






Languages
Pages
Legal

PELVIC OSTEOTOMYFOR THE TREATMENT OF
THE YOUNG ADULT WITH HIP PAIN
Emmanuel Illical, Adult Reconstruction Fellow
OUTLINE• Pelvic osteotomy introduction• Background: hip dysplasia• Bernese periacetabular osteotomy (PAO)
– Technique & Surgical adjuncts
– Advantages & Complications
– Clinical Results
• Background: acetabular retrotorsion• Reverse PAO
– Principles
– Clinical Results
• Other osteotomies• Salvage Osteotomies• Summary

• Treatment of choice for acetabular structural disorders for young pts– classical developmental hip dysplasia
– retrotorsional acetabular abnormalities
• Indications– symptomatic patient (pain / progressive limp)
– radiographically negative for advanced OA
– adequate and relatively painless passive ROM
• Rationale– restore normal hip anatomy and biomechanics
• increase joint congruity
• optimize center of rotation
– relieve symptoms
– prevent (possibly delay?) degenerative changes
• Challenges: diagnosis & predictability of outcome
PELVIC OSTEOTOMY: INTRODUCTION

• Acetabular abnormalities– shallow
– anteverted (retrortosion in up to 25%)
– lateralized
– femoral head coverage deficient anteriorly, laterally, superiorly
• Femoral abnormalities– proximal migration– femoral head small and deformed– femoral neck short and narrrow w/ varying but but anteversion– valgus neck shaft angle– femoral canal narrow
• Secondary degenerative joint disease over time contact area btwn femoral head and acetabulum
– excessive lateralization of body weight lever arm body weight lever arm
– relatively high forces transmitted through surface area
BACKGROUND: HIP DYSPLASIA

BACKGROUND: HIP DYSPLASIA

BACKGROUND: HIP DYSPLASIA

BERNESE PAO: TECHNIQUE

• Anterior arthrotomy: before or after PAO– labral pathology: debridement / repair
– femoral head neck junction: osteochondroplasty
• Proximal femoral osteotomy– severe coxa valga / vara varus / valgus producing intertrochanteric osteotomy
BERNESE PAO: SURGICAL ADJUNCTS

• Only one incision that spares ABductors• Reproducible extra-articular osteotomies• Allows large corrections in all directions• Posterior column remains intact
– minimal internal fixation required
– early mobilization w/o external immobilization
• Preservation of acetabular fragment vascularity– intra-articular examinzation w/o further risk of devascularization
• True pelvis shape is unchanged– child bearing & vaginal delivery not affected
BERNESE PAO: ADVANTAGES

• Most important factor affecting incidence = surgeon experience
• Most common complication = nerve dysfunction– lateral femoral cutaneous nerve (35%)
– femoral nerve
– sciatic / peroneal nerve
• Vascular – related ilioinguinal approach: femoral / iliac artery thrombosis
• Inadvertent extension of osteotomy to undesirable location– intra-articular extension of infra / supra – acetabular osteotomies
– sciatic notch extension of iliac osteotomies
• Femoroacetabular impingement
• Osteonecrosis of acetabular fragment
• Nonunion
• Other: HO, loss of correction, femoral head subluxation
BERNESE PAO: COMPLICATIONS

BERNESE PAO: CLINICAL RESULTS

BERNESE PAO: CLINICAL RESULTS

• Posteriorly oriented acetabular opening (sagittal plane)• Etiology
– isolated entity
– associated w/ classic hip dysplasia
– injury to tri-radiate cartilage in growing child
– associated with LCP, bladder extrophy, neuromuscular d/o
• Typical presentation is groin pain reproduced with “impingement signs”
• Recurrent impingement has been implicated in development of 2* arthrosis
BACKGROUND: ACETABULAR RETROTORSION

BACKGROUND: ACETABULAR RETROTORSION

• Treatment of choice when acetabular retrotorsion exists– +ve crossover sign AND +ve posterior wall sign (poor posterior coverage)
– addresses lack of posterior wall coverage by increasing anteversion
• Technique– same approach and osteotomies as PAO
– re-orientation achieved by combined flexion + IR of acetabular fragment
– goals: eliminate xray signs+ sufficient impingement free ROM (flexion + IR)
– posterior over-coverage is a concern
– arthrotomy / SHD to address femoral head neck offset & labral pathology
• Contra-indications– excessive posterior wall coverage / AI < 0* impingement
– significant combined CAM / pincer deformity requires surgical hip dislocation
– advanced cartilage degeneration area would end up in weight bearing zone
REVERSE PAO: PRINCIPLES

• Siebenrock et al. JBJS Am 2003. Impingement due to acetabular retroversion. Treatment with PAO.– 29 reverse PAOs to reorient retroverted acetabulum (+ve cross over / pw sign)– concominant femoral head neck osteochondroplasty in 24 hips– avg 30 month f/u– significant increase in flexion / IR / ADduction– significant d’Aubigne hip score improvement: 14.0 16.9– 28 “good / excellent” results– no pt had radiographic signs of OA– 3 revisions
• Buchler et al. JBJS Br 2011. Symptomatic acetabular retroversion: mean 10 year fu after treatment with PAO.– mean f/u 10.6 year – overall d’Aubinge score improved: 14.0 16.3– all patients had symptomatic relief at final f/u– ROM and functional scores improved in all cases– vast majority of pts continued to demonstrate no signs of radiographic OA
REVERSE PAO: CLINICAL RESULTS

OTHER OSTEOTOMIES
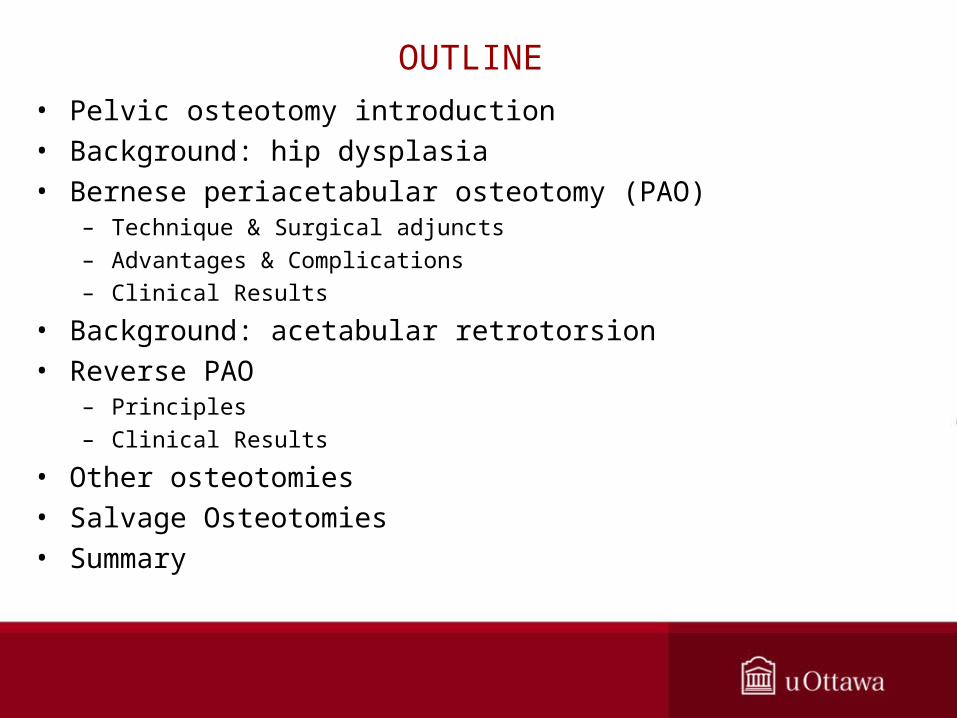
SALVAGE OSTEOTOMIES

• Full pre-operative work-up– assess degree of dysplasia and acetabular version
– assess femoral head neck offset
– assess labral pathology
• Select patients appropriately– symptomatic
– be aware of age
– no more than mild to moderate articular degenerative changes (Tonnis grade < 2)
– reasonable joint congruity (obtain functional xrays if necessary)
• Surgeon experience key to minimizing complications
SUMMARY
Top Related