
1229377 634548716590312500
39
SPINAL AND EPIDURAL ANAESTHESIA PRESENTED BY ---- Dr. KHAWER MUNEER MODERATOR ---- Dr. JAVED IQBAL
-
Upload
bandarindupriya08 -
Category
Design
-
view
29 -
download
0
Transcript of 1229377 634548716590312500

SPINAL AND EPIDURAL
ANAESTHESIA
PRESENTED BY ---- Dr. KHAWER MUNEERMODERATOR ---- Dr. JAVED IQBAL

OBJECTIVES
2
HAVE A BASIC UNDERSTANDING OF
• Anatomic structure of spine and vertebra•Anatomic structure of spinal cord•Blood supply of spinal cord•Features of neuraxial blockade•Indications/ contraindications•Patient evaluation and preparation•Techniques•Local anesthetics and factors effecting spread•complications

BRIEF HISTORY OF SPINAL ANAESTHESIA CSF DISCOVERED ---- by Domenico Catugno 1764
CSF CIRCULATION---- by F . Magendie 1825 FIRST SPINAL ANALGESIA--- by J Leonard Corning 1885 FIRST PLANNED SPINAL ANAESTHESIA--- by
August Bier in 1891 The epidural space was first described by Corning
in 1901, and Fidel Pages first used epidural anaesthesia in humans in 1921.

ANATOMY
•cervical vertebrae (7) •thoracic vertebrae (12) •lumbar vertebrae (5) •sacral vertebrae (5) •coccygeal vertebrae (4 )

LUMBAR VERTEBRA

SPINAL CORDADULTS– approx L1CHILDREN--approx L3

ARTERIAL SUPPLY OF SPINAL CORD

DERMATOMESA dermatome is an area of skin innervated by sensory fibers from a single spinal nerve

DERMATOMAL LEVELS OF SPINAL ANESTHESIA FOR COMMON SURGICAL PROCEDURES
Procedure Dermatomal Level
Upper abdominal surgery T4
Intestinal, gynecologic, and urologic surgeryTransurethral resection of the prostate
T6
Vaginal delivery of a fetus, and hip surgery
T10
Thigh surgery and lower leg amputations
L1
Foot and ankle surgery L2
Perineal and anal surgery S2 to S5 (saddle block)
PHYSIOLOGICAL EFFECTS OF NEURAXIAL BLOCKADE
• Vasomotor tone determined by sympathetic fibers arising from T5 to L1 innervating arterial & venous smooth muscle.
• A ↓ in blood pressure that may be accompanied by ↓ in heart rate.
• With high sympathetic block, sympathetic cardiac accelerator fibers arising at T1-T4 are blocked, leading to ↓ cardiac contractility.
• Bezold-Jarisch reflex has been implicated as a cause of bradycardia, hypotension and cardiovascular collapse after central neuraxial anaesthesia, in particular spinal anaesthesia.
CARDIOVASCULAR EFFECTS:

PULMONARY EFFECTS:
Even with high thoracic levels, tidal volume is unchanged.
A small decrease in vital capacity due to paralysis of abdominal muscles necessary for forced exhalation & not due to decrease in phrenic nerve or diaphragmatic function.
Effective coughing & clearing of secretions may get affected with higher levels of block.
Rare respiratory arrest associated with spinal anaesthesia due to hypoperfusion of respiratory centers in brain stem.

GASTROINTESTINAL FUNCTION:
Nausea and vomiting in upto 20% patients due to gastrointestinal hyperperistalsis caused by unopposed parasympathetic(vagal) activity.
Vagal tone dominance results in small contracted gut with active peristalsis & can provide excellent operative conditions for some laproscopic procedures when used as an adjunct to GA.
Hepatic blood flow will ↓ with reductions in mean arterial pressure.

RENAL FUNCTION:
Renal function has a wide physiological reserve. ↓ in renal blood flow is of little physiological importance.
Neuraxial blocks are a frequent cause of urinary retention which delays discharge of outpatients & necessitates bladder catheterization in inpatients.

COMMON INDICATIONS OF NEURAXIAL ANAESTHESIA
SPINAL 1. lower extremities 2. pelvic /lower abdomen 3. pain mgmt intra/post operative (narcotics)
EPIDURAL 1. similar surgeries as spinal 2. labour and delivery 3. post op pain mgmt 4. chronic pain mgmt 5. in combination with GA for abdominal & thoracic procedures.

CONTRAINDICATIONS
ABSOLUTE 1. patients refusal 2.coagulopathy 3. infection at local
site 4. severe hypovolemia
5. increased ICT 6. allergy to drugs 7. shock 8. sever AS or MS
RELATIVE 1. uncoperative pt 2. preexisting
neurological deficits 3. demyelinating lesions 4. severe spinal
deformity 5. infection at site
remote from infection 6. sepsis

SEQUENCE OF ONSET
Principal site of action is the nerve root. Sequence of onset depends on conc. of LA
achieved, duration of contact, size & myelination of nerve fibers.
CLINICALLY OBSERVED SEQUENCE1. Sympathetic nervous system fibers (B
fibers: vasodilation, skin temp ↑)2. Temperature & pain conduction (A & C
fibers)3. Proprioception & touch (Aγ & Aβ fibers)4. Motor function (A fibers)

SUMMARYMedicatio
nPreparation Dose
Lower Limbs
DoseLower
Abdomen
Dose Upper
Abdomen
Procaine 10% Solution 75 mg 125 mg 200 mg
Lidocaine 5% Solution in 7.5% dextrose
25-50 mg 50-75 mg 75-100 mg
Tetracaine 1% Solution in 10% glucose or as niphanoid crystals
4-8 mg 10-12 mg 10-16 mg
Bupivacaine
0.5-0.75% Isobaric Solution
0.5-0.75% Hyperbaric
Solution in 8.25% Dextrose
Hypobaric Solution
4-10 mg 12-14 mg 12-18 mg
Ropivacaine
0.2—1% solution 8-12mg 12-16 16-18
DOSAGE AND ACTIONS OF COMMONLY USED SPINAL ANESTHETIC DRUGS

FACTORS AFFECTING THE LEVEL OF SPINAL ANESTHESIAMOST IMPORTANT FACTORS
Baricity of the drug
Position of the patient Drug dosage Site of injection OTHER FACTORS
Age
Csf
Curvature of Spine
Intraabdominal Pressure
Needle direction
Patient Height
Pregnancy
Weight of pt

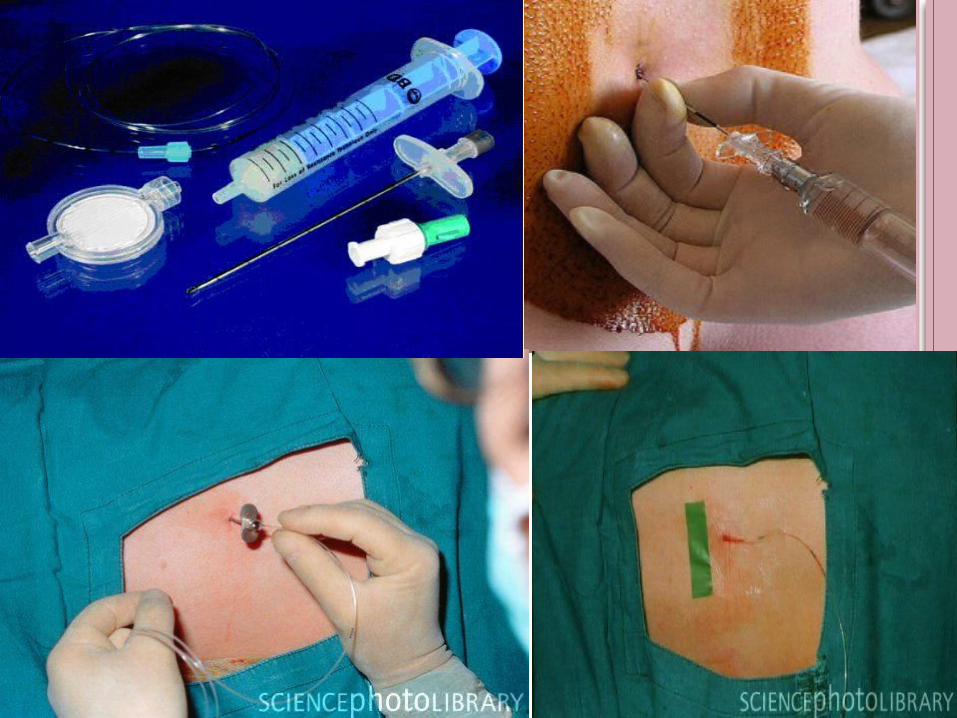
PROCEDURE PREPERATION
Remove your jewellery/watches Wash your hands I.V access/fluids bolus if needed Emergency drugs /equipment Position Sedation if needed Monitoring NIBP/SPO2/ECG• Verbal contact with pt

POSITIONING 1. Sitting 2. Lateral 3. Prone
TECHNIQUES FOR SPINAL 1. Midline 2. Paramedian 3. Taylor approach
The structures that will be passed in spinal : Skin , subcutaneous tissue, supraspinous ligament , interspinous ligament , lagementum flavum , dura mater , subdural space , arachnoid matter,subarachnoid space in midline approach

SPECIFIC TECHNIQUES FOR EPIDURAL LOSS OF RESISTANCE HANGING DROP
AGENTS FOR EPIDURAL ANAESTHESIAAGENT CONCENT
RATIONONSET SENSORY
BLOCKMOTOR BLOCK
CHLOROPROCAINE
2%3%
FastFast
AnalgesicDense
Mild to moddense
LIDOCAINE <1%1.5%2%
IntermediateIntermediateIntermediate
AnalgesicDenseDense
MinimalMild to moddense
BUPIVICAINE <0.25%0.5%0.75%
SlowSlowSlow
AnalgesicDenseDense
Minimal Mild to mod Mod to dense
ROPIVICAINE 0.2%0.5%0.75%--1.0%
SlowSlowSlow
AnalgesicDenseDense
Minimal Mild to mod Mod to dense



EPIDURAL NEEDLES

SPINAL NEEDLES
COMPLICATIONS/SIDE EFFECTS OF NEURAXIAL ANESTHESIA
Systemic toxicity Hypotension Postdural Puncture Headache High Spinal Anesthesia Total spinal anaesthesia Neurological complications Arachnoiditis / Meningitis Spinal / Epidural Hematoma Formation Epidural Abscess Backache Urinary retension Pruritus


POSTDURAL PUNCTURE HEADACHE ONSET= 12—72 hrs it is postural and it is often fronto--occipital associated with stiff neck , nausea,
vomiting , dizziness and photophobia. CAUSE---loss of CSF at a faster rate than it can be produced causing traction
on the structures supporting brain, particularly dura and tentorium. INCIDENCE---25% FACTORS---that increase the risk are young age,female,pregnancy,large gauge
needle, multiple punctures It is aggravated by sitting or standing and decreased or relieved by lying down
flat. TREATMENT----- conservative t/t involves recumbent position, analgesics, i.v
or oral fluids and caffeine.
29
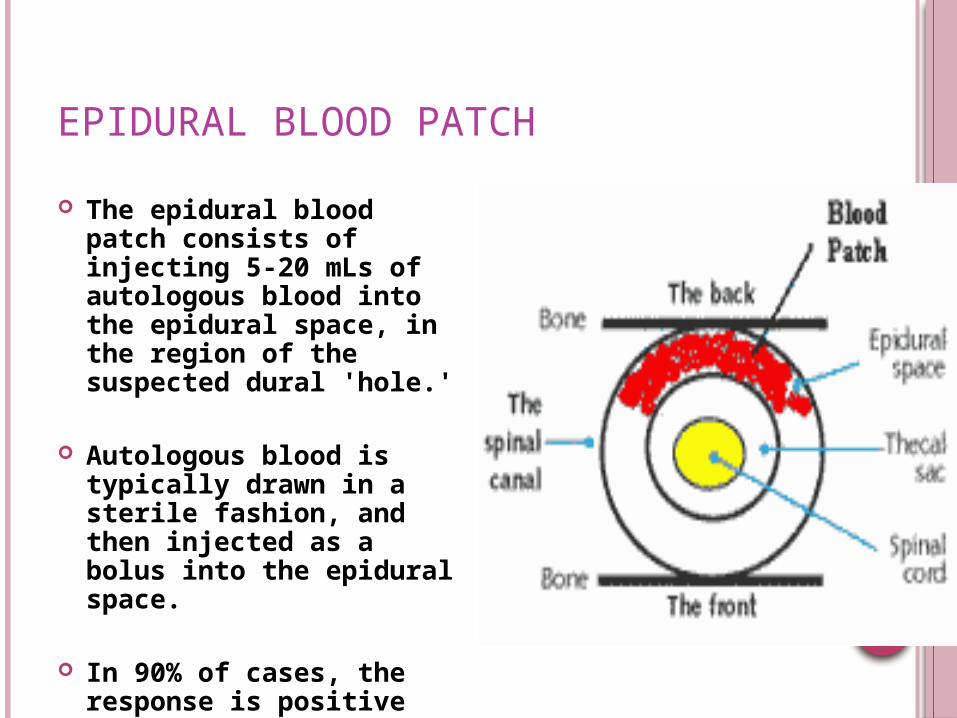
EPIDURAL BLOOD PATCH
The epidural blood patch consists of injecting 5-20 mLs of autologous blood into the epidural space, in the region of the suspected dural 'hole.'
Autologous blood is typically drawn in a sterile fashion, and then injected as a bolus into the epidural space.
In 90% of cases, the response is positive and immediate. Subsequently, long-term relief of PDPH occurs in the majority of cases

HIGH NEURAL BLOCKADE ,HIGH SPINAL AND TOTAL SPINAL ANAESTHESIA
Can occur both with spinal and epidural Admins . Of an excessive dose,failure to reduce doses
in selected pts (elderly,pregnant,obese , very short) or unusual sensitivity or spread of LA maybe responsible
SA ascending into cervical level causes severe hypotension,bradycardia and respiratory insufficiency and even apnea
Total spinal can occur following attempted epidural/caudal anesthesia if there is inadvertent intrathecal injection
TREATMENT---vasopressors,atropine ,fluids,oxygen ,assisted ventillation and even intubation and mechanical ventillation may be needed

TRANSIENT NEUROLOGICAL SYMPTOMS AND CAUDA EQUINA SYNDROME
TNS or transient radicular irritation refers to pain ,dysesthesia or both in the legs or buttocks after spinal anesthesia, resolving spontaneously within several days
Most common with hyperbaric lidocaine and after surgery in lithotomy position
CES characterized by bowel and bladder dysfunction together with evidence of multiple nerve root injury, assoc with use of continous spinal catheters and 5% lidocaine


NEURAXIAL BLOCKADE IN SETTING OF ANTICOAGULANTS AND ANTIPLATELET AGENTS---AMERICAN SOCIETY FOR REGIONAL ANESTHESIA RECOMMENDATIONS
Pts taking NSAIDS or receiving subcutaneous unfractioned heparin for DVT prophylaxsis are not viewed as being at increased risk of spinal hematoma
DISCONTINUE---ticlopidine 2 weeks, clopidogrel for 1 week ,abciximab 24 to 48 hrs, eptifibate and tirofiban 4 to 8 hrs before performing central neuraxial block.
Pt who are fully anticoagulated or who are receiving thrombolytic or fibrinolytic theraphy should not receive central neuraxial block except in very unusual circumstances where other options are not viable.
Delay atleast 10 -12 hrs after last dose of LMWH Post op t/t with LMWH delay 12hrs after compl of surgery Removal of epi ,spi catheters should take place 10—12hrs
after last dose with subs dosing delay for atleast 2hrs.
ADVANTAGES OF SPINAL ANESTHESIA (SPA)
1. Cost. The costs associated with SPA are minimal.
2. Patient satisfaction. the majority of patients are very happy with this technique.
3. Respiratory disease. SPA produces few adverse effects on the respiratory system as long as unduly high blocks are avoided.
4. Patent airway. As control of the airway is not compromised, there is a reduced risk of airway obstruction or the aspiration of gastric contents.
5. Diabetic patients. There is little risk of unrecognised hypoglycaemia in an awake patient.

ADVANTAGES OF SPA CONTD
6. Muscle relaxation. SPA provides excellent muscle relaxation for lower abdominal and lower limb surgery.
7. Bleeding. Blood loss during operation is less than when the same operation is done under general anaesthesia
8. Splanchnic blood flow. Because of its effect on increasing blood flow to the gut, spinal anaesthesia reduces the incidence of anastomotic dehiscence
9. Visceral tone. The bowel is contracted by SPA and sphincters relaxed although peristalsis continues. Normal gut function rapidly returns following surgery.
10. Coagulation. Post-operative deep vein thromboses and pulmonary emboli are less common following spinal anaesthesia.

DIFFERENCES BETWEEN SPINAL AND EPIDURAL ANESTHESIA
Spinal anaesthesia Epidural Anaesthesia
Level: below L1/L2, where the spinal cord
ends
Level: at any level of the vertebral column.
Injection: subarachnoid space i.e punture
of the dura mater
Injection: epidural space (between
Ligamentum flavum and dura mater) i.e
without punture of the dura mater
Identification of the subarachnoid space:
When CSF appears
Identification of the Peridural space: Using
the Loss of Resistance technique.
Dosis: 2.5- 3.5 ml bupivacaine 0.5% heavy Doses: 15- 20 ml bupivacaine 0.5%
Onset of action: rapid (2-5 min) Onset of action: slow (15-20 min)
Density of block: more dense Density of block: less dense
Hypotension: rapid Hypotension: slow
Headache: is a probably complication Headache: is not a probable. 37

REGIONAL VS GENERAL ANAESTHESIA

THANK YOU


















