Acoustic Schwannoma Presenting
5
Ashraf Ghobashy, M.D.,*t and Harry van Loveren, M.D.*t Acoustic Schwannoma Presenting as Acute Posterior Fossa Hematoma: Case Report and Review of the Literature Brain tumors account for 1 to 11% of all intracranial hemorrhages and 0.4% of all cases of subarachnoid hem- orrhages.1 Brain tumors commonly associated with spon- taneous intracranial hemorrhage include malignant glial tumors,2 metastatic tumors,3-6 meningioma, 6,7 choroid plexus papilloma,6,8 and pituitary adenoma.9 The associa- tion of significant hemorrhage with acoustic schwan- nomas is very rare, even though they represent 8 to 10% of all intracranial neoplasms and 71% of tumors of the cere- bellopontine angle (CPA).'O CASE REPORT A 35-year-old white man presented to a local emer- gency room on January 17, 1992, with acute onset of headache and vomiting. He described spontaneous parox- ysmal right-ear deafness (noted while speaking on the telephone), right facial palsy, right facial paresthesia, hoarseness, dysphagia, and ataxia of gait. The patient was a sound engineer for a recording studio and was consid- ered gifted with perfect pitch. Therefore, we trust that he was correct in stating his hearing was normal prior to this sudden event. Emergency computerized tomography (CT) scan revealed a 4 cm spherical mass in the right lateral cerebellar hemisphere or CPA that was hyperdense with- out contrast infusion, causing brainstem compression and mild obstructive hydrocephalus (Fig. 1). Examination During neurologic examination on January 18, the patient was alert and oriented with hypesthesia of the entire trigeminal nerve territory on the right, absent right corneal reflex, House grade I, right facial palsy, right ear deafness to tuning fork, diminished right sensory gag reflex, right cerebellar ataxia, and inability to tandem Skull Base Surgery, Volume 3, Number 3, July 1993 *University of Cincinnati College of Medicine, Department of Neurosurgery, Cincinnati, Ohio, tMayfield Neurological Institute, Cincinnati, Ohio, and tAin-Shams University, Faculty of Medicine, Department of Neurosurgery, Cairo, Egypt Reprints requests: Dr. van Loveren, University of Cincinnati College of Medicine, Department of Neurosurgery, 231 Bethesda Avenue, Cincinnati, OH 45267-0515 Copyright C) 1993 by Thieme Medical Publishers, Inc., 381 Park Avenue South, New York, NY 10016. All rights 136 reserved.
Transcript of Acoustic Schwannoma Presenting
Ashraf Ghobashy, M.D.,*tand Harry van Loveren, M.D.*t
Acoustic Schwannoma Presenting
as Acute Posterior Fossa
Hematoma: Case Report and
Review of the Literature
Brain tumors account for 1 to 11% of all intracranialhemorrhages and 0.4% of all cases of subarachnoid hem-orrhages.1 Brain tumors commonly associated with spon-
taneous intracranial hemorrhage include malignant glialtumors,2 metastatic tumors,3-6 meningioma, 6,7 choroidplexus papilloma,6,8 and pituitary adenoma.9 The associa-tion of significant hemorrhage with acoustic schwan-nomas is very rare, even though they represent 8 to 10% ofall intracranial neoplasms and 71% of tumors of the cere-
bellopontine angle (CPA).'O
CASE REPORT
A 35-year-old white man presented to a local emer-
gency room on January 17, 1992, with acute onset ofheadache and vomiting. He described spontaneous parox-
ysmal right-ear deafness (noted while speaking on thetelephone), right facial palsy, right facial paresthesia,
hoarseness, dysphagia, and ataxia of gait. The patient wasa sound engineer for a recording studio and was consid-ered gifted with perfect pitch. Therefore, we trust that hewas correct in stating his hearing was normal prior to thissudden event. Emergency computerized tomography (CT)scan revealed a 4 cm spherical mass in the right lateralcerebellar hemisphere or CPA that was hyperdense with-out contrast infusion, causing brainstem compression andmild obstructive hydrocephalus (Fig. 1).
Examination
During neurologic examination on January 18, thepatient was alert and oriented with hypesthesia of theentire trigeminal nerve territory on the right, absent rightcorneal reflex, House grade I, right facial palsy, right ear
deafness to tuning fork, diminished right sensory gag
reflex, right cerebellar ataxia, and inability to tandem
Skull Base Surgery, Volume 3, Number 3, July 1993 *University of Cincinnati College of Medicine, Department of Neurosurgery, Cincinnati,Ohio, tMayfield Neurological Institute, Cincinnati, Ohio, and tAin-Shams University, Faculty of Medicine, Department of Neurosurgery, Cairo,Egypt Reprints requests: Dr. van Loveren, University of Cincinnati College of Medicine, Department of Neurosurgery, 231 Bethesda Avenue,Cincinnati, OH 45267-0515 Copyright C) 1993 by Thieme Medical Publishers, Inc., 381 Park Avenue South, New York, NY 10016. All rights
136 reserved.

HEMORRHAGE IN ACOUSTIC SCHWANNOMA-GHOBASHY, VAN LOVEREN
Figure 1. Nonenhanced com-puterized tomography scan of theposterior fossa showing spherical hy-perdense mass in the right lateralcerebellar hemisphere (or possiblyin the right CPA).
walk. Vertebral angiography demonstrated an avascularspace-occupying mass in the right lateral posterior fossa(Fig. 2). Based on the history, clinical presentation, CTscan, and angiography, the presumptive clinical diagnosesincluded ruptured occult arteriovenous malformation(AVM) or hemorrhage caused by a cerebellar tumor.
Operation
In spite of aggressive management of intracranialpressure, the patient's level of consciousness deterioratedseveral hours after admission. Through emergency sub-occipital craniotomy, the lateral one third of the rightcerebellar hemisphere was resected until the hematomacavity was encountered. Evacuation of the hematoma pro-vided relaxation of surrounding structures, thereby re-vealing what appeared to be a relatively firm and circum-scribable tumor capsule. Frozen section biopsy of thecapsule returned a preliminary diagnosis of acousticschwannoma. Inspection of the capsule demonstrated thatthe entire seventh and eighth cranial nerve complex wasdiscolored, had been stretched severely over the dorsalaspect of the tumor capsule, and could not be recognizedduring early dissection. Once the mass was recognized asan acoustic schwannoma, it was easily totally removed bystandard microsurgical technique without complication.
Postoperative Course
The patient's overall recovery was rapid and unevent-ful. Two weeks following initial presentation, a righthypoglossal-facial nerve anastomosis was performed. The
patient was discharged from the rehabilitation service onFebruary 14 with deficits that included deafness of theright ear, facial palsy, and a mild right cerebellar ataxia.Histologic examination demonstrated an acoustic schwan-noma composed mainly of cells with uniform rod-shapednuclei (Antoni type A) mixed with areas of Antoni type B,regions of hypervascularity with thin-walled vessels, andareas of hemorrhage (Fig. 3).
DISCUSSION
Pathologic Consideration
A total of 12 cases of intracranial hemorrhage associ-ated with acoustic schwannoma have been reported in theliterature including the current case (Table 1). Lee andWang" classified these hemorrhages into two types: sub-arachnoid and intratumoral. The 12 cases reported includefive cases with subarachnoid hemorrhage only,"'12-'5 fourcases with purely intratumoral hemorrhage,'0""1,16 andthree cases with both types of hemorrhage.'5"17'18 Of thefour cases with purely intratumoral hemorrhage, one wasbelieved to be precipitated by head trauma16 and the otherswere considered spontaneous. 10,11
The mechanism of spontaneous bleeding in thesecases has not been well defined. Kasantikul et al'9 re-ported that almost 60% of tumors more than 2.0 cm indiameter have a marked increase in vascularity, which isoften associated with dilated thin-walled vessels. All 12cases of acoustic schwannoma with hemorrhage reportedwere described as "large" or were documented to be morethan 3.0 cm in diameter; in seven ofthese cases, histologic 137
SKULL BASE SURGERYNOLUME 3, NUMBER 3 JULY 1993
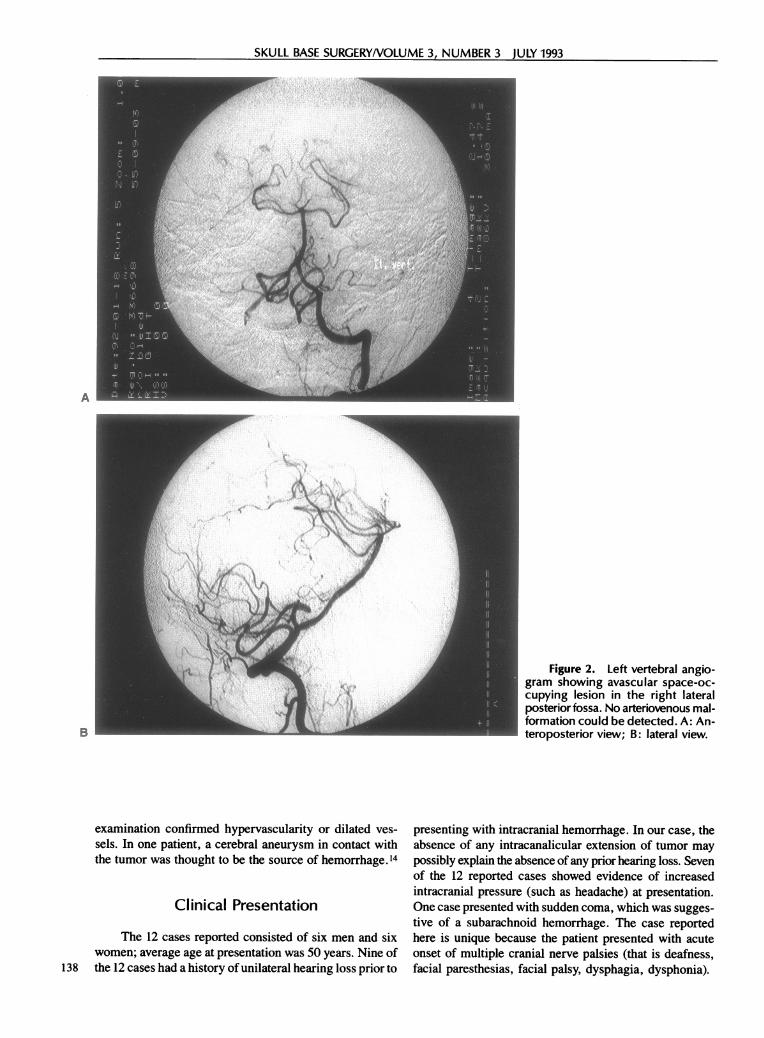
Figure 2. Left vertebral angio-gram showing avascular space-oc-cupying lesion in the right lateralposterior fossa. No arteriovenous mal-formation could be detected. A: An-teroposterior view; B: lateral view.
examination confirmed hypervascularity or dilated ves-
sels. In one patient, a cerebral aneurysm in contact withthe tumor was thought to be the source of hemorrhage. 14
Clinical Presentation
The 12 cases reported consisted of six men and sixwomen; average age at presentation was 50 years. Nine of
138 the 12 cases had a history of unilateral hearing loss prior to
presenting with intracranial hemorrhage. In our case, theabsence of any intracanalicular extension of tumor maypossibly explain the absence ofany prior hearing loss. Sevenof the 12 reported cases showed evidence of increasedintracranial pressure (such as headache) at presentation.One case presented with sudden coma, which was sugges-tive of a subarachnoid hemorrhage. The case reportedhere is unique because the patient presented with acuteonset of multiple cranial nerve palsies (that is deafness,facial paresthesias, facial palsy, dysphagia, dysphonia).
A
B

HEMORRHAGE IN ACOUSTIC SCHWANNOMA-GHOBASHY, VAN LOVEREN
# £
Figure 3. Photomicrographs of the tumor speci-mens show dilated blood vessels. (Hematoxylin & eosinstain: x250.)
Radiologic Examination
Acute CT scan was obtained in 9 of the 12 cases.Vertebral angiography was performed in 10 of the 12 cases
reported, with evidence of CPA mass in seven cases, a
posterior inferior cerebellar artery aneurysm adjacent(contact) to CPA mass in one case, and a normal studyin two cases.
Management
Eleven of the 12 patients underwent surgical treat-ment; ten reported good outcomes. One patient wastreated without surgery and died. It is notable that a
preoperative diagnosis of acoustic schwannoma was madein only 3 of the 11 patients who underwent surgery. Onepatient with a known acoustic schwannoma had a hemor-rhage while awaiting elective surgery. Two patients hadconfirmation of acoustic neuroma during the delay be-tween hemorrhage and surgery: one by posterior fossamyelogram and the other by CT scan of the internalauditory canal.
CONCLUSIONS
Posterior fossa hemorrhage is readily diagnosed byCT scan; AVM and aneurysm can be excluded by vertebral
Table 1. Summary of Reported Cases of Intracranial Hemorrhage Associated with Acoustic SchwannomaIntra- Sub-
Patient tumoral arachnoidAge, Past Clinical Hemor- Hemor- Tumor Manage-
Reference Sex History Presentation rhage rhage* Size Vasculature ment OutcomeMcCoyd et 64, F - Raised intracranial + + 2x3x3.5 Dilated Nonsurgical Death
al.18 pressure cm vesselsFine et al.'2 21, F Hearing Raised intracranial - + 3X4 cm Not Elective Good
loss pressure mentioned surgeryGlesson et 54, F Hearing Raised intracranial - + 4 cm Not Elective Good
al.13 loss pressure mentioned surgeryShephard and 37, M Coma - + Large Hypervascular Elective Good
Cheeksl 5 surgeryShephard and 66, M Hearing Facial palsy + + 3 cm Not Elective Good
Cheeks' 5 loss, mentioned surgeryataxia
Castillo et 61, M Hearing Raised intracranial + - 3 cm Dilated Elective Notal.'° loss pressure vessels surgery mentioned
Yonemitsu et 49, M Hearing Raised intracranial - + 5x5x4 Dilated Elective Goodal.' loss pressure cm vessels surgery
Goetting and 19, M Hearing Otalgia facial pain + + 3.2 cm Dilated Elective GoodSwanson'7 loss vessels surgery
Kodama et 66, F Hearing Raised intracranial - + 3 cm Aneurysm Elective Goodal. 14 loss pressure surgery
Lee and 65, F Hearing Raised intracranial + - 4X4X4 Dilated Elective GoodWang"I loss pressure cm vessels surgery
Kojima et 62, F Hearing Ataxia after head + - 3 cm Dilated Elective Goodal.'6 loss trauma vessels surgery
Present case 35, M Multiple cranial + - 4 cm Dilated Emergency Goodnerve palsies, vessels surgeryataxia
*+ = present; - = absent. 139

SKULL BASE SURGERYNOLUME 3, NUMBER 3 JULY 1993
angiography. As in all cases of mass lesions in the poste-nor fossa, the threshold to evacuate the hematoma shouldbe appropriately low. Acoustic schwannoma should beadded, albeit low on the list, to potential causes of sponta-neous posterior fossa hemorrhage. With this in mind,more careful microscopic dissection in search ofan identi-fiable tumor capsule may result in greater preservation ofcranial nerve function.
REFERENCES
1. Yonemitsu T, Niizuma H, Kodama N, Fujiwara S, Suzuki J: Acous-tic neurinoma presenting as subarachnoid hemorrhage. SurgNeurol 20:125-130, 1983
2. Shimabukuro H, Masuzawa T, Miyagi K, et al: Trigeminal neuri-noma revealed by intratumoral hemorrhage following minorhead injury. Surg Neurol 19:346-350, 1983
3. Gokalp HZ, Avman N, Ozkal E, Gokben B: Brain tumors associ-ated with intracranial arterial aneurysm. Acta Neurochir Wien53:267-273, 1980
4. Helmer FA: Oncotic aneurysms: Case report. J Neurosurg 45:98-100, 1976
5. Kochi N, Tani E, Yokota M: Neoplastic Cerebral aneurysm fromlung cancer. Case report. J Neurosurg 60:640-643, 1984
6. Abbott KH, Rollas ZH, Moegher JN: Choroid plexus papillomacausing spontaneous subarachnoid hemorrhage. Report of caseand review of literature. J Neurosurg 14:566-570, 1957
7. Yasargil MG, So SC: Cerebellopontine angle meningioma present-
ing as subarachnoid hemorrhage. Surg Neurol 6:3-6, 19768. Ersting J: Choroid plexus papilloma causing spontaneous sub-
arachnoid hemorrhage. J Neurol Neurosurg Psychiatry 18:134-136, 1955
9. Rovit RI, Fein JM: Pituitary apoplexy. A review and reappraisal. JNeurosurg 37:28-35, 1972.
10. Castillo R, Watts C, Pulliam M: Sudden hemorrhage in an acousticneuroma, case report. J Neurosurg 56:417-419, 1982
11. Lee JP, Wang ADJ: Acoustic neurinoma presenting as intratumoralbleeding. Neurosurgery 24:764-768, 1989
12. Fine R, Williams B, Dowling J: Acoustic neuroma causing sub-arachnoid hemorrhage. Med J Aust 1:137-139, 1977
13. Glesson RK, Butzer FJ, Grin OD: Acoustic neurinoma presentingas subarachnoid hemorrhage. J Neurosurg 49:602-604, 1978
14. Kodama T, Matsukado Y, Takamoto R: Acoustic schwannomapresenting as subarachnoid hemorrhage due to ruptured contactaneurysm. Surg Neurol 27:77-80, 1987
15. Shephard RH, Cheeks RE: Subarachnoid hemorrhage and acousticneuroma. (Letter.) J Neurol Neurosurg Psychiatry 44:1057, 1981
16. Kojima Y, Tanaka N, Kuwana N: Massive hemorrhage in acousticneurinoma after minor head trauma-case report. Neurol MedChir (Tokyo), 30:972-976, 1990
17. Goetting MG, Swanson SE: Massive hemorrhage into intracranialneurinoma. Surg Neurol 27:168-172, 1987
18. McCoyd K, Barron KD, Cassidy RJ: Acoustic neurinoma present-ing as subarachnoid hemorrhage (case report). J Neurosurg 41:391-393, 1974
19. Kasuntikul V, Netsky MC, Glasscock ME, Hay JW: Acousticneurilemmoma, clinicoanatomical study of 103 patients. J Neu-rosurg 52:28-35, 1980
The authors thank John M. Tew, Jr., M.D., for technicalreview, Alexis Rostoker for medical transcription, and MaryKemper for editorial assistance.
140