





Languages
Pages
Legal


Oncology emergencies: Dr Dainik Patel
Medical Oncologist
Lyell McEwin Hospital
Adelaide Cancer Centre ( Tennyson Centre, 480 specialist centre)

Agenda:
Background
cancer related emergencies
Chemotherapy related emergencies
Immunotherapy related emergencies

Background:
Cancer patients present to the ED with poorly managed symptoms or treatment related toxicities
• Most common : fever, infection, GI toxicity, pain ,respiratory illness
Some particular syndrome need to be promptly recognized to avoid long term consequences
• Multidisciplinary approach is necessary

GP’s role:
Early
• Recognize red flags
•
• Prevention
• Education
• Close monitoring
presentation
• Assessment and initial treatment
• Communication with team and ED
Post
• Follow up visits and investigations

Agenda:
Spinal cord compression
Superior ven-cava syndrome

Cancer related emergencies: spinal cord compression
5% of all cancer patients
• Common problem in prostate, lung, breast and RCC. Other includes hodgkin’s lymphoma, myeloma as well.
Thoracic: 60%, lumber: 25% and cervical 15%
• Always image whole spine MRI as third of the cases have multi-level metastasis
Survival is limited in patients with multiple spinal metastasis with cord compression

Cancer related emergencies: spinal cord compression
• Commonly,presenting symptoms is pain
• Muscle weakness (60-86%)
• 2/3 not ambulatory at time of diagnosis
• Sensory loss is less common
• Bladder and bowel dysfunction: late
• Functional capacity is the single most
predictor of outcome

spinal cord compression ; CT vs MRI
MRI Gold
standard

Cancer related emergencies: spinal cord compression (ESMO guidelines)
Recognize and expedite
Start early treatment

Cancer related emergencies: Superior Vencava Syndrome

Cancer related emergencies: Superior Vencava Syndrome

Cancer related emergencies: Superior Vencava Syndrome

Cancer related emergencies: Superior Vencava Syndrome (ESMO guideline)

Chemotherapy related emergencies
Febrile neutropenia
Diarrhea

Chemotherapy related emergencies : Febrile neutropenia
10%–50% of patients with solid tumours and >80% of those with hematological malignancies
• The degree and duration of neutropenia closely correlate with the risk of serious infectious complications.
Clinically documented infections occur in 20%–30% of febrile episodes.
GCSF has reduced significantly rate of FN

Chemotherapy related emergencies: Febrile neutropenia
Neutrophils in the activation and regulation of innate and adaptive immunity,Alberto Mantovani, Marco A. Cassatella, Claudio Costantini & Sébastien Jaillon,Nature Reviews Immunology
Volume,11,pages 519–531 (2011)
Responsible
for fungal
and viral
infection
after
prolong
duration

Chemotherapy related emergencies : Febrile neutropenia

Chemotherapy related emergencies : Diarrhea
• Common problem
• Chemo: many but not all
• TKI: any ( sunitinib, pazopanib)
• Preventable and treatable
• Could lead to ICU admission

Chemotherapy related emergencies : Diarrhoea
Mechanism of diarrohea
• Decrease surface area (secretory)
• Increase motility (like irinotecan)
• Decreased enzyme activity (osmotic)
• Bacterial overgrowth
• Increase mucous secretions
• Over-treated constipation

Chemotherapy related emergencies : Diarrhoea

Chemotherapy related emergencies : Diarrhoea management

James Allison, of the
University of Texas MD
Anderson Cancer Centre, and
Kyoto University's Tasuku
Honjo
Immunotherapy side effects: background

Immunotherapy related emergencies : Background
https://grandroundsinurology.com/immunotherapy-for-prostate-cancer/

Immunotherapy: current landscape
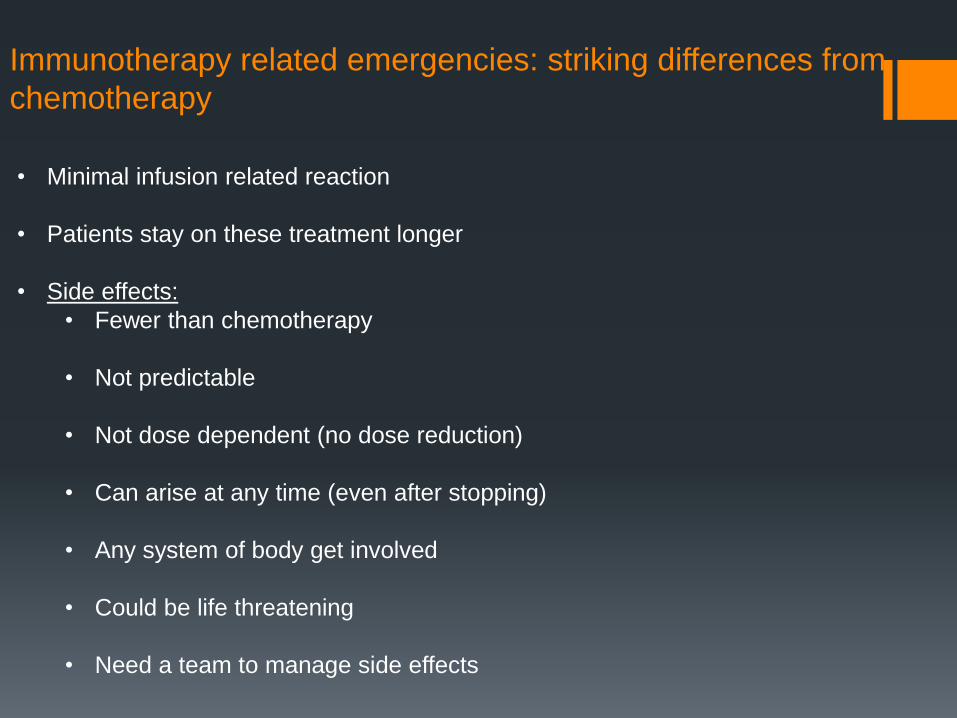
Immunotherapy related emergencies: striking differences from
chemotherapy
• Minimal infusion related reaction
• Patients stay on these treatment longer
• Side effects:
• Fewer than chemotherapy
• Not predictable
• Not dose dependent (no dose reduction)
• Can arise at any time (even after stopping)
• Any system of body get involved
• Could be life threatening
• Need a team to manage side effects

MA Postow et al. N Engl J Med 2018;378:158-168.
Possible Mechanisms Underlying Immune-Related Adverse Events.

Immunotherapy related
emergencies:
Spectrum of organ
involvement
Any system of body get
involved!
The Immune Checkpoint
Inhibitors Unleashed to Fight
Cancer
May 17, 2017 • By Dana
Direnzo, MD, Ami A. Shah,
MD, MHS, Clifton O.
Bingham III, MD, & Laura C.
Cappelli, MD, MHS

Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis, treatment
and follow-up†
Ann Oncol. 2017;28(suppl_4):iv119-iv142. doi:10.1093/annonc/mdx225
Society for Medical Oncology.)
Immunotherapy: timeline for side effects
Even after completion of treatment!
Annals of Oncology, Volume 27, Issue 4, 28 December 2015, Pages 559–574, https://doi.org/10.1093/annonc/mdv623
The content of this slide may be subject to copyright: please see the slide notes for details.
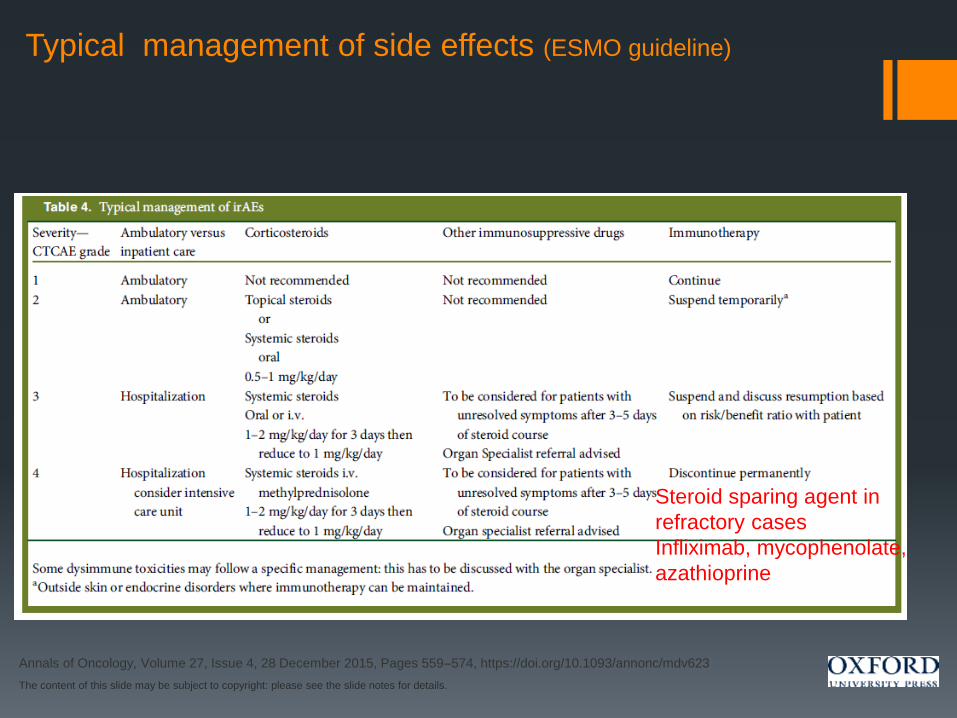
Typical management of side effects (ESMO guideline)
Steroid sparing agent in
refractory cases
Infliximab, mycophenolate,
azathioprine

Phone call from patient or carer
Need to have 24 hour hot line
Establish background and treatment regimen
Recognise red flags
Urgent vs semi-urgent
Arrange blood test (if patient has non-specific mild symptoms)
Initiate therapy (remotely located patient)
Urgent contact with physician
• Endocrinopathies
• Rest of the system
Immunotherapy: flow of management

Immunotherapy related emergencies

Immunotherapy related emergencies

58yr old
ECOG 1
Metastatic RCC
Hx of Psoriasis (local Rx)
On clinical trial with Nivolumab and cabozantinib
Tolerated well
During 2nd cycle
Abnormal LFTs
On routine bloods
Started on 1 mg/kg prednisolone
Immunotherapy case 1: Hepatitis ( only 3 doses of drug)

58yr old
ECOG 1
Metastatic RCC
Hx of Psoriasis (local Rx)
On clinical trial with Nivolumab and cabozantinib
Tolerated well
During 2nd cycle
Abnormal LFTs
On routine bloods
Started on 1 mg/kg prednisolone
Immunotherapy case 1: Hepatitis ( only 3 doses of drug)

No new symptoms
On routine bloods
Started on 1 mg/kg prednisolone
Did not have re-challenge due to severe psoriasis flare
CT shows excellent response
Immunotherapy case 1: Hepatitis ( only 3 doses of drug)

Immunotherapy case 2: Diabetes and hypothyrodism
70-Y F, ECOG 1, with metastatic lung cancer, >50% PD-L1
expression
3-weekly pembrolizumab (C1 1/5/18).
Presenting complaint:Polyuria, polydipsia and dry mouth
Examination: Unremarkable, stable vitals
Investigations: BGL 42, Ketones 6.8 mmol/L
HbA1c 8% TSH 97.6; fT4 <5
Diagnoses:
Diabetes (DKA) and hypothyrodism due to Pembrolizumab
Pembrolizumab was held
DKA protocol, started on levothyroxine 75 mcg
Diabetes education
Basal-bolus insulin regimen (insulin adjustment via phone clinic)
Keys in
history and
blood

Immunotherapy case 3: hypopitutarism
42 yr old lady
with resected high risk melanoma
On nivolumab for 4 months .
Presenting complaint: lethargy and hypotension in chemo suite
Examination: Unremarkable, hypotensive
Investigations: Cortisol <3
ACTH:3
Diagnoses:
hypopitutarism
nivolumab was held
On corticosteroid replacement
Resumed Nivolumab
Keys in
history and
blood

Immunotherapy case 4: Vasculitis and Pneumonitis
71 man, metastatic melanoma
On second line of treatment with
Combination of Ipilimumab and Nivolumab
Presented with cough, SOB and fever associated with
cold hands after 2 weeks of first infusion.
O/E: Crackles on both lower lobes

Immunotherapy case 4: Vasculitis and Pneumonitis

Immunotherapy case 4: Vasculitis and Pneumonitis
Commenced on Prednisolone 1.5mg/Kg with improvement in cough, SOB and fever after 2 days. Septic screen was negative
Hands got worse!

Immunotherapy case 4: Vasculitis and Pneumonitis
IV methylprednisolone for 3 days
Reviewed by vascular and rheumatology team
vasculitis screen and angiogram of UL was normal

Immunotherapy case 4: Vasculitis and Pneumonitis
steroids were weaned over 4 months. Not any complication except local infection.
4 months

Immunotherapy case 4: Vasculitis and Pneumonitis
▪ After a year without any treatment!
▪ FDG PET scan negative for any melanoma.

Annals of Oncology, Volume 27, Issue 4, 28 December 2015, Pages 559–574, https://doi.org/10.1093/annonc/mdv623
The content of this slide may be subject to copyright: please see the slide notes for details.
Figure 1. The five pillars of immunotherapy toxicity
management.

only possible with team approach!
Patient on immunotherapy
Emergency department
Medical oncologist
Nurse practioner
Allied health staff
General Practitioner

Take home message:
▪ More cancer patients will be on treatment and need team approach for
management
▪ Emergencies could be identified early and treat effectively
▪ Communication with other team members is crucial
▪ Steroids remained useful drug in many oncology emergencies
▪ Immune related side effects need to be considered with patient on
immunotherapy until proved otherwise.

Thank You!
Top Related