
Tratamiento con estatinas y antitrombotico Dr Briguori
53
Statin and antithrombotic therapy: Their role in risk reduction in percutaneous coronary intervention Carlo Briguori, MD, PhD Laboratoy of Interventional Cardiology Clinica Mediterranea, Naples - Italy
-
Upload
tuendocrinologo -
Category
Documents
-
view
217 -
download
0
description
Tratamiento con estatinas y antitrombotico Dr Briguori
Transcript of Tratamiento con estatinas y antitrombotico Dr Briguori

Statin and antithrombotic therapy: Their role in risk reduction in
percutaneous coronary intervention
Carlo Briguori, MD, PhD Laboratoy of Interventional Cardiology
Clinica Mediterranea, Naples - Italy

• Periprocedural myocardial infarction is a frequent and prognostically important complication of PCI 1 .
• Serum CK-MB after an uncomplicated PCI is elevated in 1 to 38% patients 1-4
• A CK-MB elevation >3X ULN (which is considered to represent an infarction large enough to be associated with short-term complications) occurs in 7-18%
Background
1 Hermann J. Eur Heart J 2005; 25: 2493 2 Testa L. et al. . QJM 2009;102:2945 3 Stone GW et al. Circulation 2001;104:642 4 Califf RM et al. J Am Coll Cardiol 1998; 31: 241
How to Prevent Periprocedural MI?

Types of Peri-procedural Myocardial Ischemic Injury
Hermann J. Eur Heart J 2005; 25: 2493
• Antiplatelet therapy:
– Glycoprotein IIb IIIa inhibitors 1
– Thienopyridine 2-4
• Beta-blockers 5
• Statins 6-7
Pharmacological approaches to prevent periprocedural MI
1 Roffi M. et al. Eur Heart J 2002 Sep;23(18):1441-8 2 Steinhubl SR J Am Coll Cardiol. 1998;32:1366-1370. 3 Patti G et al. Circulation 2005 Apr 26;111(16):2099-106 4 Mahoney EM et al. Circulation. 2010 Jan 5;121(1):71-9 5 Erbel SG et al. Circulation. 2001;104:2685-2688 6 Pasceri V. et al. . Circulation 2004;110:674-8 7 Briguori C et al. Eur Heart J 2004;25:1822-8
• The available data suggest that statin prevent periprocedural MI 1-2
Statin & periprocedural MI
1 Pasceri V. et al. Circulation 2004;110:674-8 2 Briguori C et al. Eur Heart J 2004;25:1822-8

The first ARMYDA trial (N=153 pts) has demonstrated that a 7-day
pretreatment with atorvastatin (40 mg/day) is associated with 81% risk
reduction of peri-procedural myocardial infarction in patients with stable
angina undergoing elective PCI
0
10
20
30
Placebo Atorvastatin
P=0.025
Primary end point: Incidence of MI
18
5
Pasceri V, Patti G, Di Sciascio G, et al. Circulation 2004
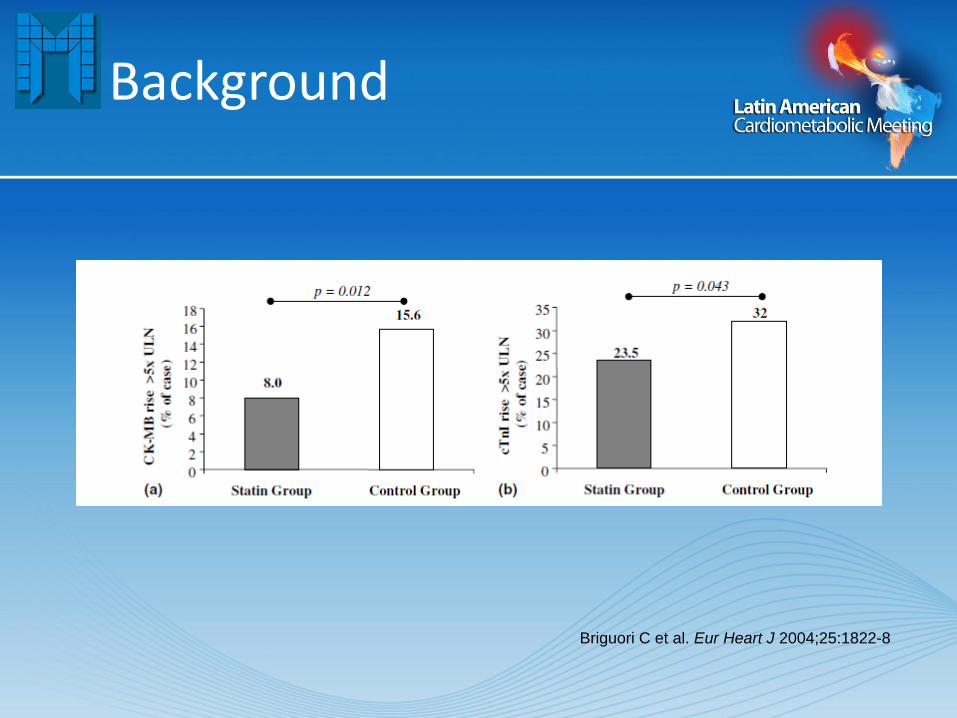
Background
Briguori C et al. Eur Heart J 2004;25:1822-8
• Previous studies suggest that atorvastatin administration should be started at least 3 - 7 days before the procedure1-2
• In the ARMYDA trial:
– Atorvastatin 40 mg started 7 days before PCI
• This may imply the need to postpone the PCI in all statin naïve patients.
When to Start Atorvastatin to Prevent Periprocedural MI?
1 Pasceri V. et al. Circulation 2004;110:674-8 2 Briguori C et al. Eur Heart J 2004;25:1822-8
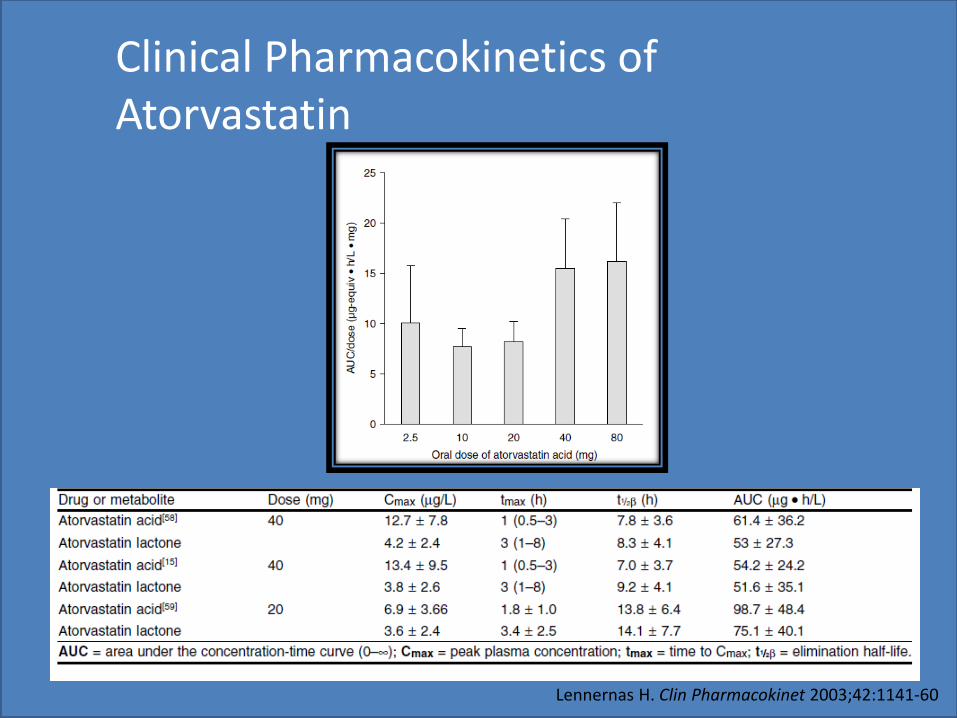
Clinical Pharmacokinetics of Atorvastatin
Lennernas H. Clin Pharmacokinet 2003;42:1141-60

• To assess whether a single, high (80 mg), loading (within 24 hours) dose of atorvastatin is effective in preventing elevation of biomarkers of MI following elective coronary stent implantation.
NAPLES II
Briguori C et al. J Am Coll Cardiol 2009;54:2157-63
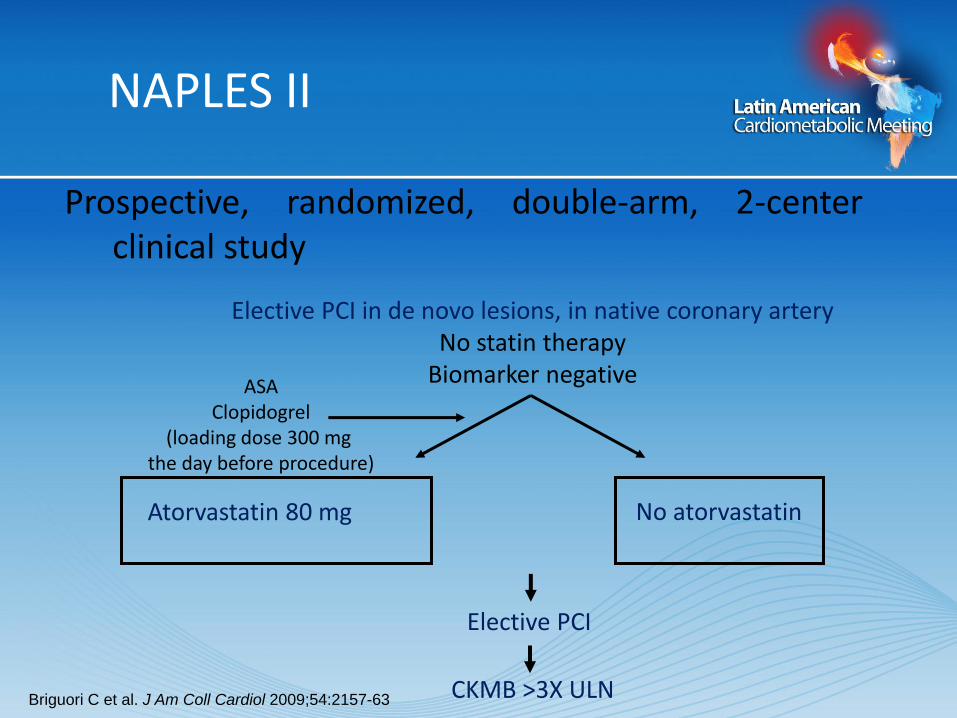
NAPLES II
Prospective, randomized, double-arm, 2-center clinical study
Elective PCI in de novo lesions, in native coronary artery
No statin therapy Biomarker negative
Atorvastatin 80 mg No atorvastatin
ASA Clopidogrel
(loading dose 300 mg the day before procedure)
Elective PCI
CKMB >3X ULN Briguori C et al. J Am Coll Cardiol 2009;54:2157-63

• Hypothesis: • Reduction in the primary endpoint from 15% in the Control group
to 8% in the Atorvastatin group1-2
• Sample size: – A total of 650 patients (325 each group) will be necessary to gave the
study 80% power and a significance level <0.05
Sample size
1 Pasceri V. et al. . Circulation 2004;110:674-8 2 Briguori C et al. Eur Heart J 2004;25:1822-8

Inclusion criteria
Age 18 y
De novo lesion in a native coronary artery
Elective PCI
Normal cardiac biomarkers
No statin therapy
Briguori C et al. J Am Coll Cardiol 2009;54:2157-63
Exclusion criteria
• Primary or rescue PCI
ACS with elevated cardiac markers
Pregnancy
Restenotic lesion
SVG or LIMA treatment
Active statin therapy
Briguori C et al. J Am Coll Cardiol 2009;54:2157-63
–Periprocedural Myocardial Infarction = CKMB 3X ULN
Definitions
Thygesen K et al. Eur Heart J 2007;28:2525-38.8

338 patients included
Patients assessed for eligibility (n=1385)
Excluded (n=31)
9 withdrew consent 28 did not meet the inclusion criteria
1348 patients randomized
676 allocated to Atorvastatin group 676 received the allocated treatment
672 allocated to Control group 672 received the allocated treatment
330 patients included
338 excluded because: 155 had coronary angiography alone and not PCI 98 had PCI for ISR and/or on a bypass vessel 80 were referred for elective CABG 5 were lost at follow-up
342 excluded because: 174 had coronary angiography alone and not PCI 91 had PCI for ISR and/or on a bypass vessel 71 were referred for eventual CABG 6 were lost at follow-up
338 patients included 330 patients included 338 patients included
Briguori C et al. J Am Coll Cardiol 2009;54:2157-63

Clinical Characteristics Atorvastatin
Group
(N=338)
Control Group
(N=330)
Age, yrs (mean SD) 64 9 65 10
Male, % 266 (78.7%) 263 (79.7%)
BMI (kg/m2) 27.8 3.8 27.4 3.5
Symptoms Asymptomatic Stable angina Unstable angina
45 (13.3%) 285 (84.3%
8 (2.4%)
34 (10.3%)
288 (87.3%) 8 (2.4%)
Family history for CAD 101 (30%) 112 (34%) Diabetes mellitus 130 (38.6%) 121 (36.8%) Hypertension, % 131 (78%) 125 (74.9%) Current smoker, % 79 (24%) 66 (20%) Prior MI, % 113 (33.4%) 97 (29.4%) Prior PCI*, % 41 (12.1%) 31 (9.4%) Prior CABG, % 24 (7.1%) 27 (8.1%) LVEF, % (mean SD) 55.7 9.5 55.5 9.9 -blockers 130 (38.5%) 129 (39.1%)
* Percutaneous intervention performed in a different vessel and/or lesion.
Briguori C et al. J Am
Coll Cardiol
2009;54:2157-63
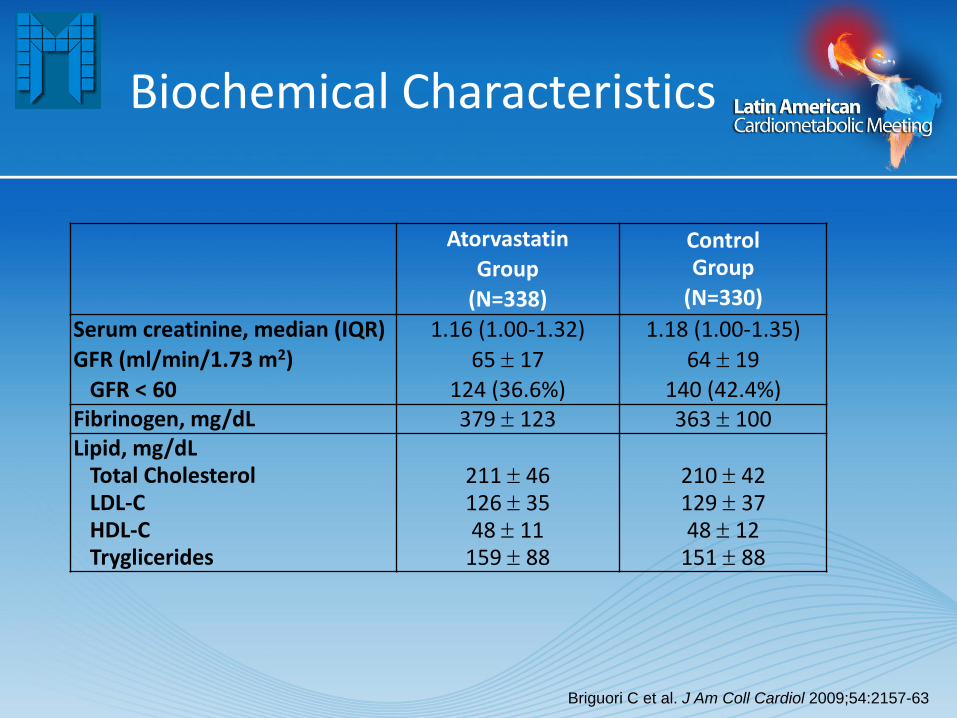
Biochemical Characteristics
Atorvastatin
Group
(N=338)
Control Group
(N=330)
Serum creatinine, median (IQR)
GFR (ml/min/1.73 m2)
GFR < 60
1.16 (1.00-1.32)
65 17 124 (36.6%)
1.18 (1.00-1.35)
64 19 140 (42.4%)
Fibrinogen, mg/dL 379 123 363 100 Lipid, mg/dL Total Cholesterol LDL-C HDL-C Tryglicerides
211 46 126 35 48 11
159 88
210 42 129 37 48 12
151 88
Briguori C et al. J Am Coll Cardiol 2009;54:2157-63

Rate of high CRP
0
10
20
30
40
50
Atorvastatin group (n= 338)
Control group (n = 330)
p = 0.31
25.4
29.4
%
Briguori C et al. J Am Coll Cardiol 2009;54:2157-63
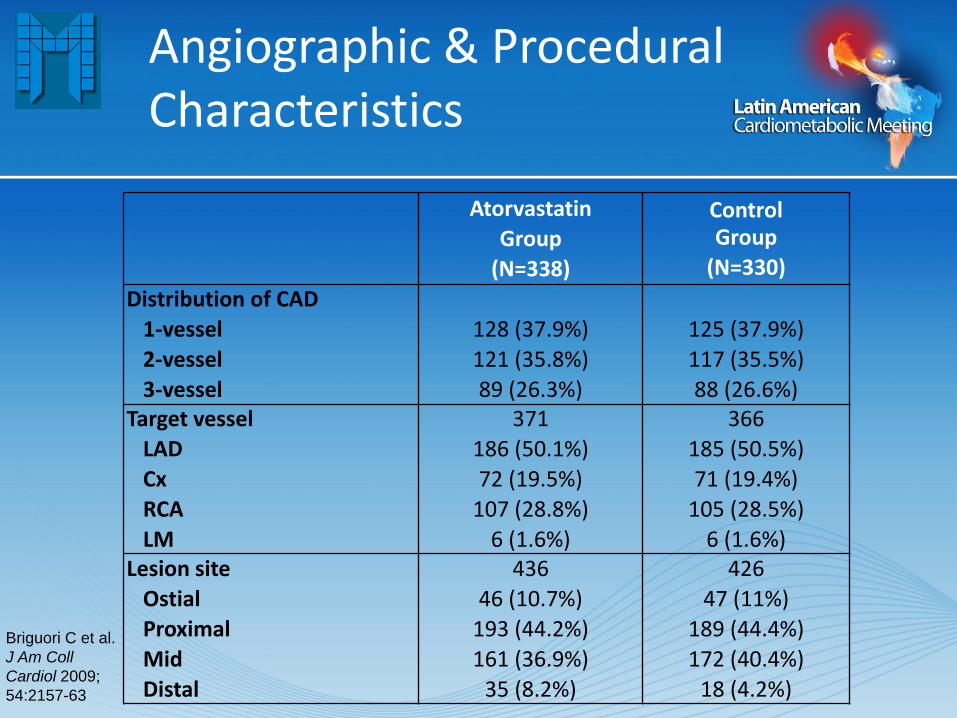
Angiographic & Procedural Characteristics
Atorvastatin
Group
(N=338)
Control Group
(N=330)
Distribution of CAD
1-vessel
2-vessel
3-vessel
128 (37.9%)
121 (35.8%)
89 (26.3%)
125 (37.9%)
117 (35.5%)
88 (26.6%) Target vessel
LAD
Cx
RCA
LM
371
186 (50.1%)
72 (19.5%)
107 (28.8%)
6 (1.6%)
366
185 (50.5%)
71 (19.4%)
105 (28.5%)
6 (1.6%) Lesion site
Ostial
Proximal
Mid
Distal
436
46 (10.7%)
193 (44.2%)
161 (36.9%)
35 (8.2%)
426
47 (11%)
189 (44.4%)
172 (40.4%)
18 (4.2%)
Briguori C et al.
J Am Coll
Cardiol 2009;
54:2157-63
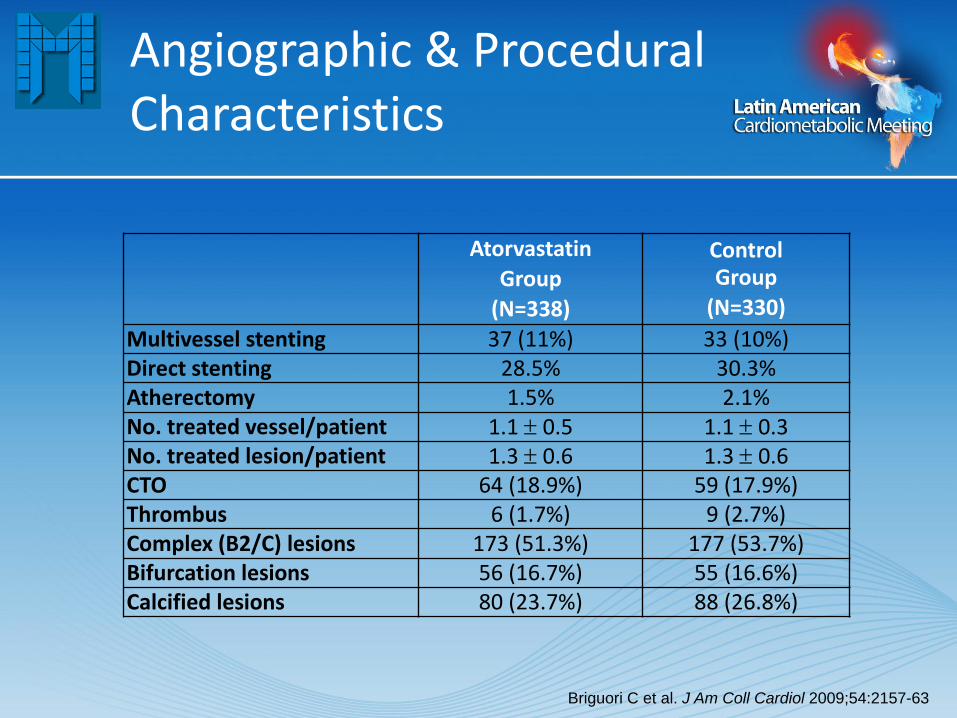
Angiographic & Procedural Characteristics
Atorvastatin
Group
(N=338)
Control Group
(N=330)
Multivessel stenting 37 (11%) 33 (10%) Direct stenting 28.5% 30.3% Atherectomy 1.5% 2.1% No. treated vessel/patient 1.1 0.5 1.1 0.3 No. treated lesion/patient 1.3 0.6 1.3 0.6 CTO 64 (18.9%) 59 (17.9%) Thrombus 6 (1.7%) 9 (2.7%) Complex (B2/C) lesions 173 (51.3%) 177 (53.7%) Bifurcation lesions 56 (16.7%) 55 (16.6%) Calcified lesions 80 (23.7%) 88 (26.8%)
Briguori C et al. J Am Coll Cardiol 2009;54:2157-63

Atorvastatin
Group
(N=338)
Control Group
(N=330) Preprocedural QCA
RVD, mm
MLD, mm
DS, %
Lesion length, mm
3.16 0.62
0.51 0.44
85 12
18 10
3.23 0.59
0.51 0.40
84 13
19 8 Postprocedural QCA
RVD, mm
MLD, mm
DS, %
3.36 0.61
3.34 0.61
2 6
3.41 0.58
3.37 0.60
2 3 Stent length, mm 30 16 30 16 Max inflation pressure, atm 15 4 15 4 TIMI flow grade pre
0/1
2/3
54 (16%)
284 (84%)
54 (16.5%)
276 (83.5%) TIMI flow grade post
0/1
2/3
1 (0.3%)
337 (99.7%)
0
330 (100%) BA ratio 1.05 0.12 1.03 0.09
Briguori C et al. J Am Coll Cardiol 2009;54:2157-63

Angiographic Complications
Atorvastatin
Group
(N=338)
Control Group
(N=330) P
Major dissection 1 (0.59%) 3 (0.90%) 0.68 Abrupt closure 1 (0.29%) 0 0.48 Slow/No reflow 2 (0.59%) 8 (2.40%) 0.06 Thrombus formation 2 (0.59%) 0 0.50 Side branch closure/compromise 5 (1.48%) 7 (2.12%) 0.57 Distal embolization 2 (0.59%) 2 (0.60%) 1.00 Perforation 2 (0.59%) 2 (0.60%) 1.00 Any of the above 16 (4.7%) 22 (6.6%) 0.31
Briguori C et al. J Am Coll Cardiol 2009;54:2157-63
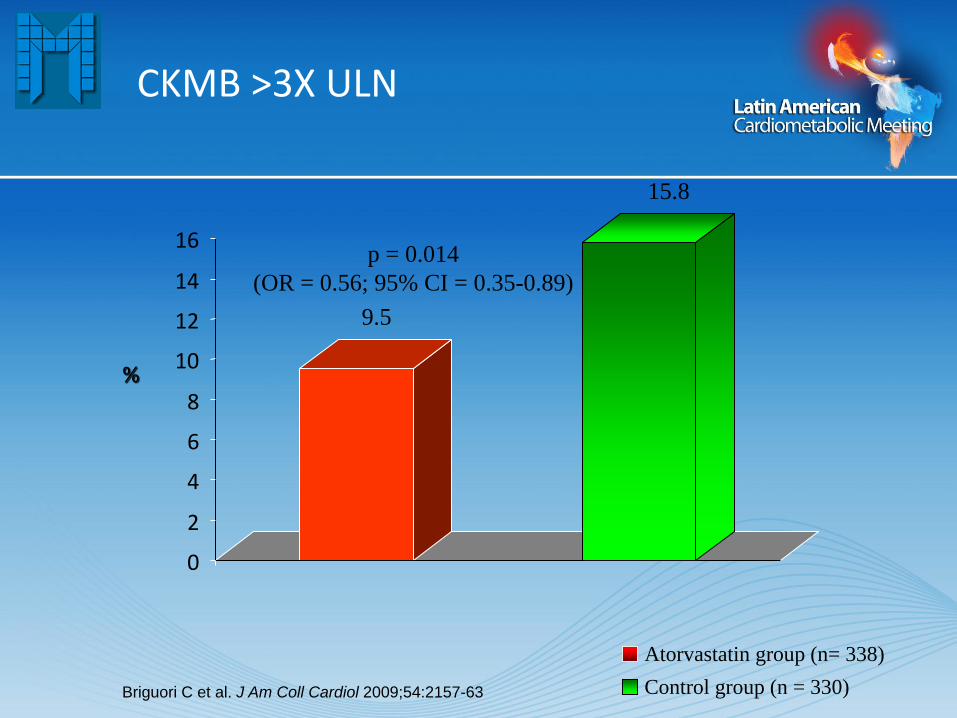
CKMB >3X ULN
0
2
4
6
8
10
12
14
16
Atorvastatin group (n= 338)
Control group (n = 330)
p = 0.014
(OR = 0.56; 95% CI = 0.35-0.89)
%
9.5
15.8
Briguori C et al. J Am Coll Cardiol 2009;54:2157-63
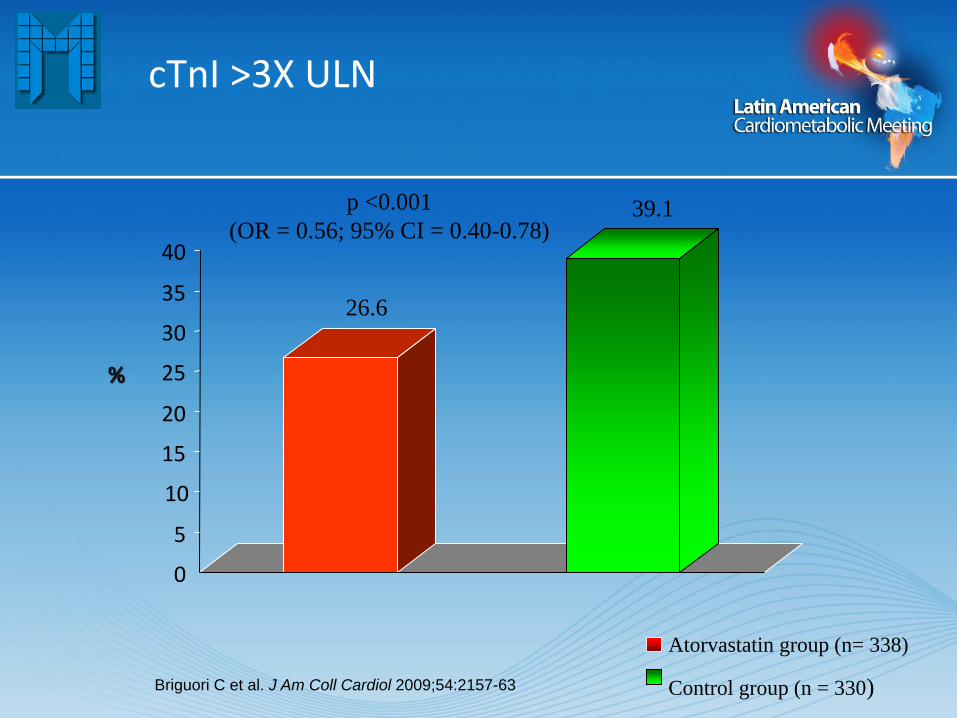
cTnI >3X ULN
0
5
10
15
20
25
30
35
40
26.6
39.1
Atorvastatin group (n= 338)
Control group (n = 330)
p <0.001
(OR = 0.56; 95% CI = 0.40-0.78)
%
Briguori C et al. J Am Coll Cardiol 2009;54:2157-63

28/252
35/233
11.1
15
4/86
16/97
4.6
16.5
0
2
4
6
8
10
12
14
16
18
Atorvastatin group (n= 338)
Control group (n = 330)
p = 0.18 p = 0.016
CKMB 3X ULN & CRP
Normal CRP High CRP
%
Briguori C et al. J Am Coll Cardiol 2009;54:2157-63
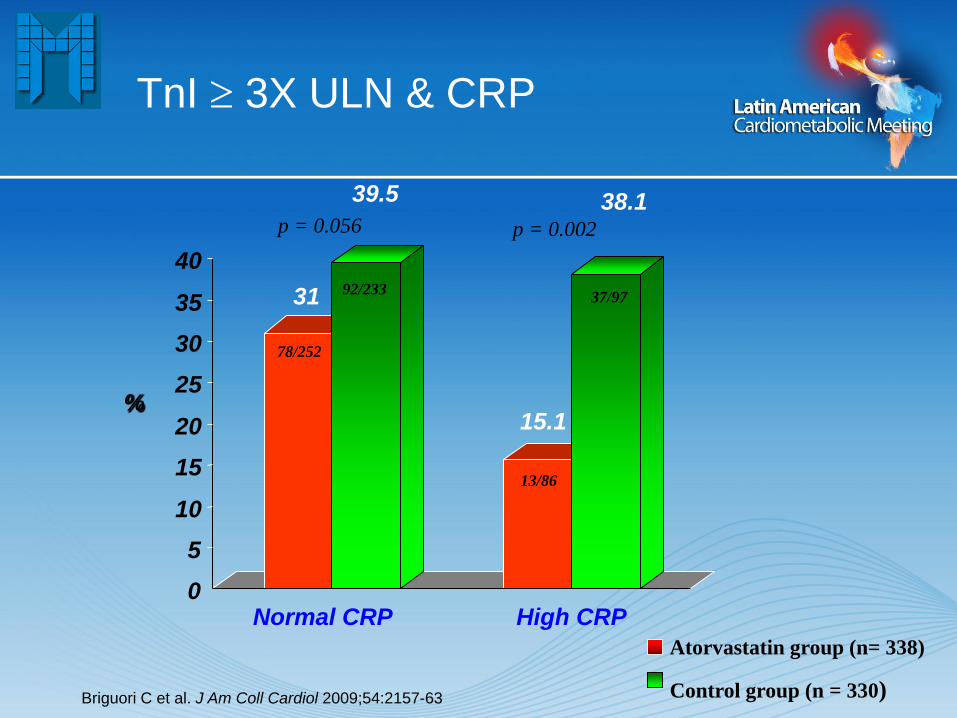
31
39.5
15.1
38.1
0
5
10
15
20
25
30
35
40
Normal CRP High CRP
Atorvastatin group (n= 338)
Control group (n = 330)
p = 0.056 p = 0.002
TnI 3X ULN & CRP
%
78/252
92/233
13/86
37/97
Briguori C et al. J Am Coll Cardiol 2009;54:2157-63
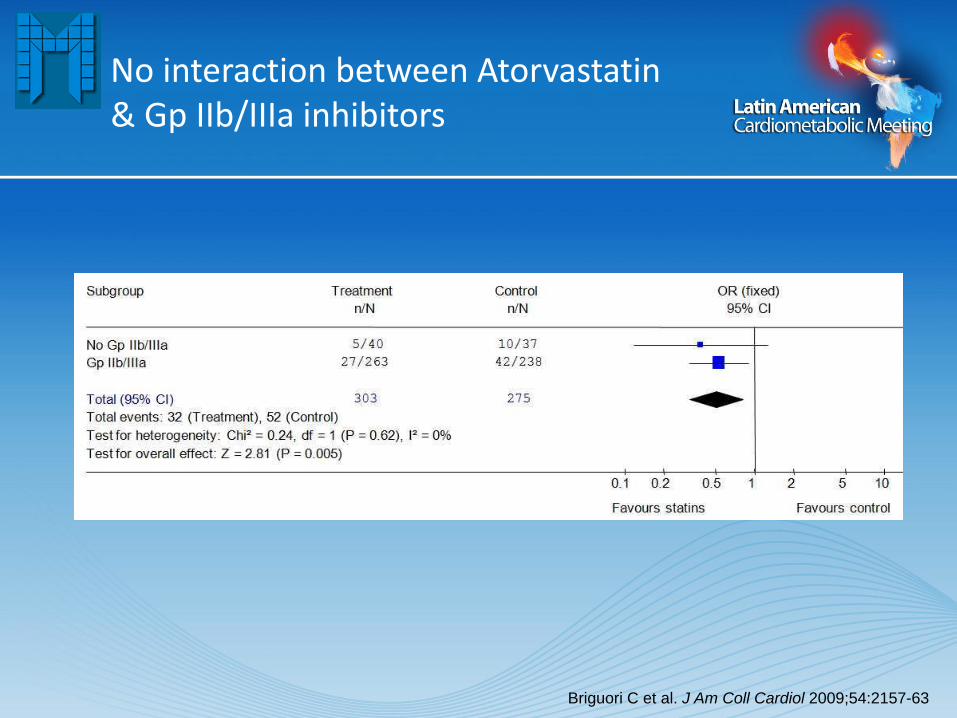
No interaction between Atorvastatin & Gp IIb/IIIa inhibitors
Briguori C et al. J Am Coll Cardiol 2009;54:2157-63

ARMYDA-RECAPTURE trial: Study design
793 Patients
with
stable angina
or NSTE-ACS
undergoing
coronary
angiography
Ran
dom
izati
on
(N
=420)
Atorvastatin reload:
80 mg
12 hrs before
angio;
further 40 mg
2 hrs before
N=210
Coronary
angiography
Placebo
12 hrs before
angio; further
dose 2 hrs
before
N=210
Primary end
point:
30-day
occurrence of
cardiac death,
MI, TVR
1st blood sample
(before PCI)
CK-MB, Troponin-I, HS-CRP
2nd and 3rd
blood samples
(8 and 24 hours
after PCI)
30 days
373 patients excluded for:
- 243 no chronic statin therapy (31%)
- 38 emergency angiography
- 82 ejection fraction <30%
- 10 severe renal failure
PCI
atorvastatin
N=177
PCI
placebo
N=175
68 patients excluded for indication to:
- medical therapy (N=30)
- bypass surgery (N=38)
N=352
Di Sciascio G, Patti G et al – J Am Coll Cardiol 2009; 54:558

Individual and Combined Outcome Measures
of the Primary Endpoint at 30 days
8.6 9.1
P=0.045
ARMYDA-RECAPTURE: RESULTS
%
Composite
Primary End Point
48% RRR at MV analysis
3.4
0
3
6
9
12
Cardiac
death
MI TVR MACE
Atorvastatin
Placebo
0.5 0.5
3.4
Di Sciascio G, Patti G et al – J Am Coll Cardiol 2009; 54:558
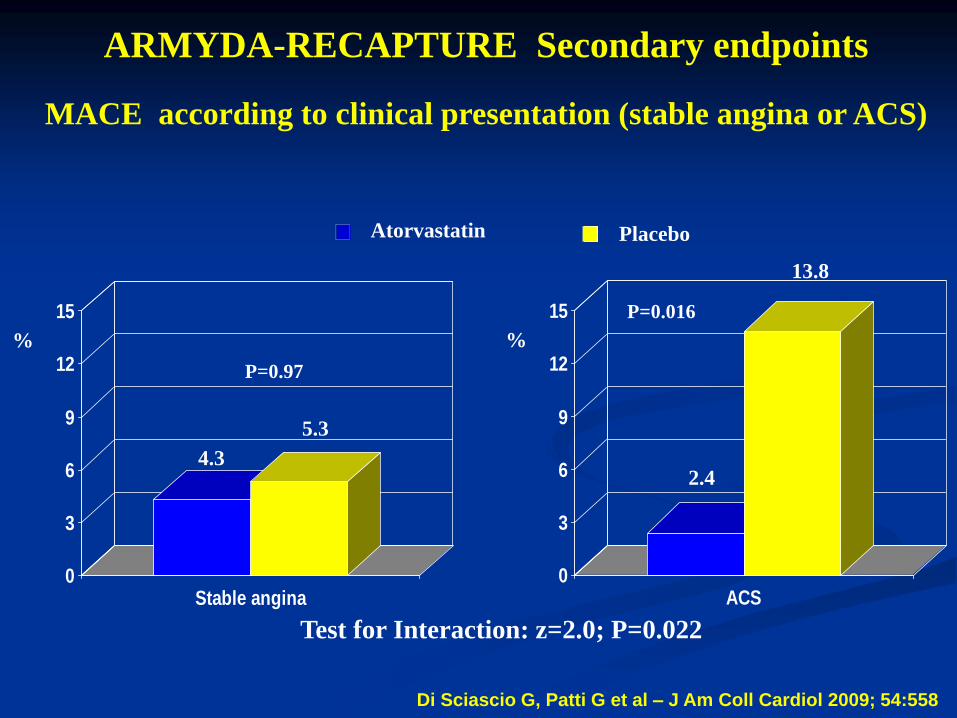
0
3
6
9
12
15
Stable angina
%
0
3
6
9
12
15
ACS
%
4.3
5.3
2.4
13.8
P=0.97
P=0.016
ARMYDA-RECAPTURE Secondary endpoints
MACE according to clinical presentation (stable angina or ACS)
Test for Interaction: z=2.0; P=0.022
Atorvastatin Placebo
Di Sciascio G, Patti G et al – J Am Coll Cardiol 2009; 54:558

Potential Mechanisms
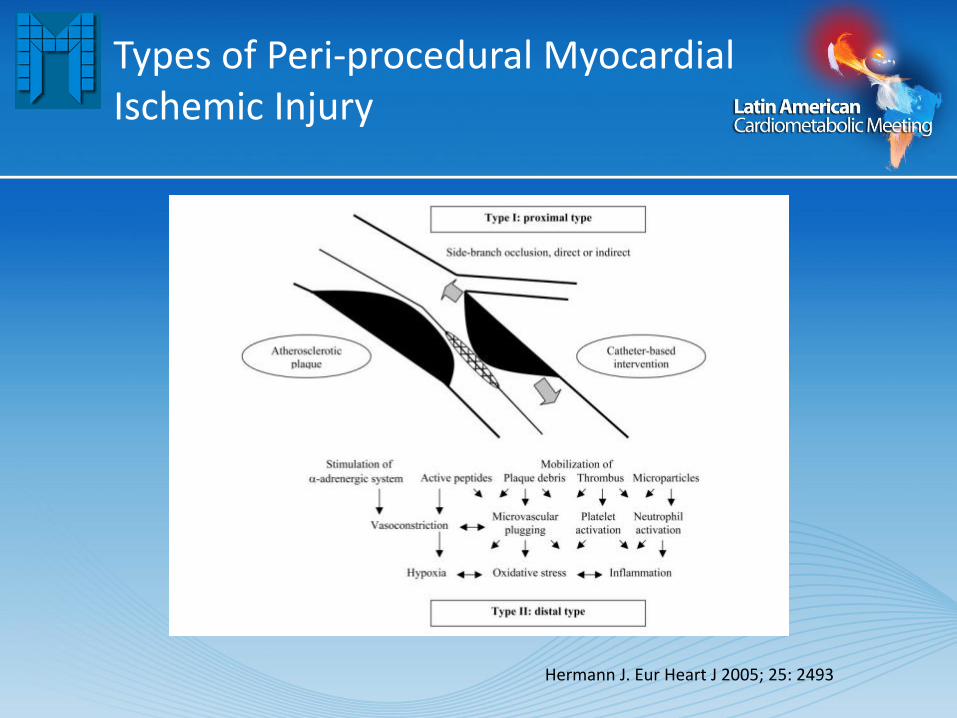
Types of Peri-procedural Myocardial Ischemic Injury
Hermann J. Eur Heart J 2005; 25: 2493
Anti-inflammatory Effects

Anti-inflammatory Effects
Morales-Villegas E. et al. International J Hypertension 2011

Statins Loading & CRP
Ostadal P. et al. Mol Cell Biochem 2003;246:45-50
Antiplatelet Effects

0,0%
5,0%
10,0%
15,0%
20,0%
0 1 2 3 4
Marcucci et al
Price et al
Patti et al
N=683
N=380
N=160
Increasing Risk With Greater Residual Reactivity
Event Rates In Prospective PCI Studies Stratified By PRU Quartile
PRU Quartile Price MJ et al. Circulation 2009; 119:2625-32
Even
t ra
te
The VerifyNow System •The first easy, rapid and proven system for measuring individual response to every major antiplatelet medication
– Aspirin – P2Y12 inhibitors (e.g. clopidogrel, prasugrel and ticlopidine) – GP IIb/IIIa inhibitors (e.g. ReoPro® and Integrilin®)
•System Consists of: – Light-Detection Instrument – Single use Test Devices – Electronic Quality Controls – Wet Quality Controls

Mechanism Of Action •Platelet response is measured as a function of an increase in light transmission through whole blood as platelets are activated by various agonists
If there is low residual platelet reactivity, there is decreased light that is transmitted and detected.
If there is high residual platelet reactivity, there is increased light that is transmitted and detected.
•
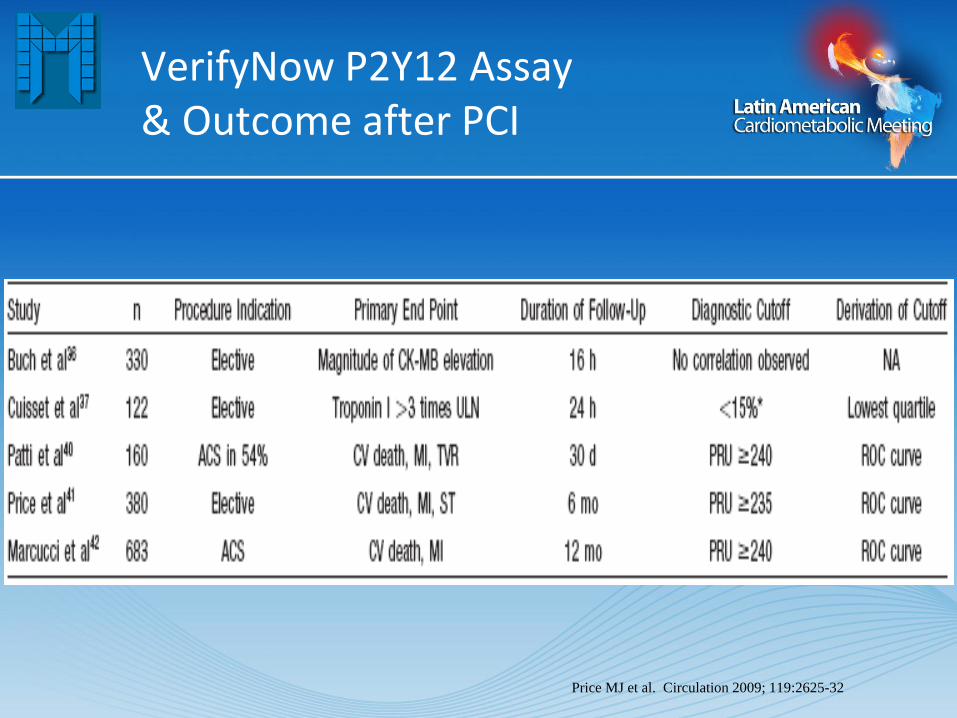
VerifyNow P2Y12 Assay & Outcome after PCI
Price MJ et al. Circulation 2009; 119:2625-32
Endothelial Effects

Statins & Endothelial cells
Morales-Villegas E. et al. International J Hypertension 2011

Endothelial Progenitor Cells
60 45 30 15 0 -15
CF
U-E
C (
4x10
6 P
BM
Cs)
105
70
35
0
stenosis (%)
r = -0.30
p = 0.004
Briguori C et al. FASEB J 2010 (in press)

Time (months)
24 18 12 6 0
Even
t F
ree S
urv
ival
1.0
0.8
0.6
0.4
0.2
0
Log rank p = 0.003
Endothelial Progenitor Cells
Briguori C et al. FASEB J 2010 (in press)
Low EPCs group
High EPCs group

Endothelial Progenitor Cells & Statins
Duckers HJ et al. Eurointerv 2007; 3: 67-75

High-dose atorvastatin reload pre-PCI increases circulating levels of EPCs
Atorvastatin Placebo
r t0 t8 t24 r t0 t8 t24 0
1
2
3
4
5
6
7
CD
45
dim
/C
D13
3+/
C
D34
+/
KD
R+ (
%)
Patti G et al. European Society of Cardiology Congress 2009

Safety concerns?
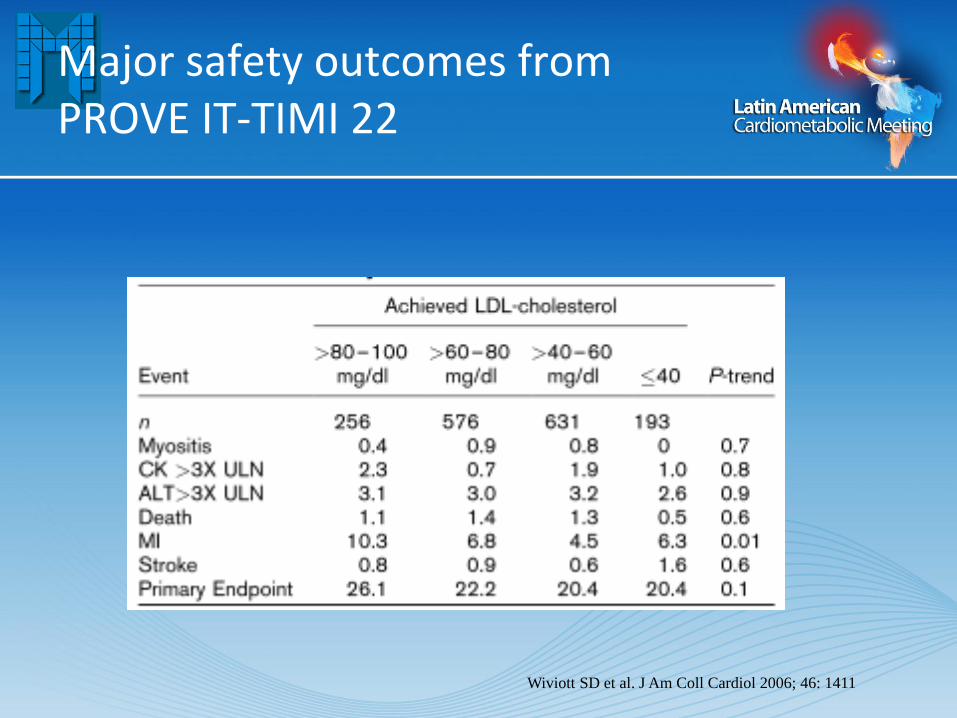
Major safety outcomes from PROVE IT-TIMI 22
Wiviott SD et al. J Am Coll Cardiol 2006; 46: 1411

Major safety outcomes
Wenger NK et al. Ann Intern Med 2007; 147: 19
Conclusions
Atorvastatin prevents per-procedural myorcadial damage
A single, high (80 mg) loading (within 24 hours) dose of atorvastatin reduces the incidence of periprocedural MI in elective PCI.
Preliminary data suggests the effect of the loading 80 mg atorvastatin dose on
Inflammatory pattern Platelet reactivity Circulating endothelial progenitor cells
The high loading dose of atorvastatin seems to be safe and effective
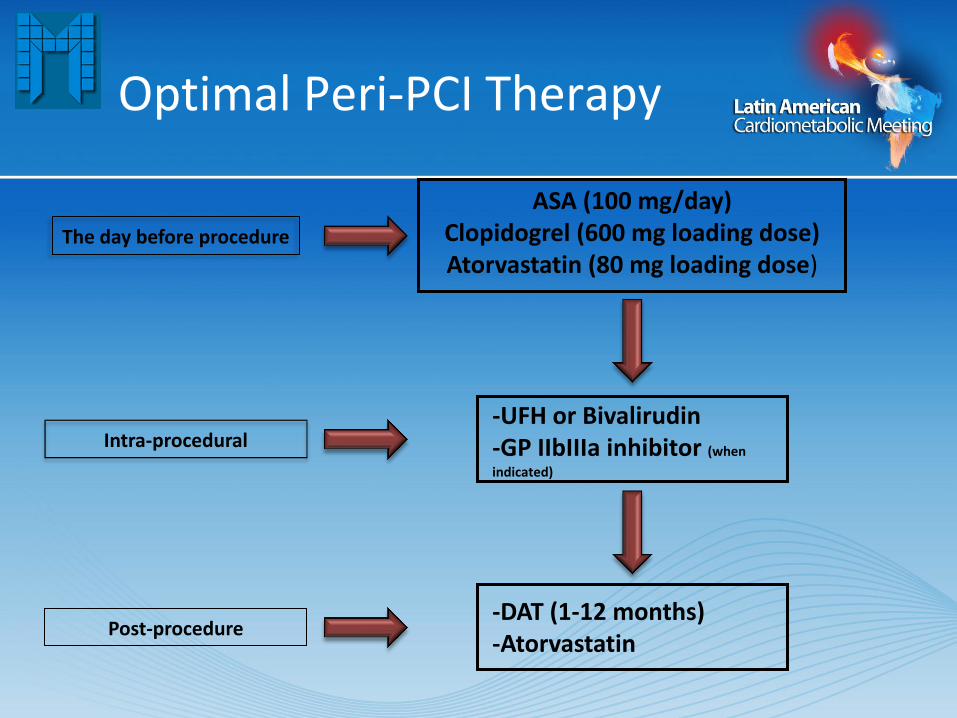
Optimal Peri-PCI Therapy
-UFH or Bivalirudin -GP IIbIIIa inhibitor (when
indicated)
ASA (100 mg/day) Clopidogrel (600 mg loading dose) Atorvastatin (80 mg loading dose)
The day before procedure
-DAT (1-12 months) -Atorvastatin
Intra-procedural
Post-procedure


















