Literature showed good doctor-patient communication promotes effective health care by enhancing the delivery of relevant health care information, to facilitate diagnoses, and to create kind relations with patients (Bredart, 2005; Duffy, 2004). This accomplished by the use of communication to exchange relevant health information, support patients' self-management, manage insecurity and sentiments, promote informed make resolution and enhance trust in the relationship between doctor-patient (Street, 2009). The past research showed the way a doctor communicates with a patient is as important as the information being delivered (Kreps, Arora & Nelson, 2003; Neumann, Edelhäuser,
Transcript of Nonverbal Communication Skill Practiced by Cardiologists...

Volume-01
Issue-08
August-2019
ISSN: 2663-0931(Print)
ISSN: 2663-2594(online)
International Journal of
Interdisciplinary Current Advanced Research www.ijicar.in
© IJICAR 2019, All Rights Reserved 6 | Page
Nonverbal Communication Skill Practiced by Cardiologists at National Heart Institute, Malaysia
*1 Vimala Govindaraju
*1 Faculty of Languages and Communication,University Malaysia Sarawak Note: * Indicates corresponding author
ARTICLE DETAILS ABSTRACT
Article History: Received Date: 14/08/2019 Revised Date: 18/08/2019 Accepted Date: 26/8/2019 e-First: 28/08/2019
Communication perceived as significant process that supports doctors convey the health care information to patients. The purpose of this research is to study nonverbal communication skills practiced by cardiologists to communicate with patients. Qualitative method thru phenomenological approach was applied to conduct in-depth interviews and observations with 8 cardiologists who participated as informants in the study at the National Heart Institute, Kuala Lumpur Malaysia. The data were transcribed verbatim and analyzed using ATLAS.ti 7 to code the key themes, sub-themes and inter-relationships. The research outcomes showed the nonverbal communication skills such as touch, body language and gesture, eye contact and tone of voice were essential elements used by the cardiologists during they consulting with their patients. The results suggested that doctors can be provided professional training to improve their nonverbal communication skills while consulting with patients. The nonverbal communication skill training can help the cardiologists effectively deliver health care service to their patients.
Keywords
Communication, nonverbal, tone, touch, body language, eye contact.
*Corresponding Author
(Vimala Govindaraju)
1. Introduction The Malaysian health care system is an efficient and widespread public and private network of health care
delivery organizations where doctors are responsible for sharing their medical knowledge, clinical skills, and
communication skills with their patients. However, there are many challenges to communicating effectively with
patients, including the use of effective Nonverbal communication skills. Nonverbal communication skills are
essential for building rapport between doctors and patients, encouraging patient information sharing, and
evaluating patients’ responses to information and treatments provided. This study examines how cardiologists use
Nonverbal communication skills when interacting with heart patients during consultations at the National Heart
Institute (IJN). The IJN is one of the institutes within the Malaysian health care system that provides advanced
treatment in cardiac services. Cardiologists at IJN are among the most skillful medical specialists in Malaysia who
are capable to treat the most complicated cardiac disease cases. This study examined how the cardiologists at IJN
used Nonverbal communication skills to interact effectively with their patients. The research objective in this study
is to identify the specific nonverbal communication skills practiced by cardiologists at IJN. This study also focused
on the uses of Nonverbal communication by cardiologists to deliver good care. For example, how do cardiologists
respond to patients’ Nonverbal cues, and how do they use Nonverbal skills to demonstrate trust. The study
examined how the effective use of Nonverbal communication skills by cardiologists can lead to positive health
outcomes and enhance patients’ satisfaction.
2. Doctor-Patient Nonverbal Communication
Communication between doctor-patient is primary element in the health care perspective. Literature
showed good doctor-patient communication promotes effective health care by enhancing the delivery of relevant
health care information, to facilitate diagnoses, and to create kind relations with patients (Bredart, 2005; Duffy,
2004). This accomplished by the use of communication to exchange relevant health information, support patients'
self-management, manage insecurity and sentiments, promote informed make resolution and enhance trust in the
relationship between doctor-patient (Street, 2009). The past research showed the way a doctor communicates with
a patient is as important as the information being delivered (Kreps, Arora & Nelson, 2003; Neumann, Edelhäuser,

Volume-01, Issue-08, August-2019 International Journal of Interdisciplinary Current Advanced Research
© IJICAR 2019, All Rights Reserved 7 | Page
Kreps, Scheffer, Lutz, Tauschel & Visser, 2010). Scholars explained that even simple Nonverbal cues such as eye
contact handshakes may help a physician communicate empathy and improve patient satisfaction (Montague,
Chen, Xu, Chewning & Barrett, 2013). Furthermore, patients understand that doctors who practice nonverbal
communication skills effectively expected to recognize health complications, understand their treatment
possibilities, modify their performance thus, and monitor their treatment plans (Stewart, 1995 & Bogardus,
Holmboe,1999)
Effective nonverbal communication skills play an important expressive part throughout the medical
consultation in doctor-patient relations. Nonverbal communication supports to build the relation, provides cues to
underlying unspoken concerns and emotions, and helps to reinforce or differ verbal comments (Hall, Harrigan &
Rosenthal ,1996). Nonverbal communication skills such as open, attending posture, active listening, eye contact at
patient thru responding by looking and nodding help to build understanding by encouraging the patient to talk
without disruption and to bring up additional issues or concerns during consultations (Usherwood, 1999 &
Buckman, 1992). Scholars clearly defined that nonverbal communication as characteristic of communication where
information is exchanged using gesture, touch, facial expression, eye contact clothing and hair style (Hall &
Montauge, 2013). Scholar pointed physicians’ patterns of nonverbal communication to their therapeutic efficacy
Ambady (2002). Scholars also added providers’ particular nonverbal behaviors have been found to guess clients’
satisfaction and impression of the physician (Roter, Hall, & Katz, 1987). Moreover, such behaviors could contribute
to the progress in self-confidence and to establish in keep interpersonal relations with clients (Ambady &
Rosenthal, 1992; Hall, Harrigan, & Rosenthal, 1995).
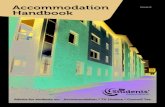
To study the nonverbal communication skills practiced by cardiologists with their patients. The Model of
Relational Health Communication Competence (RHCCM) was created in order to describe the process of
communication influences competence level in health outcomes (Kreps, 1988; Weathers, Query & Kreps, 2010).
The model referred to provider whom the health care professionals on their abilities in establishing health care
relations through sharing appropriate health information, and knowledge and manage to achieve preferred health
outcomes. The RHCCM recommends that insufficient stages of communication competence will not facilitate the
health care delivery wheel to move forward and while the wheel roll backward its consider fail to achieve health
care goals and solving health complications.
Figure 1: Relational Health Communication Competence Model (Kreps, 1988)
3. Methodology
Qualitative research methodology was used in this research to emphasis on identifying and analyzing the
nonverbal communication skills cardiologists practiced with their patients. Qualitative research creates an
understanding based on clear methodological traditions of question that explore and raise understanding of
human experience (Cresswell, 2012). Scholars recognize qualitative method as describing human experience and
behavior through the meaning of experience in human activity and is not purely based on objective observation
and description (Berg, Welman and Kruger, 1989).
A phenomenological approach was applied in this research to explain life experiences of doctors
concerning their use of nonverbal communication skills with patients. A total of 15 cardiologists were in-depth

Volume-01, Issue-08, August-2019 International Journal of Interdisciplinary Current Advanced Research
© IJICAR 2019, All Rights Reserved 8 | Page
interviewed as exhibited in Table 1. Moreover, data were triangulated through observations, field notes, and audio
recordings. The informants’ selection was based on purposive sampling with criteria of entry with working
experience as medical doctor for several years, focused on their career life experience as cardiologists, and have
experience in communicating with patients using nonverbal communication.
No Doctor’s Name Age Race Gender Specialize Working Experience (Years)
1. Dr. A 34 Indian Male Cardiologist 12
2. Dr. B 36 Indian Male Cardiologist 14
3. Dr. C 43 Chinese Male Cardiologist 21
4. Dr. D 37 Indian Male Cardiologist 15
5. Dr. E 35 Indian Male Cardiologist 13
6. Dr. F 42 Indian Male Cardiologist 13
7. Dr. G 34 Chinese Male Cardiologist 12
8. Dr. H 33 Malay Female Cardiologist 11
9 Dr. I 38 Malay Male Cardiologist 16
10 Dr. J 39 Malay Female Cardiologist 17
11 Dr. K 44 Malay Female Cardiologist 22
12 Dr. L 34 Indian Male Cardiologist 12
13 Dr. M 39 Chinese Male Cardiologist 17
14 Dr. N 37 Chinese Male Cardiologist 15
15 Dr. O 38 Indian Male Cardiologist 16
Table 1: Summary of informants
Through the in- depth interview sessions, the interviewer was tied up with the informants by questioning in
neutral manner, listen carefully to the informants’ answers, querying follow-up questions and exploratory based on
those answers. Face-to-face in-depth interviews were conducted by involved one to one interviewer and
informant. Moreover, an observational method was also used in this study. The observational method was also
applied for the reason description on the situations, people, activities and the meanings of what is witnessed by
informant’s perspective. Observations can create deep understandings than interviews alone, as it offers
knowledge in context where the events take place, and can facilitate the researcher perceive that informants
themselves not aware of, or that they are reluctant to discuss (Patton, 1990). Direct observations were used to
get an accurate scenario and clear picture of nonverbal communication skills practiced by cardiologists during
medical consultations with their patients.
Direct observations involved identifying the specific Nonverbal communication skills practiced by the
cardiologists with patients, how long the cardiologists used these Nonverbal communication activities with their
patients, and where the Nonverbal communication took place. In-depth interviews were conducted for 30 to 40
minutes and the interviews were recorded through audio-recording and later data was transcribed verbatim after
each session. The analysis method on constant comparisons was used to identifying the regularity themes and
categories from the transcribed interview data. Past literature similarly pointed constant comparison needs
frequent revision during the course of the study until the themes and categories meet saturation, moving to a new,
or restructured principle or theory of how knowledge is developed, and skills are educated (Corbin & Strauss,
2015).
4. Result of the study: Nonverbal communication skills practiced by Cardiologists.
Based on the thematic analysis, there were several specific Nonverbal communication cues used by the
cardiologist. Nonverbal communication was described by the cardiologists as an essential part in the health care
practice. Based on the interviews with the doctors, results show that there are several different forms of
Nonverbal communication that are frequently used by the doctors with their patients. The following Nonverbal
communication themes were found to be especially important for doctor-patient communication by the cardiology
doctors.

Volume-01, Issue-08, August-2019 International Journal of Interdisciplinary Current Advanced Research
© IJICAR 2019, All Rights Reserved 9 | Page
4.1.1 Touch
Touch is a tactile form of Nonverbal communication between two people. In a health care setting, touch is
an especially important communication cue for promoting the development of interpersonal relationships between
doctors and patients, that if used sensitively and appropriately can communicate empathy (Jones, 1994). The
literature has shown that doctors sometimes touch their patients to express caring and empathy (Harton, 1995).
There are several kinds of touch that may occur between a doctor and patient in the exam room.
Researchers have identified two types of touch which are closely related to the interpersonal
communication skills used by doctors; (i) social touch, which have specific social meanings, such as
handshakes or patting the shoulders and (ii) Physical touch, which is touch that has a clinical purpose,
such as a clinician’s touch during an examination. Doctors use social touch in their daily career lives as
an adjunct to verbal communication and they use physical touch during the scope of health care
practice. These were some of the factors concerning touch that were highlighted by the respondents:
4.1.2 Social touch
Generally, touch perceived as a nonverbal communication element to show positive emotions.
Furthermore, scholars have identified social touch can establish and sustain social ties such as common positive
reactions, hope and care among the dyad that keep individual closeness to others and restrain interpersonal
behaviour (Ainsworth, 1989; Hazan, 1987). A social touch in healthcare perspective can be classifying as kind
touch on patient’s hand, arm, or shoulder which conveys concern and care which can improve communication
between doctors and patients. Most patients believe expressive touch is acceptable, especially in distress
circumstances (Cocksedge, George, Renwick & Chew-Graham, 2013). Most of the responding doctors in this
current study were aware of their use of touch, but some explained that their patients may be concerned by
doctors’ use of touch in consultations, such as hand shaking and tapping shoulders in the way of giving
encouragement and support. The responding doctors expressed their concerns about the appropriateness of
touching their patients as social touch. Below are some relevant quotes concerning touch from the interview
sessions:
I will shake hands with my male patients but I am always aware and
won’t touch my Muslim female patient unless they are willing to shake
hands. For me, touch during the consulting session is necessity as its
implies the symbol of care for the patients (Dr. D)
Nonverbal communication can be also touch ya... It is kind of expression
we show patients that we care about them. We doctor used to examine
patients and another one I touch that we used to shake hands, pat
patients’ shoulder or arm in the way of giving hope to them. (Dr. H).
Doctors most likely are good companions to the patients as they show
empathy during their visit. Sometimes the doctors always involved in a
few “social touches” such as a handshake or pat at a patient’s shoulder.
(Dr. G)
Dr. D said he is willing to shake hands with his male patients, however, only if his female patients are
willing to shake hands with him will he do so with them. Dr. D practices his consultation session using touch as
more of an empathetic symbol. Literature has supported that social touch helps enable sharing emotional
experiences between doctors and patients for providing support and empathy (Adolphs, 2009). Based on these
interview responses, social touch was found in this study to be an important Nonverbal communication channel
for doctors to convey reassurance, friendliness, approval, concern, and affection to their patients.
According to Dr. H, nonverbal communication is important for showing and expressing kindness, caring
and empathy to patients. This doctor explained that in doctor-patient interactions, nonverbal communication plays
an important role in expressing caring and empathy concerning patients’ health related issues. Dr. H clearly
stated that as a doctor, typically examined patients by touching them without discriminating about patient gender.
These findings supported by literature that patient consultations doctors must measure the special value and
passion towards their patients’ emotions, pain, symptom, and doctors need make positive hopes, by providing
emotional support patient treatment (Friedman, 2010). This research suggests that social touch may have
symbolic value in healing, but it also may affect the interpersonal nature of the doctor-patient interaction

Volume-01, Issue-08, August-2019 International Journal of Interdisciplinary Current Advanced Research
© IJICAR 2019, All Rights Reserved 10 | Page
(Friedman, 2010). Interpersonal communication in health care needs face-to-face relationship between health
professionals and patients, involving nonverbal communication, and often touch.
Dr. G shared his experience that social touch is clearly connected to patient's health and doctor's
empathy. Dr. G stated that doctors play a role as a good health care companion during the consultation session.
These responses are reinforced by Hirsch (2007) who explained the doctor who recognizes every patient on their
individual level views a better chance of facing and conveying sympathy and treating the patient’s illness
efficiently. Patients seek empathy from their physicians. The data collected in this study shows that social touch
reflects a doctor’s empathy and understanding about patient feelings and concerns. Social touch also enables
doctors to strengthen their relationships with patients.
4.1.3 Physical touch
As discussed earlier, a clinically-oriented touching can be a big part of doctors’ care for their patients.
These forms of physical touch have different degree of importance for different people. Clinical physical touch, if
used appropriately, can trigger a cascade of chemical responses in human bodies that relieve stress and pain;
create feelings of security, happiness, and comfort; enhance the immune system; decrease blood pressure; and
improve blood sugar levels. In the health care perspective, physical touch is commonly used for clinical purposes
during medical examinations. In this study, the researcher identified that doctors use this form of physical touch
when they examine patients, as well as to gather biometric data from their patients, such as blood pressure, heart
rate and blood sugar levels. The respondents were highlighted their experience in using clinical physical touch
with their patients. The quote from the interviews, as follows.
As a doctor, we have to do the basic physical examination on patients.
So whenever I need to examine my patients, I have to touch my patients,
for example, to check the pulse, listen to heart beat and so on... (Dr. I)
Touch during the consulting session, for instance the purpose of patient's
physical examination such as check heartbeat, pulse checking, touch
their leg and other touch related to medical purpose (Dr. B)
When I listen to their hearts, I make sure to touch my patients by holding
their arm or hand. Sometimes, I will hold them after the physical
examination. I think it is enormously important to touch patients before I
further the medication or treatment process of the patients (Dr. J).
Dr. I in this research shared his experience as he uses this touch to check pulse and check heartbeat.
He pointed out that physical touch is an important element for every patient during medical visits. Dr. I’s quotes
were strongly supported in the literature suggesting that medical touch is a casual element in doctors and patient
relationship as the physical exam and generally patients trust doctors whom has to use physical touch for
examine purposes (Blair & Wasson, 2015). These responses from the doctors illustrate that sensitive touching of
patient during examinations promotes the development of trust by demonstrating physician commitment to the
rapport by taking the time to see, listen to, and sense what the patient's body react and reveals. Cardiologists are
physicians who are qualified with the ability to detect cardiac ailments by listening to the sounds of the heart and
treat a continually rising number of people who suffer from heart disease. This is their competitive advantage in
establishing trust with sensitive clinical touching.
Dr. B, one of the cardiologists, stated that physical touch during the consulting session is an essential
form of Nonverbal communication in the doctor and patient health care relationship. More specifically, skilled
doctors with many years of experience, always recognize the importance of this type of touching during patient
visits. Dr. B’s statement is strongly supported in existing literature that explains that the doctor’s touch can be
diagnostic, therapeutic, and, perhaps most importantly, a mean for communicating that the doctor is deeply
attuned to the problems, needs, and fears of the patient (Roter & Hall, 2006). Dr. B had a gentle, Nonverbal
communication skill that extended to shaking hands with every patient and ability to work with patients on a
simple, person-to-person level, illustrating that doctors touch their patients to create a sense of trust during
physical examinations. Almost all the doctors interviewed mentioned that they took the initiative to touch their
patients with the purpose of healing; explaining that touching could promote good health, stress relief, recovery
from an injury if the touch was gentle, relaxing, and penetrating.
Dr. J explained that she continually touched her patients throughout the physical exam and held their
hand or arm until the end of the consultation session, especially with elderly patients. Dr. J’s continuous touch of a

Volume-01, Issue-08, August-2019 International Journal of Interdisciplinary Current Advanced Research
© IJICAR 2019, All Rights Reserved 11 | Page
patient’s arm or hand, demonstrated to the patient that she remained being concerned and supportive of the
patient in the medical care process. Dr. J's actions are strongly supported in the literature that suggest that skillful
touching behaviors during physical examinations can have considerable therapeutic importance (Gordon, 2006).
Scholars also pointed the patient trust by allowing the doctor to touch in the sense of examine the patients and
how the body react on the physical examination (Olson & Roth, 2007). These results indicate that it is important to
use sensitive clinician touching during patient medical visits, and that patients prefer doctor’s touch during
consultations because these touches often indicate that the doctor is concerned about and supportive of the
patients’ health.
4.2.1 Body language and gesture
Body language forms a major part of nonverbal communication with feelings, purposes, or outlooks are
conveyed by physical manners, such as body positions, facial expressions, movements, eye contact, touch and
the space usage. Body language is an essential part in health as it can enhance effectiveness of the consultation
by applicable communication of empathy and understanding. Doctors use different forms of body language with
their patients to maintain effective doctor-patient relationships.
Research literature has supported that the following forms of a doctor's body language are powerful and
visible Nonverbal signs of encouragement to patients, such as maintaining an upright body posture, with straight
shoulders and back, and with the chin lifted slightly upward (Tacheva & Violeta, 2013). Interview responses
suggested that doctors’ body language plays an important role in the daily consulting session. The respondents
shared and highlighted the body language in their career life as follows: -
Nonverbal communication… Hmmm, I think it is about the actions
without verbal. Normally I use Nonverbal communication, for instance
listen and responding them by saying “hmm… hmm”, nodding my head,
body position, smiling, eye contact and touch. (Dr. B)
Well… Patients nowadays aware how the doctors communicating with
them. So, we also aware in communicating with patients. Using
Nonverbal communication hmm… body movement, eye contact, facial
expressions and our tone of voice. Sometimes… yes...we using during
the consultation with patients. (Dr. I)
Nonverbal communication is a step of communicates without using
words. It is a skill to interpret our message through eye contact, body
language and facial expressions. (Dr. K)
Dr. B explained that nonverbal communication is used during consulting sessions with patients with the
use of body language. For example, he stated that sometimes he nods his head when the patients tell their health
related issues, and comments nonverbally with “hum hmm”. His responses are supported in the literature as the
"right" body language, presenting an open approachable which can help health professionals to gain relevant
health care information to treat patient’s diagnosis and treatment (Gordon, 1995; Cole, 1993; Winfield &
Robinson, 1998). These results suggest that the doctor's body language can make a promising impression and
promote a patient's respect. For example, in this research, doctors practice uses open body language, such as
good eye contact and nodding, listening, hand movements, body posture, eye contact, and use of a neutral facial
expression towards their patients. The literature suggested that good body language can make a favorable
impression and receives a patient's respect, including the use of open body language, hand actions that are calm,
good position with held up head, a calm jaw, strong eye contact (but not staring), an impersonal facial expression,
and one that is applicable for the situation (Gordon & Edwards, 1995; Cole, 2000; Winfielf & Richard, 1998;
Nyman, 1996; Robinson, 1998, Kacperek, 1997; Egan, 1990).
Dr. I stated that patients seek positive nonverbal communication to reflect positive energy. Patients
appreciate reassuring verbal cues that are not accompanied by inconsistent facial expressions and vocal caution.
Dr. I’s perception is strongly supported by the literature, as scholars pointed out that doctors can tie up a person's
body position which reflecting their level of gestures and activities. On the other hand, doctors’ voice in term of
tone, volume, speed, rhythm, and pauses is also very influential during consultations with patients (Mackenzie,
2002). In this study respondents described how nonverbal communication that involves face and voice
expressions, body position, movements, and even presence can contribute to the delivery of quality health care
services.

Volume-01, Issue-08, August-2019 International Journal of Interdisciplinary Current Advanced Research
© IJICAR 2019, All Rights Reserved 12 | Page
Dr. K considers all nonverbal communication from eye contact to tone of voice to body language to be
relevant to the delivery of care to patients. Dr. K pointed out that the use of nonverbal communication must be
consistent with the total behavior pattern of a person. Dr. K's responses are supported by the literature that shows
that doctors’ nonverbal behaviors are clearly related to achieving important patient outcomes, especially when
physicians provide patients with direct eye contact, lean towards the patient, provide responsive head nods and
gestures, and establish close interpersonal distances (Roter, 2006). These results suggest that doctors who are
more emotionally communicate using nonverbal behavior are observed more favorable by patients. This area of
results was most consistent and positive.
4.2.2 Eye contact
Eye contact is another influential element of body language skills. Similarly, to other body language
elements, eye contact is a very influential form of doctor-patient communication. Eye contact enables
communicators to express their emotions, including levels of personal involvement and attraction. Generally, the
accurate level of eye contact from a presenter shows honesty and holds the listener's responsiveness, while the
exact eye contact level from a listener specifies they are giving attention and remain attentive. In the health care
system, high levels of eye contact perceived as strong influence on patients, illustrating that doctors are
empathetic. This can encourage active patient involvement in their who care, adherence to medical and
treatment advice, and to actively seek health care information concerning their illness (Martin, Williams, Haskard
& DiMatteo, 2005). Scholars also pointed eye contact helps make a positive impression by showing that the
doctor is focused concerning his/her patient. Similarly, during the doctor’s visits eye contact making meaningful by
making patients feel that the doctors understand and care about their needs (Wood, 2013). Eye contact was
mentioned by respondents in this study as a way to create relationships with patients that focus on the patient's
health care. Here are some of the comments provided by the respondents about eye contact:
Eye contact… one of the communication tools which does not involve
speech. Eye contact is something that shows we pay attention to the
patients. It can be accomplished with a combination of facial
expressions, eye contact and body language. (Dr. I)
Eye contact is looking and observing people at the same situation.
Doctors usually use eye contact at the beginning of every conversation
and discussion. (Dr. E)
I feel a doctor can give attention to the patient's health by eye contact by
focusing on their health issues. I always maintain eye contact and been
kinder and focused on patients (Dr. H).
Dr. I perceived eye contact is a communication element not involving speech. He also pointed out that
eye contact is a behavior that is similar to other nonverbal communication such as body gestures, facial
expressions and body language. The respondent's quotes are strongly supported by the literature that finds that
eye contact is an important form of nonverbal behavior that is necessary for constructing good relationship with
senior people (MacDonald, 2009). In addition, literature stated patients perceived eye contact as sign of care,
respect and kindness from a doctor (Marcinowicz, 2010). The data collected in this study illustrates that doctors
used eye contact effectively with their patients to demonstrate that they were listening to what the patients were
saying.
Dr. E pointed out that eye contact with the doctor was prominent in defining what the patient exposed in
the conversation during the consulting session. Dr. E also pointed out eye contact is a mix of verbal and
nonverbal communication as viewing, attending and speaking to patients during the consultation session.
Literature specified doctor’s eye contact is most active when it is applied appropriately using nonverbal cues and
attention. It generates emotion that doctor is responsiveness where doctors not only listening to the patient but
note down on their chart (Gorawara-Bhat, 2013). These responses illustrate that eye contact can consume a big
effect on patients’ perceptions of doctors’ empathy.
Dr. H commented that eye contact is an element doctors used to demonstrate their attention to patients
and their health related issues. In this regard, Dr. H said she tries to always maintain good eye contact with her
patients. The literature supported a good doctor creates attention for the patient as he or she looks at the patient
and strongly emphasized that a simple gesture of lowering the negative impact on patient satisfaction compared
to a regular brief visual interactions which can increase patient satisfaction (Khan, 2014). Based on these

Volume-01, Issue-08, August-2019 International Journal of Interdisciplinary Current Advanced Research
© IJICAR 2019, All Rights Reserved 13 | Page
response, it was observed that the doctors in this research study try to use good eye contact when interacting
with their patients about their health related issues. Doctors in this study focus on providing eye contact during
conversations with their patients to show that they are listening and paying attention to their patients.
4.2.3 Tone of voice
Tone of voice was another Nonverbal communication element that the doctors in this study said they
used in the health care setting, in addition to the practice of body movements and facial expressions (Silverman,
2010). Tone of voice, sometimes referred to as paralinguistic, concerns the ways that words are spoken, instead
of the actual words themselves (Schuller, 2013). Tone of voice can indicate whether the speakers pleasant and
friendly, angry and upset, or irritated and frustrated. In this study, tone of voice was found to frame the ways in
which verbal messages are interpreted.
Debra Roter & Judith Hall (1989) pointed out that different vocal styles can have powerful expressive
influences with patients. Tone of voice is an important part of doctor-patient communication. Based on the
interviews conducted in this study, the doctors expressed how they use tone of voice during their consultation
sessions with their patients.
I believed a doctor’s tone of voice is significant in the doctor's daily
career life with their patients. It reflects the doctor's concern on the
message conveys to their patients in the emphatic way. (Dr. O)
Basically doctor’s tones of voice can be a positive point for patients on
their health. For example, if I talk in positive voice, then the patients will
perceive as it is caring and if I talk negative tone, then patients will
disappoint with me (Dr. H).
The tone of voice of the doctor... is kind of “warm and supportive” in
positively. A doctor’s tone of voice will lead to the patient satisfaction in
the health care setting. We cannot harsh to the patient. Right… (Dr. F)
Dr. O believes a doctor's tone of voice is an important factor in working effectively with patients. He
explained that tone of voice shows the doctor's concern in conveying messages to patients. The literature strongly
supports this finding that with tones of voice described as “warm and supportive” or “capable and concerned”,
patients expressed that they had been given more “choice and/or control”, additional “satisfied” with doctor’s
communication, sensed they given additional “information” and required better “trust”. When the doctor’s voice
was more “enthusiastic”, the result was similar, but it was also positively associated with medication adherence
(Joyce, 2015). From the responses provided in this study we found that the doctors use of “warm and supportive”
vocal tones were positively related to patient satisfaction with their health care.
Doctors use tone of voice to communicate with their patients to create a trusted situation. Dr. H believed
tone of voice of the doctors will make the patients trust their doctors and continue to overcome their illness. On
the other hand, she also pointed that if the tone is harsh, then the patients will show disappointment with their
doctors and also create a bad reputation for other doctors at IJN. This response is supported in the research
literature that suggest that the most negative tone of voice is seen as hostile and disrespectful and is associated
with significant and sustained pain and patients’ poorer physical health (Hall, Stein, Roter & Rieser, 1999).
Obviously, the physician’s tone of voice reflects his/her satisfaction with patients (Hall, Stein, Roter & Rieser,
1999). Based on these interview responses it was concluded that the doctors’ tone of voice reflects the doctors’
levels of empathy and understanding of the patient. The research findings also suggest that doctors use
appropriate tone of voice sincerely to support the patients by providing clear and also encouraging messages
during the consultation sessions.
The vocal tones that doctors use with their patients have also been associated with patient satisfaction
(Roter, 2006). Dr. F perceived that patients were more satisfied with the doctors who used vocal tone that were
calm when delivering health care information. Dr. F feels that negative tone of voice that may sound anxious and
irritated can lead to bad patient perceptions on their doctors and lead to patient dissatisfaction. The literature
supported respondent’s quotes in this study as tone-of-voice able to precise sentimental feelings and
understanding. Scholars pointed a doctor who communicates with a patient in an undesirable way, such as using
a cruel or irritated tone of voice, was more likely to cause litigious feelings than a doctor who communicates with a
patient in a positive manner (Ambady, LaPlante, Nguyen, Rosenthal, Chaumeton & Levinson, 2002).

Volume-01, Issue-08, August-2019 International Journal of Interdisciplinary Current Advanced Research
© IJICAR 2019, All Rights Reserved 14 | Page
5. Conclusion
Based on the research reported in this study, the doctors interviewed explained that they showed
empathy through tone of voice, which is related to better conclusions, with fewer negligence claims in their career
life. At the same time, the study results showed that doctors express themselves with brief and kind voices to
avoid hostility with their patients. Based on these findings it was concluded that there were several main themes
concerning the doctors use of Nonverbal communication during interactions with their patients. These main
themes are presented in Table 4.3 as follows.
Table 2: Themes of Nonverbal communication used by doctor to their patients during interaction
session.
Themes
i. Touch
a. Social touch
b. Physical touch
ii. Body language and gesture
iii. Eye contact
Four main themes were identified from the main category.
This research concentrated on how cardiology doctors used Nonverbal communication with their patients
at the IJN Malaysia. Results from the interviews and observations suggested that the cardiology doctors depend
on their use of Nonverbal communication cues:
When they touch their patients. Touch is a form of Nonverbal interaction that was found to be especially
important for the development of empathy. For example, doctors touch their patients to express kind and
responsiveness. The study identified two types of touch in the consultation: social and physical touch. Social
touch has particular social importance, such as a handshaking, and physical touch is used for the purpose of
medical examination.
1. When the use body language and gestures with their patients. In this study, Body language and
gestures showed how doctors use their body position for instance, posture can indicate attention,
concern and perceptions about the importance of the patient’s health. Body position reflects how
open the doctor is to interacting with patients, or how attracted or interested the doctor is in the
patients.
2. When they communicate with patients using eye contact. Eye contact in this study particularly point
out the nonverbal cues related to understanding, trust, empathy, and relationship.
3. tone of voice of doctors can be related to nonverbal communication which show warmth that can
be conveyed by eye contact, interest, caring tone of voice, a touch on the arm, or a smile, or simply
leaning forward and establishing eye contact.
REFERENCES
1. AL Khalib, (2001). Nonverbal Cues: An Inevitable Assessing Skills in Doctor-Patient. Journal of
Community Health. 16(1), 45.
2. Ambady, N., Koo, J., Rosenthal, R., & Winograd, C. H. (2002). Physical therapists' Nonverbal
communication predicts geriatric patients' health outcomes. Psychology and aging, 17(3), 443.
3. Ambady, N., LaPlante, D., Nguyen, T., Rosenthal, R., Chaumeton, N., & Levinson, W. (2002).
Surgeons' tone of voice: a clue to malpractice history. Surgery, 132(1), 5-9.
4. Arora, N. K. (2003). Interacting with cancer patients: The significance of physicians’ communication
behavior. Social Science & Medicine, 57(5), 791-806.
5. Bailey, J. (2008). First steps in qualitative data analysis: transcribing. Family practice, 25(2), 127-131.
6. Banister, P., Bunn, G., Burman, E., & Daniels, J. (2011). Qualitative methods in psychology: a
research guide: a research guide, Buckingham: Open University Press. 2(1) 248.
7. Barbour, R. S. (2001). Checklists for improving rigor in qualitative research: a case of the tail wagging
the dog? British Medical Journal, 322(7294), 1115.

Volume-01, Issue-08, August-2019 International Journal of Interdisciplinary Current Advanced Research
© IJICAR 2019, All Rights Reserved 15 | Page
8. Beck, R. S., Daughtridge, R., & Sloane, P. D. (2002). Physician-patient communication in the primary
care office: a systematic review. The Journal of the American Board of Family Practice, 15(1), 25-38.
9. Buller, M. K., & Buller, D. B. (1987). Physicians' communication style and patient satisfaction. Journal
of health and Social Behavior, 28 (4) 375-388.
10. Cassell, C. (2005). Creating the interviewer: identity work in the management research
process. Qualitative Research, 5(2), 167-179.
11. Cassidy, E., Reynolds, F., Naylor, S., & De Souza, L. (2011). Using interpretative phenomenological
analysis to inform physiotherapy practice: an introduction with reference to the lived experience of
cerebellar ataxia. Physiotherapy theory and practice, 27(4), 263-277.
12. Chew, B. H., Cheong, A. T., Ismail, M., Hamzah, Z., Mohd-Radzniwan, A., Md-Yasin, M., & Ali, N.
(2014). A nationwide survey on the expectation of public health care providers on family medicine
specialists in Malaysia—a qualitative analysis of 623 written comments. BMJ open, 4(6), e004645.
13. Chio, A., Montuschi, A., Cammarosano, S., De Mercanti, S., Cavallo, E., Ilardi, A., & Calvo, A. (2008).
ALS patients and caregiver’s communication preferences and information seeking behavior. European
Journal of Neurology, 15(1), 55-60.
14. Chong, W. W., Aslani, P., & Chen, T. F. (2013). Health care providers’ perspectives of medication
adherence in the treatment of depression: a qualitative study. Social psychiatry and psychiatric
epidemiology, 48(10), 1657-1666.Cocksedge, S., George, B., Renwick, S., & Chew-Graham, C. A.
(2013). Touch in primary care consultations: qualitative investigation of doctors’ and patients’
perceptions. Br J Gen Pract, 63(609), e283-e290.
15. Cole, K. (1993). Crystal Clear Communication: Skills for understanding and being understood. (2nd
Ed). Sydney: Prentice Hall.
16. Comstock, L. M., Hooper, E. M., Goodwin, J. M., & Goodwin, J. S. (1982). Physician behaviors that
correlate with patient satisfaction. Academic Medicine, 57(2), 105-12.
17. Conner, M., & Sparks, P. (2005). Theory of planned behaviour and health behaviour. Predicting health
behavior, 2, 170-222.
18. Cortes, D. E., Mulvaney-Day, N., Fortuna, L., Reinfeld, S., & Alegría, M. (2008). Patient–provider
communication: Understanding the role of patient activation for Latinos in mental health
treatment. Health Education & Behavior. 36(1), 138-54.
19. Creswell, J. W. (2012). Qualitative inquiry and research design: Choosing among five approaches. (2nd
Ed). Thousand Oaks: Sage Publications.
20. Creswell, J. W. (2013). Research design: Qualitative, quantitative, and mixed methods approaches.
(4th Ed) Thousand Oaks, CA: Sage publications.
21. Creswell, J. W., & Plano Clark, V. L. (2007). Designing and conducting mixed methods research.
Thousand Oaks, Calif: Sage Publications.
22. Dahlui, M. & Aziz, N. A. (2012). Developing health service hub in ASEAN and Asia region country
report on health care service industry in Malaysia. Developing Asean Economic Community (Aec) Into
a Global Services Hub, 65-110.
23. De Witt, L., & Ploeg, J. (2006). Critical appraisal of rigour in interpretive phenomenological nursing
research. Journal of advanced nursing, 55(2), 215-229.
24. DeLamater, John D. & Myers, Daniel J. (2011). “Symbolic communication and language”. In Social
Psychology (7th Ed.). Belmont: Cengage Learning. pp.166 – 196.
25. Denzin, N. K., & Lincoln, Y. S. (2000). The discipline and practice of qualitative research. Handbook of
qualitative research, 2, 1-28.
26. Di Matteo, L. (2010). The sustainability of public health expenditures: evidence from the Canadian
federation. The European Journal of Health Economics, 11(6), 569-584.

Volume-01, Issue-08, August-2019 International Journal of Interdisciplinary Current Advanced Research
© IJICAR 2019, All Rights Reserved 16 | Page
27. Diana Slade, Scheeres, H., Manidis, M., Iedema, R., Dunston, R., Stein-Parbury, & McGregor, J.
(2008). Emergency communication: the discursive challenges facing emergency clinicians and
patients in hospital emergency departments. Discourse & Communication, 2(3), 271-298.
28. Dieppe, P., Rafferty, A. M., & Kitson, A. (2002). The clinical encounter‐the focal point of
patient‐centred care. Health Expectations, 5(4), 279-281.
29. Diette, G. B., & Rand, C. (2007). The contributing role of health-care communication to health
disparities for minority patients with asthma. Journal of the American College
of Chest Physicians, 132(5), 802-809.
30. DiMatteo, M. R. (2004). The role of effective communication with children and their families in fostering
adherence to pediatric regimens. Patient education and counseling, 55(3), 339-344.
31. Dixon-Woods, M., Shaw, R. L., Agarwal, S., & Smith, J. A. (2004). The problem of appraising
qualitative research. Quality and Safety in Health Care, 13(3), 223-225.
32. Dubey, A., & Gupta, S. (2015). Characteristics of Communication of Doctors during Consultation.
Asian Journal of Social Sciences, Arts and Humanities. 3 (2), 2311-3782
33. Duffy, F. D., Gordon, G. H., Whelan, G., Cole-Kelly, K., & Frankel, R. (2004). Assessing competence
in communication and interpersonal skills: The Kalamazoo II report. Academic Medicine, 79(6), 495-
507.
34. Ekayanti, F., Dwiyanti, S., & Nasrudin, N. (2015). Patients’ perception on interpersonal skills of doctor-
patient relationship in Fatmawati Public Teaching Hospital, Syarif Hidayatullah Hospital, and Harapan
Bunda Hospital Jakarta Indonesia. International Journal, 4(2), 23-33.
35. Epstein, R. M. (2007). Assessment in medical education. New England Journal of Medicine, 356(4),
387-396. Retrieved March 14, 2014 from http://dx.doi.org/10.1056/NEJMra054784.
36. Epstein, R. M., Franks, P., Fiscella, K., Shields, C. G., MelDr.um, S. C., Kravitz, R. L., & Duberstein, P.
R. (2005). Measuring patient-centered communication in patient–doctors’ consultations: theoretical
and practical issues. Social science & medicine, 61(7), 1516-1528.
37. Epstein, R., & Street, R. L. (2007). Patient-centered communication in cancer care: promoting healing
and reducing suffering (07-6225). Bethesda, MD National Institutes of Health: National Cancer
Institute, US Department of Health and Human Services, National Institutes of Health.
38. Farid, A. R. & Khalib, A. L., (2010). Stopping doctor-patient communication gap: the ten essential
methods. Journal of Community Health, 16(1) 48-53.
39. Fiscella, K., Goodwin, M. A., & Stange, K. C. (2002). Does patient educational level affect office visits
to family physicians? Journal of the National Medical Association, 94(3), 157.
40. Fiscella, K., MelDr.um, S., Franks, P., Shields, C. G., Duberstein, P., McDaniel, S. H., & Epstein, R. M.
(2004). Patient trust: is it related to patient-centered behavior of primary care physicians? Medical
care, 42(11), 1049-1055.
41. Forguione-Pérez, V. P. (2015). Communication between doctor and patient: Beyond a query, an
educational process. Revista Médicas UIS, 28(1).
42. Frith, C. (2009). Role of facial expressions in social interactions. Philosophical Transactions of the
Royal Society B: Biological Sciences, 364(1535), 3453-3458.
43. Gibbert, M., & Ruigrok, W. (2010). The" what" and" how" of case study rigor: Three strategies based
on published research. Organizational Research Methods, 13(4): 710‐737
44. Glanz, K., Saraiya, M., & Wechsler, H. (2002). Guidelines for school programs to prevent skin
cancer. MMWR. Recommendations and reports: Morbidity and mortality weekly report.
Recommendations and reports/Centers for Disease Control, 51(4), 1-18.
45. Golden-Biddle, K., & Locke, K. D. 2007. Composing qualitative research (2nd Ed.) Thousand Oaks:
Sage Publication.
46. Gorawara-Bhat, R., Dethmers, D. L., & Cook, M. A. (2013). Physician eye contact and elder patient
perceptions of understanding and adherence. Patient education and counseling, 92(3), 375-380.

Volume-01, Issue-08, August-2019 International Journal of Interdisciplinary Current Advanced Research
© IJICAR 2019, All Rights Reserved 17 | Page
47. Hall, J. A., Coats, E. J., & LeBeau, L. S. (2005). Nonverbal behavior and the vertical dimension of
social relations: a meta-analysis. Psychological bulletin, 131(6), 898.
48. Hall, J. A., Harrigan, J. A., & Rosenthal, R. (1996). Nonverbal behavior in clinician—patient
interaction. Applied and Preventive Psychology, 4(1), 21-37.
49. Halpern, J. (2007). Empathy and patient–physician conflicts. Journal of general internal
medicine, 22(5), 696-700.
50. Hassali, M. A., Alrasheedy, A. A., Ab Razak, B. A., AL-Tamimi, S. K., Saleem, F., Haq, N. U., &
Aljadhey, H. (2014). Assessment of general public satisfaction with public health care services in
Kedah, Malaysia. The Australasian Medical Journal, 7(1), 35.
51. Hook, K. M., & Pfeiffer, C. A. (2007). Impact of a new curriculum on medical students' interpersonal
and interviewing skills. Medical education, 41(2), 154-159.
52. Kacperck, L. (1997). Nonverbal communication: the importance of listening. British Journal of
Nursing, 6(5), 275-279.
53. Kaplan, S. H., Greenfield, S., & Ware Jr, J. E. (1989). Assessing the effects of physician-patient
interactions on the outcomes of chronic disease. Medical care, 27(3), 110-127.
54. Katterl, S. (2010). Doctor Patient Communication in Health Care Service Delivery: A Case of
Tribhuvan University Teaching Hospital, Kathmandu. Master in Public Policy and Governance
Program. North South University, Bangladesh. Retrieved 19 August, 2014 from http://mppg-
nsu.org/attachments/119_Final%20Thesis%20 Sarbani%20 Kattel_.pdf.
55. Khalib, A. L., & Farid, A. R. (2010). Stopping doctor-patient communication gap: the ten essential
methods. Journal of Community Health, 16(1) 48-53.
56. Khan, T. M., Hassali, M. A., & Al-Haddad, M. S. M. (2011). Patient-physician communication barrier: A
pilot study evaluating patient experiences. Journal of Young Pharmacists, 3(3), 250-255
57. Knapp ML, Hall JA. (2010). Nonverbal Communication in Human Interaction, (7th Ed) Wadsworth,
Canada: Cengage Learning.
58. Kreps, G. L. (2010). Communication and racial inequities in health care. American Behavioral
Scientist, 49(6), 760-774.
59. Kreps, G. L. (2013). Communication and palliative care: E-health interventions and pain management.
In Handbook of Pain and Palliative Care (43-51). New York: Springer.
60. Kreps, G. L., & Massimilla, D. C. (2002). Cancer communications research and health outcomes:
Review and challenge. Communication Studies, 53(4), 318-336.
61. Kreps, G. L., & Neuhauser, L. (2013). Artificial intelligence and immediacy: designing health
communication to personally engage consumers and providers. Patient education and
counseling, 92(2), 205-210.
62. Kreps, G.L. (1984). Communication and gerontology: Health communication training for providers of
health services to the elderly. In G.L. Kreps & B.C. Thornton. (1984). Health communication: Theory
and practice (210-217). New York: Longman.
63. Kreps, G.L. (2006). Communication and racial inequities in health care. American Behavioral Scientist,
49(6), 760-774. London: Sage Publication
64. Kreps, G.L., Arora, N.K. & Nelson, D.E. (2003). Consumer/provider communication research:
Directions for development. Patient Education and Counseling, 50(1), 3-4.
65. Kreuter, M. W., Farrell, D. W., Olevitch, L. R., & Brennan, L. K. (2013). Tailoring health messages:
Customizing communication with computer technology. New York: Routledge.
66. Kripalani, S., & Weiss, B. D. (2006). Teaching about health literacy and clear communication. Journal
of General Internal Medicine, 21(8), 888-890.
67. Lacey & Luff, (2001). Lacey, A., & Luff, D. (2001). Trent Focus for research and development in
primary health care: An introduction to qualitative analysis. Trent, UK: Trent Focus.

Volume-01, Issue-08, August-2019 International Journal of Interdisciplinary Current Advanced Research
© IJICAR 2019, All Rights Reserved 18 | Page
68. Larson, E. B., & Yao, X. (2005). Clinical empathy as emotional labor in the patient-physician
relationship. Jama, 293(9), 1100-1106.
69. Laverty, S. M. (2003). Hermeneutic phenomenology and phenomenology: A comparison of historical
and methodological considerations. International journal of qualitative methods, 2(3), 21-35.
70. Levinson, W., Gorawara-Bhat, R., & Lamb, J. (2000). A study of patient clues and physician responses
in primary care and surgical settings. Journal of the American Medical Association, 284(8), 1021-1027.
71. Liebal, K., Carpenter, M., & Tomasello, M. (2011). Young chilDr.en's understanding of markedness in
Nonverbal communication. Journal of Child Language, 38(04), 888-903.
72. Lisa Sparks L. (1998). Health care and care giving research, policy, and practice. Mufti-disciplinary
Coordinated Care giving: Professional Contributions. New York. Springer.
73. Lopez, K. A., & Willis, D. G. (2004). Descriptive versus interpretive phenomenology: Their
contributions to nursing knowledge. Qualitative health research, 14(5), 726-735.
74. MacDonald, K. (2009). Patient-clinician eye contact: social neuroscience and art of clinical
engagement. Postgraduate medicine, 121(4), 136-144.
75. Mackenzie, E., Farah, C. S., & Savage, N. W. (2002). Effective communication for health care
professionals. Hygiene Today, 14, 8-12.
76. Makoul, G. (2001). Essential elements of communication in medical encounters: The Kalamazoo
consensus statement. Academic Medicine, 76(4), 390-393.
77. Marcinowicz, L., Chlabicz, S., & Grebowski, R. (2010). Understanding patient satisfaction with family
doctor care. Journal of Evaluation in Clinical Practice, 16(4), 712-715.
78. Marcinowicz, L., Konstantynowicz, J., & Godlewski, C. (2010). Patients' perceptions of GP Nonverbal
communication: a qualitative study. British Journal of General Practice, 60(571), 83-87.
79. Martin, L. R., Williams, S. L., Haskard, K. B., & DiMatteo, M. R. (2005). The challenge of patient
adherence. Therapeutics and clinical risk management, 1(3), 189.
80. McQueen, D. V. (2009). Ethics and evidence in health promotion. Evidence-based public health:
Effectiveness and efficiency, (27–40). Oxford: Oxford University Press.
81. McWilliam, C. L., Brown, J. B., & Stewart, M. (2000). Breast cancer patients’ experiences of patient–
doctor communication: a working relationship. Patient Education and Counseling, 39(2), 191-204.
82. Mechanic, D., McAlpine, D. D., & Rosenthal, M. (2001). Are patients' office visits with physicians
getting shorter? New England Journal of Medicine, 344(3), 198-204.
83. Merriam, S. B. (2002). Introduction to qualitative research. Qualitative research in practice: Examples
for discussion and analysis, 3-17. San Francisco: Jossey-Bass Publication.
84. Michelle O’Daniel, A. H. (2008). Professional Communication and Team Collaboration. Retrieved 08
February, 2016, from Patient Safety and Quality: An Evidence-Based Handbook for Nurses:
http://www.ncbi.nlm.nih.gov/books/NBK2637.
85. Murray, C. J., & Frenk, J. (2000). A framework for assessing the performance of health
systems. Bulletin of the world Health Organization, 78(6), 717-731.
86. Myers, M. (2000). Qualitative research and the generalizability question: Standing firm with
Proteus. The qualitative report, 4(3/4), 1-9.
87. Neo, L. F. (2011). Working toward the best doctor-patient communication. Singapore medical
journal, 52(10), 720-725.
88. Neumann, M., Edelhäuser, F., Kreps, G.L., Scheffer, C., Lutz, G., Tauschel, D., & Visser, A. (2010).
Can patient-provider interaction increase the effectiveness of medical treatments or even substitute
them? A methodological reflection of the specific effect of the provider. Patient Education and
Counseling, 80, 307-314.

Volume-01, Issue-08, August-2019 International Journal of Interdisciplinary Current Advanced Research
© IJICAR 2019, All Rights Reserved 19 | Page
89. Norhayati, M. N., Masseni, A. A., & Azlina, I. (2017). Patient satisfaction with doctor-patient interaction
and its association with modifiable cardiovascular risk factors among moderately-high risk patients in
primary health care. Peer Journal, 5(1),2983.
90. Novak, D. R. (2010). Democratizing qualitative research: Photo voice and the study of human
communication. Communication Methods and Measures, 4(4), 291-310.
91. Nyman, K. C. (1996). Successful Consulting: A Practical Introduction to Consulting Skills in General
Practice. Victoria: Royal Australian College of General Practitioners.
92. Oates, D. J., & Paasche-Orlow, M. K. (2009). Health literacy communication strategies to improve
patient comprehension of cardiovascular health. Circulation, 119(7), 1049-1051.
93. Osheroff, J. A., Teich, J. M., Middleton, B., Steen, E. B., Wright, A., & Detmer, D. E. (2007). A road
map for national action on clinical decision support. Journal of the American medical informatics
association, 14(2), 141-145.
94. Partida, Y. (2007). Language barriers and the patient encounter. Virtual Mentor: American Medical
Association Journal of Ethics, 9(8), 566-571.
95. Patton, M. Q. (1990). Qualitative evaluation and research methods. (2nd Ed.). Newbury Park, CA:
Sage Publications.
96. Perloff, R. M., Bonder, B., Ray, G. B., Ray, E. B., & Siminoff, L. A. (2006). Doctor-Patient
Communication, Cultural Competence, and Minority Health Theoretical and Empirical
Perspectives. American Behavioral Scientist, 49(6), 835-852.
97. Pietrabissa, G., Ceccarini, M., Borrello, M., Manzoni, G. M., Titon, A., Nibbio, F. & Castelnuovo, G.
(2015). Enhancing behavioral change with motivational interviewing: a case study in a Cardiac
Rehabilitation Unit. Frontiers in psychology, 6(298). doi: 10.3389/fpsyg.2015.00298
98. Platt, F. W., & Keating, K. N. (2007). Differences in physician and patient perceptions of uncomplicated
UTI symptom severity: understanding the communication gap. International journal of clinical
practice, 61(2), 303-308.
99. Polkinghorne, D. E. (1989). Phenomenological research methods. In Existential-phenomenological
perspectives in psychology, (41-60). New York: Platinum Press.
100. Pope, C., & Mays, N. (2000). Qualitative research in health care: assessing quality in qualitative
research. British Medical Journal, 320(7226), 50–52.
101. Query Jr, J. L., & Wright, K. (2003). Assessing communication competence in an online study:
Toward informing subsequent interventions among older adults with cancer, their lay caregivers, and
peers. Health communication, 15(2), 203-218.
102. Ritchie, J., Lewis, J., & Elam, G. (2003). Designing and selecting samples. Qualitative research
practice: A guide for social science students and researchers, 2, 111-145.
103. Rose, S. L., Tidwell, A. L., Bujnoch, L. J., Kushwaha, A. C., Nordmann, A. S., & Sexton Jr, R.
(2013). Implementation of breast tomosynthesis in a routine screening practice: An observational
study. American Journal of Roentgenology, 200(6), 1401-1408.
104. Rosenberg, MA, H. J., Rosenberg, PH. D, S. D., Ernstoff, Md, M. S., Wolford, Ph. D, G. L., Amdur,
Md, R. J., Elshamy, Arnp, M. R. & Pennebaker, Ph. D, J. W. (2002). Expressive disclosure and health
outcomes in a prostate cancer population. The International Journal of Psychiatry in Medicine, 32(1),
37-53.
105. Roter, D. L., & Hall, J. A. (2004). Physician gender and patient-centered communication: a critical
review of empirical research. Annual Review of Public Health, 25, 497-519.
106. Roter, D. L., Frankel, R. M., Hall, J. A., & Sluyter, D. (2006). The expression of emotion through
Nonverbal behavior in medical visits. Journal of General Internal Medicine, 21(S1), S28-S34.
107. Schiavo, R. (2013). Health communication: from theory to practice. John Wiley & Sons. A
Francisco, CA: Jossey-Bass.

Volume-01, Issue-08, August-2019 International Journal of Interdisciplinary Current Advanced Research
© IJICAR 2019, All Rights Reserved 20 | Page
108. Serreze, M. C., Walsh, J. E., Chapin Iii, F. S., Osterkamp, T., Dyurgerov, M., Romanovsky &
Barry, R. G. (2000). Observational evidence of recent change in the northern high-latitude
environment. Climatic Change, 46(1-2), 159-207.
109. Shukla, A. K., Yadav, S. V., & Kastury, N. (2010). Doctor-patient communication: an important but
often ignored aspect in clinical medicine. Journal of the Indian Academy of Clinical Medicine, 11, 208-
11.
110. Silverman, J., & Kinnersley, P. (2010). Doctors' Nonverbal behaviour in consultations: look at the
patient before you look at the computer.
111. Smith RC, Lyles JS, Gardiner JC, Sirbu C, Hodges A, Collins C, Dwamena FC, Lein C, William
Given C, Given B, Goddeeris J. (2006). Primary care clinicians treat patients with medically
unexplained symptoms: a randomized controlled trial. Journal of General Internal Medicine, 21(7),
671-677.
112. Smith, J. A., & Osborn, M. (2015). Interpretative phenomenological analysis as a useful
methodology for research on the lived experience of pain. British journal of pain, 9(1), 41-42.
113. Smith, J., & Firth, J. (2011). Qualitative data analysis: the framework approach. Nurse
researcher, 18(2), 52-62.
114. Snyder, L. B., & Hamilton, M. A. (2002). A meta-analysis of US health campaign effects on
behavior: Emphasize enforcement, exposure, and new information, and beware the secular
trend. Public health communication: Evidence for behavior change, 357-383.
115. Soo, K. C. H., David, M. K., Kia, L. S., & Pei, A. (2011). Openings and Closings in Front Counter
Transactions of Malaysian Government Hospitals. The Journal of the South East Asia Research
Centre for Communication and Humanities, 3(1), 13-30.
116. Sparks, L., & Villagran, M. (2010). Patient and Provider Interaction. A Global Health
Communication Perspective. Cambridge: Polity Press
117. Steins, G. (2000). Motivation in person perception: Role of the others perspective. The Journal of
social psychology, 140(6), 692-709.
118. Street Jr, R. L., & Haidet, P. (2011). How well do doctors know their patients? Factors affecting
physician understanding of patients’ health beliefs. Journal of general internal medicine, 26(1), 21-27.
119. Street Jr, R. L., & Millay, B. (2001). Analyzing patient participation in medical encounters. Health
communication, 13(1), 61-73.
120. Street Jr, R. L., Gordon, H. S., Ward, M. M., Krupat, E., & Kravitz, R. L. (2005). Patient
participation in medical consultations: why some patients are more involved than others. Medical
care, 43(10), 960-969.
121. Street, R. L., Makoul, G., Arora, N. K., & Epstein, R. M. (2009). How does communication heal?
Pathways linking clinician–patient communication to health outcomes. Patient education and
counseling, 74(3), 295-301.
122. Suchman, A. L. (2001). Topics in Review: The influence of health care organizations on well-
being. Western Journal of Medicine, 174(1), 43.
123. Swinglehurst, D., Roberts, C., Li, S., Weber, O., & Singy, P. (2014). Beyond the ‘dyad’: a
qualitative re-evaluation of the changing clinical consultation. BMJ open, 4(9), e006017.
124. Tacheva, V. (2013). Communication–the master key to the patient’s heart. JAHR-European
Journal of Bioethics, 4(7), 601-620.
125. Takayama, T., Yamazaki, Y., & Katsumata, N. (2001). Relationship between outpatients’
perceptions of physicians’ communication styles and patients’ anxiety levels in a Japanese oncology
setting. Social science & medicine, 53(10), 1335-1350.
126. Travaline, J. M., Ruchinskas, R., & D'Alonzo Jr, G. E. (2005). Patient-physician communication:
why and how. The Journal of the American Osteopathic Association, 105(1), 13.

Volume-01, Issue-08, August-2019 International Journal of Interdisciplinary Current Advanced Research
© IJICAR 2019, All Rights Reserved 21 | Page
127. Upperman, J. S., Staley, P., Friend, K., Benes, J., Dailey, J., Neches, W., & Wiener, E. S. (2005).
The introduction of computerized physician order entry and change management in a tertiary pediatric
hospital. Pediatrics, 116(5), 634-642.
128. Vahdat, S., Hamzehgardeshi, L., Hessam, S., & Hamzehgardeshi, Z. (2014). Patient involvement
in health care decision making: a review. Iranian Red Crescent Medical Journal, 16(1).
129. Veldhuijzen, W., Mogendorff, K., Ram, P., van der Weijden, T., Elwyn, G., & van der Vleuten, C.
(2013). How doctors move from generic goals to specific communicative behavior in real practice
consultations. Patient education and counseling, 90(2), 170-176.
130. Vogel, B. A., Leonhart, R., & Helmes, A. W. (2009). Communication matters: the impact of
communication and participation in decision making on breast cancer patients’ depression and quality
of life. Patient education and counseling, 77(3), 391-397.
131. Warnes, C. A., Williams, R. G., Bashore, T. M., Child, J. S., Connolly, H. M., Dearani, J. A. & Hunt,
S. A. (2008). ACC/AHA 2008 Guidelines for the Management of Adults With Congenital Heart
Disease: A Report of the American College of Cardiology/American Heart Association Task Force on
Practice Guidelines (Writing Committee to Develop Guidelines on the Management of Adults With
Congenital Heart Disease) Developed in Collaboration With the American Society of
Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease,
Society for Cardiovascular Angiography and Interventions, and Journal of the American College of
Cardiology, 52(23), 1890-1947
132. Wayne, S. (2013). “Theories of Nonverbal Communication,” in eHow, Retrieved 20 July,, 2014
from http://www.com/print/info_8255853_thories-Nonverbalcommunication. html.
133. Weathers, M., Query, J. L., & Kreps, G. L. (2010). A multivariate test of communication
competence, social support, and coping among Hispanic lay caregivers for loved ones with
Alzheimer’s disease: An extension of the Relational Health Communication Competence
Model. Journal of Participative Medicine, 2(1),14.
134. Weaver III, J. B., Mays, D., Weaver, S. S., Hopkins, G. L., Eroğlu, D., & Bernhardt, J. M. (2010).
Health information–seeking behaviors, health indicators, and health risks. American Journal of Public
Health, 100(8), 1520.
135. Williams, S. L., Haskard, K. B., & DiMatteo, M. R. (2007). The therapeutic effects of the physician-
older patient relationship: effective communication with vulnerable older patients. Clinical interventions
in aging, 2(3), 453.
136. Yilmaz, T. U., Gumus, E., & Salman, B. (2015). Problems in Communications with Patients in
General Surgery Outpatient Practice. The Eurasian journal of medicine, 47(3), 184.
137. Zachariae, R., Pedersen, C. G., Jensen, A. B., Rossen, P. B., & Von Der Maase, H. (2003).
Association of perceived physician communication style with patient satisfaction, distress, cancer-
related self-efficacy, and perceived control over the disease. British Journal of Cancer, 88(5), 658-665.