Schwannoma (Mediastinal Mass)
24
-
Upload
cardiacinfo -
Category
Documents
-
view
1.441 -
download
0
Transcript of Schwannoma (Mediastinal Mass)





Evaluation of Evaluation of Mediastinal MassMediastinal Mass
Leslie Proctor, M.D.Leslie Proctor, M.D.
November 21, 2008November 21, 2008

Mediastinal AnatomyMediastinal Anatomy
Includes structures Includes structures bound by:bound by: the thoracic inletthe thoracic inlet diaphragmdiaphragm sternumsternum vertebral bodiesvertebral bodies and pleuraand pleura
Has 3 compartmentsHas 3 compartments AnteriorAnterior MiddleMiddle PosteriorPosterior

The differential diagnosis of a mediastinal mass depends upon the anatomic compartment in which it arises. Redrawn from Baue, AE, et al. Glenn's Thoracic and Cardiovascular Surgery. 5th ed. Appleton & Lange, Norwalk, CT, 1991.

Mediastinal AnatomyMediastinal AnatomyAnterior Compartment Anterior Compartment
includes:includes:
ThymusThymus Extrapericardial aorta and itsExtrapericardial aorta and its
branchesbranches The great veinsThe great veins Lymphatic tissue.Lymphatic tissue.
Middle Compartment is Middle Compartment is bounded by:bounded by:
The pericardium anteriorlyThe pericardium anteriorly The posterior pericardial The posterior pericardial
reflectionreflection The diaphragmThe diaphragm The thoracic inlet. The thoracic inlet. This compartment includes the This compartment includes the
heart, intrapericardial great heart, intrapericardial great vessels, pericardium, and vessels, pericardium, and trachea. trachea.
• Extends from the posterior pericardial reflection to the posterior border of the vertebral bodies and from the first rib to the diaphragm. • It includes the esophagus, vagus nerves, thoracic duct, sympathetic chain, and azygous venous system
Posterior Compartment:

Anatomic Distribution of Anatomic Distribution of MassesMasses
Anterior MediastinumAnterior Mediastinum
Thymic tumors and cystsThymic tumors and cysts Germ cell tumorsGerm cell tumors LymphomasLymphomas Intrathoracic goiter and Intrathoracic goiter and
thyroid tumorsthyroid tumors Parathyroid adenomasParathyroid adenomas Connective tissue tumorsConnective tissue tumors
- lipomas and liposarcomaslipomas and liposarcomas- lymphangiomaslymphangiomas- hemangiomashemangiomas
ThymomaThymoma

Anatomic Distribution of Anatomic Distribution of MassesMasses
Middle MediastinumMiddle Mediastinum
Thyroid tumor or Thyroid tumor or goitergoiter
Tracheal tumorsTracheal tumors Aortopulmonary Aortopulmonary
paragangliomaparaganglioma paracardial cystsparacardial cysts bronchogenic cystsbronchogenic cysts lymphomalymphoma
LymphadenopathyLymphadenopathy
Retrosternal GoiterRetrosternal Goiter

Anatomic Distribution of Anatomic Distribution of MassesMasses
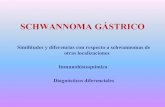
Posterior MediastinumPosterior Mediastinum
Neurogenic tumorsNeurogenic tumors including Schwannomasincluding Schwannomas
Esophageal tumorsEsophageal tumors Hiatal HerniasHiatal Hernias Neurenteric CystsNeurenteric Cysts And rarelyAnd rarely
extramedullary extramedullary hematopoiesishematopoiesis
pancreatic pseudocystpancreatic pseudocyst achalasiaachalasia
Paraspinal GanglioneuromaParaspinal Ganglioneuroma

About Neurogenic About Neurogenic tumors…tumors…
9 to 39 percent of all mediastinal tumors9 to 39 percent of all mediastinal tumors develop from mediastinal peripheral nerves, sympathetic and parasympathetic ganglia, develop from mediastinal peripheral nerves, sympathetic and parasympathetic ganglia,
and embryonic remnants of the neural tube. and embryonic remnants of the neural tube. most frequent in the posterior compartment of the mediastinummost frequent in the posterior compartment of the mediastinum Can cause neurologic symptoms by compression.Can cause neurologic symptoms by compression. Benign Schwannoma is most commonBenign Schwannoma is most common
often asymptomatic, but can be associated with Horner’s or Pancoast’s syndromeoften asymptomatic, but can be associated with Horner’s or Pancoast’s syndrome Focal calcifications and cystic changes Focal calcifications and cystic changes can extend through an intervertebral foramen, resulting in dumbbell-shaped tumors, can extend through an intervertebral foramen, resulting in dumbbell-shaped tumors,
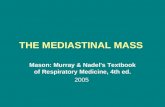
and neurologic symptoms of spinal cord compressionand neurologic symptoms of spinal cord compression Gross HistologyGross Histology
encapsulated, solid, soft, yellow-pink nodule, with the capsule attached to the encapsulated, solid, soft, yellow-pink nodule, with the capsule attached to the epineurium of the nerve that gives rise to the neoplasmepineurium of the nerve that gives rise to the neoplasm
Microscopic histologyMicroscopic histology composed of spindle cells with elongated nuclei, forming interlacing bundles with composed of spindle cells with elongated nuclei, forming interlacing bundles with
focal nuclear palisadingfocal nuclear palisading nuclear atypia, and stromal sclerosis in older lesionsnuclear atypia, and stromal sclerosis in older lesions Mitotic figures are rare. Mitotic figures are rare. Immunohistochemical studies reveal a strongly positive reaction with S-100 Immunohistochemical studies reveal a strongly positive reaction with S-100
protein.protein.

Mediastinal Benign Mediastinal Benign SchwannomaSchwannoma

Anatomic Distribution of Anatomic Distribution of MassesMasses
A mass may extend beyond these A mass may extend beyond these boundaries as it grows in sizeboundaries as it grows in size
In adults, anterior compartment In adults, anterior compartment masses are more likely to be masses are more likely to be malignant malignant

Age DistributionAge Distribution
Age can help predict etiology of the Age can help predict etiology of the massmass infants and children, neurogenic tumors and infants and children, neurogenic tumors and
enterogenous cysts are the most common enterogenous cysts are the most common mediastinal massesmediastinal masses
In adults, neurogenic tumors, thymomas, and In adults, neurogenic tumors, thymomas, and thymic cysts are most frequently encountered thymic cysts are most frequently encountered lesionslesions
In 20-40 year olds, the likelihood of a mass being In 20-40 year olds, the likelihood of a mass being malignant is greater secondary to the increased malignant is greater secondary to the increased incidence of lymphoma (Hodgkin’s and non-incidence of lymphoma (Hodgkin’s and non-Hodgkin's) and germ cell tumorsHodgkin's) and germ cell tumors

Signs and SymptomsSigns and Symptoms Depend on location of Depend on location of
massmass AsymptomaticAsymptomatic Vague symptoms Vague symptoms
aching painaching pain coughcough
Children more likely to Children more likely to be symptomaticbe symptomatic respiratory difficultyrespiratory difficulty recurrent recurrent
pulmonary pulmonary infectionsinfections

Signs and SymptomsSigns and Symptoms Airway compressionAirway compression
recurrent pulmonary recurrent pulmonary infectioninfection
hemoptysis hemoptysis Esophageal Esophageal
compression compression dysphagiadysphagia
Involvement of the Involvement of the spinal columnspinal column paralysis paralysis
Phrenic nerve damagePhrenic nerve damage elevated hemidiaphragm elevated hemidiaphragm

Signs and SymptomsSigns and Symptoms Recurrent laryngeal Recurrent laryngeal
nerve involvementnerve involvement HoarsenessHoarseness
Sympathetic ganglion Sympathetic ganglion involvementinvolvement Horner’s SyndromeHorner’s Syndrome
Ptosis, miosis, anhidrosisPtosis, miosis, anhidrosis
superior vena cava superior vena cava involvementinvolvement Superior vena cava Superior vena cava
syndromesyndrome facial neck, and UE facial neck, and UE
swelling, dyspnea, chest swelling, dyspnea, chest and UE pain, mental and UE pain, mental status changesstatus changes
Horner’s Syndrome

Signs and SymptomsSigns and Symptoms
Can also be associated with systemic Can also be associated with systemic diseasesdiseases Thymoma: myasthenia gravis, immune Thymoma: myasthenia gravis, immune
deficiency, red cell aplastic anemiadeficiency, red cell aplastic anemia Goiter: thyroxicosisGoiter: thyroxicosis Thymic carcinoid: Cushing’s syndromeThymic carcinoid: Cushing’s syndrome Parathyroid: hyperparathyroidismParathyroid: hyperparathyroidism

Evaluation: ImagingEvaluation: Imaging 2 view PA/Lat Chest X-ray2 view PA/Lat Chest X-ray
comparisons with old x-rays importantcomparisons with old x-rays important Chest CT with contrastChest CT with contrast
most important method of evaluationmost important method of evaluation Can help determine location, morphology, size, and attenutation coefficientCan help determine location, morphology, size, and attenutation coefficient Important for directing further therapyImportant for directing further therapy
MRIMRI when contrast allergy or renal failure presentwhen contrast allergy or renal failure present when vascular or chest wall involvement is suspectedwhen vascular or chest wall involvement is suspected neurogenic tumors (especially helpful in detecting intraspinal componentneurogenic tumors (especially helpful in detecting intraspinal component
UltrasoundUltrasound Differentiate cystic from solid masses and relate to surrounding structuresDifferentiate cystic from solid masses and relate to surrounding structures When mass is close to heart or pericardiumWhen mass is close to heart or pericardium Transesophageal or transbronchial useful to evaluate lymph nodes, sometimes for Transesophageal or transbronchial useful to evaluate lymph nodes, sometimes for
biopsybiopsy Radio nucleotide scanningRadio nucleotide scanning
With radioactive iodine when thyroid tumor suspectedWith radioactive iodine when thyroid tumor suspected PET scanningPET scanning
Can localize specific tumors (pheochromocytoma, paragangliomas, Can localize specific tumors (pheochromocytoma, paragangliomas, neuroblastomas, neurogangliomas by targeting their metabolic pathwaysneuroblastomas, neurogangliomas by targeting their metabolic pathways

Evaluation: LaboratoryEvaluation: Laboratory Depends on clinic setting, but may include:Depends on clinic setting, but may include:
Thyroid function testsThyroid function tests If goiter suspectedIf goiter suspected
Chemistry panel including calcium and phosphate and Chemistry panel including calcium and phosphate and PTHPTH
If parathyroid adenoma suspectedIf parathyroid adenoma suspected Fractionated 24-hour urinary metanephrines and Fractionated 24-hour urinary metanephrines and
catecholaminescatecholamines If paraganglionic tumor suspectedIf paraganglionic tumor suspected
AFP/beta HCGAFP/beta HCG In all males with anterior mediastinal tumor because In all males with anterior mediastinal tumor because
of concern for non-seminomatous germ cell tumorof concern for non-seminomatous germ cell tumor

ManagementManagement Tailored to specific or likely Tailored to specific or likely
diagnosisdiagnosis Must decide whether to excise, Must decide whether to excise,
biopsy, or aspirate lesionbiopsy, or aspirate lesion Excision should be done Excision should be done
with teratomas, thymomas, with teratomas, thymomas, and isolated masses likely and isolated masses likely to be benign (VATS, median to be benign (VATS, median sternotomy, thoracotomy)sternotomy, thoracotomy)
Needle aspiration of cystic Needle aspiration of cystic lesionslesions
Diagnostic biopsy is Diagnostic biopsy is procedure of choice when procedure of choice when suspect lymphoma, germ suspect lymphoma, germ cell tumor, or unresectable cell tumor, or unresectable invasive malignancyinvasive malignancy


ReferencesReferences Kallab, Andre MD. Kallab, Andre MD. Superior Vena Cava SyndromeSuperior Vena Cava Syndrome. Emedicine. August 10 2005. . Emedicine. August 10 2005.
http://www.emedicine.com/MED/topic2208.htmhttp://www.emedicine.com/MED/topic2208.htm
Gangadharan, Sidhu MD. Evaluation of Mediastinal Masses. UptoDate. October 7, 2008. Gangadharan, Sidhu MD. Evaluation of Mediastinal Masses. UptoDate. October 7, 2008.
Parmar, Malvinder S, MB, MS. Horner’s Syndrome. Emedicine. June 5, 2008. Parmar, Malvinder S, MB, MS. Horner’s Syndrome. Emedicine. June 5, 2008. http://www.emedicine.com/med/TOPIC1029.HTMLhttp://www.emedicine.com/med/TOPIC1029.HTML
Strolls, DC, Rosado-de-Christenson, ML, Jett, JR. Strolls, DC, Rosado-de-Christenson, ML, Jett, JR. Primary mediastinal tumors. Part I: Tumors of the Primary mediastinal tumors. Part I: Tumors of the anterior mediastinumanterior mediastinum. Chest 1997; 112:511. . Chest 1997; 112:511.
Strollo, DC, Rosado-de-Christenson, ML, Jett, JR. Strollo, DC, Rosado-de-Christenson, ML, Jett, JR. Primary mediastinal tumors: Part II. Tumors of Primary mediastinal tumors: Part II. Tumors of the middle and posterior mediastinumthe middle and posterior mediastinum. Chest 1997; 112:1344. . Chest 1997; 112:1344.
Medscape.com (multiple images)Medscape.com (multiple images)
Devouassoux-Shisheboran, Mojgan MD and Travis, William D MD. Pathology of Mediastnal Devouassoux-Shisheboran, Mojgan MD and Travis, William D MD. Pathology of Mediastnal Tumors. Uptodate. September 9Tumors. Uptodate. September 9thth, 2008., 2008.