Tratamiento antibiótico empírico de infección intraabdominal
Upload
sanjay-sainiCategory
view
214download
0
Improved Localization and Survival in Patients with
Intraabdominal Abscesses
Sanjay Saini, MD, Boston, Massachusetts
John M. Kellum, MD, Boston, Massachusetts
Michael P. O’Leary, MD, Boston, Massachusetts
Thomas F. O’Donnell, MD, Boston, Massachusetts
Francis P. Tally, MD, Boston, Massachusetts
Barbara Carter, MD, Boston, Massachusetts
Ralph A. Deterling, MD, Boston, Massachusetts
Lon E. Curtis, MD, Boston, Massachusetts
Nearly 45 years ago, Ochsner and DeBakey [I] re- ported a significant reduction of their previous 32 percent operative mortality rate for the surgical management of subphrenic abscesses with the use of extraserous drainage. However, despite the intro- duction of antibiotics, the reported mortality rate for intraabdominal abscess has remained stubbornly at about 30 percent over the ensuing decades [2]. In 1980 Fry et al [3] reported a 32 percent mortality rate in a series of 143 patients, which excluded patients with abscesses subsequent to appendicitis or perfo- rated peptic ulcer. Factors which contribute to the high morbidity and mortality associated with in- traabdominal abscesses include delay in diagnosis, failure of preoperative abscess localization, and use of the midline transabdominal approach. Delay in diagnosis leads to further debilitation of septic pa- tients and to the development of the multiple organ failure syndrome. Inability to localize the abscess site mandates the midline transabdominal drainage ap- proach with its attendant higher risks or anesthetic complications, blood loss, and bowel injury. For ex- ample, Fry et al [3] reported that surgical exploration was based on specific radiographic findings in only 29 percent of their patients and was carried out through a midline incision in 67 percent. The inci- dence of organ failure in that series was 55 percent, with an attendant mortality rate of 53 percent.
Computerized axial tomography (CAT) has been alleged to be a powerful diagnostic tool for intraab- dominal abscesses [4,5]. To assess the accuracy of this new technology and its impact on the management
From the Departments of Surgery, Medicine, and Radiology, Tufts-New England Medical Center, Boston, Massachusetts.
Requests for reprints should be addressed to John M. Kellum. MD, Tufts-New England Medical Center, 171 Harrison Avenue, Boston, Massa- chusetts 02111.
Presented at the 23rd Annual Meeting of the Society for Surgery of the Alimentary Tract, Chicago, Illinois, May 18-19, 1982.
of intraabdominal abscess, as well as the impact of newer modes of therapy which were also first em- ployed in the same period, we analyzed the first 100 consecutive patients at Tufts-New England Medical Center since the installation of the CAT scanner.
Material and Methods
In this retrospective study, we reviewed all records of patients with intraabdominal abscesses from July 1975, when the CAT scanning equipment was installed at New England Medical Center Hospital, until the end of 1981, when the 100th patient was diagnosed with it. This report analyzes all intraabdominal abscesses, including liver ab- scesses, but excludes wound and abdominal wall abscesses. Of the 100 patients in our series, abscesses developed in 71 as a result of spontaneous intraabdominal disease processes or trauma (primary group), and in 29 patients they devel- oped as a complication of an operation or procedure (sec- ondary group). Seven of these were referred to us after operations at outside hospitals. The history, physical ex- amination findings, fever, leukocyte count, and other pertinent laboratory findings were documented.
Diagnosis: The sensitivity of both conventional and newer means of diagnosis for intraabdominal abscesses was compared. During the period of study, gallium scanning and ultrasonography were available as well as CAT scan- ning. Each test was used at the discretion of the patient’s physician. Radiolabelled leukocyte scanning was not used in these patients. At the beginning of the study, all three newer diagnostic tests (gallium scanning, ultrasonography, and CAT scanning) tended to be used in combination. Towards the conclusion of the study, a more selective ap- proach was employed.
Between July 1975 and September 1980, an Ohio Nu- clear Delta 50 CAT scanner with a 2 minute scanning time was used in our hospital. After the latter date, the original scanner was replaced by a Siemen’s Somatoms-2 with a 5 second scanning time used for abdominal studies. The latter more rapid scanner was used in 13 patients or 27 percent of patients having CAT scans. During the period of study, the ultrasound equipment used included the
136 The American Journal ol Surge

Modern Management of lntraabdominal Abscesses
Unirad Sono 2 grey-scale unit and three different real-time units (Hoffrel System 201, Rohe-7000, and Phillips-2000). Gallium scanning was performed 3 to 7 days after the in- travenous injection of gallium-67 citrate using an Ohio Nuclear 84D rectilinear scanner until 1980, when a Sigma 410s wide-field gamma camera was installed.
Bacteriology: In addition to aerobic cultures, anaerobic cultures were taken in most patients. When possible, pus was aspirated into a syringe, all air bubbles expelled, and the syringe corked. The syringe was then delivered im- mediately to the anaerobic bacteriology laboratory, where it was processed by standard methods [6,7].
Surgery: Surgical mangement was analyzed for the in- dications for operation, operative approach, and the loca- tion and number of abscesses. Results were judged on the basis of hospital course, mortality and morbidity, and the recurrence or persistence of infection.
Historical control: To compare recent mortality rates with ra+ks before the availability of the CAT scanner at our hospital, we reviewed all abscesses between January 1970 and June 1975 for mortality only. The method of diagnosis was correlated with the mode of drainage. Statistical comparisons were made by chi-square analysis.
Results
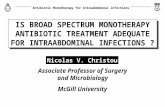
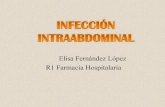
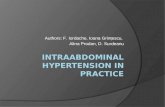
Of the 100 patients in the series, the mean age was 56 years (range 12 to 82 years). There were 57 male and 43 female patients. The causes of intraabdominal abscesses in the primary group are shown in Figure 1. Abscesses followed or attended appendicitis, the most common antecedent natural disease process, in 16 patients. Of these, 14 patients had grossly perfo- rated appendixes. Twelve patients had abscesses drained at the time of appendectomy, and 4 required drainage of abscesses that developed after appen- dectomy. Notably, abscesses developed in only two patients after perforation of peptic ulcers. Both of these were in patients with perforated duodenal ul- cers who presented to the surgeon after more than 12 hours of symptoms. The causes of abscesses in the secondary group are shown in Figure 2. Of these pa-
CAUSES
G.I. Surgery
Biliary Surgery
Non-G.I. Surgery
Endoscopy
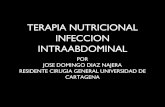
Other Flgure 2. Eiiobgy oi lnfraabdominal ab- scesses among those aflsing as compli- caflons of operations or procedures (secondary group). Numbers represent . _...
66%
m 7%
m 14%
m 10%
I 3%
I 1 I 25 50 75
pefcenr of rotai seconaafy group. rtRCENT OF POST-OPERATIVE ABSCESS PATIENTS (N=29)
CAUSES
Appendicitis
Diverticulitis
16
Trauma
Primary Hepatic
Perforated CA Colon
Crohn’s
6
Tubo-Ovarian
Perforated Ulcer
Pancrealitis 2
Miscellaneous 11 1 I
10 20
NUMBER OF PATIENTS (N=71)
Figure 1. Etiology of intraabdominal abscesses among those arising from sponianeous intraabdominal disease or trauma (primary group). Numbers represent absolute numbers of pa- tients,
tients, the majority (73 percent) had had gastroin- testinal or biliary surgery, and of this group, 73 per- cent had colonic operations. Abscesses developed after nongastrointestinal surgery in only 14 percent of the patients in the secondary group, and surpris- ingly, abscesses developed in 10 percent as compli- cations of endoscopic procedures.
Volume 145, January 1993 137

Saini et al
Subphrenic 26%
Lesser sac
Retroperitoneal
Paracolic
4%
10%
13%
Periappendicular 13
Pelvic 20%
The location of abscesses is presented in Figure 3. Twenty-one patients had two or more abscesses, and there were 130 abscesses overall. The subdiaphrag- matic location designation includes 4 abscesses in the lesser sac and 17 subhepatic collections. The rela- tively high proportion of intrahepatic abscesses (7 percent) resulted in part from referral patterns de- veloped by the Infectious Disease Service which has a special interest in this entity.
Analysis of diagnostic techniques: The decision to institute drainage was based primarily on physical examination and clinical findings in 41 percent of patients. In 57 percent, the decision for and the timing of operation were strongly affected by radio- logic findings, though clinical correlation was im- portant in all. The sensitivities of the newer diag- nostic tests were as follows: CAT scanning 92 percent, ultrasound 77 percent, CAT scanning and ultrasound 93 percent, and gallium scanning 75 percent. Gallium scanning and ultrasound were significantly less sensitive (p <0.05) than CAT scanning, and CAT scanning plus ultrasound were not significantly better than CAT scanning alone. CAT scanning was
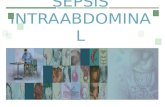
PURE AEROBIC
1 PURE ANAEROBIC
1 MIXED AEROBIC/ANAEROBIC
1 TOTAL CULTURES CONTAINING ANAEROBES
1 I I I I 1 1
20 40 60
PERCENT OF ABSCESS CULTURES
Figure 4. Aerobic and anaerobic composltion of intraabdomlnal abscess cuff ures.
Figure 3. Distributton fo 130 abscesses In 100 patients.
the definitive diagnostic study in 69 percent of the 48 patients in whom it was used. Even though 73 percent of the CAT scans in this study were per- formed with the earlier 2 minute scanner, the 92 percent sensitivity for this modality was significantly greater than ultrasonography or gallium scanning (p <0.05). CAT scanning influenced the route of drainage in 58 percent of the patients in whom it was used. Significantly more patients who had CAT scans performed had extraserous or percutaneous drainage (54 percent) than those who did not have CAT scans (34 percent) (p <0.05).
The proportion of available cultures that were processed for aerobic and anaerobic bacteria are il- lustrated in Figure 4. Sixty percent of cultures con- tained anaerobic organisms either in pure culture or mixed with aerobes. Escherichia coli was the most commonly isolated aerobe, and Bacteroides fragilis the most common anaerobe.
Operative approach: Of 100 patients who had surgical drainage of intraabdominal abscesses, the transabdominal approach was used in 53; 13 patients had extraserous drainage through a posterior ap- proach with or without rib resection; 14 patients had localized drainage of a subphrenic or subhepatic abscess by a subcostal approach; and 8 patients had drainage through the vaginal cul-de-sac or rectum. No drainage was used in 3 patients. Soft rubber Penrose drains were used in 42 percent, sump drains were used in 6 percent, and combined soft and sump drains were used in 33 percent. Closed drainage employing either a 14 gauge Argyle trocar catheter or a no. 8 F. pigtail catheter employing the technique of percutaneous drainage of abscesses, as described by Gerzof et al [a], was used in nine patients.
Mortality and morbidity: Of the 100 patients, 12 died (12 percent mortality). This mortality rate compared favorably with the 28 percent mortality rate for management of intraabdominal abscesses observed at this hospital in the period (1970 to 1975)
138 The American Journal of Surgery

Modern Management of lntraabdominal Abscesses
immediately preceding the study period (p <0.05). Of the deaths in the present study group, eight were associated with organ failure, two with hemorrhage, and two with systemic candidiasis (in combination with candidal intraabdominal abscess). Two patients in whom organ failure also developed had inoperable malignant growths. Two deaths were associated with failure of percutaneous catheter drainage, although one of the patients was moribund beforehand due to multiple organ system failure.
To compare the mortality rate in our series with that of Fry et al [3], we calculated mortality in pa- tients who had neither appendicitis nor perforated peptic ulcer. With these exclusions, the mortality rate was 13.4 percent (11 of 82 patients). The mortality rate for the 24 patients with subphrenic abscesses was 17 percent. Postoperative morbidity included 20 patients who required secondary drainage for re- current abscesses. Organ failure developed in 13 patients of whom 62 percent died. Enterocutaneous fistulas developed in three patients after their initial drainage procedure, two of which were thought to be secondary to operative injury to the intestine. Transient pancreatic fistulas developed in two pa- tients, and candidal superinfections after drainage developed in two other patients.
Comments
No area of surgery has seen more potential ad- vances in management in the last 10 years than the problem of intraabdominal abscesses. Included among these advances are diagnostic innovations such as ultrasonography, gallium and radiolabelled leukocyte scanning, and computerized axial tomog- raphy of the body cavities. Therapeutic advances include a greater appreciation of the important role that anaerobic bacteria play in intraabdominal sepsis and the necessity to fight them with specific antibi- otic therapy. The development of percutaneous drainage of intraabdominal abscesses by the inter- ventional radiologists is a promising recent advance with good initial results [8].
Despite these advances, patients with advanced intraabdominal sepsis, especially those in whom organ failure develop, have an extremely high mor- tality rate. Fry et al [3] reported an overall 32 percent mortality rate in a selected group of patients with intraabdominal abscesses. However, the mortality rate in that series was 53 percent for patients in whom organ failure developed. The patients in Fry’s series received treatment before 1975 and before the availability of CAT scanning at their medical center. In addition, antibiotic therapy aimed at both aerobic and anaerobic components of intraabdominal in- fection was not routinely employed by Fry’s group. To analyze the effects of newer diagnostic and ther- apeutic techniques on mortality in patients with in- traabdominal abscesses, we reviewed patients diag- nosed before and after 1975, when the CAT scanner
was introduced at our institution. The mortality rate of 12 percent in patients who received treatment since July 1975 (when the CAT scan became avail- able) was significantly lower (p cO.05) than the 28 percent mortality rate in patients who received treatment at our hospital before the CAT scan was available (between 1970 and 1975). Our mortality rate for the 1975 to 1981 period (13.4 percent ex- cluding patients with appendicitis and perforated ulcer) was also significantly lower than the 32 percent mortality rate in 143 patients reported by Fry et al [3] (p <O.Ol). The mortality rate for subphrenic ab- scess in our series was 17 percent, which is far better than in most of the series reported over the last 4 decades [2].
In comparing the results of modern surgical management with those achieved by percutaneous drainage of abscesses, our mortality rate was com- parable with that reported by Gerzof et al [B] (8 percent) in a series in which percutaneous drainage of intraabdominal abscesses was used exclusively. In addition, many of our patients with multiple ab- scesses would not have been candidates for percu- taneous drainage and thereby represent a higher risk group. This finding supports the contention of Welch [9] that the low mortality in the series of Gerzof et al [8] was primarily the result of early diagnosis rather than catheter drainage.
Although the improved mortality rate in our series may stem from multiple factors, it seems likely that early diagnosis was very important. Only 13 percent of the patients in our series (15 percent excluding patients with appendicitis and perforated ulcers) reached the stage of organ failure, as compared with 55 percent in the series reported by Fry et al [3] (p <O.OOl). Although our overall mortality rate was lower than in Fry’s report, our mortality rate in pa- tients with organ failure was slightly higher (62 versus 53 percent, p = 0.5). Thus, prevention of organ failure by early diagnosis and drainage appears to be the key factor in our lower mortality rate.
The superiority of CAT scanning as a definitive diagnostic technique in patients with intraabdominal abscesses was clearly demonstrated. The overall sensitivity of CAT scanning was 92 percent. This was achieved even though the older 2 minute model scanner was employed in over half of our patients. Recent reports [4,5] demonstrate an overall sensi- tivity rate as high as 96 percent with modern high- speed CAT scanning equipment. CAT scanning ap- pears to have some unique advantages in the man- agement of intraabdominal abscesses (Figure 5). The superiority of CAT scanning was especially notice- able in patients who, although suspected of harboring intraabdominal septic foci, demonstrated no specific localizing signs. It was superior to ultrasonography in pelvic abscesses where ultrasonographic inter- pretation was made difficult by interference with pelvic skeletal structure. CAT scanning was also
Volume 145, January 1983 139

Saini et al
DECISION TREE FOR SUSPECTED INTRAABDOMINAL
f
ABSCESS
4 CAT SCAN ULTRASOUND
Regional localizatton not suspected Regional localization suspected on clinical grounds (except pelvis)
Suspected pelvic abscess Adjunct to percutaneous drainage Figure 5. Recommended indication for abdominal CAT scan&g versus uttraso-
Suspected multiple abscesses Pregnancy
Interloop abscesses
superior in multiple and deep-lying intraabdominal abscesses, especially those in close proximity to the gastrointestinal tract. CAT scanning was the defin- itive test in 69 percent of all the patients in whom it was employed. Patients who had CAT scan exami- nations were significantly more likely to have ex- traserous drainage than those patients who did not have this examination. On the other hand, delinea- tion of multiple abscesses by CAT scan led to the transabdominal approach in other patients. Finally, CAT scanning proved useful for following the ade- quacy of drainage and diagnosing recurrent or per- sistent collections.
Ultrasound was beneficial in selected clinical sit- uations (Figure 5). It was very useful in patients in whom the regional locations of their abscesses were suspected on clinical grounds, as in patients with diverticulitis. It was also accurate in patients with subphrenic abscesses, especially those in proximity to the abdominal wall. Because there is no radiation hazard associated with ultrasonography, it should be used as the primary diagnostic modality in these in- stances. However, in other patients CAT scanning is more likely to define abscesses accurately. The combination of CAT scanning and ultrasonography was not significantly better than CAT scanning alone in our series. This realization should lead to cost savings for patients in whom ultrasonography is not likely to yield a definitive diagnosis.
Gallium scanning, although it had a respectable sensitivity rate in our series, was largely abandoned as a diagnostic tool for suspected intraabdominal abscess during the period of the study. This trend resulted because of a lack of specificity and an un- acceptably high rate of false-positive examinations, since gallium localizes in the colonic lumen as well as in phlegmons, neoplasms, and in healing surgical wounds. The time required for gallium localization within abscess cavities (3 to 7 days) was often un- justifiable, considering the availability of rapid di- agnosis with other modalities.
nography in patients In whom either the presence or locallxation of an Intraab- hnninal abscess is unclear tram physical exam/nation and conventtonal radlog- raphy.
The availability of accurate methods for localizing intraabdominal abscesses is leading to a shift back toward extraserous drainage routes. Transabdominal drainage is usually indicated when there is evidence of continued leakage from the gastrointestional tract, in cases of peripancreatic abscesses, and for multiple intraabdominal abscesses. We prefer open surgical drainage, although we readily acknowledge the place of percutaneous drainage in high-risk patients who are not good candidates for general anesthesia. One of the deaths in our series was directly related to in- adequate drainage by percutaneous catheter; this technique demands a rigorous follow-up by a team of surgeons and radiologists who must insure its ap- propriate application.
The relatively low yields of anaerobic organisms found in our patients are a result of our policy of in- stituting broad-spectrum antibiotic coverage for both aerobic and anaerobic organisms in all cases of in- traabdominal sepsis. In an earlier study [IO] con- ducted before the widespread use of antibiotics specifically aimed at anaerobes, a greater than 90 percent incidence of anaerobes in intraabdominal abscesses of all causes was reported. The randomized study of traumatic intestinal perforation by Thade- palli et al [II] demonstrated that the early use of antibiotics effective against anaerobes led to a lower yield of anaerobes on operative culture. Although no attempt was made to evaluate the effectiveness of antibiotic therapy in this series, some of the patients included in our series were previously reported in a randomized, prospective study of antibiotic therapy elsewhere [12]. As a general policy, patients received antibiotics effective against both aerobic and an- aerobic organisms at the first signs of intraabdominal sepsis. Although we cannot quantitate the influence of this policy on mortality in the present series, it may well have been significant, since Nobles [13] reported a dramatic reduction in mortality in patients with abdominal sepsis treated with such a policy. While antibiotic therapy cannot prevent progression of
140 The American Journal ot Surgery

Modern Management of lntraabdominal Abscesses
undrained sepsis, we believe that it is an important adjunct to appropriate drainage in that it may reduce abscess recurrence and metastatic seeding of infec- tion.
The improvement in the survival rate is attribut- able both to early diagnosis and prevention of late manifestations of systemic sepsis, such as multiple organ failure. We have been no more successful than others in preventing death in patients with estab- lished organ failure. It is likely that prevention of organ failure by early diagnosis, appropriate drain- age, and antimicrobial therapy may be a much more economic and effective plan than therapy aimed at reversing established organ failure.
Summary
A review of 100 consecutive patients with in- traabdominal abscesses treated since the advent of the CAT scanner has been presented. Each patient was analyzed with regard to etiology, bacteriology, sensitivity of preoperative diagnostic studies, method of drainage, mortality, and morbidity. Abscesses developed in 71 percent of these patients as a result of spontaneous intraabdominal disease, and in 29 percent as a complication of operation or procedures. Sixty percent of cultures grew anaerobic organisms. The sensitivity of CAT scanning (92 percent) was significantly better than that of ultrasonography (77 percent) or gallium scanning (75 percent). When ultrasound was used in conjunction with CAT scan- ning there was no improvement in sensitivity. Pa- tients who had CAT scans were more likely to have extraserous drainage (p <0.05) than those who did not. Ultrasound was indicated in selected clinical situations. The overall mortality rate of 12 percent was significantly better (p <0.05) than the mortality rate of 28 percent in the previous 5 year period. Organ failure, which carries a high mortality in septic pa- tients, was observed in only 13 percent of our patients who had CAT scans. We attribute the decrease in mortality to earlier diagnosis and drainage, wider use of extraserous drainage due to utilization of new imaging techniques, and to the use of antibiotics ef- fective against both aerobic and anaerobic organ- isms.
References
1. Ochsner A, DeBakey ME. Subphrenic abscess: collective re- view and analysis of 3.608 collected and personal cases. Int Abstr Surg 1938;66:426.
2. Ariel IM, Kazarian KK. Diagnosis and treatment of abdominal abscesses. Baltimore: Williams and Wilkins, 1971:203.
3. Fry DE, Garrison RN, Heitsch RC, Calhoun K, Polk HC. Deter- minants of death in patients with intraabdominal abscess. Surgery 1980;88:517-23.
4. Knochel JQ, Koehler PR, Lee TG, Welch DM. Diagnosis of ab- dominal abscesses with computed tomography, ultrasound, and trrln leukocyte scans. Radiology 1980;137:425-32.
5. Robison JG, Pollock TW. Comouted tomooraohv in the diaonosis and localization of intraabdominal abscess. Am J”Surg 1980;140:783-6.
6. Lenette EH, Balows A. Hausler WJ, Truant JP. Manual of clinical
microbiology. 3rd ed. Washington, DC: American Society of Microbiology, 1980:397-4 17.
7. Holdeman LV, Cato EP, Moore WEC. Anaerobic laboratory manual. 4th ed. Blacksburg: Virginia Polytechnic Institute, 197712-4.
8. Gerzof SG, Robbins AH, Johnson WC, Birkett DH, Nabseth DC. Percutaneous catheter drainage of abdominal abscesses: a five-year experience. N Engl J Med 1981;305:653-7.
9. Welch CE. Catheter drainage of abdominal abscesses (editorial). N Engl J Med 1981;305:694-5.
10. Gorbach SL. Treatment of intraabdominal sepsis. In: Finegold SM, moderator. Management of anaerobic infections. Ann Int Med 1975;83:375-88.
11. Thadepalli H, Gorbach SL, Broido P, Norsen J, Nyhus L. Ab- dominal trauma, anaerobes and antibiotics. Surg Gynecol Obstet 1973;137:270-6.
12. Tally FP, McGowan K. Kellum JM. Gorbach SL. O’Donnell TF. A randomized comparison of cefoxitin with or without ami- kacin and clindamycin plus amikacin in surgical sepsis. Ann Surg 1981;193:318-23.
13. Nobles ER. Bacteroides infections. Ann Surg 1973;177: 601-6.
Discussion Hastings K. Wright (New Haven, CT): We recently
reviewed our last 80 cases of intraabdominal abscess to determine what diagnostic step actually determined where and when the abscess should be drained. In 60 (75 percent) of those cases, physical examination in conjunction with routine roentgenographic examination was definitive. Imaging studies, although highly accurate, were merely confirmatory, and when they were performed before physical findings were determined to be positive, the re- sults were very equivocal, being reported as “consistent with but not diagnostic of, ” “must correlate with clinical findings,” and so on.
The CAT scan in our experience has been helpful pri- marily in patients who have had signs of sepsis for weeks, and who eventually show up with multiple intraabdominal abscesses. Thus, we feel that although the CAT scan complements an abdominal and rectal examination, it certainly has not replaced it.
Robert E. Condon: (Lexington, KY): I really agree with John Kellum and his group about the place of various di- agnostic procedures and the marked improvement in the overall experience we have all had in managing these sorts of patients. To a degree, I probably ought to respond to Hastings Wright, because it is with his point of view that I have some disagreement. We have found that early CAT scanning in patients with suspected intraabdominal sepsis is very highly specific. Its major advantage is that it does identify those patients who have a single focus of infection, some of whom will be appropriate for percutaneous drainage, some of whom will still require more traditional open surgical approaches. But more importantly, it also identifies within that population the subset of patients who have multiple abscesses and who do require more general exploration.
Five years ago the rule was that when pus under the di- aphragm could not be localized, and it was thought to be somewhere else, a general abdominal exploration was carried out. More often than not, our experience was that such management complicated the situation rather than improved it; those patients often went through multiple episodes and redrainage procedures because of the fact that pus spread around the abdomen in the course of the general exploration.
Volume 145, January 1983 141

Saini et al
I would disagree a bit with Dr. Kellum about the general role of ultrasound. We have found that ultrasound in terms of early diagnosis has not been very helpful even in those patients with a subphrenic abscess. When ultrasound has confirmed the presence of a subphrenic abscess, it has also been obvious on other grounds both in terms of clinical history and in terms of simpler radiologic procedures. However ultrasound does have a role, particularly when an abscess has been drained percutaneously and its location is known. It is useful for following the resolution of that abscess because it is very quick and simple to do, is much less expensive than repetitive CAT scanning and, I think it is more accurate than physical diagnosis.
John M. Kellum (closing): I would like to thank Dr. Wright and Dr. Condon for their excellent observations. I have had the pleasure of reading Dr. Wright’s paper. I noted that in his series the mortality rate was only 7.5 percent, which I think is commendable. I wonder, though, in the 25 percent of his patients in whom the CAT scan was diagnostic, whether those weren’t the patients who might have died without the benefit of the CAT scan. The CAT
scan is mostly helpful in patients with nonspecific physical findings. The patient may present with signs of early organ failure or a general septic process, and, in our experience, it is this high-risk patient in whom the CAT scan has been very helpful.
I agree with Dr. Wright about the importance of clinical correlation. When we order a CAT scan, we go to the ra- diology suite and discuss the case and the CAT scan per- sonally with the radiologist, Dr. Carter, who is one of the coauthors. Her interpretative skills have been very helpful at our hospitals.
I agree with Dr. Condon’s comments that ultrasono- graphy is less helpful than CAT scanning, in general. We have found it valuable when the localization of the abscess is suspected on clinical grounds, as, for example, a sus- pected left subphrenic abscess in a patient after splenec- tomy. It is sometimes more a question of confirming and localizing an abscess than diagnosing an abscess. I think we should remember that ultrasonography is the least in- vasive of the tests we have available, and that, as the technology improves, it may be even more useful than it is now.
142 The American Journal oi Surgery