
Left Atrial Remodeling and Response to Valsartan in the...
13
Left Atrial Remodeling and Response to Valsartan in the Prevention of Recurrent Atrial Fibrillation The GISSI-AF Echocardiographic Substudy Lidia Staszewsky, MD; Maylene Wong, MD; Serge Masson, PhD; Elena Raimondi, MSc; Silvana Gramenzi, MD; Gianni Proietti, MD; Dario Bicego, MD; Carlo Emanuelli, MD; Giancarlo Pulitano `, MD; Filippo Taddei, MD; Enrico B. Nicolis, MSc; Ernesto Correale, MD; Gianna Fabbri, MD; Federico Bertocchi, MD; Maria Grazia Franzosi, BiolD; Aldo P. Maggioni, MD; Gianni Tognoni, MD; Marcello Disertori, MD; Roberto Latini, MD; on behalf of GISSI-AF Investigators* Background—Left atrial (LA) dilation precedes or appears early after the onset of atrial fibrillation (AF) and factors in perpetuating the arrhythmia. Angiotensin receptor blockers were proposed for reversing LA remodeling. We evaluated the effect of valsartan on LA remodeling in patients with a recent episode of AF and the effect of LA size on AF recurrence (AFr). Methods and Results—LA and left ventricular (LV) echocardiographic variables were measured at baseline and 6 and 12 months in 340 patients from GISSI-AF, a trial testing valsartan prevention of AFr. Reversal of remodeling was considered as a decrease in LA size over 12 months. Changes in patients with and without recurrence and the relationship to duration of AFr were analyzed. Patients were 68.48.8 years old, with history of hypertension (85.3%) and cardioversion in the previous 2 weeks (87.4%) or 2 AFr in the previous 6 months (40.4%). Baseline LA maximal volume (LAVmax) was severely increased (40 mL/m 2 ); LV dimensions and function were relatively normal. Over 12 months, 54.4% of patients had AFr. LAVmax was unchanged by rhythm, time, or randomized treatment. Higher baseline LAVmax and lower LA emptying fraction were linearly related to increasing AFr duration during follow-up. Conclusions—GISSI-AF patients in sinus rhythm and history of AF showed severely increased LAVmax with mostly normal LV volume, mass, and systolic and diastolic function. Valsartan for 1 year did not reverse LA remodeling or prevent AFr. Half of the patients without AFr had severe LA dilation; therefore, mechanisms other than structural remodeling triggered recurrence. Clinical Trial Registration—URL: http://www.clinicaltrials.gov. Unique identifier: NCT00376272. (Circ Cardiovasc Imaging. 2011;4:721-728.) Key Words: atrial fibrillation remodeling left atrium echocardiography clinical trial angiotensin receptor antagonists T he hypothesis that long-term renin-angiotensin system (RAS) inhibition could reverse the left atrial (LA) remodeling process and thereby contribute to the prevention of atrial fibrillation recurrence (AFr) was formally tested in the double-blind, randomized, Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto Miocardico–Atrial Fibrilla- tion (GISSI-AF) trial. 1,2 The entirely neutral results of the study were somewhat surprising, 3 given the wealth of positive evidence. Data from experimental AF implicated RAS in the remodeling associated with atrial electric heterogeneity, ab- Received March 7, 2011; accepted August 9, 2011. From the Department of Cardiovascular Research, Istituto di Ricerche Farmacologiche “Mario Negri,” Milan, Italy (L.S., M.W., S.M., E.R., E.B.N., M.G.F., R.L.); Ospedale Fatebenefratelli e Oftalmico, Division of Cardiology, Milan, Italy (S.G.); Azienda USL 4, Cardiology Unit, Terni, Italy (G. Proietti); Ospedale Nuovo Girolamo Fracastoro, Cardiology Unit, San Bonifacio, Italy (D.B.); the Division of Cardiology, Presidio Ospedaliero di Cremona, Italy (C.E.); POL Madonna della Consolazione, Reggio Calabria, Italy (G. Pulitanò); Ospedale Riuniti, Cardiology Unit, Cardiovascular Department, Bergamo, Italy (F.T.); Azienda Ospedaliera Sant’Anna e San Sebastiano, Cardiology Unit, Caserta, Italy (E.C.); ANMCO Research Center, Florence, Italy (G.F., A.P.M.); Novartis Italy SpA, Origgio, Italy (F.B.); Consorzio Mario Negri Sud, Chieti, Italy (G.T.); and the Department of Cardiology, Ospedale Santa Chiara, Trento, Italy (M.D.). *A complete list of the investigators who participated in the echocardiographic substudy is presented in the Appendix in the online-only Data Supplement. This work was presented in part at the Scientific Sessions of the American Heart Association (Circulation. 2009;120:S385 and Circulation. 2010;122:A14269). The online-only Data Supplement is available at http://circimaging.ahajournals.org/lookup/suppl/doi:10.1161/CIRCIMAGING.111.965954/-/DC1. Correspondence to Lidia Staszewsky, MD, Department of Cardiovascular Research, Istituto “Mario Negri,” Via Giuseppe La Masa 19, 20156 Milan, Italy. E-mail [email protected] © 2011 American Heart Association, Inc. Circ Cardiovasc Imaging is available at http://circimaging.ahajournals.org DOI: 10.1161/CIRCIMAGING.111.965954 721 by guest on May 30, 2018 http://circimaging.ahajournals.org/ Downloaded from by guest on May 30, 2018 http://circimaging.ahajournals.org/ Downloaded from by guest on May 30, 2018 http://circimaging.ahajournals.org/ Downloaded from by guest on May 30, 2018 http://circimaging.ahajournals.org/ Downloaded from by guest on May 30, 2018 http://circimaging.ahajournals.org/ Downloaded from by guest on May 30, 2018 http://circimaging.ahajournals.org/ Downloaded from
-
Upload
trinhxuyen -
Category
Documents
-
view
216 -
download
2
Transcript of Left Atrial Remodeling and Response to Valsartan in the...

Left Atrial Remodeling and Response to Valsartan in thePrevention of Recurrent Atrial Fibrillation
The GISSI-AF Echocardiographic Substudy
Lidia Staszewsky, MD; Maylene Wong, MD; Serge Masson, PhD; Elena Raimondi, MSc;Silvana Gramenzi, MD; Gianni Proietti, MD; Dario Bicego, MD; Carlo Emanuelli, MD;
Giancarlo Pulitano, MD; Filippo Taddei, MD; Enrico B. Nicolis, MSc; Ernesto Correale, MD;Gianna Fabbri, MD; Federico Bertocchi, MD; Maria Grazia Franzosi, BiolD; Aldo P. Maggioni, MD;Gianni Tognoni, MD; Marcello Disertori, MD; Roberto Latini, MD; on behalf of GISSI-AF Investigators*
Background—Left atrial (LA) dilation precedes or appears early after the onset of atrial fibrillation (AF) and factors inperpetuating the arrhythmia. Angiotensin receptor blockers were proposed for reversing LA remodeling. We evaluatedthe effect of valsartan on LA remodeling in patients with a recent episode of AF and the effect of LA size on AFrecurrence (AFr).
Methods and Results—LA and left ventricular (LV) echocardiographic variables were measured at baseline and 6 and 12months in 340 patients from GISSI-AF, a trial testing valsartan prevention of AFr. Reversal of remodeling wasconsidered as a decrease in LA size over 12 months. Changes in patients with and without recurrence and therelationship to duration of AFr were analyzed. Patients were 68.4�8.8 years old, with history of hypertension (85.3%)and cardioversion in the previous 2 weeks (87.4%) or �2 AFr in the previous 6 months (40.4%). Baseline LA maximalvolume (LAVmax) was severely increased (�40 mL/m2); LV dimensions and function were relatively normal. Over 12months, 54.4% of patients had AFr. LAVmax was unchanged by rhythm, time, or randomized treatment. Higherbaseline LAVmax and lower LA emptying fraction were linearly related to increasing AFr duration during follow-up.
Conclusions—GISSI-AF patients in sinus rhythm and history of AF showed severely increased LAVmax with mostlynormal LV volume, mass, and systolic and diastolic function. Valsartan for 1 year did not reverse LA remodeling orprevent AFr. Half of the patients without AFr had severe LA dilation; therefore, mechanisms other than structuralremodeling triggered recurrence.
Clinical Trial Registration—URL: http://www.clinicaltrials.gov. Unique identifier: NCT00376272.(Circ Cardiovasc Imaging. 2011;4:721-728.)
Key Words: atrial fibrillation � remodeling � left atrium � echocardiography � clinical trial� angiotensin receptor antagonists
The hypothesis that long-term renin-angiotensin system(RAS) inhibition could reverse the left atrial (LA)
remodeling process and thereby contribute to the preventionof atrial fibrillation recurrence (AFr) was formally tested inthe double-blind, randomized, Gruppo Italiano per lo Studio
della Sopravvivenza nell’Infarto Miocardico–Atrial Fibrilla-tion (GISSI-AF) trial.1,2 The entirely neutral results of thestudy were somewhat surprising,3 given the wealth of positiveevidence. Data from experimental AF implicated RAS in theremodeling associated with atrial electric heterogeneity, ab-
Received March 7, 2011; accepted August 9, 2011.From the Department of Cardiovascular Research, Istituto di Ricerche Farmacologiche “Mario Negri,” Milan, Italy (L.S., M.W., S.M., E.R., E.B.N.,
M.G.F., R.L.); Ospedale Fatebenefratelli e Oftalmico, Division of Cardiology, Milan, Italy (S.G.); Azienda USL 4, Cardiology Unit, Terni, Italy (G.Proietti); Ospedale Nuovo Girolamo Fracastoro, Cardiology Unit, San Bonifacio, Italy (D.B.); the Division of Cardiology, Presidio Ospedaliero diCremona, Italy (C.E.); POL Madonna della Consolazione, Reggio Calabria, Italy (G. Pulitanò); Ospedale Riuniti, Cardiology Unit, CardiovascularDepartment, Bergamo, Italy (F.T.); Azienda Ospedaliera Sant’Anna e San Sebastiano, Cardiology Unit, Caserta, Italy (E.C.); ANMCO Research Center,Florence, Italy (G.F., A.P.M.); Novartis Italy SpA, Origgio, Italy (F.B.); Consorzio Mario Negri Sud, Chieti, Italy (G.T.); and the Department ofCardiology, Ospedale Santa Chiara, Trento, Italy (M.D.).
*A complete list of the investigators who participated in the echocardiographic substudy is presented in the Appendix in the online-only DataSupplement.
This work was presented in part at the Scientific Sessions of the American Heart Association (Circulation. 2009;120:S385 and Circulation.2010;122:A14269).
The online-only Data Supplement is available at http://circimaging.ahajournals.org/lookup/suppl/doi:10.1161/CIRCIMAGING.111.965954/-/DC1.Correspondence to Lidia Staszewsky, MD, Department of Cardiovascular Research, Istituto “Mario Negri,” Via Giuseppe La Masa 19, 20156 Milan,
Italy. E-mail [email protected]© 2011 American Heart Association, Inc.
Circ Cardiovasc Imaging is available at http://circimaging.ahajournals.org DOI: 10.1161/CIRCIMAGING.111.965954
721
by guest on May 30, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from
by guest on May 30, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from
by guest on May 30, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from
by guest on May 30, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from
by guest on May 30, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from
by guest on May 30, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from

normal conduction, atrial hypertrophy and interstitial fibro-sis.4,5 In contrast, RAS inhibitors attenuated the progressionof atrial fibrosis, shortened AF duration, and improved LAfunction.6–8 Molecular studies of atrial samples in patientswith persistent AF showed upregulated angiotensin-converting enzyme (ACE) and angiotensin II receptors thatpromoted structural and electric remodeling of the atrium.9
Clinical Perspective on p 728Post hoc analyses of clinical trials in patients with left
ventricular dysfunction showed that ACE inhibitors andangiotensin receptor blockers (ARBs) reduced the onset ofnew AF,10,11 and, in prospective studies of patients aftercardioversion of paroxysmal and persistent AF, RASinhibitors in addition to amiodarone prevented recurrencesof AF.12
We report the results from the GISSI-AF echo study thatexplored whether the expected effect of valsartan to reverseLA remodeling would prevent AF recurrences. In addition,left atrial volume (LAV) and LV anatomy and functionwere assessed to estimate left ventricular resistance to LAemptying.
MethodsThe GISSI-AF trial was a double-blind, randomized, placebo-controlled, multicenter study that enrolled 1442 patients in sinusrhythm with a history of AF to test whether the ARB valsartan couldreduce the recurrence of AF (see Expanded Methods, Patients inthe GISSI-AF Main Study, in the online-only Data Supplement). Theprimary end points were time to the first recurrence of AF andthe proportion of patients who had more than 1 episode of AF overthe 1-year observation period.
In the echocardiographic substudy, 340 patients (24% of theGISSI-AF population) were enrolled at 33 sites that were qualifiedby the central core laboratory to record echocardiograms accordingto a prespecified protocol (see Echocardiography section in theonline-only Data Supplement). The study was approved by institu-tional review committees, and subjects gave informed consent.
Heart rate and blood pressure (BP) were measured before per-forming the echo exams. The recordings were acquired on CD orvideotape and sent to the core laboratory for centralized reading withMedimatic software (Genova, Italy).
Centralized ReadingMeasurements were repeated (3 times for sinus rhythm, 5 times forAF) and followed the American and European Societies of Echocar-diography recommendations.13 Atrial and ventricular chamber di-mensions were indexed by body surface area. Because LA volumescalculated from the apical 2- and 4-chamber views (2APCH,4APCH) resulted in similar values,14 the reported LA volumes weremeasured from only 4APCH view, which was also the mostconsistently recorded and produced the most complete serial record-ings. The within-reader reproducibility for left atrial maximal vol-ume (LAVmax) was analyzed from the difference between duplicatemeasurements versus the mean measurement for each and calculatedas the limits of agreement (mean difference �1.96 times SD).Reproducibility was also estimated from the measurement error aswithin-subject SD, expressed as repeatability (2.77 times measure-ment error).15 Data from 50 randomly selected patients showedreproducibility for LAVmax as �0.03�1.98 mL and repeatability as3.95 mL.
Detection of AF RecurrenceAF recurrence was detected by the transtelephonic transmission ofECG signals sent weekly, during symptomatic episodes, and duringthe follow-up visits to the primary physician and to the Coordinating
Center. Each event was adjudicated blindly by a central reader andwas verified by an ad hoc committee.2
Statistical MethodsThe effects of treatments were analyzed according to intention totreat. Continuous variables are expressed as mean�SD or as medians[Q1-Q3] when required. Categorical variables are reported as abso-lute numbers and percentages. Differences between treatment groupsin baseline characteristics were assessed by t test for continuousvariables and by �2 test for categorical variables. Variables associ-ated with time to first recurrence of AF were identified byunivariate analysis and multivariable Cox proportional hazardsmodels. The covariates age, sex, �2 episodes of AF in the 6 monthsbefore enrollment, and successful cardioversion in the 2 weeksbefore randomization were considered in the multivariable models.The prognostic value of each echocardiographic variable was eval-uated separately. Changes of echocardiographic variables frombaseline to 12-month follow-up were normally distributed; thereforeanalysis of covariance (ANCOVA) was used to evaluate differencesin changes between valsartan and placebo groups after adjustmentfor their respective baseline values. For left atrial minimum volume(LAVmin) index and left atrial emptying fraction (LAEF), the modelwas further adjusted for LAVmax index, entered as a continuousvariable.
LA volumes showed a nonnormal distribution, therefore a logtransformation was applied.
Within-patient changes in LA volumes and LAEF over time forpatients with and without AFr were compared by means of arepeated-measures ANOVA (“proc mixed”), in which AFr wasconsidered according to its time of recurrence (0–6 months and�6–12 months). The total duration of AFr over 1 year was obtainedby summing the number of days of each episode for each patient. Acategorical variable was entered by tertiles of days of AF duration forpatients with AFr and a separate category for patients without AFr.
The association between LA volumes at baseline and at 12 monthswith the total duration of AFr were evaluated by means of ANOVA,testing for trend across tertiles whenever statistically significantassociations emerged. Differences in LA volumes and LAEF asleast-squares means from baseline to 12 months by categories ofduration of AF, adjusted for their respective baseline value, weretested using ANCOVA.
To determine the variables independently related to LAVmax �40mL/m2, univariate and multivariable stepwise logistic regressionanalyses were performed, adjusting for �2 episodes of AF in theprevious 6 months, cardioversion in previous 2 weeks from random-ization, and duration of last qualifying episode of AF �7 days; heartfailure, left ventricular ejection fraction (LVEF) �40%, or both;anticoagulants, amiodarone, statins, and aspirin as concomitanttreatments; ECG LV hypertrophy; and hemoglobin.
All probability values were 2-tailed, and a value of �0.05 wasconsidered statistically significant. The statistical analyses were donewith SAS software (version 9.1).
Sample SizeThe sample size calculation for the quantitative outcome was basedon an expected absolute reduction of LAVmax of at least 6.7�20 mL(mean�SD) between valsartan and placebo groups at 12 months.The number of patients per group required to have a power of 80%with a 2-sided � error equal to 0.05, assuming a dropout rate of 30%(due to inadequate quality of echocardiograms and /or missingexaminations), was calculated to be 200.2
ResultsPatient DataThe mean age of the 340 patients studied at baseline was68.4�8.8 years (�SD), 36.2% were women, and 85.3% hadbeen hypertensive for �6 months. The date of the firstepisode of AF in the patients clinical history was known in262 of 340 (77%) of the subjects, and the median time
722 Circ Cardiovasc Imaging November 2011
by guest on May 30, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from
between the onset of the arrhythmia to random assignmentwas 12 months (range, 6 days to 31 years). At least 2 episodesof AF in the previous 6 months were experienced by 40.4%of the patients, 87.4% were cardioverted in the previous 2weeks, and in 39.7% the duration of the last episode was �7days. There were no differences in baseline characteristics ofthe patients randomly assigned to valsartan or to placebo(Table 1), except for the more common history of stroke in
Table 1. Baseline Clinical and ECG Characteristics
CharacteristicsValsartan(n�171)
Placebo(n�169)
Age, y 68.1�8.8 68.6�8.8
Female, n (%) 68 (39.8) 55 (32.5)
Body mass index, kg/m2 28.0�4.1 27.5�4.2
Blood pressure, mm Hg
Systolic 136.4�15.3 139.6�16.9
Diastolic 81.1�8.1 81.2�8.5
Inclusion criteria, n (%)
�2 episodes of AF in previous 6 mo 70 (41.2) 66 (39.5)
Cardioversion in previous 2 wk 151 (88.3) 146 (86.4)
Duration of last qualifying episodeof AF �7 d
66 (38.6) 69 (40.8)
Heart failure, LVEF �40%, or both 18 (10.5) 18 (10.7)
History of hypertension for 6 mo or more 144 (84.2) 146 (86.4)
Diabetes mellitus 22 (12.9) 27 (16.0)
History of stroke 11 (6.4) 3 (1.8)
Peripheral artery disease 14 (8.2) 7 (4.1)
Documented coronary artery disease 23 (13.5) 15 (8.9)
AF alone 23 (13.5) 24 (14.2)
Coexisting conditions, n (%)
Peripheral embolism 3 (1.8) 3 (1.8)
Previous transient ischemic attack 11 (6.4) 3 (1.8)
Renal dysfunction 5 (2.9) 5 (3.0)
Chronic obstructive pulmonary disease 15 (8.8) 18 (10.7)
Neoplasia 5 (2.9) 6 (3.6)
Current smoker 12 (7.0) 18 (10.7)
ECG findings at random assignment
Heart rate, bpm 62.1�10.2 62.1�9.5
QRS interval �120 ms, n (%) 18 (10.5) 22 (13.0)
Left ventricular hypertrophy, n (%) 20 (11.7) 15 (8.9)
Pathological Q waves, n (%) 5 (2.9) 5 (3.0)
Concomitant cardiovascular therapies, n (%)
Amiodarone 69 (40.4) 60 (35.5)
Sotalol 11 (6.4) 14 (8.3)
Class I antiarrhythmic agents 60 (35.1) 56 (33.1)
ACE inhibitors 87 (50.9) 86 (50.9)
Calcium channel blockers 49 (28.7) 53 (31.4)
�-Blockers 50 (29.2) 42 (24.9)
Digitalis 10 (5.9) 7 (4.1)
Diuretics 68 (39.8) 59 (34.9)
Aldosterone blockers 11 (6.4) 12 (7.1)
Statins 50 (29.2) 40 (23.7)
Oral anticoagulants 102 (59.7) 104 (61.5)
Aspirin 42 (24.6) 46 (27.2)
AF indicates atrial fibrillation; LVEF, left ventricular ejection fraction; andACE, angiotensin-converting enzyme.
Table 2. Echocardiographic Variables at Baseline and 12Months (n�286 Patients)
Baseline 12 Months Change Treatment*
SBP, mm Hg 0.97
Valsartan 137�16 137�18 �0.4�1.4
Placebo 140�18 139�19 �0.5�1.4
DBP, mm Hg 0.26
Valsartan 81�9 80�9 �1.1�0.7
Placebo 82�9 82�9 0.0�0.7
Heart rate, bpm 0.94
Valsartan 64�10 65�11 1.3�0.9
Placebo 63�10 65�12 1.1�0.9
LAVmax/BSA, mL/m2 0.58
Valsartan 42.6�15.5 42.2�14.7 �0.7�0.8
Placebo 41.9�14.6 41.4�14.5 �0.1�0.8
LAVmin/BSA, mL/m2 0.34
Valsartan 23.4�12.9 22.4�12.6 �1.0�0.7
Placebo 22.5�11.6 20.6�10.9 �2.0�0.7
LAEF, % 0.16
Valsartan 47.7�13.5 50.5�13.0 2.3�0.9
Placebo 47.9�12.6 51.7�12.4 4.1�0.9
LVTH, mm 0.33
Valsartan 11.0�1.5 10.9�1.4 0.0�0.1
Placebo 10.7�1.4 10.6�1.6 �0.2�0.1
LVmass/BSA, g/m2 0.96
Valsartan 81.3�17.9 80.0�16.9 �1.6�1.2
Placebo 78.3�16.6 75.7�17.7 �1.6�1.2
LVEDV/BSA, mL/m2 0.20
Valsartan 52.8�16.9 52.3�15.0 �0.6�0.8
Placebo 52.6�14.5 52.8�14.9 0.8�0.8
LVESV/BSA, mL/m2 0.14
Valsartan 22.4�13.3 20.6�12.1 �1.8�0.6
Placebo 21.4�12.1 21.1�11.1 �0.6�0.5
LVEF, % 0.19
Valsartan 59.6�12.7 62.2�12.0 2.4�0.7
Placebo 60.5�12.3 61.5�11.3 1.2�0.7
E/A 0.09
Valsartan 1.3�0.8 1.2�0.8 0.0�0.1
Placebo 1.3�0.8 1.1�0.6 �0.2�0.1
DT, ms 0.21
Valsartan 194�56.0 194�57.0 �3.4�4.8
Placebo 202�60.0 204�56.0 5.1�4.7
IVRT, ms 0.23
Valsartan 87�22.0 87�24.0 �2.1�2.2
Placebo 88�22.0 90�24.0 1.7�2.3
E/e� 0.09
Valsartan 12.5�10.9 13.2�7.3 1.7�0.7
Placebo 12.2�5.3 11.8�5.2 0.0�0.7
HR indicates heart rate; SBP, systolic blood pressure; DBP, diastolic bloodpressure; LAVmax/BSA, left atrial maximal volume index; LAVmin/BSA, left atrialminimum volume index; LAEF, left atrial emptying fraction; LVTH, left ventricularwall thickness; LVEDV/BSA, left ventricular end diastolic volume index; LVESV/BSA,left ventricular end-systolic volume index; LVEF, left ventricular ejection fraction;E/A, early to late diastolic mitral inflow; DT, deceleration time; IVRT, isovolumetricrelaxation time; and E/e�, early diastolic mitral inflow velocity/early diastolic septalmitral annular relaxation velocity (available in 90/286 patients).
Data are mean�SD. Changes are least-squares mean�SEM.*ANCOVA used to evaluate differences in changes from baseline to
12-month follow-up between valsartan and placebo groups after adjustmentfor variables value at baseline.
Staszewsky et al LA Remodeling in AF and Valsartan 723
by guest on May 30, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from
the treatment group (P�0.03). Compared with the no-echocohort (n�1102), patients enrolled in the echocardiographicsubstudy had higher prevalence of heart failure, LVEF �40%or both; peripheral artery disease; peripheral embolism; weremore frequently current smokers; had higher heart rate; weremore likely to have a QRS �120 ms; and were less oftentreated with ACE inhibitors (see additional Table in theonline-only Data Supplement).
Echo DataAt baseline, mean LAVmax was severely increased:43.1�15.0 mL/m2 (normal LAVmax/BSA: �29 mL/ m2).LA minimal volume was moderately increased: 23.4�12.3mL/m2; and LAEF was slightly to moderately depressed:47.6�13.2%. LV end-systolic and end-diastolic volumes andejection fraction were within normal ranges, whereasmean�SD wall thickness was slightly increased (10.9�1.4 mm;normal for men: 6–10 mm) and LV mass was normal(81.2�17.7 g/m2; normal for men: 52–102 g/m2). Althoughthe mean values for Doppler mitral flow variables werenormal, 36% of patients showed abnormal E/A, 28% and48% with an abnormal DT and/or IVRT, respectively. In 128of 340 patients with both, peak mitral E velocities and tissueDoppler mitral annular velocities the mean septal E/e� was12.4�8.2 (normal: �8). Thirty-seven percent of patients hadmild mitral regurgitation, 15.0% moderate, 3% severe, and45% no regurgitation.
Echo Variables: Baseline and 12 Months byTreatment GroupNone of the echo variables were affected by valsartantreatment from baseline to 12 months (Table 2). These resultswere confirmed in a per-protocol analysis done in the 252patients (88%) who took the study drug for at least 80% daysof observation. The lack of effect of valsartan on LAVminand on LAEF over time was found to be independent ofbaseline atrial dilation (covariate LAVmax, ANCOVA:P�0.34 and 0.20, respectively).
To determine if LA volumes were influenced by thenumber of patients having recurrences of AF over time,patients in sinus rhythm at the end of the study (n�221) wereanalyzed separately and did not show any effect of treatmenton LA dimensions and function (data not shown).
AF RecurrencesAF recurred in 54% of the patients during the 1-yearfollow-up. AF recurrence was associated with a history of �2episodes of AF in the previous 6 months (P�0.0004). Themedian number of recurrences per patient was 2 [1–4], withan overall median duration of 19.5 [4–95] days over 12months. Half of the AF recurrences took place within the first2 months. Predictors of AFr were baseline LAVmin asincreases in 1 mL/m2 increments (hazard ratio, 1.02; 95%confidence interval [CI], 1.01–1.03; P�0.003) and LAEF, asdecreases in 1% units (hazard ratio, 1.02; 95% CI, 1.00–1.03;P�0.01).
Table 3. Time Course of Echocardiographic Variables According to the Time of First Recurrence of AF
Patients With No AFRecurrence (n�109)
Patients With AF Recurrence0–6 Months (n�115)
Patients With AF Recurrence�6–12 Months (n�32) P Value*
Baseline 6 Months 12 Months Baseline 6 Months 12 Months Baseline 6 Months 12 Months Time Time*AF Recurrence
LAVmax/BSA, mL/m2 40.7�12.3 41.8�13.0 40.5�13.6 44.7�15.8 44.3�15.2 44.2�14.5 38.3�13.3 38.7�11.6 37.5�13.3 0.42 0.78
LAVmin/BSA, mL/m2 21.3�10.3 20.2�9.9 19.8�10.6 25.8�13.3 23.7�13.0 23.9�12.0 19.4�9.0 19.0�7.7 18.5�10.8 0.04 0.67
LAEF, % 48.8�12.4 52.8�11.4 52.9�11.1 45.4�13.3 49.3�13.8 48.7�13.6 49.5�12.2 52.3�11.4 53.0�13.3 0.0001 0.83
AF indicates atrial fibrillation; LAVmax/BSA, left atrial maximal volume index; LAVmin/BSA, left atrial minimum volume index; and LAEF, left atrial emptying fraction.Data are mean�SD.*Repeated-measures ANOVA.
Table 4. Left Atrial Volumes and Emptying Fraction Relative to Duration of AF Recurrence
LAVmax/BSA, mL/m2 LAVmin/BSA, mL/m2 LAEF, %
Baseline 12 Months Baseline 12 Months Baseline 12 Months
No AF (n�113) 41.7�14.5 41.1�14.5 22.0�11.5 20.2�11.1 48.8�12.3 52.5�11.1
AF recurrence duration, d
Tertile 1: 1–6 (n�44) 35.4�14.0 35.7�14.4 17.2�9.6 17.0�9.8 53.9�12.3 54.9�11.6
Tertile 2: 7–58 (n�44) 44.0�15.8 44.1�14.8 24.3�13.2 22.2�12.2 47.2�12.8 52.9�11.1
Tertile 3: �59 (n�44) 49.7�14.2 48.5�13.1 31.0�13.0 29.6�12.4 40.1�13.5 41.6�14.1
ANOVA* �0.0001 �0.0001 �0.0001 �0.0001 �0.0001 �0.0001
Trend† �0.0001 0.0001 �0.0001 �0.0001 �0.0001 �0.0001
AF indicates atrial fibrillation; LAVmax/BSA, left atrial maximal volume index; LAVmin/BSA, left atrial minimum volume index; andLAEF, left atrial emptying fraction.
Data are mean�SD.*ANOVA P value.†Trend P value.
724 Circ Cardiovasc Imaging November 2011
by guest on May 30, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from
LA Volumes: With and Without AF RecurrencesLA volumes and LAEF according to rhythm and time aresummarized in Table 3 for combined treatment groups.Baseline and 6- and 12-month data were available in 256 of340 patients (75%). At baseline, patients without AFr andwith early AFr (0–6 months) had similar LAVmax that didnot change significantly over time. Patients with late AFr(�6–12 months) had smaller LAVmax compared with theother 2 groups, although differences were not statisticallysignificant. Patients with early AFr (0–6 months) tended tohave larger LAVmin and smaller LAEF than the other 2groups. Independent of AFr, LA function improved over 12months (more evident in the first 6 months), as shown by adecrease in LAVmin (P�0.04) and an increase in LAEF(P�0.0001).
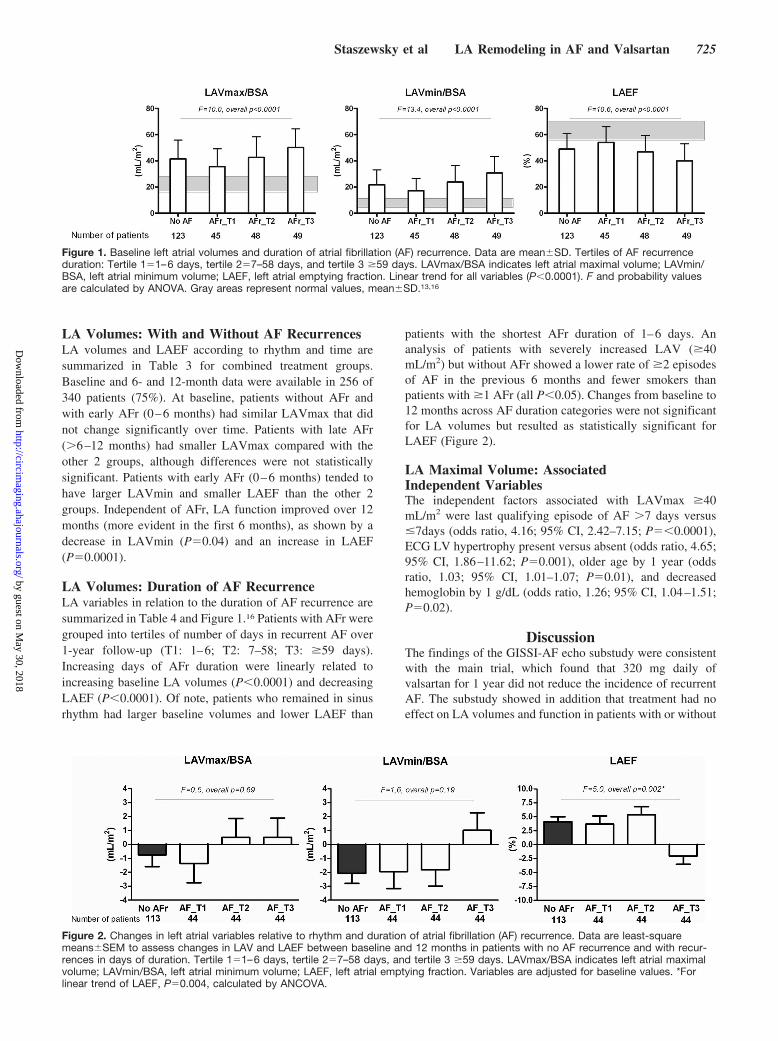
LA Volumes: Duration of AF RecurrenceLA variables in relation to the duration of AF recurrence aresummarized in Table 4 and Figure 1.16 Patients with AFr weregrouped into tertiles of number of days in recurrent AF over1-year follow-up (T1: 1–6; T2: 7–58; T3: �59 days).Increasing days of AFr duration were linearly related toincreasing baseline LA volumes (P�0.0001) and decreasingLAEF (P�0.0001). Of note, patients who remained in sinusrhythm had larger baseline volumes and lower LAEF than
patients with the shortest AFr duration of 1–6 days. Ananalysis of patients with severely increased LAV (�40mL/m2) but without AFr showed a lower rate of �2 episodesof AF in the previous 6 months and fewer smokers thanpatients with �1 AFr (all P�0.05). Changes from baseline to12 months across AF duration categories were not significantfor LA volumes but resulted as statistically significant forLAEF (Figure 2).
LA Maximal Volume: AssociatedIndependent VariablesThe independent factors associated with LAVmax �40mL/m2 were last qualifying episode of AF �7 days versus�7days (odds ratio, 4.16; 95% CI, 2.42–7.15; P��0.0001),ECG LV hypertrophy present versus absent (odds ratio, 4.65;95% CI, 1.86–11.62; P�0.001), older age by 1 year (oddsratio, 1.03; 95% CI, 1.01–1.07; P�0.01), and decreasedhemoglobin by 1 g/dL (odds ratio, 1.26; 95% CI, 1.04–1.51;P�0.02).
DiscussionThe findings of the GISSI-AF echo substudy were consistentwith the main trial, which found that 320 mg daily ofvalsartan for 1 year did not reduce the incidence of recurrentAF. The substudy showed in addition that treatment had noeffect on LA volumes and function in patients with or without
Figure 1. Baseline left atrial volumes and duration of atrial fibrillation (AF) recurrence. Data are mean�SD. Tertiles of AF recurrenceduration: Tertile 1�1–6 days, tertile 2�7–58 days, and tertile 3 �59 days. LAVmax/BSA indicates left atrial maximal volume; LAVmin/BSA, left atrial minimum volume; LAEF, left atrial emptying fraction. Linear trend for all variables (P�0.0001). F and probability valuesare calculated by ANOVA. Gray areas represent normal values, mean�SD.13,16
Figure 2. Changes in left atrial variables relative to rhythm and duration of atrial fibrillation (AF) recurrence. Data are least-squaremeans�SEM to assess changes in LAV and LAEF between baseline and 12 months in patients with no AF recurrence and with recur-rences in days of duration. Tertile 1�1–6 days, tertile 2�7–58 days, and tertile 3 �59 days. LAVmax/BSA indicates left atrial maximalvolume; LAVmin/BSA, left atrial minimum volume; LAEF, left atrial emptying fraction. Variables are adjusted for baseline values. *Forlinear trend of LAEF, P�0.004, calculated by ANCOVA.
Staszewsky et al LA Remodeling in AF and Valsartan 725
by guest on May 30, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from

AF recurrence. Earlier experimental evidence implicating theRAS in the LA remodeling process,4,5 and the reversal of thefibrosis and improvement in electric conduction and functionwith ARB and ACE inhibition,6–8 were supported by clinicalstudies that showed a significant reduction in recurrence ofAF.10–12 Why did ARB treatment fail to reverse LA remod-eling in GISSI-AF patients at high risk for AF recurrence withqualifying cardiovascular criteria?
The main trial revealed that of the 2 entry criteria, historyof AF and at least 1 cardiovascular condition, 85% had onlyhypertension for �6 months as the other criteria (Table 1).Thus, GISSI-AF patients were unlike those in successfulARB trials of preventing AF recurrence who were mainly inheart failure.11 Only 10% of our patients had a positivehistory of heart failure or LVEF of �40%. The echocardio-graphic results further substantiated the absence of overt LVdisease. LV ejection fraction was normal, as was LV end-di-astolic volume and mass and Doppler variables of LVdiastolic function. The only exceptions were the minimalincreases in LV wall thickness and in E/e� ratio. Therefore,this apparent normality in LV structure and function maypartly explain the lack of beneficial effects of the ARBvalsartan.
LA remodeling or dilation appears to progress over time,depending on the underlying cardiovascular disease17,18 or onthe arrhythmia itself.19 Although LA volume reflects anaverage effect of LV filling pressures over time,20,21 the LAvolumes were severely increased in the face of only minimalincrease in LV wall thickness. On further analysis, 25–48%of patients exceeded the normal range of Doppler diastolicmeasurements and specifically 25% recorded a septal E/e�ratio �15, a value associated with increased LV fillingpressures.22 Nevertheless, with the majority of patients dem-onstrating normal LV volumes, mass, and standard fillingvelocities, AF itself appears to be the dominant mechanismfor LA remodeling.19
What were the quantitative consequences of recurrent AFalone on LA dilation? LA volumes were severely dilated to amean of �40 mL/m2; however, the degree of dilation is notunheard of, and similar LA volumes have been reported insmall AF ablation studies.23 Further findings of severe LAdilation were that the volumes were unalterable not only toARB treatment but also unchangeable over time, independentof rhythm, intermittent sinus rhythm, and time to first AFr.Finally, with recurrent AF, the larger the LA volume, themore prolonged are the episodes of future AFr (Figure 2), achanging perspective on “AF begets AF through LA remod-eling.” The question this study raises: Is there LA remodelingbeyond which there is no reversibility and inevitable progres-sion of recurrent AF to chronic AF?
Perhaps of some encouragement, although LAVmax wasunchanged, LA function did respond during the 1 year bysignificantly increasing LAEF and decreasing LAVmin (Ta-ble 3). A possible explanation is that 87% of the patients hadbeen cardioverted within 2 weeks before random assignment.Parallel evidence from experimental AF demonstrated thatloss of atrial contractility after cardioversion is followed by apartial or full functional recovery even though the amount of
fibrosis persists.24,25 However, improvement in LA functionin our study was limited (Table 4 and Figure 2) and did notoccur in patients with the longest AFr duration of �59 days.The data again imply that there is a limit to LA dilationbeyond which the atrium is no longer responsive to apharmacological intervention or, less likely, that a longerexposure is necessary to achieve a therapeutic response.3Theneutral results with ARB treatment on atrial remodeling,independent of the severely dilated LAVmax at baseline,offer little optimism for a trial of more prolonged ARBtherapy.
The relation between LA volume and AF in patients withcardiovascular disease is complex, and few data are availableregarding LA dimensions measured over time in such pa-tients.26,27 The GISSI-AF patients were predominantly hyper-tensive with controlled BP (Table 2), and, because hyperten-sion is a significant risk factor for AF28 and predictor of LAsize,18 our results suggest that any BP in the presence ofrecurrent AF is too high and should be treated, a hypothesisyet to be tested.29 Prediction models showed that an increaseof 10 mm Hg in BP, increased the risk of AF independent ofage, sex, and ECG LV hypertrophy.30 Belluzzi et al31 crediblydemonstrated that targeting systolic BP between 130 and139 mm Hg with ramipril in patients with lone AF andnormal LA and LV structures reduced the risk of AFrecurrence. Initiating hypertensive treatment in patients withAF when systolic BP exceeds 120 mm Hg has been pro-posed,29 in particular with anti-RAS therapies.28–32 Besidesusing LA size as a target organ for the aggressive treatment ofBP in managing AF, the availability of newer drugs andprocedures will also have to prove their effectiveness. Mea-suring LAVs will be central to selecting patients, tailoringtreatment, and evaluating outcomes for this challengingrhythm.
ConclusionsIn our study population, mainly hypertensive with severelydilated left atria, valsartan treatment for 1 year had no effecton reversing LA remodeling. LAVmax did not vary over timein patients with and without AF recurrence and pointed outthat advanced atrial remodeling has a low probability ofreversal. The degree of remodeling at baseline was stronglyand linearly related to the duration of future AF recurrencesand possibly affected the time to the first AF recurrence.Patients without recurrence also had severely enlarged LAV-max (�40 mL/m2), indicating that mechanisms other thanstructural remodeling underlie recurring AF. Some of ourincidental findings called attention to specific factors in AFmechanisms that underscored the need for further research inunderstanding AF pathogenesis.
AcknowledgmentsWe thank all patients, nurses, and cardiologists who participated inthe echocardiographic GISSI-AF substudy; Maria Amigoni, MD, forher help in preparing the substudy proposal; Simona Barlera, MSc,Donata Lucci, MSc, and Chiara Favero, MSc, for statistical advice;and Alessandra Carnaghi for secretarial assistance.
726 Circ Cardiovasc Imaging November 2011
by guest on May 30, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from

Sources of FundingThe GISSI Studies as well as the present substudy are supported byAssociazione Nazionale Medici Cardiologi Ospedalieri (ANMCO)and by Istituto di Ricerche Farmacologiche Mario Negri. Fundingwas provided by Novartis, which had no role in the design or conductof the trial, the collection, analysis, or interpretation of the data, orthe writing of the report.
DisclosuresDrs Latini, Masson, Wong, Staszewsky, Maggioni, Franzosi, To-gnoni, and Disertori received institutional research support or hon-oraria from Novartis Pharma. Dr Bertocchi is an employee ofNovartis Italy SpA.
References1. GISSI-AF Investigators. Valsartan for prevention of recurrent atrial fibril-
lation. N Engl J Med. 2009;360:1606–1617.2. Disertori M, Latini R, Maggioni AP, Delise P, Di Pasquale G, Franzosi
MG, Staszewsky L, Tognoni G; GISSI-AF Investigators. Rationale anddesign of the GISSI-Atrial Fibrillation Trial: a randomized, prospective,multicentre study on the use of valsartan, an angiotensin II AT1-receptorblocker, in the prevention of atrial fibrillation recurrence. J CardiovascMed (Hagerstown). 2006;7:29–38.
3. Gillis AM. Angiotensin-receptor blockers for prevention of atrialfibrillation: a matter of timing or target? N Engl J Med. 2009;360:1669 –1671.
4. Meghji P, Nazir SA, Dick DJ, Bailey ME, Johnson KJ, Lab MJ. Regionalworkload induced changes in electrophysiology and immediate early geneexpression in intact in situ porcine heart. J Mol Cell Cardiol. 1997;29:3147–3155.
5. Li D, Fareh S, Leung TK, Nattel S. Promotion of atrial fibrillation byheart failure in dogs: atrial remodeling of a different sort. Circulation.1999;100:87–95.
6. Nakashima H, Kumagai K, Urata H, Gondo N, Ideishi M, Arakawa K.Angiotensin II antagonist prevents electrical remodeling in atrial fibril-lation. Circulation. 2000;101:2612–2617.
7. Shi Y, Li D, Tardif JC, Nattel S. Enalapril effects on atrial remodelingand atrial fibrillation in experimental congestive heart failure. CardiovascRes. 2002;54:456–461.
8. Li D, Shinagawa K, Pang L, Leung TK, Cardin S, Wang Z, Nattel S.Effects of angiotensin-converting enzyme inhibition on the devel-opment of the atrial fibrillation substrate in dogs with ventriculartachypacing-induced congestive heart failure. Circulation. 2001;104:2608 –2614.
9. Goette A, Arndt M, Rocken C, Spiess A, Staack T, Geller JC, Huth C,Ansorge S, Klein HU, Lendeckel U. Regulation of angiotensin II receptorsubtypes during atrial fibrillation in humans. Circulation. 2000;101:2678–2681.
10. Maggioni AP, Latini R, Carson PE, Singh SN, Barlera S, Glazer R,Masson S, Cere E, Tognoni G, Cohn JN; Val-HeFT Investigators. Val-sartan reduces the incidence of atrial fibrillation in patients with heartfailure: results from the Valsartan Heart Failure Trial (Val-HeFT). AmHeart J. 2005;149:548–557.
11. Schneider MP, Hua TA, Bohm M, Wachtell K, Kjeldsen SE, SchmiederRE. Prevention of atrial fibrillation by renin-angiotensin system inhibitiona meta-analysis. J Am Coll Cardiol. 2010;55:2299–2307.
12. Healey JS, Baranchuk A, Crystal E, Morillo CA, Garfinkle M, Yusuf S,Connolly SJ. Prevention of atrial fibrillation with angiotensin-convertingenzyme inhibitors and angiotensin receptor blockers: a meta-analysis.J Am Coll Cardiol. 2005;45:1832–1839.
13. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, PellikkaPA, Picard MH, Roman MJ, Seward J, Shanewise JS, Solomon SD,Spencer KT, Sutton MS, Stewart WJ; Chamber Quantification WritingGroup; American Society of Echocardiography’s Guidelines andStandards Committee; European Association of Echocardiography. Rec-ommendations for chamber quantification: a report from the AmericanSociety of Echocardiography’s Guidelines and Standards Committee andthe Chamber Quantification Writing Group, developed in conjunctionwith the European Association of Echocardiography, a branch of theEuropean Society of Cardiology. J Am Soc Echocardiogr. 2005;18:1440–1463.
14. Staszewsky L, Latini R, Wong M, Volpi, A, Barlera S, Nicolis E,Gramenzi S, Taddei F, Cioffi G, Bon S, Zeni P, Raimondi E, Franzosi
MG, Maggioni A, Tognoni G, Disertori M; on behalf of the GISSI-AFInvestigators. Transthoracic echocardiographic parameters as predictorsof atrial fibrillation recurrence: data from the GISSI-AF Echocardio-graphic Study [abstract]. Circulation. 2009;120:S385. Abstract.
15. Bland JM, Altman DG. Measurement error: Department of Public HealthSciences, St George’s Hospital Medical School, London. BMJ. 1996;313:744.
16. Kurt M, Wang J, Torre-Amione G, Nagueh SF. Left atrial function indiastolic heart failure. Circ Cardiovasc Imaging. 2009;2:10–15.
17. Casaclang-Verzosa G, Gersh BJ, Tsang TS. Structural and functionalremodeling of the left atrium: clinical and therapeutic implications foratrial fibrillation. J Am Coll Cardiol. 2008;51:1–11.
18. Abhayaratna WP, Seward JB, Appleton CP, Douglas PS, Oh JK, TajikAJ, Tsang TS. Left atrial size: physiologic determinants and clinicalapplications. J Am Coll Cardiol. 2006;47:2357–2363.
19. Wijffels MC, Kirchhof CJ, Dorland R, Allessie MA. Atrial fibrillationbegets atrial fibrillation: a study in awake chronically instrumented goats.Circulation. 1995;92:1954–1968.
20. Tsang TS, Barnes ME, Gersh BJ, Bailey KR, Seward JB. Left atrialvolume as a morphophysiologic expression of left ventricular diastolicdysfunction and relation to cardiovascular risk burden. Am J Cardiol.2002;90:1284–1289.
21. Douglas PS. The left atrium: a biomarker of chronic diastolic dys-function and cardiovascular disease risk. J Am Coll Cardiol. 2003;42:1206 –1207.
22. Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA,Waggoner AD, Flachskampf FA, Pellikka PA, Evangelista A. Recom-mendations for the evaluation of left ventricular diastolic function byechocardiography. J Am Soc Echocardiogr. 2009;22:107–133.
23. Jeevanantham V, Ntim W, Navaneethan SD, Shah S, Johnson AC, Hall B,Shah A, Hundley WG, Daubert JP, Fitzgerald D. Meta-analysis of theeffect of radiofrequency catheter ablation on left atrial size, volumes andfunction in patients with atrial fibrillation. Am J Cardiol. 2010;105:1317–1326.
24. Logan WF, Rowlands DJ, Howitt G, Holmes AM. Left atrial activityfollowing cardioversion. Lancet. 1965;2:471–473.
25. Allessie MA, Boyden PA, Camm AJ, Kleber AG, Lab MJ, Legato MJ,Rosen MR, Schwartz PJ, Spooner PM, Van Wagoner DR, Waldo AL.Pathophysiology and prevention of atrial fibrillation. Circulation. 2001;103:769–777.
26. Sanfilippo AJ, Abascal VM, Sheehan M, Oertel LB, Harrigan P, HughesRA, Weyman AE. Atrial enlargement as a consequence of atrial fibril-lation: a prospective echocardiographic study. Circulation. 1990;82:792–797.
27. Mattioli AV, Sansoni S, Lucchi GR, Mattioli G. Serial evaluation of leftatrial dimension after cardioversion for atrial fibrillation and relation toatrial function. Am J Cardiol. 2000;85:832–836.
28. European Heart Rhythm Association; European Association for Cardio-Thoracic Surgery, Camm AJ, Kirchhof P, Lip GY, Schotten U, SavelievaI, Ernst S, Van Gelder IC, Al-Attar N, Hindricks G, Prendergast B,Heidbuchel H, Alfieri O, Angelini A, Atar D, Colonna P, De Caterina R,De Sutter J, Goette A, Gorenek B, Heldal M, Hohloser SH, Kolh P, LeHeuzey JY, Ponikowski P, Rutten FH; ESC Committee for PracticeGuidelines, Vahanian A, Auricchio A, Bax J, Ceconi C, Dean V, Fil-ippatos G, Funck-Brentano C, Hobbs R, Kearney P, McDonagh T,Popescu BA, Reiner Z, Sechtem U, Sirnes PA, Tendera M, Vardas PE,Widimsky P; Document Reviewers, Vardas PE, Agladze V, Aliot E,Balabanski T, Blomstrom-Lundqvist C, Capucci A, Crijns H, Dahlof B,Folliguet T, Glikson M, Goethals M, Gulba DC, Ho SY, Klautz RJ, KoseS, McMurray J, Perrone Filardi P, Raatikainen P, Salvador MJ, SchalijMJ, Shpektor A, Sousa J, Stepinska J, Uuetoa H, Zamorano JL, Zupan I.Guidelines for the management of atrial fibrillation: the Task Force forthe Management of Atrial Fibrillation of the European Society of Car-diology (ESC). Europace. 2010;12:1360–1420.
29. Wachtell K. Atrial fibrillation, maybe it is not so lone? J Am Coll Cardiol.2009;53:30–31.
30. Wachtell K, Lehto M, Gerdts E, Olsen MH, Hornestam B, Dahlof B,Ibsen H, Julius S, Kjeldsen SE, Lindholm LH, Nieminen MS, DevereuxRB. Angiotensin II receptor blockade reduces new-onset atrial fibrillationand subsequent stroke compared to atenolol: the Losartan InterventionFor End Point Reduction in Hypertension (LIFE) study. J Am CollCardiol. 2005;45:712–719.
31. Belluzzi F, Sernesi L, Preti P, Salinaro F, Fonte ML, Perlini S. Preventionof recurrent lone atrial fibrillation by the angiotensin-II converting
Staszewsky et al LA Remodeling in AF and Valsartan 727
by guest on May 30, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from

enzyme inhibitor ramipril in normotensive patients. J Am Coll Cardiol.2009;53:24–29.
32. Kirchhof P, Bax J, Blomstrom-Lundquist C, Calkins H, Camm AJ,Cappato R, Cosio F, Crijns H, Diener HC, Goette A, Israel CW, KuckKH, Lip GY, Nattel S, Page RL, Ravens U, Schotten U, Steinbeck G,
Vardas P, Waldo A, Wegscheider K, Willems S, Breithardt G. Earlyand comprehensive management of atrial fibrillation: executivesummary of the proceedings from the II AFNET-EHRA consensusconference ‘research perspectives in AF.’ Eur Heart J. 2009;30:2969 –2977.
CLINICAL PERSPECTIVEAtrial fibrillation (AF) imposes a symptomatic burden and the risk of cardiovascular events that increase in frequency withthe progression of atrial electric and structural remodeling. The hypothesis that long-term renin-angiotensin systeminhibition could reverse left atrial (LA) remodeling and thereby favor the prevention of AF recurrence was tested in theGruppo Italiano per lo Studio della Sopravvivenza nell’Infarto Miocardico–Atrial Fibrillation (GISSI-AF) trial. The resultsrevealed a neutral effect of valsartan treatment for 1 year on AF recurrence. The echocardiographic substudy results wereconsistent with those of the main study by showing valsartan to have no effect on LA volume. Severe LA enlargement(�40 mL/m2) recorded in 55% of the patients with only minimal increase in LV wall thickness and Doppler E/e� arguesfor the arrhythmia itself as the main cause of LA remodeling. Additionally, in the patients without AF recurrence in 1 year,LA maximal volume was equally and severely dilated; therefore, mechanisms other than remodeling need considerationin future studies. Although LA maximal volume was not predictive of first recurrence of AF, in patients with recurrent AF(54%), larger LA volumes and lower LA emptying fraction did forecast longer episodes of AF recurrence. The entry of85% hypertensive patients and only 10% with left ventricular dysfunction and heart failure emphasizes the causal role ofblood pressure in AF. Aggressive treatment of blood pressure targeted to increasing LA volumes could slow and possiblyhalt progressive LA remodeling and prevent or reduce the burden of recurrent AF.
728 Circ Cardiovasc Imaging November 2011
by guest on May 30, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from
Gianni Tognoni, Marcello Disertori and Roberto LatiniErnesto Correale, Gianna Fabbri, Federico Bertocchi, Maria Grazia Franzosi, Aldo P. Maggioni,Proietti, Dario Bicego, Carlo Emanuelli, Giancarlo Pulitanò, Filippo Taddei, Enrico B. Nicolis, Lidia Staszewsky, Maylene Wong, Serge Masson, Elena Raimondi, Silvana Gramenzi, Gianni
Fibrillation: The GISSI-AF Echocardiographic SubstudyLeft Atrial Remodeling and Response to Valsartan in the Prevention of Recurrent Atrial
Print ISSN: 1941-9651. Online ISSN: 1942-0080 Copyright © 2011 American Heart Association, Inc. All rights reserved.
Dallas, TX 75231is published by the American Heart Association, 7272 Greenville Avenue,Circulation: Cardiovascular Imaging
doi: 10.1161/CIRCIMAGING.111.9659542011;4:721-728; originally published online September 16, 2011;Circ Cardiovasc Imaging.
http://circimaging.ahajournals.org/content/4/6/721World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circimaging.ahajournals.org/content/suppl/2011/09/16/CIRCIMAGING.111.965954.DC1Data Supplement (unedited) at:
http://circimaging.ahajournals.org//subscriptions/
is online at: Circulation: Cardiovascular Imaging Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
requested is located, click Request Permissions in the middle column of the Web page under Services. FurtherCenter, not the Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright ClearanceCirculation: Cardiovascular Imagingin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on May 30, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from
CIRCCVIM/2011/965954_R2 1
SUPPLEMENTAL MATERIAL
Supplemental methods:
Patients in the GISSI-AF main study: inclusion criteria were two or more episodes of
symptomatic ECG-documented AF in the previous 6 months or successful cardioversion,
electrical or pharmacological between 48 hours and 14 days before randomization).
Patients had to have one of the following conditions: heart failure or a history of
documented left ventricular dysfunction (ejection fraction <40%), history of hypertension
for 6 months or longer, type 2 diabetes, a history of stroke, peripheral vascular disease,
coronary artery disease or lone atrial fibrillation with left atrial dilatation (left atrial diameter
of >45 mm in men and >40 mm in women). All participants had been on a stable regimen
of treatment for AF and of any underlying cardiovascular disorder for at least 1 month
before enrollment and were permitted to continue previously prescribed ACE inhibitors,
beta-blockers and amiodarone. Patients were excluded if they had clinically significant
valvular disease; or were scheduled to undergo catheter ablation or implantation of a
pacemaker or defibrillator.
Echocardiography: The recordings were taken in parasternal long-axis and short-axis at
the levels of the aortic valve, chordae and mid papillary muscle, and apical two and four-
chamber views. Baseline tracings were recorded at randomization and at 6 and 12
months. The measurements were left atrial (LA) diameters, maximal LA volume (before
mitral valve opening) and minimal LA volume (after atrial contraction), LA total emptying
fraction [maximal–minimal LA volumes/maximal LA volume] (LAEF), left ventricular (LV)
end-systolic and end-diastolic volumes, LV end-diastolic mean wall thickness and, LV
mass (2D method) (1). All patients had Pulsed-wave Doppler recordings of mitral inflow
velocities and pulmonary venous flow waveforms to measure, transmitral early diastolic
velocity (peak E wave) late diastolic velocity (peak A wave), E/A ratio, deceleration time of
E velocity (DT), isovolumic relaxation time (IVRT), pulmonary systolic, diastolic and
CIRCCVIM/2011/965954_R2 2
reversed atrial flow. The values out of the normal range according to age groups (41-60
and >60 years) (2) were considered for the identification of patients with abnormal mitral
inflow velocities and time intervals, Tissue Doppler recordings were provided by 19 sites
with sufficient technical and recording capabilities. Peak E wave velocities from four apical
chamber transmitral inflow and diastolic relaxation e’ velocities from mitral septal and
lateral annular tissue Doppler were combined to derive E/e’. Mitral regurgitation (MR) was
measured as regurgitant area/LA area in the apical view displaying the largest regurgitant
area and was graded: mild (5-20%), moderate (>20 -<40%), and severe (≥40%) an
eccentric jet increased the degree of MR by 1 grade (3).
References
1. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, Picard MH,
Roman MJ, Seward J, Shanewise JS, Solomon SD, Spencer KT, Sutton MS, Stewart
WJ; Chamber Quantification Writing Group; American Society of Echocardiography's
Guidelines and Standards Committee; European Association of Echocardiography.
Recommendations for chamber quantification: a report from the American Society of
Echocardiography's Guidelines and Standards Committee and the Chamber
Quantification Writing Group, developed in conjunction with the European Association
of Echocardiography, a branch of the European Society of Cardiology. J Am Soc
Echocardiogr. 2005;18: 1440-1463.
2. Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, Waggoner
AD, Flachskampf FA, Pellikka PA, Evangelista A. Recommendations for the evaluation
of left ventricular diastolic function by echocardiography. J Am Soc Echocardiogr. 2009;
22:107-133.
3. Helmcke F, Nanda NC, Hsiung MC, Soto B, Adey CK, Goyal RG, Gatewood RP Jr.
Color Doppler assessment of mitral regurgitation with orthogonal planes. Circulation
1987; 75: 175-183.
CIRCCVIM/2011/965954_R2 3
APPENDIX
Participating Centers and Investigators
Switzerland - Lugano (E. Pasotti). Italy - Bagno a Ripoli (A. Fantini), Bari Carbonara (N. D’Amato), Bergamo (A. Gavazzi, F. Taddei), Bovolone (G. Rigatelli, S. Boni), Catania (M. Gulizia, G. Francese), Catanzaro (F. Perticone), Città di Castello (D. Severini), Cremona (S. Pirelli, C. Emanuelli), Fidenza (P. Pastori), Firenze (GM. Santoro, C. Minneci), Napoli Federico II (M. Prastaro), Palermo Cervello (L. Buffa), Pavia (R. Rordorf), Pesaro (A. Pierantozzi), Pietra Ligure (A. Nicolino), Reggio Calabria (G. Pulitanò, A. Ruggeri), Roma Sant’Andrea (L. De Biase, S. Cangianiello), Saluzzo (P. Allemano), San Bonifacio (R. Rossi, D. Bicego), San Daniele del Friuli (L. Mos, O. Vriz), Sarzana (R. Petacchi, D. Bertoli), Terni (M. Bernardinangeli, Gianni. Proietti, M. Gagliardi), Trento Villa Bianca (G. Cioffi, E. Buczkowska), Trento Santa Chiara (M. Disertori, P. Zeni), Varese (F. Caravati).
CIRCCVIM/2011/965954_R2 4
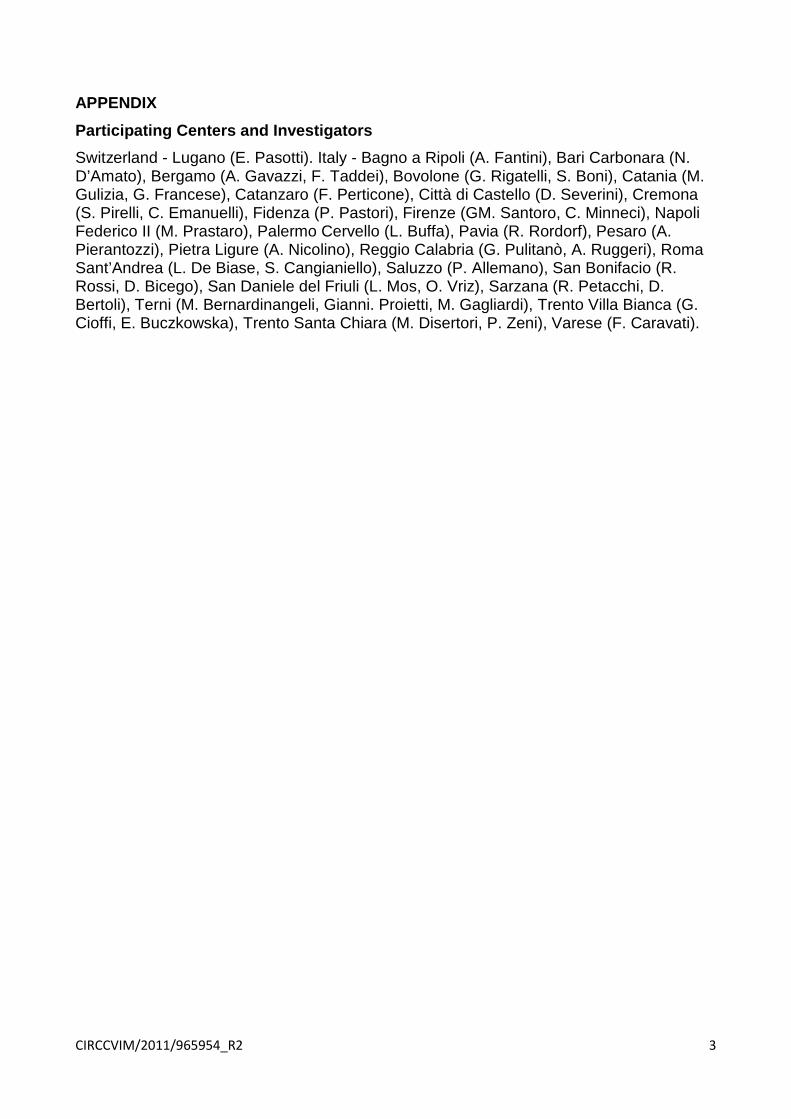
Supplemental Table:
Baseline Clinical and ECG Characteristics in Echo-Cohort and Non Echo-Cohort patients
Characteristics Echo-cohort
N=340
Non-Echo
cohort
N=1110
§P value
Age-yr 68.4±8.8 67.6±9.4 0.20
Female sex - no.(%) 123 (36.2) 421 (38.2) 0.50
Body-mass index - Kg/m2 27.7±4.2 27.9±4.4 0.57
Blood pressure - mmHg
Systolic 138.0±16.2 138.8±17.0 0.46
Diastolic 81.2±8.3 81.7±8.9 0.33
Inclusion criteria - no.(%)
≥2 episodes of AF in previous 6 mo 136 (40.4) 445 (42.2) 0.59
Cardioversion in previous 2 wk 297 (87.4) 979 (88.8) 0.45
Duration of last qualifying episode of AF >7 days 135 (39.7) 328 (29.8) 0.001
Heart failure, LVEF<40%, or both 36 (10.6) 78 (7.1) 0.04
History of hypertension for 6 mo or more 290 (85.3) 941 (85.4) 0.97
Diabetes mellitus 49 (14.4) 162 (14.7) 0.89
History of stroke 14 (4.1) 45 (4.1) 0.98
Peripheral artery disease 21 (6.2) 38 (3.5) 0.03
Documented coronary artery disease 38 (11.2) 141 (12.8) 0.43
Atrial fibrillation alone 47 (13.8) 125 (11.3) 0.22
Coexisting conditions - no.(%)
Peripheral embolism 6 (1.8) 4 (0.4) 0.01
Previous transient ischemic attack 15 (4.4) 39 (3.5) 0.46
Renal dysfunction 10 (2.9) 30 (2.7) 0.83
Chronic obstructive pulmonary disease 33 (9.7) 73 (6.6) 0.06
Neoplasia 11 (3.2) 34 (3.1) 0.89
Current smoker 30 (8.8) 91 (8.3) 0.05
Electrocardiographic findings at randomization
Heart rate - bpm 62.1±9.8 64.1±10.7 0.003
QRS interval>120 msec - no.(%) 40 (11.8) 87 (7.9) 0.03
Left ventricular hypertrophy - no. (%) 35 (10.3) 96 (8.7) 0.38
Pathologic Q waves - no. (%) 10 (2.9) 53 (4.8) 0.14
Concomitant cardiovascular therapies - no. (%)
Amiodarone 129 (37.9) 372 (33.8) 0.16
Sotalol 25 (7.4) 75 (6.81) 0.73
Class I antiarrhythmic agents 116 (34.1) 351 (31.9) 0.44
ACE inhibitors 173 (50.9) 649 (58.9) 0.009
Calcium-channel blockers 102 (30.0) 326 (29.6) 0.88
Beta-blockers 92 (27.1) 344 (31.2) 0.14
Digitalis 17 (5.0) 46 (4.2) 0.51
Diuretics 127 (37.4) 405 (36.8) 0.84
Aldosterone blockers 23 (6.8) 69 (6.3) 0.74
Statins 90 (26.5) 278 (25.2) 0.65
Oral anticoagulants 206 (60.6) 609 (55.3) 0.08
Aspirin 88 (25.9) 307 (27.9) 0.48
AF = atrial fibrillation; LVEF = left ventricular ejection fraction . §P value compare Eco-cohort
to Non-Echo cohort















![Dysrhythmias (002) [Read-Only] - Aventri · Atrial AV node Ventricular Classification of Rhythm Abnormalities Supraventricular Atrial origin Atrial fibrillation Atrial flutter Atrial](https://static.fdocuments.net/doc/165x107/5f024baa7e708231d4038f22/dysrhythmias-002-read-only-aventri-atrial-av-node-ventricular-classification.jpg)


