
estatinas e influenza.ppt
10
USO DE ESTATINAS EN INFLUENZA INSTITUTO MEXICANO DEL SEGURO SOCIAL DIRECCIÓN DE PRESTACIONES MÉDICAS
-
Upload
josealberto-arenas -
Category
Documents
-
view
30 -
download
0
Transcript of estatinas e influenza.ppt

USO DE ESTATINAS EN INFLUENZA
INSTITUTO MEXICANO DEL SEGURO SOCIALDIRECCIÓN DE PRESTACIONES MÉDICAS
RECOMENDACIÓN PARA EL USO DE ESTATINAS
PACIENTE CON DIAGNÓSTICO O SOSPECHA DE INFLUENZAMAS NEUMONÍA
•Grupo con alta mortalidad.
•Probable causa la “tormenta de citocinas”, caracterizada por una rápida acumulación de citocinas durante el reconocimiento del virus por el organismo con el consecuente daño a nivel pulmonar.
•Daño observado principalmente en pacientes con co-morbilidad asociada a un proceso inflamatorio crónico, como: obesidad, DM2, enfermedad cardiovascular, asma y cáncer entre otros.
RECOMENDACIÓN PARA EL USO DE ESTATINAS
PACIENTE CON DIAGNÓSTICO O SOSPECHA DE INFLUENZAMAS NEUMONÍA
•Estatinas.
•Las estatinas han demostrado una reducción de la enfermedad cardiovascular independiente de la reducción en los lípidos. Efecto atribuido a una acción de inmunomodulación y anti-inflamación.
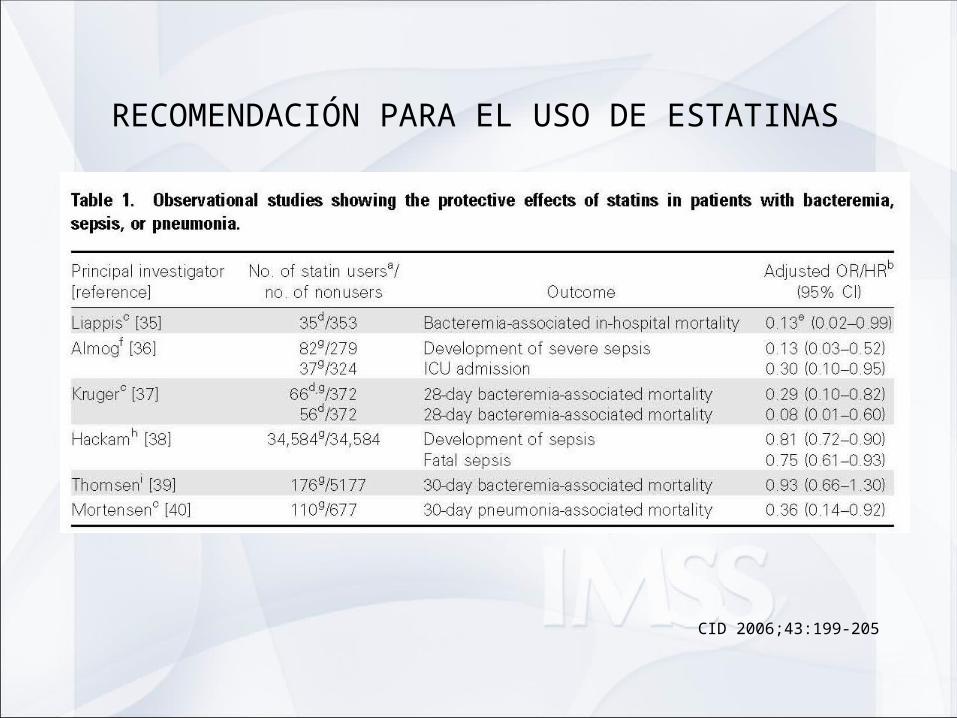
•Estudios observacionales han mostrado un incremento de la sobrevida de pacientes que cursan con enfermedades infecciosas como sepsis neumonía bacteriana e infecciones virales como dengue, virus sincicial respiratorio e influenza.
RECOMENDACIÓN PARA EL USO DE ESTATINAS
CID 2006;43:199-205

RECOMENDACIÓN PARA EL USO DE ESTATINAS
CHEST Original Research NOVEL PHARMACOTHERAPY
Influenza and COPD Mortality Protection as Pleiotropic, Dose-Dependent Effects of Statins* Floyd J. Frost, PhD; Hans Petersen, MS; Kristine Tollestrup, PhD; and Betty Skipper, PhD
Background: Published data on antiinflammatory and immunomodulatory effects of statins suggest they may reduce mortality risks associated with an unchecked immune response to selected infections, including influenza and COPD. We assessed whether statin users had reduced mortality risks from these conditions. Methods: We conducted a matched cohort study (n = 76,232) and two separate case-control studies (397 influenza and 207 COPD deaths) to evaluate whether statin therapy is associated with increased or decreased mortality risk and survival time using health-care encounter data for members of health maintenance organizations. For the cohort study, baseline illness risks from all causes prior to initiation of statin therapy were used to statistically adjust for the occurrence of outcomes after initiation of treatment. Results: For moderate-dose (> 4 mg/d) statin users, this cohort study found statistically significant reduced odds ratios (ORs) of influenza/pneumonia death (OR, 0.60; 95% confidence interval [CI],0.44 to 0.81) and COPD death (OR, 0.17; 95% CI, 0.07 to 0.42) and similarly reduced survival hazard ratios. Findings were confirmed with the case-control studies. Confounding factors not considered may explain some of the effects observed. Conclusions: This study found a dramatically reduced risk of COPD death and a significantly reduced risks of influenza death among moderate-dose statin users.
(CHEST 2007; 131:1006–1012)
CHEST Original Research NOVEL PHARMACOTHERAPY
Influenza and COPD Mortality Protection as Pleiotropic, Dose-Dependent Effects of Statins* Floyd J. Frost, PhD; Hans Petersen, MS; Kristine Tollestrup, PhD; and Betty Skipper, PhD
Background: Published data on antiinflammatory and immunomodulatory effects of statins suggest they may reduce mortality risks associated with an unchecked immune response to selected infections, including influenza and COPD. We assessed whether statin users had reduced mortality risks from these conditions. Methods: We conducted a matched cohort study (n = 76,232) and two separate case-control studies (397 influenza and 207 COPD deaths) to evaluate whether statin therapy is associated with increased or decreased mortality risk and survival time using health-care encounter data for members of health maintenance organizations. For the cohort study, baseline illness risks from all causes prior to initiation of statin therapy were used to statistically adjust for the occurrence of outcomes after initiation of treatment. Results: For moderate-dose (> 4 mg/d) statin users, this cohort study found statistically significant reduced odds ratios (ORs) of influenza/pneumonia death (OR, 0.60; 95% confidence interval [CI],0.44 to 0.81) and COPD death (OR, 0.17; 95% CI, 0.07 to 0.42) and similarly reduced survival hazard ratios. Findings were confirmed with the case-control studies. Confounding factors not considered may explain some of the effects observed. Conclusions: This study found a dramatically reduced risk of COPD death and a significantly reduced risks of influenza death among moderate-dose statin users.
(CHEST 2007; 131:1006–1012)

RECOMENDACIÓN PARA EL USO DE ESTATINAS
Influenza Hazard COPD Hazard
Variables Ratio (95% CI) Ratio (95% CI)
All users 0.61 (0.41–0.92)* 0.23 (0.13–0.42)*
Low compliance 0.81 (0.44–1.51) 0.45 (0.21–0.94)*
Moderate compliance 0.51 (0.30–0.89)* 0.13 (0.05–0.32)*
Without COPD-related deaths
Low compliance 0.99 (0.54–1.80)
Moderate compliance 0.54 (0.31–0.93)*
Table 4. Proportional Hazard Survival Analysis
CHEST 2007; 131:1006–1012

RECOMENDACIÓN PARA EL USO DE ESTATINAS
CRITERIOS PARA CONSIDERAR LA TERAPIA
•En quienes sí:•Pacientes con neumonía asociada a infección por el virus de la influenza AH1N1.•Pacientes mayores de 13 años (con más de 40 kgs. de peso).
•En quienes no:•Pacientes con daño hepático, renal, CPK >2 valor de referencia, con hipotiroidismo descontrolado, con embarazo, uso crónico de warfarina, alergia a estatinas.

RECOMENDACIÓN PARA EL USO DE ESTATINAS
DOSIS RECOMENDADA
•Atorvastatina 80 mgs/día por 5 días en pacientes ≥16 años.
•Atorvastatina 40 mgs/día por 5 días en pacientes de 13 a 15
años (peso ≥40 kgs).
Debe recibir su tratamiento antiviral de base.

RECOMENDACIÓN PARA EL USO DE ESTATINAS
MEDICIONES DE SEGURIDAD
•Si en algún momento, las mediciones de CPK son >10 x ULN ó > 5
X ULN y se acompañan de dolor muscular, dolor a la palpación o
debilidad inexplicables.
•Si se presentan niveles persistentes de TGO/ TGP >3 x ULN (2
mediciones con diferencia de 48 hrs).
Con el fin de cuidar la seguridad de los pacientes se desarrolló un
sistema electrónico de vigilancia .

OTRAS ACCIONES DE LA DPM CON EL FIN DE INCREMENTAR LA CALIDAD DEL SUSTENTO A LA
ACTUAL RECOMENDACIÓN
Promoción y apoyo en forma independiente al desarrollo de un
Ensayo clínico, aleatorizado, comparado contra placebo y triple ciego.
Mismo que habrá de iniciarse en las siguientes semanas en un número
reducido de Hospitales.

![Efetividade de Estatinas em Dose Alta, Moderada e Baixa na ... · Ribeiro e cols. Custo-Efetividade de Estatinas no Brasil Arq Bras Cardiol. 2014; [online].ahead print, PP.0-0 Introdução](https://static.fdocuments.net/doc/165x107/5be5741509d3f22b448c0734/efetividade-de-estatinas-em-dose-alta-moderada-e-baixa-na-ribeiro-e-cols.jpg)
















