MELAS Syndrome in a Child: CT and MR Findings · 2019-09-17 · DC, Rowland LP. Mitochondrial...
5
1993 ; 29 (1) : 164 Jou rna l of Korean Radiological Societ y , Ja nuar y , 1993 MELAS Syndrome in a Child: CT and MR Findings Hye Young Choi , M.D. , SOO Jong Hong , M.D.* , Jeong Hee Cho , M.D.** , Dae Chul Suh , M.D. , Chang Yee Hong , M.D. * 01 Radiology, Asan Medical 01 - Abstract - MELAS (mitochondrial myop at hy , encephalopathy , lactic acidosis , a nd stroke-Ii ke e pi sodes) is one of the mitochondrial encephalomyopathy , A rare disease caused by a dis turb ance of the mitochondrial chain of respiration MELAS is confirmed by typicallight and e1 ectron micros co pic findings “ ragged red fib ers" by modified Gomori trichrome stain on Ii ght microscope and numerous abormal mit oc hondria on e1 ectron microscope. We experienced a boy with the characteristic c1 inical a nd pathologic findings of MELAS. Our patient de monstrat ed bilater al basal ganglia calcifications and inf arction at right parieto-occipital and thalamic areas on CT and MR. We found that MRI was mor e sensitive and re presented the infarcted Ie sions better than C T. Detection 0 1" ce rebral insults of MELAS by MRI is importa nt in makin g d ec ision on patient treatm ent a nd also in pr edicion of the p at ient pro gno sis. Index Words: Brain , MR studi es Br a in , CT Brain , diseases Mu scl es , diseases Children , tral uerous system INTRODUCTION We ex peri en ce d a bo y with MELAS which is char ac te rized by mitochondrial m yo p at hy , e nc e phalopathy , lactic acidosis , and stroke-like e pi so des. Th e pati e nt demons t rated followin g car dinal characteristics of MELAS: norm al ea r- ly de ve l opm e nt , short stature , seizures , he miparesis and “ ragged red fibers" on muscl e biop sy . MELAS represents a syndrome distinct from two other clin ical disord ers that are also assoc iat ed with mitochondrial myopathy and cerebral disease:K ea rns-Sayr e syndrome and th e m yoclo nus epilepsy w ith ragged red fiber (MERRE) sydrome. MELAS was con firm ed by de monstrating “ ragged red fibe rs " by modified Gomori trichrom e stain on light mi c ro sc ope and num ero us abnorm al mitoch o ndri a contained with paracrystall in e or osmophilic inclusion bodi es on electron microscopic examination. Th e co mputed tomographic (CT) findings of MELAS have b ee n reported in the r ece nt * Deþa rtment 01 Pediatrics, Medical University 01 Ulsan. ** ** 01 Pathology, Asan University 01 Received September 21 , Accepted N ovember 17, 1992 - 160
Transcript of MELAS Syndrome in a Child: CT and MR Findings · 2019-09-17 · DC, Rowland LP. Mitochondrial...

대 한 망 사 선 의 학 회 지 1993 ; 29 (1) : 160~ 164
Jou rnal of Korean Radiological Society, Ja nuary, 1993
MELAS Syndrome in a Child: CT and MR Findings
Hye Young Choi, M.D. , SOO Jong Hong, M.D.* , Jeong Hee Cho , M.D.** , Dae Chul Suh, M.D. , Chang Yee Hong, M.D. *
Departmeηt 01 Di,αgnostic Radiology, Asan Medical Ceηter, U:ηzveηsty 01 Ulsaη
- Abstract -
MELAS (mitochondrial myopathy, encephalopathy, lactic acidosis , and stroke-Iike episodes) is one of
the mitochondrial encephalomyopathy , A rare disease caused by a di sturbance of the mitochondrial chain
of respiration
MELAS is confirmed by typicallight and e1ectron microscopic findings “ ragged red fibers" by modified
Gomori trichrome stain on Iight microscope and numerous abormal mitochondria on e1ectron microscope.
W e experienced a boy with the characteristic c1 inical and pathologic findings of MELAS. Our patient
demonstrated bilateral basal ganglia calcifications and infarction at right parieto-occipital and thalamic areas
on CT and MR. We found that MRI was more sensitive and represented the infarcted Iesions better than CT.
Detection 0 1" cerebral insults of MELAS by MRI is important in making decision on patient treatment
and also in predicion of the patient prognosis.
Index Words: Brain , MR studies
Brain , CT
Brain , diseases
Muscles , diseases
Children , ce、 tral uerous system
INTRODUCTION
We experie nced a boy with MELAS which is
characterized b y mitochondrial m yopath y , encephalopathy , lactic acidosis , and stroke-like
episodes. The patient demonstrated following
cardinal characteristics of MELAS: normal ear
ly development , short stature , seizures , hemiparesis and “ ragged red fibers" on muscle
biopsy . MELAS represents a syndrome distinct
from two other clin ical disorders that are also
*울산대학교 의과대학 소아과학교실
associated with mitochondrial myopathy and
cerebral disea se: K earns-Sayre syndrome and the
m yoclonus epilepsy with ragged red fibe r
(MERRE) sydrome.
MELAS was confirmed b y demonstrating
“ ragged red fibers " b y modified Gomori
trichrome stain on light micro scope and
numerous abnormal mitochondria contained
with paracrystall ine or osmophilic inclusion
bodies on electron microscopic examination.
The computed tomographic (CT) findings of
MELAS have been reported in the recent
* Deþartment 01 Pediatrics, Asaη Medical Ceηter, University 01 Ulsan. ** 울산대학교 의과대학 병리학교실 ** Departmeηt 01 Pathology, Asan Medic,αl Ceηter, University 01 Ulsaη.
이 논문은 1992년 9월 21일 접수하여 1992년 11월 17일에 채택되었음.
Received September 21 , Accepted N ovember 17, 1992
- 160

literatures . but not the MRI findings. CT & MRI of our patient showed calcifications in both basal ganglia and infarction in right parieto
occipital and thalamic areas. However , MRI was
more sensitive and clearly defined the lesion bet
ter than CT. W e report a case of a child with
characteristic clinical, pathologic and radiologic
findings of MELAS
CASE REPORT
A 8-year-old boy was admitted with fever , vomiting, poor consiousness , and involuntary
myoclonic jerk in his left arm. One day before
admission , he complained right sided headache
and eye pain. H e also presented with visual and
speech disturbance. This boy had a normal
prenatal and perinatal period , and h ad ordinary
a b
c d
Hye Young Choi , et al : MEALS Syndrome in a Child
family history . At the age of 6, he was first ad
mitted with left facial paralysis and frequent headache , leg pain , and low exercise tolerance.
At that time , his growth and development had
been slowed down resulting in short stature and
underweigh t. Brain CT performed with CT/T
9800 (General Electric, Milwaukee, Wisconsin)
showed no sighificant abnormalities.
On his second admission 2 yrs later, blood lac
tate level was elevated to 48 mg/dl (normal , 10-20
mg/dl) , EEG showed epileptic and ischemic
n a ture , and EMG was compatible with
myopathic process. Brain CT showed low den
sity lesion in the right parieto-occipital a reas and
calcifications in both basal ganglia (Fig. la)
T l-weighted image (T 1 WI) obta ined in a
1 .5T MR unit (Signa, General E letric , Milwaukee , Wisconsin) showed low signal inten
sity in right parieto-occipital and thalamic areas ,
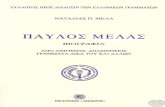
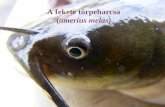
Fig. 1. a . Axial non-enhanced CT scan shows bilateral basal ganglia calcifìcations and low density infarction in right parietal region (arrows) . b. T 1 weighted axial MR image shows high intensity calcifications in both basal ganglia and low intensity infarction in right thalamus and parieto-occipital parenchyma (arrows). c. T2 weighted ax ial MR image shows high intensity in right thalamus and parieto-occipital parenchyma d. Gd-enhanced T 1 weighted MR image shows linear enhancement at leptomeninges of the right parieto-occipital lesion (arrows)
- 161 -

Journal 01 Korean Radiological Society 1993; 29 (1) 160~ 164
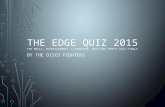
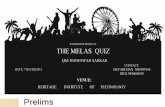
Fig.2. Elect ron microscopic findi맨s of muscle biopsy . An at rophi c fiber shows proliferative dysmorphic mitochondria in the subsarcolemmal and interfibrill ary space ( O ~4000)
and focal high signal intensities in both basal
ganglia (Fig. 1 b) ‘ T2-weighted image (T2WI) revealed high signal intensity in right parieto
occipital and thalamic lesions (Fig. 1c). However
bilateral basal ganglia lesions were not definite
ly identified in T2WI. Gd-enhanced T1 WI
revealed definite linear enhancement w i.thin the
right pa rieto-occipital lesi.on (Fig . 1d) . High
signal intesities in the both basal ganglia on
T1 WI corresponded to the areas of calcifications
on brain CT
Electron microscopic findings of muscle biopsy
specimen included an atroph ic fiber with heavy
accumulation of dysmorph ic mitochondria in the
subsarcolemmal and interfïbrillary spaces and
abnormal arrangem ent of cirstae and osmophilic inclusions in the highly polymorphic mitochon
dria (Fig . 2)
DISCUSSION
Mitochondrial encephalopathies are rare
diseases caused by a disturbance of the mitochon
drial chain of respiration. This prevents pyru、mte
from being completely in tegrated into the tricar
boxylic acid ( Kreb ’ s) cycle , and hence there is
an accum ulat ion of lactate. The clinical pattern ca n vary great ly and ran ges from
ophthalmoplegia via m ainly m yopathic to
encephalopathic froms. The patterns of signs and
symptoms enable subcl assification into three main syndromes. Three ofthem are the K earns
Sayre syndrome (KKS , defined by the invariant
triad:onset before age 20 , ophthalmoplegia , and
pigmentary retin얘athy) , MERRF (characteriz
ed by cerebellar ataxia and myoclonus) , and
MELAS (1). Pavlakis et al. have recently
described the syndrome of MELAS since Luft
introduced the concept of mitochondrial m yopathies with multiorgan involvement . The
classic clinical findings of MELAS were
myopathy , short stature, seizures, hemiparesis , hemianopsia , cortical blindness, and migrane
like h eadache (1 ,2). Our p a ti ent a ls o
demonstrated early normal development , m yopathy , short stature , stroke with
hemiparesis , and headache
Histologically, mitochondrial myopathies are
characterized by “ ragged red fibers " which were
pathologic accumulation of mitochondria on light
microscope with Gomori trichrom e stain
modified by Engel and Cunningham and ultrast ructural mitochondrial disorders , such as
megaconial (enlarged mitochondria with
disoriented cristae) and pleoconial (proJiferation of normal-looking mitochondria) myopathy on
elect ron microscope which was explored
system atically by Shy .and Gonatas (1 ,3). Our
case was also confirmed by showing structural morphological abnormalities of mitochondria in tissue from muscle biopsy on both light and electron mlcroscope.
The CT findings of mitochondrial myopathies
included focallow density lesions , basal ganglia
calcification , ventriculomegaly and cortical atrophy . Many other reported cases also revealed
bilaterallow density lesions in temporo-parieto
occipital areas with or without basal ganglia
calcifications especially in patients with MELAS
(2 ,3,4). In our patient , initial CT showed no
significant abnormalities , but CT obtained 2
years later revealed lower density lesion in right
parietooccipital regions and bilateral basal
- 162 -

Hye Young Choi , et al : MEALS Syndrome in a Child
ganglia calcifications which did not correspond clude that early detection of CNS abnormalities
to vascular territories ‘ Angiographic findings of by MRI is important for treatment of the pa-
MELAS were focal areas of capillary blush a nd tients with mitochondrial myopathies
early venous filling in the regions oflow density
seen on CT which did not correspond to vascular
territories (5). MRI fíndings in our patient were
consistent with CT findings , but ìv1RI wa.s more
sensitive and nicely demonstrated the lesions in
the right thalamic and parieto-occipital areas and
bilater외 basal gna빙ia abnormality. The thalamic
Jesion was detected on1y by MR I. These findings
are compatible with other recent reports on MRI
findings of mitochondria1 myopathies: one case
with mu1tiple migrating infarcts in posterior tem
por띠, parietal and occipital regions without basal
ganglia calcificat ion (6) and anoth er with high
signal intensity ofbasal gangli a calcification (7)
The pathogenesis of these manifestations of cen
tral nervous system (CNS) still remains unclear
According to OJdendorf et al (8) , CNS capillaries
have more abundant mitochondria compared
with those of other or!la ns. It mav be assumed 。 J
tha t CNS cap illaries and blood-brain barriers
might be especiaJJy vuJnerable to mitochondrial
dysfunction. Pavlakis et al (4). have specuJated
that mitochondrial dysfunction inv01ving the en
dOlheliu m of brain capillaJ‘ ies may cont ribute to
the deve10pment of stroke-like events. T he
neuropathological characteristics of these syn
dromes are spongy degeneration with microcystic
liguefaction and vascular proliferation , neu ronal
10ss , and demyelination, but microcystic liguefac
tion or focal softening and basal ganglia calcifica
tions are most prominent În MELAS (1,4)
The course of MELAS is variably progressive , punctuated by acute cerebral insults. We con-
REFERENCES
1. DiMauro S, Bonilla E , Lombes A , Shanske S, Min etti C , Moraes CT. Mitochondrial encephalom yo pathies . Ne llrologic Clinics 1990;8 :483-506
2. Myu댄 HJ , KimJS , Seo YL , C hiJG. MELAS syndrome (A Case report). The Seolll JOllmal of ~↑ edicine 1988;29 :315-322
3. Di~’ allro S, Bonilla E , Zeviani M , Nakagawa M , DeVivo DC. Mithochondrial myopathies Ann Neurol 1985; 17: 521 -538
4. Pavlakis S, Ph illips PC , DiMallro S, DeVivo DC , Rowland LP . Mitochondrial myopathy, encephalopathy, lactic acidosis , and strokelike episodes: A distinctive llinical syndrome. Ann Neurol 1984; 16:48 1-488
5. Hasup K , T am ura S, Yasllmori K et al. Com pllted tomography and angiography in MELAS (mitochondrial myopathy , encephalopathy, lartic ac idosis , and stro ke-Iike ep isode) ‘ report 01'
3 cases. Neuroradiology 1987;29:393-397 6. Rosen L, Phillips S, Enzmann D. Magnetic
resonance imag lD g in MELAS syndrome. Nellroradioiogy 1990 ;32: 168-171
7. Henkelman RM , 씨'atts JF , Kllcharczyk W. High signal intens ity in MR images of calcified brain tissue. Radiology 1991; 1 79: 199-206
8. OldendorfWH , Cornford ME , Brown WJ. The large apparent work capability of the blood-brain barrier:a st:lldy of the mitochondrial contcnt of capillary endothelial cells in brain and other ti sslles ofthe ra t. Ann. NeuroJ. 1977 ;1: 409-417
m …

Journal of Korean Radiological Society 1993; 29 ( 1 ) 160~ 164
〈국문 요약〉
소아에서 MELAS 증후군의 CT와 MR소견
울산대학교 의과대학 진단방사선과학교실, 소아과학교실 * 병리학교실**
최혜영 • 홍수종* . 조정희** . 서대철 • 홍창의*
MELAS 증후군은 미토콘드리아의 이상에 의해서 여러 장기가 침범되어 다양한 증상을 야기하는 드문 질환이다.
MELAS 증후군의 진단은 특징적인 여러 임상증상과 더불어 근육생검에서 특이한 “ ragged red fibers"와 비정상적
인 미토콘드리아가 보여야 가능한 것으로 되어있다.
저자들도 8세된 남아가 MELAS시 보일 수 있는 여러 임상증상과 더불어 특정적인 병리학적 소견을 나타내면서
CT와 MR에서도 특징적인 소견인 양측 기저핵의 석회화 병변 및 두정후두부와 시상에 경색 소견을 나타내는 것을
경험하였으며 특히 MR이 CT보다 더 확실하고 예민하게 명변의 위치와 범위를 보여주는 것을 알 수 있었다.
MELAS시 MRI로 두부병변을 빨리 알아내는 것은 치료의 결정과 환자의 예후를 예견하는데 중요하다고 생각한
다.
- 164 -