Gastroenterology Review. Gastroenterology History Dyspepsia & Heartburn Dyspepsia & Heartburn...
108
Gastroenterology Gastroenterology Review Review
-
Upload
ira-spencer -
Category
Documents
-
view
246 -
download
4
Transcript of Gastroenterology Review. Gastroenterology History Dyspepsia & Heartburn Dyspepsia & Heartburn...
Gastroenterology Gastroenterology ReviewReview
Gastroenterology HistoryGastroenterology History Dyspepsia & HeartburnDyspepsia & Heartburn Dysphagia & OdynophagiaDysphagia & Odynophagia Nausea and vomitingNausea and vomiting Abdoinal painAbdoinal pain Abdominal swellingAbdominal swelling Appetite/weight gainAppetite/weight gain DiarrhoeaDiarrhoea ConstipationConstipation BleedingBleeding JaundiceJaundice PruritusPruritus
DyspepsiaDyspepsia&&
Peptic Ulcer Peptic Ulcer DiseaseDisease
DYSPEPSIA DYSPEPSIA (INDIGESTION )(INDIGESTION )
UPPER ABDOMINAL UPPER ABDOMINAL SYMPTOMSSYMPTOMS
*EPIGASTRIC PAIN .*EPIGASTRIC PAIN .
*BLOATING.*BLOATING.
*FULLNESS.*FULLNESS.
* BELCHING. * BELCHING.
*HEARTBURN .*HEARTBURN .
*NAUSIA & VOMITING*NAUSIA & VOMITING
*EARLY SATIETY.*EARLY SATIETY.

DyspepsiaDyspepsia Common problem in the community - affects Common problem in the community - affects
up to 40% of individuals in 1 yearup to 40% of individuals in 1 year Up to 60% of patients do not have an Up to 60% of patients do not have an
identifiable organic cause - “functional”identifiable organic cause - “functional” Nevertheless can be the presenting symptom Nevertheless can be the presenting symptom
of a number of serious conditionsof a number of serious conditions May be the only symptom of malignancyMay be the only symptom of malignancy Has Eesophageal, Stomach and Duodenal Has Eesophageal, Stomach and Duodenal
pathologiespathologies May indicate underlying gallstone diseaseMay indicate underlying gallstone disease Warrants OGD in patients over 55 or with Warrants OGD in patients over 55 or with
alarming symptoms & signsalarming symptoms & signs
Etiology of DYSPEPSIAEtiology of DYSPEPSIA 1-NON-ULCER (Functional) DYSPEPSIA (50 % ).1-NON-ULCER (Functional) DYSPEPSIA (50 % ). {Dyspepsia of at least 3 Months duration for which no {Dyspepsia of at least 3 Months duration for which no
biochemical or structural abnormality is found to biochemical or structural abnormality is found to explain the patients symptoms }.explain the patients symptoms }.
2- PEPTIC ULCER DISEASE (20 % ).2- PEPTIC ULCER DISEASE (20 % ). 3-REFLUX ESOPHAGITIS (15 – 20 % ).3-REFLUX ESOPHAGITIS (15 – 20 % ). 4-N.E.R.D,Motility disorders4-N.E.R.D,Motility disorders 5 -Pancreatico-Biliary Disorders. 5 -Pancreatico-Biliary Disorders. 6- Medications :NSAIDs ,Antibiotics ,Theophyllins , Irons.6- Medications :NSAIDs ,Antibiotics ,Theophyllins , Irons.7-Dietary factors :Caffeine , Alcohol.7-Dietary factors :Caffeine , Alcohol.8- Metabolic & Endocrine : D.M , Hyperthyroidism ,8- Metabolic & Endocrine : D.M , Hyperthyroidism ,9-H .pylori.9-H .pylori.
10 –GASTRIC MALIGNANCY Is found in 1 – 2 % of 10 –GASTRIC MALIGNANCY Is found in 1 – 2 % of patients with dyspepsia, Age > 55 years + Alarm patients with dyspepsia, Age > 55 years + Alarm
symptoms.symptoms.
SYMPTOM PATTERNS IN DYSPEPSIASYMPTOM PATTERNS IN DYSPEPSIA
Ulcer-type symptoms Ulcer-type symptoms Epigastric pain Relief with food Epigastric pain Relief with food or Antacid or Antacid
Pain worse Pain worse at nightat night
Reflux symptoms Reflux symptoms Acid Acid regurgitationregurgitation
HeartburnHeartburn U.G.I. FlatulenceU.G.I. Flatulence Retrosternal painRetrosternal pain
Dysmotility symptomsDysmotility symptoms Anorexia /Early satietyAnorexia /Early satiety Postprandial Postprandial
bloatingbloating Nausea & or VomitingNausea & or Vomiting
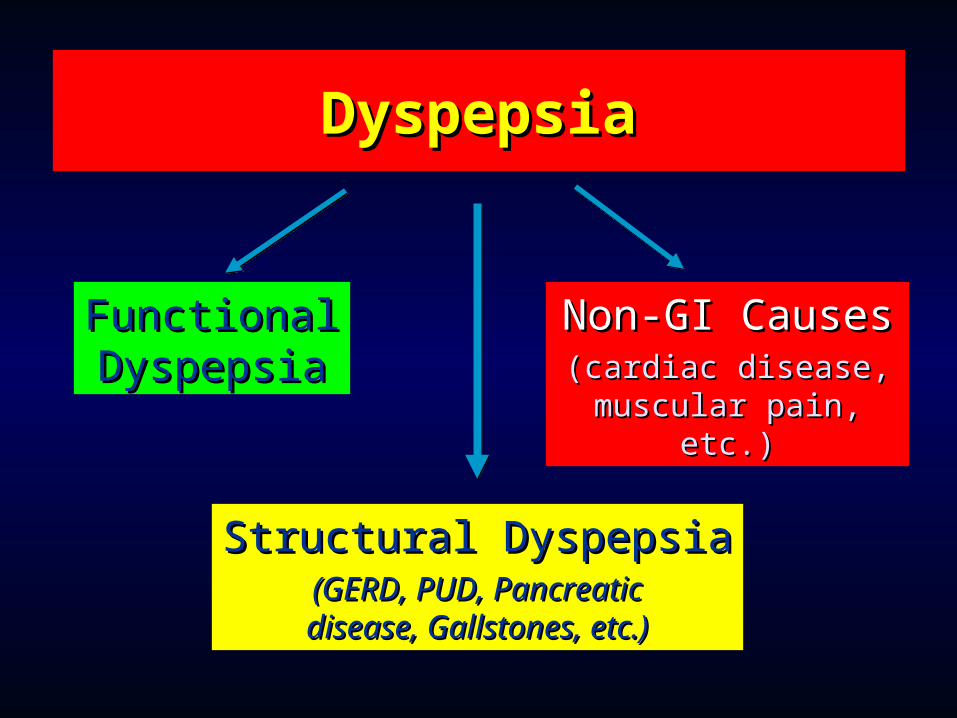
DyspepsiaDyspepsia
FunctionalFunctionalDyspepsiaDyspepsia
Non-GI CausesNon-GI Causes(cardiac disease,(cardiac disease,
muscular pain, etc.)muscular pain, etc.)
Structural DyspepsiaStructural Dyspepsia(GERD, PUD, Pancreatic(GERD, PUD, Pancreaticdisease, Gallstones, etc.)disease, Gallstones, etc.)

(Alarm Symptoms & Signs)(Alarm Symptoms & Signs)Indicators for investigationIndicators for investigation
Vomiting (persistent)Vomiting (persistent) Bleeding/anaemiaBleeding/anaemia Abdominal mass/unexplained Abdominal mass/unexplained
weight lossweight loss Dysphagia (progressive)Dysphagia (progressive) (Age > 55)(Age > 55)

Hiatal Hernia and Hiatal Hernia and Gastroesophageal RefluxGastroesophageal Reflux
GERDGERD
Gastroesophageal reflux Gastroesophageal reflux (GERD)(GERD)
GER is the reflux of chyme from the stomach GER is the reflux of chyme from the stomach to the esophagusto the esophagus
If GER causes inflammation of the If GER causes inflammation of the esophagus, it is called reflux esophagitisesophagus, it is called reflux esophagitis
A normal functioning lower esophageal A normal functioning lower esophageal sphincter maintains a zone of high pressure sphincter maintains a zone of high pressure to prevent chyme refluxto prevent chyme reflux
Conditions that increase abdominal pressure Conditions that increase abdominal pressure can contribute to GER can contribute to GER
More common in people with hiatus herniaMore common in people with hiatus hernia ManifestationsManifestations
Heartburn, regurgitation of chyme, and upper Heartburn, regurgitation of chyme, and upper abdominal pain within 1 hour of eatingabdominal pain within 1 hour of eating

Characteristics of Heartburn
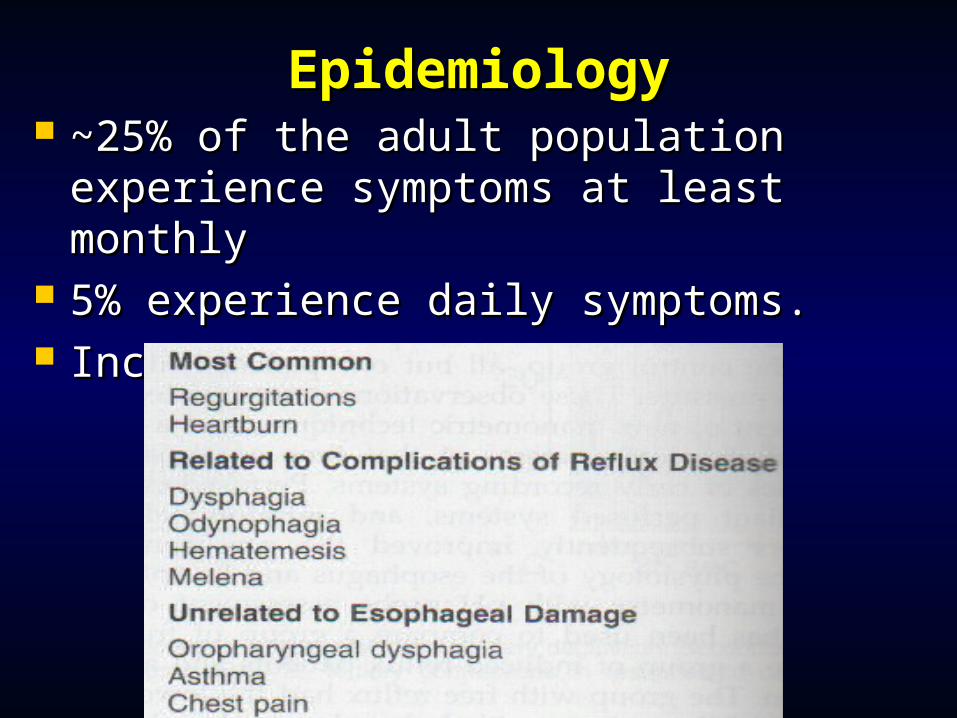
EpidemiologyEpidemiology ~~25% of the adult population 25% of the adult population
experience symptoms at least monthlyexperience symptoms at least monthly 5% experience daily symptoms.5% experience daily symptoms. Incidence increases with ageIncidence increases with age
““Alarm Symptoms” Alarm Symptoms” Urgent referral for endoscopy for patients Urgent referral for endoscopy for patients
of any age with dyspepsia when of any age with dyspepsia when presenting with any of:presenting with any of: Chronic gastrointestinal bleeding Chronic gastrointestinal bleeding Progressive unintentional weight loss Progressive unintentional weight loss Progressive difficulty swallowing Progressive difficulty swallowing Persistent vomiting Persistent vomiting Iron deficiency anaemiaIron deficiency anaemia Epigastric massEpigastric mass Choking (acid causing coughing, shortness of breath , Choking (acid causing coughing, shortness of breath ,
or hoarsness) or hoarsness) Chest painChest pain Longstanding symptoms requiring continuous Longstanding symptoms requiring continuous
treatmenttreatment
DiagnosisDiagnosis Therapeutic trial (3 months)Therapeutic trial (3 months) Endoscopy Endoscopy
Alarm sxAlarm sx To note mucosal changesTo note mucosal changes Esophageal biopsiesEsophageal biopsies
Motilitiy studiesMotilitiy studies Low LES pressures are associated with refluxLow LES pressures are associated with reflux
pH monitoring pH monitoring ( GOLD STANDARD )( GOLD STANDARD ) The most precise measure for the presence The most precise measure for the presence
of acid in the esophageal lumen (24 hour of acid in the esophageal lumen (24 hour monitoring)monitoring)
GERD ComplicationsGERD Complications Benign strictureBenign stricture PerforationPerforation HaematemesisHaematemesis Barrett’s oesophagusBarrett’s oesophagus
>3cm columnar epithelium in lower 1/3 of oesophagus
Must be confirmed by biopsy
Risk of adenocarcinoma (20% for low grade dysplasia, 50% for high grade displasia
Monitor with OGD, PPI, ? Oesophagectomy for high grade dysplasia in young fit adults
GERD ManagementGERD Management Advice – weight loss, stop smoking, stop Advice – weight loss, stop smoking, stop
alcohol, avoid stoopingalcohol, avoid stooping Medical – exclude CA if >55, control acid Medical – exclude CA if >55, control acid
secretion (PPI/Hsecretion (PPI/H22antagonist), protect antagonist), protect oesophagus (alginates), prokinetics oesophagus (alginates), prokinetics (metoclopramide)(metoclopramide)
Surgical –Surgical – Nissen fundoplication Nissen fundoplication Failed medical management Failed medical management Complications Complications Long term dependance on medical therapyLong term dependance on medical therapy
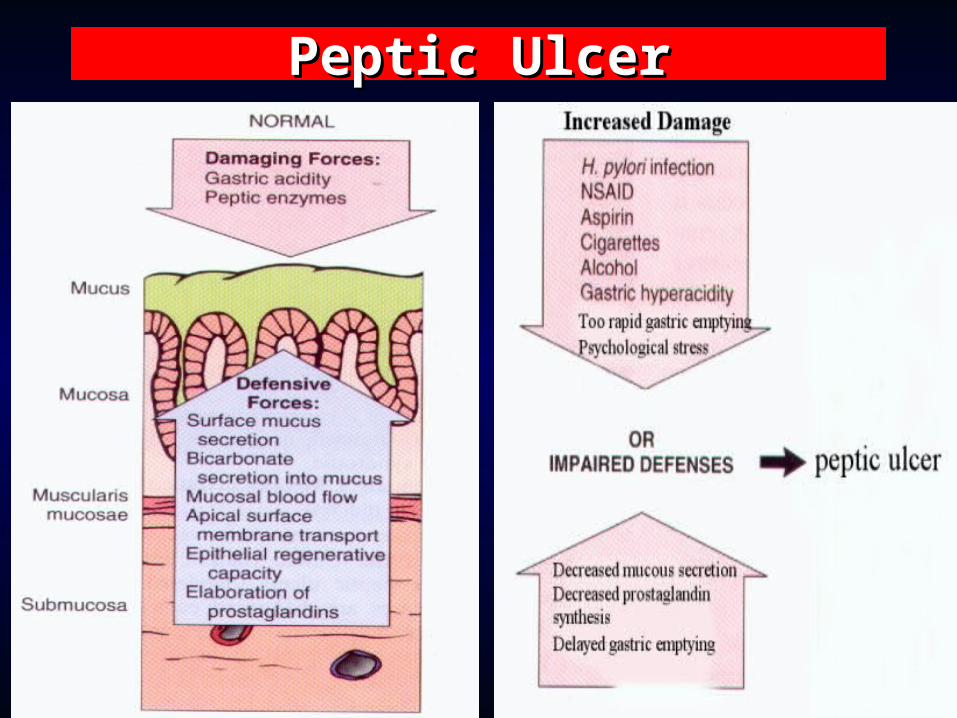
Peptic Ulcer DiseasePeptic Ulcer Disease A break in the epithelium of the A break in the epithelium of the
oesophagus, stomach or duodenumoesophagus, stomach or duodenum 5 – 10% of the general population will have 5 – 10% of the general population will have
PUD in their lifetime, 50% will recurPUD in their lifetime, 50% will recur Due to Imbalance between protective and Due to Imbalance between protective and
aggressive factorsaggressive factors Investigations – FBC, FOB, OGD, Investigations – FBC, FOB, OGD,
Urease breath testUrease breath test 0001% mortality rate0001% mortality rate
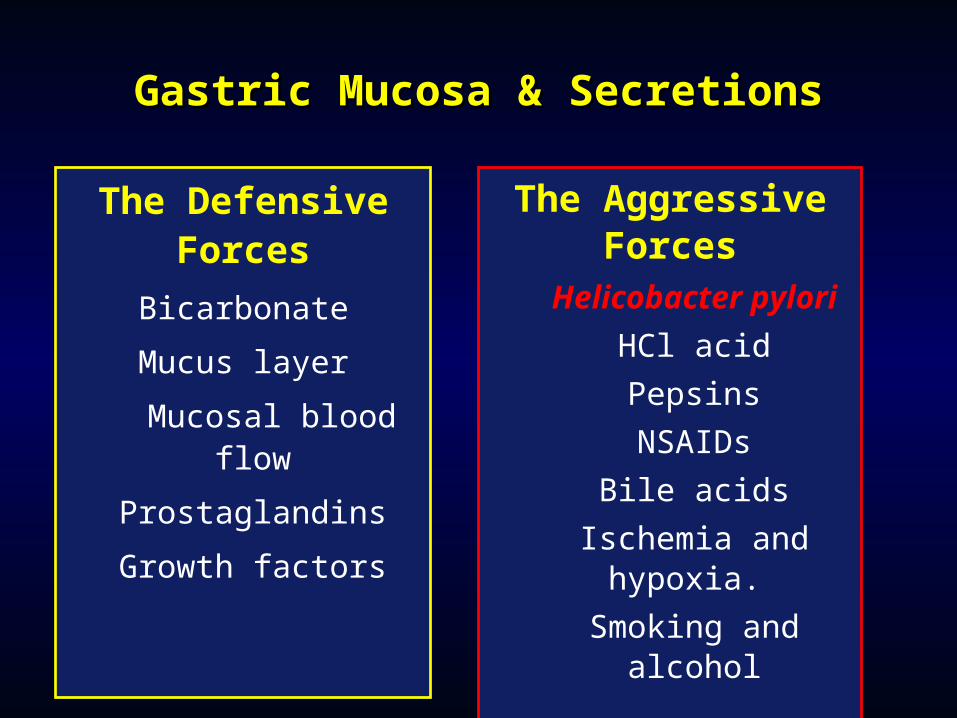
Gastric Mucosa & SecretionsGastric Mucosa & Secretions
The Defensive Forces
Bicarbonate
Mucus layer
Mucosal blood flow
Prostaglandins
Growth factors
The Aggressive ForcesHelicobacter pylori
HCl acid
Pepsins
NSAIDs
Bile acids
Ischemia and hypoxia.
Smoking and alcohol
Peptic UlcerPeptic Ulcer
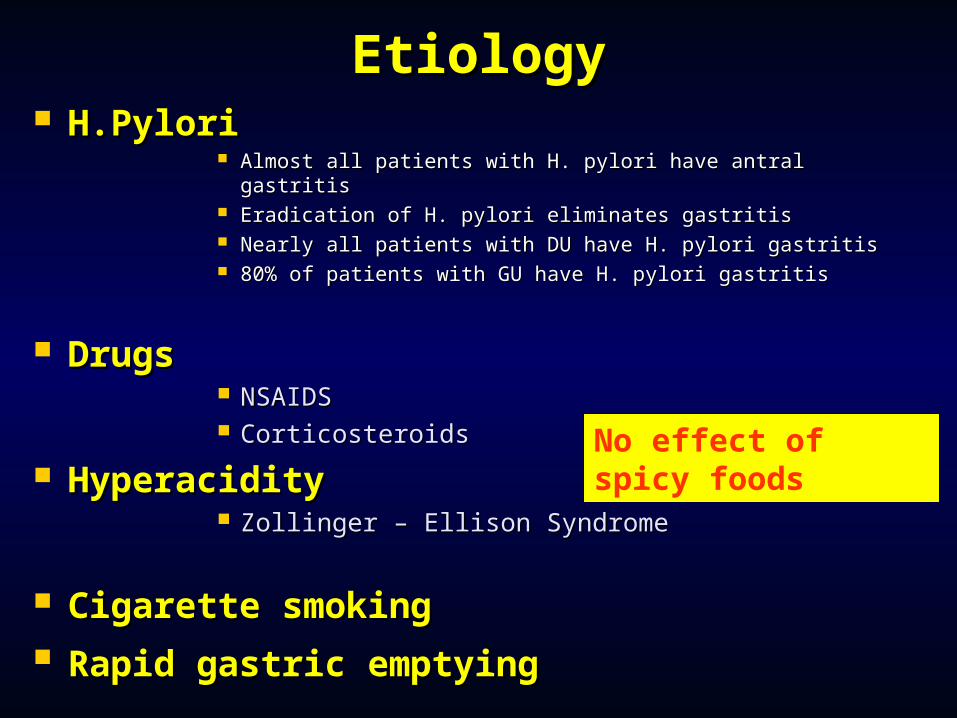
EtiologyEtiology H.PyloriH.Pylori
Almost all patients with H. pylori have antral gastritisAlmost all patients with H. pylori have antral gastritis Eradication of H. pylori eliminates gastritisEradication of H. pylori eliminates gastritis Nearly all patients with DU have H. pylori gastritisNearly all patients with DU have H. pylori gastritis 80% of patients with GU have H. pylori gastritis80% of patients with GU have H. pylori gastritis
DrugsDrugs NSAIDSNSAIDS CorticosteroidsCorticosteroids
HyperacidityHyperacidity Zollinger – Ellison SyndromeZollinger – Ellison Syndrome
Cigarette smoking Cigarette smoking Rapid gastric emptyingRapid gastric emptying
No effect of spicy foods
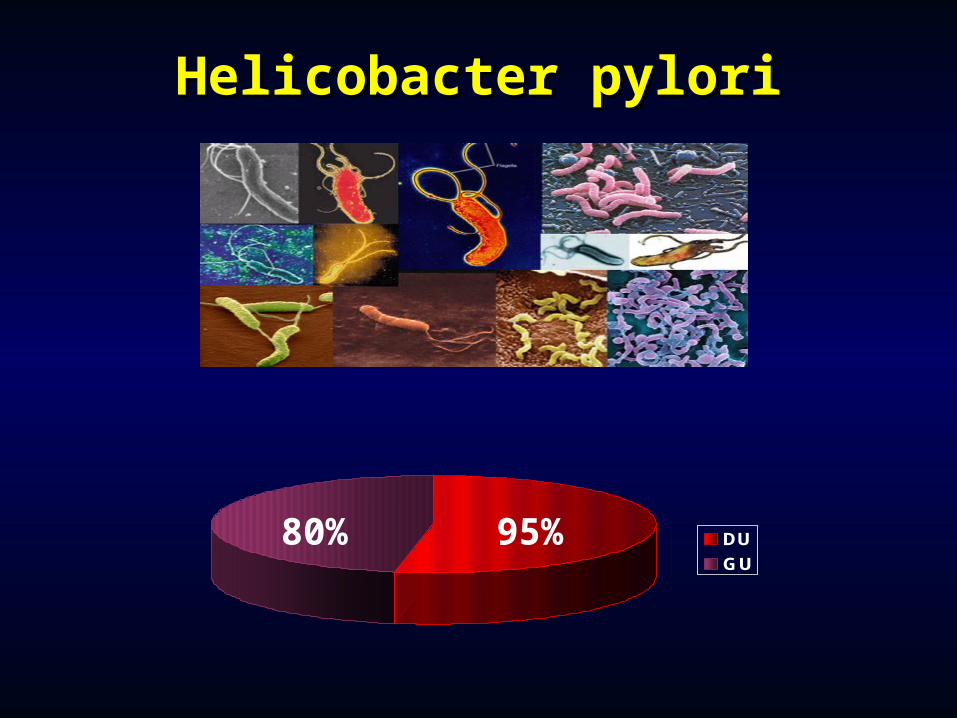
Helicobacter pyloriHelicobacter pylori
DU
GU
80% 95%
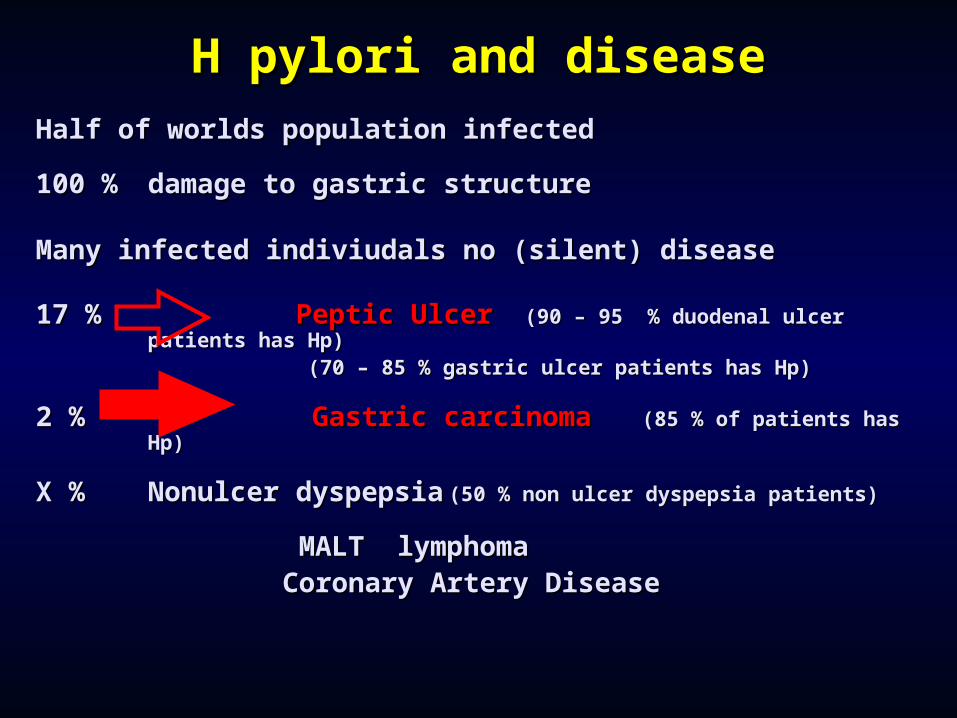
H pylori and diseaseH pylori and diseaseHalf of worlds population infectedHalf of worlds population infected
100 %100 % damage to gastric structuredamage to gastric structure
Many infected indiviudals no (silent) diseaseMany infected indiviudals no (silent) disease
17 % 17 % Peptic UlcerPeptic Ulcer ((90 – 95 90 – 95 % duodenal ulcer patients% duodenal ulcer patients has has Hp)Hp)
((7070 – 85 – 85 % gastric ulcer patients% gastric ulcer patients has Hp)has Hp)
2 %2 % G Gastric carcinomaastric carcinoma ((8585 % % of of patients patients has Hp)has Hp)
X %X % Nonulcer dyspepsiaNonulcer dyspepsia (5(500 % non ulcer dyspepsia patients% non ulcer dyspepsia patients))
MALT lymphomaMALT lymphoma Coronary Artery DiseaseCoronary Artery Disease
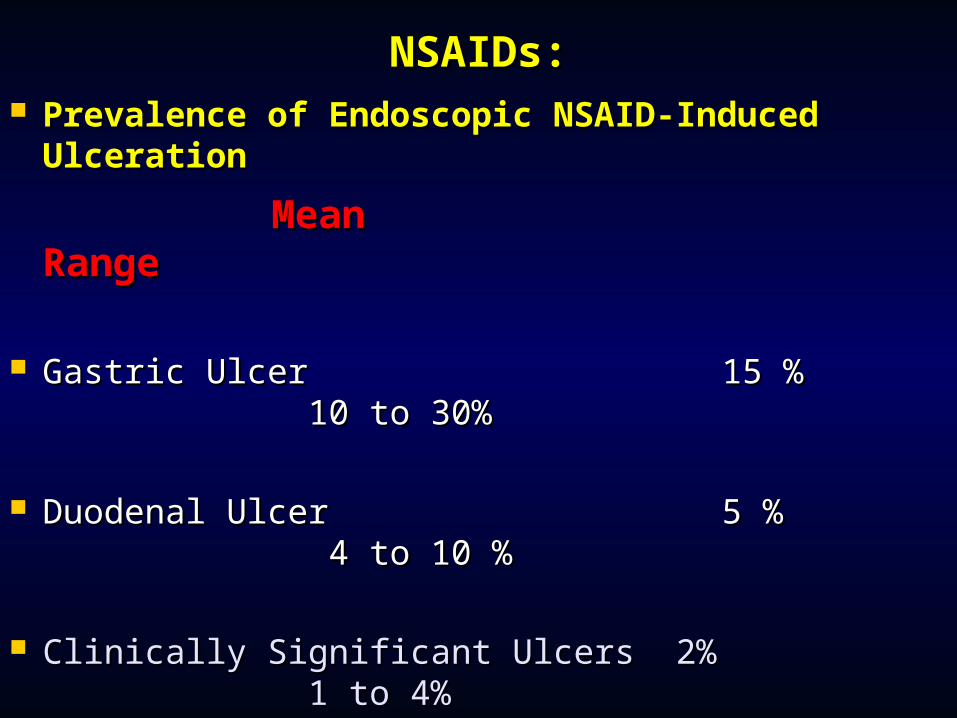
NSAIDs:NSAIDs: Prevalence of Endoscopic NSAID-Induced Prevalence of Endoscopic NSAID-Induced
UlcerationUlceration
MeanMean Range Range
Gastric UlcerGastric Ulcer 15 % 15 % 10 to 10 to 30%30%
Duodenal UlcerDuodenal Ulcer 5 % 5 % 4 4 to 10 %to 10 %
Clinically Significant Ulcers 2%Clinically Significant Ulcers 2% 1 to 4%1 to 4%
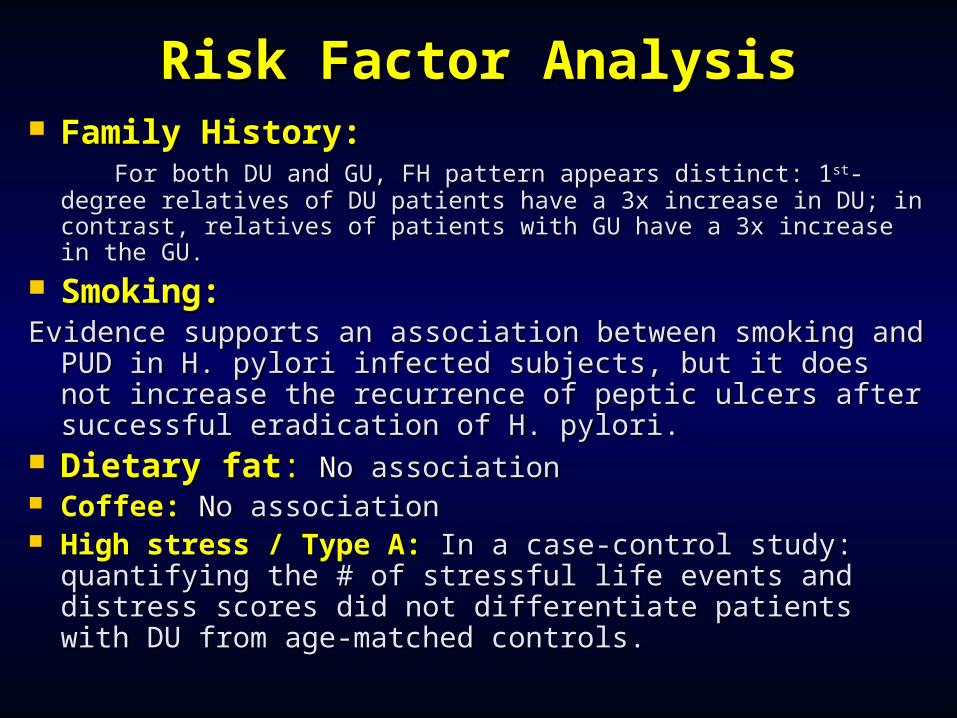
Risk Factor AnalysisRisk Factor Analysis Family History:Family History: For both DU and GU, FH pattern appears distinct: 1For both DU and GU, FH pattern appears distinct: 1stst-degree -degree
relatives of DU patients have a 3x increase in DU; in contrast, relatives of DU patients have a 3x increase in DU; in contrast, relatives of patients with GU have a 3x increase in the GU.relatives of patients with GU have a 3x increase in the GU.
Smoking:Smoking:Evidence supports an association between smoking Evidence supports an association between smoking
and PUD in H. pylori infected subjects, but it does and PUD in H. pylori infected subjects, but it does not increase the recurrence of peptic ulcers after not increase the recurrence of peptic ulcers after successful eradication of H. pylori.successful eradication of H. pylori.
Dietary fatDietary fat:: N No associationo association Coffee:Coffee: N No associationo association High stress / Type A:High stress / Type A: In a case-control study: In a case-control study:
quantifying the # of stressful life events and distress quantifying the # of stressful life events and distress scores did not differentiate patients with DU from scores did not differentiate patients with DU from age-matched controls.age-matched controls.
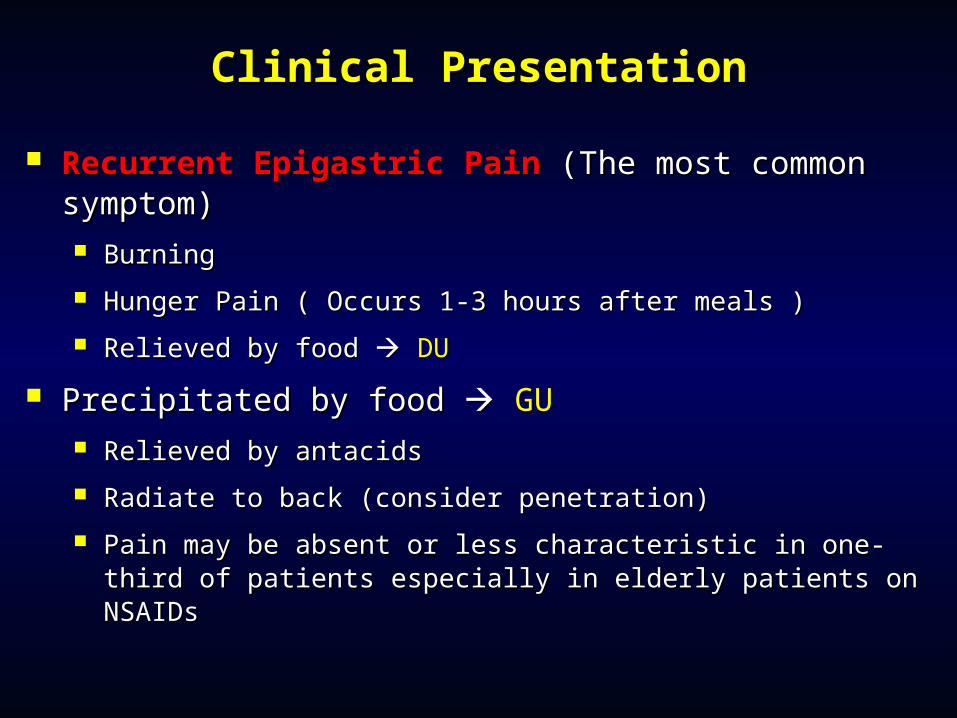
Clinical PresentationClinical Presentation
Recurrent Epigastric PainRecurrent Epigastric Pain (The most common (The most common symptom)symptom) BurningBurning
Hunger Pain ( Occurs 1-3 hours after meals )Hunger Pain ( Occurs 1-3 hours after meals )
Relieved by food Relieved by food DUDU
Precipitated by food Precipitated by food GUGU Relieved by antacidsRelieved by antacids
Radiate to back (consider penetration)Radiate to back (consider penetration)
Pain may be absent or less characteristic in one-third of Pain may be absent or less characteristic in one-third of patients especially in elderly patients on NSAIDspatients especially in elderly patients on NSAIDs
Duodenal Ulcer and Type II Duodenal Ulcer and Type II Gastric Ulcer (Prepyloric and Gastric Ulcer (Prepyloric and
Antral)Antral) MaleMale Hunger pain, relieved by food, Hunger pain, relieved by food,
periodicityperiodicity Back pain if ulcer is penetratingBack pain if ulcer is penetrating Posterior erosion – haematemesisPosterior erosion – haematemesis Anterior erosion – peritonitisAnterior erosion – peritonitis Pyloric stenosis – gastric outflow Pyloric stenosis – gastric outflow
obstructionobstruction
Type I Gastric Ulcer (Proximal)Type I Gastric Ulcer (Proximal)
Less male predominance (still more Less male predominance (still more common in males)common in males)
Older age group (>50)Older age group (>50) Epigastric pain worse on eatingEpigastric pain worse on eating Weight lossWeight loss Nausea and vomitingNausea and vomiting Gastritis and chronic anaemiaGastritis and chronic anaemia
Peptic Ulcer DiseasePeptic Ulcer Disease Duodenal UlcersDuodenal Ulcers 20 to 50 years old20 to 50 years old High stress occupationsHigh stress occupations Genetic predispositionGenetic predisposition Pain when stomach is Pain when stomach is
emptyempty Pain at nightPain at night Frequency = 4 times more Frequency = 4 times more
common than gastric common than gastric ulcersulcers
Usually associated with Usually associated with hyperacidityhyperacidity
Gastric UlcersGastric Ulcers > 50 years old> 50 years old Work at jobs Work at jobs
requiring physical requiring physical activityactivity
Pain after eating or Pain after eating or when stomach is when stomach is fullfull
Usually no pain at Usually no pain at nightnight
H. Pylori DiagnosisH. Pylori Diagnosis
Serology– 90% sensitive, 95% specific – Serology– 90% sensitive, 95% specific – not good for following treatmentnot good for following treatment
Biopsy– 98% sensitive – 98% specificBiopsy– 98% sensitive – 98% specific Urea breath test– 95% specific, 98% Urea breath test– 95% specific, 98%
specific – can be used to document specific – can be used to document eradicationeradication
Stool antigen test – 90% sensitive, 95% Stool antigen test – 90% sensitive, 95% specific – can be used to confirm specific – can be used to confirm eradication eradication

Natural HistoryNatural History 20 – 50% heal untreated20 – 50% heal untreated 80% heal in 4 weeks of treatment80% heal in 4 weeks of treatment 75% recur in 6 – 12 months75% recur in 6 – 12 months More recur in patients with More recur in patients with
H. pylori, smokers, NSAID usersH. pylori, smokers, NSAID users Milk and tobacco slow healingMilk and tobacco slow healing
Management of Peptic Management of Peptic UlcerationUlceration
Medical :Medical : Eradication therapy for H pyloriEradication therapy for H pylori ( Tripple Therapy )( Tripple Therapy )
Surgical – Elective treatment for ulcers Surgical – Elective treatment for ulcers no longer performed, therapeutic no longer performed, therapeutic OGD/laparotomy for acute OGD/laparotomy for acute complicationscomplications

Strategies in Ulcer therapyStrategies in Ulcer therapy
Pre-HpPre-HpReduce acidReduce acid
Take antacidsTake antacids
SurgerySurgery
Post-HpPost-HpFind causeFind cause
Eliminate causeEliminate cause
Control symptoms in the meantimeControl symptoms in the meantime
Long-term therapy!!
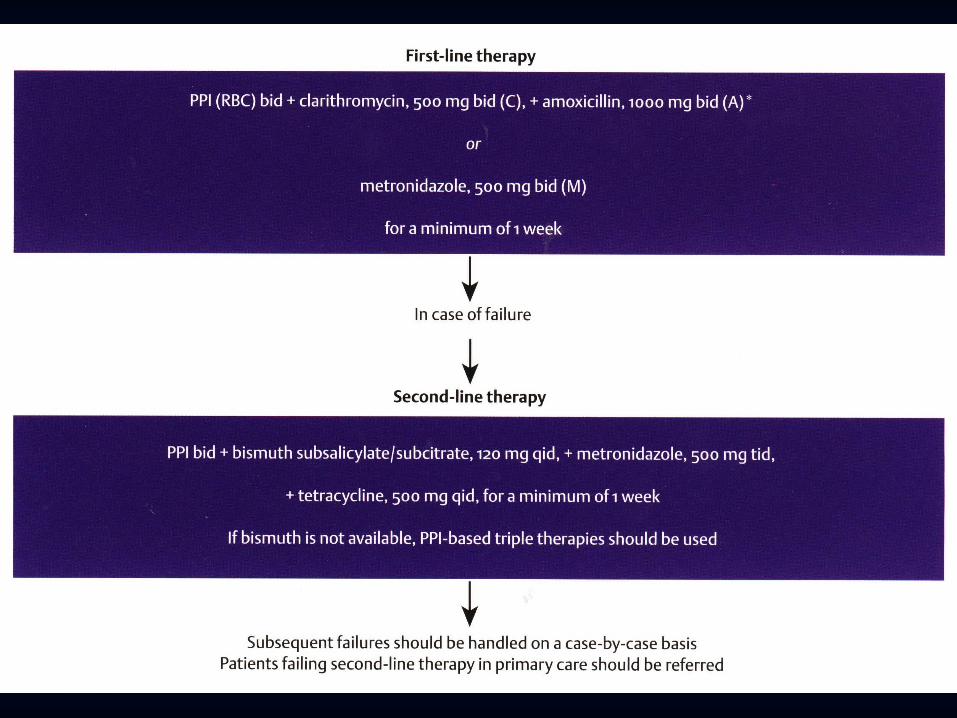

H. Pylori TreatmentH. Pylori Treatment
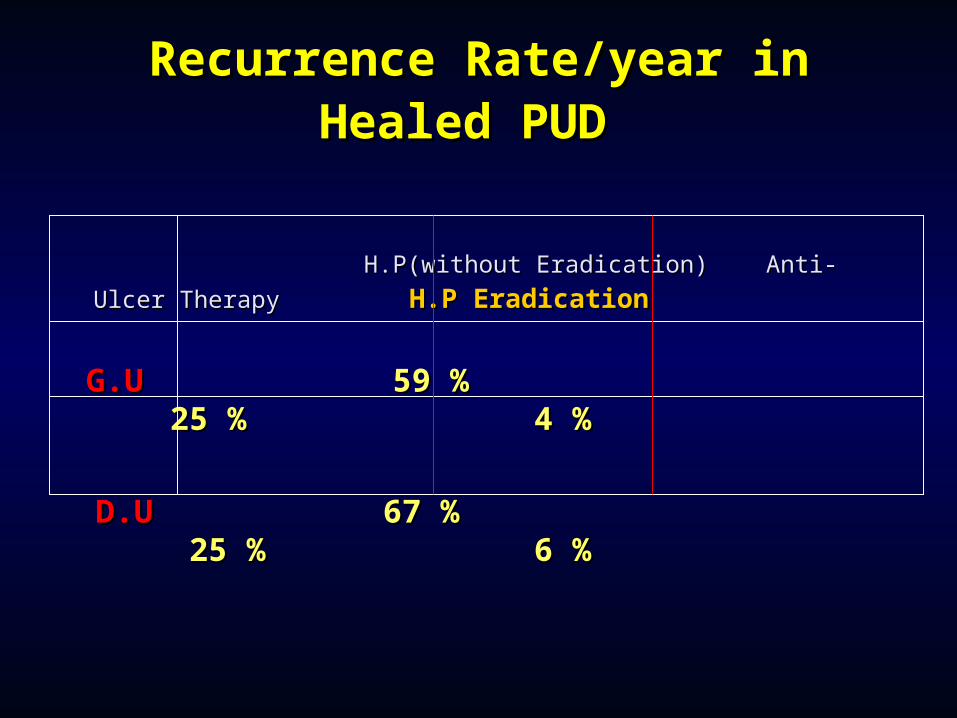
Recurrence Rate/year inRecurrence Rate/year inHealed PUDHealed PUD
H.P(without Eradication) Anti-Ulcer Therapy H.P(without Eradication) Anti-Ulcer Therapy
H.P EradicationH.P Eradication
G.U G.U 59 % 25 % 59 % 25 % 4 % 4 %
D.UD.U 67 % 25 % 67 % 25 % 6 % 6 %
DysphagiaDysphagia Difficulty SwallowingDifficulty Swallowing TypesTypes
Mechanical obstructions ( Tumours / Stricture )Mechanical obstructions ( Tumours / Stricture ) Neuromuscular ( Stroke , Myasthenia Gravis )Neuromuscular ( Stroke , Myasthenia Gravis ) Motility & Functional obstructions ( Achalasis & Motility & Functional obstructions ( Achalasis &
DES )DES ) Common causesCommon causes
Young adults –Reflux strictures, AchalasiaYoung adults –Reflux strictures, Achalasia Older adults –Malignancy, Reflux stricturesOlder adults –Malignancy, Reflux strictures
Investigations CBC Gastroduedenoscopy vs. Barium Swallow CXR
Carcinoma of the Carcinoma of the OesophagusOesophagus
Common (Common (90% are malignant )90% are malignant ) Presents with dysphagia, weight loss, Presents with dysphagia, weight loss,
anaemia, anorexiaanaemia, anorexia Associated with male sex, alcohol, Associated with male sex, alcohol,
esophagitis, achalasia, smokingesophagitis, achalasia, smoking 8% of Barrett’s develop into 8% of Barrett’s develop into
adenocarcinomasadenocarcinomas 90% are squamous , 10% adenocarcinoma90% are squamous , 10% adenocarcinoma Diagnosed on Ba swallow/OGDDiagnosed on Ba swallow/OGD 5 year survival rate : 5 15 %5 year survival rate : 5 15 %
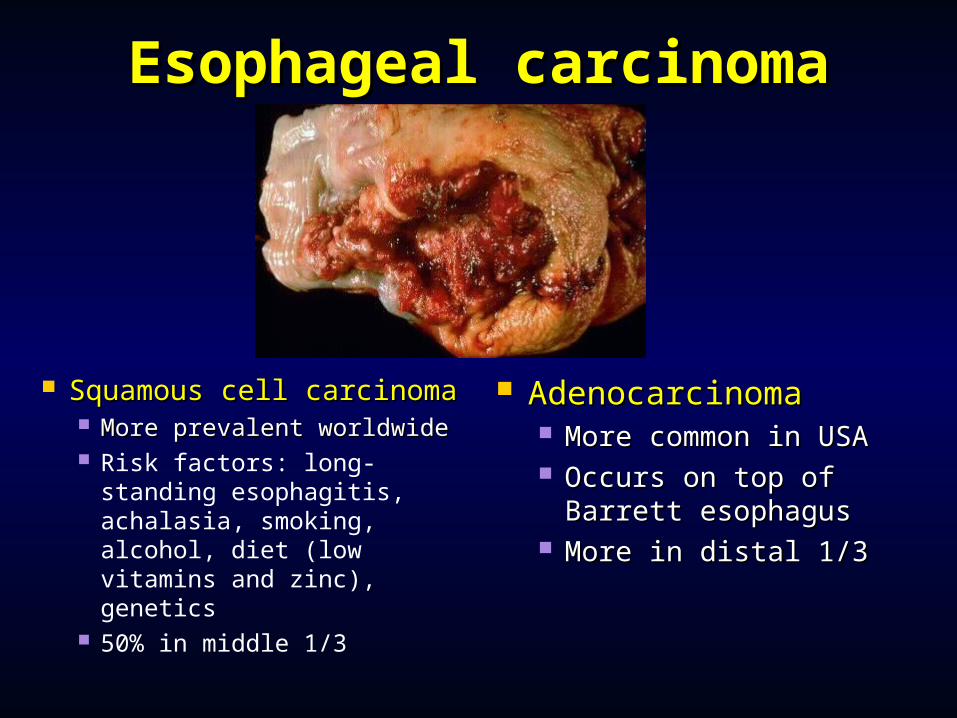
Esophageal carcinomaEsophageal carcinoma
Squamous cell carcinomaSquamous cell carcinoma More prevalent worldwideMore prevalent worldwide Risk factors: long-standing
esophagitis, achalasia, smoking, alcohol, diet (low vitamins and zinc), genetics
50% in middle 1/3
AdenocarcinomaAdenocarcinoma More common in More common in
USAUSA Occurs on top of Occurs on top of
Barrett esophagusBarrett esophagus More in distal 1/3More in distal 1/3

Achalasia: Clinical PearlsAchalasia: Clinical Pearls Majority present between 20 to 40 yearsMajority present between 20 to 40 years Solid and liquid dysphagia common >90%Solid and liquid dysphagia common >90% Regurgitation, weight loss, chest pain 40-60%Regurgitation, weight loss, chest pain 40-60% Barium Study: Accuracy ~95%Barium Study: Accuracy ~95% EndoscopyEndoscopy
Decreased Sensitivity (retained food)Decreased Sensitivity (retained food) Necessary to r/o pseudoachalasiaNecessary to r/o pseudoachalasia
More rapid onset of symptomsMore rapid onset of symptoms Late onset (age >60)Late onset (age >60) Difficult to pass scope through EGJDifficult to pass scope through EGJ
ManometryManometry Gold StandardGold Standard ↑↑LES tone, ↓LES relaxation, aperistalsis distal 2/3 LES tone, ↓LES relaxation, aperistalsis distal 2/3
esophagusesophagus
Achalasia: Clinical Pearls, Achalasia: Clinical Pearls, cont.cont.
TreatmentTreatment Medical (don’t usually work)Medical (don’t usually work)
NitratesNitrates CCBCCB
Botulinum toxinBotulinum toxin Pneumatic DilationPneumatic Dilation Surgical MyotomySurgical Myotomy Heller's Myotomy. Open or Heller's Myotomy. Open or
laparoscopiclaparoscopic

Diffuse Esophageal Spasm Diffuse Esophageal Spasm (DES)(DES)
Related Disorders of Esophageal HypermotilityRelated Disorders of Esophageal Hypermotility Barium StudyBarium Study
Corkscrew patternCorkscrew pattern ManometryManometry
>20% simultaneous nonperistaltic contractions (>30mmHg)>20% simultaneous nonperistaltic contractions (>30mmHg) Potential Therapeutic options (most ineffective)Potential Therapeutic options (most ineffective)
Medical (Medical (TCAsTCAs, Nitrates, CCBs), Nitrates, CCBs) DilationDilation Botox InjectionBotox Injection
ODYNOPHAGIAODYNOPHAGIA
Painful SwallowingPainful Swallowing CAUSES OF ODYNOPHAGIACAUSES OF ODYNOPHAGIA
1- Drug Induced Esophagitis:1- Drug Induced Esophagitis:
2-Infectious Esophagitis :2-Infectious Esophagitis : Candidia Candidia /HSV /CMV./HSV /CMV.
3- Corrosive Esophagitis .3- Corrosive Esophagitis .
4- Severe Reflux Esophagitis4- Severe Reflux Esophagitis
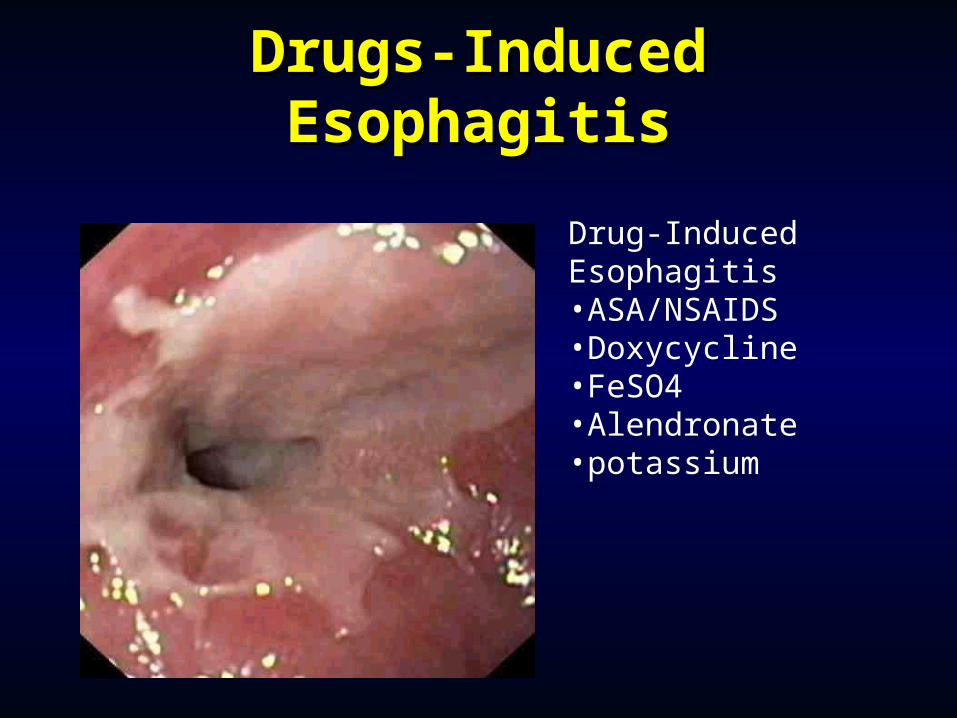
Drugs-Induced Drugs-Induced EsophagitisEsophagitis
Drug-Induced Esophagitis•ASA/NSAIDS•Doxycycline•FeSO4•Alendronate•potassium
Gastrointestinal Gastrointestinal DysfunctionDysfunction Nausea Nausea
A subjective experience that is associated with a number A subjective experience that is associated with a number of conditionsof conditions
The common symptoms of vomiting are hypersalivation The common symptoms of vomiting are hypersalivation and tachycardiaand tachycardia
AnorexiaAnorexia A lack of a desire to eat despite physiologic stimuli that A lack of a desire to eat despite physiologic stimuli that
would normally produce hungerwould normally produce hunger RetchingRetching
Nonproductive vomitingNonproductive vomiting
Vomiting Vomiting ( Neuromuscular reflex )( Neuromuscular reflex ) The forceful emptying of the stomach and intestinal The forceful emptying of the stomach and intestinal
contents through the mouthcontents through the mouth Several types of stimuli initiate the vomiting reflexSeveral types of stimuli initiate the vomiting reflex
Projectile vomitingProjectile vomiting Projectile vomiting is spontaneous vomiting that does not Projectile vomiting is spontaneous vomiting that does not
follow nausea or retchingfollow nausea or retching
Causes of Nausea and Causes of Nausea and VomitingVomiting
Peptic ulcer diseasePeptic ulcer disease Gastric outlet obstructionGastric outlet obstruction Intestinal obstructionIntestinal obstruction Acute gastritisAcute gastritis Acute cholecystitisAcute cholecystitis Acute pancreatitisAcute pancreatitis Acute hepatitisAcute hepatitis
HICCUPS (HICCOUGHS ) HICCUPS (HICCOUGHS ) CAUSESCAUSES
*Gastric Distention.*Gastric Distention.
*Sudden temperature changes.*Sudden temperature changes.
*C.N.S . Pathology.*C.N.S . Pathology. *Metabolic : *Metabolic : Uraemia /D.M / Hypocapnia Uraemia /D.M / Hypocapnia
/Electolytes/Electolytes imbalance /Toxic drugs &Alcoholimbalance /Toxic drugs &Alcohol..
*Vagus &Phrenic nerve irritation.*Vagus &Phrenic nerve irritation.
*Surgical :Anaesthesia *Surgical :Anaesthesia &postoperative.&postoperative.
*Psychogenic &Emotional stress*Psychogenic &Emotional stress..
ConstipationConstipation
Constipation is defined as infrequent Constipation is defined as infrequent or difficult defecationor difficult defecation
PathophysiologyPathophysiology Neurogenic disorders, functional or Neurogenic disorders, functional or
mechanical conditions, low-residue diet, mechanical conditions, low-residue diet, sedentary lifestyle, excessive use of sedentary lifestyle, excessive use of antacids, changes in bowel habitsantacids, changes in bowel habits**MedicationsMedications
opioidsopioidscalcium-channel blockerscalcium-channel blockersanticholinergicanticholinergic
**Decreased motilityDecreased motility
IleusIleus
**Mechanical obstructionMechanical obstruction
**Metabolic abnormalitiesMetabolic abnormalities
Spinal cord compressionSpinal cord compression
**DehydrationDehydration
**Autonomic dysfunctionAutonomic dysfunction
**MalignancMalignanc
DIARRHEADIARRHEA
It is a It is a Symptom or a Sign Symptom or a Sign NOTNOT a a DiseaseDisease
AS A SYMPTOMAS A SYMPTOM Frequency of bowel action Frequency of bowel action Looseness of stools Looseness of stools Increase in stool volumeIncrease in stool volume
AS A SIGNAS A SIGN Stools weight more than 240 gm/24 Stools weight more than 240 gm/24
hourshours
A A CombinationCombination
of theseof these
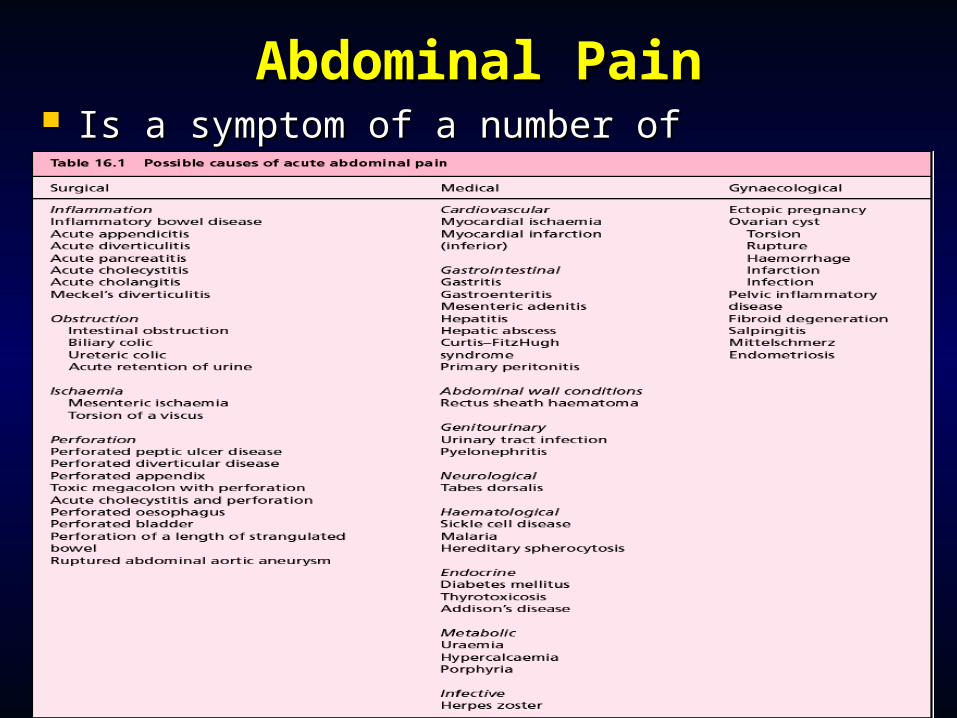
Abdominal PainAbdominal Pain Is a symptom of a number of Is a symptom of a number of
gastrointestinal disordersgastrointestinal disorders
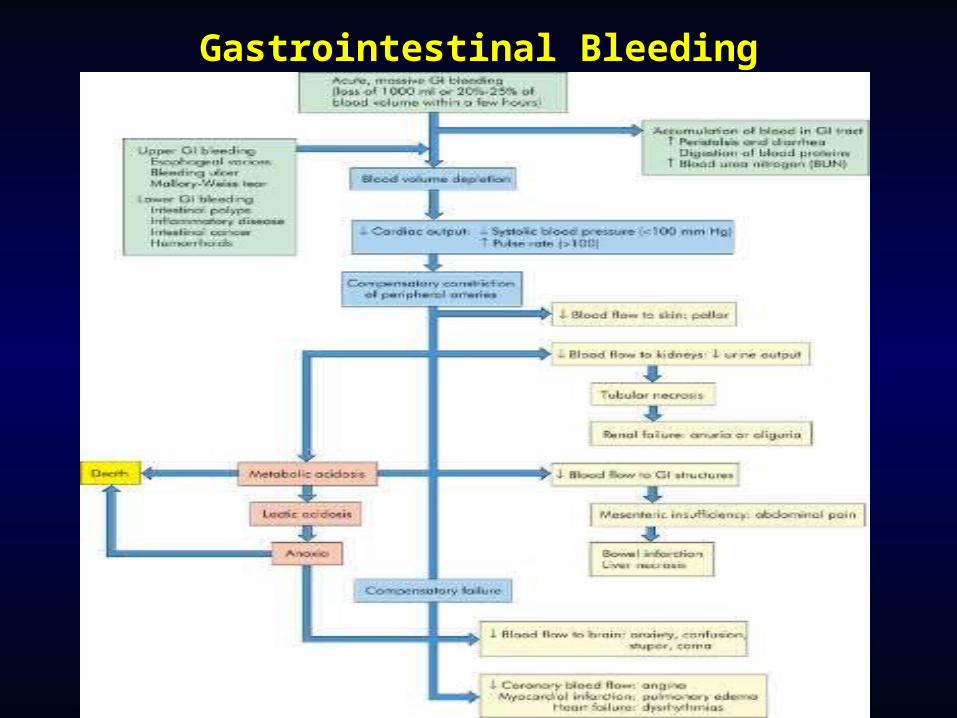
Gastrointestinal bleedingGastrointestinal bleeding Upper gastrointestinal bleedingUpper gastrointestinal bleeding
Esophagus, stomach, or duodenumEsophagus, stomach, or duodenum Lower gastrointestinal bleedingLower gastrointestinal bleeding
Below the ligament of Treitz, or bleeding Below the ligament of Treitz, or bleeding from the jejunum, ileum, colon, or rectumfrom the jejunum, ileum, colon, or rectum
HematemesisHematemesis HematocheziaHematochezia MelenaMelena Occult bleeding ? MalignancyOccult bleeding ? Malignancy
Upper Gastrointestinal Upper Gastrointestinal BleedingBleeding
AcuteAcute (> 90% of cases) (> 90% of cases) NSAIDsNSAIDs Peptic ulcer diseasePeptic ulcer disease Erosive gastritisErosive gastritis Ruptured esophagogastric varicesRuptured esophagogastric varices Mallory-Weiss tearMallory-Weiss tear Erosive esophagitisErosive esophagitis
Upper GI BleedsUpper GI Bleeds
Young – PUD, congenital lesions, varicesYoung – PUD, congenital lesions, varices Old – Tumours, PUD, angiodysplasiaOld – Tumours, PUD, angiodysplasia Investigations –CBC, Fluid balance, Investigations –CBC, Fluid balance,
LFTs, clotting, OGD, angiography, cross LFTs, clotting, OGD, angiography, cross matchmatch
Minor bleeds – observe, monitor, Minor bleeds – observe, monitor, arrange OGDarrange OGD
Major bleeds – resuscitate, urgent OGD Major bleeds – resuscitate, urgent OGD (PPI given afterwards only), treat the (PPI given afterwards only), treat the causecause
Oesophageal BleedsOesophageal Bleeds
Reflux – small volumes, bright red, HxReflux – small volumes, bright red, Hx CA – scanty debris, rusty, other CA – scanty debris, rusty, other
symptomssymptoms Varices – sudden onset, painless, Varices – sudden onset, painless,
large volumes, darker, portal HT large volumes, darker, portal HT *treat with pressors**treat with pressors*
Mallory-Weiss – bright red, history of Mallory-Weiss – bright red, history of vomitingvomiting
Stomach BleedsStomach Bleeds
Gastritis – small volumes, bright, Gastritis – small volumes, bright, follows NSAIDS/alcohol/stressfollows NSAIDS/alcohol/stress
Ulcer – larger size, painless, herald Ulcer – larger size, painless, herald smaller bleeds, ? coffee groundssmaller bleeds, ? coffee grounds
CA – rare, small bleeds, suggestive CA – rare, small bleeds, suggestive historyhistory
Congenital lesions – spontaneous in Congenital lesions – spontaneous in young, otherwise well, moderate young, otherwise well, moderate bleedsbleeds
Duodenal BleedsDuodenal Bleeds
Ulcer – history, usually melaena Ulcer – history, usually melaena present, risk factors, coffee groundspresent, risk factors, coffee grounds
Aorto-enteric fistula – rare (except in Aorto-enteric fistula – rare (except in post-op AAA patients), fatalpost-op AAA patients), fatal
Rectal bleeding - Rectal bleeding - QuestionsQuestions
Duration of symptoms – yrs, monthsDuration of symptoms – yrs, months Previous episodes or treatmentPrevious episodes or treatment Is the blood:Is the blood:
mixed in with stoolmixed in with stool separate – found on toilet paper/splashes in toilet separate – found on toilet paper/splashes in toilet
bowlbowl Fresh or altered blood - ? Lower vs upper GI Fresh or altered blood - ? Lower vs upper GI
bleedbleedMain differentials :Main differentials : Haemorrhoids (piles)Haemorrhoids (piles) Colonic carcinomaColonic carcinoma Diverticular disease / bleeding ulcerDiverticular disease / bleeding ulcer Anal fissureAnal fissure Anal carcinoma (rare) Anal carcinoma (rare)
Lower Gastrointestinal Lower Gastrointestinal BleedingBleeding
AcuteAcute (> 90% of cases) (> 90% of cases) DiverticulosisDiverticulosis Ischemic colitisIschemic colitis AngiodysplasiaAngiodysplasia Colonic polypsColonic polyps CarcinomaCarcinoma HemorrhoidsHemorrhoids Radiation colitisRadiation colitis
Gastrointestinal BleedingGastrointestinal Bleeding

Gastric CarcinomaGastric Carcinoma Clinical features of all upper GI presentations Clinical features of all upper GI presentations
with post-prandial fullnesswith post-prandial fullness Male/Female 2:1,Male/Female 2:1, Predisposing factorsPredisposing factors – diet (fish, pickled – diet (fish, pickled
vegetables), atrophic gastritis, pernicious vegetables), atrophic gastritis, pernicious anaemia, previous gastric surgery, polyps, blood anaemia, previous gastric surgery, polyps, blood group Agroup A
InvestigationsInvestigations –CBC, LFT, OGD, Ba Meal, CT scan –CBC, LFT, OGD, Ba Meal, CT scan 5 year survival rate : 5% 5 year survival rate : 5%
Common sites of metastasis include peritoneum, spleen, pancreas, transverse colon
Treatment of Gastric CATreatment of Gastric CA
Most are not resectableMost are not resectable Poor response to combination Poor response to combination
chemotherapychemotherapy Palliative surgery – gastrectomy, Palliative surgery – gastrectomy,
gastrojejunostomygastrojejunostomy If resectable usually total gastrectomy If resectable usually total gastrectomy
and oesophagojejunostomy with node and oesophagojejunostomy with node clearanceclearance
EsophagoscopyEsophagoscopy
Indications and Indications and ContraindicationsContraindications
Indications include:Indications include: DysphagiaDysphagia RefluxReflux HematemesisHematemesis Atypical chest painAtypical chest pain Many other conditionsMany other conditions
Contraindications:Contraindications: To assess reflux symptoms that respond to To assess reflux symptoms that respond to
medical managementmedical management A uncomplicated sliding hiatal herniaA uncomplicated sliding hiatal hernia
ComplicationsComplications The minor ones:The minor ones:
Lacerations of the lips or tongueLacerations of the lips or tongue Dislodgment or fracture of teeth and possible Dislodgment or fracture of teeth and possible
aspirationaspiration Major complicationMajor complication
Esophageal perforationEsophageal perforation Cervical esophagus (40%)Cervical esophagus (40%) Mid esophagus (25%)Mid esophagus (25%) Distal esophagus (35%)Distal esophagus (35%)
Morbidity and mortality from perforation is Morbidity and mortality from perforation is directly related to the time interval between directly related to the time interval between the occurrence of injury, diagnosis and repairthe occurrence of injury, diagnosis and repair
MalabsorptionMalabsorption Mostly medical causesMostly medical causes Giardiasis ( Watery Diarrhoea )Giardiasis ( Watery Diarrhoea ) Coeliac disease – clasically diarrhoea, Coeliac disease – clasically diarrhoea,
steatorrhoea and weight loss, steatorrhoea and weight loss, although often vague symptomsalthough often vague symptoms
Whipples disease – fat malabsorption Whipples disease – fat malabsorption secondary to infection, presents with secondary to infection, presents with steatorrhoea, arthralgia and malaisesteatorrhoea, arthralgia and malaise
Radiation and ischaemic enteropathyRadiation and ischaemic enteropathy
Surgical CausesSurgical Causes Crohn’s diseaseCrohn’s disease Short bowel syndrome - <50cm functioning Short bowel syndrome - <50cm functioning
terminal ileum, global malabsorptionterminal ileum, global malabsorption B12 deficiency after terminal ileum B12 deficiency after terminal ileum
resectionresection Iron deficiency after gastrectomyIron deficiency after gastrectomy Blind loop bacterial overgrowth – exclusion Blind loop bacterial overgrowth – exclusion
of a loop of ileum (Crohn’s, post surgery, of a loop of ileum (Crohn’s, post surgery, fistula) with bacterial growth digesting fistula) with bacterial growth digesting nutrientsnutrients
Diagnosis of Infectious DiarrheaDiagnosis of Infectious Diarrhea History History WorkWork TravelTravel EatingEating Ill contactsIll contacts Recent antibioticsRecent antibiotics HIV or immunocompromisedHIV or immunocompromised Stool C&S, O&P (x1), fecal blood and leukocytes if Stool C&S, O&P (x1), fecal blood and leukocytes if
no improvement in 48 hours or severe disease with no improvement in 48 hours or severe disease with bloody stools, fever, dehydration : Consider bloody stools, fever, dehydration : Consider sigmoidoscopysigmoidoscopy
Liver Diseases Liver Diseases & &
DentistryDentistry
Liver : Normal physiologyLiver : Normal physiology
Secretion of bile for fat absorption Short term sugar storage (glycogen) Aged RBC breakdown and excretion
of bilirubin Synthesis of coagulation factors Synthesis of albumin Drug metabolism
ESLD:ESLD: (Regardless of Cause)
Loss of Synthetic function: Vit K dependant coagulation factors (II, VII,
IX, X) Hypoalbuminemia (edema)
Portal hypertension Esophageal, umbilical, hemorroidal varices Ascites (abdominal fluid build-up) Splenomegaly (thrombocytopenia)
Loss of de-toxification function: ammonia Encephalopathy
ESLD:ESLD: (Regardless of Cause)
Bone marrow toxicity: anemia, leukopenia and thrombocytopenia
Endocrine disturbances: testicular atrophy and
gynecomastia Esophagitis / gastritis
Elevated Liver enzymes: AST / ALT
ESLD:ESLD: (Regardless of Cause)
Elevated bilirubin: causing Jaundice
Elevated INR: causing bleeding
Decreased albumin: causing edema and ascites
Altered drug metabolism: unpredictable
Drug effect can be Up or Down
CHRONIC LIVER DISEASECHRONIC LIVER DISEASE (Any cause)(Any cause)
PORTAL HYPERTENSION HEPATOCELLULAR FAILURE PORTAL HYPERTENSION HEPATOCELLULAR FAILURE
HCC HCC **P.S.E. *JAUNDICE. P.S.E. *JAUNDICE.
*VARICES. *COAGULOPATHY.*VARICES. *COAGULOPATHY.*ASCITES.*ASCITES.*S.B.P*S.B.P*H.R.S*H.R.S
Etiology of Chronic Liver Diseases Etiology of Chronic Liver Diseases & Cirrhosis& Cirrhosis
Alcoholic liver diseaseAlcoholic liver disease Viral hepatitis Viral hepatitis Parasites (schistosomiasis)Parasites (schistosomiasis) Autoimmune Liver Diseases( Biliary disease )Autoimmune Liver Diseases( Biliary disease ) Primary hemochromatosisPrimary hemochromatosis
Cryptogenic cirrhosisCryptogenic cirrhosis Wilson’s, Wilson’s, 1AT def1AT def
Hepatic-Venous outflow obstructionHepatic-Venous outflow obstruction Toxicant and drugsToxicant and drugs Metabolic abnormalityMetabolic abnormality NASHNASH MalnutritionMalnutrition
Clinical ManifestationClinical Manifestation
Onset:Onset: Slowly ProgressiveSlowly Progressive
Majority: Majority: 3~53~5 years or years or 1010 yearsyears
Minority: Minority: 3~63~6 months months
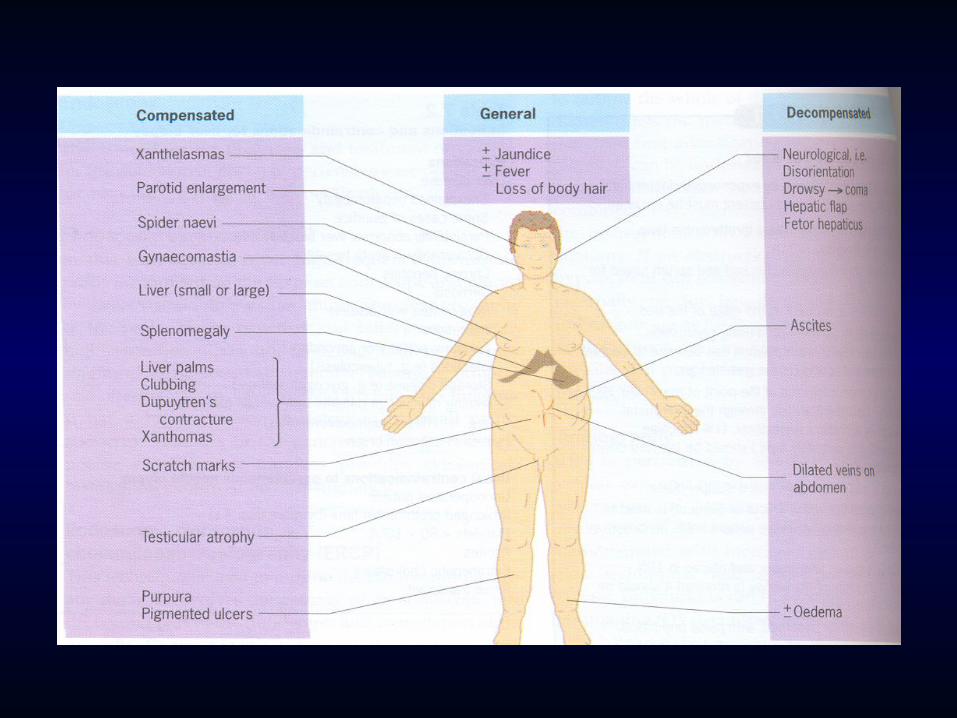
Stages:Stages: CompensatedCompensated
DecompensatedDecompensated
Compensated StageCompensated Stage
FatigueFatigue Loss of appetiteLoss of appetite AnorexiaAnorexia Abdominal discomfortAbdominal discomfort Abdominal painAbdominal pain
Hepatomegaly (slightly or moderately)Hepatomegaly (slightly or moderately) SplenomegalySplenomegaly

Decompensated StageDecompensated Stage
Deterioration of Liver Deterioration of Liver FunctionFunction
Feature of Portal Feature of Portal HypertentionHypertention
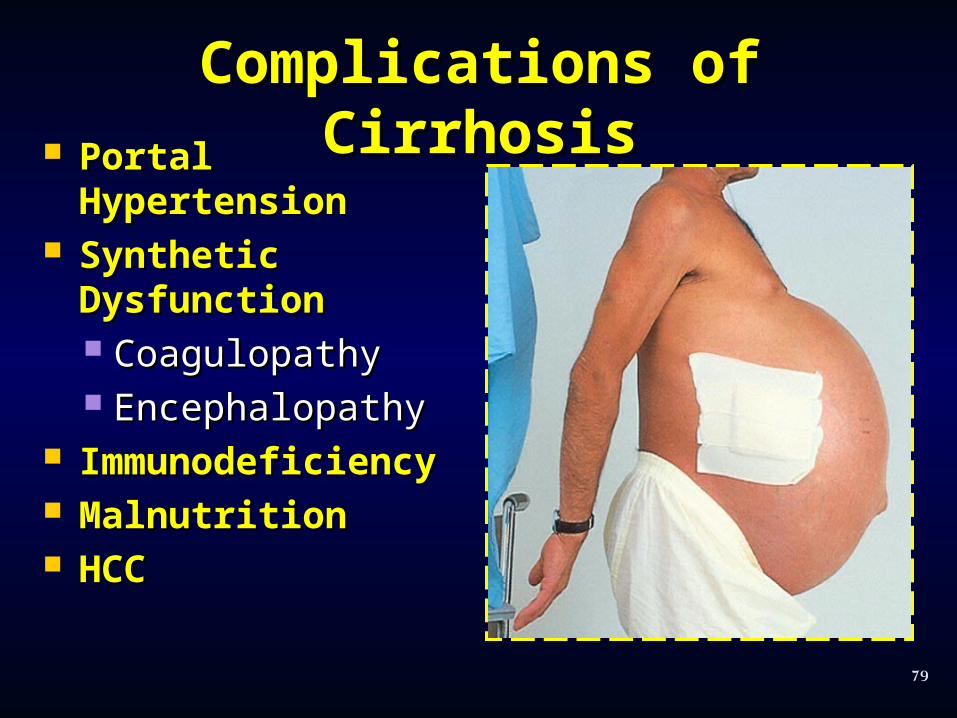
Complications of Complications of CirrhosisCirrhosis Portal Portal
HypertensionHypertension Synthetic Synthetic
DysfunctionDysfunction CoagulopathyCoagulopathy EncephalopathyEncephalopathy
ImmunodeficiencImmunodeficiencyy
MalnutritionMalnutrition HCCHCC
79
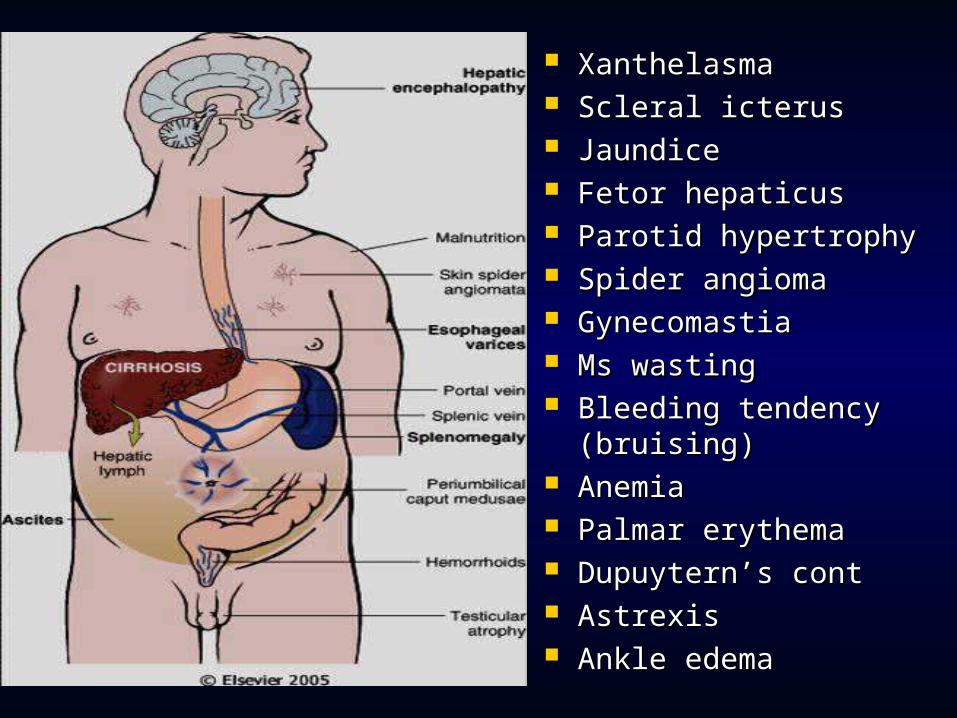
XanthelasmaXanthelasma Scleral icterusScleral icterus JaundiceJaundice Fetor hepaticusFetor hepaticus Parotid hypertrophyParotid hypertrophy Spider angiomaSpider angioma GynecomastiaGynecomastia Ms wastingMs wasting Bleeding tendency Bleeding tendency
(bruising)(bruising) AnemiaAnemia Palmar erythemaPalmar erythema Dupuytern’s cont Dupuytern’s cont AstrexisAstrexis Ankle edemaAnkle edema

JaundiceJaundice
JaundiceJaundice
Jaundice is a yellowish discoloration of the Jaundice is a yellowish discoloration of the sclera, skin, mucus membranes, and body fluids sclera, skin, mucus membranes, and body fluids caused by the deposition of bile pigmentscaused by the deposition of bile pigments
It is usually caused by either an increased It is usually caused by either an increased production or decreased excretion of bilirubin production or decreased excretion of bilirubin from the bodyfrom the body
Jaundice can be classified into:Jaundice can be classified into: Prehepatic jaundice (increased production)Prehepatic jaundice (increased production) Hepatic jaundice (decreased excretion)Hepatic jaundice (decreased excretion) Post-hepatic jaundice (decreased excretion)Post-hepatic jaundice (decreased excretion)
Pre-HepaticPre-Hepatic Haemolytic anaemia – hereditary Haemolytic anaemia – hereditary
spherocytosis, sickle cell, spherocytosis, sickle cell, thalassaemia, Gilbert’s syndromethalassaemia, Gilbert’s syndrome
High levels of unconjugated High levels of unconjugated bilirubin, normal LFTs, raised bilirubin, normal LFTs, raised reticulocytesreticulocytes
Investigate further with blood film Investigate further with blood film and autoantibody screenand autoantibody screen

HepaticHepatic
Hepatic injury – viral hepatitis, Hepatic injury – viral hepatitis, sclerosis, cirrhosis, poisons, drugssclerosis, cirrhosis, poisons, drugs
Bilirubin tends to be conjugated, Bilirubin tends to be conjugated, (jaundice occurs out of failure to (jaundice occurs out of failure to excrete, not conjugate)excrete, not conjugate)
Abnormal LFTs (raised ALT/AST)Abnormal LFTs (raised ALT/AST) Investigate further with viral titres, Investigate further with viral titres,
USS, liver biopsyUSS, liver biopsy
Post-HepaticPost-Hepatic
WallWall LumenLumen Outside Outside LumenLumen
•Raised conjugated bilirubin (absorbed from biliary tree)
•Decreased urinary urobilinogen (bilirubin does not make it to the small bowel)
•Obstructed LFTs (raised ALP and GGT)
•Further investigation with USS, and then ERCP/CT as appropriate
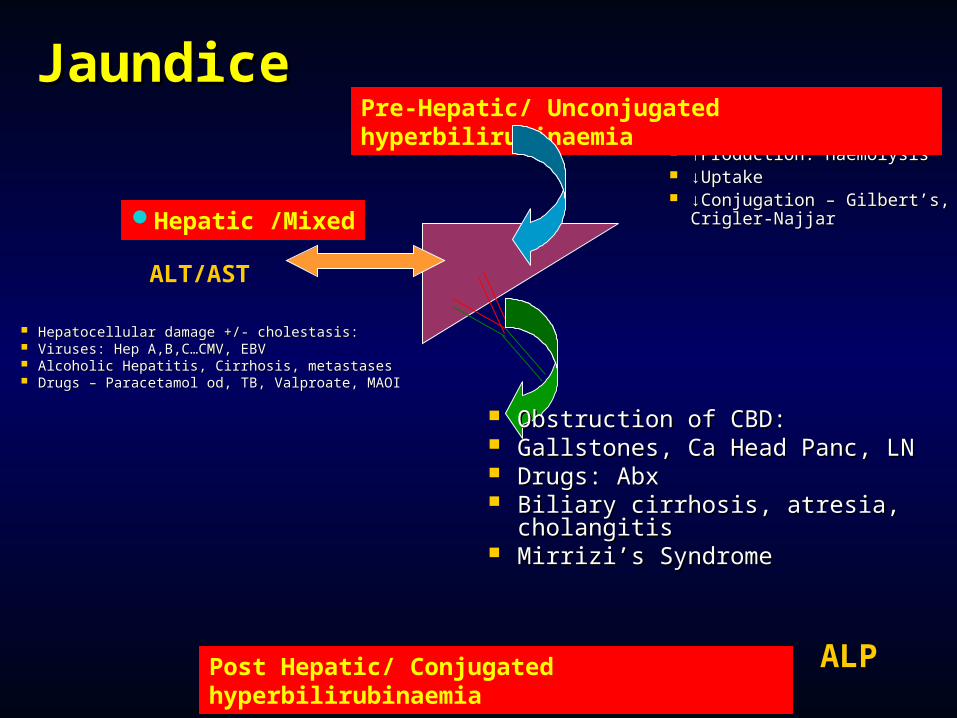
JaundiceJaundice ↑↑Production: HaemolysisProduction: Haemolysis ↓↓UptakeUptake ↓↓Conjugation – Gilbert’s, Conjugation – Gilbert’s,
Crigler-NajjarCrigler-Najjar
Pre-Hepatic/ Unconjugated hyperbilirubinaemia
Hepatic /Mixed
Post Hepatic/ Conjugated hyperbilirubinaemia
Hepatocellular damage +/- cholestasis:Hepatocellular damage +/- cholestasis: Viruses: Hep A,B,C…CMV, EBVViruses: Hep A,B,C…CMV, EBV Alcoholic Hepatitis, Cirrhosis, metastasesAlcoholic Hepatitis, Cirrhosis, metastases Drugs – Paracetamol od, TB, Valproate, Drugs – Paracetamol od, TB, Valproate,
MAOIMAOI Obstruction of CBD:Obstruction of CBD: Gallstones, Ca Head Panc, LNGallstones, Ca Head Panc, LN Drugs: AbxDrugs: Abx Biliary cirrhosis, atresia, Biliary cirrhosis, atresia,
cholangitischolangitis Mirrizi’s SyndromeMirrizi’s Syndrome
ALT/AST
ALP
JaundiceJaundice
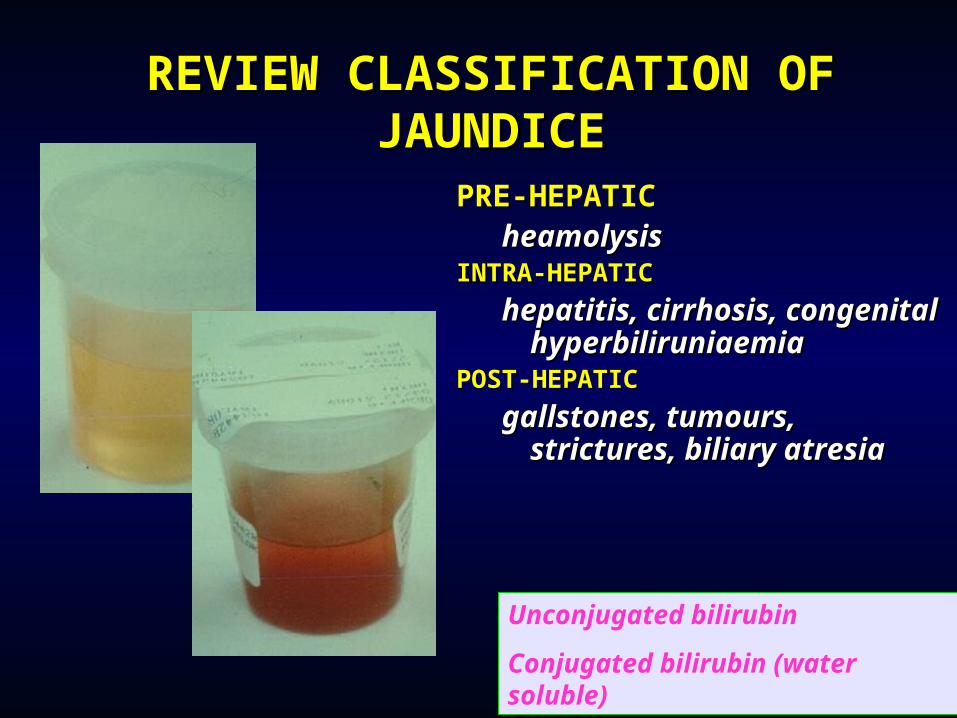
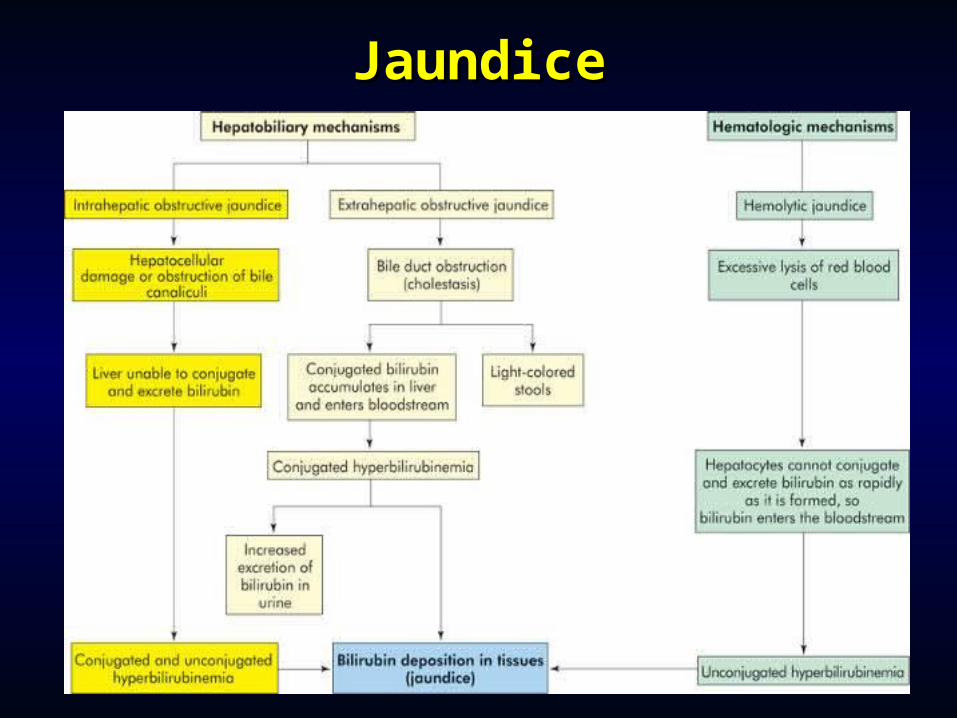
REVIEW CLASSIFICATION REVIEW CLASSIFICATION OF JAUNDICEOF JAUNDICE
PRE-HEPATICPRE-HEPATICheamolysisheamolysis
INTRA-HEPATICINTRA-HEPATIC
hepatitis, cirrhosis, hepatitis, cirrhosis, congenital congenital hyperbiliruniaemiahyperbiliruniaemia
POST-HEPATICPOST-HEPATIC
gallstones, tumours, gallstones, tumours, strictures, biliary atresiastrictures, biliary atresia
Unconjugated bilirubin
Conjugated bilirubin (water soluble)
Causes of HepatomegalyCauses of Hepatomegaly
Regular generalized enlargement without jaundiceRegular generalized enlargement without jaundice
Regular generalized enlargement with jaundiceRegular generalized enlargement with jaundice
Irregular generalized enlargement without jaundiceIrregular generalized enlargement without jaundice
Irregular generalized enlargement with jaundiceIrregular generalized enlargement with jaundice
Localized swellingsLocalized swellings
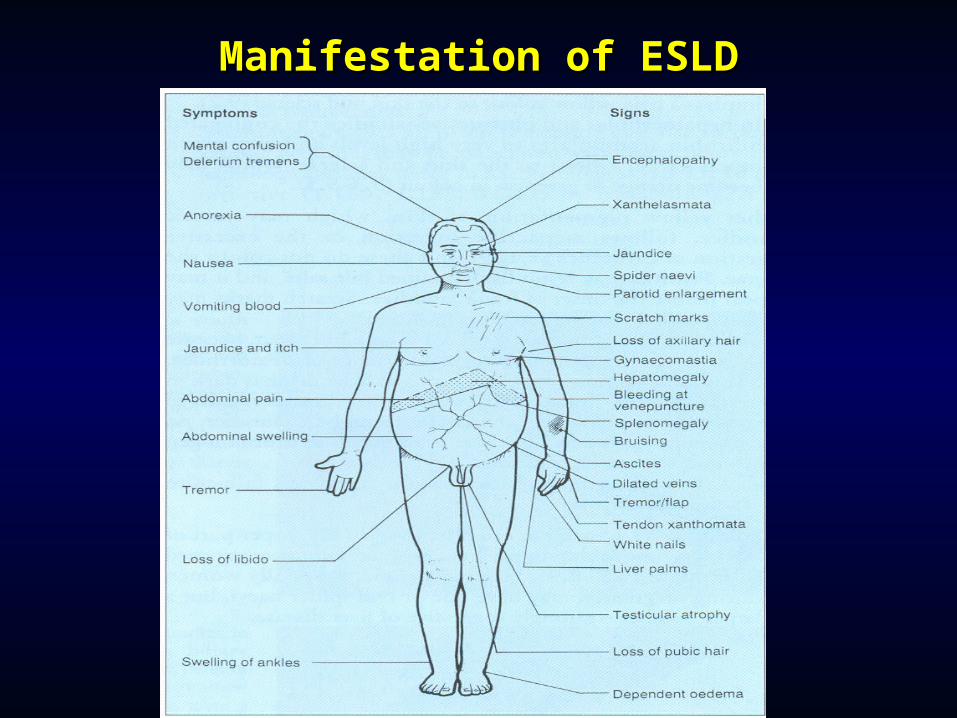
Manifestation of ESLDManifestation of ESLD
Manifestation of ESLDManifestation of ESLD
Spider Spider telangiectasias telangiectasias
Palmar erythema Palmar erythema Nail changes Nail changes Dupuytren's Dupuytren's
contracture contracture Gynecomastia Gynecomastia Testicular atrophy Testicular atrophy Hepatomegaly Hepatomegaly
Splenomegaly Splenomegaly Ascites Ascites Caput medusae Caput medusae Fetor hepaticus Fetor hepaticus Jaundice Jaundice AsterixisAsterixis
Symptoms of Advanced Symptoms of Advanced CirrhosisCirrhosis
Fatique, weaknessFatique, weakness Nausea, vomiting and Nausea, vomiting and
loss of appetiteloss of appetite Weight loss, muscle Weight loss, muscle
wastingwasting Jaundice, dark urineJaundice, dark urine Unusual bruisingUnusual bruising Spider naevi, caput Spider naevi, caput
MedusaeMedusae Bloody, black stools or Bloody, black stools or
unusually light-colored unusually light-colored stoolsstools
Vomiting of bloodVomiting of blood
Abdominal swellingAbdominal swelling Swollen feet or legs Swollen feet or legs Red palmsRed palms GynecomastiaGynecomastia Loss of sex driveLoss of sex drive Menstrual changes in Menstrual changes in
women women Generalized itchingGeneralized itching Sleep disturbances, Sleep disturbances,
confusion,desorientaticonfusion,desorientation,on,tremor, ataxia, tremor, ataxia, asterixisasterixis

Gynecomastia
Ascites
Caput Medusae
Umbilical hernia
Visible signs of advanced liver
cirrhosis
Complications of ESLDComplications of ESLD MalnutritionMalnutrition EncephalopathyEncephalopathy CoagulopathyCoagulopathy Portal HypertensionPortal Hypertension Variceal HemorrhageVariceal Hemorrhage
Pulmonary Pulmonary HypertensionHypertension {Hepatopulmonary {Hepatopulmonary syndrome}syndrome}
Hepatorenal Hepatorenal SyndromeSyndrome {HRS} {HRS}
Spontaneous Spontaneous Bacterial Bacterial PeritonitisPeritonitis {SBP} {SBP}
HyponatremiaHyponatremia
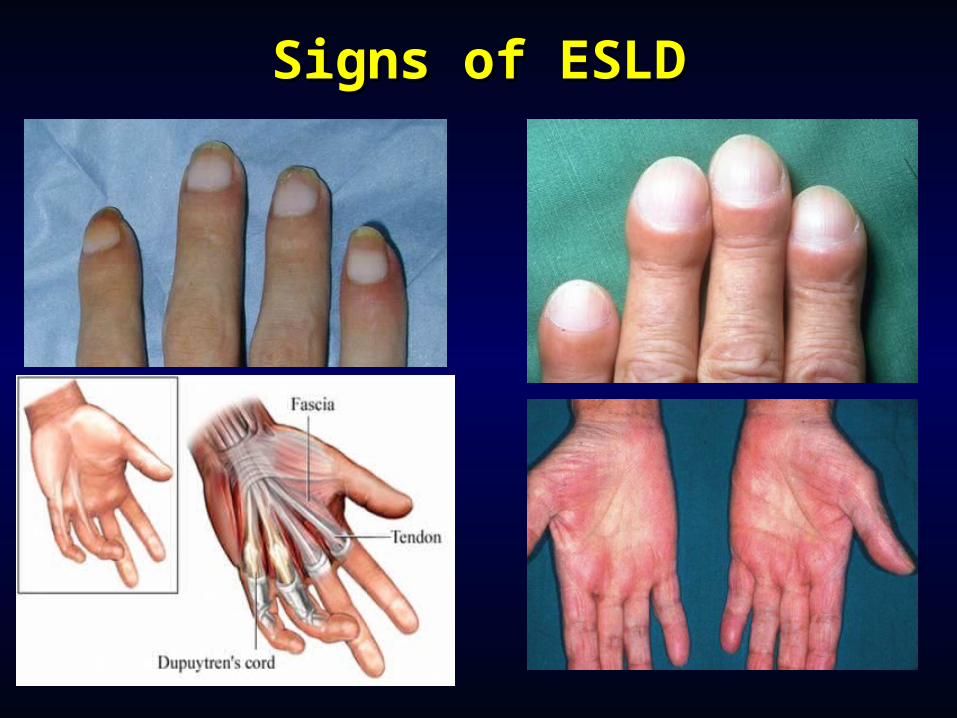
Signs of ESLDSigns of ESLD

Caput MedusaeCaput Medusae

Spider AngiomasSpider Angiomas

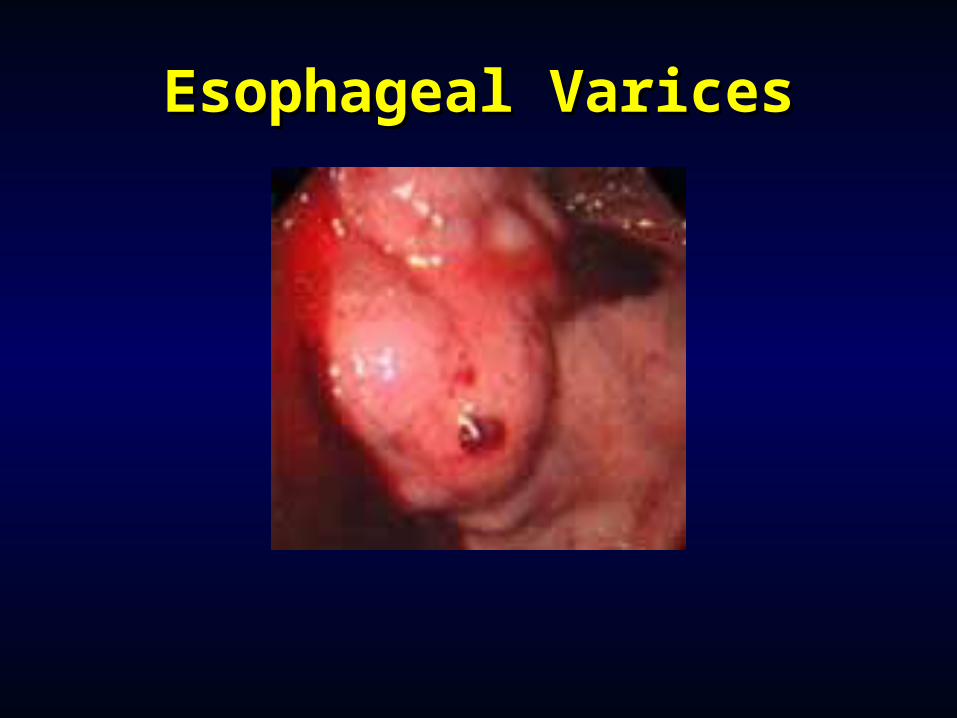
Esophageal VaricesEsophageal Varices
Laboratory FindingsLaboratory Findings Aminotransferases Aminotransferases
-AST & ALT -AST & ALT Alkaline phosphatase Alkaline phosphatase Gamma-glutamyl Gamma-glutamyl
transpeptidase (GGT)transpeptidase (GGT) Bilirubin Bilirubin Albumin Albumin
Globulins Globulins Serum sodium Serum sodium Hematologic Hematologic
abnormalities abnormalities -- Anemia Anemia -Thrombocytopenia-Thrombocytopenia -Leukopenia-Leukopenia -Neutropenia-Neutropenia -Coagulation defects-Coagulation defects (PT & INR)(PT & INR)
PancreatitisPancreatitis Caused by gallstones and/or alcoholCaused by gallstones and/or alcohol Enzymatic spillage, inflammation, oedema Enzymatic spillage, inflammation, oedema
and necrosis of the pancreasand necrosis of the pancreas Presents with moderate upper abdominal Presents with moderate upper abdominal
pain radiating to back, nausea, vomiting, pain radiating to back, nausea, vomiting, pyrexia, tachycardia, paralytic ileus and pyrexia, tachycardia, paralytic ileus and occasionally retroperitoneal bleeding (Grey occasionally retroperitoneal bleeding (Grey Turner’s and Cullen’s signs)Turner’s and Cullen’s signs)
Confirm diagnosis with amylase >1000 (lab Confirm diagnosis with amylase >1000 (lab dependent)dependent)
ABG, CXR, ECG – these patients are often ABG, CXR, ECG – these patients are often very sickvery sick
ComplicationsComplications Acutely – abscess, sepsis, necrosis, Acutely – abscess, sepsis, necrosis,
ATN, haemorrhage, pseudocyst ATN, haemorrhage, pseudocyst formationformation
Chronic pancreatitisChronic pancreatitis
- CBD obstruction, diabetes, fibrosis, - CBD obstruction, diabetes, fibrosis, inflammation, steatorrhoeainflammation, steatorrhoea
- Surgical management (drainage of - Surgical management (drainage of dilated ducts) appropriate in a small dilated ducts) appropriate in a small minorityminority
Treatment of PancreatitisTreatment of Pancreatitis
IV fluids, analgesia, anti-emeticIV fluids, analgesia, anti-emetic Monitor observations, renal and Monitor observations, renal and
respiratory functionrespiratory function Analgesia Analgesia Evidence for ERCP if proven CBD Evidence for ERCP if proven CBD
stonestone Highly conservativeHighly conservative
Pancreatic NeoplasmsPancreatic Neoplasms Adenocarcinoma affecting any part of the pancreasAdenocarcinoma affecting any part of the pancreas Endocrine tumours cause a variety of syndromes Endocrine tumours cause a variety of syndromes
from secreted peptidesfrom secreted peptides M>F, more common after age 50M>F, more common after age 50 Predisposed to by smoking, diabetes, chronic Predisposed to by smoking, diabetes, chronic
pancreatitispancreatitis Symptoms and presentation dependent on siteSymptoms and presentation dependent on site
- Tail (15%) malignant ascites, anaemia, metastases - Tail (15%) malignant ascites, anaemia, metastases (peritoneal, liver)(peritoneal, liver)- Body (25%) back pain, anorexia, weight loss, - Body (25%) back pain, anorexia, weight loss, steatorrhoea, diabetessteatorrhoea, diabetes- Head (55%) painless progressive jaundice - Head (55%) painless progressive jaundice - Periampullary (5%) as above, occasionally with - Periampullary (5%) as above, occasionally with duodenal obstruction causing vomitingduodenal obstruction causing vomiting
Investigations and Investigations and PrognosisPrognosis
USS – biliary tree, occasionally visible USS – biliary tree, occasionally visible massmass
CT scan +/- biopsy or ERCP +/- CT scan +/- biopsy or ERCP +/- biopsy biopsy
90% of patients are dead within 12 90% of patients are dead within 12 months of diagnosismonths of diagnosis
Tissue type important (better Tissue type important (better prognosis for non-pancreatic peri-prognosis for non-pancreatic peri-ampullary tumour)ampullary tumour)
Management Management PalliationPalliation Coeliac nerve ablation (body tumours)Coeliac nerve ablation (body tumours) Enzyme supplements, insulinEnzyme supplements, insulin Relieve jaundice by ERCP Relieve jaundice by ERCP SurgerySurgery
CurativeCurative Rarely appropriateRarely appropriate Requires early presentation Requires early presentation Whipple’s pancreatico-duodenectomyWhipple’s pancreatico-duodenectomy












![Amador ledger (San Francisco) 1900-02-16 [p ] · Cures heartburn, raising of the food,distress after eating or any formof dyspepsia. One littletablet gives immediate relief; 25cents](https://static.fdocuments.net/doc/165x107/5f35ea3708105503551c941f/amador-ledger-san-francisco-1900-02-16-p-cures-heartburn-raising-of-the-fooddistress.jpg)