Teasdale-1999-Clinical Psychology & Psychotherapy
10
Click here to load reader
-
Upload
costel-pacuraru -
Category
Documents
-
view
4 -
download
1
description
metacognicion
Transcript of Teasdale-1999-Clinical Psychology & Psychotherapy

Metacognition, Mindfulness and theModification of Mood Disorders
John D. Teasdale*Medical Research Council Cognition and Brain Sciences Unit, Cambridge, UK
A distinction is made between metacognitive knowledge (knowing thatthoughts are not necessarily always accurate) and metacognitive insight(experiencing thoughts as events in the field of awareness, rather thanas direct readouts on reality). This distinction, and its relevance topreventing relapse and recurrence in depression, is examined withinthe Interacting Cognitive Subsystems (ICS) theoretical framework. Thisanalysis suggests, as an alternative to cognitive therapy with its focuson changing the content of depression-related thought, the strategy ofchanging the configuration, or mode, within which depression-relatedthoughts and feelings are processed, i.e. changing one's relationship toinner experience. Specifically, facilitating a metacognitive insightmode, in which thoughts are experienced simply as events in themind, offers an alternative preventative strategy. Mindfulness trainingteaches skills to enter this mode, and forms a central component ofMindfulness-based Cognitive Therapy, a novel, cost-efficient grouppreventative programme, for which there is encouraging evidence ofeffectiveness. Copyright # 1999 John Wiley & Sons, Ltd.
A recovered depressed patient attending a relapseprevention programme developed the liberatingmetacognitive insight `thoughts aren't facts'. Whenshe excitedly shared this insight with her husband,he responded `I was born knowing that'. Allowinga little poetic licence on the exact age at which heacquired this metacognitive knowledge, his com-ment reflected the fact that, at one level, thisinformation about thoughts is commonplace.Indeed, at that level, the patient herself alreadyknew it. And yet, in that form, this metacognitiveknowledge had had little `saving' power in protect-ing her from the effects of depressive thoughtpatterns. On the other hand, the metacognitiveinsight acquired in the relapse prevention pro-gramme appeared to be one of the most importantoutcomes contributing to the preventative effects ofthe programme, not just for this woman, but forparticipants more widely.
How can we best describe and understandthe distinction between what I have called
metacognitive insight and what is usually describedas metacognitive knowledge? How can we under-stand the ways in which such insights might helprecovered depressed patients avoid relapse andrecurrence of depression? How can we foster thedevelopment of such insights? This paper attemptsto answer these questions.
METACOGNITIVE KNOWLEDGE ANDMETACOGNITIVE EXPERIENCE
A traditional teaching story (Shah, 1974, p. 122) mayhelp illustrate further the distinction that I havereferred to as the contrast between insight andknowledge: Uwais was asked `How do you feel?'.He replied `Like one who has risen in the morningand does not know whether he will be dead in theevening'. His questioner responded `But this is thesituation of all men'. Uwais replied `Yes, but howmany of them feel it?'.
This story points the contrast between the`factual' knowledge that we may all die at anytime, and the direct `experiential' awareness, from
CCC 1063±3995/99/020146±10$17.50Copyright # 1999 John Wiley & Sons, Ltd.
Clinical Psychology and PsychotherapyClin. Psychol. Psychother. 6, 146±155 (1999)
*Correspondence to: John D. Teasdale, MRC Cognition andBrain Sciences Unit, 15 Chaucer Road, Cambridge CB2 2EF,UK.
Costel Pacuraru
resaltar
Costel Pacuraru
resaltar
Costel Pacuraru
resaltar
Costel Pacuraru
resaltar
Costel Pacuraru
resaltar
Costel Pacuraru
resaltar
Costel Pacuraru
resaltar
Costel Pacuraru
resaltar

one moment to the next, that life is transient, and itsend unpredictable. The former, even if frequentlyrepeated, can remain isolated `cold' information,whereas the latter is likely to have profound effectson our views of everything, and can radically affectthe way we live from moment to moment. Appliedto our introductory example, this contrast high-lights the difference between, on the one hand,actually experiencing thoughts as thoughts (that is, asevents in the mind, rather than as direct readouts onreality) in the moment that they occur, and, on theother hand, simply thinking about thoughts as`other than facts'.
How, if at all, have researchers in metacognitiondealt with this issue? Within the study of metacog-nition, a distinction is made between metacognitiveknowledge and metacognitive experience. Does thisdistinction clarify the contrast I wish to make?Metacognitive knowledge has been defined as `thatsegment . . . of stored world knowledge that has todo with people as cognitive creatures and with theirdiverse cognitive tasks, goals, actions and experi-ences. An example would be a child's acquiredbelief that unlike many of her friends, she is betterat arithmetic than at spelling,' (Flavell, 1979, p. 906).Metacognitive experiences, on the other hand, havebeen defined as `any conscious cognitive or affectiveexperiences that accompany and pertain to anyintellectual enterprise. An example would be thesudden feeling that you do not understand some-thing another person just said' (Flavell, 1979,p. 906). Another, highly researched, examplewould be the `feeling of knowing', the intuitivesense that one knows a certain piece of informationeven though, at the moment of feeling that sense,one cannot actually recall the information (Nelsonet al., 1984). Some metacognitive experiences arebest described as items of metacognitive knowledgethat have entered experience. Others, such as thefeeling that one is still far from reaching the solutionto a puzzle, are not. Thus, metacognitive knowl-edge and metacognitive experiences can beregarded as partially overlapping sets (Flavell,1979, p. 908).
Unfortunately, the distinction between metacog-nitive knowledge and metacognitive experience thatis made by workers in metacognition, such asFlavell, does not accurately capture the distinctionbetween knowledge and insight that I wish tomake: the experience of knowing that thoughts arenot facts is just as much a metacognitive experienceas directly experiencing thoughts as thoughts (thatis, as events in the mind, rather than as, necessarily,accurate reflections of reality).
The distinction I wish to make between meta-cognitive insight and metacognitive knowledge is ofpotentially great importance and can be graspedfairly directly on the basis of one's personalexperience, and yet, in other ways, this distinctionis quite subtle and does not seem to map neatlyonto the contrasts that are currently made withinresearch on metacognition. If we are to discuss thisissue in more detail, and to explore its potentialclinical implications, it would be helpful to do sowithin a systematic cognitive framework. Interact-ing Cognitive Subsystems (ICS) (Barnard andTeasdale, 1991; Teasdale and Barnard, 1993;Teasdale, 1993, 1996) provides such a framework.
THE INTERACTING COGNITIVESUBSYSTEMS (ICS) FRAMEWORKÐTWO KINDS OF MEANING
Interacting Cognitive Subsystems (ICS) is a com-prehensive conceptual framework, within which, inprinciple, accounts of all aspects of information-processing can be developed. ICS is based on a few,basically simple, ideas. One central assumption isthat the mind works using a number of qualitat-ively different kinds of information, or mentalcodes. Each of these codes represents a distinctaspect of experience. Of particular relevance to thepresent discussion are the mental codes related tomeaning. ICS recognizes two qualitatively distinctkinds of meaning, a specific and a more generic,and suggests that emotion is linked directly only tothe more generic form of meaning.
In ICS, specific meanings are represented bypatterns of Propositional code, and refer to specificconcepts and the relationships between them, as in,for example, `the cat sat on the mat'. Meaning at thislevel is not difficult to grasp, and corresponds fairlyclosely to the meanings conveyed by singlesentences in language. This kind of meaning hasalso been referred to as explicit, or declarativeknowledge. Such meanings have a truth value thatcan be assessed, and the examination of suchmeanings, by the collection of data, considerationof evidence and the like, is, of course, the focus ofmuch activity in cognitive therapy (Beck et al.,1979). Nonetheless, according to ICS, such specificmeanings, themselves, have no direct relationship toemotion production (Teasdale, 1993). In this way, itis possible to discuss `coolly', at an intellectual level,specific emotion-related meanings without, necess-arily, feeling the associated emotions or beingdrawn into emotion-related behaviours; this, of
Copyright # 1999 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. 6, 146±155 (1999)
Metacognition, mindfulness, mood disorders 147
Costel Pacuraru
resaltar

course, is one of the potential advantages of havingsuch a symbolic level of representation.
ICS also recognizes a more generic level of mean-ing, corresponding to schematic mental models ofexperience, and represented in patterns of Implica-tional code. Such meanings represent deep regular-ities, themes, interrelationships and prototypicalfeatures extracted from the patterns of specificmeanings and sensory features that recur acrossexperiences that share deep similarities, eventhough they may be superficially different. Thesehigher order meanings are much more difficult toconvey than specific meanings as there is no directcorrespondence between this level of representationand language. Implicational meanings are implicit,rather than explicit, and do not have a truth valuethat can be evaluated or tested by the collection ofevidence. Sensory features, such as tone andloudness of voice, or proprioceptive feedback (e.g.from bodily sensations related to posture or facialexpression), can make a direct contribution toImplicational meaning.
Implicational meanings are associated with intui-tive, holistic, `felt senses' or feelings with implicitmeaning content. For example, a sense of confid-ence marks the processing of schematic modelsassociated with themes of competence, worth,optimism and positive expectancy. Similarly, inthe earlier example of the teaching story, Uwais'stress on the importance of feeling the awarenessthat he could be dead by evening would beinterpreted, within ICS, as emphasizing the import-ance of actively creating schematic models encodingthemes related to the impermanence of life and theunpredictability of its end.
ICS proposes that only the generic Implicationallevel of meaning is directly linked to emotion;specific Propositional meanings only contributeindirectly to the production of emotion throughtheir contribution to emotion-related Implicationalmeanings.
The relationship between specific and genericmeanings is analogous to the relationship betweenthe letters that make up a sentence and the meaningof the sentence. A sentence conveys a specificmeaning that is qualitatively different from andgreater than the sum of its individual letters. In thesame way, the generic meaning of a schematicmodel is qualitatively different from and greaterthan the sum of the patterns of specific meaningsthat contribute towards it. Poetry illustrates thisrelationship (Teasdale and Barnard, 1993, p. 73):
O what can ail thee, knight at arms.
Alone and palely loitering?The sedge has wither'd from the lake.And no birds sing.
The sense of melancholy and abandonment con-veyed by this poem marks the synthesis from thepattern of specific meanings, imagery and sounds,of Implicational schematic models (higher ordermeanings) encoding such themes; the total effect ofthe poem cannot be conveyed by a single specificmeaning, nor can it be simply reduced to the sum ofthe components contributing towards it.
As far as treatment is concerned, the importantpoints arising from the distinction between twokinds of meaning recognized within the ICSframework are the following: (i) only genericmeanings are directly linked to emotion; (ii) genericand specific meanings are qualitatively different sothat one cannot simply be reduced to another; and(iii) different forms of intervention are likely to berequired for these two kinds of meaning (Teasdale,1993, 1997).
METACOGNITIVE KNOWLEDGE ANDMETACOGNITIVE INSIGHT WITHIN ICS
How can ICS, with its distinction between twodistinct kinds of meaning, help us to understand thedistinction between metacognitive insight andmetacognitive knowledge, as I used these terms inmy introductory example?
Metacognitive knowledge, of a specific factualform, such as `All thoughts are not necessarilyfactually correct', corresponds to stored specificPropositional meanings encoding the relationsbetween the designated concepts. Such meaningswould be manipulated when we think `intellect-ually' about thoughts. Just as we can acquire theknowledge `Canberra is the capital of Australia'without having to take a trip there ourselves, thestored Propositional meanings representing meta-cognitive knowledge can be acquired `vicariously',encoded in the verbal input from others (or frombooks) without, for example, having to repeatedlyexperience, personally, the disconfirmation of thefactual content of our thoughts.
According to ICS, specific Propositional mean-ings, on their own, will have little impact onemotional state; it is only to the extent that theycontribute to emotion-related generic Implicationalmeanings that they will affect emotion. Fromthis perspective, it is, therefore, unsurprising thatthe `intellectual' metacognitive knowledge that
Copyright # 1999 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. 6, 146±155 (1999)
148 J. D. Teasdale

`thoughts aren't facts', alone, offers little help tothose in distress. What about metacognitive insight?From an ICS perspective, whereas metacognitiveknowledge is represented at the level of specific,Propositional meanings, metacognitive insight isrepresented at the level of higher order, schematicImplicational meanings.
Changes in representations at the Implicationallevel have to be acquired by some form ofexperiential learning in which the componentscontributing to the new representation are actuallyexperienced in new patterns for new representa-tions to be laid down; such learning cannot beacquired vicariously by `book knowledge' alone. Atthe Implicational, schematic level, representationscan have direct effects on emotion production, andso it is quite possible for changes in Implicationalmetacognitive representations to have importanttherapeutic consequences, as in the case of thewoman who acquired the deeply felt insight`thoughts aren't facts'. It is useful to distinguishtwo aspects of metacognitive insight: (i) the general`view' within which, for example, thoughts andfeelings would be seen as `only' transient events inthe field of awareness; (ii) the instantiation of thatgeneral view with respect to particular thoughtsand feelings as they are being processed. The formercorresponds to a stored Implicational schematicmodel concerning the interrelationships betweenthoughts, feelings and reality that is much richer inimplicit meaning than the bare Propositional state-ment `thoughts are not facts'. The latter correspondsto the on-line application of such a model to thethoughts and feelings that are being concurrentlygenerated in that moment. Such processing merits amore detailed description.
METACOGNITIVE INSIGHT AND THEINTERACTION BETWEENPROPOSITIONAL AND SCHEMATICLEVELS OF MEANING
In multi-level cognitive theories, such as ICS, repre-sentations of a topic at one level of information, inone mental code, can feed the creation of repre-sentations related to that topic at other levels ofinformation, in other mental codes, and thosedistinct representations, both related to the sametopic, can be processed, in different parts of theprocessing system, in close temporal proximity. Inthis way, different aspects of any experience ortopic can be processed concurrently at a number ofdifferent levels. For example, the affective qualities
of the sound of someone's voice as they are talkingto us can be extracted in one part of the system,while the specific meanings of their verbal utter-ances are being decoded in another part of thesystem. Information from these two levels ofrepresentation can then be integrated in a differentpart of the system to derive higher order meaningsreflecting both the patterns of specific meanings inwhat is being said and the voice tone in which it isbeing said.
Applied to metacognitive insight, these con-siderations suggest that representations of thespecific Propositional meanings encoded in verbal-izable thought can both contribute to the produc-tion of Implicational schematic models encodinghigher order meanings, and, themselves, be thetopic of those higher order meanings.
In the usual mode of interaction between Proposi-tional and Implicational meanings, as, for example,in thinking through a problem, or analysing asituation, patterns of specific Propositional mean-ings contribute to the synthesis of problem- orsituation-relevant schematic models, without them-selves becoming the topic of the schematic modelscreated. In this non-metacognitive mode, the sche-matic models accessed from memory will be relatedto problem-solving, and the like. These models willprovide an informational context in which frag-ments of Implicational code derived from specificmeanings are treated as `factual' building blocksfrom which schematic models related to theanalysis or solution of the currently presentingproblem or situation can be derived.
By contrast, in the metacognitive mode in whichthoughts are concurrently experienced as mentalevents rather than facts, generic `thoughts aren'tfacts' schematic models will have been accessedfrom memory. These models will provide aninformational context, at the Implicational level, inwhich fragments of Implicational code derivedfrom the specific meanings determining thoughtcontent in other parts of the processing system will,at this level, be treated as `mental events'. The resultwill be that, subjectively, thoughts are experienced,simultaneously, as both thoughts and as `events inthe mind'. Note that such simultaneity would notbe possible if the metacognitive information that`thoughts are not facts' were represented at thesame (specific Propositional) level as the specificmeanings of the thoughts; just as the teeth cannotbite themselves, it is not possible for the level ofthe information processing system dedicated toprocessing specific Propositional meanings simul-taneously to process both specific meanings related
Copyright # 1999 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. 6, 146±155 (1999)
Metacognition, mindfulness, mood disorders 149

to thought content and specific meanings indicatingthat those thoughts are only events. Rather, meta-cognitive processing at this level might involvethoughts about thoughts, either before or after theyhave occurred, rather than experiencing thoughts asthoughts as they occur.
Within ICS, the existence of two levels of mean-ing, with specific level meanings standing in thesame relation to higher order meanings as do lettersto the specific meaning of a sentence, allowsconcurrent processing of cognitive and metacogni-tive levels of representation. There is a directparallel with, at lower levels of representation,the relation of the letter `f' to the meaning ofthe sentence `The last letter of this sentence isan ``f'' '.
How does this detailed analysis help us tounderstand why metacognitive insight might beuseful clinically? In answering this question, I shallfocus primarily on the persistence and prevention ofdepression.
INTERACTIONS BETWEEN TWO LEVELSOF MEANING IN THE PERSISTENCEOF DEPRESSION
Within the ICS framework, Implicational schematicmodels encoding higher order meanings arederived from patterns of specific Propositionalmeanings. Equally, Implicational schematic modelsgenerate specific Propositional meanings. In otherwords, specific meanings feed the creation ofschematic models, which in turn lead to morespecific meanings and so on. According to ICS,these reciprocal transformations form the founda-tion of cycles of continuing exchange of informationand mutual influence between subsystems proces-sing these two levels of representation. Thisexchange is so central to a wide range of informa-tion processing in tasks involving so-called `con-trolled processing' that it has been dubbed the`central engine of cognition' (Teasdale and Barnard,1993, p. 76).
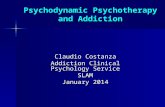
As well as playing a pivotal role in cognitivetasks such as comprehension, planning, problemsolving and directed memory search, central engineactivities have been implicated in the onset andpersistence of emotional disorders, specificallydepression (Teasdale, 1993, 1996, 1997; Teasdaleand Barnard, 1993). Figure 1 shows a sketch of theICS analysis of a self-perpetuating `depressiveinterlock' processing configuration, which, it hasbeen suggested, can act to maintain states of
depression by ruminative, negative self-focusedcognitive processing.
In the configuration shown in Figure 1, theimmediate antecedent to the generation of depres-sion is the processing of schematic models encodinghigher order meanings with depressogenic themes,such as globally negative view of the self as patheticor worthless, a view of present difficulties as highlyaversive, uncontrollable and likely to persist and thelike. According to this analysis, the maintenance ofthe depressed state is dynamic and depends on thecontinuous creation and regeneration of schematicmodels encoding depressogenic themes; if thesynthesis of such models ceases, then depressionwill lift.
Figure 1 illustrates two interconnected feedbackloops that, once established, can act to regeneratedepressogenic schematic models and so maintaindepression. The first `cognitive loop' involves thecentral engine; in the depressive interlock configur-ation the interaction between the subsystems deal-ing with specific and higher order meaningsbecomes dominated by processing informationwith negative, depressive content; depressogenicschematic models generate negative specific mean-ings (such as attributions for particular failures topersonal, global characterological inadequacies, orexpectations of future failures and continuingdepression); patterns of such meanings, in turn,can regenerate depressogenic schematic modelsclosely similar to those from which they, them-selves, were derived, and so the cycle can bemaintained.
The other `sensory loop' operates through theeffects of sensory feedback from the effects ofdepression on the body. Schematic models canreceive contributions from both patterns of specificmeanings and from patterns of sensory informationthat have been recurring features of situations inwhich those patterns of specific meanings havepreviously been processed. Sensory feedback fromthe bodily consequences of the depressed state willhave been a recurring feature of previous situationsin which depression has been experienced for anylength of time. It follows that such feedback, inconjunction with the contributions from thecognitive loop, can act to regenerate furtherdepressogenic schematic models and so endowthe depressive interlock configuration with self-perpetuating properties.
It is assumed that the type of informationcirculating round the cognitive loop of the depres-sive interlock configuration is similar to thatsuggested by negative self-focus (Pyszczynski and
Copyright # 1999 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. 6, 146±155 (1999)
150 J. D. Teasdale

Greenberg, 1987) and ruminative (Nolen-Hoeksema, 1991) cognitive models of depression.This content is predominantly negative, self-related,focused on discrepancies between the currentperceived state of the self and the desired state,and often seems to be related to attempts to reducedepression by understanding its causes in relationto aspects of personal inadequacy. Unfortunately,the ruminative cognitive strategies employed inthese attempts often seem to involve extendedpondering over irremediable personal inadequaciesand deficiencies. Such pondering not only fails toachieve the intended goals, but also maintainsdiscrepancies between present and desired
self-states as the topic of processing cycles, soperpetuating, rather than reducing depression. Thepredominant subjective quality of such processingis thinking about the self, about depression-relatedthoughts and feelings and about how to understandwhat is going on. From the ICS perspective, thesubjective quality of thinking about is a marker ofcentral engine processing cycles in which thedominant controlling influence is at the Proposi-tional (specific thought) level (cf. Hurlburt, 1993,chapter 5).
The ICS analysis assumes that cognitive vulner-ability to persistent depression, and to relapse todepression after recovery, is related to the ease with
Figure 1. Depressive interlock: a self-perpetuating processing configuration that can establish/maintain the depressedstate. The central engine of cognition (Implicational±Propositional±Implicational cycles) is shown in broad, hatchedarrows. (From Teasdale (1996), with permission.)
Copyright # 1999 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. 6, 146±155 (1999)
Metacognition, mindfulness, mood disorders 151

which the depressive interlock configuration can bere-established at times of dysphoric mood. Consist-ent with this view, a measure of ruminativeprocessing style developed by Nolen-Hoeksemahas been shown to be predictive of risk andpersistence of depression (Nolen-Hoeksema andMorrow, 1991). Sample items from this scaleinclude, in response to a request to the respondentto indicate what they normally do when feelingdepressed, `Think about all your shortcomings,failings, faults, mistakes', `Think about how sadyou feel', `Isolate yourself and think about thereasons why you feel sad'. Again, such items,focusing on thinking about, suggest central engineprocessing dominated by the relatively specificPropositional level.
From this perspective, the target of interventionsto prevent relapse and recurrence in depression is toreduce the probability that ruminative processingcycles, of the kind supported by the depressiveinterlock configuration, become established at timesof increasing dysphoria.
PREVENTING THE ESTABLISHMENT OFDEPRESSIVE INTERLOCK TO REDUCERISK OF RELAPSE
In principle, there are a variety of strategies thatcould be used to prevent the establishment of thedepressive interlock configuration or to interrupt it,once established. At the simplest level, one couldengage the central engine in processing informationquite unrelated to depression, as in an engagingdistraction task, such as describing in detail thecontents of a visual scene. Because the cognitiveresources of the central engine can only process acertain amount of information in a given time,loading up those resources with the processing ofnon-depressive information would reduce thecapacity available for processing the depressiveinformation necessary to sustain the interlockconfiguration. Consequently, this configurationwould be less likely to become established, or tobe maintained, if already established. Althoughdistraction does seem to be a useful strategy fordealing with mild, `normal' depressed moods(Nolen-Hoeksema, 1991), experience suggests thatits effects on clinical depression are short lived(Fennell et al., 1987), and that it may not offer aviable approach to preventing relapse.
Another strategy is to focus on changing thenegative self-related meanings, both specific andschematic, that sustain the depressive interlock
configuration. This, of course, is the approach ofcognitive therapy, and, as is well known, there isgood evidence for the effectiveness of cognitivetherapy for depression, both as an acute treatmentand as a way to reduce risk of relapse followingcompletion of the acute treatment phase (e.g.Blackburn et al., 1986; Evans et al., 1992; Simonset al., 1986).
The ICS analysis suggests a further strategy toavoid becoming trapped in the depressive interlockconfiguration at times of relapse that is in manyways complementary to the cognitive therapyapproach. This strategy involves neither redirectingprocessing to non-depressive material, as in distrac-tion, nor directly changing the content of negativethinking. Rather, it involves processing similarcontents (negative self-related thoughts and feel-ings), but within a different processing configura-tion. That is, the topic of processing remainsbroadly the same, but, because this topic isprocessed through a different configuration, withdifferent input±output relationships, the systemavoids `settling' into the vicious self-perpetuatingcycles of the depressive interlock configuration.Rather, alternative configurations can allow acontinuing development and evolution of the wayin which depression-related material is processedover successive cycles, so that processing does notget stuck in the well worn `mental grooves' of thedepressive interlock configuration.
An example of such an alternative configurationwould be one in which, in contrast to the `thinkingabout' depression-related material that character-izes Propositionally dominated, ruminative, inter-lock processing, central engine processing iscontrolled from the Implicational, schematic, level.Subjectively, such processing would be character-ized more in terms of processing depression-relatedmaterial `experientially', rather than ruminatively`thinking about' it. Because such a configurationwould also make heavy demands on central engineresources, the establishment of this processingconfiguration would be mutually incompatiblewith the interlock configuration. Accordingly, ifthe chance of processing the kinds of negativethought and feeling that become accessible at timesof potential relapse through such alternative con-figurations can be increased, the chances of proces-sing them through the interlock configuration aredecreased, and the risk of relapse is reduced.
The detailed rationale for the strategy of shiftingthe processing configuration through which depres-sion-related material is processed, rather thanprocessing non-depressive content, or attempting
Copyright # 1999 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. 6, 146±155 (1999)
152 J. D. Teasdale

to change depression-related thoughts, is complexand cannot be presented in full here. Aspects of thisrationale have been presented elsewhere (Teasdaleet al., 1995). It may help to characterize thisapproach as focusing on changing an individual'srelationship to depression-related thoughts andfeelings, rather than (as in cognitive therapy)focusing on the content of those thoughts andfeelings. Alternatively, one could describe thisstrategy as establishing a different mode of cogni-tive processing within which to handle depression-related cognition (cf. Beck, 1996; Teasdale, 1996,1997). For example, the Implicationally controlledcognitive mode, in which negative, self-criticalthoughts are experienced with metacognitiveinsight as `events in the mind', is quite differentfrom the Propositionally dominated depressiveinterlock cognitive mode in which they are experi-enced as reflections of reality. Consequently, if, attimes of potential relapse, negative depressivematerial could be processed through this meta-cognitive mode, rather than through the interlockmode, probability of relapse to depression could bereduced.
How, practically, do we train individuals at riskfor depression in the skills of establishing themetacognitive insight mode? As would be expectedfrom the emphasis placed on experiential learningfor changing representations at the Implicationallevel (where the main action is as far as meta-cognitive insight is concerned), the answer to thisquestion is likely to involve an emphasis on practicerather than verbal discussion.
MINDFULNESS-BASED COGNITIVETHERAPY, METACOGNITIVE INSIGHTAND PREVENTION OF RELAPSE ANDRECURRENCE IN DEPRESSION
Training individuals to relate, with detached mind-fulness, to thoughts as events in the mind has beenused as a way to reduce psychological suffering forat least 2500 years, from the time of the Buddhaonwards (Goldstein and Kornfield, 1987). Practicesdeveloped within this tradition are central to Kabat-Zinn's (1990) Mindfulness-Based Stress Reductionprogramme (see below). Beck (1976, pp. 243±244)has underlined the importance of `distancing' and`decentering' from thoughts in the practice ofcognitive therapy. Acceptance and CommitmentTherapy (originally called Comprehensive Distanc-ing) (Kohlenberg et al., 1993), based on Hayes'(1987) contextual approach to cognitive activity,
trains individuals to relate to thoughts as hypoth-eses to be tested; there is preliminary evidence forthe effectiveness of such comprehensive distancingin the treatment of depression (Zettle and Hayes,1987; Zettle and Rains, 1989). Wells and Matthews(1996, p. 886), from their S-REF analysis ofemotional disorder, have recommended training in`detached mindfulness' as a component of cognitivetreatment for emotional disorders.
Based on analyses similar to those described inpreceding sections, Zindel Segal, Mark Williamsand I have developed a cost-efficient, group, skills-based programme specifically designed to helppatients who have recovered from depression,following treatment with anti-depressant medica-tion, learn psychological skills that will help themto reduce their risk of future relapse and recurrence.The programme, known as Mindfulness BasedCognitive Therapy (MBCT), draws heavily on theMindfulness-Based Stress Reduction Programmedeveloped by Jon Kabat-Zinn and his colleaguesat the University of Massachusetts Medical Center(Kabat-Zinn, 1990). This programme has alreadydemonstrated preliminary encouraging evidencefor its effectiveness in treating chronic pain(Kabat-Zinn, Lipworth and Burney, 1985; Kabat-Zinn et al., 1986), generalized anxiety and panic(Kabat-Zinn et al., 1992), and psoriasis (Bernhardet al., 1988). The relevance of this programme to thegoal of preventing relapse and recurrence indepression by fostering the ability to establishprocessing configurations (cognitive modes) charac-terized by metacognitive insight will be apparentfrom the following excerpts from Jon Kabat-Zinn's (1990) descriptions of the effects of thisprogramme:
It is remarkable how liberating it feels to be ableto see that your thoughts are just thoughts andthey are not `you' or `reality'. For instance, if youhave the thought that you have to get a certainnumber of things done today and you don'trecognize it as a thought but act as if it's `thetruth', then you have created a reality in thatmoment in which you really believe that thosethings must all be done today.
. . . On the other hand, when such a thoughtcomes up, if you are able to step back from it andsee it clearly, then you will be able to prioritizethings and make sensible decisions about whatreally does need doing. You will know when tocall it quits during the day. So the simple act ofrecognizing your thoughts as thoughts can freeyou from the distorted reality they often create
Copyright # 1999 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. 6, 146±155 (1999)
Metacognition, mindfulness, mood disorders 153
Costel Pacuraru
resaltar

and allow for more clear sightedness and agreater sense of manageability in your life(Kabat-Zinn, 1990. pp. 69±70; original italics).
Within mindfulness-based stress reduction, andwithin MBCT, the ability to see thoughts asthoughts, with a detached but inclusive awareness,is acquired by systematic, repeated practice inmindfulness training. Mindfulness has been definedas `paying attention in a particular way: onpurpose, in the present moment, and non-judgementally' (Kabat-Zinn, 1994, p. 4). From thepresent perspective, the essence of mindfulness is touse intentional control of attention to establish atype of alternative information processing con-figuration (or cognitive mode), that is incompatiblewith the depressive interlock configuration (and,also, with the configurations maintaining a range ofother disorders). This cognitive mode has beenpopularly characterized as one of `being', incontrast to the more usual `doing' modes that makeup so much of our lives and which, when distorted(as in the depressive interlock configuration), canlock us into dysfunctional emotional states.
In practice, mindfulness training involves inten-tionally maintaining awareness on a particularobject of attention, such as the physical sensationsin the body as the breath moves in and out, fromone moment to the next. Whenever the mindwanders, as it inevitably will, to thoughts, feelings,sounds or other bodily sensations, the contents ofawareness are noted, and the attention is thengently but firmly escorted back to the designatedobject of attention. This process is repeated over andover again within repeated daily periods of mind-fulness practice. Such practice provides repeatedexperiences in which the ability to relate tothoughts as events in the field of awareness isfacilitated by designating a non-thought ( frequentlybodily) primary focus of attention, against whichthe experience of thoughts can be registered assimply another event in awareness rather than asthe primary `stuff' of the mind or the self. Thisdetached perspective of moment to moment meta-cognitive insight with respect to thoughts is furtherfacilitated by the instruction to note the content ofthoughts as they arise and then to let go of themand return to the primary focus of attention. In thisway, a primary focus such as the breath can serve asan `anchor' which can be used to return awarenessto the present moment and limit the extent to whichone becomes `lost' in the `reality' created by thethought streams in which we are so oftenimmersed. Mindful observation of thoughts also
allows us to recognize familiar, recurring patternsin thought content, so facilitating further the abilityto see them as patterns of the mind rather than asnecessarily valid readouts on reality. Within theAC(M)T programme, extended mindfulness prac-tice with the thoughts, feelings and bodily sensa-tions that occur in the non-depressed state is used togive recovered depressed participants the skills toenter the `being' cognitive mode, characterized by arelation of metacognitive insight to the contents ofconsciousness. The programme then preparesparticipants to use these skills at times of potentialrelapse to pre-empt the establishment of thedepressive interlock configuration and so reducethe risk of relapse and recurrence of depression.
Mark Williams, Zindel Segal and I have recentlycompleted a clinical trial evaluating the effective-ness of Mindfulness-Based Cognitive Therapy in agroup of patients with recurrent depression(median of three previous episodes of majordepression). The results, as yet unpublished, areencouraging, suggesting that this approach can leadto significant reductions in rates of relapse.Such findings suggest that approaches such asMBCT, which focus directly on establishing adifferent metacognitive relationship to dysfunc-tional thoughts rather than trying to change thecontent of thoughts, may have considerable thera-peutic potential, and offer a complementary inter-vention strategy to that of more traditionalcognitive (therapy) approaches to treatment.
REFERENCES
Barnard, P. J. and Teasdale, J. D. (1991). Interactingcognitive subsystems: a systemic approach tocognitive±affective interaction and change. Cognitionand Emotion, 5, 1±39.
Beck, A. T. (1976). Cognitive Therapy and the EmotionalDisorders. New York: International Universities Press.
Beck, A. T. (1996). Beyond belief: a theory of modes,personality, and psychopathology. In: P. M. Salkovskis(Ed.), Frontiers of Cognitive Therapy. New York: Guil-ford, pp. 1±25.
Beck, A. T., Rush, A. J., Shaw, B. F. and Emery, G. (1979).Cognitive Therapy of Depression. New York: Guilford.
Bernhard, J. D., Kristeller, J. and Kabat-Zinn, J. (1988).Effectiveness of relaxation and visualization techniquesas an adjunct to phototherapy and photochemotherapyof psoriasis. Journal of the American Academy ofDermatology, 19, 572±573.
Blackburn, I. M., Eunson, K. M. and Bishop, S. (1986). Atwo-year naturalistic follow-up of depressed patientstreated with cognitive therapy, pharmacotherapy, and acombination of both. Journal of Affective Disorders, 10,67±75.
Copyright # 1999 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. 6, 146±155 (1999)
154 J. D. Teasdale

Evans, M. D., Hollon, S. D., De Rubeis, R. J., Piasecki, J.,Grove, W. M., Garvey, M. J. and Tuason, V. B. (1992).Differential relapse following cognitive therapy andpharmacotherapy for depression. Archives of GeneralPsychiatry, 49, 802±808.
Fennell, M. J. V., Teasdale, J. D., Jones, S. and DamleÂ, A.(1987). Distraction in neurotic and endogenous depres-sion: an investigation of negative thinking in majordepressive disorder. Psychological Medicine, 17, 441±452.
Flavell, J. H. (1979). Metacognition and cognitive monitor-ing. American Psychologist, 34, 906±911.
Goldstein, J. and Kornfield, J. (1987). Seeking the Heartof Wisdom: the Path of Insight Meditation. Boston:Shambhala.
Hayes, S. C. (1987). A contextual approach to therapeuticchange. In: N. S. Jacobson (Ed.), Psychotherapists inClinical Practice: Cognitive and Behavioral Perspectives.New York: Guilford, pp. 327±387.
Hurlburt, R. T. (1993). Sampling Inner Experience inDisturbed Affect. New York: Plenum.
Kabat-Zinn, J. (1990). Full Catastrophe Living: the Program ofthe Stress Reduction Clinic at the University of Massa-chusetts Medical Center. New York: Dell.
Kabat-Zinn, J. (1994). Wherever You Go There You Are:Mindfulness Meditation in Everyday Life. New York:Hyperion.
Kabat-Zinn, J., Lipworth, L. and Burney, R. (1985). Theclinical use of mindfulness meditation for the self-regulation of chronic pain. Journal of Behavioral Medicine,8, 163±190.
Kabat-Zinn, J., Lipworth, L., Burney, R. and Sellers, W.(1986). Four-year follow-up of a meditation-basedprogram for the self-regulation of chronic pain: treat-ment outcomes and compliance. The Clinical Journal ofPain, 2, 159±173.
Kabat-Zinn, J., Massion, A. O., Kristeller, J., Peterson,L. G., Fletcher, K. E., Pbert, L., Lenderking, W. R. andSantorelli, S. F. (1992). Effectiveness of a meditation-based stress reduction program in the treatment ofanxiety disorders. American Journal of Psychiatry, 149,936±943.
Kohlenberg, R. J., Hayes, S. C. and Tsai, M. (1993). Radicalbehavioral psychotherapy: two contemporaryexamples. Clinical Psychology Review, 13, 579±592.
Nelson, T. O., Gerler, D. and Narens, L. (1984). Accuracyof feeling-of-knowing judgements for predictingperceptual identification and relearning. Journal ofExperimental Psychology: General, 113, 282±300.
Nolen-Hoeksema, S. (1991). Responses to depression andtheir effects on the duration of depressive episodes.Journal of Abnormal Psychology, 100, 569±582.
Nolen-Hoeksema, S. and Morrow, J. (1991). A prospectivestudy of depression and posttraumatic stress symptomsafter a natural disaster: the 1989 Loma Prieta earth-quake. Journal of Personality and Social Psychology, 61,115±121.
Pyszczynski, T. and Greenberg, J. (1987). Self-regulatoryperseveration and the depressive self-focusing style: aself-awareness theory of reactive depression. Psycho-logical Bulletin, 102, 122±138.
Shah, I. (1974). Thinkers of the East. Harmondsworth:Penguin.
Simons, A. D., Murphy, G. E., Levine, J. L. and Wetzel,R. D. (1986). Cognitive therapy and pharmacotherapyfor depression: sustained improvement over one year.Archives of General Psychiatry, 43, 43±48.
Teasdale, J. D. (1993). Emotion and two kinds of meaning:cognitive therapy and applied cognitive science. Beha-viour Research and Therapy, 31, 339±354.
Teasdale, J. D. (1996). Clinically relevant theory: integrat-ing clinical insight with cognitive science. In: P. M.Salkovskis (Ed.), Frontiers of Cognitive Therapy. NewYork: Guilford, pp. 26±47.
Teasdale, J. D. (1997). The relationship between cognitionand emotion: the mind-in-place in mood disorders. In:D. M. Clark and C. G. Fairburn (Eds), Science andPractice of Cognitive Behaviour Therapy. Oxford: OxfordUniversity Press, pp. 67±93.
Teasdale, J. D. and Barnard, P. J. (1993). Affect, Cognitionand Change: Re-Modelling Depressive Thought. Hove:Erlbaum.
Teasdale, J. D., Segal, Z. V. and Williams, J. M. G. (1995).How does cognitive therapy prevent depressive relapseand why should attentional control (mindfulness)training help? Behaviour Research and Therapy, 33, 25±40.
Wells, A. and Matthews, G. (1996). Modelling cognition inemotional disorder: the S-REF model. BehaviourResearch and Therapy, 34, 881±888.
Zettle, R. D. and Hayes, S. C. (1987). Component andprocess analysis of cognitive therapy. PsychologicalReports, 61, 939±953.
Zettle, R. D. and Rains, J. C. (1989). Group cognitive andcontextual therapies in treatment of depression. Journalof Clinical Psychology, 45, 436±445.
Copyright # 1999 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. 6, 146±155 (1999)
Metacognition, mindfulness, mood disorders 155