
Mid-Year Review of the Consolidated Appeal for Somalia ... Web viewORGANISATIONS PARTICIPATING IN...
92
REVISION
Transcript of Mid-Year Review of the Consolidated Appeal for Somalia ... Web viewORGANISATIONS PARTICIPATING IN...
REVISION

UN
DP
/Som
alia
/200
6
REVISION
ORGANISATIONS PARTICIPATING IN CONSOLIDATED APPEALS DURING 2007:
AARRECAASAAABSAbt AssociatesACF/ACH/AAHACTEDADRAAfricareAGROSPHEREAHAANERAARCIARMAVSICADICAMCARECARITASCCFCCIJDCEMIR Int’lCENAP
CESVICHFICINSCIRIDCISVCLCONCERNCOOPICORDCPARCRSCUAMMCWDCADRCEMSFERMEQUIPFAOGAA (DWH)GH
GSLGHDOHIHISAN - WEPAHorn ReliefILOINTERSOSIOMIRCIRDIRINJVSFMALAOMCIMDAMDMMENTORMERLINNANNANRCOA
OCHAOCPHODAGOHCHRPARACOMPARCPHGPMRSPRCSPSIPURFEPSADOSC-UKSECADEVSFCGSNNCSOCADIDOSolidaritésSPSTF
UNAIDSUNDPUNDSSUNESCOUNFPAUN-HABITAT UNHCRUNICEFUNIFEMUNMASUNODCUNRWAUPHBVETAIDVIAVTWFPWHOWVIWRZOARC
Consolidated Appeals Process (CAP)
The CAP is much more than an appeal for money. It is an inclusive and coordinated programme cycle of:
strategic planning leading to a Common Humanitarian Action Plan (CHAP); resource mobilisation (leading to a Consolidated Appeal or a Flash Appeal); coordinated programme implementation; joint monitoring and evaluation; revision, if necessary; and reporting on results.
The CHAP is a strategic plan for humanitarian response in a given country or region and includes the following elements:
a common analysis of the context in which humanitarian action takes place; an assessment of needs; best, worst, and most likely scenarios; stakeholder analysis, i.e. who does what and where; a clear statement of longer-term objectives and goals; prioritised response plans; and a framework for monitoring the strategy and revising it if necessary.
The CHAP is the foundation for developing a Consolidated Appeal or, when crises break or natural disasters strike, a Flash Appeal. Under the leadership of the Humanitarian Coordinator, the CHAP is developed at the field level by the Inter-Agency Standing Committee (IASC) Country Team. This team mirrors the IASC structure at headquarters and includes UN agencies and standing invitees, i.e. the International Organization for Migration, the Red Cross and Red Crescent Movement, and NGOs that belong to ICVA, Interaction, or SCHR. Non-IASC members, such as national NGOs, can be included, and other key stakeholders in humanitarian action, in particular host governments and donors, should be consulted.
The Humanitarian Coordinator is responsible for the annual preparation of the consolidated appeal document. The document is launched globally each November to enhance advocacy and resource mobilisation. An update, known as the Mid-Year Review, is to be presented to donors in July 2007.
Donors provide resources to appealing agencies directly in response to project proposals. The Financial Tracking Service (FTS), managed by the United Nations Office for the Coordination of Humanitarian Affairs (OCHA), is a database of donor contributions and can be found on www.reliefweb.int/fts.
In sum, the CAP works to provide people in need the best available protection and assistance, on time.
TABLE OF CONTENTS
1. EXECUTIVE SUMMARY.................................................................................................................... 1Table I: Summary of Requirements – by Appealing Organisation and by Cluster............3
2. COMMON HUMANITARIAN ACTION PLAN....................................................................................52.1 CHANGES IN THE CONTEXT AND ASSOCIATED CONSEQUENCES.................................................5
2.1a Context.............................................................................................................................. 5
2.1b Humanitarian Consequences............................................................................................9
3. MODIFIED RESPONSE PLANS......................................................................................................163.1 ACCESS AND SECURITY – CLUSTER LEADS: OCHA (ACCESS), UNDSS (SECURITY)...............16
3.2 FOOD SECURITY AND LIVELIHOODS – CLUSTER LEAD: WFP (FOOD), FAO (LIVELIHOODS)......18
Table A: Proposed Food Security and Livelihood Cluster Activities................................203.3 PROTECTION/HUMAN RIGHTS/RULE OF LAW – CLUSTER LEAD: UNHCR................................22
3.4 SHELTER FOR IDPS – CLUSTER LEAD: UNHCR....................................................................24
3.5 HEALTH – CLUSTER LEAD: WHO..........................................................................................25
3.6 NUTRITION – CLUSTER LEAD: UNICEF.................................................................................28
3.7 WATER AND SANITATION – CLUSTER LEAD: UNICEF.............................................................30
3.8 EDUCATION – CLUSTER LEAD: UNICEF.................................................................................32
CROSS-CUTTING SECTORS..................................................................................................353.9 EARLY RECOVERY (CROSS-CUTTING) – CLUSTER LEAD: UNDP.............................................35
3.10 GENDER (CROSS-CUTTING)...................................................................................................37
3.11 HIV/AIDS (CROSS-CUTTING) – CLUSTER LEAD: UNAIDS........................................................39
SUPPORT SECTORS...............................................................................................................403.12 LOGISTICS/SUPPORT – CLUSTER LEAD: WFP........................................................................40
3.13 COORDINATION/SUPPORT .....................................................................................................41
Table II: Summary of Requirements – by Sector...............................................................42
ANNEX I. INTEGRATED FOOD SECURITY AND HUMANITARIAN PHASE CLASSIFICATION REFERENCE TABLE...................................................................................................................... 43
ANNEX II. ESTIMATED RURAL POPULATION BY REGION IN HUMANITARIAN EMERGENCY AND ACUTE FOOD .................................................................................AND LIVELIHOOD CRISIS
45ANNEX III.LONG-TERM NUTRITION TRENDS (1999 - 2005)...........................................................46ANNEX IV..............NUMBER OF ORGANISATIONS CONSULTED DURING CAP CONSULTATION
PROCESS 2007............................................................................................................................... 47ANNEX V. CISS (FORMER SACB) AND IASC ORGANIGRAMME...................................................48ANNEX VI........................................................................UNITED NATIONS AGENCIES IN SOMALIA
49ANNEX VII...................................................................................ACRONYMS AND ABBREVIATIONS
50
Please note that appeals are revised regularly. The latest version of this document is available on http://www.humanitarianappeal.net.
iii
PROJECT SUMMARY SHEETS ARE IN A SEPARATE VOLUME ENTITLED “PROJECTS”
iv
v
SOMALIA – REVISION
1. EXECUTIVE SUMMARY
While still recovering from the worst drought in over a decade, Somalis suffered during the last months of 2006 and early 2007 both extensive flooding due to heavy Deyr rains and widespread conflict between the Transitional Federal Government and allied Ethiopian forces and the Islamic Courts Union.1 However, the Deyr rains of October-December, while causing large-scale displacement (estimated at 255,000) and the destruction of homes and assets, resulted in exceptionally good crop production and continued pastoral recovery. The recently completed post-Deyr 2006/07 assessment by the Food and Agriculture Organization/Food Security Analysis Unit shows many rural parts of Somalia – mainly in the north and central regions – experiencing an improvement in livelihood and food security. Around one million Somalis (including 400,000 internally displaced persons [IDPs]) are now in need of assistance and protection for the next six months, as compared to the 1.8 million identified in August 2006. In order to better reflect the improved food security situation and related humanitarian needs, the 2007 Consolidated Appeal (CAP) has been revised.
This revision takes account of the fact that any gains in food security must be viewed within Somalia’s long-standing humanitarian and security contexts. The post-Deyr food security analysis, while an essential tool, is not the only measure of humanitarian needs. Somalia has had no effective central government since 1991, leading to a destruction of infrastructure, disintegration of basic health and social services, widespread human rights abuses and some of the worst human development indicators in the world. Acute malnutrition rates continue to exceed the emergency threshold of 15% in many districts of South/Central. Following recent flooding, food security in riverine areas of the Juba and Shabelle Valleys deteriorated; the Juba Valley is facing a sustained humanitarian emergency. Moreover, the entire country remains chronically food-insecure. The population is highly vulnerable to any shocks – conflict or natural disaster – as evidenced by the recent outbreak of acute watery diarrhoea in South/Central Somalia. Since the start of 2007, acute watery diarrhoea (AWD) has resulted in 341 deaths out of 7,976 confirmed cases. Furthermore, several factors could negatively impact food security in the coming months. Aside from the risk of further conflict, the March 2007 Climate Outlook Forum forecasts normal to above-normal rainfall in the Ethiopian highlands and coastal areas of the Juba Valley. Such an eventuality may result in renewed flooding in riverine areas not yet recovered from Deyr floods.
The political landscape has been volatile over the last several months. In June 2006 – with the Transitional Federal Government (TFG) in command of little more than the government seat of Baidoa and warlords controlling most of southern Somalia – the ICU took control of Mogadishu. By mid-September the ICU controlled much of the south. However, in December 2006, just as floodwaters began to recede and flood response was moving into the Juba Valley, tension between the TFG and the ICU erupted into conflict in critical locations. By January, ICU militia had been defeated and TFG forces, backed by Ethiopian troops and air strikes, controlled much of southern Somalia, including Mogadishu. Since then, insecurity in Mogadishu has escalated, with regular attacks by anti-TFG factions on Ethiopian and TFG troops, as well as assassinations of persons seen as TFG supporters. Indiscriminate mortar attacks have resulted in hundreds of civilian casualties. Key installations such as Mogadishu airport and seaport have been shelled. Following the adoption by the Security Council of Resolution 1744, the first wave of the African Union Mission in Somalia (AMISOM) troops arrived in Somalia in early March. AMISOM troops and those providing logistical support to them have come under attack. On 23 March, an African Union-contracted aircraft was shot down on take-off from Mogadishu airport, killing all eleven passengers and crew members.
While there are an estimated 400,000 long-term internally displaced persons (IDPs) in Somalia, three new waves of displacement have occurred since November 2006. Deyr flooding displaced 255,000, while an estimated 65,000-70,000 people moved at the height of the fighting in December. The vast majority of both groups of IDPs have since returned home. More recently, there has been significant movement out of Mogadishu: between 1 February and 5 April 2007, around 124,000 people have fled Mogadishu due to the fighting. (Of these, around 47,000 fled in the last ten days of March alone.) They are in need of shelter, water and food. To date, access to IDPs and other vulnerable groups in need of assistance has been hampered by conflict, lack of security guarantees, ongoing military air operations, and clan tension. The Government of Kenya’s closure of its border with Somalia on security grounds for several weeks from early January also hindered humanitarian access and delivery of assistance.
1 ICU, also known as the Supreme Council of the Islamic Courts (SCIC) or Union of Islamic Courts (UIC).
1

SOMALIA – REVISION
Given the current context, the creation of an enabling environment for the delivery of humanitarian assistance must be supported. If Somalia slips back into anarchy, humanitarian space will inevitably be constricted. In order to respond effectively within the evolving environment, the humanitarian community is taking a number of steps, including: Moving towards a needs-based approach and away from an access-based approach to providing
assistance; Stepping up investment in the security sector, enabling – among other things – an increase in
personnel and the rehabilitation of UN compounds to render them compliant with Enhanced Minimum Operating Security Standards (EMOSS);
Increasing investment in South/Central Somalia, where the vast majority of humanitarian needs are, and encouraging more international partners to be present in South/Central Somalia;
Continuing to develop and strengthen partnerships with local NGOs and Somali partners, enhancing capacity for delivery of assistance through Somali channels.
In addition, to ensure principled action and a ‘do no harm’ approach, the humanitarian community has developed a set of Joint Operating Principles to promote behaviours in line with humanitarian principles and avoid fuelling the re-establishment of the system of coercion and violence perpetrated in the past by ‘gatekeepers.’
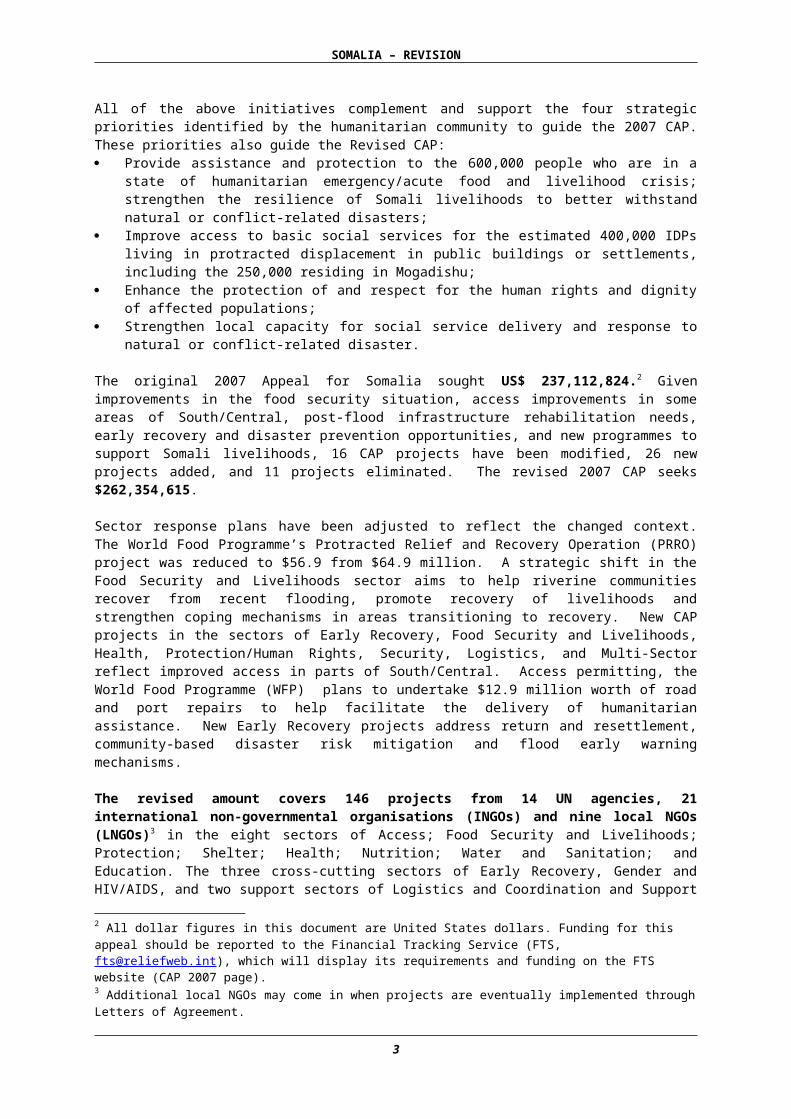
All of the above initiatives complement and support the four strategic priorities identified by the humanitarian community to guide the 2007 CAP. These priorities also guide the Revised CAP: Provide assistance and protection to the 600,000 people who are in a state of humanitarian
emergency/acute food and livelihood crisis; strengthen the resilience of Somali livelihoods to better withstand natural or conflict-related disasters;
Improve access to basic social services for the estimated 400,000 IDPs living in protracted displacement in public buildings or settlements, including the 250,000 residing in Mogadishu;
Enhance the protection of and respect for the human rights and dignity of affected populations; Strengthen local capacity for social service delivery and response to natural or conflict-related
disaster.
The original 2007 Appeal for Somalia sought US$ 237,112,824.2 Given improvements in the food security situation, access improvements in some areas of South/Central, post-flood infrastructure rehabilitation needs, early recovery and disaster prevention opportunities, and new programmes to support Somali livelihoods, 16 CAP projects have been modified, 26 new projects added, and 11 projects eliminated. The revised 2007 CAP seeks $262,354,615.
Sector response plans have been adjusted to reflect the changed context. The World Food Programme’s Protracted Relief and Recovery Operation (PRRO) project was reduced to $56.9 from $64.9 million. A strategic shift in the Food Security and Livelihoods sector aims to help riverine communities recover from recent flooding, promote recovery of livelihoods and strengthen coping mechanisms in areas transitioning to recovery. New CAP projects in the sectors of Early Recovery, Food Security and Livelihoods, Health, Protection/Human Rights, Security, Logistics, and Multi-Sector reflect improved access in parts of South/Central. Access permitting, the World Food Programme (WFP) plans to undertake $12.9 million worth of road and port repairs to help facilitate the delivery of humanitarian assistance. New Early Recovery projects address return and resettlement, community-based disaster risk mitigation and flood early warning mechanisms.
The revised amount covers 146 projects from 14 UN agencies, 21 international non-governmental organisations (INGOs) and nine local NGOs (LNGOs)3 in the eight sectors of Access; Food Security and Livelihoods; Protection; Shelter; Health; Nutrition; Water and Sanitation; and Education. The three cross-cutting sectors of Early Recovery, Gender and HIV/AIDS, and two support sectors of Logistics and Coordination and Support Services, are also represented. The Revised CAP retains the two-pillar structure – humanitarian relief and early recovery – of the original appeal. Early recovery activities aim to restore services, livelihood opportunities and governance capacity; 2 All dollar figures in this document are United States dollars. Funding for this appeal should be reported to the Financial Tracking Service (FTS, [email protected]), which will display its requirements and funding on the FTS website (CAP 2007 page).3 Additional local NGOs may come in when projects are eventually implemented through Letters of Agreement.
2
SOMALIA – REVISION
stabilise security; and address underlying risks that trigger conflict, drought and floods. As of 12 April, according to reports from donors and recipient organizations to the Financial Tracking Service (FTS), the original CAP 2007 was 33% funded, with $85,558,199 received. As with past appeals, funding has again favoured the food sector at 95%. Other key sectors such as Water and Sanitation (20%), Food Security and Livelihoods (8%), Health (4%), and Protection (2%) remain under-funded. Education has received no funds.4 It is essential that donors provide balanced funding so that humanitarian actors can mount a coherent and integrated response capable of addressing chronic vulnerabilities in Somalia.
Table I: Summary of Requirements – By Appealing Organisation and by Cluster
4 Though it is likely that agencies have allocated some flexible funds to education projects.
3
SOMALIA – REVISION
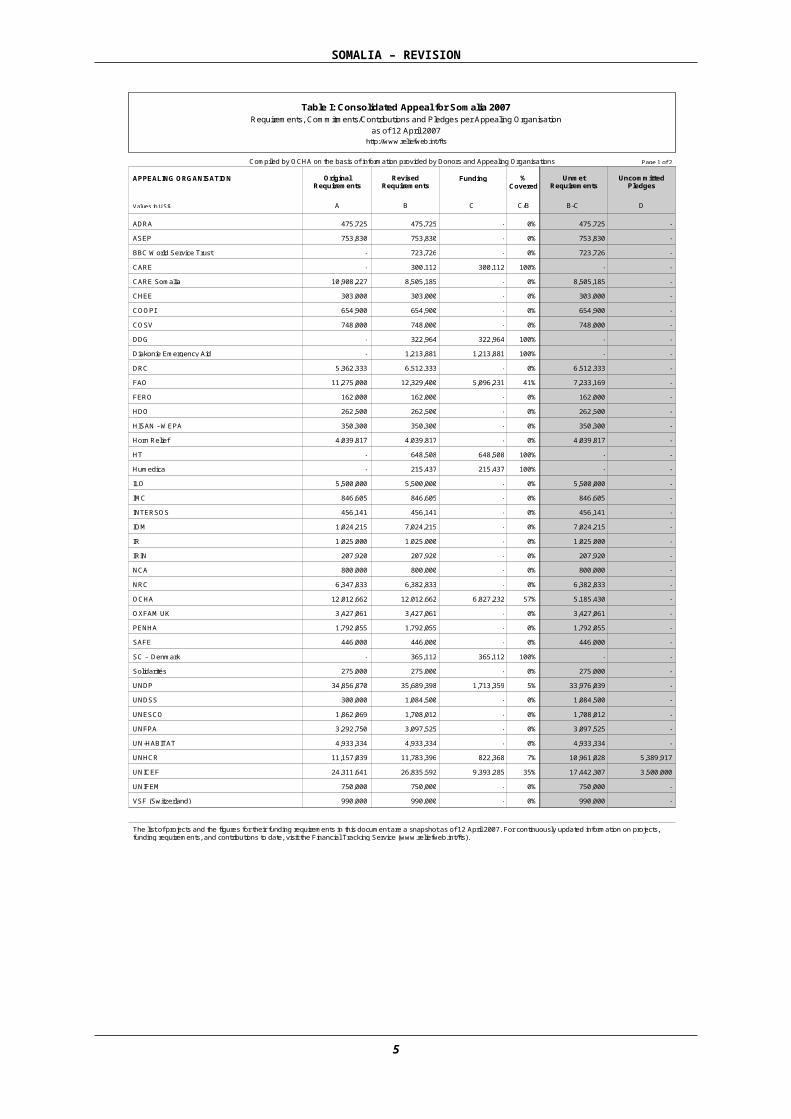
Table I: Consolidated Appeal for Somalia 2007 Requirements, Commitments/Contributions and Pledges per Appealing Organisation
as of 12 April 2007 http://www.reliefweb.int/fts
Compiled by OCHA on the basis of information provided by Donors and Appealing Organisations Funding Uncommitted
Pledges
APPEALING ORGANISATION % Covered Unmet
Requirements
Revised Requirements
Original Requirements
Values in US$ D A B C C/B B-C
Page 1 of 2
475,725 475,725 ADRA 0% - - 475,725 753,830 753,830 ASEP 0% - - 753,830
- 723,726 BBC World Service Trust 0% - - 723,726 - 300,112 CARE 100% - 300,112 -
10,908,227 8,505,185 CARE Somalia 0% - - 8,505,185 303,000 303,000 CHEE 0% - - 303,000 654,900 654,900 COOPI 0% - - 654,900 748,000 748,000 COSV 0% - - 748,000
- 322,964 DDG 100% - 322,964 - - 1,213,881 Diakonie Emergency Aid 100% - 1,213,881 -
5,362,333 6,512,333 DRC 0% - - 6,512,333 11,275,000 12,329,400 FAO 41% - 5,096,231 7,233,169
162,000 162,000 FERO 0% - - 162,000 262,500 262,500 HDO 0% - - 262,500 350,300 350,300 HISAN - WEPA 0% - - 350,300
4,039,817 4,039,817 Horn Relief 0% - - 4,039,817 - 648,508 HT 100% - 648,508 - - 215,437 Humedica 100% - 215,437 -
5,500,000 5,500,000 ILO 0% - - 5,500,000 846,605 846,605 IMC 0% - - 846,605 456,141 456,141 INTERSOS 0% - - 456,141
1,024,215 7,024,215 IOM 0% - - 7,024,215 1,025,000 1,025,000 IR 0% - - 1,025,000
207,920 207,920 IRIN 0% - - 207,920 800,000 800,000 NCA 0% - - 800,000
6,347,833 6,382,833 NRC 0% - - 6,382,833 12,012,662 12,012,662 OCHA 57% - 6,827,232 5,185,430
3,427,061 3,427,061 OXFAM UK 0% - - 3,427,061 1,792,055 1,792,055 PENHA 0% - - 1,792,055
446,000 446,000 SAFE 0% - - 446,000 - 365,112 SC - Denmark 100% - 365,112 -
275,000 275,000 Solidarités 0% - - 275,000 34,856,870 35,689,398 UNDP 5% - 1,713,359 33,976,039
300,000 1,084,500 UNDSS 0% - - 1,084,500 1,862,069 1,708,012 UNESCO 0% - - 1,708,012 3,292,750 3,097,525 UNFPA 0% - - 3,097,525 4,933,334 4,933,334 UN-HABITAT 0% - - 4,933,334
11,157,039 11,783,396 UNHCR 7% 5,389,917 822,368 10,961,028 24,311,641 26,835,592 UNICEF 35% 3,500,000 9,393,285 17,442,307
750,000 750,000 UNIFEM 0% - - 750,000 990,000 990,000 VSF (Switzerland) 0% - - 990,000
The list of projects and the figures for their funding requirements in this document are a snapshot as of 12 April 2007. For continuously updated information on projects, funding requirements, and contributions to date, visit the Financial Tracking Service (www.reliefweb.int/fts).
4
SOMALIA – REVISION
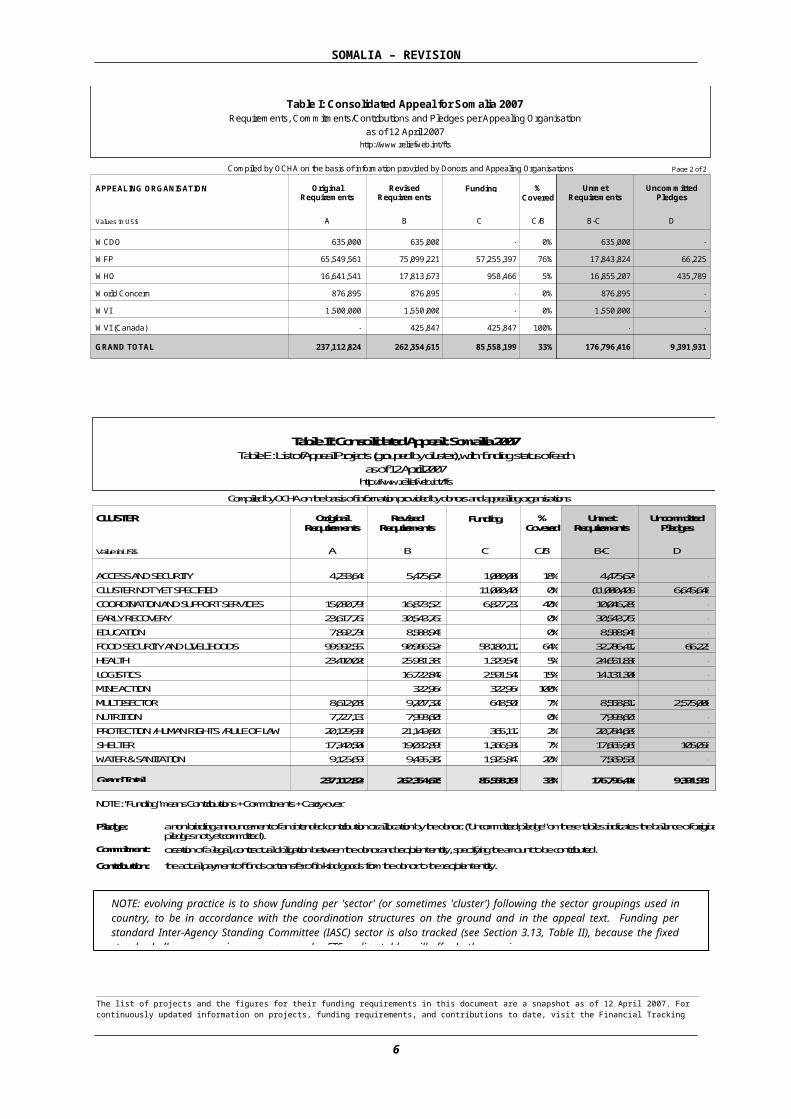
Table I: Consolidated Appeal for Somalia 2007 Requirements, Commitments/Contributions and Pledges per Appealing Organisation
as of 12 April 2007 http://www.reliefweb.int/fts
Compiled by OCHA on the basis of information provided by Donors and Appealing Organisations Funding Uncommitted
Pledges
APPEALING ORGANISATION % Covered Unmet
Requirements
Revised Requirements
Original Requirements
Values in US$ D A B C C/B B-C
Page 2 of 2
635,000 635,000 WCDO 0% - - 635,000 65,549,561 75,099,221 WFP 76% 66,225 57,255,397 17,843,824 16,641,541 17,813,673 WHO 5% 435,789 958,466 16,855,207
876,895 876,895 World Concern 0% - - 876,895 1,500,000 1,550,000 WVI 0% - - 1,550,000
- 425,847 WVI (Canada) 100% - 425,847 - 237,112,824 262,354,615 176,796,416 GRAND TOTAL 33% 85,558,199 9,391,931
Compiled by OCHA on the basis of information provided by donors and appealing organisations Original
Requirements Revised Requirements Funding %
Covered
Table II: Consolidated Appeal: Somalia 2007 Table E: List of Appeal Projects (grouped by cluster), with funding status of each
as of 12 April 2007 http://www.reliefweb.int/fts
CLUSTER
Value in US$ A B C C/B
Unmet Requirements
B-C
Uncommitted Pledges
D 5,475,674 4,233,646 4,475,674 - 1,000,000 18% ACCESS AND SECURITY
- - (11,000,409) 6,645,648 11,000,409 0% CLUSTER NOT YET SPECIFIED 16,873,521 15,030,795 10,046,289 - 6,827,232 40% COORDINATION AND SUPPORT SERVICES 30,543,763 23,617,763 30,543,763 - - 0% EARLY RECOVERY 8,588,945 7,892,736 8,588,945 - - 0% EDUCATION
90,966,524 99,992,557 32,786,412 66,225 58,180,112 64% FOOD SECURITY AND LIVELIHOODS 25,981,381 23,410,026 24,651,836 - 1,329,545 5% HEALTH 16,722,840 - 14,131,300 - 2,591,540 15% LOGISTICS
322,964 - - - 322,964 100% MINE ACTION 9,207,320 8,612,039 8,558,812 2,575,000 648,508 7% MULTI-SECTOR 7,993,605 7,727,131 7,993,605 - - 0% NUTRITION
21,149,801 20,129,938 20,784,689 - 365,112 2% PROTECTION / HUMAN RIGHTS / RULE OF LAW 19,032,895 17,340,500 17,665,965 105,058 1,366,930 7% SHELTER 9,495,382 9,125,693 7,569,535 - 1,925,847 20% WATER & SANITATION
Grand Total 262,354,615 237,112,824 176,796,416 9,391,931 85,558,199 33%
a non-binding announcement of an intended contribution or allocation by the donor. ("Uncommitted pledge" on these tables indicates the balance of original pledges not yet committed).
Pledge: creation of a legal, contractual obligation between the donor and recipient entity, specifying the amount to be contributed.
Commitment: Contribution: the actual payment of funds or transfer of in-kind goods from the donor to the recipient entity.
NOTE: "Funding" means Contributions + Commitments + Carry-over
The list of projects and the figures for their funding requirements in this document are a snapshot as of 12 April 2007. For continuously updated information on projects, funding requirements, and contributions to date, visit the Financial Tracking Service (www.reliefweb.int/fts).
NOTE: evolving practice is to show funding per 'sector' (or sometimes 'cluster') following the sector groupings used in country, to be in accordance with the coordination structures on the ground and in the appeal text. Funding per standard Inter-Agency Standing Committee (IASC) sector is also tracked (see Section 3.13, Table II), because the fixed standard allows comparison across appeals. FTS on-line tables will offer both groupings.
5
SOMALIA – REVISION
2. COMMON HUMANITARIAN ACTION PLAN
The Common Humanitarian Action Plan (CHAP) for the 2007 CAP – which outlines strategies for addressing the needs of Somalis affected by conflict and natural disaster – is essentially still valid, as the underlying causes of the protracted humanitarian crisis remain. However, changes in the political and humanitarian context have occurred in recent months. These changes – along with their immediate consequences for vulnerable populations and possible climatic and political scenarios for the near future – are outlined in the sections that follow.
2.1 CHANGES IN THE CONTEXT AND ASSOCIATED CONSEQUENCES2.1A CONTEXTSomalia has experienced a deterioration in humanitarian and security contexts since late 2006 due first to extensive flooding in south and central regions of the country and then to widespread conflict between TFG/Ethiopian forces and the ICU that broke out in December and the insecurity that has prevailed since, particularly in Mogadishu. However, while the heavy Deyr rains caused flooding, they also resulted in exceptionally good crop production and continued pastoral recovery. According to the recently completed Food and Agriculture Organization/Food Security Analysis Unit (FAO/FSAU) post-Deyr 2006/07 assessments, many parts of Somalia – mainly in the north and central regions – are thus experiencing an improvement in livelihoods and food security. Around one million Somalis are now in need of assistance and protection for the next six months (including 400,000 IDPs), as compared to the 1.8 million identified in August 2006. (See Annex II: Estimated Rural Population by Region in Humanitarian Emergency and Acute Food and Livelihood Crisis)
Both positive and negative recent developments must be seen in the context of chronic underlying problems and a humanitarian situation that has been critical for several years. Somalia has had no effective central government since 1991. Its population has been without basic health and social services and has suffered ongoing-armed conflict, human rights abuses, repeated displacement, and chronic food insecurity. Consequently, Somalia has some of the worst human development indicators in the world. Approximately 43% of Somalis live below the extreme poverty line, with less than 30% consuming the minimum dietary daily energy requirements.5 Life expectancy is 48 years. Gross school enrolment rates are 34% for boys and 22% for girls. Approximately one in six Somali children dies before the age of five, and 1,013 Somali women die of complications related to pregnancy or childbirth for every 100,000 live births.6 At present, acute malnutrition rates exceed the emergency threshold of 15% in districts of South/Central Somalia, and over 50,000 children are estimated to be malnourished and at risk of death. Moreover, the entire country remains classified as chronically food-insecure.
As a result of the above, the population remains extremely vulnerable to any new shock. The current insecurity in Mogadishu has left at least 124,000 people displaced, exposed to multiple threats to their health and safety. Furthermore, renewed flooding may be imminent. Weather forecasts call for near normal rainfall over much of Somalia during the upcoming Gu season (mid-April to mid-June) and a high probability of above normal rain in the upper catchments of the Ethiopian highlands. Such an eventuality could cause flooding in downstream riverine areas of southern Somalia and have a detrimental affect on food security, particularly in riverine areas that have not yet recovered from Deyr floods. Flooding could also worsen the acute watery diarrhoea situation (as of 17 March, there were 7,976 cases of AWD, with 341 deaths) and would likely compound existing difficulties vis-à-vis humanitarian access.
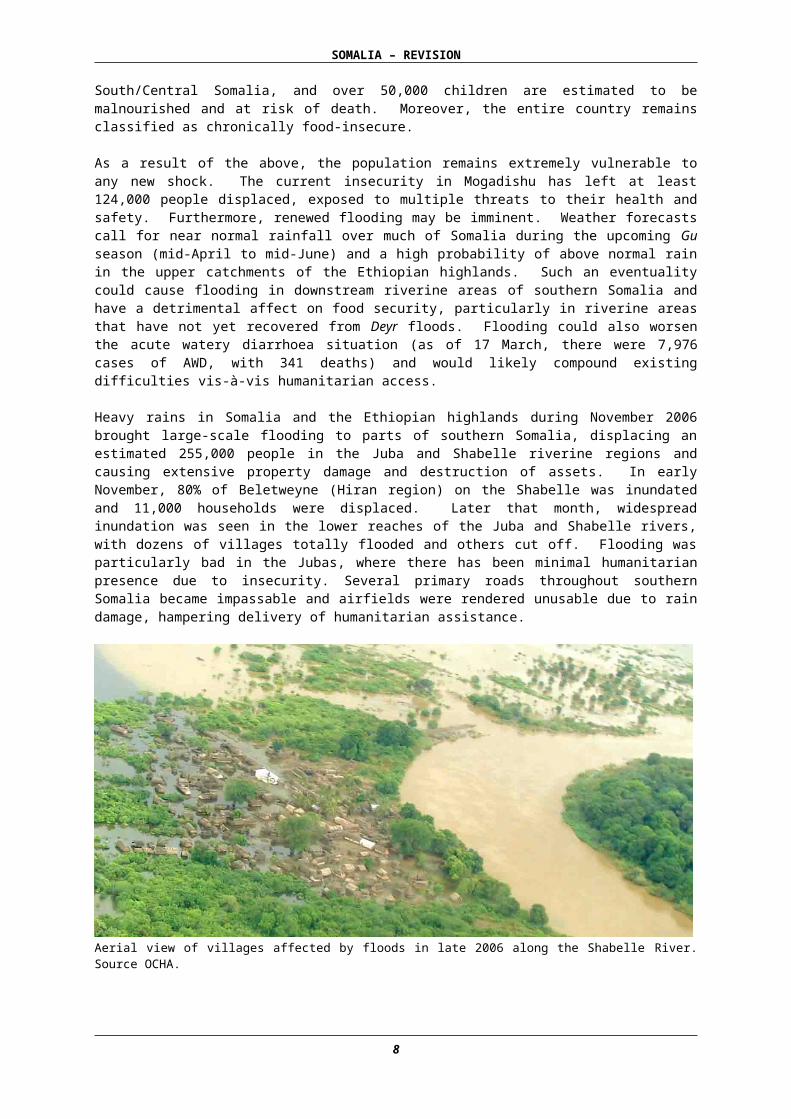
Heavy rains in Somalia and the Ethiopian highlands during November 2006 brought large-scale flooding to parts of southern Somalia, displacing an estimated 255,000 people in the Juba and Shabelle riverine regions and causing extensive property damage and destruction of assets. In early November, 80% of Beletweyne (Hiran region) on the Shabelle was inundated and 11,000 households were displaced. Later that month, widespread inundation was seen in the lower reaches of the Juba and Shabelle rivers, with dozens of villages totally flooded and others cut off. Flooding was particularly bad in the Jubas, where there has been minimal humanitarian presence due to insecurity.
5 UNDP Socio Economic Survey 2002 reports that about 43% of the Somali population is estimated to be in extreme poverty (per capita income less than $1 per day) with 23% in urban and 53% in rural and nomadic areas. General poverty in Somalia (per capita income less than $2 per day) is estimated as 73% (60% urban and 79% rural and nomadic).6 UNICEF Preliminary results of the 2006 Multiple Indicator Cluster Survey (MICS).
6
SOMALIA – REVISION
Several primary roads throughout southern Somalia became impassable and airfields were rendered unusable due to rain damage, hampering delivery of humanitarian assistance.
Aerial view of villages affected by floods in late 2006 along the Shabelle River. Source OCHA.
Just as the situation along both rivers began to stabilise – with flood waters receding and humanitarian flood response moving into the Jubas – tension between the TFG and the ICU erupted into conflict in critical locations in southern Somalia. In early December, fighting spread from around Baidoa (seat of the TFG), to central Galkayo, Hiran and Middle Shabelle, with ICU militia retreating and TFG forces, backed by Ethiopian troops and air strikes, taking control of areas previously held by the ICU. By early January, Ethiopian/TFG forces were in control of much of southern Somalia, including Mogadishu.
Since then, southern Somalia has seen a return of generalised insecurity, with the re-establishment of checkpoints (along with reports of banditry, extortion and rape), sporadic clan fighting and the re-appearance of warlords. Insecurity in Mogadishu, meanwhile, has escalated, with a number of assassinations, several mortar attacks on key sites (airport, seaport, presidential palace, military bases) and indiscriminate shelling resulting in dozens of civilian casualties. In early March, the first AMISOM troops arrived in Mogadishu. The mission’s mandate includes protecting the transitional federal institutions (TFIs), supporting dialogue and reconciliation, and contributing to the creation of the necessary security conditions for the provision of humanitarian assistance. So far, the presence of AMISOM troops has not resulted in enhanced security. The third week of March saw three serious incidents. A UN convoy, accompanied by Somali Special Protection Unit (SPU), was attacked by a roadside bomb and small arms fire 30 kms from Mogadishu. The attack did not result in any death. As of today, it is not yet clear whether the attack was against the UN or the SPU. Days later, an AU-contracted aircraft was shot down on take-off from Mogadishu airport, killing all eleven passengers and crew. A suspected suicide bomb followed at an Ethiopian base north of Mogadishu, killing at least eight soldiers.
Access to both flood-affected and conflict-affected populations was complicated by a number of factors in late 2006 and early 2007. Conflict, military air operations (including two United States [US] air strikes) and the resulting insecurity seriously compounded access difficulties to South/Central Somalia. With the onset of the conflict and the temporary closure by the TFG of Somalia’s borders, UN agencies and NGOs relocated their international staff to Nairobi in December 2006. In early January, the Government of Kenya sealed its border with Somalia on security grounds, preventing all overland movement of humanitarian cargo or staff. The closure order prevailed into the first weeks of February when, following extensive negotiations between humanitarian actors and the Government of Kenya, cargo began to cross. Furthermore, 2007 has seen the harassment and arbitrary detention of aid workers by Ethiopian forces. In February, the first act of piracy in nine months occurred when a WFP-contracted ship was hijacked after having delivered food in Puntland.
In spite of the above obstacles, it is essential that humanitarian partners remain committed to building on positive developments and new opportunities for access. Some improvements in access have already occurred. After being closed since 1991 in the south and for over a year in the north, the
7
SOMALIA – REVISION
divided city of Galkayo (Puntland), which hosts a large IDP population, is now open and a multi-agency response to IDPs has begun. There is now permanent international presence in north Galkayo serving both sides of the city, and joint north/south technical committees on water and education have been established. Moreover, multi-agency missions have travelled to Mogadishu during January and February to focus on response to the IDP population there (est. 250,000), and profiling of IDPs in all sixteen districts was concluded in February. A number of airstrips within the country have opened again, as security clearance is gained or flood damage repaired, enabling increased movement within Somalia of national and international staff. Capacity-building of national NGOs and greater interest from international NGO partners has increased potential to assist IDPs in South/Central.
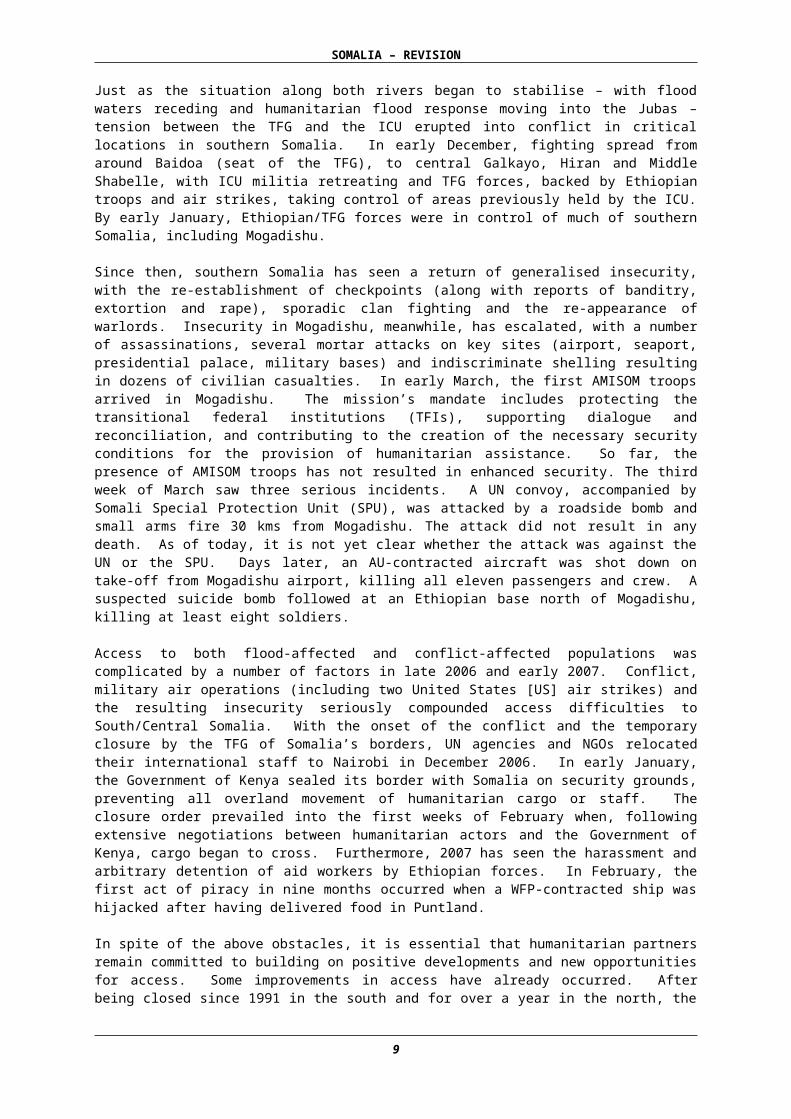
Several long-standing protection concerns have continued into late 2006 and early 2007. Reports continue of arbitrary detentions without trial and mistreatment of prisoners. Sexual and gender-based violence (SGBV) is of grave concern and is particularly high among marginalised clans and in IDP settlements. Women and girls risk being raped when collecting firewood or water. In 2006, the Protection Monitoring Network monitored 639 women who had reported rape; after six months, 10% of these women had committed suicide and another 20% were missing. IDPs and minority clans continue to have limited access to shelter, water, sanitation, education, and health care. (More recent protection concerns that have arisen following the conflict are described in the Humanitarian Consequences section.)
Three significant waves of displacement occurred between November 2006 and the present. Flooding displaced an estimated 255,000 people, while between 65,000 and 70,000 people are thought to have been displaced at the peak of the recent conflict. Some of the latter had already moved due to flooding. Most conflict-related displacement was localised and the vast majority of these IDPs have since returned home, as have those displaced by flooding. Additionally, an estimated 124,000 people were displaced from Mogadishu between 1 February and 5 April due to insecurity. All of the above displacement has occurred in the context of a large caseload of protracted internal displacement. There are an estimated 400,000 long-term IDPs throughout Somalia, with 250,000 of these in Mogadishu. There are also large populations of IDPs in Kismayo (Lower Juba) and Hargeisa (Somaliland), as well as Bossaso, Garowe and Galkayo (Puntland). Those in protracted displacement tend to have no clan-based protection and thus are particularly vulnerable; they are not hosted by the local community and live in settlements and public buildings. Due to lack of access, IDPs in Mogadishu particularly have received very limited humanitarian assistance over the last several years.
Most IDPs live in shelters made of scrap material or in public buildings. They lack adequate sanitary facilities and the incidence of communicable diseases is high. The majority are women and children, experiencing multiple and protracted displacements and facing discrimination, exploitation and physical violence. In some cases, de facto authorities divert humanitarian assistance and deny IDPs access to basic services, such as water and food. Poverty forces IDP girls into exploitative work relationships, and child labour is one of several survival mechanisms for IDP families. Casual work and begging provide some income but are barely sufficient for one meal a day, resulting in high malnutrition and mortality rates. Levels of acute malnutrition among IDPs are generally above those of resident communities.7 Access to education is often related to the protection environment, as is access to health facilities. Currently, IDPs in Mogadishu (and other urban centres) face potential eviction from public buildings, as the government continues to move the TFIs into the capital.
7 In an inter-agency survey conducted in two IDP settlements in Wajid in February 2006, a total of 142 children from 111 households were assessed with a global acute malnutrition of 27.1% and severe acute malnutrition of 9%. During the survey, it was noted that the main reasons for movement were a lack of food and/or water (77.3%), civil insecurity (9%) and lack of income generating opportunities (9%). The rates of malnutrition were higher than the surrounding area. (FSAU Monthly Nutrition Update, February 2006)
IDPs in Galkayo, Puntland, living in deplorable conditions. Source OCHA
8
SOMALIA – REVISION
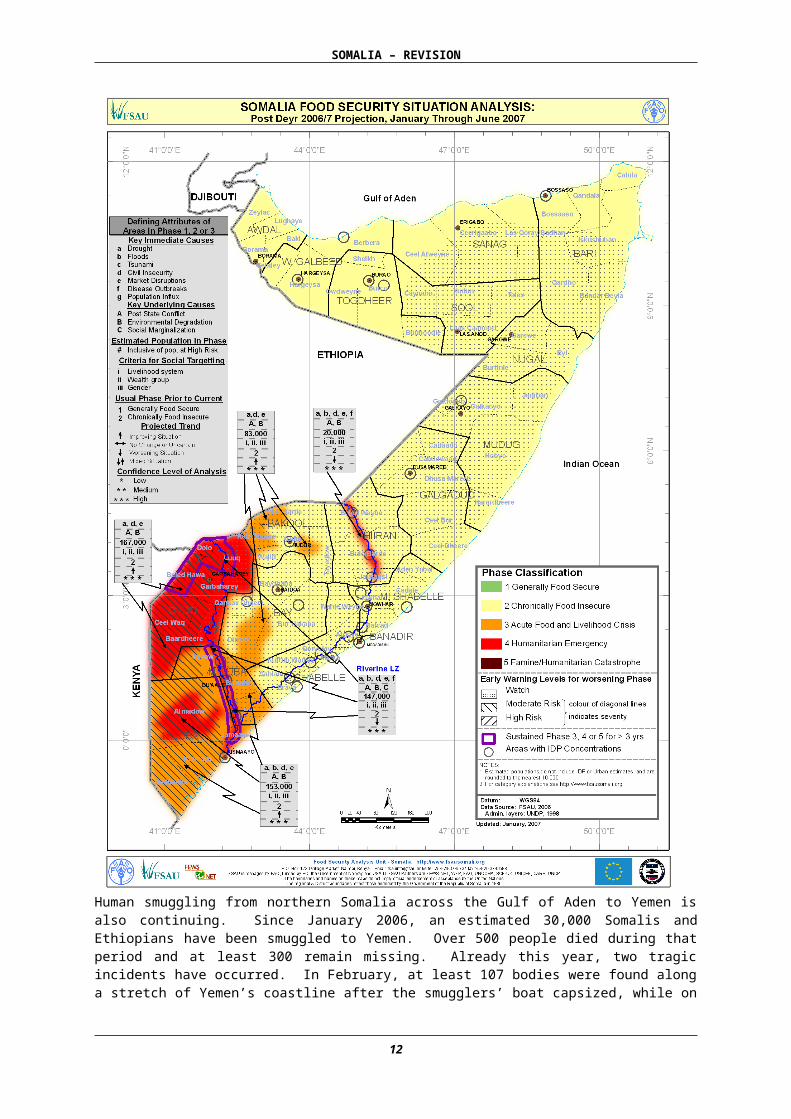
Human smuggling from northern Somalia across the Gulf of Aden to Yemen is also continuing. Since January 2006, an estimated 30,000 Somalis and Ethiopians have been smuggled to Yemen. Over 500 people died during that period and at least 300 remain missing. Already this year, two tragic incidents have occurred. In February, at least 107 bodies were found along a stretch of Yemen’s coastline after the smugglers’ boat capsized, while on 22 March, at least 29 people died and 71 others went missing after smugglers forced some 450 Somalis and Ethiopians into the sea during the journey to Yemen.
9
SOMALIA – REVISION
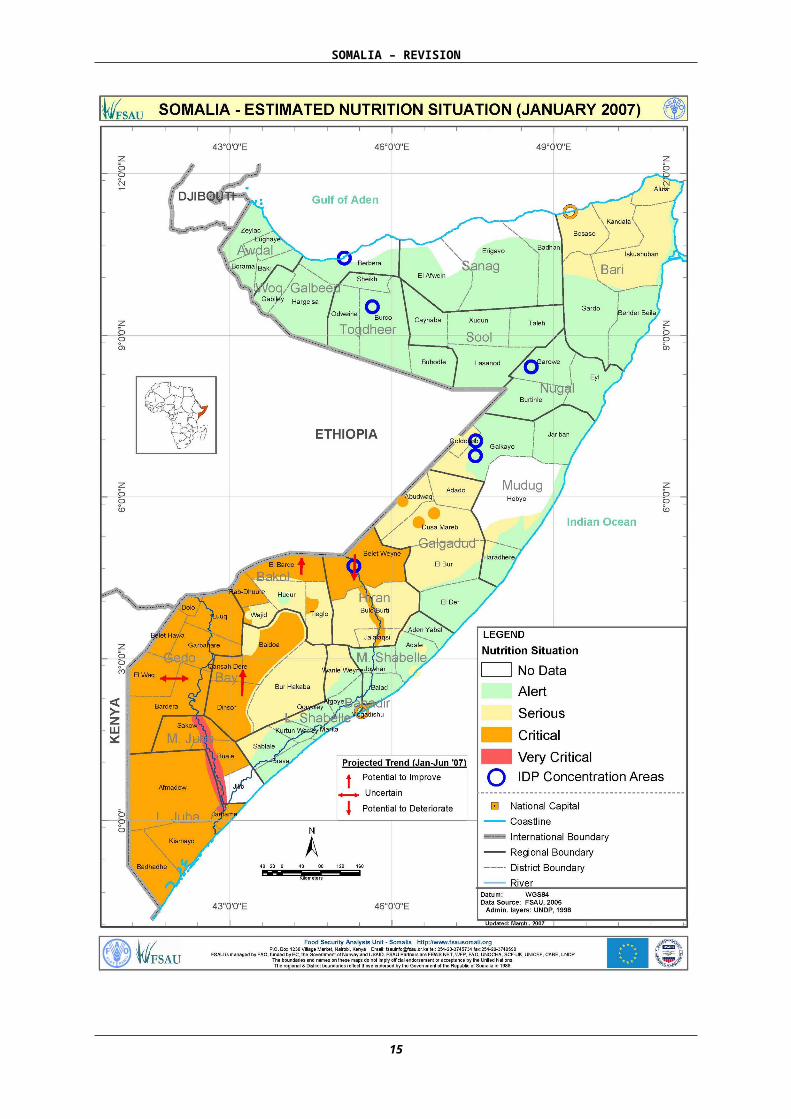
2.1B HUMANITARIAN CONSEQUENCESAccording to the findings of the FAO/FSAU-led Post-Deyr Assessment (January 2007), 600,000 Somalis in rural areas and 400,000 IDPs will be in need of assistance and protection for at least the coming six months, as compared to the 1.8 million identified in August 2006. The improvement is primarily due to heavy 2006/7 Deyr rains, which resulted in good to exceptional crop production in many areas – mainly in northern and central regions. The food security and livelihoods situation has improved in all regions except riverine areas along the Juba and Shabelle rivers; riverine areas of Gedo and Middle and Lower Juba remain in a state of Humanitarian Emergency, while the riverine areas of Hiran have seen a deterioration in livelihood and food security. Hiran, Bay and Bakool (except for some pockets) are now out of Acute Food and Livelihood Crisis, as is the north of Somalia. The map Somalia – Food Security Situation Analysis Jan-June 2007 (Page 11) outlines the current location and degree of vulnerability throughout Somalia.
Despite the overall improvement, the humanitarian situation in Somalia remains critical. The post-drought nutrition crisis persists, with acute malnutrition rates continuing to exceed the emergency threshold of 15% in districts of South/Central Somalia (critical levels in Lower Juba and Gedo regions, and in large parts of Middle Juba, Bay, Bakool and Hiran). Over 50,000 children are estimated to be malnourished and at risk of death in South/Central. Marginalised groups, and IDPs present particularly high malnutrition levels. Moreover, the entire country remains classed as Chronically Food-insecure.
Gains in food security are therefore tenuous and do not automatically translate into widespread improvement in the nutrition situation. Multiple aggravating factors prevail – poor dietary diversity, poor maternal and childcare practices, inadequate health services and poor hygienic conditions. Risks remain which may negatively impact on the situation, including further conflict and diseases such as cholera. Meanwhile, the benefits of good post-Deyr crop production will partly depend on the security situation in South/Central Somalia, as localised or widespread conflict could impede access to markets and production areas, as well as lead to increased prices, population displacement and loss of assets. The performance of the next rainy season (Gu: March-April) will also have an effect. While heavy Gu rains could help crop production, localised flooding may have a detrimental effect on food security, especially in riverine areas still recovering from Deyr flooding.
The humanitarian consequences of the Deyr flooding were multiple: estimated 255,000 people were displaced; cross-border movement was limited having cut off many roads. Although the vast majority of these IDPs have since returned to their places of origin, many returned to destroyed or damaged homes, and severe asset loss. Moreover, the impact of recent flooding on the nutrition situation is only now emerging, with increased admissions to feeding programmes in riverine areas. Vector and water-borne diseases especially AWD rose significantly. As of 17 March 2007, 7,976 cases of AWD had been confirmed, with 341 deaths in eight regions of South/Central Somalia. Due to initiatives by health partners, the incidence of AWD is decreasing in some regions. However, in Banadir (Mogadishu) and Lower Shabelle regions, AWD continued to rise into mid-March. In Lower Shabelle, this was due at least in part to the influx of IDPs from Mogadishu and the additional strain placed on already inadequate water sources. Concern is growing about AWD in Mogadishu as any increase in insecurity may inhibit humanitarian response to the caseload. Any localised flooding resulting from the upcoming Gu rains could worsen the AWD situation.
10
SOMALIA – REVISION
11
SOMALIA – REVISION
The flooding exacerbated long-standing problems in Somalia related to water and sanitation. It is estimated that up to 70% of the population does not have reliable access to safe water throughout the year. Less than 40% of Somalis live in households with sanitary means of disposing of excreta.8
Diarrhoeal disease-related dehydration, respiratory infections, and malaria are the main killers of infants and young children, together accounting for more than half of all child deaths. The major underlying causes of diarrhoea are the lack of access to safe water and poor food and domestic hygiene, while a main underlying cause of child morbidity is lack of access to safe drinking water. The destruction and looting of water supply installations during the civil war, continuing conflict, and a general lack of maintenance of water supply systems have all contributed to the lack of access to potable water. The situation is compounded by erratic rainfall patterns that produce both drought and flooding.
The conflict of late 2006 between TFG/Ethiopian forces and the ICU, although violent, was brief and mostly took place outside of urban centres, therefore not resulting in significant damage to existing infrastructure. The death toll may have been high but remains unconfirmed. The United Nations High Commissioner for Refugees (UNHCR) has estimated that 65,000-70,000 people were displaced at the peak of the fighting. Many Somalis attempted to seek asylum in Kenya. However, as a result of the Kenyan border closure, approximately 4,700 would-be asylum seekers were stranded in Dhobley (Somalia) in early January in deteriorating conditions. (This number included more than 400 Somali asylum-seekers who were deported from Kenya on 3 January despite, in many cases, having already been screened and registered by Kenyan authorities). People living on the Somali side of the border who would normally have crossed to Liboi for health care and schooling have been unable to access either due to the border closure. Meanwhile, many of the IDPs have scattered to nearby towns and others have moved to larger IDP settlements in Kismayo and Jilib. The issue of asylum-seekers remains unresolved, as Somalis are still unable to cross the border into Kenya.
Since the cessation of major hostilities, Mogadishu has experienced escalating violence, including mortar attacks in which many civilians have been killed or injured. According to the International Committee of the Red Cross (ICRC), between the start of 2007 and 25 February more than 430 war-wounded were admitted to two Mogadishu hospitals. UNHCR has estimated that between 1 February and 5 April, 124,000 people moved out of Mogadishu due to insecurity. Many of these went to Middle and Lower Shabelle, Bay, Gedo, Somaliland and Puntland.
In addition to long-standing protection concerns, new or increased human rights abuses have accompanied the recent conflict. All parties to the fighting carried out child recruitments. Indiscriminate mortar and rocket propelled grenade (RPG) attacks in Mogadishu have resulted in dozens of civilian deaths. There were reports of Ethiopian troops arbitrarily arresting and harassing members of the Oromos minority. Revenge killings of individuals thought to have sympathised with the ICU have occurred and, more recently, assassinations in Mogadishu of TFG supporters have taken place. IDPs have been moved from some public buildings – such as Mogadishu’s Digfir hospital – so that military forces could occupy them. Finally, there has been an increase in freelance militia looting, harassing, and raping civilians at checkpoints in southern Somalia.
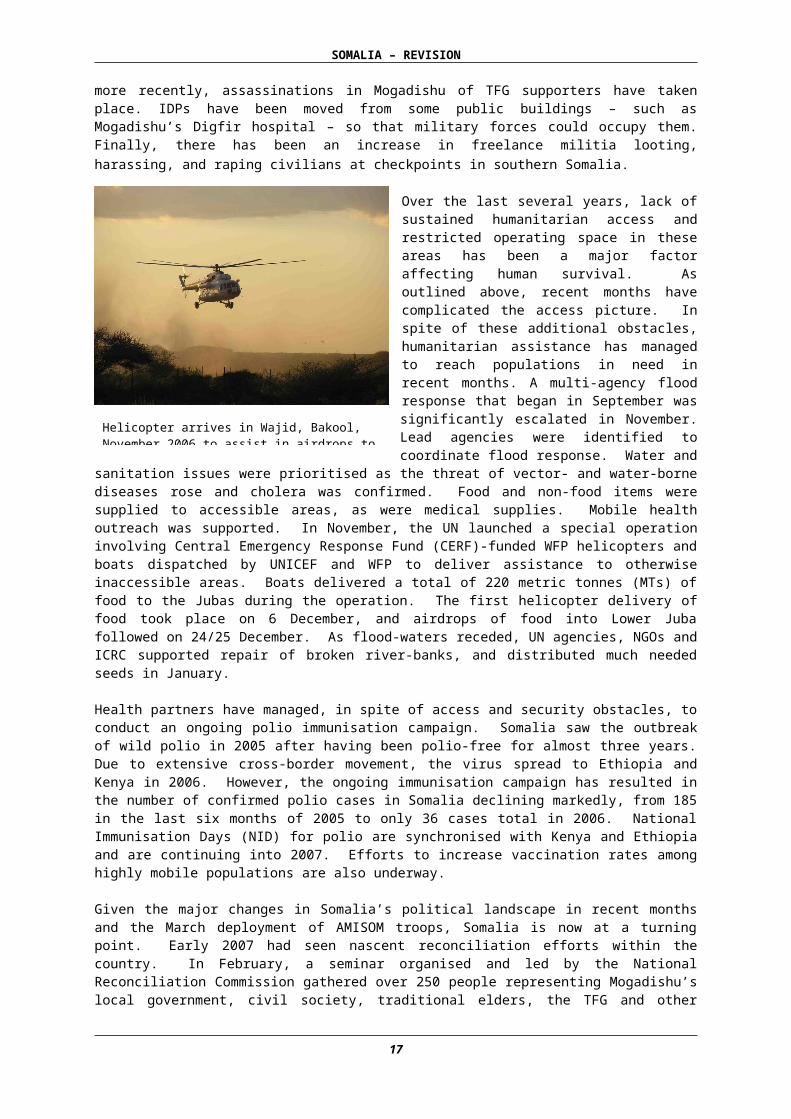
Over the last several years, lack of sustained humanitarian access and restricted operating space in these areas has been a major factor affecting human survival. As outlined above, recent months have complicated the access picture. In spite of these additional obstacles, humanitarian assistance has managed to reach populations in need in recent months. A multi-agency flood response that began in September was significantly escalated in November. Lead agencies were identified to coordinate flood response. Water and sanitation issues were prioritised as the threat of vector- and water-borne diseases rose and cholera was confirmed. Food and non-food items were supplied to accessible areas, as were medical supplies. Mobile health outreach was supported. In November, the UN
8 UNICEF Preliminary results of the 2006 Multiple Indicator Cluster Survey (MICS).
Helicopter arrives in Wajid, Bakool, November 2006 to assist in airdrops to flood-affected areas.
12
SOMALIA – REVISION
launched a special operation involving Central Emergency Response Fund (CERF)-funded WFP helicopters and boats dispatched by UNICEF and WFP to deliver assistance to otherwise inaccessible areas. Boats delivered a total of 220 metric tonnes (MTs) of food to the Jubas during the operation. The first helicopter delivery of food took place on 6 December, and airdrops of food into Lower Juba followed on 24/25 December. As flood-waters receded, UN agencies, NGOs and ICRC supported repair of broken river-banks, and distributed much needed seeds in January.
Health partners have managed, in spite of access and security obstacles, to conduct an ongoing polio immunisation campaign. Somalia saw the outbreak of wild polio in 2005 after having been polio-free for almost three years. Due to extensive cross-border movement, the virus spread to Ethiopia and Kenya in 2006. However, the ongoing immunisation campaign has resulted in the number of confirmed polio cases in Somalia declining markedly, from 185 in the last six months of 2005 to only 36 cases total in 2006. National Immunisation Days (NID) for polio are synchronised with Kenya and Ethiopia and are continuing into 2007. Efforts to increase vaccination rates among highly mobile populations are also underway.
Given the major changes in Somalia’s political landscape in recent months and the March deployment of AMISOM troops, Somalia is now at a turning point. Early 2007 had seen nascent reconciliation efforts within the country. In February, a seminar organised and led by the National Reconciliation Commission gathered over 250 people representing Mogadishu’s local government, civil society, traditional elders, the TFG and other stakeholders. The seminar focused on ways to resolve Mogadishu’s insecurity and pave the way for the TFG to dialogue with constituents in Mogadishu; it concluded with several recommendations. The TFG and Parliament have since agreed to convene a 45-day National Reconciliation Congress for all Somali people. The Congress, scheduled to begin in April, may be delayed until May due to the escalation of insecurity in Mogadishu. The international community must support and ensure inclusive reconciliation efforts at national, regional and district levels, as it is only through inclusive dialogue that sustainable peace and stabilisation can be achieved. Part of this international support is coming in the form of a set of priorities developed by the UN for the six-month period February-August 2007. This plan aims to increase potential for re-engagement and assistance provision, bolstering stabilisation in Somalia through strengthened TFIs and provision of urgently needed services, particularly in Mogadishu. It focuses on five key areas: institutional capacity building; rule of law and security; provision of basic social services; urgent assistance to IDPs; and employment/livelihoods recovery.
POLITICAL SCENARIOS
Following the ousting of the ICU from Mogadishu and other parts of South/Central Somalia by a coalition of forces loyal to the TFG in late December/early January, the TFG has been involved in efforts to reach out to stakeholders in the peace and reconciliation process. A National Reconciliation Congress is scheduled for May 2007. A consultative meeting held in early February in Mogadishu laid a foundation for this upcoming Reconciliation Congress. The TFG insists that the Congress be held on the basis of clan. However, the international community has insisted that the process should be inclusive, opening the door to all elements of society with an expressed commitment to peace and stability for Somalia.
Best-Case Scenario: The TFG announces that it is open to an inclusive dialogue and political process that allows for the successful implementation of the Transitional Federal Charter, including the drafting of a new constitution and the holding of a national census and referendum. The outcome of the Reconciliation Congress paves the way for free and fair elections and sustainable peace in Somalia. The presence of AMISOM helps to create a more secure environment for the delivery of humanitarian assistance – particularly in Mogadishu – and UN agencies and INGOs are able to establish much greater permanent presence in South/Central, including Mogadishu.
Most Likely Scenario: The Reconciliation Congress is held on the basis of clan, consistent with the Transitional Federal Charter. The TFG proceeds with a reconciliation process on its own terms, excluding some key political actors. It resists international pressure to bring other actors on board, and thus maintains the status quo. As a consequence, the TFG continues to rely on AMISOM for protection as the current anti-TFG military operation persists and most likely intensifies. Although challenges to access remain, humanitarian actors invest more in security and seek to continue to implement activities on a needs basis throughout South/Central.
13
SOMALIA – REVISION
Worst-Case Scenario: In the absence of a genuine, inclusive reconciliation process, the anti-TFG military operation intensifies and escalates, gaining popular support. AMISOM forces are embroiled in the fighting or are targeted, along with government officials, police, foreigners, etc. South/Central Somalia, and particularly Mogadishu return to the violence and anarchy that characterised the country and the capital for the last several years. Foreign interference increases and engenders long-term instability for the entire Horn. There is large-scale internal displacement from Mogadishu and other flashpoints such as Kismayo, and rising cross-border movement to Kenya and Yemen. Humanitarian space shrinks as the vulnerable population grows.
CLIMATIC SCENARIOS
Rainfall ForecastThe nineteenth Climate Outlook Forum for the Greater Horn of Africa (GHA) was held in Nairobi in March 2007. The consensus regarding the upcoming Gu rains (April-June) is that there is an increased likelihood of near normal rainfall over much of the GHA between March and May. However, there is high probability that some parts of the upper catchments of Juba and Shabelle River valleys in the Ethiopian highlands will receive near to above normal Gu rains. In most of Somalia itself there is enhanced probability of near normal to below normal rains. The only exceptions within Somalia are some coastal areas of the Juba valley where an increased likelihood of near normal to above normal rainfall is forecast.
ConsequencesClimatic conditions will affect livelihoods, food security, nutrition, health, and population movements. Given the fact that most of Somalia received above normal Deyr rains, another season of normal rainfall may further improve crop production and rangeland condition and enhance the post-drought recovery process. However, even normal to above normal rainfall in the Ethiopian highlands will likely result in another season of flooding in riverine areas of southern Somalia, where flood-damaged river-banks remain saturated, weak and damaged. The majority of the population in the river valleys is still suffering the effects of the flooding of the last Deyr season. If the above forecast holds true, the rains and any subsequent flooding can be expected to exacerbate the humanitarian emergency, especially in Juba valley.
Contingency Plans Given the high probability and continuing cycles of natural and man-made disasters in Somalia, and current levels of vulnerability, the need for inter-agency contingency planning remains paramount. Cluster-led emergency preparedness and response planning for renewed widespread conflict, Gu season flooding, and a deterioration of nutritional and livelihood status, among other scenarios, will continue to use an operational based approach and ensure geographical coverage, especially in the most vulnerable parts of Somalia. The Inter-Agency Standing Committee (IASC) Emergency Preparedness and Response Plan for Somalia will be updated to reflect the current context, which includes the above political scenarios, the post-Deyr assessment, and the possibility of additional flooding during the Gu.
The Office for the Coordination of Humanitarian Affairs (OCHA) is continuing to update the mapping and response capacity of humanitarian partners, particularly Somali NGOs, in the most vulnerable and under-served parts of Somalia. Where clusters are not present or active, OCHA will seek individual agency commitments (UN or NGO) by sector to assume lead or shared responsibilities for future emergency response. The IASC Emergency Preparedness and Response Plan continues to be developed in close coordination with regional partners in neighbouring Kenya and Ethiopia, and is designed to complement other agency and organisation contingency/emergency preparedness plans.
STRATEGIC PRIORITIES and COORDINATION STRUCTURES
The Consolidated Appeals Process (CAP)Consultations for the 2007 Somalia CAP took place in Hargeisa, Garowe, Baidoa, Mogadishu, and Nairobi in August 2006 with more than 330 participants, including representatives from 16 UN agencies, 40 local NGOs, 30 international NGOs, local authorities and the TFG. Thirteen donors were consulted in a separate meeting in the first week of September. (See Annex Four: Organisations Consulted During CAP 2007 Consultation Process). The Revised 2007 CAP, done in consultation with cluster leads and cluster members, aims to better reflect current humanitarian needs in Somalia following the release of the FAO/FSAU post-Deyr 2006/7 assessments. The Revised CAP takes into
14
SOMALIA – REVISION
account recent changes in the overall political picture and their potential effect on humanitarian operations.
The focus of the CAP 2007 – and of the Revised CAP – is on providing humanitarian assistance and protection to vulnerable populations in Humanitarian Emergency or Acute Food and Livelihood Crisis and to 400,000 IDPs. The CAP is structured along two pillars – humanitarian relief and early recovery – and its focus is on assisting populations in south and central regions which have been difficult to access in the past due to insecurity and lack of local partners. Such assistance seeks to save lives, reduce human suffering and promote self-reliance and sustainable livelihoods. The humanitarian community will also focus on overcoming major response constraints through more systematic advocacy on access and strengthening the capacity of local partners.
AdvocacyOn behalf of the IASC, OCHA Somalia is facilitating the development and implementation of a collaborative advocacy strategy, the overall goal of which is to improve the conditions for delivery of humanitarian assistance and protection of vulnerable populations. As this is an important element of CAP 2007, there is an urgent need for far greater resources – both financial and human – to ensure that activities are carried out at local, national, and international levels. The OCHA advocacy strategy focuses on four elements: increasing humanitarian access, protection of civilians, improving the credibility of the humanitarian community, and increasing the profile of Somalia internationally. With the current political uncertainty, the need for advocacy, including the promotion of humanitarian principles and prioritisation of the most vulnerable groups within Somalia, has never been greater. One of the primary policy elements of the advocacy strategy will be the finalisation and implementation of the Joint Operating Principles, which aim to promote behaviour in accordance with humanitarian principles and avoid fuelling the re-establishment of the system of coercion and violence perpetrated in the past by ‘gatekeepers’. (See Executive Summary)
Early RecoveryEarly recovery activities under the CAP require the coordinated involvement of the CAP clusters in the identification of priority needs for sustainable results alongside the purely humanitarian response. Early recovery activities should increase in significance over time as they bridge the gap between humanitarian and development assistance. These activities are crucial for stabilisation and should begin in the humanitarian phase in order to prepare for more development-oriented activities. Through greater UN field presence and coordination capacity, an integrated and more comprehensive early recovery response can be put in place, building beyond short-term humanitarian support to establishing foundations for longer-term development. Whereas activities are concentrated on the community level, conditions for engagement are the presence of nascent government structures, increased access, basic reconciliation and peace-building, as well as local administration planning capacity, all of which will contribute to more sustainable reintegration of displaced population.
While the CAP concentrates on meeting urgent humanitarian and early recovery needs, the Somalia Reconstruction and Development Programme (RDP) builds on the Joint Needs Assessment for Somalia and lays out immediate priorities for recovery, aiming to support the transition from humanitarian assistance to development. The RDP will function as an instrument for mobilising, distributing, and coordinating international recovery assistance. The UN will implement significant portions of the RDP beginning in 2007 and will broaden implementation in 2008 with the harmonised UN Transition Plan. The Early Recovery pillar of the CAP 2007 therefore focuses on increasing the impact of humanitarian assistance and laying the foundation for later-stage recovery. It is separate from the implementation of the RDP but will, over time, be integrated with it. Likewise, early recovery links with the UNHCR-initiated Comprehensive Plan of Action for Somali Refugees, Returnees and IDPs, which seeks durable solutions for displaced Somalis in the region, partly through creating conditions conducive to their return and reintegration in their country of origin.
15
SOMALIA – REVISION
CoordinationIn 2006, in line with global humanitarian reform initiatives, Somalia was one of four countries that piloted a national IASC9–supported by OCHA and chaired by the Humanitarian Coordinator (HC), with membership from seven UN agencies, seven NGOs and the ICRC as an observer. It developed clusters10 of relevant partners to improve preparedness and response and fill gaps across the sectors and cross-cutting issues. The cluster approach will be continued in 2007 to meet the humanitarian needs of highly vulnerable Somalis. Inter-cluster coordination meetings are now held twice monthly. Other coordination mechanisms have been adapted and strengthened. Efforts are ongoing to streamline coordination mechanisms, most recently between the Coordination of International Support to Somalis (CISS)/Somalia Support Secretariat (SSS) and the IASC cluster coordination modalities.
CISS/SSS: The Somalia Aid Coordination Body (SACB) has been phased out and replaced by the CISS (Coordination of International Support to Somalis) and remains focused on medium/longer-term development/transition issues in Somalia. Under its new name, the Secretariat began functioning in August 2006. It is a single, harmonised, transitional secretariat to support the political, planning, and technical coordination between the international community and Somalia through various joint committees. The Coordination and Monitoring Committee (CMC) is the highest-level mechanism for coordination between the TFG and the international community. The Joint Planning Committee (JPC), which will eventually address planning, and operational matters, and the Joint Thematic Committee (JTC), which will be responsible for thematic/technical and sectoral issues on aid coordination, have not been operational since 2005. In the absence of these committees, the Secretariat is essentially providing support to the CISS constituencies (United Nations Country Team [UNCT], IASC, Somali Donor Group [SDG], NGO consortium and Sectors Chairs).
HC/RC Integration: In addition to existing coordination mechanisms, the UNCT for Somalia has developed a plan for strengthening its coordination function and its ability to provide coordination support services to government and international partners. The plan includes moving towards “One UN” – through the adoption of a single results-based country programme (the UN Transition Plan for 2008-2009), joint programming, and improved capacity for joint implementation. The UNCT will set up an integrated structure to support the Resident Coordinator (RC) and HC functions so as to better respond to needs in Somalia through a mix of relief, recovery, and development. The UNCT is also strengthening links between the HC/RC functions and the SSS/CISS to streamline services and maximise use of resources. Coordination support and secretariat services in the field and for all constituencies would be enhanced through the opening of field coordination offices by the UN HC/RC office and the SSS, which would – as far as possible – be imbedded in national authorities.
9 The IASC membership includes OCHA, United Nations Development Programme (UNDP), United Nations Children's Fund (UNICEF), WFP, FAO, World Health Organization (WHO), UNHCR, Cooperative for Assistance and Relief Everywhere (CARE), Gedo Health Consortium (GHC), Danish Refugee Council (DRC), OXFAM/Nederlandse Organisatie voor Internationale Bijstand (NOVIB), CONCERN, Save the Children (SC)-UK and Advancement for Small Enterprise Programme (ASEP). ICRC participates as an observer, while FAO/FSAU and Famine Early Warning System Network (FEWS-Net) are technical advisors. It meets on a monthly basis. 10 Somalia’s Nine Clusters: Health, Nutrition, Water and Sanitation (WASH), Shelter, Food, Education, Agriculture and Livelihood, Protection and Logistics.
16
SOMALIA – REVISION
3. MODIFIED RESPONSE PLANS
3.1 ACCESS AND SECURITY – CLUSTER LEADS: OCHA (ACCESS), UNDSS (SECURITY)Analysis of NeedsSomalia remains one of the most worrying humanitarian crises in the world. Currently, there are approximately one million people projected to be in need of humanitarian assistance until at least June 2007. The majority of these people are in south/central Somalia, in areas in which the delivery of effective and timely humanitarian assistance is most hampered by lack of sustained access. Reliable access and improved security conditions are essential if the urgent needs of the most vulnerable are to be addressed. Following changes in the political landscape in late 2006 and early 2007, access to south/central Somalia remains a formidable challenge. The continued presence of troops and military operations in the Juba valley, closure of the Kenya-Somali border, sporadic clan conflict, recent violence in Mogadishu and the lack of local authorities/counterparts all characterise the operational environment.
While some relief response could be achieved even in a narrowing humanitarian space, initiation of early recovery activities requires more sustained access. The new political environment, despite existing challenges, presents possibilities for enhanced humanitarian access. Current re-engagement and investment plans for Somalia place increased emphasis on making the security posture sufficiently robust in order to sustain a field presence despite varying levels of volatility. Essential to achieving these goals are: the establishment of sufficiently "hardened" UN compounds in key locations, the provision of adequate communications and protective equipment, the availability of effective contingency capacity (e.g. medical support), and the provision of enhanced security training to allow staff to work effectively under the prevailing conditions (see Executive Summary). In addition to up-scaling operational support to more effectively manage security risks, efforts should be geared towards better engagement at local level, support of peace-building and reconciliation, and advocacy at local, regional and global levels.
Objectives Enhance and ensure the safety and security of humanitarian staff and operations. Establish and implement a humanitarian advocacy strategy with the objective of improving
conditions for effective, efficient, and timely delivery of humanitarian assistance. Enhance engagement with local communities and consolidate emerging peace-building initiatives
and local reconciliation efforts to facilitate implementation of early recovery and livelihood support.
Enhance emergency preparedness through thematic and geographically based inter-agency contingency plans, including the participation of local partners and taking into account prioritised vulnerabilities of the Somali population.
Develop a common access approach to better inform and sustain humanitarian actions in complex environments.
Development of common inter-agency security system, based on the United Nations Department of Safety and Security (UNDSS) Minimum Operating Security Standards (MOSS) and Enhanced Minimum Operating Security Standards (EMOSS) for two locations in south/central Somalia (locations to be decided).
Rehabilitation of UN common premises in Mogadishu to meet EMOSS and Minimum Operating Residential Security Standards (MORSS) requirements.
Partnerships OCHA, UNDSS, UNDP, IASC members, CISS, local, national and de-facto authorities.
Key Indicators Mechanisms in place for the safety and security of humanitarian operations/activities and aid
workers (information, secure premises and accommodation, adequate security equipment, training and operational support).
Humanitarian advocacy plan developed and disseminated, awareness raising about, and support mobilisation for the needs of the one million people most affected by the on-going crisis.
Local reconciliation efforts supported, leading to enhanced access. Adequate contingency plans in place, including necessary preparedness measures (mapping of
capacities, stock piling and human resources mobilisation).
17
SOMALIA – REVISION
Regions with sustained humanitarian access and where early recovery response has been initiated.
Activities Ensure the availability and dissemination of timely and accurate security risk assessments with
regard to programme activities in the region. Ensure that all staff are optimally informed on security measures and receive appropriate security
training. Upgrade and implement safety/security measures at selected airstrips, mainly in central and
south Somalia. Strengthen information dissemination activities on humanitarian access issues and required
actions targeting stakeholders at all levels. Strengthen engagement and participation of national and local authorities in existing inter-agency
coordination mechanisms (clusters) as the basis for more transparent and accountable humanitarian response.
Negotiate access with local authorities on the ground, including de-facto authorities, with focus on priority areas in central and south.
Develop a national contingency planning exercise (at both strategic and operational levels). Focus on enhanced emergency preparedness and response capacity building. Facilitate coordination of a common access approach through the existing Access Working
Group. Promote basic humanitarian principles and ensure the buy-in and commitment of local and
national authorities and leadership.
Monitoring The organisations and agencies working in this sector will monitor – depending on their expertise, mandates, and areas of responsibilities and deployment – progress in achieving the sector objectives. This will be realised through regular reporting on the state of dissemination and implementation of the advocacy plan, contingency plans, security of humanitarian action and staff, and a common access approach. Reporting will be coordinated and consolidated by OCHA.
Projects listed under this sector mainly focus on security. On the other hand, activities to enhance access (such as advocacy, contingency planning and enhanced coordination) are mainstreamed across the other operational sectors. Reconciliation and peace-building activities will be pursued within a project submitted by UNDP under the Early Recovery Sector.
Implications If the Response Plan is Not ImplementedIn view of the direct implication of security and access on the delivery of humanitarian assistance, failure to implement this response plan will result in a lack of urgently needed assistance and increased humanitarian suffering. Approximately one million people, including those in humanitarian emergency and livelihood crisis, IDPs, and other vulnerable groups are at risk of increased malnutrition rates, further depletion of assets, collapse of basic services, and even more vulnerable groups are put at risk.
18
SOMALIA – REVISION
3.2 FOOD SECURITY AND LIVELIHOODS – CLUSTER LEADS: WFP (FOOD), FAO (LIVELIHOODS)Analysis of NeedsThe livestock sector remains a crucial element in the economy of Somalia. Drought and floods are a recurrent phenomenon in the region where pastoralists experience prolonged dry seasons and high variability in precipitation. During prolonged dry seasons, households expect a degree of austerity as livestock production and values decline, and grain prices increase. In a chronic situation, where water availability falls below the requirements for average crop and rangeland production, a prolonged dry season becomes a drought. Normally, pastoralists in Somalia experience such a widespread failure once every three to five years and a major drought once every ten years. Though localised seasonal flooding is common in parts of the Juba valley, serious localised riverine flooding events occur on average once every five years, extensive flooding such as occurred in 1997/98 and 2006/2007 roughly every ten years and major widespread catastrophic riverine flooding around once in every fifty years. The consequences of drought and riverine flooding are compounded in Somalia by other factors such as civil unrest and population movement.
Somalia is historically a cereal deficit country; consequently, a large proportion of the national cereal requirement is imported (either commercially or through food aid). Poor rural households produce 20 to 60% of their own food requirements in any given year and the balance is either purchased or obtained through barter. Therefore, individual production and the ability of households to purchase food are key determinants to food security in Somalia. The direct effects of drought, floods, insecurity and lack of governance on food security, nutrition, and livelihood include: Limited own food production (cereal stock consumed during preceding poor harvests and
drought, and, in areas affected by flooding, lost due to inundation of underground grain stores by flood waters);
Low Terms of Trade cereal relative to labour and livestock; Reduction in livestock holdings from drought or increased prevalence of disease in flooded areas; Reduced access to markets; Low prices for agricultural and livestock commodities; Low labour opportunities; Poor food utilisation because of high incidence of diseases (e.g. diarrhoea, acute respiratory
infection (ARI), malaria, aflatoxin contamination of stored grain, etc.); High incidence of diseases and limited health services.
However, since the recent Deyr 2007 harvest, the overall livelihood and food security situation in Somalia has improved as compared to the situation between June and December 2006. The improvements are reflected in a decrease in the overall numbers of people requiring humanitarian assistance and livelihood support from 1.8 million to about a million. Of the 590,000 rural populations in need of humanitarian assistance, 80% are in Gedo, Lower, and Middle Juba regions, while 20% are in Bay, Bakool and Hiran regions. Well-distributed Deyr rainfall significantly above normal (150-300% of long-term mean) has been beneficial for most agro-pastoral and pastoral livelihood groups. However, exceptionally high river flows during November/December 2006 led to the displacement of some 255,000 people along the Juba and Shebelle rivers with severe flooding of villages, loss of grain in underground stores, inundation of farmland and destruction of standing crops. Failure of most of the Juba and Shebelle riverine maize production as a consequence of riverine flooding resulted in maize production of only 50% of the post-war average (PWA). Overall, however, cereal production, at 113% of the PWA, for the recent Deyr season has been above normal. Both in the rain-fed sorghum production areas of the Bay (228% of PWA) and Bakool (398% of PWA) regions, sorghum grain production have been exceptional.
To foster recovery but also respond to the pressing humanitarian needs, the Food Aid and the Agriculture and Livelihood clusters recognise and stress the need for long-term solutions for the agriculture and livestock sectors, in conjunction with humanitarian actions. The fact that the Deyr 2006 rains were above average and well distributed does not imply that the impacts of drought and the crisis, especially in the livestock sector, are over. It is estimated that recovery times for agro-pastoralists and pastoralists, especially for households relying on cattle, could take between four to ten years to recover from the 2005 drought. With the subsequent impact of floods in the riverine areas, the impact of sporadic conflict and the possibility of flooding in the coming 2007 “Gu” season, the recovery process could easily be prolonged.
19
SOMALIA – REVISION
The response strategy of the Food Security and Livelihoods sector is based on agreement that the crises affecting the livelihoods of pastoral, agro-pastoral and agricultural communities warrant a sound mechanism over time at two levels: immediate relief action to the most vulnerable areas, as well as short to early recovery actions targeting different livelihood groups. As in 2006, the strategy aims at preventing families in the “Chronically food-insecure” phase to fall into “Acute Livelihood Crisis” and “Humanitarian Emergency” phases; while it should allow families in “Humanitarian Emergency” to resume livelihoods, regain productive assets and return progressively to a sustainable livelihood.
Cluster Objectives Protect and improve household food security, including asset base, through increasing access
and availability to food and means of production. Ensure that resource allocation for food security and livelihood support is proportional to the
Integrated Food Security and Humanitarian Phase Classification or IPC11. Increase participation and involvement of women in food security and livelihoods actions. Strengthen local institutional and community capacity in order to maximise response for most
vulnerable areas/groups. Strengthen community capacity to cope with future shocks.
Partnerships Reflected in the CAPFAO/FSAU/Somalia Water and Land Information Management system (SWALIM), Famine Early Warning System Network (FEWSNET), UNDP, WFP; Action Contre la Faim (ACF), African Rescue Committee (AFREC), Agrosphere, Advancement for Small Enterprise Programme (ASEP), Candlelight for Health, Education and Environment (CLHEE), CARE, European Committee for Agricultural Training (CEFA), Cooperazione Internazionale (COOPI), Comitato di Coordinamento delle Organizzazioni per il Servizio Volontario (COSV), DRC, Family Empowerment and Relief Organisation (FERO), Grada, Green Hope, Horn of Africa Relief and Development Organization (HARDO), Horn Relief, Humanitarian Development Organisation (HDO), Jubaland Charity Centre (JCC), OXFAM GB, Pastoral and Environmental Network in the Horn of Africa (PENHA), Social-Life and Agricultural Development Organisation (SADO), Save the Children-United Kingdom (SC-UK), Solidarites, UNDP, Veterinary Aid (VETAID), Vétérinaires Sans Frontières (VSF)-Switzerland, World Concern, World Vision International (WVI).
Indicators and Monitoring Provision of food through general food distribution, food for assets and social support programme
to 850,000 people. Reduction of the number of households in “Humanitarian Emergency” phase in southern
Somalia. Near complete and irreversible depletion of key livelihood assets is averted (preventing
households in “Acute Livelihood crisis” phase to fall to “Humanitarian Emergency” phase). Increased number of national NGOs partners involved in planning and implementation of
humanitarian response.
11 See Annex One: Integrated Food Security and Humanitarian Phase Classification Reference Table.
20
SOMALIA – REVISION
Table A: Proposed Food Security and Livelihood Cluster Activities
Cluster Priority Programmes in Support of Strategic PrioritiesFOOD SECURITY and LIVELIHOODS
Specific Objectives Priority Actions to Achieve Cluster ObjectivesProtect and improve household food security, including asset base, through increasing access and availability to food and means of production.
1. Food distribution to vulnerable and displaced populations with no visible means of support in Gedo, Lower and Middle Juba, Hiran, Middle Shabelle, Bay and Bakool, Mudug and Galgaduud.
2. Livelihoods diversification in Lower and Middle Juba regions.3. Targeted cash relief and cash for work for key infrastructure
rehabilitation in support of livelihoods in Gedo, Lower and Middle Juba.
4. Agropastoralist community drought mitigation activities in Bakool.5. Strengthening of public rural infrastructure, increased fodder
production, construction of sand dams in seasonal rivers in drought-prone areas, rehabilitation of river embankments in line with SWALIM recommendations, and improved capacity of veterinary services for diseases surveillance and emergency treatment in flood-impacted areas, as well as in relation to the Lower, Middle Shabelle, Bakool and Hiran regions, and the carcass and live animal export trade.
6. Targeted Seed distribution to areas with significant crop failure, improved run-off water utilisation for agriculture in Gedo region, animal re-distribution to marginalised pastoralists, provision of pack camels for increased mobility of pastoralist households in Sanaag region, targeted de-stocking in event of “Gu” failure, and other livestock interventions where and when appropriate.
7. Improved food storage, processing and marketing by women in Middle Juba and Bay regions.
8. Large-scale community-based water conservation, floodwater management and controlled irrigation and rangeland management in support of sustainable livelihoods and food security in Middle Shabelle, Bari, Nugaal, Togdheer, Sool and Sanaag regions.
9. Support to riverine fisheries activities through inputs distribution and training (Lower and Middle Shabelle).
10. HIV/AIDS12 prevention, treatment, home-based care, and enhancement of food security for affected, in particular, women-headed households in southern Somalia.
Ensure that resource allocation for food security and livelihood support is proportional to the “Integrated Food Security and Humanitarian Phase Classification” (IPC).
1. Coordination (Somali Support Secretariat, IASC Clusters), support for regional emergency coordination structures at the field level, and general advocacy.
Increase participation and involvement of women in food security and livelihoods actions.
1. Mainstream gender dimension in every project proposal;2. Promotion of participatory needs assessments and women’s
representation in local community committees.
Strengthen local institutional and community capacity in order to maximise response for most vulnerable areas/groups.
1. Direct support to “credible” Somali partners (e.g. in monitoring and evaluation, reporting, and financial tracking) through direct funding of Somali proposals.
2. Training and support of local relief committees (focus on women’s groups).
3. Support to local initiatives addressing conflict prevention.4. Capacity building for key line ministries and regional/district
service-oriented representation.Strengthen community capacity to cope with future shocks.
1. Food-for-Work and Cash-for-Work to support key infrastructure rehabilitation in support of rural livelihoods in Gedo, Lower and Middle Juba, Hiran, Bakool, Mudug, Galgaduud, Lower and Middle Shabelle, Bari, Nugaal, Sool, Sanaag, Togdheer.
2. Agropastoralist community drought mitigation activities in Bakool.3. Strengthening of public rural infrastructure improved run-off water
utilisation for agriculture in Gedo region, increased fodder production, animal re-distribution to marginalised pastoralists, provision of pack camels for increased mobility of pastoralist
12 Human Immuno-deficiency Virus /Acquired Immuno-deficiency Syndrome.
21
SOMALIA – REVISION
Cluster Priority Programmes in Support of Strategic PrioritiesFOOD SECURITY and LIVELIHOODS
Specific Objectives Priority Actions to Achieve Cluster Objectiveshouseholds in Sanaag region, targeted de-stocking in event of “Gu” failure, and other livestock interventions where and when appropriate.
4. Improved livestock diseases surveillance, emergency disease control capacity and improved animal health in Gedo, Lower and Middle Juba, Bakool, Hiran , Lower and Middle Shabelle).
5. Support to livelihood diversification in the Lower and Middle Juba, and for destitute pastoralists in Sool, Sanaag, Bari, Nugaal, and Togdheer regions.
6. Environmental protection and soil conservation (all pastoral areas);
7. Water conservation activities, including sub-surface dams, water harvesting (Gedo, Lower and Middle Juba, W. Galbeed).
8. Improved food storage, processing and marketing by women in Middle Juba and Bay regions.
9. Input distribution and training (Lower and Middle Shabelle) to support riverine fisheries activities.
10. HIV/AIDS prevention, treatment, home-based care and enhancement of food security for affected, in particular, women-headed households in southern Somalia.
Implications If the Response Plan is Not Implemented Marginalised groups will fall into destitution or, at best, livelihood recovery will be delayed and
slow, exposing them further to future shocks. Increased potential conflict over resources. Increased number of households engaged in unsustainable coping mechanisms. Limited access to vulnerable populations in remote or insecure areas if local capacity is not
strengthened; Continued closure of livestock export markets will impact severely on pastoralist household
economy, not only in Somalia but in Ethiopia also. Increased or maintained high malnutrition rates in most affected districts.
22
SOMALIA – REVISION
3.3 PROTECTION/HUMAN RIGHTS/RULE OF LAW – CLUSTER LEAD: UNHCRAnalysis of Needs With continuing instability and sporadic violence in many parts of the country, weak governance structures, and limited access to some vulnerable populations, 2006 was characterised by a broad range of systematic patterns of protection and human rights violations. Among these was an increase in displacement, particularly in South/Central Somalia. During the last half of 2006, 255,000 people fled their homes due to flooding and over 100,000 are estimated to have fled violence, insecurity, and discrimination. Targeted forced relocation and displacement have also been reported in several areas, particularly due to religious or clan affiliations. In addition, a significant increase in the number of people being smuggled from the northern coastline of Bossaso has been noted. In 2006, 14,151 Somalis and 11,727 Ethiopians were smuggled to Yemen, and Somalis have continued in 2007 to attempt the very dangerous journey, with dozens already having lost their lives this year. An additional 34,000 Somalis crossed the border into Kenya during 2006.
Protection monitoring reports showed that the build-up of the TFG-ICU conflict resulted in the degradation of an already tense situation, with reports of arbitrary arrests, detentions, and expulsions, as well as alleged cases of beating, torture, and murder. When full-scale conflict broke out, daily reports of protection and human rights violations highlighted the indiscriminate effects on the civilian population, with IDP settlements hit by mortars and civilians killed in the crossfire. Not least affected were UNHCR persons of concern – the Ethiopian Oromos – at the hands of Ethiopian forces. Even with the cessation of major hostilities in early 2007, ongoing battles continue to affect the civilian population; during the month of February, an estimated 40,000 people left Mogadishu due to insecurity and violence.
While displaced populations are among the most vulnerable targets of protection violations, other populations are subject to multiple violations. Women and girls, especially within minority communities, continue to be victims of SGBV. Reports of rape are high in IDP camps, with more than a third of cases reported against children under the age of sixteen. In addition, there has been widespread use of child soldiers by all parties involved in conflicts. Minorities are particularly vulnerable to violations due to a lack of clan protection. These include denial of access to basic services, violence, and harassment. Evictions from public buildings have become an increasing concern. Also of grave concern has been the Kenyan Government’s decision to close its borders with Somalia in early January 2007. The order violates the right of individuals to seek asylum and has left thousands stranded in the border area, unable or unwilling to return to their places of origin, either due to insecurity or because their homes were destroyed by flooding.
The protection response planned for 2007 will build on inter-agency initiatives from the previous years, focusing on proactively responding to systematic patterns of protection violations. This will include a strengthened focus on developing national protection capacity, as well as collaborative advocacy actions, rights-based programming, and developing national preventative mechanisms. Focus will remain on the most vulnerable, including displaced populations, vulnerable women, minorities, and children. The humanitarian community will continue to work within the framework of the IDP strategy as well as within other common frameworks (e.g., the Comprehensive Plan of Action [CPA]), the inter-agency advocacy strategy, joint action plans on SGBV in development), ensuring a collaborative response to addressing protection actions. The cluster will concentrate on building upon synergies, enhancing existing monitoring/reporting systems, promoting mechanisms for prevention, and strengthening advocacy efforts.
PartnershipsDRC, International Organization for Migration (IOM), Islamic Relief (IR), Norwegian Refugee Council (NRC), OXFAM-NOVIB, OCHA, Joint United Nations Programme on HIV/AIDS (UNAIDS), UNDP, UNESCO, United Nations Population Fund (UNFPA), UNHCR, UNICEF and United Nations Development Fund for Women (UNIFEM), Somali Human Rights NGOs and networks.
Objectives Strengthen the prevention of and response to violations of human rights and humanitarian law, at
local and national levels, particularly for displaced populations, women, minorities, and children. Improve the mainstreaming of human rights, humanitarian law and protection within de jure and
de facto Somali governance structures for the practical development and application of protection policies and frameworks, incorporating Early Recovery concepts and criteria.
23

SOMALIA – REVISION
Advocate for the responsibility, accountability and action of local and regional authorities and CBOs, as well as the displaced and other vulnerable communities with regard to human rights and humanitarian law, building their capacity for an improved protective environment, particularly in South/Central Somalia.
Promote a rights-based programming approach and protection focus within the objectives and indicators of all clusters, with respect to the most vulnerable in Somalia.
Indicators Protection Working groups in the three zones support community-driven protection responses:
south and central regions – Mogadishu, Beletweyne and Wajid, Northwest Somalia (Hargeisa, Burao), Northeast Somalia (Bossaso and Galkayo).
Greater awareness of SGBV issues and other protection concerns, through advocacy and community mobilisation in IDP settings in the areas mentioned above.
Technical advice provided to ensure that IDP policies and SGBV policies affecting IDPs and other vulnerable populations adhere to Human Rights law and the Guiding Principles.
The IASC Advocacy Strategy is applied in all of the priority IDP locations, and with regard to other priority vulnerable groups (eg, vulnerable women and children, minority groups), with specific campaigns developed, implemented, and monitored.
Capacity building programmes focusing on increasing national capacity to intervene and prevent protection violations; gender and protection checklists developed for each cluster ensuring human rights based programming and the application of ‘do no harm’ principles.
Monitoring All objectives, indicators and activities are interlinked and work to support national and local systems and mechanisms needed to accomplish the overall goal: to improve the protection environment in Somalia, particularly for the most vulnerable. As such, through the reinforcement of the existing coordination mechanisms, the specific activities undertaken through joint implementation and/or programming will be closely monitored. Special attention will be paid to the mainstreaming of gender issues in all aspects of humanitarian and development work, including strategically targeted assistance to women and girls in their search for equality. With regard to SGBV, solutions must be found which utilise protection tools and rights-based approaches.
International Help Required to Stop People-Smuggling from Somalia Across the Gulf of Aden
Deer, a Somali girl of about 10, lies on a striped plastic sheet on the ground inside a large tent, staring blankly ahead and barely registering the many people gathered around her.
In shock and dehydrated, she's just been rescued – along with about 125 others – after eight days adrift in the Gulf of Aden in a tiny fishing boat. The desperate journey to what they hoped would be a land of better opportunities has brought them right back to the northeastern Somalia coast.
Most of them, anyway. After a week at sea with no food and water, under an unrelenting sun, people on the overcrowded open boat began to go mad, survivors say. Deer's uncle, with whom she was travelling, handed her over to a woman on the boat and threw himself into the sea, vowing to swim to shore – perhaps days away – for help. He hasn't been seen since and is presumed to be one of the hundreds who drown every year on this perilous voyage to Yemen.
"It's not true, he's just in the hospital," protests Deer, briefly rousing herself.
"That's what we're letting her think," another survivor, an older woman, says quietly, turning away so as not to upset Deer.
Bossaso is not only the chief commercial port of Puntland, a self-declared autonomous area in north-east Somalia, but also one of the world's busiest smuggling hubs. Guns, cigarettes and drugs come in; people go out. For at least three years, thousands of Somalis, and increasingly, Ethiopians, have set off from the coastline in tiny open fishing boats hoping to reach Yemen. From there many hope to move on to work illegally in Saudi Arabia, which looms large in the local imagination as a land of riches. (Once in Yemen, some Somalis register with UNHCR as refugees, but many more are economic migrants.) All too often the boats capsize. Even if they make the trip successfully, smugglers often beat the passengers to force them to jump overboard as they near the coast, even though few can swim. The passengers, mostly young men and women between the ages of 15 and 30, often include children as well.
Source: UNHCR Somalia
24
SOMALIA – REVISION
Implications If the Response Plan is Not ImplementedIf implementation is lacking, human rights violations and protection needs will go unreported or unaddressed. With regard to access and advocacy, organisations and agencies will face increased difficulty in designing effective prevention and response mechanisms, and local and regional authorities will pay minimal attention to international instruments and standards. Further deterioration of the material, physical, and legal safety of vulnerable individuals and groups will occur, in addition to lack of progress on sustainable reintegration of returnees, IDPs and other affected groups.
3.4 SHELTER FOR IDPS – CLUSTER LEAD: UNHCRAnalysis of Needs Some 400,000 Somalia’s IDPs live together with other vulnerable communities such as urban poor, returnees, migrants, and others, in the same undignified living space of IDP settlements. The conditions in these settlements are appalling; people live in makeshift structures with no sanitary facilities and a level of congestion that creates security risks and health hazards. The combination of congestion, high temperatures and strong seasonal winds increases the risk of fires; fires have broken out in various IDP locations in the last few years, causing deaths and leaving many people homeless again. Lack of access to land during displacement coupled with constant threat of eviction, causes additional insecurity among IDPs in settlements and public buildings in all parts of Somalia.
In the medium to long term, the authorities must be encouraged and assisted to enact and enforce certain norms regarding the layout of IDP settlements and the obligations of land-owners on provision of basic services. The international community in Somalia is setting up a shelter action programme in selected locations targeting a limited number of beneficiaries; this will eventually be replicated on a larger scale depending on access and collaboration with authorities, land-owners and IDPs. The actions aimed at medium- to long-term solutions will target major urban centres in the north, i.e. Bossaso, Garowe, Gardo, Hargeisa, Burao, and, depending on security and access, Merka and Mogadishu. Particular attention will be paid to any evictions of IDPs from their current locations, while response to new displacement and emergency needs will be undertaken as required. The proposed actions must be in line with future urban planning which will make it possible for IDPs to be integrated in the growing urban centres of Somalia, either in their current locations or in their original places of abode. At the same time, populations facing new displacement as a consequence of flooding and other natural disasters as well as conflict require quick shelter and non-food item relief actions.
On conceptual basis, the shelter actions are divided into four stages: Emergency shelter assistance/actions in case of new displacements, including contingency
planning and stocks; Improvement of current living conditions in the current IDP settlements, including provision of
temporary shelter mobile units that can be relocated to eventual new, permanent locations; Relocation to permanent shelter sites. Development of new sites under the cluster framework.
Land tenure issues to be addressed; Development of permanent shelter solutions for IDPs, incl. construction of permanent shelter.
PartnershipsDRC, NRC, UNICEF, UNHCR, UNHABITAT, UNDP, and a number of national NGO partners.
The proposed actions are in line with the Joint IDP Strategy, as well as other common approaches (i.e. the CPA, Humanitarian Charter and Minimum Standards in Disaster Response [SPHERE] standards, etc.) and will link with other longer-term processes (i.e. RDP) that focus on the consolidation of peace in Somalia. They are based on a human rights-based approach to programming and on selection criteria that have been set according to the vulnerability of beneficiaries, and in line with the principles of the humanitarian law, and are thus intrinsically linked to the protection work of the international community in Somalia.
Objectives To meet immediate shelter needs of newly displaced through provision of non-food items and
emergency shelter supplies. To develop and implement temporary shelter solutions for the long term displaced in their current
locations.
25
SOMALIA – REVISION
To identify durable living space solutions and secure land tenure for the displaced in their current locations and/or in their original places of abode.
To assist the displaced to construct their permanent shelter in identified locations of permanent settlement.
Indicators Shelter needs of the newly displaced populations as identified through rapid emergency
assessments and population tracking are met; number of non-food items and shelter supplies distributed.
Acceptable temporary shelter solution provided to 25% of those identified in need of shelter assistance by IDP profiling. The quality of living conditions measured against SPHERE standards for those with security of tenure.
Number of households with security of tenure and durable living space. Quality of living conditions measured against SPHERE standards for those with security of tenure.
Number of vulnerable households receiving permanent shelter; percentage of vulnerable households in selected locations receiving shelter assistance.
MonitoringThe objectives for all the planned actions are quantifiable and the achievements will be measured as part of the progress monitoring. Moreover, the SPHERE standards will be applied throughout as a planning benchmark, i.e. in the design of shelter and the sites, in terms of density of dwellings, number of beneficiaries per shelter unit, number of beneficiaries who rely on available basic services, etc. All actions are underpinned by efforts to support national and local systems and mechanisms needed to dramatically improve the shelter situation in Somalia and especially in the urban centres.
Through the reinforcement of the existing coordination mechanisms, the specific activities undertaken through joint implementation and/or programming will be implemented and closely monitored. Special efforts must and will be paid to the mainstreaming of gender issues in all aspects of humanitarian and development work, including strategically targeted assistance to women and girls.
Implications If the Response Plan is Not implementedIf the response plan is not implemented, newly displaced populations will face the risk of increased morbidity and mortality due to the effects of exposure and poor household hygiene conditions. The living conditions in most of the IDP settlements are set to deteriorate, given the prospects of new displacement within the country that traditionally leads to further overcrowding in existing settlements and the overstretching of meagre basic services. Such conditions compound ongoing human rights violations in the settlements, especially those of women and children. Subsequently, the newly displaced, if not in receipt of assistance within the country’s borders, will likely seek assistance across the border, exacerbating the refugee problem in the region. Related to access and advocacy, organisations and agencies will face increased difficulty in designing effective prevention and response mechanisms, and there will be minimal attention given to adhering to international instruments and standards by the local and regional authorities.
3.5 HEALTH – CLUSTER LEAD: WHOAnalysis of Priority Needs Access to and quality of health care in Somalia remains inequitable, with inadequate distribution of services and human and financial resources in areas where vulnerable populations reside, such as IDP camps and rural areas. Infant/child mortality rates in Somalia are among the highest in the world at 96 and 156 per 1,000 live births, respectively, and Somalia has an estimated maternal mortality rate of 1,013 per 100,000 live births.13
Despite an emphasis on primary health care, many health care programmes still are managed in a project-dependent vertical or top-down fashion. There are only 39 qualified doctors per one million inhabitants, unequally distributed throughout the country and concentrated in cities. That there are as few as 141 well-qualified midwives contributes to the very high rates of overall infant and under-five mortality rates. There is a need to increase access to basic health care by increasing the number of functional health facilities to ensure the coverage of health needs of vulnerable populations in
13 UNICEF Preliminary results of the 2006 Multiple Indicator Cluster Survey (MICS).
26
SOMALIA – REVISION
underserved areas. Rehabilitating/rebuilding the Somali health system would reduce the high levels of mortality and morbidity, especially among women and children.
Access to basic services is very poor and cumulative indicators reveal an alarming picture: only 30% of the population has access to safe drinking water, 45% has access to local health care, and 50% have access to adequate excreta disposal facilities. For IDPs and returnees, indicators for access to basic services are lower than for the average Somali. Routine immunisation coverage for measles and Diphtheria/Pertussis/Tetanus (DPT3) vaccine is 28% and 27% respectively. However, since November 2005, the first measles catch-up mass-vaccination campaign in 13 years was undertaken with great success for children aged 9 months to 12 years.
The recent outbreak of polio in Somalia, after nearly three years of being polio-free, underscores the gravity of the health situation. The risk of polio spreading to the rest of the Horn of Africa highlights the need to respond adequately to the ongoing outbreak, and such response is an important strategic component of this response plan. Although cholera outbreaks have been prevented since 2004, systematic prevention measures should continue in 2007. Moreover, bloody diarrhoea, meningitis, malaria and other outbreak-prone diseases require continuous attention. In South/Central Somalia, for instance, there has been an increase in AWD cases following the flooding of late 2006. Preparedness against Avian and pandemic influenza also requires scaling up in 2007.
Among the major causes of pregnancy-related death at childbirth are complications such as haemorrhage, prolonged labour, obstructed labour, infections, and eclampsia. Women who survive, live in misery with chronic anaemia, chronic infections, and fistulas. Contributing to the high rates of maternal mortality and disability are: poor antenatal, delivery and postnatal care; female genital mutilation, and the complete lack of emergency medical obstetric referral care. Furthermore, about 80% of childbirth takes place at home, with the help of family members and attendants who have limited delivery skills.
Mental health services in Somalia are at present limited to four in-patient facilities in Berbera, Bossaso, Hargeisa and Mogadishu. These are, for all practical purposes, custodial and asylum facilities. Due to ongoing conflict, mental health problems are becoming increasingly prominent as a major cause of ill health. However, mental health is not considered a priority in the general health system and most mental health services are provided by NGO-run health institutions with limited coverage capacity and low quality of care.
The overall sector objective is to reduce excess mortality and morbidity of the Somali people with particular attention to the vulnerable populations noted in the CHAP. The response plan will focus on providing appropriate and adequate emergency assistance to mitigate the effects of the humanitarian crisis on the most vulnerable groups through an established, decentralised field response. The agencies involved in the sector will work through multidisciplinary teams with international and local partners to identify, implement, and monitor rapid response to the most affected. Humanitarian partners have agreed to propose and implement coordinated initiatives that target humanitarian, emergency and early recovery needs of the most vulnerable in order to maximise available resources under the CAP, leaving the medium- to long-term recovery and development needs to be met by other funding streams.
Objectives Increase access to quality essential health services for vulnerable populations, with special focus
on IDPs, women, and children. Increase coverage of Expanded Programme of Immunisation (EPI) and Vitamin A distribution. Increase availability and utilisation of quality reproductive health services including Emergency
Obstetric Care (EmOC) and family planning. Build capacity of service providers at all levels. Strengthen integration and capacity of existing surveillance systems and health information
system at all levels. Strengthen epidemic preparedness, including for avian and pandemic influenza. Strengthen coordination of health activities and stakeholders at all levels with special emphasis
on emergency preparedness, humanitarian response, gap filling, early recovery and capacity building.
Increase availability of mental health services to communities.
27
SOMALIA – REVISION
PartnershipsThe cluster approach has been rolled out in Somalia in 2006. WHO is the lead agency for the health cluster. Since the initial roll-out, the partner agencies of the health cluster have met many times in Nairobi. Partners are WHO, UNICEF, UNFPA, WFP, OCHA, FSAU/FAO, Gedo Health Consortium (GHC), Health Sectoral Committee (HSC)/SACB, International Federation of Red Cross and Red Crescent Societies (IFRC), International Medical Corps (IMC), Comitato Internazionale per lo Sviluppo dei Popoli (CISP), International Somalia Rehabilitation Association (ISRA), SC-UK, Medical Emergency Relief International (MERLIN), Médecins Sans Frontières (MSF)-Switzerland, MSF-Holland, United States Agency for International Development (USAID)/Office of U.S. Foreign Disaster Assistance (OFDA), WVI, Action Contre la Faim (ACF), InterSOS, COOPI, CARE, COSV, Muslim Aid-UK, African Muslim Agency and Humedica (a German NGO). Main issues addressed include activities being carried out by the health sector partners in response to the drought, Mogadishu contingency planning, response to outbreaks of Rift Valley Fever and planning/response to flood and conflict in South/Central Somalia. At field level, six meetings have been held in Wajid, Bakool region to define and implement the strengthening of the emergency response to drought and formulate appropriate policies in collaboration with Ministry of Health (MoH) and UN agencies.
The main action pillars of the national health cluster are: monitoring health trends, activities and outcomes, joint decisions and follow-up, developing operational and contingency plans, collection, preparation and dissemination of health information, resource mapping (Who What Where [3W]), needs/gap analysis, advocacy, resource mobilisation and inter-cluster linkages.
In the field (provincial and district level) the action pillars are: supporting local authorities, coordination and joint planning with stakeholders, assessment and quantification of needs, preparedness planning, resource mapping (3W), regular coverage/gap analysis, joint decisions and follow-up, collecting, analysis and reporting health-related information and activities, and other inter-cluster linkages at regional level.
Indicators Percentage of the population with access to health facilities. Number of health facilities/health partners providing outreach services for IDPs. EPI coverage (%) and percentage of children under one fully immunised. Number of women in child-bearing age visiting basic reproductive health services. Number of mother and child health (MCH) and hospitals providing basic EmOC. Number of facilities rehabilitated/reconstructed. Number of functional laboratories. Percentage of facilities submitting timely and complete reports. Number of health facilities providing mental health services. Percentage of regions with an emergency preparedness plan. Number of trainings on emergency preparedness and response delivered in the regions.
Activities Strengthen and decentralise health cluster coordination to regions and at field level to improve
service delivery, implementation, and monitoring. Rehabilitation/reconstruction of health facilities. Ensure optimal functioning of existing and new health facilities and increase outreach service
delivery activities. Immunise all children in the identified most vulnerable target groups against measles and polio. Ensure all women in the identified most vulnerable groups have access to quality reproductive
care services (EmOC) and family planning. Integrate HIV/AIDS and Sexually Transmitted Infections (STIs) services to health facilities. Training of service providers in, among others, case management of major diseases (e.g.
malaria, acute respiratory infections, bloody diarrhoea, cholera, measles, under nutrition, etc.), laboratory diagnosis, and EmOC.
Improve the data collection and reporting system at various levels and distribution of timely surveillance and other reports to all stakeholders.
Decentralise health cluster response to regional level and establish health cluster focal agencies in each region.
Prepare disaster and outbreak preparedness and response plans at regional level, including for avian and pandemic influenza, and implement them as per need and identified risks.
Ensure adequate pre-positioning of needed supplies and equipment.
28
SOMALIA – REVISION
Promote health education and awareness-raising on major health issues including environmental sanitation and hygiene practices, nutrition & diet, reproductive health & family planning, mental health, HIV/AIDS, malaria, tuberculosis, zoonotic and outbreak prone diseases.
Provide laboratory diagnostic facilities in under served and IDP concentrated areas.
MonitoringOrganisations will continue to deliver assistance in their areas of respective strength and cooperate with all health partners concerned to provide optimum results for the Somali people. Health cluster coordination at central and regional levels will monitor and follow up on these activities in order to prevent duplication and ensure rational utilisation of resources. It is essential that all partners continue to provide and exchange information and report and update on their project activities. Coordination among all partners will be decentralised to regions and strengthened at field level to improve the monitoring of planned activities.
Implications If This Response Plan is Not ImplementedIf this plan is not implemented, outbreaks of polio, cholera, and other diseases may occur, significantly increasing the disease burden from infectious and communicable diseases. The spread of the wild polio virus is a major threat for neighbouring countries and to the global goal of eradicating polio. Mortality, as an indicator of severity of crises and complex emergency, will continue to surpass the unacceptable threshold of overall Crude Mortality Rate (CMR) of 1/10,000/day and an under-five mortality rate 2/10,000/day, due to communicable diseases and malnutrition. Similarly, limited access to safe water and sanitation facilities will continue to exacerbate the existing poor health and nutritional situation. Lack of interlinked water, health, nutrition, and sanitation services/facilities will hamper IDP and refugee return, as the absorption capacity will be insufficient. Already, IDPs are perceived as a burden by host communities in many areas, and large-scale refugee returns may over-stretch the hospitality of the local communities further, leading to conflict rather than to reconciliation and peace-building.
3.6 NUTRITION – CLUSTER LEAD: UNICEF
Analysis of NeedsThe nutrition situation in most parts of South and Central Somalia is of great concern, with acute malnutrition levels of 10% and above being recorded over the last seven years. The worst drought in a decade further depressed nutrition levels. A strong emergency response in 2006 saved lives and alleviated immediate suffering among vulnerable populations in the affected areas. However, the nutrition response has not totally relieved the population of the risks of malnutrition. There were programme setbacks linked to increased insecurity and floods in the last quarter of 2006, delaying and/or interrupting some of the post-drought nutrition response. Population displacement occurred, with accompanying risk factors to the population’s nutritional well-being – compromised child-care, exposure to extreme weather conditions, poor sanitation and associated diseases, etc. These shocks and the resultant programmatic setbacks have led to persistence of an unacceptable prevalence in acute malnutrition levels of 15% and above across much of South/Central Somalia (See Map: Nutrition Situation Jan 2007).
Multiple aggravating factors prevail, including increased disease incidence, poor household dietary diversity, poor maternal and childcare practices, inadequate health services and poor hygienic conditions. There is also notable convergence between critical malnutrition prevalence and high insecurity that limits humanitarian access in south and central regions of Somalia. Marginalised groups and IDP populations present unacceptably high malnutrition levels, e.g., global acute malnutrition rates of over 15% in Bossaso IDPs. Based on the estimated population and the acute malnutrition prevalence, it is believed that over 50,000 children are malnourished and at risk of death in South/Central Somalia.
The nutrition cluster will continue to build on the ongoing emergency response, which commenced in mid-2006 at the height of the drought.
Children share porridge at Ufurow feeding centre in Qansadhere, Bay Region (IMC SFP). Source IMC
29
SOMALIA – REVISION
Efforts will be supported towards both reducing excess preventable mortality associated with malnutrition and promoting improved nutrition in Somalia. Particular attention will be paid to the most vulnerable populations and to inaccessible areas with limited humanitarian coverage. An integrated approach (multi-sector public nutrition programming) to the nutrition crisis will continue to be adopted, with initiatives in both short-term life-saving strategies and medium-term strategies. Early recovery activities such as micronutrient intake promotion and supplementation, nutrition education, growth monitoring and promotion remain cores of this response strategy. This approach will provide appropriate and adequate emergency response through a coordinated yet decentralised field response that harnesses each cluster member’s strengths in the context of prevailing insecurity. Rigorous monitoring of the nutrition situation and the impact of the response will be undertaken.
ObjectivesThe overall Nutrition Cluster objective is to avert excess mortality due to malnutrition and to promote better nutrition among the population in the affected areas.
Specific Objectives Support intensive selective feeding programmes (ongoing and planned) to improve coverage of
the emergency nutrition activities of detecting and rehabilitating severely and moderately malnourished children.
Strengthen technical capacity for local NGOs/CBOs and national staff on emergency and long- term strategies of addressing malnutrition.
Foster linkages of the selective feeding response with medium-term programmes addressing the underlying causes of malnutrition (including maternal and child care practices, food security and livelihood promotion, water and sanitation).
Strengthen and expand the regular public health and nutrition programmes through expansion of the Primary Health Care (PHC) programmes and improvement of the quality of services in the existing PHC programmes in South and Central Somalia.
PartnershipsWVI, IMC, MSF-Belgium, MSF-Holland, MSF-Switzerland, GHC, Muslim Aid, Somali Red Crescent Society (SRCS), SC-UK, ACF, Adventist Development and Relief (ADRA), World Concern International (WCI), Deeg-Roor Medical Organisation (DMO), African Muslim Agency (AMA), Somalia Aid Foundation (SAF), AFREC, Child Aid Somalia (CAS), COSV; INTERSOS, Green Hope, WHO, UNICEF, WFP, FAO/FSAU and Handicap International (HI).
The agencies will work through the cluster to implement the nutrition response in a coordinated manner, thereby enhancing both effective resource utilisation and impact. Different programmes with potential for complementarities will target common beneficiaries and agencies will explore innovative and alternative approaches to complement their current planned or ongoing activities.
IndicatorsSome of the key indicators of performance include: The prevalence of acute malnutrition rates and crude and under five child mortality rates; Number of previously malnourished children cured in the selective feeding programmes by region
(coverage analysis including admissions trends and specific selective feeding programme performance indicators based on Sphere Guidelines recommendations);
Number of additional programmes established within health and nutrition facilities that address underlying causes of malnutrition, e.g. kitchen garden demonstrations, water points, hygiene promotion, locally available food preservation and preparation demonstration centres, etc.;
Number of additional national NGOs trained and involved in the management of acute malnutrition in south and central regions;
Percentage coverage of (multiple) micronutrient supplementation through routine, accelerated campaign and through expanded selective feeding programmes;
Number of health and nutrition workers from supporting and implementing agencies trained on maternal and child feeding/nutrition response in emergencies.
Activities Technical support and capacity improvement of the selective feeding implementing agencies
(training and supportive supervision). Support the current routine and emergency nutrition response activities and advocate for
integration of complementary programmes including food security and livelihood promotion projects, comprehensive public health services, water, and sanitation.
30
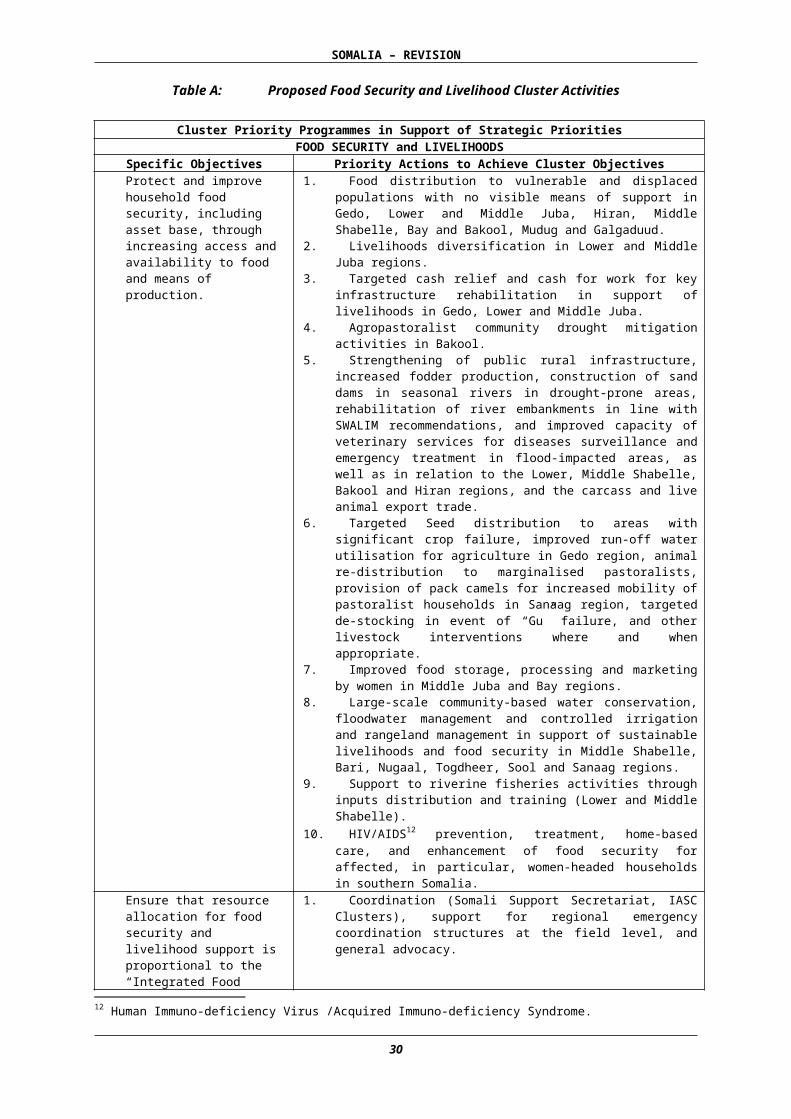
SOMALIA – REVISION
Emergency nutrition supply procurement and delivery to affected regions and support to the warehousing facilities for buffer stock.
Promote dietary diversity in all seasons through improved awareness on storage/preservation methods of locally available foods and promote appropriate feeding habits (including breastfeeding and complementary feeding).
Identify and support Community Based Organisations (CBOs) and Somali nationals with potential to improve nutrition response coverage in both accessible and inaccessible areas.
Improve intra-cluster coordination and inter-sectoral programme coordination to enhance field level information sharing, programme complementarities and resource utilisation.
Monitoring Through periodic assessment, the nutrition situation will be closely monitored and influencing factors documented for appropriate action. Programme performance feedback will be given to relevant stakeholders through sharing of monthly project reports and discussions facilitated in the regular monthly nutrition cluster/nutrition working group meetings. The database of the nutrition reports will be improved. Critical assessment/analysis of the overall emergency nutrition response and the integration with the complementary programmes will be done jointly by the implementing and supporting agencies on a quarterly basis to enhance quality and coverage of programmes.
Implications If the Response Plan is Not implemented Nutrition is a late indicator and failure or delay in response plan implementation increases risk of death and/or permanent impairment of many children currently at risk. Chronic malnutrition is likely to be more prevalent. The cycle of malnourished children becoming malnourished adults who later produce malnourished children presents a risk of a future population in south and central Somalia that will never achieve its full physical and mental potential. Rectifying such problems and avoiding death and/or impairment will be less expensive than correcting an impaired population in the future.
3.7 WATER AND SANITATION – CLUSTER LEAD: UNICEFAnalysis of Needs Access to safe water was approximately 29.3% and safe means of excreta disposal 37.3% in south and central Somalia in 2006. For IDPs and returnees, indicators for access to basic services are lower than for the Somali population generally, as the former often do not receive support from family/clan members and their access to services is often impeded by discrimination. Inadequate water services and lack of sanitation throughout Somalia has resulted in high levels of mortality among children and adults in IDP camps and other vulnerable communities. Cholera is endemic and the cholera season requires intensification of cholera prevention and control activities. The high prevalence of water-related diseases is compounded by both the lack of water available and poor hygiene practices. Competition and conflict around scarce water supply sources persists, and improving access to water will remain a major factor in averting impending disaster.
The current water, sanitation, and hygiene (WASH) flood response reached 58% of the flood-affected population. However, with the regular conflict in southern Somalia, improving access to safe water and sanitation remains a priority area of emergency response activities. In addition, vulnerable IDPs in Mogadishu, Galkayo and the major towns in southern Somalia require critical support. Key areas where water and environmental sanitation need to be addressed are Mogadishu, Gedo and the Juba regions.
The WASH cluster plans to increase water supply through diversification of water supply systems, locally suitable sanitation options, and hygiene promotion activities. An integrated approach will be utilised to combine short-term life-saving strategies with medium-term recovery strategies that support sustainable water supply and sanitation initiatives to generate wider improvements in livelihood security. A major focus will be on strengthening the capacity of local civil society partners to ensure effective coverage of areas to which there is limited access. The cross cutting issue of gender will be addressed through the involvement of both women and men in the selection of the location, design and maintenance of water and sanitation facilities in the response activities.
ObjectivesThe overall WASH objective is to contribute to the well-being of affected populations by reducing the transmission of diseases through promotion of good hygiene practices, providing safe drinking water and reducing health risks related to poor sanitation.
31
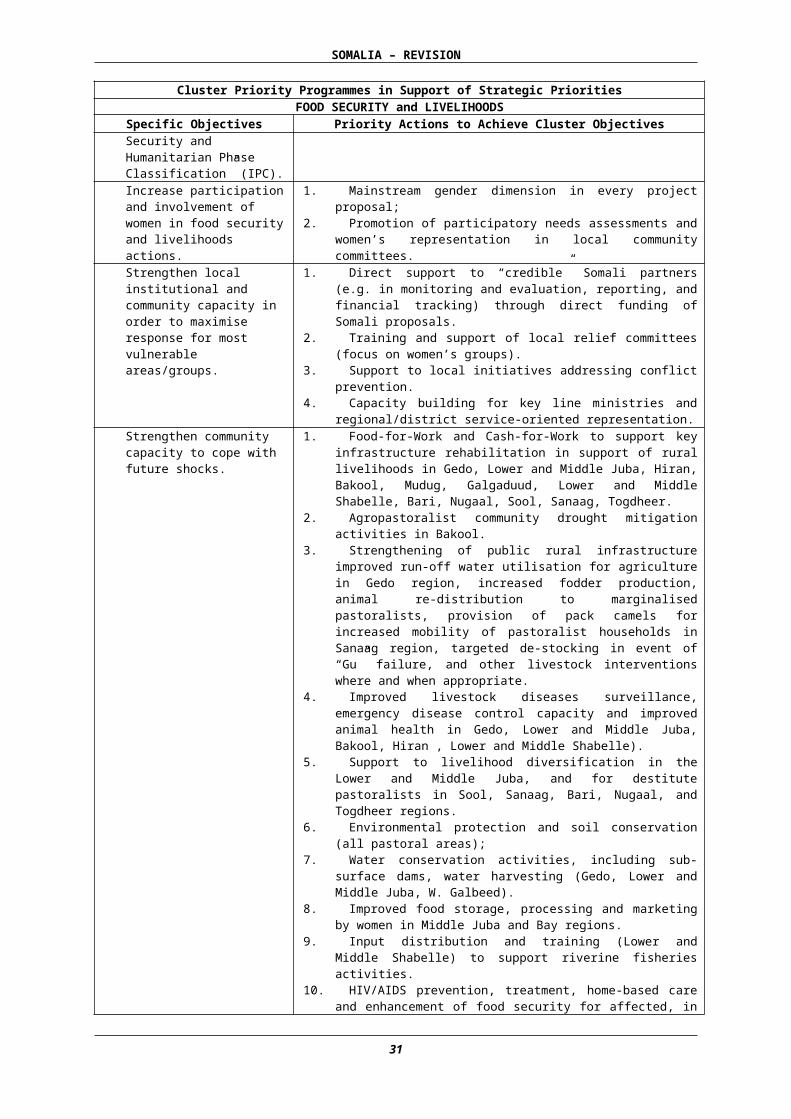
SOMALIA – REVISION
The specific objectives are:1. Increase access to sustainable water and environmental sanitation services for a million people, in
particular women and children, identified as in need of emergency assistance;2. Strengthen local capacity for provision of safe drinking water and environmental sanitation
services to 400,000 people, especially women and children, in vulnerable situations (particularly IDPs).
PartnershipsWVI, COOPI, Norwegian Church Aid (NCA), CARE, OXFAM-GB, Concern Worldwide, WCI, Solidarités, IR, Horn Relief, COSV/JCC, ASEP, ADRA, INTERSOS, WHO, NRC UNICEF, among others. International partners are expected to work in close collaboration with local NGOs to ensure coverage.
Key indicatorsKey indicators of performance include: Percentage of people with improved access to safe water sources (one million people in need of
emergency assistance and 400,000 people in vulnerable situations); Number of people having access to and utilising sanitation facilities (350,000 people); Percentage of people directly reached by hygiene awareness campaigns (700,000 people).
Activities Strengthen the local capacity of civil society partners and community in social mobilisation on
hygiene, environmental sanitation, and WASH management. Improve the capacity of local civil society, partners, and the community in operational
maintenance of water supply systems. Increase safe water supply and diversify water supply systems. Increase improved sanitation options. Provide water-trucking services when no other solutions are available. Chlorinate water points in cholera prone areas, post-action evaluation and expand water quality
monitoring mechanism. Increase WASH cluster coordination and regular monitoring through updating contingency plans,
organising frequent coordination meetings and ensuring adequate pre-positioning of supplies in strategic locations.
Monitoring Partner assessment and monitoring reports will be regularly shared through the monthly WASH cluster meetings both in Nairobi and in the field. Through regular monitoring, needs will be identified and response mobilised to link water and sanitation interventions to schools, health and feeding centres to ensure improved quality and coverage of programme implementation.
Implications If This Response Plan is Not Implemented If this plan is not implemented, the mortality rate, as an indicator of severity of crises and complex emergency, will continue to surpass the unacceptable threshold of overall CMR of 1/10,000/day and an under-five mortality rate 2/10,000/day. In addition limited access to safe water and sanitation facilities will continue to exacerbate the existing health and malnutrition calamities.
3.8 EDUCATION – CLUSTER LEAD: UNICEFAnalysis of NeedsThe humanitarian situation in south and central regions remains uncertain due to the effects of localised conflicts and recurrent natural disasters (such as droughts and floods). This poses a serious threat to the already fragile situation of the education sector that is chronically under-resourced.
Despite an increase in access to primary education across Somalia (28%), approximately 40% of schools in the drought-affected areas (Bay, Bakool, Gedo, Lower/Middle Juba) were closed down. With limited educational opportunities and a lawless environment, the risk of children joining militias is elevated. Through increasing access to educational opportunities and promoting life skills based education for out-of-school youth, education can be considered both life-saving and life-sustaining.
32
SOMALIA – REVISION
The main targets of emergency education programmes are the marginalised and vulnerable groups in southern and central Somalia and the displaced population in the northeast, and west. Due to the imposing threat of conflict, and the likelihood of natural disasters, it is essential that the capacity of local communities and authorities be strengthened for emergency education preparedness.
Objectives To increase sustainable access to quality education amongst vulnerable groups, children and
youth in emergencies. To retain children and youth in formal and non-formal education during emergencies and
disseminate key survival messages through educational programmes. To create awareness and build the capacity on emergency preparedness at all levels (Ministry of
Education [MoE], Regional Education Officers [REOs], District Education Boards [DEBs], Community Education Committees [CECs] and teachers).
Activities
Support the establishment of child-friendly and secure learning spaces for vulnerable groupsThis activity is aimed at providing learning spaces to the target population. Where possible, Somali authorities will be involved in the response. Two different strategies for displaced pupils are foreseen:a) Integration: innovative strategies will be developed to ensure displaced children can be
integrated into the existing educational facilities of the host communities;b) Return: Where integration policies for displaced children are not feasible or return is
anticipated, tented learning spaces and educational materials shall be provided.
This activity is consistent with Strategic Priority 1: Increase access to basic education services for an estimated 157,607 long-term displaced people (UNHCR IDP Profiling in Lower Shabelle, Bossaso, Hargeisa, Berbera and Burao and about 300,000 new displaced in Central Southern Somalia (UNHCR new displacement map at 31 July 2006).
Support of School Fees for Marginalised Groups or Teachers’ IncentivesThis activity will support access to education for marginalised and vulnerable groups and retain teachers in school during emergency situations in the IDP emergency affected zones of Central South, North East and North West zones of Somalia. Teacher incentives will be targeted at female teachers to increase the number of role models for girls. Awareness and understanding shall be raised to avoid payment to a selected group creating hostility. An exit strategy will be included to ensure programme sustainability in the long-term.
This activity is consistent with Strategic Priority 1: Increase access to basic education services for an estimated 157,607 long-term displaced people in all Somalia and about 300,000 new displaced in Central Southern zones.
33
SOMALIA – REVISION
School Feeding ProgrammeBased on the outcomes of the school feeding component of the drought emergency response in 2006, this activity will be continued on a performance and needs basis. It will be delivered alongside other actions targeting obstacles to enrolment and retention to ensure that quality remains the first priority and that food does not become the key motivation for attending school. Capacity building of the MoE shall contribute to gradual ownership of the programme. School adjustments to include the necessary infrastructure for feeding will be promoted.
This activity is consistent with Strategic Priority 2: Alleviate the suffering and increase access to basic humanitarian services.
Life Skills-Based EducationThis activity includes promotion of peace education, reintegration programmes for former youth militia, and dissemination of key survival messages through multiple educational channels. Innovative strategies such as story-telling and radio education will be used to transmit messages.
This activity is consistent with Strategic Priority 1: Save lives of an estimated 322,000 children in Central Southern zones of Somalia.
Teacher TrainingTeacher training for high priority groups (unqualified, barely trained, IDP teachers) on teaching methodologies and lesson planning in line with the ongoing programmes (e.g. Strengthening Capacity of Teacher Training [SCOTT]); priority will be given to teachers in the IDP camps of Central South, North West and North East zones of Somalia. The number of teachers will be defined by a capacity assessment of the existing displaced teachers.
Strengthening Local and Regional Capacity for an Effective Emergency Response in the Education Sector This activity is consistent with the overall Strategic Priority 4: Strengthen capacity for social service delivery and response to natural or conflict related disasters. Moreover, it contributes to strengthening resilience of Somali authorities to respond in emergency situations. The programme will focus on: Capacity building of the MoE, REOs and DEBs to coordinate the emergency response through:
training in conducting rapid assessments, advocacy, mobilisation and standards (Minimum Standards for Education in Emergencies);
Training in management functions for the MoE, REOs and DEBs to support a rapid response for education in emergencies (this will include Minimum Standards in Education Emergencies [MSEE]);
Support to the CECs to coordinate the local level response to an emergency: training in advocacy and social mobilisation, mobilisation of human and financial resources, management and planning;
Support to the development of the Education Management Information System (EMIS) to ensure information is collected on the number and location of children displaced or affected by emergency; the availability and conditions of school facilities; and the availability of learning materials and teachers.
PartnershipsUNICEF, WFP, UNESCO, UNDP, a Swedish NGO (Diakonia), Water for Life (WFL), Intersos, NCA, NRC, WCI, International Aid Service (IAS), IR, Education Development Centre (EDC), Irish Aid Agency (Trocaire), SC-UK, CISP, COOPI, Centre for British Teachers (CfBt), WVI, Africa Educational Trust (AET), ADRA, COSV, Hisan-Wepa, Candle Africa International and Mogadishu University, CAS.
IndicatorsAccess Indicators: Number of schools with adequate gender sensitive sanitation facilities and water;Number of children and youth (disaggregated by gender) enrolled in educational institutions; Number of teachers employed (by gender); Number of learners and teachers are retained throughout the school year during the emergency.
Quality Indicators: Number of teachers trained (by gender and level); Pupils’ cognitive achievement (measurable through tests and examination documents); Completion ratio (measurable through the annual Primary Education Survey [PES]); Interaction of students and teachers (measurable through
34
SOMALIA – REVISION
school visits); Teaching and learning processes (measurable through school visits); Number of textbooks and instructional materials.
Strengthening Emergency Preparedness indicators: Number of stakeholders and education authorities trained and enabled to address and respond to emergency situations in the education sector; number of gender sensitive emergency preparedness plans developed; number of authorities trained in EMIS.
MonitoringMonitoring mechanisms of the sector response plan will be managed by the Education Sectoral Committee (ESC) of the Somalia Support Secretariat. Implementing agencies will monitor at field level and progress reports will be shared at the monthly educational forum. Data will be disaggregated by gender. Input from Somali authorities, including assessments and monitoring activities, will be coordinated through the SSS and implementing agencies.
Implications If the Plan is Not ImplementedThe sector response plan addresses the basic human right of ensuring educational opportunities to all the children in emergencies in line with the millennium development goals. If the response plan is not implemented displaced and vulnerable children in the south and central regions of Somalia may be denied the right to quality basic education.
35
SOMALIA – REVISION
CROSS-CUTTING SECTORS
3.9 EARLY RECOVERY (CROSS-CUTTING) – CLUSTER LEAD: UNDPAnalysis of NeedsRecognising that humanitarian aid is the first line of action in Somalia, supporting the resilience and coping mechanisms of households and communities under continual threat is critical, as recurrent conflicts and natural disasters jeopardise the capacities of people to protect their families and livelihoods. Early recovery programming is needed to restore services, livelihood opportunities, and governance capacity as well as to reduce vulnerability to future crises. The earlier in the humanitarian phase that planning and work on early recovery begins, the sooner country institutions can move forward in providing basic services and assuming governance functions to stabilise affected areas. In humanitarian assistance programmes the focus is on the needs of individuals, while early recovery programming focuses on their support systems. Emphasis should shift from humanitarian response to early recovery as soon as possible. Recognising the differential impact of conflict and disaster on women and men, boys and girls, early recovery actions will also seek to redress gender inequalities, support spontaneous transformation of gender relationships in the recovery process, and raise the status of women in society.
The Early Recovery pillar of the CAP links to the Joint Needs Assessment and the initial stage of the Reconstruction and Development Programme14 (RDP) by including some of the first-year priorities which are emerging from the RDP, and which can be undertaken in a humanitarian setting.
ObjectivesEarly recovery begins in a humanitarian setting. It is a multi-dimensional process, guided by development principles. It aims to generate self-sustaining, nationally-owned, and resilient processes for post-crisis recovery. The main objectives for the CAP in 2007 are:
Ensure planning that aims both at saving lives and preserving livelihoods by strengthening essential local governance capacities; ensuring broad-based participation in a framework for early recovery; and protecting assets for sustainable livelihoods;
Address underlying causes of vulnerability by strengthening mechanisms for peace-building and reconciliation and by addressing root causes of disasters triggered by natural hazards;
Create a conducive environment for stabilisation of vulnerable communities and the sustainable reintegration of displaced populations by providing early access to social services and economic networks and strengthening the rule of law.
Where access permits, an integrated area-based approach will be implemented to help address the needs of populations affected by the crisis by enabling or reinforcing community capacities. The approach promotes increased security, economic recovery, and social reconciliation at the local level using a human rights-based approach. The area-based approach targets well-defined geographical areas and aims to serve the vulnerable populations within these, while engaging international and local institutions and stakeholders.
PartnershipsAn early recovery coordination network will bring together key partners around requirements for an integrated response and provide a space to elaborate detailed area-based action plans. It will also ensure the joint monitoring of progress, funding allocation, and performance of key partners against commitments.
Early recovery programmes will work with local leaders and civil society, ensuring representation and effective participation of women’s networks through agreed upon mechanisms (e.g. district recovery committees) to define immediate priorities. While one result of the programme is the rehabilitation of infrastructure, and the short-term employment created to build it, the process importantly provides the space for local administration to establish legitimacy and build its own capacity in recovery planning – a space in which dialogue, reconciliation and the initial delivery of peace dividends can take place.
14 Early recovery also links up directly with the UNHCR initiated Comprehensive Plan of Action for Somali Refugees which aims at durable solutions for Somali refugees in the region, through creating in the country of origin conditions conducive for the return and reintegration of Somali refugees and IDPs.
36
SOMALIA – REVISION
The restoration of government functions and responsibilities is critical to consolidate peace in Somalia. Early recovery programming must be driven by, and engage, country partners and institutions in all aspects of programming. Systems of decentralised responsibility and accountability will need to be developed early in the process.
Early recovery stakeholders will help to increase the participation of NGOs and CBOs in planning and decision-making, within an overall local governance framework. Community-driven approaches will strengthen relationships between civil society and local government through partnerships, promoting the joint ownership of resources, and planning by local stakeholders. Deliberate measures to ensure the inclusion of women at all stages of early recovery will contribute to women’s empowerment and to addressing gender inequalities.
It is critical to ensure that flexible funding is made available as soon as new areas open so that critical early recovery activities can be put in place in time to facilitate stabilisation efforts.
Criteria for Early Recovery ActionsThe conditions for implementing an area-based approach in support of Early Recovery are: Access and security have been negotiated with legitimate or de facto authorities; Sustained reduction of armed conflict with initial conditions for peace-building in place, so that
foundations for stabilisation and later development can be laid; Conditions for the emergence of nascent governance structures are present; Need for stabilising or consolidating emerging peace and continuing support to communities and
populations recovering from conflict, and for initiating strategic planning, coordination and capacity-building for rule of law and security;
Stable conditions for development have not yet emerged but planning for development is possible.
Project Selection ProcessA project validated under the pillar of Early Recovery meets all or most of the following criteria: Phasing out relief or addressing the next step after saving lives; Activities address underlying causes of crisis or disaster (drought, floods, other disasters
triggered by natural hazards or conflict); Immediate or basic capacities of communities to build beyond crisis strengthened; Potential or existing capacities of local authorities to plan, manage, and coordinate actions to
deal with crises as well as for subsequent recovery phase strengthened; Action undertaken with sustainability in mind; particularly inclusive of communities in shaping
and implementing the action and thus building capacity; Action will be planned and coordinated through an area-based framework; Mainstreams peace-building and reconciliation activities; Mainstreams gender and human rights based approaches and integrates protection activities; Not longer term recovery/reconstruction/development in nature; Not emergency/relief in nature.
ActivitiesEarly Recovery activities will largely be concentrated in areas of south/central Somalia as access permits. The 2007 CAP includes Early Recovery activities in each of the Clusters within respective response plans; the build-up of country capacities for transition and recovery; support to the early stages of governance, peace building and conflict prevention; community-driven social and economic recovery; small scale recovery infrastructure; the management of disaster risk triggered by natural hazards and coordination of Early Recovery. Consequently, the following main activities will be undertaken: Protection of productive assets in support of food security, and strengthening of community
capacities (e.g., through livelihood diversification) to cope with future shocks; Capacities and mechanisms for sustainable social service delivery, notably water and sanitation,
education, and essential health services in early recovery areas; Support to nascent governance structures, in particular district-level local authorities’ coordination
and advocacy of early recovery, with emphasis on basic service delivery and capacities for civic participation;
Support to non-state stakeholders: community organisations, CBOs and NGOs in areas affected by crisis and disaster;
Peace building and reconciliation; Rule of law, including law enforcement and access to justice in areas of early recovery;
37
SOMALIA – REVISION
More sustainable reintegration of displaced population and demobilised militia; Strengthening of capacities (local authorities, civil society) to manage and reduce disaster risks
emanating from natural hazards; Small infrastructures to enhance recovery, strengthen reintegration, improve security, or remove
bottlenecks to humanitarian assistance.
Monitoring and IndicatorsProgress on Early Recovery can be monitored, using inter-agency monitoring mechanisms as far as possible, with the following indicators: Access permitting an Early Recovery response; Capacity development and sustainability within the humanitarian emergency response; Country capacities for recovery coordination; Community physical capacity development; Mechanisms for managing and reducing the risk from disasters emanating from natural hazards; Sustained efforts and capacity built for inclusion and participation of women in early recovery
response.
3.10 GENDER (CROSS-CUTTING)Analysis of NeedsThe complex and prolonged emergency situation in Somalia is characterised by fragile governing structures dependent on clan-based militia systems that exclude women and minority groups that are not armed. The matrilineal clan social structures demand allegiance and material support; in return they provide protection and assistance to vulnerable groups. Although women are not part of the clan decision-making structures, they are involved in providing services such as health, food preparation, and mobilisation of resources for the clan militia and leadership. The social costs of the clan-based civil war resulted in displacement within and beyond the borders. Multiple disasters – conflict, drought, floods, and poverty – have taxed social structures to the extent that traditional coping mechanisms and limited resources are unable to sustain. The situation has generated dramatic changes in traditional structures, such as disintegration of family and social networks, while men’s inability to fend and provide for their families has resulted in women taking on additional roles. The prolonged crisis has also led to a dramatic increase in the number of women heads of households with responsibilities for meeting the needs of households coping with stress. These activities expose women to risks and they are often physically and sexually abused, as men have developed a low self-esteem and resent women’s roles as key providers of household incomes.
According to the socio-economic survey of Somalia 2002, an estimated 58% of female-headed households are widows, while the remainder consist of women who have either been divorced or abandoned. There is, therefore, a need for gender analysis and identification of gender-specific needs in the following humanitarian response sectors.
Livelihoods: Women have limited access to diverse livelihood options due to low levels of literacy and lack of access and control of land and other major productive resources this situation is made worse by recurrent drought and intermittent clan-conflicts.
Health: Access to health services during the on-going emergency is restricted, especially for women in rural and inaccessible areas, IDPs, returnees, and the disabled. Poor public health infrastructure, absence of skilled health professionals, and limited resources at household and state level has contributed to high maternal, and child mortality rates.
Nutrition: Household food security is the responsibility of women who have limited knowledge and income. Changing gender roles and heavy burden of generating income in a difficult environment has negatively impacted on the ability of women in poor households to sustain household food security and provide quality care for young and ageing members of the household.
Water and Sanitation: Traditional gender roles allocate the responsibility of providing water to the households to women on girls, while men and boys provide water for livestock. However, most water and sanitation programmes often do not build on the knowledge of women and girls and often, exclude them from planning and management of water and sanitation programmes. Limited information also exists on the cultural and biological water needs of women and girls.
38
SOMALIA – REVISION
Education: Somalia has the lowest primary enrolment in Africa and female enrolment rates are very poor with a gross enrolment rate of girls of 15% and female adult literacy rate 27% compared to 27% for boys and 50% male adult literacy rate. Limited information exists on drop out rates of both girls and boys during emergencies. Low literacy levels limits the ability of women in vulnerable communities to participate in public decision making processes and reduce their capabilities to fulfil their productive as well as reproductive roles.
Capacity Building: Local capacities for coping with disaster and emergencies remain weak, especially among gender-based organisations and institutions. Exclusion, non-representation or unacceptably low representation of women in humanitarian response mechanisms and decision-making structures prevail, affecting the quality and outcome of humanitarian response. Coordination of a common gender response strategy will also need to be strengthened in order to ensure that the humanitarian response effectively addresses gender inequalities in its response.
Objectives The IASC Policy statement for the integration of a gender perspective in Humanitarian Assistance (1999), commits as priority the participation of women in planning, designing and monitoring of all emergency programmes. The focus on women is recognition that they have less access to decision makers due to their low representative in community leadership structures and other factors such as low literacy and limited mobility and time constraints. However, in the context of the Somali clan-based patrilineal culture which has strict gender disaggregated roles it will be important to negotiate with community leaders for an integrated approach which expands participation to include all marginalised groups. The strategy will also have targeted support for capacity building for women’s organisation to enable them to participate as service provider in humanitarian and early recovery. The community-based approach should also include advocacy initiatives targeting community leaders and women’s group on the need to include gender equality and human rights needs in the humanitarian response. Targeted training should be provided for community leaders, women, and youth groups on issues of protection and capabilities as rights holders and duty bearers.
Promote and enhance gender mainstreaming in analysis, design, and implementation, monitoring evaluation of humanitarian recovery response. Indicators: gender disaggregated data; gender responsive programming tools; gender balanced teams;
Enhance equality of access to humanitarian assistance by marginalised groups (minorities, women, IDPs, returnees and disabled) Indicators: Representation of decision making committees engaged in management of humanitarian response;
Promote humanitarian recovery response that addresses specific needs of women and girls (Reproductive health, pregnant lactating women Female Genital Mutilation [FGM], SGBV). Indicators: Percentage of projects that specifically address needs of women and girls;
Establish a gender coordination mechanism and strengthen capacities of the ministries of women and family affairs, women, and youth networks to better respond to emergencies and crises. Indicators: Percentage of women benefiting from capacity strengthening initiatives.
Enhanced gender mainstreaming of the humanitarian response in Somalia will result in a reduction of gender inequalities and ensures equal access to resources by women, men, boys, and girls in vulnerable groups.
Partnerships CISS Gender working group members, UNIFEM, OCHA, UNDP, UNICEF, UNFPA, UNHCR, Heinrich Böll Foundation (HBF), NOVIB, WVI, and other INGOs.
39

SOMALIA – REVISION
3.11 HIV/AIDS (CROSS-CUTTING) – CLUSTER LEAD: UNAIDSAnalysis of NeedsThere are an estimated 40,000 Somalis living with HIV/AIDS. The number of women of 15 years and over is estimated to be 23,000. The HIV/AIDS projects in the 2007 CAP were identified on the basis that the actions are targeting the most vulnerable, including women and children. By mainstreaming HIV/AIDS into CAP sectoral actions, access to HIV/AIDS services will increase among Somalis. Increased and frequent movement of populations within and across borders due to natural and manmade disasters contributes to vulnerability to HIV infection. In addition, loss of livelihood is likely to be accompanied by a rise in commercial sex workers and other harmful coping mechanisms, which leave women and children vulnerable to exploitation and HIV infection. For those infected, poor nutritional status increases the risk of mortality and morbidity. In turn, increased mortality deprives children of parents and households of income generators and contributes to long-term vulnerability. Provision of Prevention of Mother to Child Transmission (PMTCT) services and paediatric anti- retroviral therapy will reduce HIV/AIDS mortality among children and ultimately prevent HIV infection in the next generation.
Cross-cutting Sector ObjectivesTo ensure that most vulnerable have equitable access to integrated prevention, treatment, care and support services especially orphans, women and children and people living with HIV/AIDS.
PartnershipsUNAIDS, UNICEF, UNFPA, HDO, FERO, and IOM.
40
SOMALIA – REVISION
SUPPORT SECTORS
3.12 LOGISTICS/SUPPORT – CLUSTER LEAD: WFPAnalysis of NeedsSince the submission of inputs for the 2007 CAP, major developments have taken place in Somalia that now greatly impact not only on the required logistics capacity but also on the priorities on which the Logistics Cluster will focus in 2007.
On the one hand, the flooding of late 2006 resulted in a considerable increase in beneficiaries that needed to be reached. Response activities undertaken since the floods, and that are anticipated to extend well into the first half of 2007, have required an increase in logistical capacity. While the Logistics Cluster emergency preparedness plan was activated and implemented in good time, and transport capacity was able to respond to the needs quickly, the destruction of the transport infrastructure in country has resulted in significant additional logistical obstacles. Thus, emergency repairs of key transport infrastructure, e.g. targeted road and bridge repairs, need to be urgently addressed in order to support continued flood- and conflict-response activities. Moreover, these repairs will be critical to allow for all-year-round access in preparedness of expected recurrences of natural disasters.
On the other hand, increasingly restricted access has considerably slowed down and even suspended relief activities. The closure of the Kenya/Somalia border at the end of December 2006 and the lack of security guarantees for use of sea- and airports in large parts of humanitarian priority areas has increased the need for advocacy on humanitarian access.
While agencies themselves will need to carry out internal reviews and, where necessary, make internal logistical adjustments to operations, improvement in targeted areas will need to be coordinated amongst agencies. Consequently, the shift in focus during the second half of the 2007 CAP cycle will be as follows:
Advocacy on access and customs/taxes, particularly vis-à-vis the Kenya/Somalia border closure and customs issues in Kenya and Somalia;
Establishing of contacts and information-sharing with external counterparts vital to logistics operations inside Somalia, notably the TFG and AU but also the commercial sector and development partners;
Logistics preparedness for recurring seasonal emergencies, particularly in Middle and Lower Juba, including emergency repair of critical transport infrastructure.
Insecurity, poor infrastructure, and adverse seasonal weather conditions remain the key logistical obstacles to timely and efficient aid delivery in Somalia, leaving some areas of humanitarian priority difficult or impossible to reach. Finding solutions to some of these complex obstacles goes beyond the scope of the work of the Logistics Cluster. Thus, a solid integration with early recovery efforts, linkages with development partners and advocacy efforts with key stakeholders will be one of the priorities in 2007.
ObjectiveEnsuring a timely and sufficient pipeline that corresponds to programme needs and priorities through synchronised logistical support and, where possible, the use of common resources.
PartnershipsWFP, UNHCR, UNICEF, WHO, FAO, ACF, ADRA, CARE, GHC, Horn Relief, IMC, IR, Nardo, OXFAM, SC–UK, SPO, World Vision.
Indicators On-time delivery of relief items corresponding to programme priorities and timelines. Percentage of requests for logistics support by other Clusters responded to. Adequate storage in strategic locations. Relief goods and other supplies procured locally, where possible. Logistical obstacles resolved through advocacy, where appropriate. Logistics Cluster Emergency Response Plan implemented.
41
SOMALIA – REVISION
Number of resources pooled and costs shared. Number of trainings conducted and number of local staff trained, particularly on cargo handling
and storage.
Implications If the Response Plan is Not Implemented Considering the cost-intensive logistics operation for Somalia, continued efforts to improve the effectiveness and efficiency of these life-saving operations are crucial. Failure to do so not only risks preventable loss of life but also keeps the running cost of operations high.
3.13 COORDINATION/SUPPORT
Analysis of NeedsIn 2006, in collaboration with local authorities, UN agencies and NGO partners, OCHA Somalia has continued to conduct and lead inter-agency assessment missions, identify urgent priorities, and facilitate the planning of common responses to meet the needs of affected populations.
Working with partners, coordination activities in Somalia will be strengthened in 2007 through an increased field staff presence (both in the number and seniority of international and national staff), especially in the more difficult operating environments of southern and central Somalia. This increased staff presence will enhance the delivery of humanitarian assistance by improving access through negotiations with local authorities, promoting humanitarian principles at the local level, and supporting grass-roots reconciliation initiatives in collaboration with the local authority structures. OCHA will continue its coordination role to support UN agencies, NGOs, and other partners in their efforts to strengthen protection of the most vulnerable in Somalia, including women and ethnic minorities. OCHA will also work to mobilise resources to improve the humanitarian community’s response capacity, and, through coordination and information sharing, improve the timeliness of humanitarian response. OCHA and its UN and NGO partners will advocate at local and international levels on the humanitarian situation in south and central Somalia that has been neglected and inaccessible for many years. OCHA will also support the two intricately linked pillars of the 2007 CAP – humanitarian assistance and early recovery – working closely with the UNDP RC Office on integrated coordination support.
In 2007 OCHA and UNDP, through the RC’s Office, will contribute to integrated UN coordination arrangements to support early recovery and peace-building initiatives being undertaken in Somalia. The RC’s Office will establish a field presence in parts of Somalia where the conditions for early recovery programmes are most conducive and where OCHA has reduced its field presence as a result of diminishing humanitarian needs. Integrated coordination will help to support the dual pillars of the 2007 CAP: early recovery and humanitarian assistance.
Following the implementation of the Humanitarian Reform, Somalia is now one of four pilot countries to implement the cluster leadership approach, aimed at improving the predictability, timeliness, and effectiveness of humanitarian response. In early 2006, OCHA facilitated the establishment of eight clusters (now nine) and the creation of a Somalia IASC to support the Humanitarian Coordinator. The cluster approach will continue to be strengthened in 2007.
ObjectiveTo provide timely, cost-effective, and integrated humanitarian response and to advocate for increased access and operational capacity in areas of south/central Somalia previously neglected due to insecurity.
PartnershipsIASC members, cluster leads, United Nations Political Office for Somalia (UNPOS), United Nations Country Team (UNCT), NGO Consortium, UNDSS, CISS, national, local, and de facto authorities.
42
SOMALIA – REVISION
Table II: Summary of Requirements – By Sector
Table I: Consolidated Appeal for Somalia 2007
Requirements, Commitments/Contributions and Pledges per Sector as of 12 April 2007
http://www.reliefweb.int/fts
Unmet Requirements Funding Revised
Requirements Original Requirements
Compiled by OCHA on the basis of information provided by donors and appealing organisations Uncommitted
Pledges % Covered SECTOR
A B C B-C D C/B Value in US$ 32,245,986 35,024,628 29,655,520 - 2,590,466 8% AGRICULTURE 33,596,361 15,030,795 24,177,589 - 9,418,772 28% COORDINATION AND SUPPORT SERVICES 30,543,763 23,617,763 30,543,763 - - 0% ECONOMIC RECOVERY AND INFRASTRUCTURE
8,588,945 7,892,736 8,588,945 - - 0% EDUCATION 58,720,538 64,967,929 3,130,892 66,225 55,589,646 95% FOOD 33,974,986 31,137,157 32,645,441 - 1,329,545 4% HEALTH
322,964 - - - 322,964 100% MINE ACTION 9,207,320 8,612,039 8,558,812 2,575,000 648,508 7% MULTI-SECTOR
21,149,801 20,129,938 20,784,689 - 365,112 2% PROTECTION/HUMAN RIGHTS/RULE OF LAW - - (11,000,409) 6,645,648 11,000,409 0% SECTOR NOT YET SPECIFIED
5,475,674 4,233,646 4,475,674 - 1,000,000 18% SECURITY 19,032,895 17,340,500 17,665,965 105,058 1,366,930 7% SHELTER AND NON-FOOD ITEMS
9,495,382 9,125,693 7,569,535 - 1,925,847 20% WATER AND SANITATION GRAND TOTAL 262,354,615 237,112,824 176,796,416 9,391,931 85,558,199 33%
the actual payment of funds or transfer of in-kind goods from the donor to the recipient entity.
Contribution: creation of a legal, contractual obligation between the donor and recipient entity, specifying the amount to be contributed.
Commitment: a non-binding announcement of an intended contribution or allocation by the donor. ("Uncommitted pledge" on these tables indicates the balance of original pledges not yet committed).
Pledge: NOTE: "Funding" means Contributions + Commitments + Carry-over
The list of projects and the figures for their funding requirements in this document are a snapshot as of 12 April 2007. For continuously updated information on projects, funding requirements, and contributions to date, visit the Financial Tracking Service (www.reliefweb.int/fts).
43

SOMALIA – REVISION
ANNEX I. INTEGRATED FOOD SECURITY AND HUMANITARIAN PHASE CLASSIFICATION REFERENCE TABLE
PhaseClassification
Key Reference Characteristics Strategic Response Framework
(Current or imminent outcomes on lives and livelihoods; based on convergence of evidence)
(Mitigate immediate outcomes, support livelihoods, and address
underlying/structural causes)
5
Gen
eral
lyFo
od S
ecur
e
Crude Mortality Rate < 0.5 / 10,000 / day
Wasting <3 % (w/h <-2 z-scores) Strategic assistance to pockets of food-insecure groups.
Stunting <20% (w/age <-2 z-scores) Investment in food and economic production systems.
Food Access/ Availability Usually adequate (> 2,100 kcal ppp day), stable
Enable development of livelihood systems based on principles
Dietary Diversity Consistent quality and quantity of diversity
of sustainability, justice, and equity.
Water Access/Avail. Usually adequate (> 15 litres ppp day), stable
Prevent emergence of structural hindrances to food security.
Hazards Moderate to low probability and vulnerability
Advocacy.
Civil Security Prevailing and structural peace
Livelihood Assets Generally sustainable utilisation (of 5 capitals)
4
Chr
onic
ally
Food
-inse
cure
Crude Mortality Rate 0.5-1/10,000/day; U5MR<= 2/10,000/day
Wasting >3% but <10 % (w/h <-2 z-score), usual range, stable
Design & implement strategies to increase stability, resistance,
Stunting 20-40% (w/age <-2 z-scores) and resilience of livelihood systems, thus reducing risk.
Food Access/ Availability Borderline adequate (2,100 kcal ppp day); unstable
Provision of ‘safety nets’ to high risk groups.
Dietary Diversity Chronic dietary diversity deficit Initiatives for optimal and sustainable use of livelihood assets.
Water Access/Avail. Borderline adequate (15 litres ppp day); unstable
Create contingency plan.
Hazards Recurrent, with high livelihood vulnerability
Redress structural hindrances to food security.
Civil Security Unstable; disruptive tension Close monitoring of relevant outcome and process indicators.
Coping ‘Insurance strategies’ Advocacy.
Livelihood Assets Stressed and unsustainable utilisation (of five capitals)
Structural Pronounced underlying hindrances to food security
3
Acu
te F
ood
and
Live
lihoo
d C
risis
Crude Mortality Rate 1-2 /10,000/day, >2x reference rate; U5MR 2-4/10,000/dy
Support livelihoods and protect vulnerable groups.
Wasting 10-15 % (w/h <-2 z-score), > than usual, increasing
Strategic and complimentary initiatives to immediately ↑ food access/
Disease Endemic outbreak; increasing availability and support livelihoods.
Food Access/ Availability Lack of entitlement; 2,100 kcal ppp day via asset stripping
Selected provision of complimentary sectoral support (e.g., water, shelter,
Dietary Diversity Acute dietary diversity deficit sanitation, health, etc).
Water Access/Avail. 15 litres ppp day accessed via asset stripping
Strategic initiatives at community to national levels to create, stabilise,
Destitution/Displacement Emerging; diffuse rehabilitate, or protect priority livelihood assets.
Civil Security Limited spread, low intensity conflict
Create or implement contingency plan.
Coping ‘Crisis strategies’; CSI > than reference; increasing
Close monitoring of relevant outcome and process indicators.
Livelihood Assets Accelerated and critical depletion or loss of access
Use ‘crisis as opportunity’ to redress underlying structural causes.Advocacy.
44
SOMALIA – REVISION
PhaseClassification
Key Reference Characteristics Strategic Response Framework
(Current or imminent outcomes on lives and livelihoods; based on convergence of evidence)
(Mitigate immediate outcomes, support livelihoods, and address
underlying/structural causes)
2
Hum
anita
rian
Emer
genc
yCrude Mortality Rate 2-4 / 10,000 / day, increasing;
U5MR > 4/10,000/day
Wasting >15 % (w/h <-2 z-score), > than usual, increasing Urgent protection of vulnerable groups.
Disease Pandemic outbreak Urgently ↑ food access through complimentary initiatives.
Food Access/ Availability Severe entitlement gap; unable to meet 2,100 kcal ppp day
Selected provision of complimentary sectoral support (e.g., water, shelter,
Dietary Diversity Regularly 2-3 or fewer main food groups consumed
sanitation, health, etc).
Water Access/Avail. < 7.5 litres ppp day (human usage only)
Protection against complete livelihood asset loss and/or advocacy for access.
Destitution/Displacement Concentrated; increasing
Civil Security Widespread, high intensity conflict
Close monitoring of relevant outcome and process indicators.
Coping ‘Distress strategies’; CSI significantly > than reference
Use ‘crisis as opportunity’ to redress underlying structural causes.
Livelihood Assets Near complete & irreversible depletion or loss of access Advocacy.
1
Fam
ine
/ Hum
anita
rian
Cat
astr
ophe
Crude Mortality Rate > 4 /10,000 /day (example: 6,000/500,000/30 days)
Critically urgent protection of human lives and vulnerable groups.
Wasting > 30 % (w/h <-2 z-score) Comprehensive assistance with basic needs (e.g. food, water, shelter,
Disease Pandemic outbreak sanitation, health, etc).
Food Access/ Availability Extreme entitlement gap; much below 2,100 kcal ppp day
Immediate policy/legal revisions where necessary.
Water Access/Avail. < 4 litres ppp day (human usage only)
Negotiations with varied political-economic interests.
Destitution/Displacement Large scale, concentrated Use ‘crisis as opportunity’ to redress underlying structural causes.
Civil Security Widespread, high intensity conflict Advocacy.
Livelihood Assets Effectively complete loss; collapse
Early Warning Levels
Probability / Likelihood of Worsening
PhaseSeverity Key Reference Characteristics Implications for Action
WatchAs yet unclear Not applicable
Hazard: occurrence of, or predicted event stressing livelihoods; with low or uncertain vulnerability
Close monitoring and analysis.
Process Indicators: small negative change from normal
Moderate Risk
Elevated probability / likelihood Colour of diagonal
lines on map match predicted
Phase Class
Hazard: occurrence of, or predicted event stressing livelihoods;
Close monitoring and analysis.
With moderate vulnerability Contingency planningProcess Indicators: large negative change from normal
Step-up current Phase initiatives.
High Risk
High probability; ‘more likely
than not’
Hazard: occurrence of, or strongly predicted major event stressing livelihoods; with high vulnerability
Preventative initiatives--with increased urgency for High Risk populations.
Process Indicators: large and compounding negative changes
Advocacy.
Source: FAO/FSAU
45
SOMALIA – REVISION
ANNEX II. ESTIMATED RURAL POPULATION BY REGION IN HUMANITARIAN EMERGENCY (HE) AND ACUTE FOOD AND LIVELIHOOD CRISIS (AFLC)
Affected RegionsUNDP 2005 Total
Population15
Assessed and Contingency Population in AFLC and HE
Acute Food and Livelihood Crisis
(AFLC)16
Humanitarian Emergency (HE)Error:
Reference sourcenot found
Total in AFLC or HE as % of Region
population
North17 Awdal 305,455 0 0 0Bari 387,969 0 0 0Nugaal 125,010 0 0 0Sanaag 270,367 0 0 0Sool 150,277 0 0 0Togdheer 402,295 0 0 0Woqooyi Galbeed 700,345 0 0 0
Sub-Total 2,341,718 0 0 0CentralGalgaduud 330,057 0 0 0Mudug 350,099 0 0 0
Sub-Total 680,156 0 0 0SouthBakool 310,627 80,000 0 26Bay 620,562 10,000 0 2Gedo 328,378 90,000 110,000 61Hiraan 329,811 10,000 10,000 6Juba Lower 385,790 90,000 40,000 34Middle Juba 238,877 80,000 70,000 63Lower Shabelle 850,651 0 0 0Middle Shabelle 514,901 0 0 0Banadir 901,183 0 0 0
Sub-Total 4,480,780 360,000 230,000 13
GRAND TOTAL 7,502,654 360,000 230,000 8
Table 1B: Summary TableError: Reference source not found
Assessed and Contingency Rural Population Numbers in AFLC and HE 590,000 8Error: Referencesource not found
Estimated Number of IDP’s18 400,000 5Error: Referencesource not found
Estimated Total Population in Crisis 990,000 1419
Source: FAO/FSAU
15 Source: Population Estimates by Region/District, UNDP Somalia, August 1, 2005. Note this only includes population figures in affected regions. FSAU does not round these population estimates as they are the official estimates provided by UNDP16 Estimated numbers are rounded to the nearest five thousand, based on resident population not considering current or anticipated migration, and are inclusive of population in High Risk of AFLC or HE for purposes of planning17 Dan Gorayo is included within Bari Region following precedent set in population data prior to UNDP/WHO 200518 Source: UN-OCHA updated April 2004 (376,630) and UNHCR IDP map Dec.2005 (407,000), rounded to 400,000 as an estimate19 Percent of total population of Somalia estimated at 7,502,654 (UNDP/WHO 2005)
46
SOMALIA – REVISION
ANNEX III. LONG-TERM NUTRITION TRENDS (1999 - 2005)
47
SOMALIA – REVISION
ANNEX IV. NUMBER OF ORGANISATIONS CONSULTED DURING CAP CONSULTATION PROCESS 2007
Number of CAP ParticipantsBAIDOA GAROWE HARGEISA MOGADISHU NAIROBI
Somali Local NGOs 14 12 11 - 29
UN Agencies 7 9 12 9 15
International NGOs 7 3 7 3 28
SCRS 1 - - - 1
TOTAL 29 24 30 12 73
NO OF PARTICIPANTS MOGADISHU BAIDOA GAROWE HARGEISA NAIROBI TOTAL
TOTAL 14 60 56 56Day One = 168
Day Two= 135
331
(1) Total Number of UN Agencies Consulted: 161.UNICEF, 2.OCHA, 3.ILO, 4.UNDSS, 5. UN-HABITAT, 6.FAO, 7.WHO, 8.WFP, 9.UNHCR, 10.UNIFEM, 11.UNAIDS, 12.UNPOS, 13.UNESCO, 14.UNDP, 15.UNFPA 16.UNPOS
(2) Major International Non Governmental Organisations consulted: 301. African Education Trust (AET), 2. Swiss Caritas, 3. Concern, 4. CRD, 5. Norwegian Refugee Council (NRC), 6. Concern Worldwide, 7. World Vision, 8. IUCN, 9. Diakonia, 10. CARE, 11. IAS, 12. Intersol-Denmark, 13. Handicap 14. Save The Children UK and Denmark 15. Danish Refugee Council (DRC) 16.Oxfam 17. ACF 18. AGROSPHERE 19. ADRA 20.Creative Associates International 21. FEWS-Net 22. Gedo Health Consortium (GHC) 23. Horn Relief 24. HDO (Human Development Organization) 25. INTERSOS 26. Solidarites 27. WSP 28. IOM 29. COOPI 30. Intel-Denmark
(3) International Red Cross Movement: 11.Somali Red Crescent Society;
(4) Total Number of Somali NGOs: 40Baido: BWOU, Baidoa Intellectuals, Community Care Centre Baidoa, DMO Bay, GREDO, Greenhope, IHRO, IRRDA, LORDO, SACOD, TRDA, Taqwa, Fahrd Kismayo, Wajid Intellectuals Garowe: Dan Dor Bossaso; PASWEN, SOHDO Galkayo, RMCO Bossaso Office, KAALO, NUUDAN, NEESHA, MUDAN, SRWU, TAAKULO, DAVYEEH, SORERDOHargeisa: Agriculture Development Organization (ADO), Academy For Peace, NAGAAD, Havoyoco, Candlelight, Samotalis (Human Rights), Somali Rights Watch, Gashan IDPs, Community Based Reintegration of Human Rights (CCBRS), VOSOMWO (Minority women’s group), Somaliland National Disability Forum (SNDF), EDC (Education Development Communication), PENHA
(5) AuthoritiesAuthorities were represented in Hargeisa, Garowe and Baidoa and in Nairobi where the Minister of Foreign Affairs was present.
(6) Others: Inter-agency team from the Real Time Evaluation – Somalia
48
SOMALIA – REVISION
ANNEX V. CISS (FORMER SACB) AND IASC ORGANIGRAMME
CISS SECTORS Health
(Includes Nutrition)
Governance(Gender &
Human Rights) Education Water & Sanitation
Food Security & Rural
Development (includes Food and Agriculture and Livelihoods)
HIV/AIDS
IASC CLUSTERS Protection ** Logistics Emergency
Shelter
49
ACCESS REGIONAL OVERVIEW
PRIVATE SECTOR
GOVERNMENT CIVIL SOCIETY
CISSExCom
NGO CONSORTIUM
UN COUNTRY TEAM(UNCT)
SOMALI DONOR GROUP (SDG)
Relief to D
evelopment
Sector Chairs Committee (SCC)
FUNDING TOOLS INCLUDE : INTERIM SUPPORT FUND FOR SOMALIA
PLANNING TOOL: RECONSTRUCTION AND DEVELOPMENT PLAN THROUGH THE JNA
Support services provided by Coordination of
Interim Support to Som
alia (CISS), form
erly SA
CB
/SSS
Secretariat support services provided by UN
O
CH
A
IASC: Chaired by HC
IDP Working Group
Focus Hum
anitarian/Com
plex Emergency
Humanitarian Response Group: Technical Inter cluster Mechanism
FUNDING TOOLS INCLUDE: HUMANITARIAN RESPONSE FUND
PLANNING TOOL: CONSOLIDATED APPEAL PROCESS 2007 (CAP)
** Protection cluster feeds into Governance Sector to promote the protection of civilians
& vulnerable groups and vice-versa
SOMALIA
ANNEX VI. UNITED NATIONS AGENCIES IN SOMALIA
50
SOMALIA
ANNEX VII. ACRONYMS AND ABBREVIATIONS3W Who, Where, What?
ACF Action Contre la FaimADRA Adventist Development and Relief AgencyAET Africa Educational TrustAFLC Acute Food and Livelihood CrisisAFREC African Rescue CommitteeAIDS Acquired Immuno-Deficiency SyndromeAMA African Muslim Agency AMISOM African Union Mission in SomaliaASEP Advancement for Small Enterprise ProgrammeAU African UnionAWD Acute watery diarrhoea
CAP Consolidated Appeal Process; or, consolidated appealCARE Cooperative for Assistance and Relief EverywhereCAS Child Aid SomaliaCBO community-based organisationCCBRS Comprehensive Community-Based Rehabilitation in SomaliaCEC Community Education CommitteeCEFA European Committee for Agricultural TrainingCERF Central Emergency Response Fund CfBT Centre for British TeachersCHAP common humanitarian action planCISP Comitato Internazionale per lo Sviluppo dei PopoliCISS Coordination of International Support to SomalisCLHEE Candlelight for Health, Education, and EnvironmentCMC Coordination and Monitoring CommitteeCMR crude mortality rateCOOPI Cooperazione InternazionaleCOSV Comitato di Coordinamento delle Organizzazioni per il Servizio VolontarioCPA Comprehensive Plan of Action
DEB District Education Board DMO Deeg-Roor Medical OrganisationDPT diphtheria/pertussis/tetanusDRC Danish Refugee Council
EDC Education Development CentreEMIS Education Management Information System EmOC emergency obstetric careEMOSS Enhanced Minimum Operating Security StandardsEOD explosive ordnance disposal EPI Expanded Programme of ImmunisationESC Education Sectoral CommitteeEXCOM CISS’ Executive Committee
FAO Food and Agriculture Organization of the United NationsFERO Family Empowerment and Relief OrganisationFEWS-Net Famine Early Warning System NetworkFGM female genital mutilationFSAU Food Security Analysis UnitFTS Financial Tracking Service
GAM global acute malnutritionGHA Greater Horn of AfricaGHC Gedo Health ConsortiumGoK Government of KenyaHARDO Horn of Africa Relief and Development OrganizationHBF Heinrich Böll FoundationHC Humanitarian CoordinatorHDO Humanitarian Development OrganisationHE humanitarian emergencyHI Handicap InternationalHIV Human Immuno-Deficiency VirusHRF Humanitarian Response Fund
51

SOMALIA
HRG Humanitarian Response GroupHSC Health Sectoral Committee
IAS International Aid ServiceIASC Inter-Agency Standing Committee ICRC International Committee of the Red CrossICU Islamic Courts UnionICVA International Council of Voluntary AgenciesIDP internally displaced personIFRC International Federation of Red Cross and Red Crescent SocietiesIGAD Inter-Governmental Authority on DevelopmentILO International Labour Organization IMC International Medical CorpsINGOs International non-governmental organisationsIOM International Organization for MigrationIPAC IGAD Climate Prediction and Applications CentreIPC Integrated Food Security and Humanitarian Phase Classification IR Islamic ReliefIRIN Integrated Regional Information NetworksISFS Interim Support Fund for SomaliaISRA International Somalia Rehabilitation Association
JCC Jubaland Charity CentreJNA Joint Needs AssessmentJPC Joint Planning CommitteeJTC Joint Thematic Committee
LNGO local non-governmental organisation
MCH mother and child healthMERLIN Medical Emergency Relief InternationalMICS multiple indicator cluster surveyMoE Ministry of EducationMoH Ministry of HealthMORSS Minimum Operating Residential Security StandardsMoU memorandum of understandingMSEE Minimum Standards in Education Emergencies MSF Médecins Sans FrontièresMT metric tonne
NCA Norwegian Church AidNID national immunisation daysNGO non-governmental organisationNOVIB Nederlandse Organisatie voor Internationale Bijstand NRC Norwegian Refugee Council
OCHA Office for the Coordination of Humanitarian AffairsOFDA United States Office of Foreign Disaster Assistance
PENHA Pastoral and Environmental Network in the Horn of AfricaPES primary education surveyPHC primary health carePMTCT prevention of mother-to-child transmissionPWA post-war averageRC Resident CoordinatorRDP Reconstruction and Development ProgrammeREO Regional Education OfficerRPG rocket propelled grenadeRTE real-time evaluation
SACB Somalia Aid Coordination Body/SecretariatSADO Social-Life and Agricultural Development Organisation SAF Somalia Aid FoundationSAFE Southern African Fund for EducationSC Save the Children SCHR Steering Committee for Humanitarian ResponseSCIC Supreme Council of the Islamic CourtsSCOTT Strengthening Capacity of Teacher Training SDG Somali Donor Group
52
SOMALIA
SGBV sexual and gender-based violenceSPHERE Humanitarian Charter and Minimum Standards in Disaster ResponseSPU Special Protection UnitSRCS Somali Red Crescent SocietySSS Somalia Support SecretariatSST sea surface temperaturesSTI sexually transmitted infectionSWALIM Somalia Water and Land Information Management SWRDA South West Relief Development Agency
TFG Transitional Federal GovernmentTFI Transitional Federal Institution
UIC Union of Islamic CourtsUN United NationsUNAIDS Joint United Nations Programme on HIV/AIDS UNCAS United Nations Common Air ServicesUNCT United Nations Country TeamUNDP United Nations Development ProgrammeUNDSS United Nations Department of Safety and SecurityUNESCO United Nations Educational, Scientific, and Cultural OrganizationUNFPA United Nations Population FundUNHABITAT United Nations Human Settlements ProgrammeUNHCR United Nations High Commissioner for RefugeesUNICEF United Nations Children's FundUNIFEM United Nations Development Fund for WomenUNPOS United Nations Political Office for SomaliaUSAID United States Agency for International Development
VCT voluntary counselling and testingVETAID Veterinary AidVSF-S Vétérinaires Sans Frontières-Switzerland
WASH water, sanitation, and hygieneWatSan water and sanitationWCI World Concern InternationalWFL Water For LifeWFP World Food ProgrammeWHO World Health OrganizationWVI World Vision International
53
NOTES:
Consolidated Appeal Feedback Sheet
If you would like to comment on this document please do so below and fax this sheet to + 41–22–917–0368 (Attn: CAP Section) or scan it and email us: [email protected] Comments reaching us before 1 September 2007 will help us improve the CAP in time for 2008. Thank you very much for your time.
Consolidated Appeals Process (CAP) Section, OCHA
Please write the name of the Consolidated Appeal on which you are commenting:
1. How could it be improved?
2. Is the context and prioritised humanitarian need clearly presented?How could it be improved?
3. To what extent do response plans address humanitarian needs?How could it be improved?
4. To what extent are roles and coordination mechanisms clearly presented?How could it be improved?
5. To what extent are budgets realistic and in line with the proposed actions?How could it be improved?
6. Is the presentation of the document lay-out and format clear and well written?How could it be improved?
Please make any additional comments on another sheet or by email.
Name:Title & Organisation:Email Address:
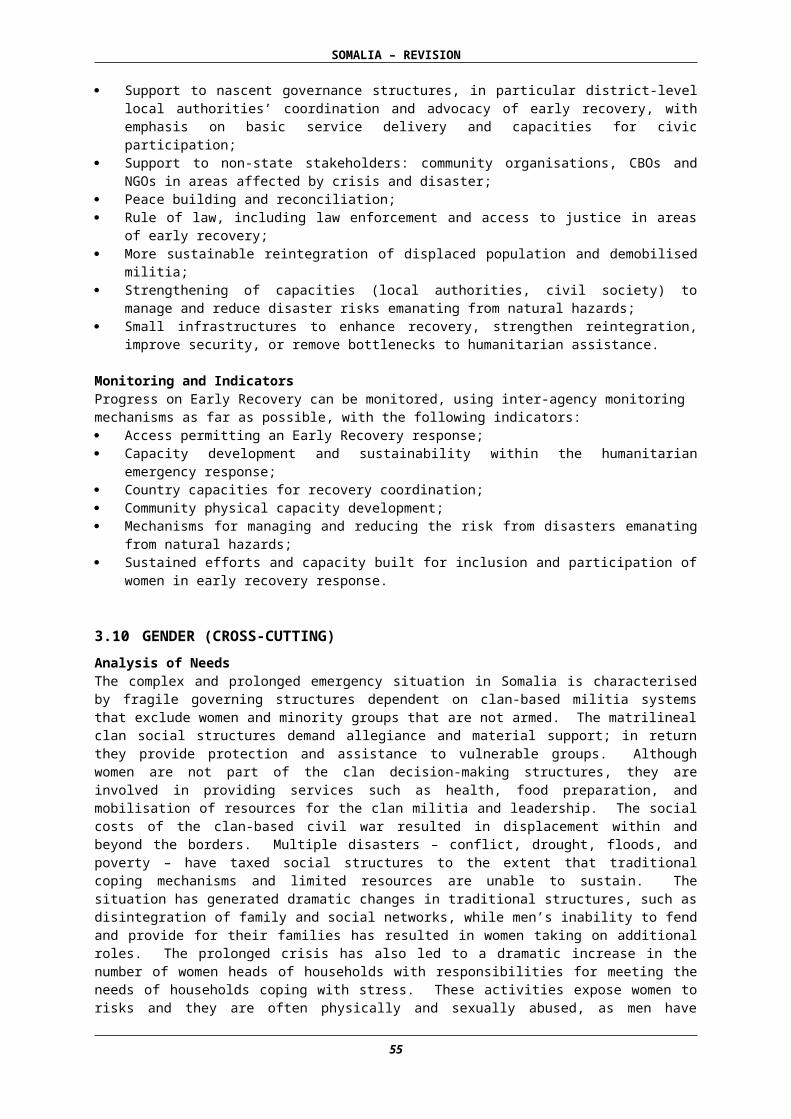
OFFICE FOR THE COORDINATION OF HUMANITARIAN AFFAIRS(OCHA)
UNITED NATIONS PALAIS DES NATIONSNEW YORK, N.Y. 10017 1211 GENEVA 10
USA SWITZERLAND


















