~AA·· ~. hale...include insomnia, depression. weIght g~in. inahility to maintain employment,...
38
hale HIV/AIDS Legal Centre Innrporaled INSWl IBN 39045530926 Ref : 1'000513 Q March 2016 Ann Burke Victims St:f\ ices Tribunal .ill stice Precinct Lucked Bag 51 1H Parramatw N SW 2124 Dear Ms Burke. L fXA ___ --1I < ,-cler to our suhmiss ions for XA s application for compensation from the Victims Services Tribunal dated 14 Mil)' 1015. You requested fUl1h cr eviden ce that I BXA Is loss uf camings is a direct resull of the act uf violen ce against her. We have sillce been able to obtain infonnation suhmitted to Centrcl ink in support of her applications lor the Disabilit), Support Pension. Allached in this regard are: I. Application Ii" Disabilit)' Support Pension. completed 23 June 2010 2. Supporting Medical Report completed by Professl'" John Quinn. Liverpool lIospital. dated 18 June 20 10 3. Ceotrcltnk dcctr()nic file note 9 June 20lD 4. CCOIrelink daim for Disability SuppO/1 I 'ensi'ln or Sickness AlIuwance cump leted 23 June 20 I 0 In addition, Ih ese submissions make to the report of Dr 1 ,11uisc Evans da ted R January 201 S. pre"iously pmvidcd 10 the Tribunal on 14 May 2U15. We apologi$e for the extended time that this mailer lws taken. The Ccntrelink recortl s were ob t <tincd bv wav ofFO I which , for rC;Jsons outside our control. took II sign i ficant period " fti mc. BXA has no fhrtlter motcri"lto suhm it. We thcrdore ask the T rib unal to make a dee,sltln soones! pussihle. foll"wing receip! "f this material. Background The documents evi de nce 8XA s illnt:ss. ami diagnoses and directly link these tll her inability 0 une Ion and undertake work for several years between 2003 and 20 The IIIV transmission at the "ge of8 years old has progressively lead I suffering from AIDS defining illnesses "fOesophageal Candidiasis in 200.1 UJl(II'CP Pneuillonia in 20 I O. 414 ElIzabeth SLreel SUrry Hills NSW 2010 email: [email protected] WWW.I1alc.Org.8U Tel: £02J 9206 2060 Fax: 102J 9206 2053 Freecall: 1800 063 060 STAT.0971.001.0175_R
Transcript of ~AA·· ~. hale...include insomnia, depression. weIght g~in. inahility to maintain employment,...

~.
~AA··
hale HIV/AIDS Legal Centre Innrporaled INSWl IBN 39045530926 Ref: 1'000513
Q March 2016
Ann Burke Victims St:f\ ices Tribunal .illstice Precinct Oflic~s Lucked Bag 51 1 H Parramatw N SW 2124
Dear Ms Burke.
LfXA ___ --1I<
\~rc ,-cler to our suhmissions for XA s application for compensation from the Victims Services Tribu nal dated 14 Mil)' 1015. You requested fUl1hcr evidence that IBXA Is loss uf camings is a direct resull of the act uf violence against her.
We have sillce been able to obtain infonnation suhmitted to Centrcl ink in support of her applications lor the Disabilit), Support Pension . Allached in this regard are:
I . Application Ii" Disabilit)' Support Pension . completed 23 June 2010 2. Support ing Medical Report completed by Professl'" John Quinn. Liverpool
lIospital . dated 18 June 20 1 0 3. Ceotrcltnk dcctr()nic file note 9 June 20lD 4. CCOIrelink daim for Disability SuppO/1 I'ensi'ln or Sickness AlIuwance
cumpleted 23 June 20 I 0
In addition, Ihese submissions make rcfcr~ncc to the report of Dr 1,11uisc Evans dated R January 201 S. pre"iously pmvidcd 10 the Tribunal on 14 May 2U15.
We apologi$e for the extended time that this mailer lws taken . The Ccntrelink recortls were obt<tincd bv wav ofFOI which , for rC;Jsons outside our control. took II significant period " fti mc. BXA has no fhrtlter motcri"lto suhm it. We thcrdore ask the T rib unal to make a dee,sltln soones! pussihle. foll"wing receip! "f this material.
Background
The atta(,.~hcu documents evidence 8XA s illnt:ss. ~yJl1pt0111S , ami diagnoses and directly link these tll her inability 0 une Ion and undertake work for several years between 2003 and 20 I~.
The IIIV transmission at the "ge of8 years old has progressively lead t,~BXA I suffering from AIDS defining illnesses "fOesophageal Candidiasis in 200.1 UJl(II'CP Pneuillonia in 20 I O.
414 ElIzabeth SLreel SUrry Hills NSW 2010 email: [email protected] WWW.I1alc.Org.8U
Tel: £02J 9206 2060 Fax: 102J 9206 2053
Freecall: 1800 063 060
STAT.0971.001.0175_R

At the time of diagnosis EXA Is CD4+ T cell COUllt wa' less than 200 x 10' 61i. The World Health Organisation 51 ages a ('04+ T ccllnf less than 200 x 10''6/1 as slage 4 AIDS.'
Dr Evans indicalcs Ihe incidence "fHIV amongsl Australian bom girls "I IBXA ~ s :lgc oftHlllsmission to be extremely raTe and too low tu uccuratcly quantitate. The significant impact or her assaull and HIV tral1smissio" as an 8 year (lId girl and subsequent AIDS related illnesses has leaclto depression. anxiety, alld severe posttraumatic slress disorder.
DiSllbility Support Pension
On 9 June 2010 CcnlrC\ink actioncd a claim for" Disability SUPPOl1 Pension. II was found thatEXA Ihad a physiclll, intellectuat or psychiatric impainnent of at least 20 points under the Social Security impaim,ent tables lor work related impainnenl. This impainllent was sufficient to prevent M!\~froJ11 undertaking educational or vocational or on lhcj ob training or from doing any work for a period of 2 years. Ms E:lat Ihis time satisfied the qualification required 10r the Disahility Support
Pension outlined in sectinn 94 of the Soci,,1 Sec"rity Act 1991. Please sec attachment archived CentrelinK Computer enlry.
Centreliok Claim for Disability Support Pension or Sickness Allowance
2
EXA I applied for a Disability Support Pension 011 23 June 2010. At quesliolls 79-81 oflhe claim, EXA Ilists H IV ~nd Depre.~sion (IS illnesses that she is suffc'Ting. she is receiving medicatIOn and counselling for these illnesses and Ihis affects her ability to work or study. fXA Isays"t question 137 that prior to claiming a disability pension her acu\'J1ICS wen: unl.'lnploymcllt "d,u! in }wIHi.'/l's.\'IrC',\',\' lIlItl heillK I·e ,)' sick·' . This evidence XA sown reeognilion that her HI V illness directly prevents her from undcrta mg wor or study and reduces her canting capacity. resultmg in ecunumic loss.
Medical Report for Disabilit), Support Pension
Associate Professor John Quinn. Consulumt 11l""unologist al verilied that lBXA ~vas unfit tor work for a period of three mn,11l11S
May 20 I 0 and 25 August 20 I () and unticipated Ihis would persist Ihr " period or at least 2 years.
Section 2 and 3 nfthe "Hached Centrciink Medical Report uuliined BXA s medical conditions that had a significant impact on her ability to func ton me uding ability to sit/stand/move, endurance. cOIl"itive limction. ability of selt~care and need for support for daily activities.
Associate Professor Quinn lists HIV Infection CDC stage B as the condition with the most impact on her functional ab ilities. 1111d Ihe only d iDllnosis Ihat supports D
Disability Support Pension applicatillil. The problems associaled with this diagnosis
, !lttQ.:/ www.cdc.govlm wljpr..evlew[!!J1Il'!JrhtmIJrr5710a3.htmHtaQ
STAT.0971.001.0176_R

-include insomnia, depression . weIght g~in . inahility to maintain employment , financial problems and poor adherence 10 medical therapy.
Sections H-J of the Ccntrclink MedIcal Report indicated that the efTect (If the HIV dillgnosis would persist ti" at least a thrther 24 months and was expected to remain unchanged for the period of 2 years.
Associate Professor Quinn indicated at question 4 that there were no other medical conditions that impacted M:BXA ability to limction aparl frum HIV and the ",,"eiated AIDS delining illness.
3
Medieol Report of22 JaulIal'y 20lS
In support ufthe Disability SUPPol1l'ension. Dr Louise Evans. a Staff Special ist at the Immunology Dept of liverpoOl Hospitlll outiined!BXA fs HIV diagnosis. The first AIDS defining illness of Oesophageal Candidiasis was diagnosed in 2003 . The second A IDS defining illness uf PCP pncumunia was diagnosed in 20 I O.
IBXA Iha" suffered from AIDS defining illness at least twice in her lite along with exlenslve human papilloma virus warts which have heen debrided through cryotherapy.
Dr Evans indicated that the significant impact of contracting HIV has contributed to depression. anxiety. and severe post-traumatic stress syndrome. The medical report SUppurIs the applicatiun fur u Disability Suppurt Pension in 20 IS.
Please find all ached a Centrclink Electronic rile note. A Centrelink medical reporl frum Associate Protessor Quin and a Medical repurl fmlll Dr Louise Evans.
It is our submission thnt the direct act or violence of HIV transmission tof XA I BXA esulted in severe medical conditill11s including AIDS defining illnesses. ThIS IS unl4ue 10 a persun o~s demographic und has caused significant health implications and sev~aumll1ie s tress disorder. This subsequently prevented
IBXA Ifrom being able to work and directly contriuuted to her economic loss.
It is our submission thaqBXA Ircc.ivcs compensation for this economic loss 10 the maximum value available under Ihe Victims Compensation Scene. Plcn~c refer to our previolls suhmissitlils dalcd 261h Octnhcr 20 15. estimating an actual economic loss ors 172.443.84.
Your assislam:c in this malter is apprecialed. I f you have any questions in relation to this letler. please do not hesitate 10 contact us.
Yours sinccrcl~ ? . ~ ,~p-, ~ \ ;. Indrovecr Chatterjee
Solicitur
STAT.0971.001.0177_R

"1(,~ . 9(
}S
rUt U::X 1 ("LU( - t-'Al31:: 0 01 Uj
. ~..o.\l <.!"~
I Document Recording (ODRIDOC) Archive
90l1l84833V
J /
jlJll1 e 11 t S
,)lIs 10 opu or cl01~ IIU Cold""
I.lp,:e.1I I
ReceIpt Oato Rgn Chnl Src Summary
1 JUN 2010 IGP LET SA317 CSO el.M asp -DSP NCL G/onl
Arthi,' cnvironWCQI S ()O 24 JUt. 2012 for eRN 20J884SJ3V
N.loc: XA
S,rvRen: 05P AdlServ : EnquhyClM Type;
Who:CSO annel Type: lET
Source:SA)17
DOA DOC:· Stofilgo: ON
Otnec: IGP
Rec eIpt Oat.,; 09 JUN 2010 Explry: -
Storage Date: ·
CSOClMDSP Ext Detail: OSP NCL: Grant
ClI\lomCr SCI'\'ltC Officer Ic.lioncd record 011_ 5> JUN 1010 rcgcudulJ
Clllim rorOiubiliry Support Pcmioo, 1nCormaliou W"l cbtaint.d \; .,
Auth:s22
New Claim tonu (or DSP SKA NSA SPB usin, P-bil. DoCUruCDI erc",rcd by
s22 011_7 JUL 2010. CuSIOWCf b.a~ a pL)'\ical. tin clIcenl:!1 or p~ychi.tnc lmpai.nnctu alld
Ibe impainlu:nt n lull bA\ bct.1\ :l;u;cs.~d I\f bcinS 31 le1\1 20 poisu"
TIll: impl inllt.ol j, cfilld( \ufficic:nt to prc\'cnllhc «="\10111" {rom
doin,auy wOlk wilhin lhe nut 2 yCM"Sl\nd cilller prevenl IheiU (roUl
undertaking edlleatiodolll or \'ouliOiW or on the job IrDmin, duriul
Ihe: lIc:<12 yc;,n, ol1l1ch Ir.tUUJlI h \Ul.lil;ely 10 cunb!c We """outer
10 do Il!1Y woO; \\;Ihin tbe nUl ! yeaD. 594 of lhe Soci .. 1 Sctluity ACI j, Ibert-fort. ~I'\fied.
DOC by 522 . AMR: 1549
F
17 JUN 2008 PEN PER INV CUS CLM VAL • VAL gnm'od 6 JUN 2008 F
en Hdp XA Ar~hi\';~d &om CII\'irolUucnl S 01124 JUt 2012 forCRN 20JSS4S3JV
_~IU:C: I S.rvRsn: YAL
Who;CUS ,onnel Type: PER
AdlServ :
Soutce: INV OOAOOC : ·
SIOflloe:ON Office: fJEN
EnqulryClM Typ.:
Receipt Qat&: 17 JUN 2008 expiry:·
Storugc DllIte : · Auth : 522
n: CUS ClM YAl Ext Oetoll: YN... 0181~DCI 5 JUN 2008
Cm,IOlUcrCOUUIUcd PENRln-I on 17 JUN lOGS tcgl'fdl.ng CIAlm (orYolllh
AlIow:ance. 111lom"1,iou \\A~ obtllU:!cd ... i" lJ'IIcmcw u~iai PersonDI ~ In
Office. Document CCClllcd by s22 on 17 /UN 2008
Cl.illl (<< Ycnllb AlloWMI:t. hn~ been itAnled under 040 SSA
POI Tier Le".",l Aeh.iC\·td: .3 Tot,1 POI Poiau Achieved: 100
03 MIIR 2008 PEN PER PHO CUS CLM CSIl YAL • YAl rojocl.d 11 FEB 2008
.... \-1 .. 1.. Archi\'cd bOUl cn\yoJWlml S on 14 nJL 2012 for CRN lOJS848j3V
_............, ____ N_·une:_ ... r_XA _________ ~-
ServRsn: YAL AdlServ:
Who:CUS Source: PHO
EnqullY elM CSR Type:
Rtc~lpt Date: 03 MAIl 2008
F
P,;n,jnp InfomllJtlon end fAO
STAT.0971.001.0178_R

When to use this form Use this form if you arc claiming one of the following:
.. " ..
Disability Support Pension
A payment for people who:
• are permanently blind, OR
• have disabilities, illnesses or Injuries which prevenlthem from working or retraining for work for 2 years or more, AND
• are aged 16 or over and under Age Pension age at the timB of claiming.
Sickness Allowance A payment for people who are lemporarily unable to work or study due to a disability, iIIflilSS or Injury and are:
• aged 21 or over and employed, OR /\ ' aged 21 or over and on ABSTUDY, OR
/ -. aged 25 or oyer and on AUS1udy, AND
> ve work or sludy 10 return 10 When tlley are better.
V ,.' & You sh lid have received the booklet Information yau need /0 know aboul your claim far Disability " • '\.r::.~ Suppa ension, Sickness Allowance and Mablllty Allowance with this form. In th is claim (onn, 6" ~....... ~~ Ihl~,litfOk will be referred to as the Informatlon Booklet. If you do not have this booklet, call us () '\. -:. ••• o~ ) 17 or go to our website at www.centrellnk.gov.au
" .,. ... . ,~ '
rwpt~ .' Gall Cenlrelink on 13 2717, visit your local Centre link Customer SelVice Centro or go to our website
If you have a hearing or speech impairment
Interpreters and translations
What else you will need to provide
Filling in this form
SA311{bj. l003
at www.centrelink.goY.au
To speak to Centrellnk In languages other than English, call 13 1202.
Note: Calls from your home phone to Centrellnll 13 numbers from anyWhere In Australia are charged at a fixed rale. That rate may vary from the price of a lOcal call and may also vary between telephone service providers. Galls (rom public and mobile phones may be timed and charged at a higher rate.
T1Y service FreecaUTM 1800 810 SOB. A m phone Is required to use this service.
II you need an Interpreter or 'rBnslation of any documents for Cenlrellnk business, we can arrange this for you free of charge.
You will need to provide proof of Identlly. There is a complete list of acceptable documents In the Information Booklet.
This form tells you which other documents yO\) need to provide to support your claim.
Depending on your circumstances, you may have to fill In other forms.
Please use black or blue pen.
Mark boxes like thisO wlih a ticK v or )(.
Where you see a box like this [-::. Go to 5 skip 10 the quesllon number shown. You do not need 10 answer the questions In between.
1 of 26
STAT.0971.001.0179_R

-.R~tufning your.forlT!(s)
Form.s in your claim pack
.•
.-
What to do next if you are claiming Disability Support Pension
"
i>isa~ilily Support Pension for people who Clre I)ermanently blind
What to do next if you are claiming SlckneS's Allowance .
rUI U:X 1/'LUI - t-'AGl: 1:J4 or 'L'L3 Check that you have answered all the questions you need to answer and that you have signer1d dated this form. • . ~ • . , ~
If you return required documents (and your claim form): • by post- we will photocopy your documents and return Ihe originals to you by registered post.
• in person - we will phOtocopy your documents and return the originals to you.
Return this form, all additional documenls and any other forms you are required 10 complele to a Cenlrelink Customer Service Cenlre within 14 days to ensure you are paid from the earliest date possible.
II you cannot return all the forms or documents williin 14 days, contact Centrelink for extra time.
In your claim pack, you should have the followkJg: • Information you need to know about your claim for Disability Support Pensioll, Sickness
AllowanCB and Mobility Allowance (CI001) (Informallon Booklet)
• Claim for Disability SUPPDrt Pension or Sickness Allowance form (SA317(b)) • Medical Report Disability Support Pension form (SAOI2)
• Income snd Assets form (SA369)
You must get the doctor who normally IrealS you to complete the Medical Report Disability Support Pension form (SA012) included in this pack, unless any 01 the circumstances below apply to you.
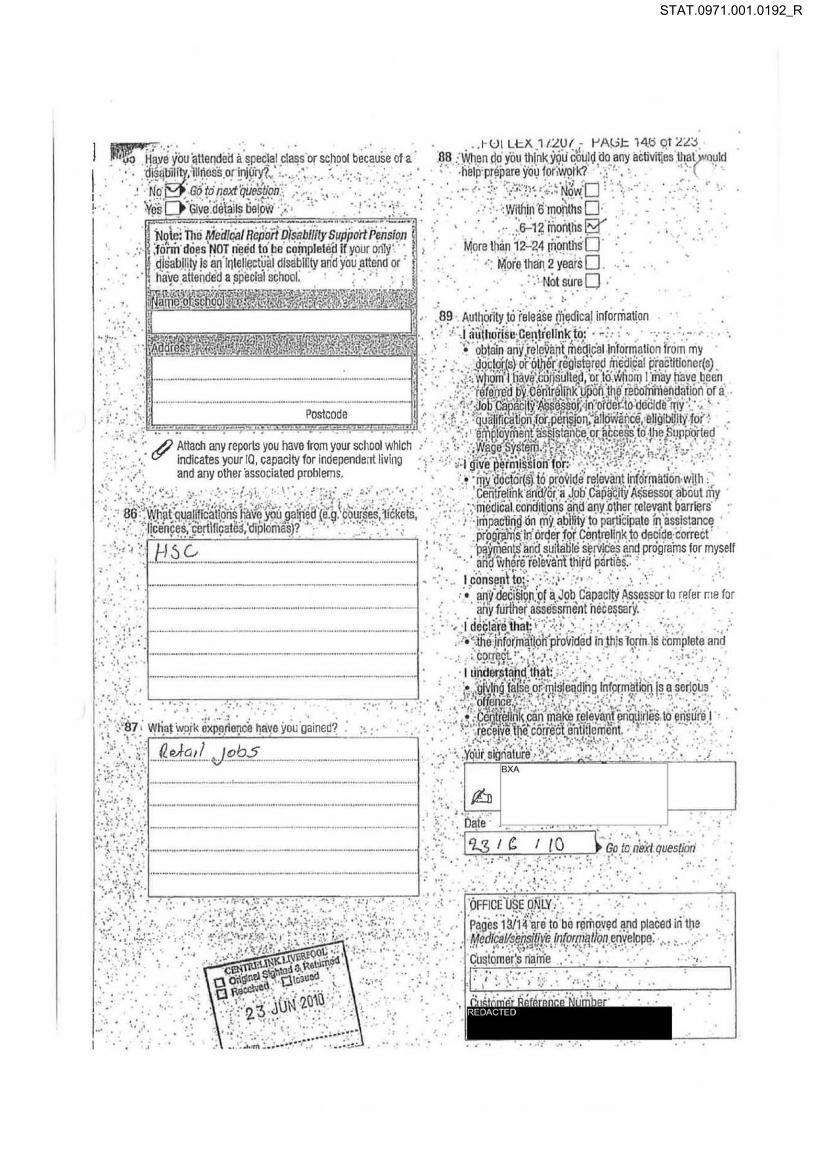
111e MedIcal Repolf Disability Suppolf Pension does N01 need to be completed H:
• your only disability Is an intelleclual disability and you attend or have attended a speCial school and are able to provide a reportlrom your school which Indicates your 10, capacity lor Independent living and any olher associated problems, or
• you arB claiming on Ihe basis lhat you are permanently blind and you are able to provide a reparl from an ophthalmologist or
• you have been assessed as being a profoundly disabled child and you had a carer who was receiving Carer Payment up to the time you tumed 16 years of age, or
• you are receiving Disability Pension at tlte Special Rate [Totally and Permanently Incapacllated) from the Departmenl 01 Veterans' Affairs.
Make an appointment with the ophlhalmologlsVoptomctrist who usually treats you. You should have received from Centrelink. a Request for Ophthalmologist/Optometrist Report form (SAOI3).
When you make 100 appointment, tell tha receptionist Ihat you need the ophthalmologlsVoptomellist to complete a form for Centrellnl(, as they may need to alloVi more time. 1hey may complete the repon and give it bacl( to you or they may send it directly to Cenlrelink. Make sure the report has your name and address an It and you have signed the declarallon.
Do NOT complete the Medical Report Disability Support Pension Included in this pack.
You must atlach an approved Centrellnk Medical Certificate completed by your treating daclor. Your doclor will be able to provide you wilh Ihls Medical Certificate.
2 012G
STAT.0971.001.0180_R

( onal details
1 . Indicate which payment you are claiming
2
3
Noto: If you are not sure whether you ara claiming Sickness Allowance or Disebility Support Pension call Centrellnk on 13 2717.
Tick ONE box only
Disability Support Pension 0 Sickness Allowance II
00 you need an Interpreter when dealing with Centre link? This Includes an Interpreter lor people who have a hearing or speech impairment.
No 9 Go 10 noxt question Yes D What is your preferred spol(cn language?
[ ____ _ _ --,I What is your prelerred written language?
L ____ ___ 1
Your name
MrO Mrs D MISS~Sn Other \ -:==1 Family name
I':-BXA...,.-,--_-'L----. __ l First given name _ _ ::oJ
4 Havo you evor used Of' been known by any other name (e.g. name at birth, malden name, previous married name, Aboriginal or tribal name, alias, adoptive name, foster name)?
No 9 Go fo next qU8s/lon Yes 0 Give details below - ---lIt Other name -=:]1 ,-Type of name (e.o. name at birth)
I -- - .-fiJOiher name
- -
.H .. _H._. __ .... _ 11 ....... _ .. _ .... _ ...... _ ..... __ ......... _ ....
I Type of name (e.g. malden name) . - -
I If you have more than 2 other names, attach a separate sheet with details.
I
I
5 Your sex
. Malc D Female E?/
6 Your date 01 birth
7 Your Customer Reference Number (if knoVln) REOACl( [) --- -
B Your permanent address
9 Your postal address (if different to above)
REDACT{ [)
•••• ••• ••• •• _. __ M ... ....... ..
_____ _ _ _ os_t_co_de--'18I-
STAT.0971.001.0181_R

10 Vour contact details
Home phone number 1...1 ( _____ -=,-_::::'
15 this a silent number? No 0 Yes 0 Mobile phOne number REDACT! 0
Fax number ~===~
Work phone number 1 (
~===~ Alternative phone number 1...1 ( ________ --'
11 Are you claiming Disability Support Pension and are you under 2~~h no dependent children?
No ~ Go 10 next Queslion @!CS ~'Give details below
Whose name is lIle phone account tn?
My name 0 My partner's name 0
Another name 0
WhOse name is the mobile phone account tn?
My name E( My partner's name 0
Anotller name 0
Name of your I10me Internet Service Provider (ISP) The ISP Is the company that provides your Internet access.
1 I
Whose name Is the ISP account in?
My name 0 My partne~s name 0
Another name 0
12 Ar~YOU lalming Sickness Allowance? No ~ Go /0 nexl quos/ion
Give delalls beloVi
Whose name is the phone account In?
My name 0 My partner's name 0
Another name 0
Whose name Is the mobile ~one eccountln?
My name ~ My partner's name 0
Another name 0
CUI Li::1\ 1 I"LUI - t-'AGt: l~o at "L"L~
13 Questions 13 and 14 are optional aM will not alIcct ( payment. If you do answer, the informaUon will help ·us to continu6to Improve services to Abenglnal, Torres Strait · and Australian South Sea Islander peoples.
Are you of Abonglnal or Torres Strait Islander origin? If you are of both Aboriginal and Torres Strait Islander origin, please IIcl( both 'Ves' boxes.
No Q / Yes - Aboriglnat ~
Ves - Torres Straltlslander 0
14 Iva you of Australian South Sea ISlander origin?
Nog'
Yes 0
15 Please read this before answering the following qucstions.
Questions 16 to 21 are optional and will not affect yet" payment. If you do answer, the inlormalion will help us to continue to improve our Etectronic Messaging Services. You can now receive reminders and Important information via ShOrt Message Service (SMS) or email Irom Centrelink. You MUST read the Terms and Conditions for SMS, email and Online Leiters In tho Information Booklet before you complete the following questions.
16 Do you wish to receive reminders and important Information via SMS or email from Centrelink?
This service is voluntalY and you are able to wllhdraw lrom it at any time.
No 0 Go fo next quesllotr Yes ~ SMS contact number
(if different to contact detailS)
OR Email address {if (Iifterent to contact details)
I@
17 Do you wish to view some 01 your Centre link and Family Assistance ONlce letters via the Online Letters facility on the Ccntrelinl( website?
This service is voluntary and you are able to withdraw from it at any time.
N00 Go 10 19
Ves 0 Go to next question
STAT.0971.001.0182_R

1 r \~hat Is your preferred method of notification?
_. Centreffnk will noilly you when you have a letter available for viewing In the Online Lotters faCility.
Ticlf ONE}ax only SMS IS!) SMS contact number
rlf different to contact details)
Email [} Email address (If different to contact derails)
I@
19 Did you answer 'No' 10 either Question 16 or question In NO~GOI022
Yes [} Go fa next question
20 What Is Ule reason for not wanting 10 use Ihls service?
The Intormatlon will help us to continue to Improve services.
Do not trust the Inlernet 0 Do not have a mobile phone 0 00 not have Ihe lechnology 0
Other [} Giva reason
21 Would you lII\e to be reminded of Ihls service In Ihe future?
No [} Go to next quesYon Yes [} When would you like to be reminded?
in 6 months 0 In 12 months 0
Payment details
22 Where do you want your payment made? Tha bank, building society or credit union account must be In your name. A JOint account Is acceplable.
Name of bank, building society or cred~ union
Branch where your account is held
Branch number (BSS) Account number (this may nol be
your card number)
REOA( TED
IREDACTED
REfJA( TED
REDACTED
Account held in tile name(s) of
f -]
~Ulll::)\ 1 f"-Uf- "AGI:: 1:l( 01 a:l
Relationship details
23 What Is your CURRENT relationship status?
Please read this belore you answer this question.
From 1 July 2009, Ccntrellnk reccgnlses both opposite· sex and same·sex relallonshlps. This Includes de lacto relationships and retationships registered under state or territory law. Select ONE option below that best describes your current relationship slatus.
Married D Go 10 24
Registered retatlonShlp (opposlte·sox Of same·sex relationsl1lp reglstored under slate or terrilolY law) [} Go to 24
Partnered ffll1ng logether In an opposl/e-sex or same-sex relationship, Inc/udlng de facio) [} Go /025
Separated (previously lived with an opposlfe-sex or same-sex partner, Including in 8 marriage, regislered or de facio re/allonsl1ip) D Go /0 32
Divorced [} Go 1032
Widowed (previously partnerod willI an opposile·sex or samo·sox partnor. inCluding In a merriage, fegls/Bred or de facio relationship) [} Go to 31
Never married or tived with a partner ~ Go to 41
24 What is your date 01 marriage Of relationship registration?
'-_ , _____ -T Go to 20
25 When did you and your partner start living together as e couple?
I ' 26 00 you currently live In the same home as your partner?
No [} Go 10 next question Yes [} Go to 34
27 Your partner"s pemlanent address
I Postcode
28 Your partner's postal address Cn different to above)
1==:::==-==-==1 . postcode.
STAT.0971.001.0183_R

29 Wny ars you not living with your partner?
Partner's illness [] Yourlllness[]
Partner In prison 0 Partner's employment []
other 0 Give details below
30 Period not living with your partner
From I I I I To It~" 1 -~ORI~d~O
Go to 34
31 Please give the following details about your deceased partner,
Full name
[ D~at~e~of~b~lrt~h~ ____ ~~Da~t~e~m~d~ea~th~ ____ ~
L_ 1 1 II 1 I
;'Gof040 -------------,,---------
32 Do you live In the same home as your former partner?
No 0 Go to next Question YesD Go fo 40
ssm
33 Please give Ule following details about your former partner,
Full name
1 __ " ."_--=-_"-=-_"=_-- , ~_=I Date of birth Date relatlonshl~ ended
l ___ --lll 1 1
;. Got04u __ .I
Partner's details
34 Your partner's name
MrrJ Mrs[j Miss[J MsO otherC - -]
FamilY name
[ =oJ First given name
Second given name
r UI U :)\ 1/'LU (" I-'AGc 1 ~ts aT L'L~
35 Has your partnor ever used or been.known by any ot~- , name (e,g, name at birth, maiden name, previous rna" ,.-J name, AbOriginal or tribal name, alias, adoptive name, foster name)?
No 0 Go to next question Yes 0 Give detailS below
~hername
L, " I
'TYpe of name (e,g, name at birth) '--" '- --_. ::::J L-Efother name
-- ._-,,-
F---' = ........... _ ........... __ ..... • ~ .... - .•• « ,,,,,,,,,,, ,,,,,,·,,,,,,,,,-,,-,,,,,,-,,,,,,1
Type of name (e,g, molden name)
I , " ..
If your partner has more than 2 other names, anach a separate sheet with detailS,
36 Your partner's sex
MaleO Female [I
37 Your partner's date of birth
1,,_' .,! ''' ~:,~ .~=J 38 Your partner's Customer Reference Number (if known)
I I-L'.J-[~~]-rJ
39 00 you give permiSSion for your partner to discuss your payments with us? You can change this authOrity at any time.
NogGot043 YesG
Your living arrangements
1
40 Are you mallied, in a registered relationsilip or partnered (including de facto)?
No 0 Go to -next question Yes I-} Go to 43
41 00 you share your accommodation with anyone other than an Immediate member of your family? Nag Go to 43
Yes 0 Go to next Quesffon
STAT.0971.001.0184_R

42~ Dlease read this before you answer Ihe following. ( . The following Queslions are to be completed If you share
your accommodation with anyone other Ihan an immediate family membor. This Includes anyone wilo: • regularly stays any number of nighls per week • uses your home as a base (e.g. lruck drivers, miners,
nighl allondanls, fishermen, members of the armed forces).
Centrelink needs some details about your living arrangemenls to work out your correct payment. The questions on this form will assist us to decide whether we need additional information.
Give details of each person who shares your accommodalion. 00 not include Immediate members.
Name Ago ;===..:.:.:::.::..:....-----.1 D Sex
When did you start sharing \'Iml this pel son?
G aleO ~m~e CDC==_' ___ ' ____ ~1 Whal Is your relationship to this person?
Have you shared accommodation, at another address, with this person? NoD
YasD
J
Have you and this person previously lived together as a couple (e.g. married, partnered, de facto or In a registered relationship)? NoD Yesil
55293
00 you and this person share the parenVguardiansilip of any children?
NoD Yes 0
ssm Hava you and this person ever had any joint financial commilmen~ (e.g. joint bank account, mortgage or other loans)? NoD
If you partlcipale In activities jointly with this person, are you considered to be a couple? • NoD
Yes 0 Give details below
5528./ .......... _ .......... _ .... ..... _ ...... _ .•• _ .. _ ... _ ............... /
Continued
~Name Age
L-I ___ __ ..-JID When did you start
,..S.;:.CX_=- __ -:=-, sharing with this person?
~~Ie 0 .. Fen:.~~ L I I =oJ What Is your relationship to this person?
Have you shared accommodation, at another address, with this person? No D
Yes 0 Have you and this person previously lived together as a couple (e.g. married, partnered, de facio or in a rcglstered relationship)? NoD
Yes 0 55293
Do you and this person share the parenVguardianship of any children?
NoD Yes 0
ssm liave you and tilis person ever had WlY Joint flnoncial commitments (e.g. join! bank account, mortgage or olher loans)? NoD Yes 0 Give details below
55293
1 ..... - ... - .. - . ... - ............................... -.=3 If you participate in activities jOintly with this person, are you considered to be a couple? No D
Yes 0 Give details below ssm
..•• _ ... _ ....••. _·····_··_ .. ·1
If you share with more than 2 other people, attach a separate sheet with detaits.
STAT.0971.001.0185_R

Residence details
43 In the last 14 days have you received or claimed any of the following payments (not Including Family Tax Benefit)?
• A8STUOV • Parenting Payment • Austudy - single, or • Carer Payment - partnered • Disability Support • Partner Allowance
Pension • Sickness Allowance -Including pension • Special Benefit for permanently blind • Widow
• NewstartAliowance Allowance/Pension
No [} Go to next quesUon Yes9(;0/06f
• Wife Pension • Youth Nlowance.
44 Please read this before answering lite question.
'Permanently' means you normally live In Auslralia on a long-term basis. Holidays or short tr1ps outside Austra lia would nol affect this.
Are you living permanently In Australia?
~Jo [} Go to next question Yes [} Go /0 46
45 What country do you permanently live in?
I 46 Have you lived or travelled outside Australia since
1 September 1994, Including short trips and holidays?
No [} Go to next question Ves [} Give details below Passport number
I I Counlry_ol_ls:.,:s-'-ue'--_____ _____ _
~. J 47 Are you an Australian citizen who was born In Australia?
No [ } # You will need to provide pr<?Of 01 your residence status (e.g. citizenship papers, passport or other documentation).
~ Go to next quest/on
YesD 60/060
4B What is your country of birth?
I 49 WIlen did you start living In Australia?
I I ,
I-UI LeX 1 ''LU' - t-'A\3e 14U 01 a~
50 Did you start living In Australia before 19657
No [} Go to next ques/Ion Yes [} Give delai ls below
Name of the ship or airline on which you arTived
c
Name of the place where you first arrived/disembarked
I What was your name when you first arrived In Australia?
I 1
51 Are you an Australian cllizen?
No [} Go to next quest/Off Yes 0 Date you became an Australian cillzen
[ /, ~ Go to 57
52 What is your country of clllzenship?
New Zealand 0 Go to next question Other [} Give details below
53 Old you arrive on a New Zealand passporJ?
No Ll YesU
54 What type of visa did you arrive on? Permanent 0 Go to next question Temporary [} Go /0 next question
Unlmown (e.g. arrived on [) Go to 56 mothor'sf/ather's passport)
55 Your visa details on arrival Visa sub class _ _ --, Date vtsa granted
1_ _ __--'11<--_' _ ' _ _ J 56 Has your visa changed since you arrived In Australia?
No [} Go to next question Yes 0 Current visa details ;.:.VI",sa",s",ub::..c",la",s,,-s ___ -, Dale visa granted
1<--___ 0]1 ' / 57 Did someone provide you with an Assurance of Support for
your migration to Australia?
NoD Not sure 0
Yes 0
STAT.0971.001.0186_R

5a r" YOU iI refugee 0( former refugee?
',01:] Yes 0
59 Did elthor of your parents arrive on a refugee or humanitarian visa?
NoD Yes 0
60 Except for Short trips or holidays, have you EVER lived outside Australia?
No 0 Go to next quesuon
Yes [) List All counlrles, tNCLUDtNG AUSTRALIA, you have lived in StNCE BIRTH.
Include Ihe perlod(s) you have lived in Australia.
It you were born outside Australia, Include the country where you were born.
Do NOr include short trips or holidays.
~CO;;~ - ~"'~ :=i I --;:=:===-=::::;--;==-.-J I fr~1 I -. ] ro[/' D
~~nlry of residence 3
I I ~o-mlr==I===/~I-rn~I=='= I ]
_. -=-a 9 Country oi residence -
I from I I I I To[ I I I =- _.
~ COO.". rn"~. I I From I I I I ro l I I I ~'counIrY of resldonco
it I from I I I I To I I I I m Country of residence
I J from i I I I ro l I I I If you require more space, aUach a separate sheet with details.
rUI li::i<. 1 rLUI - I"f\l;;t: 141 at LLJ
61 Do you .!Jave a partner?
No@ Ou not 811swer quesllons 62 to 77. Gala 78
Yes 0 Go to next question
62 In the last 14 days has your partner received or ctalmed any of the following payments (not Including Family Tax
Benefit)?
• ABSTUDY • Parenling Payment
• Age Pension - single, or
• Austudy - partnered
• Carer Payment • Partner Allowance
• Disability Support • Sickness Allowance
Pension • Special Benefit - includinll pension for • Widow permanently blind Allowance/Pension
• NewstartAliowance • Wife Pension • Youth Allowance.
No [',; Go 10 next question
Ves C~ Go to 78
63 Please read this before answering the question.
'Permanently' means your partner normally lives in Australia on a long-term basis. Holidays or short trips outside Australia would not affect this.
Is your partner living permanentlv in Australia?
No 0 Go /0 next question
Yes 0 Go to 65
64 What counlry does your partner permanently live In?
L ]
65 Has your partner lived or trnvelled outside Austrnlla since 1 September 1994, including shortlrips and holidays?
No 0 Go /0 next question
Yes [) Give detailS below
Passport number
I Country of Issue
C 66 Is your partner an Australian citizen WilD was born in
Australia?
No D ' # You will need 10 provide proof of your partner's rnsldence status (e.g. cftlzcnsllifl pallors, passport or other documentation). ~ Go to next question
Yes 0 Go to 77
STAT.0971.001.0187_R

67 What is your partner's country 01 birth?
I 68 When did your partner start living in Australia?
I / 1
69 Old your partner slart living In Austratia belore 19657 No IJ Go to next quesl/on
Yes 0 Give details below
Name of the ship or airline on which your partner arriVed
i :=oJ Name of the place where your partner lirst arrived/disembarked
'-- _ ._---------' What was your partner's name when they first arrived in Australra_' ?:...' __________ __ -,
1'" _-_______ ---'
70 Is your partner an Australian citizen?
No 0 60 to next quesl/on Yes 0 Date your partner became an Australian citizen
I. / / ~ Gol07B
71 What Is your partner's country of citizenship?
New Zealand 0 Go to next quest/on Other 0 Give details below
C --',,,.,,1 72 Old your partner arrive on a New Zealand passport?
NO[] YesCi
73 What type of visa did your partner arriVe on?
Permanent 0 Go to next quest/on TemporaryD Go (0 next question
Unknown (e,g. arrived on 0 Go to 75 mother's/father's passport)
74 Your partner's visa details on arrival Visa sub class Date vise granted
1 " I I
rUI Lt:X 1 /~U(· t-'AGt: 14£ at ££:l
75 Has your partner's visa changed since they arrtve~ '-. Australia? \
No 0 Go to next question Yes 0 Current ~isa details Visa sub class Date visa granted r=.:.=-::cc.:::......--
II / I
76 Is your partner a refugee or former refugee?
NoD Yes O
77 Except for short trips or holidays, has your partner EVER lived outside Australia?
No 0 Go to next question
Yes 0 List All countries, INCLUDtNG AUSTRALIA, your partner has lived In SINCE BIRTH. Include the perlod(s) your partner has lived In Austrnlia. If your partner was born outside Australia, Include the country where they were born. Do NOT include short trips or holidays.
II!l. Country ot residence
I I From 1 I / I Tal / / I
.~--. --I!2l Country of residence
L ~ From i / i 1 Ta l / I I ...
Country of residence
L-;:====;-;====I From 1 1 Tal I I 1
fountry of residence ~
~~t=ml ====;--1 Tori =d ~ Country of residence
3 I From[ I I ITOC:= .I
~ Country of residence
1
From I I / I To l / I
II you require more space, attach a separate sheet with details.
I
I
STAT.0971.001.0188_R

rUI LI=)( 11LUI - I-'AL;t: 14;) 01 LL;)
(' . ,ndent children details
ZS Do y~!:l.9are for any children under 18 years of age IJ( fUll-time students under 22 years of age? No ~ Go to next Question
Yes 0 Give the follOwing details of each child
If you have more than 2 dependent children, aUacl) a separate sheet With details.
CI A
-1Iid 1 Family name
I Flrst given name
I Second given name
I
... -
····r ~
I
fCh A
I
lid 2 Family name ,-First given name
I Second given name
I
- -- -
B Has lhls child ever been known by any other names? B Has Ihis child ever been known by any other names?
No 0 Go /0 C for this child No 0 Go to G (or 11115 child
Yes 0 List the oth8( names Yes 0 List the other names
C ~ C c Sex c Sex
Male 0 Male 0 Female 0 Female 0
o Date of birth o Date of birth
I I I =:J ~I I ~ -E What Is thiS child's country of birth? E Whet is this child's country of birth? 1 -·----__ . --I ,
I
---
-, I I
I
J F Has thIs child lived or travelled outside Australia since F Has Ulls child lived or travelled outsIde Australia since
1 September 1994, Including short trips and hOlidays? 1 September 1994, Including short trips and holidaYll? No 0 Go /0 G for fhis child No 0 Go to G (or this cMld
Yes 0 Give details belOW Yes 0 Gille details below Passport number -I I
Pass~ort number
I I Country of issue Country of Issue 1 I L I I
au flStions for IMs child continue on /110 next page aue sffons for Ilris child continuB on the next page - - - -
STAT.0971.001.0189_R

Continued r-------------------------Child 1
G Please mad this before you answer the queslion.
The lerm 'parent' refers 10 a natural parent, adoplive parenl or a person who Is legally responsible lor a child born II1rough an arlificlal conceplion procedure or where a surrogacy court order Is in place.
Which of Ihe following best describes your relationship to this child?
Parent 0 Grun~parent 0 Step-parent 0 Fosler carerO
DlIlerD Give details below
H Does this child currenlly live with you?
NoD YesD
00 you landlor your partne~ slme lI1e care of this child with another person? Do not include schooVday care arrangements.
No D Go to J for this cftild Yes 0 What Is the percentage of your (or your
partner's) care of this chUd?
1 %1 J Does this Cllild receive a payment from any
Commonwealth, state or llnitory government'?
No 0 Go to K for this child Yes D Give details below
,'------] K Is this child 5 years or older?
No IJ Go to N for /lJis child Yes 0 Go to L for this child
L Is Ihis child In full-time education?
No D Yes D
M Does this child have any income? No D Go to N for tllis child
YesDAmount rl$--~------pe-r-W-e-el('1
N Do you receive Family Tax Benefit for thts child?
No D # Attach proof of birth (e.g. birth certificate) for Ihis child if you have not previously provided it to Centrelink.
YosD
rUI LI=X 1 t'LUt - J-'AGI= 144 ot 'L'L:.l
r----- - ----------------.( Child 2 G Please read this before you answer the question.
The term 'parent' refers to a natural parent, adoptive parent or a person who Is legally responsible for a child born through an artificial conception procedure or whore a surrogacy court order is in place.
Which of the following best describes your relationship to this child?
Parent[)
Grandparent 0 Slep-parent[) Foster carer[)
otherO Give details below
Ii Does this child currently live with you?
No D Yes 0 Do you (and/or your partner) share the care of this child with another person? 00 not include school/day care arrangements.
No 0 Go to J for this child Yes 0 What is Ihe percentage 01 your (or your
partner's) care of this child?
I %1 J Does this child receive a payment from any
Commonwealth, state or territory government? No [) Go to K for this child
Yes [) Give details below
K Is this child 5 years or older?
No 0 Go to N for this child Yes 0 Go to L fOf this child
L Is this child in full-time education?
NoLI Yes Ci
M Does III Is child have any Income? No [) Go to N (or Ihls child
Yes [) Amount rl $-'--'--- -p-er-w-ee-,k I
N Do you receive Family Tax Benefit for this child?
NoO # JIUnch proof of birth (e.g. birth certificate) for this child 1/ you tlave not previously provided it to Centrellnk.
Yes 0
STAT.0971.001.0190_R

..
. '
list any disalJililles.lllnesses or injuries that you ~ave
I·II.,} PrS-r'" ('() 0 .0 lob ue.s -~" "'-" "r-.--.. --.--.. ---I .. - .. ---••. -.-... - .. _ _ ._l __ •.•. _ ••
. _~L~S :.01"1 __ ..... _ ..... __ .. __ . __ .: .. _
.- ._-_._ .. __ ....• _ .••. __ ._-_. __ ... _ ... _ ..•. _ ....••. _._ .. " '."'.'
, ~"
80 . Are 'YQ~ currently r~~eivIJg 'any tr~~tirlent (0(' ~ur . ~Isaqilities.llln·ess~s or Injuries (e.g'l)ledi.catior:ilhyslcal therapy. ~punsel1lng. s~rgery)? ... .. . N~"[} Go ID nokr quesUon .... .
Yes 9' Give details below
---_ .. _._-------------------_._-_ .. -
, . If you need more space. attach a separate sheet with details.
. . ;','., ...... . . · . . · . '", .. '. '. .
81 Does this treatment affect yOur ability 'to \ilork or Jitudy .• (e.g. Y.9.~r in.ob!lIty;.c~p~tI!Y t9.I!ftIcarry, ~a'y to .. ~~Y 1I~lng,
ability to rel)1embtir ahd c9mmunlCllte (v1ti1 Olher people)? . • '. " • " 4. .. , ' . ' ~. .. No O.)3rJ to next queStion . . . ' . Yes ~ Give. details ~~lo\Y . . ' . ., ' .
. __ . ____ ... __ ... N._ .. ' .. ___ ... _ ........ _, __ ......... . _._----_ ... _ .. ---_ ........ -. __ .. _ .. _. __ .. .'
If you need more space, attach a separate sheet with details.
.' . .. '
. ' .
8,2 . Are you ~~6rlntg{b Aa'~'8~ ape'titibiNn 1~tlMr6¥J N~-mo 'to .next quesUon
Yes 0 G.lve details' below
If you need more space. attach a separate sheet with details.
83 'ust .8!1Y d~tor~ (apait.l~iP·Ute .d~.ctor cotllpleting the ·M.~iffMllJqfio!J O!s~bi!i(y ~uPP9f! Pe!,si~nfO(fil or qelllril?i/1~ lyJe.r!lc~IP~rl!fI.c.~~e) •. ¥fl,ec;janst~:er other professionals who coula teir us abbut your disabtlltles. ijlnesses or InJunes (e.g. cillinsellor. social worker, Ef!lploym~pt Servi.ces Prpvid~r. psychologist, community Ii~ili~ wor.ker, ppyslotherap.~I. sPec!all~t, .rehab!litapon provider). ' .' .
If you have morc than 1 professlon,1 10 list. attach a separate sheet with details.
/} Attach any professional's reports you have that are if relevanl to your dalm .
'84 W!1iI1 Is tiie hl9h~ le~~1 of eduCation you have COlllpleted . (e .. g. Year.9 .. ye~r11.Te.rtJalY. OIjJlorl)8)? .• '.' .
Note: If completed outside AUstralia, Indicate the . Australian equivalent. If you are not sure of the Australian
equivalent, call us on 13 2717.
ILleo( 12.. ." "
' . ' ..
. 136f26 . " ',. . .
STAT.0971.001.0191_R
I I· I ! . .
II ' : .. ' I : ~ II' REDACTED
... :' ". ... .
. .
STAT.0971.001.0192_R

Tf' ' ''!~_.~s
90 Please read this before answering the following questions about tax.
You are not breaking the law If you do not give us your (and your partner's) tax file number(s), but if you (and your partner) do not provide them, or authorise us to get them Irom the Australian TaxatIOn Office, you may not be paid.
Have you (and your partner) given us your tax file number(s) before?
No 0 Go to next question Not sure 9 Go to next question
Yes~ Go 10 92
91 00 you (and your partner) have a tax file number(s)?
No C~ Please call us on 13 2n7. Yes [) Your tax lIIe number
DIHJJJ-CD] .-------=-=~
No 0 Please call us on 13 2717.
Yes 0 Your partner's tax file number
[[JJ-C:TI-[Lj]
92 Are you claiming Disability Support Pension?
No g Go to next quesYon Yes~ Go to 94
93 Please read this before answering tho question.
11 your only Ircome tor this financial year Is the payment you are now claiming, you may not havo to pay any tax. However, you may have to pay tax il you get any other Incomo this financial year, such as salary or wages. It you think you will have to pay tax this year, you can ask us to deduct tax Instatments from your payment. You can chango this at eny lime. II you are not sure how much tax to have taken out 01 your payment, contact tM Australian Taxation Oftlco.
00 you "ant tax taken out 01 your payment?
No@ Go to next Question Yes C~ Enter Ihe amount OR percentage of tax you wont
taken out per fortnigllt
Amount Percentage ('!o) (must be in whole dollars) of taxable payment
Is .00 per fortnight 10RI % per fortnight I
rUt LI::>I lI:lUI - C'Alil:: 141 01 4Z:S
Accommodation detoils
94 Have YOll (and/or your partner) claimed or been paid any of the fOllowing payments in the last 14 days?
• ABSTUOY • Portner Allowance • Age Pension • Parenting Payment • Austudy • Sickness Allowance • Carer Payment • Speclat Benefit • Disability Support Pension • Widow AllowancelPension • family Tax Benelit • Wife Pension • Newstart Allowance • YouUl rutowance.
No 0 Go 10 next quastion Yes ~ 00 not answor questions 95 fa 124,
Go to 125
95 Do you (and/or your partner) own a home bullive elsewhere?
No 0 Go 10 next quesflon Yes C) What ts Ihe reason you live away from the
110me you own? Travelling away from your home 0
Being cared for away from your home 0 Caring for someone away from your 0
home
Living away from home to study rJ Other 0 Give details
~____ . __ ._~ow __
I=-=-~=' .~='~." .. "- .-- ~"-l
STAT.0971.001.0193_R

96 Which of the following bnst describes where you live? Vou are single, under 21 years of age and living in the principal home of a parent D Go 10 125
In a home which Is owned by a privata company or a pr ivate trust that you have an Interest in 0 Go to 125
In a home you (and/or your partner) own or you own Jointly with another person, this can include: • paying it off (mortgage) • a caravan, transportable home or
boat 0 Go 10 97
In a hospital or home for people with disabilities [} Go /0 1 17
In a nursing home or aged care hostel 0 Go 10 101
In a retirement village 0 Go to 707
In accommodation whiCh you (andfor your parlner) have the right to use for tlfe 0 Go 10 110
In public housing (e.g. housing owned by the Housing Authority). This does not include paying rent to a Community Housing organisation. 0 Go to 98
In a place where you (andfor your partne~ pay private rent (this includes site or mooring fees) I~ Go to 115
In a boarding housefhostelfprivate hotel D Go to 117
In accommodation where you pay no rent D Go 10 125
Olher (e.g. lids could be where you (end/or your partner) do not have a [) Give details
F~.address~_. __ •.•••.• _. ___ . _:.e:~-=l I .. ·· .. ·· .... -.,,_ .. _._._.- -····-~·G~-I~-mj
97 Do you (andfor your partner) pay site, ground or mooring fees for the home you own (this could be for a caravan, transportable home or boat)?
No 0 Do not answer questions 98 to 124. Go to 125
YesO Go 10 115
t-UI LI::X 1 ( 'LU( - t-'AGt:: 14t! ot aJ , . <
98 Are you (andfor your partner) the primary tenant? (-
That Is, your (and/or your partner's) name Is on U,e JeIli1i1cy agreement (lease) with Ule publiC housing authority.
No 0 Go 10 next quesllon Yes 0 Do not answer questions 99 10 124.
Go to 125
99 Does the primary tenanl pay rent at the market rale?
No 0 Go 10 next queslion Not sure 0 Go 10 next question
VesD Go 10 116
100 Do you (and/or your partner) live with the primary lenant AND your (and/or your parlner's) Income has been taken Into account by the public housing aulhority when calculating the rent? NoO Do nol answerqueslions 101 to 124.
Go 10125
YesO Go to 116
102 What date did you move Into the aged care hoslel or enter the nursing home?
C i 103 How long wil l you be staying?
Long term or 0 Go 10 next queslion Indefinitely
Respite care 0 When do you expect 10 leave?
[ I I I ~ Do not answer questions 104 to 124.
Go to 125
104 Does this aged care hOstel or nursing home reC€ive an Australian Government subsidy for your accommodation?
Check wj(h your service provider to lind out if they receive any Australian Government subsidy.
No 0 ~ Attach documents to verify the detailS of the entry agreement for daily fens. ~ Go 10 next question
Not sure D Go to next question Yes 0 Go 10 next question
STAT.0971.001.0194_R

l?S Did you pay an· accommodation bond or charge?
.. Your accommodation bond may have been 8 donation, a loan or some type of payment which may be repayable to you in whole or in part, if you teave. An accommodation bond does nollnclude gifts or loans above tlle amount you had to pay for the right to your accommoliation.
No G Go /0 next quesNon Ves[} HoVi much accommoliation bond did you pay?
1-$ -.- ---,
# Attach the accommodntion bond or the accommodation charge agreement.
106 Did you malle a gift and/or loan in addition to the accommodation bond?
NoD Go to 125 Ves How much was ~he gift?
L -: HoVi much was tile loan?
Is "] ~ Go to 125
107 What date did you (and/or your partner) move Into the retirement village?
I I I ~
108 Did you (and/or your partner) pay an entry contribution?
Your entry contribution may have been a donation, a loan or some type of payment which may be repayable to you In whole or In part, if you leave. An entry cuntrtbution does net include gll1s or loans above the amount you had to pay for the right to your accommodation.
NoD Go (0 next question YesD How much enhy contribulion did you pay?
~ I # Attach documents to verify the details of
your entry contribution (e.g. your contract).
109 Old you (andlor your partner) make a gift alld/or loan in addition to the entry contribution?
NoD Go to 116 Yes D How much was the gift?
Is How much was the loan?
Is ~ Gala 116
t-UI LI::i<. 1 FLUI - I-'AGt: 14\1 or ££;j 110 Old you (and/or your partner) pay a sum of money andlor
transfer assets to another person In relurn for Ihis accommodation for life? No D Go 10 next Question ves[) Go to 112
111 TIck which option describes how you (andlor your partner) oblained a life interest in a home without any exchange of money or transfer of assets:
Inherited Ihe life interest D Go to 125 Have a formal agreement documenting D Go 10 125
your right to accommodation for life
Have an informal arrangement WiU1D Go to 115 children to live at their home and
pay rent Informal arrangemenl, no rent paldD Go to 125
DlherD Give dl!tails below
112 Wllat date did you (and/or your pa~ner) make this paymenVtransfer?
I I I J
113 DetailS of the paymenVtransfer How much did you (and/or your partner) pay?
Is I AND/OR What assets were transferred?
1······_-- .. _ ....... -....... ............ __ ...... _ .. _ ... _........ ..... ..-.. j Market value of assets transferred?
Is 114 Details of the person or oroanisation the paymenVtransfer
was made to
Futi name (of IIle person or organisation)
Address E-------:- ~---- I " "M" ••• _R.HH.MM •••• M.'._·~ ... · •. M_ ... _______ M~._.
I'1lstcode
STAT.0971.001.0195_R

115 What type of accommodation do you (and your partner) live In?
Private house or townhouse/unitJtIat Community housing c::
Defence housing Caravan/cabin/mobile home L
Boat
Go to next question
Boarding house/hostel! [} Go to 117 private hotel
other [} Give details below
1_... 1 ~_GO fo next questiOi! _____ _ __ _
r UI LI::X 1 f"LU f - I-'Aljl:: l oU or ;a:1 116 00 you (and your partner) share your accommodation .''';11i
other people? !. Sharing your accommodaUon means tIlat you have the right to use a kitchen, bedroom or bathroom with one or more persons. This Includes ALL family members, people who regula~y stay at your accommodation and people who work away from home (e.g. truck drlwrs, miners, night attendants, fishermen, members of the armed forces).
No [} Go fa next question Yes [}Give details below of people who share your
accommodation
Iii;;~rson's name .. . __ .-
Age
1- '=:JD Sex Your relationship to this person
I Male [j Fem-;Ie[}j C - , When did thoy move In? Their share of the renl/Iodglngs
I , , lis ,
How olten do they pay? I I _ ... -[fJPerson's name Age
I ID Sex Your relationship to this person
~leO F~maleDJ I I When did they move in? Their share olthe rentltodgings
1 ___ , _'=-:JI~ •• _ 1 How often do Ihey pay? 1-- - '
J '--'. - -- . -I§J -.•.•. -. _ .... Person's name Age
C ID Sex Your relaUonship to Ihls person
Gi~ISO Fema'eDJI I When did they move In? Their share of the rentltodgings
I ~E - ] I ,
How often do they pay? L .J ~on';name
. _ .. .. --Age
I -10 Sex Your relationship to this person I---- Q] . Male 0 FemaleD 1 I When did they move in? Their share of the rentltodglngs
I I I lis --.J How often do they pay? I
.. If you share with mare than 4 people, attach a separate sheot with details.
I
STAT.0971.001.0196_R
, 17 (~ you' (and/or"your partner) pay board and/or lodgings?
doard means you (and/or your partner) arc provided wilh some regular meals. Lodgings means no meals are provided to you (andlor your partner).
NoD Go to 119 Yes 0 Go to next Question
118 Can you separate the amounls you (and/or your partner) pay for board and/or kldglngs?
No 0 Tolal board and lodgings cl13lged per day, week, fortnight, 4 weeks or calendar month
/$ per
Yes 0 Amount paid for board (meals) per day, weell, fortnlght,4 weeks or calendar month
c.;.ls _____ pe_r _____ J Amount paid for lodgings (accommodation only) per day, week, fortnight, 4 weeks Of calendar monlh
C per 1 ~ Go t.::..o :.::.12::.0 __________ _
119 HoVi much do you (and/or your pariner) pay per day, week, tortnlght, 4 weeks or calendar month (e.g. rent, maintenance or s~e lees)?
Tills would be the total you (andlor your partner) pay for the property minus any subsidy/rebate or contrtbulion from another person ororganlsnlion.
• 20 When did you (and/or your partner) start paying this amount?
/
121 Do you (and your parlner) live In a boarding house, hostel, private hotel, hospital or disability housing? No 0 Go trJ next question YesD Go to 123
122 What is the total amount of rent charged for the property per day, week, fortnight, 4 weeks or calendar month?
1$ per I
t-UllioX lI:lUI - (-'AGe 101 ot :.!:.!:J 123 Details of your landtord, authorised agent or person you
(and/or your partner) pay rent to FUll name
L _ ______ ----I Address
I.-.... -.--..... - ..... --.--.-........ -.~ ..... ---.-. ··-·---·--_····-·--·1 t-- .. -----·------·-·--··Po;;;~-·--==J Contact phone I1Umber
G- :J 124 Do you (and/or your partner) have a current lease or
tenancy agreement wilh written evidence of Ihe CURRENT amounl of rent, fees, lodgings or board and lodgings you (and/or your partnc~ pay?
No 0 Go to next quesllon
Yes 0 # Al\ach a full copy of your signed lease Of tenancy agreement.
Other details
125 Ate you (and/or your partner) receiving a Disabil~ Pension at Ihe Special Rate (Totally and Permanently Incapacitated) from t1 1~opartment of Veterans' Affairs?
No @ Go to 128
Yes 0 Go to next question
126 00 you have the Special Rate decision letter from the Deparlment of Veterans' Affairs?
No 0 Go to next question
YesO # "ttacll the Special Rate decision latter. ~ Go to 128
127 Do you au:horlse Centre link to obtain Information, from tho Department of Veterans' Affairs, required for this claim?
No 0 You will need to complete a Medical Report Disability Support Pansion fonm lSA012) included In this pack ~ Go to next quesllon
Yes 0 Go /0 next question
STAT.0971.001.0197_R

128 Are you claiming Disability Support Pension because you are permanently blind?
No ~ Do 110/ answer questions 129 to 135. Go to 137
Yes IJ Go 10 next question
129 Are you sludying?
No 0 Go 10 next question
Yes [} If you are currently studying you may be eligible for Pensioner Education Supplement. For more Information about Pensioner fIiucation Supplement see 1119 Informalion Booklet.
130 fire you (an~/or your partner) claiming rent assistance?
No 0 Go 10 next question YCSl,) # You will need to complete and anach an
Income and Asse/slorm (511369) included In this pack. If you do not have lhls 10rm, call us on 13 2717 or go 10 our website al www.cenlrellnk.gov.au
~ Do not answer questions 131 to 153. Go to 164
131 lire you (and/or your partner) receiving a New Zealand Government payment?
I~o D Go 10 next quesl/on
Yes C} # Anoch a latter or other document .Alich gives the reference number and details of the payment.
132 lire you (and/or your partner) receiving any other payment from the Department of Veterans' Melrs?
NO C::~ Go to 134
Yes l) Go 10 lIext queslion
133 Which other payment do you (and/or your partner) receive from the Department of Veterans' Affairs?
Tick aI/ tllnt apply
Disability Pension rIIar Pension) 0 Income Support Supplement 0
Service Pension 0 War Widow's Pension 0
War Widower's Pension 0 DlharD
Not sure 0 # Anach a lener or other document which gives the
reference number and details 01 each payment.
t-Ut Lt::/\ 1/'LU( - f-'AGI= lo'L 01 'L'L:';
134 lire you (end/or your partner) receiving payments un~",the New Enterprise Incentive Scheme (NElS) or Comml J Development Employment Projecls (CDEP)?
No 0 Go 10 next question
Yes 0 ./) Attech a letter or document which gives (Y the reference number and details of each
payment.
135 Please read this before answering the foll~wing questions about compensallon, Insurance and/or damages.
tnctude: • werkers' compensation/damages as a result of a
work injury • third party damages as a result of a motor vehicle
accident • personal accident and sickness Insurance or income
replacement Insurance • sporting Injury compensation • public liability compensation • medical negligence compensation • damages paid to victims of crtme or as a result of
criminal injuries.
Have you (or your partner) ever CLAIMED or are you (or your partner) ABLE TO CLAIM compensation, insurance and/or damages?
No [) Go fa next question
Yes r'-~ # You will need to complete and attach a Compensation snd damages form (Mod C). If you do not have this form, eall us on 13 2717 or go to our website www.centrellnk.gov.au
136 Are you (and/or your partner) RECEIVING or have you (and/or your partner) EVER BEEN PAlO compensation, insurance and/or damages?
NoO Go to 154
Yes C~ # You will need to complete and aUach a Compens8t/on 8nd damages form (Mod G). If you do not have this form, call us on 13 2717 or go to our website www.cenlrelink.gov.au . ~ Go 10 154
STAT.0971.001.0198_R
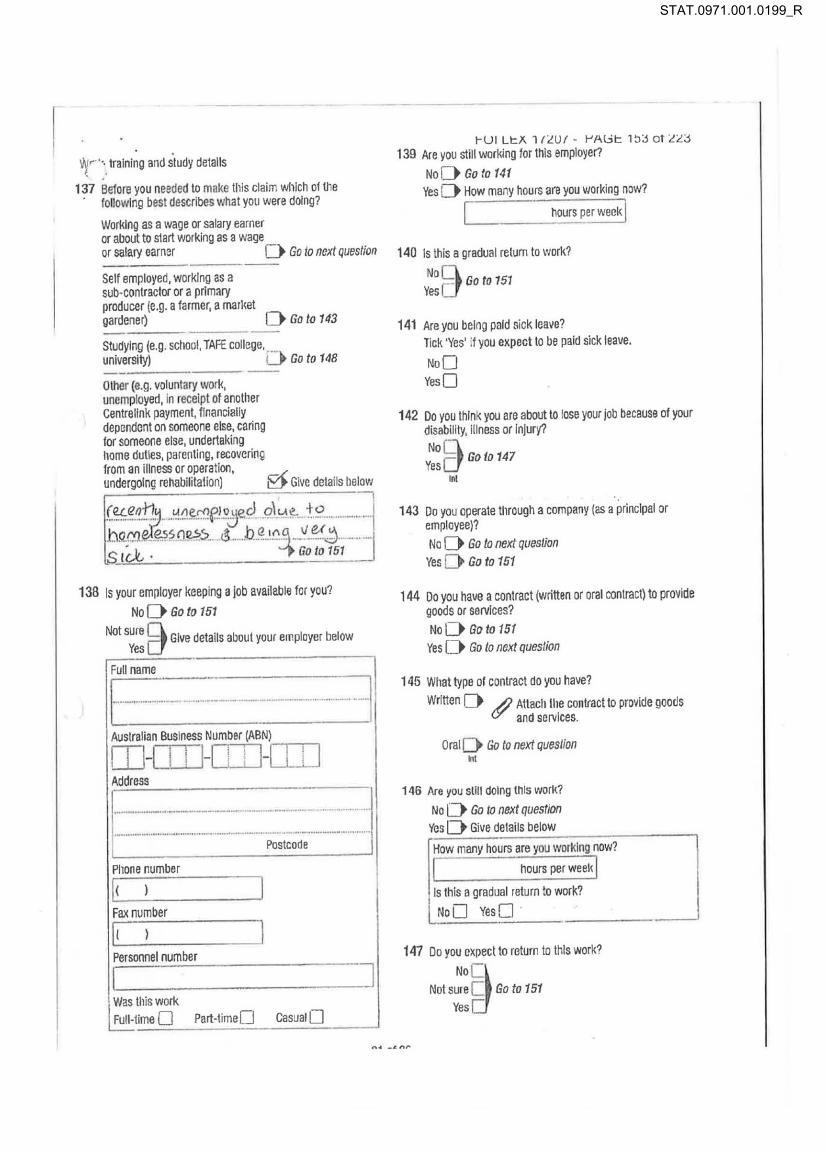
Voir ", training and sludy details ( :
137 Belore you needed to make this claim Wlllch olll1e , lollowlng best describes what you were doing?
Working as a wage or salary earner or alJout to start working as a wage or salary carner 0 Go to next question
Self employed, working as a sub-conlractor or a primary producer (e,g, a farmer, a market gardener) 0 Go to 143
Studying (e,g, school, TAFE college, ,_ univerSity) IJ Go to 148
Other (e,g. voluntary work, unemployed, in receipt of another Centre link payment, financially dependent on someone else, caring for someone else, undertaking home duties, parenting, recovering Irom an illness or operation, undergoing rehabilitation) ~ Give details Ilelow
(~,q.qi1~_ .. ~~~~p.2Jjecl g'-lol ~_ 4:.9 ....... _ .. . .. ~~f"t~~~ ()~~-... ~_._b._~~:\ 1!fo~i- -_.-
138 Is your employer keeping a job availeble for you?
NoD GOlD 151
Not sure Q Give details about your employer below Yes a
Full name
1-.. -.... ,---·:- _ .... __ ..... ---.. ,-- ...... _ ......... _ .. , .. ··1 Australian Business Number (ABN)
DJ-lJJJ-OJl-UJ] Address 1---------1 ~-.-•• -~ • • • • • • • -.-•• --• • ' • • " ... _ ......... ~._ ........ _ .. _. · •• · ~ •• • ••• M •• N __ •••• ••
Postcode
Phone number
II ) I Fax number
II ) I Personnei number
I l Was this Vlork Full-time D Part-timeD Casual 0 L-.
t-UI U:I\ 1 a Uf - I-'A!jt: 1~:.l 01 L L :.l 139 Are you still working for this employer?
NoD Go to 141 Yes 0 How many hours are you working now?
I hours per weell I 140 Is this a gradual return to work?
NoQ Go to 751 Yes a
141 Are you being paid sick leave? lick 'Yes' if you expect to be paid sick leave,
NoD Yes 0
142 Do you think you are about to lose your Job because of your disabilily, illness or Injury?
NoQ Yes a Go to 147
tnt
143 00 you operate tI1rough a company (as a principal or employee)?
No 0 Go 10 next question Yes [} Go to 151
144 00 you have a contract (wntten or oral oonlract) to provide goods or services?
NoD Go to 151 Yes 0 Go 10 next question
145 What type of conlract dO you have?
Written 0 ./) Attach Ihe contract to provide goods (II' and services.
Oral D Go to next quesllon . t
146 Are you sUIl doing (his work?
No 0 Go 10 next question Ves 0 Give details below
How many hours are you lVorklng now?
I hours per weel, I Is (his a gradual return to work?
NoD YesD ' ~--------------~
147 00 you expect to return to this work?
NO~ Not sure c:: Go to 151
Yes c::
STAT.0971.001.0199_R

148 Have you completed your studies?
NoD Go to next question Yes 0 Wi,en did you fin ish?
LI __ ' _ ___ ~ Go to 757
149 Are you currenlly studying?
t,)o 0 Go to next question Ves 0 Give details below
If you are currenlly studying, you may be.ollgible for Pensioner Education Supplement. For more Information about Pensioner Education Supplement, see the Information Booklet.
Name of school, TAFE college, universily, olher
, .......... _ ........................................ _ ................................. j
Address
~---- ....... -- -------- -j r ...... ···--.. · .... -... -- ... -... -...... -.......... -..... -.... -....... Poslcode
PhOne number
[( ) I How many hours are you studying now?
I .. - --;;;"per week ~ Go to 151 - - ---
150 DO you expect to return 10 your studies?
No D Go to next question
Not sure Q Give details below vesa
..J
Name of school, TAFE college, university, olher
t·· .... ·· ........... -.-.-............. --.. -... ... -..... ---.-... ] Address
~ ----------. --I -···-· .. ···· .. ··-.... ·•• .... ••• .. ····-·-··Posi;.;d~·-··-· ......... ...
Phone number
I ( ) I
151 ~UI U:i<. l/LUI· t-'AGt: lb4 or LLj'
In Ihe last 14 days have you (andfor ~our parlner) recrhled' or claimed any of the following paymenls (nollncludl Family Tax Benefit)?
• ABSTUOY • Parenting Payment • Ausludy • Sickness Allowance • Carer Payment • Special Benefit • Disability Support Pension • Widow Anowance/Pension • Newslart Allowance • Wife Pension • Partner Allowance • Youth Allowance.
No 0 /) You (and your partner) will need 10 complete (Y and attach an Income and Assets form
(SA369) included In this pack. If you. do not have thfs form, call us on 13 2717 or go to our website at www.centrelfnk.gov.3U
Ves &j Go to next question
STAT.0971.001.0200_R

15;>.· In the last 12 months, have you (or your partner), or do you ( IX your partner) expect to receive, any leave entitlement
payments from an employer you have worked for?
tnctude: • annualleava • maternity leave • long service leave • sick leave • leave loading.
No ~ Go to next question Yes 0 Give details below
# Attach documents which confirm leave entitlement payments (e.g. letter from employer).
P"Type of le~~~ ;~tii~-m-en-t--- --. -I ~.--------
Amount you recelvod or J
r:ra~~t~t~ee~e~~~~~I:s ~I $===:===.::~= Number of working days I - -, ,: covared by the payment -.J
-I Date paid or date payable I I I , ;
L-. __ .--1: Name of employer I r= ___ -~~~~~_..JI
~::: ~=---·· ~,~=--:Ii Phone nUJn:::b:::er~ ___ --.
C-) ... __ ._ ] Job doscription
I --_._-----
I-UI Lc}\ l lZUI - I-'Al:ic 1!:>!:l 01 Z<:J Ccnunued
i -TYPO of leave enfitlement -
I Amount you received or expect to receive before tax and other deductions 1$ I Number of working days I ] covered by the payment
Date paid or date payable 1_: I I Name of emeloyer -
II [ - _.-Address
f ::::-.:::::::=--:=.:::.::::=-:::::: Postcode
Phone number
II 1 I
JOb description , .. 1... •• ..,
If you have payments from more Ulan 2 employers, attach a separate sheet with detalle.
153 Have you received a redundancy payment since 20 September 2006?
No D Go to next question
j
YesG # AIlach documents which confirm any redundancy payments (e.g. Employment Separation Cor/lliea/cform (SUOOt). letter from employer). It you do not have this form, call us on 13 2717 or go to our website at www.centrelink.gov.au
STAT.0971.001.0201_R

Independent rate
154 Are you under 21 years of age?
NO~ Donotanswerquest/ons 15510 171. Go to 172
Yes 0 Go to next question
155 Please read this before answering the following Questions.
If you want to test your eligibility for Youtlt Allowance while awaiting the outcome of your claim for Disability Support Penslnn, your parents will need to complete a P8rent(s)/Guardian(s) details form (Mod JY) if you are considered dependent on them. If you do not have litis form, call us 01113 2717 or 00 to our website at www.centrelink.gov.au Note: Disability Support Pension Is not subject to tlte parental income test, however, Youth Allowance is subject to the parental Income test if you are considered dependent on your parents.
156 What date did you leave secondary school?
I J J I 157 Since leaving secondary school, have you worked and
eamed 75% or more of the National Training Award in an 18 month period?
For more inlormalion about the National Training Award, refer to the Information Booklet.
No D Go 10 next question
vesD # Attach proof of emjJIoyment (e.g. payslips, letter from tha employer or group certificates). ~ Do nat answer questions 158 to 171.
Go to 172
158 Since leaving secondary schooillave you worked in part-time paid employment for at least 15 hours a weel, for 2 years?
No 0 Go to next question
Ves C» # Anach prool of employment (e.g. paysllps, letter from the employer). ~ Do no/ answerquesllons 159 to 171.
Go 10 172
159 Have you worked for at least 30 hours a week for 18 months in a 2 year period?
No D Go to next question
Ves D # Ahach proof of employment (e.g. paysllps, letter 110m tile employer). ~ Do not answer questions 16010171.
Go to 172
I-Ut Lt:X 1 (LUI - t-'Al;;t: loti or a:J
160 Are you, or have you been, married or in a reglstere~r. relallonship? I,. No D Go 10 next questlan
Yes D # AUacll proof 01 marriage or relationship registration. ~ Do nal answer questions 161 to 171.
Go 10 172
161 Do you have or have you had a dependent child (natural or legally adopted)'!
No D Go 10 next queslion
Ves D # Attad\ prool of bllth for Ihls clllld, It you have not already done so. ~ Do nol answer queslions 16210 171.
Go 10 172
162 Have you lived, or arc you living, as a member of a couple In a relationship that has lasted: • for atleast 12 months, or , for at least 6 months where the relationship ended due
to exceptional circumstances (such as domesUc violence or dealh of a partner)?
No D Go 10 next queslion Ves D Do not answer questions 163 to 171.
Go to 172
163 Do you live wllh your parentIs)?
No [) Go to nexl question Yes C~ Do nol allswerquestions 164 to 171.
Go 10 172
164 Are you 1 a or 17 years ot age?
No D Do not answer questIons 165 to 171. Go 10 172
Ves D Go 10 next quesllon
165 Do you live away trom your parents' Itome because of a dlsabltily, Illness or Injury? No [) Go 10 next quesllon
Ves D Give details below
1------------------- 1 ..... _.,._ ..... _ ... _ ...... _ ............ __ . __ .. _. __ ._._ .. __ ... __ ._ ..... _._-
~ Do not answer quesllans 16610 171. Go to 172
STAT.0971.001.0202_R

166 .,~ you an orphan?
( . ,0 0 Go to next question
. Yes 0 You may need to provide evldencc.
~ Go to 172
167 Are you a refugee without parents In Austratia?
No 0 Go to next question Yes 0 Go fa 172
168 Are your parent(s) unable to exercise their parental responsibilities?
For more Information, refer to the Information Booktet.
No D Go fa nexf questiOll Yes 0 Go to 172
169 Is It unreasonable for you to live at home?
For more infc rmatlon. refer to the Information Booklet.
No 0 Go fa next question
Yes 0 # You will need to c9mplete and attach an Unreasonablo to Live af Home form (Mod Y). If you do not have this form, cali us on 132717 or go to our webs~e at www.centrelink.gov.au
~ Go fa 172
170 Are you, or have you bllen, in state or territory care?
NoO Go 10 172 Yes 0 Go to nexf queslion
'71 Do you, or does anyone else on your behalf, get a p~yment from a state and/or territory government? This Includes any organlsetion that gets a payment for you.
No D Go to nexf question Yes D Give details of the department or organlsatiOIl betow
Ful l name
Address
~UI LeX 1/<'U/- r'A G e: lbl or<'~:J
Another person or organisation to act
172 Do you IVant another person or organisation to enquire or act on 'Pur behalf when dealing with us?
No B Go fa next quesllon YesD /) You will noed to comptete and attaoh an
(j' /luillorlsing a person or organlsallon to enqulro or act on your bellalffonn (SS313).1I you do not have IIlls form, call us on13 2717 or go to our website at www.centrellnk.gov.au
Other payments
173 Do your disabilities, illnesses or Injuries mal(e it difficult for you to ~ public transport?
No ~ Go 10 noxt ques/Ion
Yes 0 You may be eligible for Mo~lIity Allowance which Is paid to people with a disability who are ooable to use public transport, wllhout substantial assistance, permanenUy or for an extended period of limo (1 year or more). You must be undertalting work, vocallonal training or vo luntary work or participating In job search activities. For more information, call us on 13 2717.
174 Do your disabilities, illnesses or Injuries make It dlNlcult for you to ~e for yourself?
No 13 Go fo next Queslion
Yes D If you have someone caring for you. they may be elioibie lor carer Payment BOil/or Carer Allowance. For more Information, call us on 132717.
STAT.0971.001.0203_R

Checklist
176 Which of the following forms, documenls and o\ller attachments are you (and/or your partner) providing with this form? If you are not sure, check tire question to see if you shOuld attaclrthe documents.
Where you are asked to supply documents, please attach original documents.
Proot 01 Identity 0
Proof of resldcnce status 0 (if you answered No at quesl/ons 47and 66)
Dependent children proof of birth [.1 (if required for question 78)
Reports you have thai are relevant to your c'alm C (if required for quesl/on 83)
Reports from school 0 (if you answered Yes at question 85)
Documents to verify the details of the entry 0 agreement for dally fees
(if you ansViered No at quesl/on 104)
Documents to verify detalts of an accommodation 0 bond or accommodatton charge agreement
(if you answered Yes at questIon 105)
Documents to verify details of an enlry cootribullon 0 (If you answered Ills at quasI/on 108)
Signed lease or tenancy agreement 0 (If you Rnswered Yes 8t question 124)
Special Rate deciSion letter from the Department of [l Veterans' Affairs -
(if you answered Yes af question 126)
Income and Assets form (SA369) [] (il you answered Yes at question 130 or
if you answered No 8t question 151)
Document which provides delalls of payment rocoived 0 (If you answered Ills at questioll 13/)
A letter or documsnt which gives details of retorenca 0 number and details of the payment received
(if required for question 133)
A letter or docu111t!nt which gives details of reterence CI number and details of the \lilyment received
(/fyou answered Yes af question 134)
Compensation and damoges form (Mod C) lJ (if you answered Yes at question 135 or 136)
The contract to provide goods and services 1--1 (if required for questioll 145) -
Documents which confirm your leave entltle111t!nts [) (/I you answered Yes at question 162)
Documents which confirm any redundancy 0 payment received OR Emptoyment Separal/on
Certillcate form (SUDOl ) (il you answered Yes at questIon 153)
Proof of employment [) (If you answered Yes at quest/on 157, 158 or 159)
t-UI U:X 11<.U 1 - t-'Al3t: 1::>!S 0 1. <.<.;S Continued . •
Proof of marriage or relationship reglstr£~ c: (if you answered Yes 8/ question 160) .
Statemenl
Dependent children proof of birth c: (If you answered Yos at question 161)
Unreasonable /0 Live a/ Home form (Mod y) [ . (il you answared l~s at question 169)
Aufllorislng a person or organlsalion L. fo enquire or act on your belralfform (5S313)
(if you answered Yes at question 172)
176 Statement I declara that: • the tnformatlon provided in this form is complete and
correct. • I have received the Information Booktet whiCh includes
the privacy notice.
I understand thaI: • giving false or misleading information is a serioos
offence. • CentrelinK can make relevant enquiries to ensure I
receive the correct entlttement. • t must notifY Centrellnk of any changes to tilis
information within 14 days of the change(s) occurring.
Your partner's signature
I~fb, _ ._ Dnte
CZ._I __ "" )
STAT.0971.001.0204_R

Customer's ~de~ta~i",IS _________ ~---'-____ l-______ -'
Oale 01 birth :
Phone number "I ( _--'
This report must be completed by the ctis,tofliler's IrO:iTIiiii . " Instructions for the customer Instructions for the doctor
. 0 Comptete your details above.
@ Make an appointment with the doctor or spectan,t. Whon you make your appointment, please let the recaptionlst know that you will need this report completed. The Ume taken to complele the medical report may be clal .. ed by your doclor under a Medicare Item when Included as part 01 a consultallOn.11 yoor doclor ooes nol bulk bill, your consulfallon lee may be more than usual because of Ihe extra time laken 10 complele !he report.
E) Read and sIgn Ihis Authority \0 release Informallon. I authorise Centrelink to oblain any ralavanl medlcel lnfonmalion necessary to decide my Quelificatlon for penSion, allowance, eijglbllily for emplol'1lenl ass~tance or access 10 Iha Supported Wage System from my doctor(s), or other regislered medlc.1 praclliioner(s) whom I have consulted, Dr to lllhOm I may be referred by Canlrellnl< upon the recommendallon 01 a Job Capacity Assessor. and I give permissIon for any relevant medical detalls and clinical noles about rna to be supplied 10 a Job Capacity Assessor; and
• t give permission for my doclor(s) 10 exchange relevanl inlormallon with Cenlrelink, andior n Job capacity Assessor "-1lf'1 my medlcol condlllon(s) and any olher relevanl barriers Impacting on my ability 10 partlclpale In assistance programs in order fo< Cantrellnk to decide coneet paymenls and sullable services and programs lor myself and whete relevanl th'rd parties; and III am required to have 8 further assessmenl In addition 10 Ihe assessment by the Job Capacity ASsessor,laulhOrlse Cen~,;k1k or the Job Capacity Assessor 10 release this medical report and other relevanl documenls 10 Ihc assessing practitioner or agency.
Cuslomer's signature r -- --,_. ~rA 1 __ . Dale L-__________________ ~
Lt e -(~ .. ~! I'?_·.:~J o Give this repon to Ihe Ooclor to complele.
'j I I
This 'rap~r1 fTlay 60 used to: . • . decld.rVlhlcl] paym~nl \'O!!r patlanl may ba r:nedleally eligible
. for . • d~clde If your patienl could bene III jr6m ,vocational
rehabllifaijilft or traIning • Oeclde If your pallenl Is abla to enler the Supported Wage
System.
Paymenl for your report
We have asked your pallenl to let you know at the lime 01 rnakk10 their appointment thai IMy raqulre you 10 complele thIS report. This Is to ensure thai you have ,uHlclenl lime lor th. e,,!,mlna.llon·
. The time taken 10 compiele the medical report may De claimed under a Medlcara Item whan Included as part of a conslJllalion.
Compl.ting Ulls report
In Utls report you Vim be asked to provide delalls 01 your patient's I)!edlcat condilion(s). Pleas. complele aJllhe r.qulred questions in I~I' r~port. If you have any Questions aboul this report. call . Ca~tr.llnkon 13 2nI.
Returnin~ this report 10 us
You. can give Ihls report and any attachments 10 your patient or you can return Ihls reportdlrecUy 10 Centre link.
For Information about confidentlailly and dlsclosur. of inlonn~tlon
See Questions 11 and 14.
Thank you for yOur asftl~lanc. . / . .
~:
,/:/ \" ,
/or t':. \ . ro"
Id~~/~ '> .. ~~ .. ,. /0." .~.' ,- .. ~, 'I: -I '
A ' .. :-' ..... , ." .'~~ 'f;,'" /' i
,r' ,,'
if/" #'
STAT.0971.001.0205_R

1
rUI LI=X 1 (£U I - I-'AGI= ltiU 01 ££J
, . , ;-' " " '.l " ., i'
t . ~ "
No . Does the po~IOf1 ve a 1erminaJ conditioo with a prognOsis 01 less than 24 months?
Gc 10 next QUeSlion Uncertain
Yes 0 Diagnosis
I )
~ Go to 10
J
2 000. Ihe patlenl have on~ or more modical conditions thai have a slgnilicanlimpaci on lhelr :lblilly 10 lunction? (e.g. ablilly 10 sil!6I2n<Vmo·,., endurance, communlcalion, cognitive funclion, abilily for self care, need 101 support in .cINnies of dany lving)
No 0 ~ not nced to complete quesYon 3. Go to 4
Yes ~; ~extques#on
3 Give details abrut the Coodiilons Ulal have a significant Impact on the.poUoni's ablillyto flin~tIo~. list conditions in order of degree of Impacl on abiijly 10 fun~lon, sla~ing wnh condition wll~ ITlQst lnip.act :
Condition 1-condillon willi most Impact
DI.gnosis
A Diagnosis
I .. -.--.. ~:-~.- ::S:~.:t<:-_~~ .. Tho diagnosis Is .. :/"
Conflnned g-' Presumptive ONo fUlth~sllgalionsllesls planned 10 confirm tho diagnosis?
No ff VesO
Date of Onset ~f known) I L _______ -'
Clinic~1 fealures
B History
Dale 01 diagnosis Of confirmed) I L __ ( ___ , __ --'
---J
Provlds delails including etiology, plec;pltatlng faclors, underlying causes, reoults snd dales of Investigations/procedures end speclalisl w.'SUltatloos (e.g. radiology, pathology, AFTs, spec.alisl reports).
f~ --::-' ... ,~ . . $~ . .. .a-~~.~_ ... ~ .. . . ~.~. lO~ .\?_"'~ .~.~ ...... ~.~.o . ... ~--'::::-. "'-~~ ... ..' .
0.- "Irrrl""c. I»~~ .~ .... -.. -............ - .
C Gurrentsymploms Provide details 01 the cunllnl clinical leawr •• and symploms, Indudlng frequency and severily, expertsnced by the patient duc 10 Ulls condiU"". Be specific in Indicallng tho severtty 01 lhe medical Impalnnenl
, ..... , :.:.. .~_-.::. :C2:- ':J '_H~~~'~' .-~. , I
1.,-0 '-:::--:-~.""' .~ ____ ~"""'~~..lJ'1 " "-'--!.""'~~-...,J< "&r.. ..... -. ')' .;;-. ~ )~#.".~._~
h:::,,4'-:::'.'~~~ (?~ k?-\V--~ .. ~ ~~,,,, :t?";-L~·~ ''''''~ \-c
~c<Dlo ~ e.g T..,.
STAT.0971.001.0206_R

' f'UI LI::J<. 1 f"U f - I-'AGI:: 101 at "":J Condition 1-contlnued Treatment
o Currenllrea1menl Provide delalls of all currenllrealmenl for this condlUon (e.g. surgery. medicallon. counselling. physicallherapy, reh2bllllallon). Indude spectfic delails such as datss of commencement of treatmenl, frequency. durntlon,iypeS; elc.
I E Pasllreatmenl
Provide detaR. 01811 slgnlflcanl past treatment. dureUon end responsllS. tndude specific delails such as dales of commencement ollreatmenl, frequency. duraflon, types. elc .
. .>-<:t~!'a ~ ~ u ~ ~ ... " ........... _ .. _. -' ' .. _ .... ~
F Futurnlplanned lreatmenl
"-'--1
Provide delails of any fuMer scheduled or proposed treatmenl with .. Umales of likely dales 01 commencemenl and expecled duration.
\. ~ ........... ~"'-- 0iI!.~ _ --_. ·---1 • • ~ •••• MH' •• __ • ••• _ . _, _ _ .M. ••
G Patien t's compliance with recommendod I~ent
Very compllanl 0 Usually compllant !B' Rarefy complient 0 Uncertain 0 OetBli any Issues relaled to assessIng or under1aking sullable treatment thai affect the level of compliance.
=--.-••••.•.•. -..... ~ ..... ... ....... -......,..I'I., ~~''- I - .;) " ... n_. " _ ....... _. ___ •
tmpact 011 obrlity to funct ion
H Details about how this condiijon currently affecls the patienl's ability to function
Be specific and consijer tho effecls due to the condition elone. Consider: • ablity to slVstand/muve • abmty for sell care • endlK8nce • need for support in activities of dally living • communication • need for hlQh levels 01 car. (e.g. nursing home level of care) • cognitive function • any adverse effect9 of treatment.
.~ ..... ~f c--;,~ .. _ .. ,~ .. " .0.<!. ~ ... ~·:~~:~-:- .. ... ~ ... ~~ .) .... _ ~_ c.),. ~ ~ ~- ~.~ ~--e.~'
TIl. current Impact of Ihls condition on Ihe patient's abifity to function Is ~cted 10 persist for:
Loss than 3 monlhs 0 3-24 months 0 More Ihan 24 months'2f
J Within the next 2 years Ule effect 01 this condition on the pallenl's ability to tunc"on Is expected to:
SlgnlfrcanUy improve g / SomB~lhallrnprnve 0 Fluctuate 0 . Remain unchanged Er Oele<iorele 0 Uncertain 0 Not applicable 0
Provide details, " relevant
<;"--, ... :"'::--
(..c...~~
1-.-...... - ...... . j ~=============================.~ For e second condition thai has a signnicsnt Impact on ability to function, go to the nCKI page. ! H Ihar. are no other conditions that have a "gntncant impact on abifJty to function, go to 4 • . _------. ,-- .. _---. --------_ ... _----- .. -.-..... _- .. '. - .- ."
STAT.0971.001.0207_R

I-UI U:iI. 1 I"LUI - I-'AGt: ltiZ ot "LZ~
. . ... , "" .'. , . . . ~ :COllililion 2 ' " . . " • , •••• ". . ' J
, _ Diagnosis
A Diagnosis
, .... _. __ .-
The diagnosis Is ...
ConftrmadD Presumptive OAr. lurther investigatlonS/lests planned 10 confirm lhe diagnosis?
NDD VasD
I Dale of onset 01 known) I '-__ I ___ ' __ -.J Date 01 diagnosis (If confirmed) I
'-------' Clinical features
B HlstOlY Provide details Incl.Jdlng etiolOgy, preclpitatlng lactors. underlying causes, resuhs and dates ollnvesllgationsJprncadures and specialist consullatlOns (e.g. rad""ogy, pathology, AFTs, specialist reportsl .
C Curnlnt symptoms Provide delalls 01 the current clinical faalures and symptoms, Including treQuency and severlly, experienced by the patlent due 10 tills condilion. Se specnlc In indlcaUng the .averily of Ihe medical Impairment
1-· .. ·• .. _ ......... ---
Trealment
D Currenttreatmll/1t Provide details of all current treatmentfOllhls condnion (e.g. surgery, medlcellon, counselling, physical therapy, "hablUration). Include specnlc details such as dates of commancement of mlmant,freQuency, duratIOn. types, etc.
E Postlreatment Provide details of all slgn,"cant past traalmen~ duration and responses. Include speciNc details such as dates of commoocement 01 treatment, freQuency. duration. types, ate.
· 1 F Future'planned treatment
Pro~de details ot any furth.r scl1eduJed Of proposed treatment with estimates of likely dates 01 commencement and expected duration.
'-l --- _._------- I
STAT.0971.001.0208_R
. ~ Condition 2-continued Treatment-continuod
'I-UI U::X 1 I'LUI - r'At,;1:; 1o~ 01 :a~
G PaVent's compliance with recommended treatment Vel'f oompHanl 0 Usually compliantO Rarely compliant 0 Uncertain 0 Oelall any Issues relaled 10 assessing or UO<Iertaklng suitable lrealmem lIlal affocl 11\. level of compliance.
\......_._-_.. ._. -_ . Impact 011 ability to functIOn
H Details about how Ihls condlUon currenUy affacls the patient's ability to lunction
Be specific and consider the effects due to the condition .Ione.
Conailler: • ability to siVstandimove • abliKy for Sllil care
• endurance • need lor support In activttles 01 dal~ living
• communication • need for hfgh levels 01 care (e.g. nursing homa level of care) • cogn~lveluncUon • any adverse effecls 01 Ireetment.
I· .. · .. · .. ·· '. ...... _-' .. -._ ......... __ ....... -I The current Impact of this condition on the patient's ability 10 function Is expected to pOTslst lor:
Less than 3 months 0 3-24 months 0 More 1han 24 months 0 J Within Itte next 2 years the effect 01 this condition on the paUenfs ebllity to funcllon is expected to:
Slgnnrcan~y Improve 0 Somewhat Impl1l'le 0 Fluctuate 0 Remain unChanged 0 Detenorate 0 Uncertain 0 Not applicable 0
Provide details, If relevant
/ ... ... -..."
1 If there arB more U,an 2 coodlUons !hat have a slgnHlcant Impact on ability to lunctlon, attach. separate sheet wHh details.
STAT.0971.001.0209_R
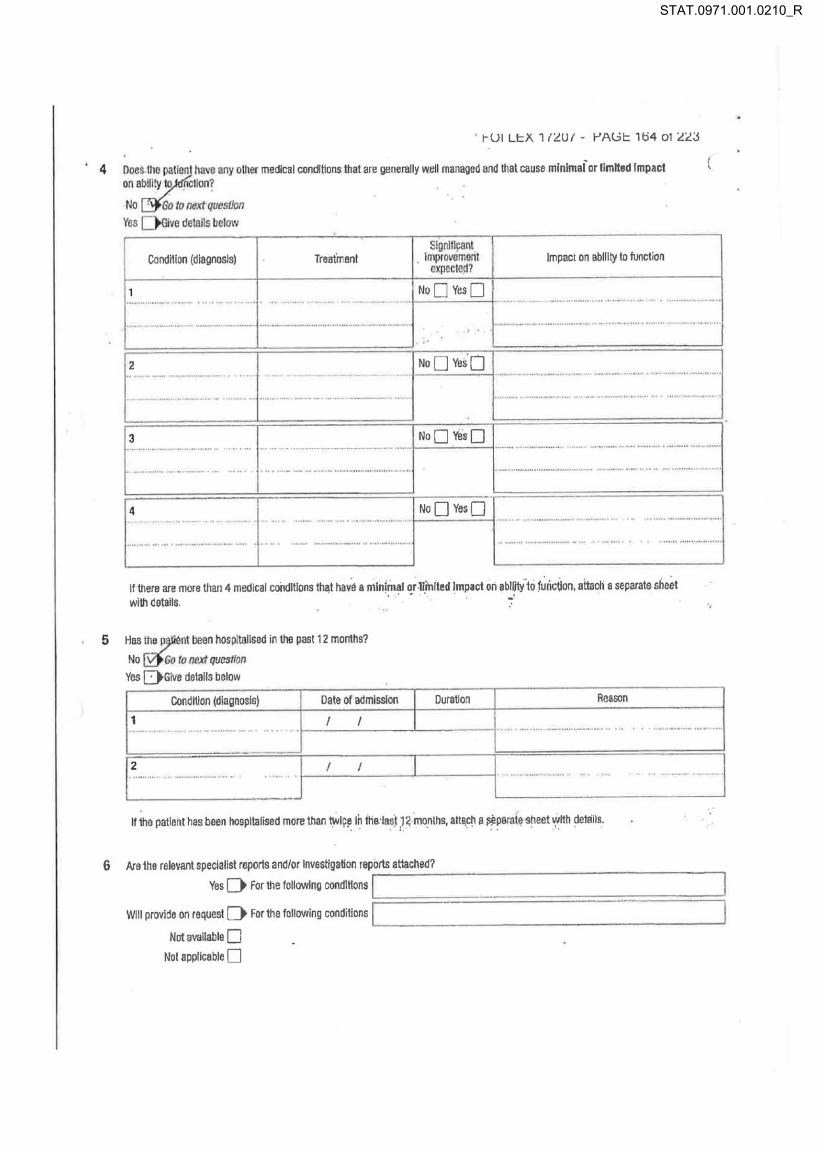
t-UI LI=X 1 I'LUI - t-'AGI= 104 o t 'L'L:J
. 4 Does.lhe pallent hava any OUlt!< mec!jcal cond~ons thai are generally w~1I managed and thai cause mlnlmai or fimHad Impact on ability 10 • lion?
5
No Go 10 Il8Xt qvestJon
Yes ve details below
Cond~lon (diagnosis) lrealmanl
I'
Slgnlflpanl . Improvomenl
.'pccle<l?
No D Yes 0
Impact on ability to function
1
4 • • .. " I ...... -... -. ... _........ 1 No 0
Yes 0 1- .... .. ............ -. . .. _. .. ---........ -·1
.... ' =-_-_ .. __ ' _ ... _-_ ... _._-._.'-.. __ -_-_-_._.~_._-._ .... _-._ .. -J....... ..-.. -.. - -... .. ............. .. .
If there are mora than 4 medical coildJllons I~t havs. mln!~~1 ~r .1lJn(ted !mpact on .bl~·to r~ri~on, attach. separate sheet with datalls. . 7
Hes tha ~nt been hospitallsad In \ha past t2 months?
No @Go 10 I1IlXI quesllon
Yes DGive details belolY
Condition (diagnosis) Date or admission
1 I I .
r· .. I I
Durallon Reason
... . - ...... -_ .. ..
If the palleht has been hospitalised more than twice In IHe:l.st J< months. an~ch a i'l!p8l'3i~ ~heet wHh demit •. . " . . • :. ' . . . . . 1 . .
._ .n·._ ... .
"
6 Arathe relevant specialist repons andlor Investigation reports attached? Yes [) for the following condlHons Ir---------------------'
Will provide on request [) for the following conditions 1'--_____________________ --' Not available 0
Not applicable 0
STAT.0971.001.0210_R
~,' t-UI LI::X 1IZUI . I~A~I:: 100 ell <'<';I
. l ClIMr Information Ihat you would like to provide. . This may Include, but Is nol res~icled 10, commsnls In relation 10 1he patienl's i~, circumstances such as socl.:.conomlc, soclo'rotunil, educational and employmenl facto .. , general abiily 10 cope/manage, elc. . . '
__ . ~_,,_.,, ___ ._. __ . - .. " .. _______ ". ___ .-"" .. ,,.,,--._._-".----0""--" .. _ .
8 Does Ih8 patienl have a t1!mporary Oe" lhan 24 months) reduction In abiily 10 funcUon becau~ of the~. me~iti\.t ~ndlljO[l(S)?
NOD GVV'O '. Yes ~ td next question . . . . .
9 00 you wish 10 pr vide medical certillcale1lelalls on this report?
No D nliXt quesUofl Yes
I examined IIlls person 00 1,,;2Je;,-.::.../_";; _ _ 1).-c. _ _ ,_C>_-,
In my opinion this person is lemporarily unfitlorvlOrWsludy from !2;; I..,. 1;>=.",- 110 120- I €: I ~,::. I
In my opinion this person can 0 cannot 0 currooUy do their usual worWsludy, or lny other work for 6 hours or male per Vleek.
10 This person has been: my patient since I i -:=n L. I~ o(?,
a pallenl al this practice since 1'-_______ -' 11 Release 01 medlcallnfonnation
The Freedom ollnfOfT1l8UonAct 1982 allows for the disclosure of med!cal or psychiatric InformaUon drectiy 10 Ihe individual concerned. If there Is any Informallon in your report wl1lch, If released 10 your patienl, may harm his or her physic~1 or menial well·being, please ldenlify It and bnefly stall! below why you believe K should nol bo released dr.clly 10 the pallent Similarty, please specify any other special cln:umstances which should be laken Into accounl when deciding on lhe ,aleese 01 your repon.
Is there ~rmatlon In this report which, If released to the paUenl, mlghl be prejudicial to hlslhei physical or ~.enlal hoalth?
No ~ Go flJ next quesffon '. Yes D Idontlfy tho Inform.Hen and stale why il should not be released directly to 111. patient
.--
Please return this report directly 10 Centrelink.
STAT.0971.001.0211_R

. . 11 Would yo~ to discuss any aspects at this report willt Centrellnk?
Noe:( YesO~1
I-UI L!=X 1/'LUI - I-'At;;!= 100 ot 'L'LJ
13 If someone from Centrellnk, or another assessor nominated by Cen\r.link. needs to contact you 10 discuss any aspects of Ihls repon.
14
whal daysltimes suit you?
Day Time
r'-I ~-·~------'II ' ~ I;=,....=,-"-=~====;II
Confidentiality 01 InlomaUon The per.;onai Information that Is provided to you for the purpose of this report must be kept confldenlla1 under saction 202 01 the Social Security (Admlnlsll4ilon)Act 1999.11 caflnat be disclosed to anyone else unless authOlis.d by law. Tltere are penall1es for offences agelnst secUon 202 of the Social Security (Administration) Act 1999.
15 Oelalls of doclor completing this report Please print In BLOCK LffiERS or use stamp. NiII1IB
Professional quanlllcatlons
Address
Phone number REOACTf 0 I
9 ..
\)(). I Date
fl:n / ';:)
~~ I f:. I C-> I Stamp Of applid Ie) /
' .../
Returning this report You can give this report and any attachments to your patient or you can return this report direclly to Centrellnk. However, if you answered 'Yes' at question 11, please make sure to return this report directly to Centreiink.
STAT.0971.001.0212_R