Permissible Intraabdominal Hypertension Following.40 (1)
14
Copyright © 2015 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited. www.PRSJournal.com 868 I ntraabdominal pressure greater than 12 mmHg is known as intraabdominal hypertension, and abdominal compartment syndrome is defined as an intraabdominal pressure greater than 20 mmHg associated with new organ dysfunction. 1 A measure- ment of abdominal perfusion pressure [abdomi- nal perfusion pressure = (mean arterial pressure – intraabdominal pressure)] can be considered a more accurate measurement of visceral perfu- sion and valuable resuscitation endpoint, as sur- vival from abdo minal compa rtment synd rome has been associated with an abdominal perfusion pres- sure of greater than 60 mmHg. 2–6 Increasingly, a Disclosure: None of the authors has financial dis- closures or commercial associations that would po- tentially create a conflict of interest with information presented in this article. Copyright © 2015 by the American Society of Plastic Surgeons DOI: 10.1097/PRS.0000000000001621 Clayton C. Petro, M.D. Siavash Raigani, B.S. Mojtaba Fayezizadeh, M.D. James R. Rowbottom, M.D. John C. Klick, M.D. Ajita S. Prabhu, M.D. Yuri W. Novitsky, M.D. Michael J. Rosen, M.D. Cleveland, Ohio Background: Repair of hernias with loss of domain can lead to elevated intraab- dominal pressure. The authors aimed to characterize the effects of elective hernia repair on intraabdominal pressure, as well as its predictors and associa- tion with negative outcomes. Methods: Patients undergoing elective hernia repair requiring myofascial release had intraabdominal and pulmonary plateau pressures measured pre- operatively , postoperatively, and on the morning of the first postoperative day . Loss of domain was measured by preoperative computed tomography. Out- come measures included predictors of an increase in plateau pressure, respira- tory complications, and acute kidney injury. Results: Following 50 consecutive cases, diagnoses of intraabdominal hyper- tension (92 percent), abdominal compartment syndrome (16 percent), and abdominal perfusion pressure less than 60 mmHg (24 percent) were deter- mined. Changes in intraabdominal pressure (preoperative, 12.7 ± 4.0 mmHg; postoperative, 18.2 ± 5.4 mmHg; postoperative day 1, 12.9 ± 5.2 mmHg) and abdominal perfusion pressure (preoperative, 74.7 ± 15.7; postoperative, 70.0 ± 14.4; postoperative day 1, 74.9 ± 11.6 mmHg) consistently resolved by post- operative day 1, and were not associated with respiratory complications or acute kidney injury. Patients who remained intubated postoperatively for an elevation in pulmonary plateau pressure ( ≥6 mmHg) all demonstrated an improvement in plateau pressure by postoperative day 1 (preoperative, 18.9 ± 4.5 mmHg; postoperative, 27.4 ± 4.0 mmHg; postoperative day 1, 20.1 ± 3.7 mmHg), and could be identified preoperatively as having a hernia volume of greater than 20 percent of the abdominal cavity ( p < 0.001), but were still more likely to have postoperative respiratory events ( p = 0.01). Conclusions: Elevated intraabdominal pressure following elective hernia repair requiring myofascial releases is common but transient. Change in pla- teau pressure by 6 mmHg or more following repair can be expected with a loss of domain greater than 20 percent and is a more useful surrogate than intraabdominal pressure measurements with regard to predicting postopera- tive pulmonary complications. The perception and management of elevated intraabdominal pressure should be considered distinct and “permissible” in this context. (Plast. Reconstr. Surg. 136: 868, 2015.) From the Case Comprehensive Hernia Center and the De- partment of Anesthesiology and Perioperative Medicine, University Hospitals Case Medical Center. Received for publication November 6, 2014; accepted March 26, 2015. Presented at the 16th American Hernia Society Annual Hernia Repair Meeting, in Las Vega s, Nevada, March 12 through 15, 2014, Fruchaud Award for Best Poster Presentation. Permissible Intraabdominal Hypertension following Complex Abdominal Wall Reconstruction RECONSTRUCTIVE
-
Upload
david-diaz -
Category
Documents
-
view
220 -
download
0
Transcript of Permissible Intraabdominal Hypertension Following.40 (1)

7/25/2019 Permissible Intraabdominal Hypertension Following.40 (1)
http://slidepdf.com/reader/full/permissible-intraabdominal-hypertension-following40-1 1/14
Copyright © 2015 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.
www.PRSJournal.com868
I
ntraabdominal pressure greater than 12 mmHgis known as intraabdominal hypertension, and
abdominal compartment syndrome is defined asan intraabdominal pressure greater than 20 mmHg
associated with new organ dysfunction.1 A measure-ment of abdominal perfusion pressure [abdomi-
nal perfusion pressure = (mean arterial pressure– intraabdominal pressure)] can be considereda more accurate measurement of visceral perfu-sion and valuable resuscitation endpoint, as sur- vival from abdominal compartment syndrome hasbeen associated with an abdominal perfusion pres-sure of greater than 60 mmHg.2–6 Increasingly, a
Disclosure: None of the authors has financial dis- closures or commercial associations that would po- tentially create a conflict of interest with information presented in this article.Copyright © 2015 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0000000000001621
Clayton C. Petro, M.D.Siavash Raigani, B.S.
Mojtaba Fayezizadeh, M.D. James R. Rowbottom, M.D.
John C. Klick, M.D. Ajita S. Prabhu, M.D.
Yuri W. Novitsky, M.D.Michael J. Rosen, M.D.
Cleveland, Ohio
Background: Repair of hernias with loss of domain can lead to elevated intraab-dominal pressure. The authors aimed to characterize the effects of electivehernia repair on intraabdominal pressure, as well as its predictors and associa-tion with negative outcomes.Methods: Patients undergoing elective hernia repair requiring myofascialrelease had intraabdominal and pulmonary plateau pressures measured pre-operatively, postoperatively, and on the morning of the first postoperative day.Loss of domain was measured by preoperative computed tomography. Out-come measures included predictors of an increase in plateau pressure, respira-tory complications, and acute kidney injury.Results: Following 50 consecutive cases, diagnoses of intraabdominal hyper-tension (92 percent), abdominal compartment syndrome (16 percent), and
abdominal perfusion pressure less than 60 mmHg (24 percent) were deter-mined. Changes in intraabdominal pressure (preoperative, 12.7 ± 4.0 mmHg;postoperative, 18.2 ± 5.4 mmHg; postoperative day 1, 12.9 ± 5.2 mmHg) andabdominal perfusion pressure (preoperative, 74.7 ± 15.7; postoperative, 70.0± 14.4; postoperative day 1, 74.9 ± 11.6 mmHg) consistently resolved by post-operative day 1, and were not associated with respiratory complications oracute kidney injury. Patients who remained intubated postoperatively for anelevation in pulmonary plateau pressure (≥6 mmHg) all demonstrated animprovement in plateau pressure by postoperative day 1 (preoperative, 18.9± 4.5 mmHg; postoperative, 27.4 ± 4.0 mmHg; postoperative day 1, 20.1 ± 3.7mmHg), and could be identified preoperatively as having a hernia volume ofgreater than 20 percent of the abdominal cavity ( p < 0.001), but were still morelikely to have postoperative respiratory events ( p = 0.01).Conclusions: Elevated intraabdominal pressure following elective herniarepair requiring myofascial releases is common but transient. Change in pla-teau pressure by 6 mmHg or more following repair can be expected with aloss of domain greater than 20 percent and is a more useful surrogate thanintraabdominal pressure measurements with regard to predicting postopera-tive pulmonary complications. The perception and management of elevatedintraabdominal pressure should be considered distinct and “permissible” inthis context. (Plast. Reconstr. Surg. 136: 868, 2015.)
From the Case Comprehensive Hernia Center and the De- partment of Anesthesiology and Perioperative Medicine,University Hospitals Case Medical Center.Received for publication November 6, 2014; accepted March26, 2015.Presented at the 16th American Hernia Society Annual HerniaRepair Meeting, in Las Vegas, Nevada, March 12 through 15,2014, Fruchaud Award for Best Poster Presentation.
Permissible Intraabdominal Hypertension followingComplex Abdominal Wall Reconstruction
RECONSTRUCTIVE

7/25/2019 Permissible Intraabdominal Hypertension Following.40 (1)
http://slidepdf.com/reader/full/permissible-intraabdominal-hypertension-following40-1 2/14
Copyright © 2015 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.
Volume 136, Number 4 • Permissible Intraabdominal Hypertension
869
heightened awareness of these measurements andtheir significance has led to the formation of expertconsensus definitions and clinical practice guide-lines by the World Society of the Abdominal Com-partment Syndrome first in 2006 and most recentlyupdated in 2013.1,7,8 Despite growing attentivenesstoward these diagnoses, intraabdominal hyperten-sion and abdominal compartment syndrome havebeen characterized almost exclusively in the con-text of an acute abdomen from abdominal trauma,pancreatitis, or perforated viscus.8–14
As a referral center for large complex inci-sional hernias with loss of domain, we have grownprogressively conscious of the potential for induc-ing elevated intraabdominal pressure followingrepair with primary fascial approximation. Previ-ously, we identified an elevation in plateau pres-sure of greater than 6 mmHg following repair as
an important predictor of postoperative respi-ratory complications, confirming that an eleva-tion of intraabdominal pressure in this setting isnot inconsequential.15 In our clinical experience,keeping patients with a change in plateau pres-sure of greater than 6 mmHg intubated after theiroperation would consistently allow for normalizedplateau pressures by the following morning. There-fore, we sought to prospectively characterize theeffects of complex large hernia repairs requiringmyofascial releases on intraabdominal pressureand identify both preoperative predictors of these
changes and potential associations with these mea-surements and adverse outcomes. We hypothesizedthat in the aforementioned context, diagnoses ofintraabdominal hypertension, abdominal compart-ment syndrome, and abdominal perfusion pressureless than 60 mmHg would be common immediatelyafter repair. Furthermore, we hypothesized that anelevated intraabdominal pressure would improveby the first postoperative day. If so, this transientelevation—in the absence of an association withnegative outcome—could be viewed as “permis-sible,” and not require further intervention.
PATIENTS AND METHODSFollowing institutional review board
approval, all patients undergoing open inci-sional hernia repair requiring myofascial releasefor fascial medialization were consecutivelyenrolled at University Hospitals Case MedicalCenter by three surgeons (M.J.R., Y.W.N., and A.S.P.). Those patients that did not require a myo-fascial release were excluded. All patients under- went medical optimization by our Center for
Perioperative Medicine. Patient demographics,
comorbidities, and operative characteristics were obtained. Chronic kidney disease wasdefined as having a baseline glomerular filtra-tion rate of less than 60 ml/minute/1.73 m2—orstage III chronic kidney disease as defined by theNational Kidney Foundation.16
Hernia Volume and Loss of Domain
When available, preoperative computed tomo-graphic scans were used to calculate the herniasac volume relative to the abdominal cavity vol-ume. Briefly, these volumes are estimated by mul-tiplying the length (l ), width (w ), and height (h )of a hernia sac or abdominal cavity by a constantto generate the volume of an ellipsoid [(l × w × h )× 0.52]. As described previously, the ratio of thehernia sac volume to abdominal cavity volume isreported as a volume ratio percentage.17
Intraabdominal Pressure Measurements
Following induction of general anesthesia, aFoley catheter was placed, as is our current standardof care. Before preparing and draping the patient,intraabdominal pressure was measured by means ofa sterile closed system through the patient’s blad-der catheter. According to World Society of the Abdominal Compartment Syndrome guidelines,25 cc of sterile saline was instilled into a clampedurinary catheter. The table was flattened and the
pressure system was zeroed at the midaxillary line. Aplateau pressure was measured concurrently oncethe patient was confirmed to be adequately anesthe-tized. Following hernia repair with primary fascialclosure, bladder and pulmonary plateau pressuremeasurements were repeated. Patients whoseplateau pressure increased by less than 6 mmHg were extubated once the operation was com-plete. Patients whose pulmonary plateau pressureincreased by greater than 6 mmHg remained intu-bated and were transferred to the surgical intensivecare unit. Once their plateau pressure normalized
to baseline, the patient was extubated. Bladder pres-sure measurements were repeated on the morningof the first postoperative day for all patients—again,the patients were placed in the supine position.Finally, abdominal perfusion pressure was calcu-lated at the time of all bladder pressure measure-ments by subtracting the intraabdominal pressurefrom the mean arterial pressure taken concurrently.
Operative Technique
Patients underwent open incisional herniarepair with a complete adhesiolysis and excision
of all previously placed mesh. Myofascial release

7/25/2019 Permissible Intraabdominal Hypertension Following.40 (1)
http://slidepdf.com/reader/full/permissible-intraabdominal-hypertension-following40-1 3/14
Copyright © 2015 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.
870
Plastic and Reconstructive Surgery • October 2015
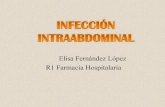
consisted of a retrorectus dissection followed byour previously described transversus abdominismuscle release, and was performed for all patientsincluded in the study. Figures 1 through 3 dem-onstrate lateral retromuscular dissection achievedby a transversus abdominis muscle release.18 Asynthetic or biological prosthetic was placed inthe retrorectus space after the viscera were com-pletely excluded by the posterior fascial layer. Theanterior fascia was closed, reconstructing the lineaalba entirely in all patients, after which postopera-tive pressure measurements were recorded.
Airway Management
All patients received standardized anesthesiacare. Ventilatory support was achieved using a volume control modality, with tidal volumes calcu-
lated from ideal body weight (6 to 8 ml/kg). Pla-teau pressure measurements preoperatively andpostoperatively were based on consistent tidal vol-ume and peak end-expiratory pressure settings.
Outcomes
Outcome measures included patient demo-graphics; operative characteristics; and the incidence
of intraabdominal hypertension, abdominal com-partment syndrome, abdominal perfusion pressureless than 60 mmHg, prolonged intubation, respira-tory events, and acute kidney injury. Intraabdomi-nal hypertension was defined as an intraabdominalpressure greater than 12 mmHg. Abdominal com-
partment syndrome was defined as an intraabdomi-nal pressure greater than 20 mmHg in a patient who remained intubated after their operation for achange in plateau pressure of greater than 6 mmHg.The significant change in plateau pressure indicatesnew pulmonary dysfunction as a consequence ofthe induced intraabdominal pressure from fas-cial closure.15 Respiratory events were defined aseither reintubation or transfer to a higher level ofcare. Acute kidney injury was strictly defined as anincrease in serum creatinine level by 0.3 mg/dl fromthe patient’s baseline.19 Resolution of acute kidney
injury and the need for renal replacement therapy were also chronicled. Finally, hernia outcomes withregard to wound morbidity and recurrence arereviewed for completeness.
Statistical Analysis
Data analysis was performed using GraphPadPrism version 6.0 (GraphPad Software, Inc., La
Fig. 1. Transversus abdominis muscle release technique. ( Above) The
posterior rectus sheath is incised just medial to the linea alba to expose
the rectus muscle. (Below ) The retrorectus plane is then developed lat-
erally to the linea semilunaris, with care taken to preserve the epigastric
vessels. (Reprinted with permission from Novitsky YW. Open retromus-
cular ventral hernia repair. In: Rosen MJ, ed. Atlas of Abdominal Wall
Reconstruction. Philadelphia; Elsevier; 2011:74–96.)

7/25/2019 Permissible Intraabdominal Hypertension Following.40 (1)
http://slidepdf.com/reader/full/permissible-intraabdominal-hypertension-following40-1 4/14
Copyright © 2015 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.
Volume 136, Number 4 • Permissible Intraabdominal Hypertension
871
Jolla, Calif.). Continuous variables were evaluatedusing descriptive statistics, and categorical vari-ables are summarized using frequency and per-centages. Statistical analysis was performed usinga t test for continuous variables and Fisher’s exacttest for categorical variables. A value of p < 0.05 was considered significant.
RESULTSDuring a 6-month period from 2013 to
2014, 50 patients underwent complex abdomi-
nal wall reconstruction with myofascial release
at University Hospitals Case Medical Center.Patient demographics, comorbidities, and opera-tive characteristics are summarized in Table 1.Notably, patients had an average body mass indexof 34.6 ± 6.7 kg/m2, 50 percent had a history ofobstructive sleep apnea or chronic obstructivepulmonary disease, and 18 percent had chronickidney disease. Although 16 percent of patientsquit smoking within 3 months of their operation,all had abstained from smoking for a minimumof 4 weeks. The size of the hernias is character-ized by a mean width of 14.0 ± 5.8 cm and mean
area of 310.5 ± 195.7 cm2
as measured during the
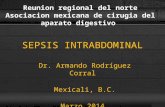
Fig. 2. ( Above) The posterior rectus sheath—just medial to laterally per-
forating neurovascular bundles—is reincised to expose the underly-
ing transversus abdominis muscle. The transversus abdominis muscle
inserts onto the posterior rectus sheath medial to the linea semiluna-
ris, allowing access to this intramuscular plane. (Below ) The transver-
sus abdominis muscle is then carefully elevated and divided from the
underlying transversalis fascia and peritoneum, which remains con-
tiguous with the posterior rectus sheath. (Reprinted with permission
from Novitsky YW. Open retromuscular ventral hernia repair. In: Rosen
MJ, ed. Atlas of Abdominal Wall Reconstruction. Philadelphia; Elsevier;
2011:74–96.)

7/25/2019 Permissible Intraabdominal Hypertension Following.40 (1)
http://slidepdf.com/reader/full/permissible-intraabdominal-hypertension-following40-1 5/14
Copyright © 2015 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.
872
Plastic and Reconstructive Surgery • October 2015
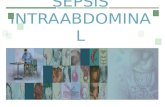
Fig. 3. The retromuscular plane is then developed laterally to the ret-
roperitoneum or psoas muscle. Closure of the posterior rectus sheath
allows placement of a prosthetic in the retromuscular space, followed
by closure of the anterior rectus sheath. Regarding mesh placement, our
preference is to use a 30 × 30-cm piece of uncoated, lightweight, mono-
filament polypropylene for clean and clean-contaminated cases, and a
similar sized non–cross-linked porcine dermis for contaminated cases.
Following closure of the posterior rectus sheath with a running absorb-
able suture, the prosthetic is placed in a diamond fashion in the retro-
muscular space with corners tucked beneath the xiphoid process, pubis,
and laterally into the retroperitoneum to the psoas. Superior, inferior, and
lateral fixation is achieved with no. 1 slowly absorbable monofilament
suture—typically one stitch superior/inferiorly and three laterally on
each side. The anterior fascia is then closed above the mesh. For closures
under a significant amount of tension, interrupted figure-of-eight stitches
with no. 1 slowly absorbable suture are used. Potential benefits of the
transversus abdominis muscle release over other component separationtechniques include the following: obviating any need to raise skin flaps
to access the external oblique muscle, as in a classic anterior component
separation (this may account for our experience of diminished wound
morbidity following a transversus abdominis muscle release compared
to anterior component separation) (Krpata DM, Blatnik JA, Novitsky YW,
Rosen MJ. Posterior and open anterior components separations: A com-
parative analysis. Am J Surg. 2012;203:318–322; discussion 322); release of
a muscle (transversus abdominis) whose vector of force directly opposes
medial traction, compared with the obliques; compared with a lateral
intramuscular dissection (between the internal oblique and transver-
sus abdominis muscle), transversus abdominis muscle release does not
require division of the laterally perforating neurovascular bundles, andtherefore maintains the neurovascular integrity of the abdominal wall (it
is also worth noting that intramuscular dissection and purely preperito-
neal dissections do not offer any myofascial release for medialization);
wide lateral dissection in the retromuscular plane allows for wide overlap
and bilaminar fascial coverage of the prosthetic (transversus abdominis
above and transversalis fascia/peritoneum below) (this allows for giant
prosthetic reinforcement of the visceral sac without direct exposure of
the viscera to a foreign body); and bilaminar fascial coverage of the pros-
thetic also protects the prosthetic from superficial wound morbidity.
(Reprinted with permission from Novitsky YW. Open retromuscular ven-
tral hernia repair. In: Rosen MJ, ed. Atlas of Abdominal Wall Reconstruction.
Philadelphia; Elsevier; 2011:74–96.)

7/25/2019 Permissible Intraabdominal Hypertension Following.40 (1)
http://slidepdf.com/reader/full/permissible-intraabdominal-hypertension-following40-1 6/14
Copyright © 2015 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.
Volume 136, Number 4 • Permissible Intraabdominal Hypertension
873
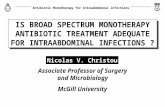
operation. For the 42 preoperative computedtomographic scans available, the mean hernia volume ratio percentage was 13.1 ± 14.2 percent.Figure 4 demonstrates a patient characterized ashaving loss of domain.
Bladder pressure, pulmonary plateau pressure,and abdominal perfusion pressure measurementsrecorded after the induction of anesthesia (preop-erative), following fascial closure (postoperative),
and the morning after the operation (postopera-tive day 1) are listed in Table 2. The mean pre-operative, postoperative, and postoperative day1 intraabdominal pressure measurements—asmeasured by bladder pressure—were 12.7 ± 4.0,18.2 ± 5.4, and 12.9 ± 5.2 mmHg, respectively.
Following repair, 45 of 50 patients (90 percent)demonstrated an increase in intraabdominal pres-sure from baseline, and by postoperative day 1,intraabdominal pressure had decreased in 46 of50 patients (92 percent) since the postoperativemeasurement. The incidence of intraabdominalhypertension was 92 percent immediately follow-ing repair based on the postoperative measure-ment of intraabdominal pressure alone.
The mean preoperative, postoperative, andpostoperative day 1 abdominal perfusion pressuremeasurements were 74.7 ± 15.7, 70.0 ± 14.4, and
74.9 ± 11.6 mmHg, respectively. Following repair,36 of 50 patients (72 percent) demonstrated adecrease in abdominal perfusion pressure frombaseline, and by postoperative day 1, abdomi-nal perfusion pressure had increased in 30 of 50patients (60 percent) since the postoperative mea-surement. The incidence of abdominal perfusionpressure less than 60 mmHg immediately follow-ing repair was 24 percent, and was not associated with adverse outcomes (Table 3).
The mean preoperative and postopera-tive plateau pressure measurements were 17.5
± 3.8 and 21.5 ± 4.7 mmHg, respectively, for allpatients. Following repair, 48 of 50 patients (96percent) demonstrated an increase in pulmonaryplateau pressure. Ten patients (20 percent) withan increase in plateau pressure by greater than 6mmHg remained intubated after their operation, with a mean postoperative plateau pressure of 27.4± 4.0 mmHg compared with 19.9 ± 3.8 mmHg forthose who were extubated. Of these 10, eight hada postoperative intraabdominal pressure greaterthan 20 mmHg and were designated as havingabdominal compartment syndrome. Patients who
remained intubated had a mean plateau pressureof 20.1 ± 3.7 mmHg on the morning of postopera-tive day 1, and all demonstrated a decrease fromtheir immediate postoperative plateau pressuremeasurement (Fig. 5).
Variables associated with an increase in pla-teau pressure by greater than 6 mmHg after her-nia repair are summarized in Table 4. Underlyinglung disease (obstructive sleep apnea or chronicobstructive pulmonary disease), hernia width, her-nia area, postoperative intraabdominal pressureand plateau pressure, change in intraabdominal
pressure and abdominal perfusion pressure after
Table 1. Patient Demographics and OperativeCharacteristics
Variable Value
No. of patients 50Female 56%Mean age ± SD 59.6 ± 12.9 yrMean BMI ± SD 34.6 ± 6.7 kg/m2
Diabetes 40%
Smoking history 22%Smoking within 3 mo 16%COPD 18%History of wound infection 24%Chronic kidney disease 18%Obstructive sleep apnea 32%Cirrhosis 2%Hernia width, cm Mean ± SD 14.0 ± 5.8 Range 8–40Hernia length, cm Mean ± SD 20.3 ± 6.2 Range 4–30Hernia area, cm2
Mean ± SD 310.5 ± 195.7Range 20–1200
VR = HSV/ACV Mean ± SD 13.1 ± 14.2%Range 0.3 – 51.1%
OR time, min Mean ± SD 256.0 ± 114.0
Range 156–616Technique Transversus abdominis muscle release 100%Prosthetic Lightweight polypropylene 78% Heavyweight polypropylene 16% Non–cross-linked porcine
dermis (Strattice; LifeCell Corp.,Branchburg, N.J.) 6%
Operative I/O In, ml
Mean ± SD 2495.0 ± 1136.2 Range 600–5500 Total out, ml Mean ± SD 633.8 ± 380.9 Range 5–1300 EBL, ml Mean ± SD 167.8 ± 160.9 Range 5–500 Urine output, ml Mean ± SD 475.8 ± 279.1 Range 80–1450 Net I/O, ml Mean ± SD 1886.0 ± 927.8 Range 150–4150
BMI, body mass index; COPD, chronic obstructive pulmonary disease; VR, volume ratio; HSV, hernia sac volume; ACV, abdominal cavity vol-
ume; OR, operating room; I/O, in/out; EBL, estimated blood loss.

7/25/2019 Permissible Intraabdominal Hypertension Following.40 (1)
http://slidepdf.com/reader/full/permissible-intraabdominal-hypertension-following40-1 7/14
Copyright © 2015 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.
874
Plastic and Reconstructive Surgery • October 2015
repair, operative time, volume ratio percentageand volume ratio greater than 20 percent were allassociated with an increase in plateau pressure bygreater than 6 mmHg ( p < 0.05). Although a posi-tive fluid balance during the operation and imme-diate postoperative course (“In”) was associated with patients who remained intubated, the dis-crepancy becomes equivalent when corrected forthe operative time. Finally, patients who had an
elevated plateau pressure of greater than 6 mmHg
were more likely to have a respiratory event aftertheir extubation ( p = 0.01).
Other factors associated with respiratory eventsare summarized in Table 5. Other than remain-ing intubated for a plateau pressure greater than6 mmHg, volume ratio; volume ratio percentagegreater than 20 percent; and net fluid balance onpostoperative days 0, 2, and 3 were all associated
with developing a respiratory event. Measure-ments of intraabdominal pressure, abdominalperfusion pressure, and plateau pressure were notsignificantly different between the two groups.
Variables associated with the development ofacute kidney injury are summarized in Table 6. Apreoperative glomerular filtration rate less than60 ml/minute/1.73 m2, elevated baseline plateaupressure, and elevated postoperative plateau pres-sure were all associated with postoperative acutekidney injury. Intraabdominal pressure, abdominalperfusion pressure, change in plateau pressure,
and fluid balance had no independent relationship with this outcome measure. All 10 cases of acutekidney injury resolved by the time of discharge andnone required renal replacement therapy.
Finally, surgical outcomes are summarized inTable 7. Wound morbidity (16 percent) consistedof three seromas, three superficial surgical-siteinfections, one deep surgical-site infection, andone hematoma. There were no instances of meshinfection, excision, or enterocutaneous fistula for-mation, and all wounds eventually healed. Withlimited mean follow-up of 5.2 months, one recur-
rence was documented at 14 months.
Fig. 4. Preoperative (left ) and postoperative (right ) representation of “loss of domain.”
Table 2. Bladder, Plateau, and Abdominal PerfusionPressure Measurements
Variable Value* Range
Bladder pressure, mmHg Preoperative 12.7 ± 4.0 4–22 Immediate postoperative 18.2 ± 5.4 6–34 POD 1 12.9 ± 5.2 2–24 Abdominal perfusion
pressure, mmHg
Preoperative 74.7 ± 15.7 49–108 Immediate postoperative 70.0 ± 14.4 42–97 POD 1 74.9 ± 11.6 51–99Plateau pressure, mmHg Preoperative 17.5 ± 3.8 10–25 Immediate postoperative, all 21.5 ± 4.7 12–32 Extubated patients 19.9 ± 3.8 12–26 Remained intubated
(increased >6 mmHg) 27.4 ± 4.0 20–32 POD 1, if kept intubated 20.1 ± 3.7 16–27Intraabdominal hypertension
(IAP >12) 92% — Abdominal compartment
syndrome† 16% — Abdominal perfusion pressure
<60 mmHg 24% —
POD, postoperative day; IAP, intraabdominal pressure.*Mean ± SD or %.†IAP >20 and patient remained intubated (i.e., organ dysfunction).

7/25/2019 Permissible Intraabdominal Hypertension Following.40 (1)
http://slidepdf.com/reader/full/permissible-intraabdominal-hypertension-following40-1 8/14
Copyright © 2015 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.
Volume 136, Number 4 • Permissible Intraabdominal Hypertension
875
DISCUSSIONElective complex hernia repair requiring
myofascial release can generate elevated intraab-
dominal pressure immediately following repair,
the time course and clinical significance of which were previously unknown. Following these repairs, we frequently demonstrated diagnostic criteria
for intraabdominal hypertension, abdominal
Table 3. Postoperative Abdominal Perfusion Pressure <60 mmHg
Variable APP <60 mmHg APP >60 mmHg p
No. of patients 112 38Female 8 19 0.5 Age, yr 66.2 ± 9.2 57.3 ± 13.4 0.038*BMI, kg/m2 34.4 ± 5.3 34.8 ± 7.2 0.85
Underlying COPD or OSA 5 13 0.73Hernia width, cm 13.6 ± 4.9 14.2 ± 6.2 0.76Hernia area, cm2 337 ± 193 306 ± 203 0.68 VR% 15.8 ± 13.4 12.4 ± 14.8 0.52 VR >20% 4/10 6/31 0.22IAP Postoperative 20.9 ± 6.7 17.2± 4.6 0.037* ∆ (postoperative – preoperative) 7.9 ± 5.4 4.4 ± 3.7 0.015* POD 1 12.9 ± 5.3 12.9 ± 5.4 0.98 APP Postoperative 52 ± 6.2 75.7 ± 11 <0.001* ∆ (postoperative – preoperative) 20.2 ± 14.3 −0.2 ± 17.9 <0.001* POD 1 73 ± 4 75.4 ± 13.1 0.53Plateau Preoperative 17.7 ± 3.3 17.2 ± 3.9 0.24 Postoperative 23.1 ± 4.3 21± 4.9 0.17
∆ (postoperative – preoperative) 4.5 ± 3.1 3.8 ± 3.8 0.57Remained intubated 4 6 0.23OR time, min 280 ± 149 245 ± 101 0.35OR I/Os Net I/O 1966 ± 905 1825 ± 942 0.65 Total In 2576 ± 1289 2438 ± 1096 0.72 Total Out 610 ± 494 646 ± 351 0.78 EBL 211 ± 251 153 ± 119 0.29 Urine output 435 ± 252 453 ± 296 0.56Net I/O POD 0 1345 ± 1076 732 ± 1106 0.1 POD 1 547 ± 1337 1022 ± 1381 0.3 AKI 3 7 0.68RE (transfer to SICU) 2 4 0.62
APP, abdominal perfusion pressure; BMI, body mass index; COPD, chronic obstructive pulmonary disease; OSA, obstructive sleep apnea; VR%, volume ratio percentage; VR, volume ratio; IAP, intraabdominal pressure; POD, postoperative day; OR, operating room; I/O, in/out; EBL,
estimated blood loss; AKI, acute kidney injury; RE, reintubation; SICU, surgical intensive care unit.*Statistically significant.
Fig. 5. Plateau pressure (in millimeters of mercury) for intubated and
extubated patients.

7/25/2019 Permissible Intraabdominal Hypertension Following.40 (1)
http://slidepdf.com/reader/full/permissible-intraabdominal-hypertension-following40-1 9/14
Copyright © 2015 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.
876
Plastic and Reconstructive Surgery • October 2015
compartment syndrome, or abdominal perfusionpressure less than 60 mmHg that consistently nor-malized by the morning of the first postoperativeday. Pulmonary plateau pressure measurements were associated with postoperative respiratoryevents and acute kidney injury, suggesting that
plateau pressure is a meaningful surrogate formeasuring the physiologic sequelae of elective pri-mary fascial approximation. Transient changes inintraabdominal pressure following complex her-nia repair requiring myofascial releases that resultin frequent diagnoses of intraabdominal hyper-tension or abdominal compartment syndromeshould be viewed as permissible in the aforemen-tioned context. Aggressive methods to correct oravoid these changes are likely unwarranted in thisdistinct scenario.
As recognized by the World Society of the
Abdominal Compartment Syndrome, intraab-dominal hypertension and abdominal compart-ment syndrome have traditionally been diagnosesrecognized in the critically ill.8–14 Growing aware-ness of these syndromes has led to earlier detectionand therapeutic intervention to avert subsequentpatient morbidity and mortality.6,20–23 In its mostrecent clinical practice guidelines, the World Soci-ety of the Abdominal Compartment Syndromeoutlines the treatment of primary or secondaryabdominal compartment syndrome with neworgan dysfunction: “perform/revise abdominal
decompression with temporary abdominal closureas needed to reduce intraabdominal pressure.”1 After complex hernia repair requiring myofascialrelease, 38 percent of our patients had an intraab-dominal pressure greater than 20 mmHg and 16percent—having both an intraabdominal pres-sure greater than 20 mmHg and new respiratorycompromise caused by an increase in pulmonaryplateau pressure of greater than 6 mmHg—wouldcarry a diagnosis of abdominal compartmentsyndrome. By the following morning, the uni-form decrease in plateau pressure of those who
remained intubated and consistent resolution ofelevated intraabdominal pressure and diminishedabdominal perfusion pressure suggest that thesechanges are transient. Clearly, the elective natureof these cases and use of myofascial release cre-ates a patient cohort very different from the con-text in which intraabdominal hypertension andabdominal compartment syndrome is typicallyencountered.
The use of myofascial release during repair—specifically, the transversus abdominis muscle—provides a theoretical mechanism to explain the
subacute resolution of elevated intraabdominal
pressure. The transversus abdominis muscleis critical to the generation of intraabdominalpressure.24–26 Specifically, more than any otherabdominal muscle, transversus abdominis activ-ity has been shown to most closely correlate withchanges in intraabdominal pressure in a normal
physiologic state.26 Rationally, its release lim-its the ability of patients to somatically generateincreased intraabdominal pressure. Furthermore,incising the posterior rectus sheath and trans- versus abdominis muscle allows the remainingabdominal fascia to stretch and accommodatethe added viscera when the abdominal domainis reestablished. Compared with division of theoblique muscles, one would expect division ofthe transversus abdominis muscle—whose vectorof force directly opposes fascial medialization—to provide optimal myofascial advancement.
The initial elevation in intraabdominal pressureimmediately following primary fascial approxima-tion, before systemic paralysis has subsided, andconsistent improvement in intraabdominal pres-sure by morning indicates that the abdominal wallhas stretched to accommodate the newly added viscera.
Not uncommonly, traditional definitions andparadigms require modification as additionalexperience accrues. The recognition of permissi-ble hypercapnia as an acceptable consequence ofefforts to reduce ventilator-associated lung injury
illustrates such adaptation. Specifically in the set-ting of acute lung injury and acute respiratory dis-tress syndrome, low tidal volumes have consistentlydemonstrated reduced mortality and reduced ventilator days.27–29 A sequela of the reduced min-ute ventilation generated from low tidal volumesis commonly a hypercapnic acidosis. The signifi-cant benefits of low tidal volume therapy and therelative safety of a mild respiratory acidosis led toa description of this clinical scenario as “permis-sible hypercapnia.”30,31 This example underscoresthe notion that producing physiologic normalcy
in the face of extreme conditions is not always inthe patient’s best interest. Likewise, we suggestthat intraabdominal hypertension or abdominalcompartment syndrome immediately followingan elective hernia repair creates a scenario thatmust be distinguished from the settings in whichthese terms were originally defined. Surely, revi-sion of an abdominal wall closure in a patient with elevated intraabdominal pressure who hada ruptured abdominal aortic aneurysm or openabdomen after a penetrating abdominal injury would be entertained in a different fashion than
in a patient whose primary elective procedure was

7/25/2019 Permissible Intraabdominal Hypertension Following.40 (1)
http://slidepdf.com/reader/full/permissible-intraabdominal-hypertension-following40-1 10/14
Copyright © 2015 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.
Volume 136, Number 4 • Permissible Intraabdominal Hypertension
877
a definitive abdominal wall reconstruction. Possi-bly, our data will shed light on the natural timecourse of these transient elevations in intraab-dominal pressure following elective hernia repair with myofascial release and its relative safety.
To support the allowance of transientlyelevated intraabdominal pressure in the afore-mentioned context, we sought to ensure thatnegative outcomes were not associated withshort-lived changes in intraabdominal pressure
and abdominal perfusion pressure. Specifically,acute kidney injury has long been associated with intraabdominal hypertension and abdom-inal compartment syndrome.32–34 We foundthat changes in intraabdominal pressure andabdominal perfusion pressure were not statis-tically different in the 10 patients who had anincrease in serum creatinine of 0.3 mg/dl frombaseline. Importantly, all cases of acute kidneyinjury resolved by the initial hospital stay, andnone required renal replacement therapy. Inter-estingly, baseline and postoperative plateau
pressure measurement (but not the change in
plateau pressure alone) were the only variablesthat were found to be statistically associated withacute kidney injury. To our knowledge, this is thefirst time such an association has been reported. Although a straightforward mechanism forthis relationship is difficult to conceive, onemight speculate that elevated plateau pressureis an overall indicator of poor health, such thatunderlying associations with smoking, obesity,and diabetes could also contribute to marginal
or diminished renal function. Although an asso-ciation with elevated plateau pressure is note- worthy, a history of underlying kidney diseasehad a more significant impact on the develop-ment of postoperative acute kidney injury thantransient elevations in intraabdominal pressure,and those episodes that did occur were of littlelong-term significance. Thus, although impairedrenal function is a frequent sequela of abdomi-nal compartment syndrome, this does not seemto correlate with transient elevations in intraab-dominal pressure following complex abdominal
wall reconstruction requiring myofascial release.
Table 4. Change in Plateau Pressure >6 mmHg for Patients Who Remained Intubated*
Variable Remained Intubated (n = 10) Extubated (n = 40) p
∆ (postoperative − preoperative) plateau pressure 8.5 ± 3.8 2.9 ± 2.5 <0.001†Female 5 23 0.73 Age, yr 64.3 ± 8.4 58.4 ± 13.6 0.19BMI, kg/m2 37.6 ± 2.1 33.7 ± 1.0 0.09
Underlying COPD or OSA 7 12 0.03†Hernia width, cm 21.3 ± 2.8 12.6 ± 0.6 <0.001†Hernia area, cm2 572.5 ± 98.7 252.3 ± 18.6 <0.001† VR% 35.2 ± 9.8 7.8 ± 9.2 <0.001† VR >20% 8/8 2/34 <0.001†IAP Postoperative 22.3 ± 4.2* 17.2 ± 5.2 0.006† ∆ (postoperative − preoperative) 9.8 ± 4.0 4.4 ± 4.2 <0.001† POD 1 14.3 ± 6.0 12.6 ± 5.1 0.36 APP Postoperative 64.6 ± 16.2 71.3 ± 13.8 0.19 ∆ (postoperative − preoperative) −21.0 ± 15.0 −0.6 ± 17.7 0.001† POD 1 79.9 ± 12.6 73.6 ± 11.1 0.12Plateau pressure Preoperative 18.9 ± 4.5 17.2 ± 3.5 0.21 Postoperative 27.4 ± 4 20.1 ± 3.7 <0.001†
OR time, min 374.2 ± 115.1 226.4 ± 93.8 <0.001†OR I/O Net In/Out 2504 ± 708 1723 ± 929 0.02† Total In 3326 ± 785 2285 ± 1134 0.009† In/Or time, ml/min 6.9 ± 1.6 8.3 ± 9.2 0.58 Total Out 821 ± 378 591 ± 375 0.09 EBL 250 ± 100 149 ± 169 0.07 Urine output 571 ± 341 453 ± 263 0.24 AKI 4 6 0.10Respiratory event 4 2 0.01†
BMI, body mass index; COPD, chronic obstructive pulmonary disease; OSA, obstructive sleep apnea; VR%, volume ratio percentage; VR, volume ratio; IAP, intraabdominal pressure; POD, postoperative day; APP, abdominal perfusion pressure; OR, operating room; I/O, in/out;EPL, estimated blood loss; AKI, acute kidney injury.*Eight patients who remained intubated had a postoperative IAP >20 mmHg, providing criteria for a diagnosis of abdominal compartmentsyndrome.†Statistically significant.

7/25/2019 Permissible Intraabdominal Hypertension Following.40 (1)
http://slidepdf.com/reader/full/permissible-intraabdominal-hypertension-following40-1 11/14
Copyright © 2015 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.
878
Plastic and Reconstructive Surgery • October 2015
Regarding the development of postoperativerespiratory events, again changes in intraabdom-inal pressure and abdominal perfusion pres-sure were not predictive of such complications. Although change in plateau pressure alone wasnot predictive of respiratory events as a continu-ous variable, remaining intubated for an increase
in plateau pressure by greater than 6 mmHg fol-lowing repair was predictive.15 Of the 10 patients who remained intubated after their operation, all were extubated on postoperative day 1 because ofan improvement in plateau pressure by a mean of6.8 mmHg. Of these patients, four (40 percent)developed a respiratory event after extubation,accounting for 66 percent of these cases. Thisindicates that, although keeping patients intu-bated after their operation for an increase in pla-teau pressure greater than 6 mmHg allows for animprovement in intraabdominal pressure, abdom-
inal perfusion pressure, and plateau pressure by
the following morning, these patients are still atrisk for respiratory events after extubation. Theimprovement in intraabdominal pressure param-eters should not beget a false sense of security,and these patients should still be monitored care-fully in the early postoperative period for acuterespiratory failure.
Being able to predict which patients wouldsuccumb to respiratory compromise—as definedby an increase in plateau pressure of greater than6 mmHg—would be invaluable in terms of identi-fying high-risk patients with critical care needs inthe immediate postoperative period. Although itis not surprising that a history of underlying lungdisease was predictive in this regard, we also iden-tified hernia volume ratio percentage as an impor-tant predictor for patients who would remainintubated. A volume ratio percentage greaterthan 20 percent was present in all patients who
would develop an increase in plateau pressure
Table 5. Respiratory Events*
Variable Respiratory Events No Respiratory Events p
No. of patients 6 44Female 2 26 0.38 Age, yr 68.8 ± 6.7 58.3 ± 13.0 0.06BMI, kg/m2 38.4 ± 8.1 34.0 ± 6.4 0.13
Underlying COPD or OSA 5 14 0.47Hernia width, cm 17.0 ± 3.2 13.7 ± 6.0 0.23Hernia area, cm2 436 ± 140 295 ± 199 0.13 VR% 28.1 ± 17.2 11.5 ± 13.2 0.025† VR >20% 3/4 7/38 0.036†IAP Postoperative 19.8 ± 4.7 18.0 ± 5.5 0.45 ∆ (postoperative − preoperative) 7.8 ± 4.8 5.2 ± 4.6 0.20 POD 1 13.3 ± 6.5 12.9 ± 5.1 0.84 APP Postoperative 67.6 ± 13.9 70.3 ± 14.6 0.66 ∆ (postoperative − preoperative) −13.7 ± 8.9 −3.5 ± 19.7 0.22 POD 1 94.7 ± 12.4 86.8 ± 10.8 0.11Plateau Preoperative 18.3 ± 5.3 17.4 ± 3.6 0.59 Postoperative 24.3 ± 5.6 21.2 ± 4.6 0.13
∆ (preoperative − postoperative) 6.0 ± 2.4 3.7 ± 3.6 0.15Remained intubated 4 6 0.01†OR time, min 327 ± 114 246 ± 112 0.10OR In/Out Net In/Out 2365 ± 750 1822 ± 949 0.19 Total In 3083 ± 861 2422 ± 1166 0.19 Total Out 718 ± 321 628 ± 393 0.59 EBL 225 ± 94 162 ± 168 0.38 Urine output 493 ± 289 476 ± 284 0.24Net I/O POD 0 2030 ± 1802 716 ± 902 0.005† POD 1 1251 ± 1779 888 ± 1325 0.54 POD 2 943 ± 387 −136 ± 1278 0.047† POD 3 668 ± 537 −330 ± 1054 0.03† AKI 3 7 0.10
BMI, body mass index; COPD, chronic obstructive pulmonary disease; OSA, obstructive sleep apnea; VR%, volume ratio percentage; VR, volume ratio; IAP, intraabdominal pressure; POD, postoperative day; APP, abdominal perfusion pressure; OR, operating room; I/O, in/out;EPL, estimated blood loss; AKI, acute kidney injury.*Transfer to surgical intensive care unit or reintubated.†Statistically significant.

7/25/2019 Permissible Intraabdominal Hypertension Following.40 (1)
http://slidepdf.com/reader/full/permissible-intraabdominal-hypertension-following40-1 12/14
Copyright © 2015 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.
Volume 136, Number 4 • Permissible Intraabdominal Hypertension
879
of greater than 6 mmHg and remain intubated.Only two patients demonstrated a hernia volumeratio greater than 20 percent and were able to be
extubated, and these exceptions are accountedfor by abdominal compliance. For instance, amore compliant abdominal wall would allow forthe return of a large volume ratio percentage
without causing a substantial increase in intraab-dominal pressure. Still, volume ratio percentageis tremendously sensitive, easily calculated frompreoperative computed tomographic scan (whenavailable), and can serve as a useful tool in iden-tifying high-risk patients who will require closeobservation in the critical care unit in the imme-diate postoperative period.
Although our aim was to characterize the safetyand transient nature of postoperative intraabdomi-nal pressure following complex hernia repair, itis necessary to acknowledge that every hernia is
not safe to close. Unfortunately, understanding
Table 6. Acute Kidney Injury
Variable AKI No AKI p
No. of patients 10 40Female 6 22 1.00 Age, yr 62.6 ± 13.4 58.8 ± 12.8 0.41BMI, kg/m2 36.2 ± 9.0 34.1 ± 6.1 0.39
Preoperative GFR <60 6 3 0.001*DM 6 15 0.29COPD 4 5 0.07Hernia width, cm 13.4 ± 3.8 14.2 ± 6.2 0.73Hernia area, cm2 313 ± 164 309 ± 206 0.97 VR% 14.6 ± 17.7 12.7 ± 13.6 0.71 VR >20% 3/8 7/34 0.37IAP Postoperative 19.7 ± 4.4 17.9 ± 5.6 0.34 ∆ (postoperative − preoperative) 6.5 ± 6.5 5.2 ± 4.2 0.46 POD 1 13.4 ± 4.2 12.8 ± 5.5 0.76 APP Postoperative 68.9 ± 15.3 70.2 ± 14.3 0.79 ∆ (postoperative − preoperative) −9.4 ± 22.3 −3.5 ± 18.2 0.39 POD 1 76.1 ± 16.3 74.5 ± 10.3 0.60Plateau
Preop 20.2 ± 4.0 16.9 ± 3.5 0.01* Postoperative 24.3 ± 6.3 20.9 ± 4.1 0.04* ∆ (preoperative – postoperative) 4.1 ± 2.3 4.0 ± 0.6 0.92Remained intubated 4 6 0.10OR time, min 248 ± 99 258 ± 119 0.80OR In/Out Net In/Out 1897 ± 757 1892 ± 985 0.98 Total In 2244 ± 1005 2568 ± 1180 0.45 Total Out 668 ± 456 632 ± 371 0.80 EBL 173 ± 136 170 ± 169 0.95 Urine output 495 ± 390 475 ± 256 0.85POD 0
In 2640 ± 1479 2017 ± 924 0.22 OP 832 ± 164 978 ± 542 0.15 Net I/O 1465 ± 1491 726 ± 965 0.06Net I/O
POD 1 1485 ± 1552 793 ± 1306 0.13 POD 2 248 ± 1045 −70 ± 1306 0.51 POD 3 173 ± 621 −306 ± 1122 0.20Respiratory event 3 3 0.09
AKI, acute kidney injury; BMI, body mass index; GFR, glomerular filtration rate; DM, diabetes mellitus; COPD, chronic obstructive pulmonarydisease; VR, volume ratio; IAP, intraabdominal pressure; POD, postoperative day; APP, abdominal perfusion pressure; OR, operating room;I/O, in/out; EPL, estimated blood loss.*Statistically significant.
Table 7. Outcomes
Variable Value (%)
Mean follow-up, mo 5.2 ± 4.7 Wound morbidity SSO 8/50 (16) Enterocutaneous fistula 0/50 (0) Hematoma 1/50 (2) Seroma 4/50 (8) SSI Superficial 3/50 (6) Deep 1/50 (2)Recurrence No. (%) 1/50 (2) Time to recurrence, mo 14
SSO, surgical-site outcome; SSI, surgical-site infection.

7/25/2019 Permissible Intraabdominal Hypertension Following.40 (1)
http://slidepdf.com/reader/full/permissible-intraabdominal-hypertension-following40-1 13/14
Copyright © 2015 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.
880
Plastic and Reconstructive Surgery • October 2015
the limitations of abdominal wall reconstructionis incredibly difficult and certainly an ongoingstruggle by the authors. We do not have any formalcriteria for denying patients surgery. It is always sur-prising to us how some abdominal walls will cometogether and some will not. We certainly do denypatients surgery, but often for medical reasons suchas home oxygen use, morbid obesity, or smoking. Although baseline plateau pressures likely wouldnot be used to negate a repair—as we would alreadybe in the operating room—we do feel that thesepressures can be used to guide the surgeon as to whether it is appropriate to attempt muscular clo-sure or a bridging repair. Likewise, these numberscan be used to follow the clinical course or suggestappropriate level of care for these complex patients.
CONCLUSIONSElevations in intraabdominal pressure after
abdominal wall reconstruction requiring myofas-cial release are both common and transient. Theassociation between postoperative respiratoryevents and acute kidney injury with plateau pres-sure makes it a valuable measurement in terms ofcorrelating the physiologic impact of reestablish-ing abdominal domain with meaningful outcomeparameters. Patients who remain intubated for anincrease in plateau pressure—identified preop-eratively as having a hernia volume ratio percent-
age of greater than 20 percent—are still at risk forrespiratory events after extubation, despite thenormalization in intraabdominal pressure. Thesefindings should characterize elevated intraab-dominal pressure in the context of abdominal wall reconstruction requiring myofascial release.
Clayton C. Petro, M.D.Department of General Surgery
11100 Euclid Avenue7th Floor Lakeside
Cleveland, Ohio [email protected]
REFERENCES
1. Kirkpatrick AW, Roberts DJ, De Waele J, et al. Intra-abdominalhypertension and the abdominal compartment syndrome:Updated consensus definitions and clinical practice guide-lines from the World Society of the Abdominal CompartmentSyndrome. Intensive Care Med . 2013;39:1190–1206.
2. Diebel LN, Dulchavsky SA, Wilson RF. Effect of increasedintra-abdominal pressure on mesenteric arterial and intesti-nal mucosal blood flow. J Trauma 1992;33:45–48; discussion48–49.
3. Schein M, Ivatury R. Intra-abdominal hypertensionand the abdominal compartment syndrome. Br J Surg .
1998;85:1027–1028.
4. Ivatury RR, Diebel L, Porter JM, Simon RJ. Intra-abdominalhypertension and the abdominal compartment syndrome.Surg Clin North Am . 1997;77:783–800.
5. Caldwell CB, Ricotta JJ. Changes in visceral blood flow withelevated intraabdominal pressure. J Surg Res . 1987;43:14–20.
6. Cheatham ML, White MW, Sagraves SG, Johnson JL, BlockEF. Abdominal perfusion pressure: A superior parameter in
the assessment of intra-abdominal hypertension. J Trauma 2000;49:621–626; discussion 626–627.
7. Balogh Z, De Waele JJ, Kirkpatrick A, et al. Intra-abdominalpressure measurement and abdominal compartment syn-drome: The opinion of the World Society of the AbdominalCompartment Syndrome. Crit Care Med . 2007;35:677–678;author reply 678–679.
8. Malbrain ML, Cheatham ML, Kirkpatrick A, et al. Resultsfrom the international conference of experts on intra-abdominal hypertension and abdominal compartment syn-drome: I. Definitions. Intensive Care Med . 2006;32:1722–1732.
9. Malbrain ML, Chiumello D, Pelosi P, et al. Incidence andprognosis of intraabdominal hypertension in a mixed popu-lation of critically ill patients: A multiple-center epidemio-logical study. Crit Care Med . 2005;33:315–322.
10. Malbrain ML, Chiumello D, Pelosi P, et al. Prevalenceof intra-abdominal hypertension in critically ill patients: A multicentre epidemiological study. Intensive Care Med .2004;30:822–829.
11. Balogh Z, McKinley BA, Cocanour CS, et al. Secondaryabdominal compartment syndrome is an elusive earlycomplication of traumatic shock resuscitation. Am J Surg .2002;184:538–543; discussion 543–544.
12. Sugrue M. Abdominal compartment syndrome. Curr OpinCrit Care 2005;11:333–338.
13. Ivatury RR, Sugerman HJ, Peitzman AB. Abdominal com-partment syndrome: Recognition and management. AdvSurg . 2001;35:251–269.
14. Malbrain ML. Is it wise not to think about intraabdominal
hypertension in the ICU? Curr Opin Crit Care 2004;10:132–145. 15. Blatnik JA, Krpata DM, Pesa NL, et al. Predicting severe post-
operative respiratory complications following abdominal wall reconstruction. Plast Reconstr Surg . 2012;130:836–841.
16. Moschella C. National Kidney Foundation developspractice guidelines for chronic kidney disease. JAAPA 2003;16:17–18.
17. Tanaka EY, Yoo JH, Rodrigues AJ Jr, Utiyama EM, BiroliniD, Rasslan S. A computerized tomography scan method forcalculating the hernia sac and abdominal cavity volume incomplex large incisional hernia with loss of domain. Hernia 2010;14:63–69.
18. Novitsky YW, Elliott HL, Orenstein SB, Rosen MJ. Transversusabdominis muscle release: A novel approach to posteriorcomponent separation during complex abdominal wall
reconstruction. Am J Surg . 2012;204:709–716. 19. Khwaja A. KDIGO clinical practice guidelines for acute kid-
ney injury. Nephron Clin Pract. 2012;120:c179–c184. 20. Cheatham ML, Safcsak K, Llerena LE, Morrow CE Jr, Block
EF. Long-term physical, mental, and functional consequencesof abdominal decompression. J Trauma 2004;56:237–241;discussion 241–242.
21. Balogh Z, McKinley BA, Holcomb JB, et al. Both primaryand secondary abdominal compartment syndrome can bepredicted early and are harbingers of multiple organ failure. J Trauma 2003;54:848–859; discussion 859–861.
22. Hong JJ, Cohn SM, Perez JM, Dolich MO, Brown M,McKenney MG. Prospective study of the incidence and out-come of intra-abdominal hypertension and the abdominal
compartment syndrome. Br J Surg . 2002;89:591–596.

7/25/2019 Permissible Intraabdominal Hypertension Following.40 (1)
http://slidepdf.com/reader/full/permissible-intraabdominal-hypertension-following40-1 14/14
Volume 136, Number 4 • Permissible Intraabdominal Hypertension
881
23. Balogh Z, McKinley BA, Cocanour CS, et al. Supranormaltrauma resuscitation causes more cases of abdominal com-partment syndrome. Arch Surg . 2003;138:637–642; discussion642–643.
24. De Troyer A, Estenne M, Ninane V, Van Gansbeke D, GoriniM. Transversus abdominis muscle function in humans. J ApplPhysiol (1985) 1990;68:1010–1016.
25. Cresswell AG, Oddsson L, Thorstensson A. The influ-ence of sudden perturbations on trunk muscle activity andintra-abdominal pressure while standing. Exp Brain Res .1994;98:336–341.
26. Cresswell AG, Grundstrom H, Thorstensson A. Observationson intra-abdominal pressure and patterns of abdominal intra-muscular activity in man. Acta Physiol Scand . 1992;144:409–418.
27. Ventilation with lower tidal volumes as compared with tradi-tional tidal volumes for acute lung injury and the acute respi-ratory distress syndrome. The Acute Respiratory DistressSyndrome Network. N Engl J Med . 2000;342:1301–1308.
28. Putensen C, Theuerkauf N, Zinserling J, Wrigge H, PelosiP. Meta-analysis: Ventilation strategies and outcomes of the
acute respiratory distress syndrome and acute lung injury.Ann Intern Med . 2009;151:566–576.
29. Petrucci N, De Feo C. Lung protective ventilation strategyfor the acute respiratory distress syndrome. Cochrane DatabaseSyst Rev . 2013;2:CD003844.
30. Tuxen DV. Permissive hypercapnic ventilation. Am J RespirCrit Care Med . 1994;150:870–874.
31. Mackenzie I. Core Topics in Mechanical Ventilation . Cambridge:Cambridge University Press; 2008.
32. Sugrue M, Buist MD, Hourihan F, Deane S, Bauman A,Hillman K. Prospective study of intra-abdominal hyper-tension and renal function after laparotomy. Br J Surg .1995;82:235–238.
33. Sugrue M, Jones F, Deane SA, Bishop G, Bauman A,Hillman K. Intra-abdominal hypertension is an indepen-dent cause of postoperative renal impairment. Arch Surg .1999;134:1082–1085.
34. De Waele JJ, De Laet I, Kirkpatrick AW, Hoste E. Intra-abdominal hypertension and abdominal compartment syn-drome. Am J Kidney Dis . 2011;57:159–169.
American Society of Plastic Surgeons Mission Statement The mission of the American Society of Plastic Surgeons is to support its members in their efforts to provide
the highest quality patient care and maintain professional and ethical standards through education, research,
and advocacy of socioeconomic and other professional activities.