3-Chronic Pancreatitis 1-Acute & Chronic Pancreatitis 2-CT Imaging of Acute Pancreatitis.
Pancreas
Pancreas And it’s different diseases | S.M. Jasim Uddin
(Southern University BangladeshPancreas)
Pancreas
From Wikipedia, the free encyclopedia
For other uses, see Pancreas (disambiguation).
Pancreas
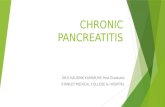
the pancreas
1: Head of pancreas2: Uncinate process of pancreas3: Pancreatic notch4: Body of pancreas5: Anterior surface of pancreas6: Inferior surface of pancreas7: Superior margin of pancreas8: Anterior margin of pancreas9: Inferior margin of pancreas10: Omental tuber11: Tail of pancreas12: Duodenum
Gray's
subject #251 1199
Artery
inferior pancreaticoduodenal artery, superior pancreaticoduodenal artery, splenic artery
Vein
pancreaticoduodenal veins, pancreatic veins
Nerve
pancreatic plexus, celiac ganglia, vagus[1]
Precursor
pancreatic buds
MeSH
Pancreas
Dorlands/Elsevier
Pancreas
The pancreas is a gland organ in the digestive and endocrine system of vertebrates. It is both an endocrine gland producing several important hormones, including insulin, glucagon, and somatostatin, as well as an exocrine gland, secreting pancreatic juice containing digestive enzymes that pass to the small intestine. These enzymes help to further break down the carbohydrates, proteins, and lipids in the chyme.
Histology
Under a microscope, stained sections of the pancreas reveal two different types of parenchymal tissue. Lightly staining clusters of cells are called islets of Langerhans, which produce hormones that underlie the endocrine functions of the pancreas. Darker staining cells form acini connected to ducts. Acinar cells belong to the exocrine pancreas and secrete digestive enzymes into the gut via a system of ducts.
Structure
Appearance
Function
Islets of Langerhans
Lightly staining, large, spherical clusters
Hormone production and secretion (endocrine pancreas)
Pancreatic acini
Darker staining, small, berry-like clusters
Digestive enzyme production and secretion (exocrine pancreas)
Function
The pancreas is a dual-function gland, having features of both endocrine and exocrine glands.
The part of the pancreas with endocrine function is made up of approximately a million[3] cell clusters called islets of Langerhans. Four main cell types exist in the islets. They are relatively difficult to distinguish using standard staining techniques, but they can be classified by their secretion: α cells secrete glucagon (increase glucose in blood), β cells secrete insulin (decrease glucose in blood), δ cells secrete somatostatin (regulates/stops α and β cells), and PP cells secrete pancreatic polypeptide. The islets are a compact collection of endocrine cells arranged in clusters and cords and are crisscrossed by a dense network of capillaries. The capillaries of the islets are lined by layers of endocrine cells in direct contact with vessels, and most endocrine cells are in direct contact with blood vessels, by either cytoplasmic processes or by direct apposition. According to the volume The Body, by Alan E. Nourse,[5] the islets are "busily manufacturing their hormone and generally disregarding the pancreatic cells all around them, as though they were located in some completely different part of the body." The pancreas as an exocrine gland helps out the digestive system. It secretes pancreatic juice that contains digestive enzymes that pass to the small intestine. These enzymes help to further break down the carbohydrates, proteins, and lipids (fats) in the chyme. The pancreas receives regulatory innervation via hormones in the blood and through the autonomic nervous system. These two inputs regulate the secretory activity of the pancreas.
Sympathetic (adrenergic)
α2: decreases secretion from beta cells, increases secretion from alpha cells, β2: increases secretion from beta cells
Parasympathetic (muscarinic)
M3: increases stimulation of alpha cells and beta cells[6]
Anatomy
Surface projections of the organs of the trunk, showing pancreas at the transpyloric plane
The pancreas lies in the epigastrium and left hypochondrium areas of the abdomen
It is composed of the following parts:
· The head lies within the concavity of the duodenum.
· The uncinate process emerges from the lower part of head, and lies deep to superior mesenteric vessels.
· The neck is the constricted part between the head and the body.
· The body lies behind the stomach.
· The tail is the left end of the pancreas. It lies in contact with the spleen and runs in the lienorenal ligament.
The superior pancreaticoduodenal artery from gastroduodenal artery and the inferior pancreaticoduodenal artery from superior mesenteric artery run in the groove between the pancreas and duodenum and supply the head of pancreas. The pancreatic branches of splenic artery also supply the neck, body and tail of the pancreas. The largest of those branches is called the arteria pancreatica magna; its occlusion, although rare, is fatal.
The body and neck of the pancreas drain into splenic vein; the head drains into the superior mesenteric and portal veins.
Lymph is drained via the splenic, celiac and superior mesenteric lymph nodes.
Diseases
Pancreatic disease
Pancreatic disease
Classification and external resources
ICD-10
K85.-K86., Q45.0-Q45.3
ICD-9
577, 751.7
MeSH
D010182
Pancreatic diseases include:
Pancreatitis
Pancreatitis is inflammation of the pancreas. There are two forms of pancreatitis, which are different in causes and symptoms, and require different treatment:
· Acute pancreatitis is a rapid-onset inflammation of the pancreas, most frequently caused by alcoholism or gallstones.
· Chronic pancreatitis is a long-standing inflammation of the pancreas.
Diabetes mellitus
The pancreas is central in the path physiology of both major types of diabetes mellitus. In type 1 diabetes mellitus, there is direct damage to the endocrine pancreas that results in insufficient insulin synthesis and secretion. Type 2 diabetes mellitus, which begins with insulin resistance, is characterized by the ultimate failure of pancreatic β cells to match insulin production with insulin demand.
Exocrine pancreatic insufficiency
Exocrine pancreatic insufficiency (EPI) is the inability to properly digest food due to a lack of digestive enzymes made by the pancreas. EPI is found in humans afflicted with cystic fibrosis and Shwachman-Diamond syndrome. It is caused by a progressive loss of the pancreatic cells that make digestive enzymes. Chronic pancreatitis is the most common cause of EPI in humans. Loss of digestive enzymes leads to maldigestion and malabsorption of nutrients.
Cystic fibrosis
Cystic fibrosis, also known as mucoviscidosis, is a hereditary disease that affects the entire body, causing progressive disability and early death. It is caused by a mutation in the cystic fibrosis transmembrane conductance regulator (CFTR) gene. The product of this gene helps create sweat, digestive juices, and mucus. The name cystic fibrosis refers to the characteristic 'fibrosis' (tissue scarring) and cyst formation within the pancreas, which causes irreversible damage to the pancreas, often resulting in painful inflammation (pancreatitis).
Pseudocysts
A pancreatic pseudocyst is a circumscribed collection of fluid rich in amylase and other pancreatic enzymes, blood and necrotic tissue, typically located in the lesser sac.
Cysts
X-ray computed tomography (CT scan) findings of cysts in the pancreas are common, and often are benign. In a study of 2,832 patients without pancreatic disease, 73 patients (2.6%) had cysts in the pancreas.[1] About 85% of these patients had a single cyst. Cysts ranged in size from 2 to 38 mm (mean, 8.9 mm). There was a strong correlation between the presence of cysts and age. No cysts were identified among patients less than 40 years of age, while 8.7 percent of the patients aged 80 to 89 years had a pancreatic cyst.
Cysts also may be present due to intraductal papillary mutinous neoplasm.
Congenital malformations
Pancreas divisum is a malformation in which the pancreas fails to fuse. It is a rare condition that affects only 6% of the world's population, and of these few, only 1% ever have symptoms that require surgery.
Annular pancreas
Annular pancreas is characterized by a pancreas that encircles the duodenum. It results from an embryological malformation in which the early pancreatic buds undergo inappropriate rotation and fusion, which can lead to small bowel obstruction.
NeoplasmBenign
· Serous cystadenoma of the pancreas
· Solid pseudopapillary neoplasm
Zollinger-Ellison syndrome
Zollinger-Ellison syndrome is a collection of findings in individuals with gastrinoma, a tumor of the gastrin-producing cells of the pancreas. Unbridled gastrin secretion results in elevated levels of the hormone, and increased hydrochloric acid secretion from parietal cells of the stomach. It can lead to ulceration and scarring of the stomach and intestinal mucosa.
Hemosuccus pancreaticus
Hemosuccus pancreaticus, also known as pseudohematobilia or Wirsungorrhage, is a rare cause of hemorrhage in the gastrointestinal tract. It is caused by a bleeding source in the pancreas, pancreatic duct, or structures adjacent to the pancreas, such as the splenic artery, that bleed into the pancreatic duct. Patients with hemosuccus may develop symptoms of gastrointestinal hemorrhage, such as blood in the stools, maroon stools, or melena. They may also develop abdominal pain. Hemosuccus pancreaticus is associated with pancreatitis, pancreatic cancer and aneurysms of the splenic artery. Angiography may be used to diagnose hemosuccus pancreaticus, where the celiac axis is injected to determine the blood vessel that is bleeding. Concommitant embolization of the end vessel may terminate the hemorrhage. Alternatively, a distal pancreatectomy may be required to stop the hemorrhage
Because the pancreas is a storage depot for digestive enzymes, injury to the pancreas is potentially very dangerous. A puncture of the pancreas generally requires prompt and experienced medical intervention.
Pancreatic cancers, particularly cancer of the exocrine pancreas, remain one of the most deadly cancers, and the mortality rate is very high.
Diabetes mellitus type 1 is a chronic autoimmune disorder in which the immune system attacks the insulin-secreting cells in the pancreas.
History
The pancreas was first identified for western civilization by Herophilus (335–280 BC), a Greek anatomist and surgeon. Only a few hundred years later, Rufus of Ephesus, another Greek anatomist, gave the pancreas its name. The term "pancreas" is derived from the Greek πᾶν ("all", "whole"), and κρέας ("flesh"). – presumably because of its fleshy consistency.
Embryological development
Schematic illustrating the development of the pancreas from a dorsal and a ventral bud. During maturation the ventral bud flips to the other side of the gut tube (arrow) where it typically fuses with the dorsal lobe. An additional ventral lobe which usually regress during development is omitted.
The pancreas forms from the embryonic foregut and is therefore of endodermal origin. Pancreatic development begins [with] the formation of a ventral and dorsal anlage (or buds). Each structure communicates with the foregut through a duct. The ventral pancreatic bud becomes the head and uncinate process, and comes from the hepatic diverticulum.
Differential rotation and fusion of the ventral and dorsal pancreatic buds results in the formation of the definitive pancreas. As the duodenum rotates to the right, it carries with it the ventral pancreatic bud and common bile duct. Upon reaching its final destination, the ventral pancreatic bud fuses with the much larger dorsal pancreatic bud. At this point of fusion, the main ducts of the ventral and dorsal pancreatic buds fuse, forming the duct of Wirsung, the main pancreatic duct.
Differentiation of cells of the pancreas proceeds through two different pathways, corresponding to the dual endocrine and exocrine functions of the pancreas. In progenitor cells of the exocrine pancreas, important molecules that induce differentiation include follistatin, fibroblast growth factors, and activation of the Notch receptor system. Development of the exocrine acini progresses through three successive stages. These include the predifferentiated, protodifferentiated, and differentiated stages, which correspond to undetectable, low, and high levels of digestive enzyme activity, respectively.
Progenitor cells of the endocrine pancreas arise from cells of the protodifferentiated stage of the exocrine pancreas. Under the influence of neurogenin-3 and Isl-1, but in the absence of notch receptor signaling, these cells differentiate to form two lines of committed endocrine precursor cells. The first line, under the direction of Pax-0, forms α- and γ- cells, which produce glucagon and pancreatic polypeptides, respectively. The second line, influenced by Pax-6, produces β- and δ-cells, which secrete insulin and somatostatin, respectively.
Insulin and glucagon can be detected in the human fetal circulation by the fourth or fifth month of fetal development.
In animals
Pancreatic tissue is present in all vertebrate species, but its precise form and arrangement varies widely. There may be up to three separate pancreases, two of which arise from ventral buds, and the other dorsally. In most species (including humans), these fuse in the adult, but there are several exceptions. Even when a single pancreas is present, two or three pancreatic ducts may persist, each draining separately into the duodenum (or equivalent part of the foregut). Birds, for example, typically have three such ducts.
In teleosts, and a few other species (such as rabbits), there is no discrete pancreas at all, with pancreatic tissue being distributed diffusely across the mesentery and even within other nearby organs, such as the liver or spleen. In a few teleost species, the endocrine tissue has fused to form a distinct gland within the abdominal cavity, but otherwise it is distributed amongst the exocrine components. The most primitive arrangement, however, appears to be that of lampreys and lungfish, in which pancreatic tissue is found as a number of discrete nodules within the wall of the gut itself, with the exocrine portions being little different from other glandular structures of the intestine.
Pancreatitis
On this page:
· What is pancreatitis?
· What is acute pancreatitis?
· What is chronic pancreatitis?
· How common is pancreatitis in children?
· Hope through Research
What is pancreatitis?
Pancreatitis is inflammation of the pancreas. The pancreas is a large gland behind the stomach and close to the duodenum—the first part of the small intestine. The pancreas secretes digestive juices, or enzymes, into the duodenum through a tube called the pancreatic duct. Pancreatic enzymes join with bile—a liquid produced in the liver and stored in the gallbladder—to digest food. The pancreas also releases the hormones insulin and glucagon into the bloodstream. These hormones help the body regulate the glucose it takes from food for energy.
Normally, digestive enzymes secreted by the pancreas do not become active until they reach the small intestine. But when the pancreas is inflamed, the enzymes inside it attack and damage the tissues that produce them.
Pancreatitis can be acute or chronic. Either form is serious and can lead to complications. In severe cases, bleeding, infection, and permanent tissue damage may occur.
The gallbladder and the ducts that carry bile and other digestive enzymes from the liver, gallbladder, and pancreas to the small intestine are called the biliary system.
Both forms of pancreatitis occur more often in men than women.
What is acute pancreatitis?
Acute pancreatitis is inflammation of the pancreas that occurs suddenly and usually resolves in a few days with treatment. Acute pancreatitis can be a life-threatening illness with severe complications. Each year, about 210,000 people in the United States are admitted to the hospital with acute pancreatitis.1 The most common cause of acute pancreatitis is the presence of gallstones—small, pebble-like substances made of hardened bile—that cause inflammation in the pancreas as they pass through the common bile duct. Chronic, heavy alcohol use is also a common cause. Acute pancreatitis can occur within hours or as long as 2 days after consuming alcohol. Other causes of acute pancreatitis include abdominal trauma, medications, infections, tumors, and genetic abnormalities of the pancreas.
Symptoms
Acute pancreatitis usually begins with gradual or sudden pain in the upper abdomen that sometimes extends through the back. The pain may be mild at first and feel worse after eating. But the pain is often severe and may become constant and last for several days. A person with acute pancreatitis usually looks and feels very ill and needs immediate medical attention. Other symptoms may include
· a swollen and tender abdomen
· nausea and vomiting
· fever
· a rapid pulse
Severe acute pancreatitis may cause dehydration and low blood pressure. The heart, lungs, or kidneys can fail. If bleeding occurs in the pancreas, shock and even death may follow.
Diagnosis
While asking about a person’s medical history and conducting a thorough physical examination, the doctor will order a blood test to assist in the diagnosis. During acute pancreatitis, the blood contains at least three times the normal amount of amylase and lipase, digestive enzymes formed in the pancreas. Changes may also occur in other body chemicals such as glucose, calcium, magnesium, sodium, potassium, and bicarbonate. After the person’s condition improves, the levels usually return to normal.
Diagnosing acute pancreatitis is often difficult because of the deep location of the pancreas. The doctor will likely order one or more of the following tests:
· Abdominal ultrasound. Sound waves are sent toward the pancreas through a handheld device that a technician glides over the abdomen. The sound waves bounce off the pancreas, gallbladder, liver, and other organs, and their echoes make electrical impulses that create a picture—called a sonogram—on a video monitor. If gallstones are causing inflammation, the sound waves will also bounce off them, showing their location.
· Computerized tomography (CT) scan. The CT scan is a noninvasive x ray that produces three-dimensional pictures of parts of the body. The person lies on a table that slides into a donut-shaped machine. The test may show gallstones and the extent of damage to the pancreas.
· Endoscopic ultrasound (EUS). After spraying a solution to numb the patient’s throat, the doctor inserts an endoscope—a thin, flexible, lighted tube—down the throat, through the stomach, and into the small intestine. The doctor turns on an ultrasound attachment to the scope that produces sound waves to create visual images of the pancreas and bile ducts.
· Magnetic resonance cholangiopancreatography (MRCP). MRCP uses magnetic resonance imaging, a noninvasive test that produces cross-section images of parts of the body. After being lightly sedated, the patient lies in a cylinder-like tube for the test. The technician injects dye into the patient’s veins that helps show the pancreas, gallbladder, and pancreatic and bile ducts.
Treatment
Treatment for acute pancreatitis requires a few days’ stay in the hospital for intravenous (IV) fluids, antibiotics, and medication to relieve pain. The person cannot eat or drink so the pancreas can rest. If vomiting occurs, a tube may be placed through the nose and into the stomach to remove fluid and air.
Unless complications arise, acute pancreatitis usually resolves in a few days. In severe cases, the person may require nasogastric feeding—a special liquid given in a long, thin tube inserted through the nose and throat and into the stomach—for several weeks while the pancreas heals.
Before leaving the hospital, the person will be advised not to smoke, drink alcoholic beverages, or eat fatty meals. In some cases, the cause of the pancreatitis is clear, but in others, more tests are needed after the person is discharged and the pancreas is healed.
Therapeutic Endoscopic Retrograde Cholangiopancreatography (ERCP) for Acute and Chronic Pancreatitis
ERCP is a specialized technique used to view the pancreas, gallbladder, and bile ducts and treat complications of acute and chronic pancreatitis—gallstones, narrowing or blockage of the pancreatic duct or bile ducts, leaks in the bile ducts, and pseudocysts—accumulations of fluid and tissue debris.
Soon after a person is admitted to the hospital with suspected narrowing of the pancreatic duct or bile ducts, a physician with specialized training performs ERCP.
After lightly sedating the patient and giving medication to numb the throat, the doctor inserts an endoscope—a long, flexible, lighted tube with a camera—through the mouth, throat, and stomach into the small intestine. The endoscope is connected to a computer and screen. The doctor guides the endoscope and injects a special dye into the pancreatic or bile ducts that helps the pancreas, gallbladder, and bile ducts appear on the screen while x rays are taken.
The following procedures can be performed using ERCP:
Sphincterotomy. Using a small wire on the endoscope, the doctor finds the muscle that surrounds the pancreatic duct or bile ducts and makes a tiny cut to enlarge the duct opening. When a pseudocyst is present, the duct is drained.
Gallstone removal. The endoscope is used to remove pancreatic or bile duct stones with a tiny basket. Gallstone removal is sometimes performed along with a sphincterotomy.
Stent placement. Using the endoscope, the doctor places a tiny piece of plastic or metal that looks like a straw in a narrowed pancreatic or bile duct to keep it open.
Balloon dilatation. Some endoscopes have a small balloon that the doctor uses to dilate, or stretch, a narrowed pancreatic or bile duct. A temporary stent may be placed for a few months to keep the duct open.
People who undergo therapeutic ERCP are at slight risk for complications, including severe pancreatitis, infection, bowel perforation, or bleeding. Complications of ERCP are more common in people with acute or recurrent pancreatitis. A patient who experiences fever, trouble swallowing, or increased throat, chest, or abdominal pain after the procedure should notify a doctor immediately.
Complications
Gallstones that cause acute pancreatitis require surgical removal of the stones and the gallbladder. If the pancreatitis is mild, gallbladder removal—called cholecystectomy—may proceed while the person is in the hospital. If the pancreatitis is severe, gallstones may be removed using therapeutic endoscopic retrograde cholangiopancreatography (ERCP)—a specialized technique used to view the pancreas, gallbladder, and bile ducts and treat complications of acute and chronic pancreatitis. Cholecystectomy is delayed for a month or more to allow for full recovery. For more information, see the Gallstones fact sheet from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK).
If an infection develops, ERCP or surgery may be needed to drain the infected area, also called an abscess. Exploratory surgery may also be necessary to find the source of any bleeding, to rule out conditions that resemble pancreatitis, or to remove severely damaged pancreatic tissue.
Pseudocysts—accumulations of fluid and tissue debris—that may develop in the pancreas can be drained using ERCP or EUS. If pseudocysts are left untreated, enzymes and toxins can enter the bloodstream and affect the heart, lungs, kidneys, or other organs.
Acute pancreatitis sometimes causes kidney failure. People with kidney failure need blood-cleansing treatments called dialysis or a kidney transplant.
In rare cases, acute pancreatitis can cause breathing problems. Hypoxia, a condition that occurs when body cells and tissues do not get enough oxygen, can develop. Doctors treat hypoxia by giving oxygen to the patient. Some people still experience lung failure—even with oxygen—and require a respirator for a while to help them breathe.
1Russo MW, Wei JT, Thiny MT, et al. Digestive and liver disease statistics, 2004. Gastroenterology. 2004;126:1448–1453.
What is chronic pancreatitis?
Chronic pancreatitis is inflammation of the pancreas that does not heal or improve—it gets worse over time and leads to permanent damage. Chronic pancreatitis, like acute pancreatitis, occurs when digestive enzymes attack the pancreas and nearby tissues, causing episodes of pain. Chronic pancreatitis often develops in people who are between the ages of 30 and 40.
The most common cause of chronic pancreatitis is many years of heavy alcohol use. The chronic form of pancreatitis can be triggered by one acute attack that damages the pancreatic duct. The damaged duct causes the pancreas to become inflamed. Scar tissue develops and the pancreas is slowly destroyed.
Other causes of chronic pancreatitis are
· hereditary disorders of the pancreas
· cystic fibrosis—the most common inherited disorder leading to chronic pancreatitis
· hypercalcemia—high levels of calcium in the blood
· hyperlipidemia or hypertriglyceridemia—high levels of blood fats
· some medicines
· certain autoimmune conditions
· unknown causes
Hereditary pancreatitis can present in a person younger than age 30, but it might not be diagnosed for several years. Episodes of abdominal pain and diarrhea lasting several days come and go over time and can progress to chronic pancreatitis. A diagnosis of hereditary pancreatitis is likely if the person has two or more family members with pancreatitis in more than one generation.
Symptoms
Most people with chronic pancreatitis experience upper abdominal pain, although some people have no pain at all. The pain may spread to the back, feel worse when eating or drinking, and become constant and disabling. In some cases, abdominal pain goes away as the condition worsens, most likely because the pancreas is no longer making digestive enzymes. Other symptoms include
· nausea
· vomiting
· weight loss
· diarrhea
· oily stools
People with chronic pancreatitis often lose weight, even when their appetite and eating habits are normal. The weight loss occurs because the body does not secrete enough pancreatic enzymes to digest food, so nutrients are not absorbed normally. Poor digestion leads to malnutrition due to excretion of fat in the stool.
Diagnosis
Chronic pancreatitis is often confused with acute pancreatitis because the symptoms are similar. As with acute pancreatitis, the doctor will conduct a thorough medical history and physical examination. Blood tests may help the doctor know if the pancreas is still making enough digestive enzymes, but sometimes these enzymes appear normal even though the person has chronic pancreatitis.
In more advanced stages of pancreatitis, when malabsorption and diabetes can occur, the doctor may order blood, urine, and stool tests to help diagnose chronic pancreatitis and monitor its progression.
After ordering x rays of the abdomen, the doctor will conduct one or more of the tests used to diagnose acute pancreatitis—abdominal ultrasound, CT scan, EUS, and MRCP.
Treatment
Treatment for chronic pancreatitis may require hospitalization for pain management, IV hydration, and nutritional support. Nasogastric feedings may be necessary for several weeks if the person continues to lose weight.
When a normal diet is resumed, the doctor may prescribe synthetic pancreatic enzymes if the pancreas does not secrete enough of its own. The enzymes should be taken with every meal to help the person digest food and regain some weight. The next step is to plan a nutritious diet that is low in fat and includes small, frequent meals. A dietitian can assist in developing a meal plan. Drinking plenty of fluids and limiting caffeinated beverages is also important.
People with chronic pancreatitis are strongly advised not to smoke or consume alcoholic beverages, even if the pancreatitis is mild or in the early stages.
Complications
People with chronic pancreatitis who continue to consume large amounts of alcohol may develop sudden bouts of severe abdominal pain.
As with acute pancreatitis, ERCP is used to identify and treat complications associated with chronic pancreatitis such as gallstones, pseudocysts, and narrowing or obstruction of the ducts. Chronic pancreatitis also can lead to calcification of the pancreas, which means the pancreatic tissue hardens from deposits of insoluble calcium salts. Surgery may be necessary to remove part of the pancreas.
In cases involving persistent pain, surgery or other procedures are sometimes recommended to block the nerves in the abdominal area that cause pain.
When pancreatic tissue is destroyed in chronic pancreatitis and the insulin-producing cells of the pancreas, called beta cells, have been damaged, diabetes may develop. People with a family history of diabetes are more likely to develop the disease. If diabetes occurs, insulin or other medicines are needed to keep blood glucose at normal levels. A health care provider works with the patient to develop a regimen of medication, diet, and frequent blood glucose monitoring.
For more information about diabetes, see the booklet Your Guide to Diabetes: Type 1 and Type 2 from the NIDDK.
How common is pancreatitis in children?
Chronic pancreatitis in children is rare. Trauma to the pancreas and hereditary pancreatitis are two known causes of childhood pancreatitis. Children with cystic fibrosis—a progressive and incurable lung disease—may be at risk of developing pancreatitis. But more often the cause of pancreatitis in children is unknown.
Hope through Research
The National Institute of Diabetes and Digestive and Kidney Diseases’ Division of Digestive Diseases and Nutrition supports basic and clinical research into gastrointestinal diseases, including the causes of pancreatitis and cell injury in the gastrointestinal tract. In addition, researchers are studying the genetics of hereditary pancreatitis and risk factors such as cystic fibrosis.
Participants in clinical trials can play a more active role in their own health care, gain access to new research treatments before they are widely available, and help others by contributing to medical research.
Pancreatic cancer
Pancreas Cancer
Classification and external resources
ICD-10
C25.
ICD-9
157.9
OMIM
260350
DiseasesDB
9510
MedlinePlus
000236
eMedicine
med/1712
MeSH
D010190
Pancreatic cancer
is a malignant neoplasm of the pancreas. It is estimated that in 2010 more than 43,000 individuals in the United States have been diagnosed with this condition, and 36,800 have died from the disease. The prognosis is poor, with fewer than 5% of those diagnosed still alive five years after diagnosis. Complete remission is still rare. About 95% of exocrine pancreatic cancers are adenocarcinomas (M8140/3). The remaining 5% include adenosquamous carcinomas, signet ring cell carcinomas, hepatoid carcinomas, colloid carcinomas, undifferentiated carcinomas, and undifferentiated carcinomas with osteoclast-like giant cells. Exocrine pancreatic tumors are far more common than pancreatic endocrine tumors, which make up about 1% of total cases.
Signs and symptomsPresentation
Pancreatic cancer is sometimes called a "silent killer" because early pancreatic cancer often does not cause symptoms, and the later symptoms are usually nonspecific and varied. Therefore, pancreatic cancer is often not diagnosed until it is advanced. Common symptoms include:
· Pain in the upper abdomen that typically radiates to the back (seen in carcinoma of the body or tail of the pancreas)
· Loss of appetite and/or nausea and vomiting
· Significant weight loss
· Painless jaundice (yellow tint to whites of eyes and/or yellowish skin in serious cases, possibly in combination with darkened urine) when a cancer of the head of the pancreas (about 60% of cases) obstructs the common bile duct as it runs through the pancreas. This may also cause pale-colored stool and steatorrhea. The jaundice may be associated with itching as the salt from excess bile can cause skin irritation.
· Trousseau sign, in which blood clots form spontaneously in the portal blood vessels, the deep veins of the extremities, or the superficial veins anywhere on the body, is sometimes associated with pancreatic cancer.
· Diabetes mellitus, or elevated blood sugar levels. Many patients with pancreatic cancer develop diabetes months to even years before they are diagnosed with pancreatic cancer, suggesting new onset diabetes in an elderly individual may be an early warning sign of pancreatic cancer.
· Clinical depression has been reported in association with pancreatic cancer, sometimes presenting before the cancer is diagnosed. However, the mechanism for this association is not known.
Causes
Risk factors for pancreatic cancer include:
· Age (particularly over 60)
· Male sex (likelihood up to 30% greater than females)
· Smoking. Cigarette smoking has a risk ratio of 1.74 with regard to pancreatic cancer; a decade of nonsmoking after heavy smoking is associated with a risk ratio of 1.2.
· Diets low in vegetables and fruits
· Diets high in red meat
· Diets high in sugar-sweetened drinks (soft drinks) - risk ratio 1.87. In particular, the common soft drink sweetener fructose has been linked to growth of pancreatic cancer cells.
· Obesity
· Diabetes mellitus is both risk factor for pancreatic cancer, and, as noted earlier, new onset diabetes can be an early sign of the disease.
· Chronic pancreatitis has been linked, but is not known to be causal. The risk of pancreatic cancer in individuals with familial pancreatitis is particularly high.
· Helicobacter pylori infection
· Family history, 5–10% of pancreatic cancer patients have a family history of pancreatic cancer. The genes responsible for most of this clustering in families have yet to be identified. Pancreatic cancer has been associated with the following syndromes; autosomal recessive ataxia-telangiectasia and autosomal dominantly inherited mutations in the BRCA2 gene and PALB2 gene, Peutz-Jeghers syndrome due to mutations in the STK11 tumor suppressor gene, hereditary non-polyposis colon cancer (Lynch syndrome), familial adenomatous polyposis, and the familial atypical multiple mole melanoma-pancreatic cancer syndrome (FAMMM-PC) due to mutations in the CDKN2A tumor suppressor gene.[2][16]
· Gingivitis or periodontal disease[17]
Australia and Canada, members of the International Cancer Genome Consortium, are leading efforts to map pancreatic cancer's complete genome.
Alcohol
It is controversial whether alcohol consumption is a risk factor for pancreatic cancer. Drinking alcohol excessively is a major cause of chronic pancreatitis, which in turn predisposes to pancreatic cancer. However, chronic pancreatitis associated with alcohol consumption does not increase risk of pancreatic cancer as much as other types of chronic pancreatitis. Overall, the association is consistently weak and the majority of studies have found no association.
Some studies suggest a relationship, with risk increasing with increasing amount of alcohol intake. Risk is greatest in heavy drinkers mostly on the order of four or more drinks per day. But there appears to be no increased risk for people consuming up to 30g of alcohol a day, so most of the U.S. consumes alcohol at a level that "is probably not a risk factor for pancreatic cancer".
Several studies caution that their findings could be due to confounding factors. Even if a link exists, it "could be due to the contents of some alcoholic beverages"other than the alcohol itself. One Dutch study even found that drinkers of white wine had lower risk.
A pooled analysis concluded, "Our findings are consistent with a modest increase in risk of pancreatic cancer with consumption of 30 or more grams of alcohol per day".
Diagnosis
Axial CT image with i.v. contrast. Macrocystic adenocarcinoma of the pancreatic head.
Most patients with pancreatic cancer experience pain, weight loss, or jaundice.
Pain is present in 80% to 85% of patients with locally advanced or advanced metastatic disease. The pain is usually felt in the upper abdomen as a dull ache that radiates straight through to the back. It may be intermittent and made worse by eating. Weight loss can be profound; it can be associated with anorexia, early satiety, diarrhea, or steatorrhea. Jaundice is often accompanied by pruritus and dark urine. Painful jaundice is present in approximately one-half of patients with locally unresectable disease, while painless jaundice is present in approximately one-half of patients with a potentially resectable and curable lesion.
The initial presentation varies according to location of the cancer. Malignancies in the pancreatic body or tail usually present with pain and weight loss, while those in the head of the gland typically present with steatorrhea, weight loss, and jaundice. The recent onset of atypical diabetes mellitus, a history of recent but unexplained thrombophlebitis (Trousseau sign), or a previous attack of pancreatitis are sometimes noted. Courvoisier sign defines the presence of jaundice and a painlessly distended gallbladder as strongly indicative of pancreatic cancer, and may be used to distinguish pancreatic cancer from gallstones. Tiredness, irritability and difficulty eating because of pain also exist. Pancreatic cancer is often discovered during the course of the evaluation of aforementioned symptoms.
Liver function tests can show a combination of results indicative of bile duct obstruction (raised conjugated bilirubin, γ-glutamyl transpeptidase and alkaline phosphatase levels). CA19-9 (carbohydrate antigen 19.9) is a tumor marker that is frequently elevated in pancreatic cancer. However, it lacks sensitivity and specificity. When a cutoff above 37 U/mL is used, this marker has a sensitivity of 77% and specificity of 87% in discerning benign from malignant disease. CA 19-9 might be normal early in the course, and could be elevated because of benign causes of biliary obstruction. Imaging studies, such as computed tomography (CT scan) and endoscopic ultrasound (EUS) can be used to identify the location and form of the cancer.
Pathology
Micrograph of pancreatic ductal adenocarinoma (the most common type of pancreatic cancer). H&E stain.
The definitive diagnosis is made by a endoscopic needle biopsy or surgical excision of the radiologically suspicious tissue. Endoscopic ultrasound is often used to visually guide the needle biopsy procedure.
The most common form of pancreatic cancer (ductal adenocarcinoma) is typically characterized by moderately to poorly differentiated glandular structures on microscopic examination. Pancreatic cancer has an immunohistochemical profile that is similar to hepatobiliary cancers (e.g. cholangiocarcinoma) and some stomach cancers; thus, it may not always be possible to be certain that a tumour found in the pancreas arose from it.
Micrographs of normal pancreas, pancreatic intraepithelial neoplasia (precursors to pancreatic carcinoma) and pancreatic carcinoma. H&E stain.
Like colorectal carcinoma, pancreatic carcinoma is thought to arise, typically, from nonmalignant precursor lesions; i.e., it is thought to follow a preneoplasm-neoplasm-carcinoma sequence. In the prototypical colorectal cancer, the lesion has arisen from a tubular adenoma, which developed from colorectal mucosa with an adenomatosis polyposis coli gene mutation. In pancreatic adenocarcinoma, the preneoplastic lesion is pancreatic intraepithelial neoplasia 1a (PanIN1a) and pancreatic intraepithelial neoplasia 1b (PanIN1b) the neoplastic lesions pancreatic intraepithelial neoplasia 2 (PanIN2) and pancreatic intraepithelial neoplasia 3 (PanIN3).
Screening
Patients with high risk of pancreatic cancer (hereditary) can be followed, however the method to do this is continuously debated in scientific circles. Several very small underpowered studies have shown promising results in new biomarkers, but so far nothing has been tested in a larger scale. Such studies should always be validated in large cohorts before being introduced to the public, even if they are performed at MD. Anderson or other high-volume cancer treatment institutions.
Prevention
According to the American Cancer Society, there are no established guidelines for preventing pancreatic cancer, although cigarette smoking has been reported as responsible for 20–30% of pancreatic cancers.
The ACS recommends keeping a healthy weight, and increasing consumption of fruits, vegetables, and whole grains, while decreasing red meat intake, although there is no consistent evidence this will prevent or reduce pancreatic cancer specifically. In 2006, a large prospective cohort study of over 80,000 subjects failed to prove a definite association. The evidence in support of this lies mostly in small case-control studies.
In September 2006, a long-term study concluded taking vitamin D can substantially reduce the risk of pancreatic cancer (as well as other cancers) by up to 50%, but this study needs to evaluate fully the risks, costs and potential benefits of taking vitamin D.
Several studies, including one published on 1 June 2007, indicate B vitamins, such as B12, B6, and folate, can reduce the risk of pancreatic cancer when consumed in food, but not when ingested in vitamin tablet form.[45][46]
TreatmentSurgery
Treatment of pancreatic cancer depends on the stage of the cancer. The Whipple procedure is the most common surgical treatment for cancers involving the head of the pancreas. This procedure involves removing the pancreatic head and the curve of the duodenum together (pancreato-duodenectomy), making a bypass for food from stomach to jejunum (gastro-jejunostomy) and attaching a loop of jejunum to the cystic duct to drain bile (cholecysto-jejunostomy). It can be performed only if the patient is likely to survive major surgery and if the cancer is localized without invading local structures or metastasizing. It can, therefore, be performed in only the minority of cases.
Cancers of the tail of the pancreas can be resected using a procedure known as a distal pancreatectomy. Recently, localized cancers of the pancreas have been resected using minimally invasive (laparoscopic) approaches.
After surgery, adjuvant chemotherapy with gemcitabine has been shown in several large randomized studies to significantly increase the 5-year survival (from approximately 10 to 20%), and should be offered if the patient is fit after surgery (Oettle et al. JAMA 2007, Neoptolemos et al. NEJM 2004, Oettle et al. ASCO proc 2007). Addition of radiation therapy is a hotly debated topic, with groups in the US often favoring the use of adjuvant radiation therapy, while groups in Europe do not, due to the lack of any large randomized studies to show any survival benefit of this strategy.
Surgery can be performed for palliation, if the malignancy is invading or compressing the duodenum or colon. In that case, bypass surgery might overcome the obstruction and improve quality of life, but it is not intended as a cure.
Chemotherapy
In patients not suitable for resection with curative intent, palliative chemotherapy may be used to improve quality of life and gain a modest survival benefit. Gemcitabine was approved by the United States Food and Drug Administration in 1998, after a clinical trial reported improvements in quality of life and a 5-week improvement in median survival duration in patients with advanced pancreatic cancer. This marked the first FDA approval of a chemotherapy drug primarily for a nonsurvival clinical trial endpoint. Gemcitabine is administered intravenously on a weekly basis.
2005: On the basis of a Canadian-led Phase III randomised controlled trial involving 569 patients with advanced pancreatic cancer, the US FDA in 2005 licensed the use of erlotinib (Tarceva) in combination with gemcitabine as a palliative regimen for pancreatic cancer. This trial compared the action of gemcitabine/erlotinib to gemcitabine/placebo, and demonstrated improved survival rates, improved tumor response and improved progression-free survival rates (Moore et al. JCO 2005). The survival improvement with the combination is on the order of less than four weeks, leading some cancer experts to question the incremental value of adding erlotinib to gemcitabine treatment. New trials are now investigating the effect of the above combination in the adjuvant (post surgery) and neoadjuvant (pre-surgery) setting.
Addition of oxaliplatin to Gemcitabine (Gem/Ox) was shown to confer benefit in small trials, but is not yet standard therapy.
Prognosis
Patients diagnosed with pancreatic cancer typically have a poor prognosis, partly because the cancer usually causes no symptoms early on, leading to locally advanced or metastatic disease at time of diagnosis. Median survival from diagnosis is around 3 to 6 months; 5-year survival is less than 5%. With 37,170 cases diagnosed in the United States in 2007, and 33,700 deaths, pancreatic cancer has one of the highest fatality rates of all cancers, and is the fourth-highest cancer killer in the United States among both men and women. Although it accounts for only 2.5% of new cases, pancreatic cancer is responsible for 6% of cancer deaths each year.
Pancreatic cancer may occasionally result in diabetes. Insulin production is hampered, and it has been suggested the cancer can also prompt the onset of diabetes and vice versa.