TB CARE€¦ · • In Afghanistan, TB CARE I interventions (SOPs for case detection...
34
1 TB CARE I PROGRAM YEAR 2 Second Quarter Performance Monitoring Report January 1st, 2012 – March 31st, 2012 May 15, 2012 TB CARE
Transcript of TB CARE€¦ · • In Afghanistan, TB CARE I interventions (SOPs for case detection...

1
TB CARE IPROGRAM YEAR 2
Second Quarter Performance Monitoring ReportJanuary 1st, 2012 – March 31st, 2012
May 15, 2012
TB CARE

2
TB CARE I Partners
American Thoracic Society (ATS)FHI 360
Japan Anti-Tuberculosis Association (JATA)KNCV Tuberculosis Foundation (KNCV)
Management Sciences for Health (MSH)International Union Against Tuberculosis and Lung Disease (The Union)
World Health Organization (WHO)

3
ContentsList of Abbreviations ............................................................................................................................. 41.0 Introduction .............................................................................................................................. 62.0 Project Management Unit (PMU) .................................................................................................. 72.1 Knowledge Exchange .................................................................................................................. 73.0 Core projects ............................................................................................................................ 84.0 Country projects ........................................................................................................................ 18 PMDT ....................................................................................................................................... 18 GeneXpert ................................................................................................................................ 204.1 Afghanistan .............................................................................................................................. 204.2 Botswana.................................................................................................................................. 214.3 Cambodia ................................................................................................................................. 224.4 CAR-Kazakhstan ........................................................................................................................ 224.5 CAR-Kyrgyzstan ......................................................................................................................... 234.6 CAR-Uzbekistan ......................................................................................................................... 234.7 Djibouti .................................................................................................................................... 234.8 Dominican Republic .................................................................................................................... 234.9 Ethiopia .................................................................................................................................... 244.10 Ghana ...................................................................................................................................... 244.11 Indonesia ................................................................................................................................. 254.12 Kenya ...................................................................................................................................... 254.13 Mozambique.............................................................................................................................. 264.14 Namibia .................................................................................................................................... 274.15 Nigeria ..................................................................................................................................... 284.16 Pakistan ................................................................................................................................... 294.17 South Sudan ............................................................................................................................. 294.19 Uganda .................................................................................................................................... 294.20 Vietnam ................................................................................................................................... 304.21 Zambia ..................................................................................................................................... 304.22 Zimbabwe ................................................................................................................................. 315.0 Regional Projects ....................................................................................................................... 335.1 Center of Excellence (CoE) for PMDT ............................................................................................ 335.2 East Africa Supranational Reference Laboratory (SNRL) ................................................................... 335.3 ECSA (East, Central and Southern Africa) ...................................................................................... 335.4 Central Asian Republic (CAR) Regional Funding .............................................................................. 335.5 Central Asian Republic (CAR) Regional Funding .............................................................................. 33
TablesTable 1: Summary of visitors to the TB CARE I website .............................................................................. 7Table 2: Completed Year 1 Core Projects and Deliverables .......................................................................... 9Table 3: Overview of Extended Year 1 Core Projects .................................................................................. 11Table 4: Overview of Approved Year 2 Core Projects .................................................................................. 13Table 5: MDR-TB cases diagnosed by drug sensitivity testing (DST) and put on second-line drug treatment ...... 19Table 6: Number of Xpert tests performed ............................................................................................... 20Table 7: TB CARE I-funded procurements of GeneXpert instruments and cartridges ....................................... 20
FiguresFigure 1: Status of Approved Core Projects by Fiscal Year, .......................................................................... 8Figure 2: Map of TB CARE I countries ...................................................................................................... 18Figure 2: Results of SOP Implementation in Afghanistan ............................................................................ 21

4
List of Abbreviations
ACSM Advocacy Communication Social MobilizationAFB Acid Fast BacilliART Anti-retroviral TherapyBinfar Directorate General of Pharmaceutical and Medical Devices (Indonesia)BPPM Directorate of Medical Services (Indonesia)CAR Central Asian RepublicsCB-DOTS Community-Based DOTSCBTBC Community-Based TB CareCCM Country Coordinating MechanismCDC Center for Disease Control and PreventionCoE Center of ExcellenceCDR Case Detection RateCSO Civil Society OrganizationDEWG DOTS Expansion Working GroupDOT Directly Observed TreatmentDOTS Directly Observed Treatment Short CourseDR Drug ResistanceDRS Drug Resistance SurveyDST Drug Susceptibility TestingECSA East, Central and Southern AfricaEQA External Quality AssuranceERR Electronic Recording & ReportingFIND Foundation for Innovative New DiagnosticsGDF Global Drug FacilityGFATM Global Fund for Aids, Tuberculosis and MalariaGLC Green Light CommitteeGLI Global Laboratory InitiativeHIV HumanImmunodeficiencyVirusHMIS Health Management Information SystemsHRD Human Resource DevelopmentHSS Health System StrengtheningIC Infection ControlIEC Information, Education and CommunicationIQC Internal Quality ControlILEP International Federation of Anti-Leprosy AssociationsJATA Japan Anti-Tuberculosis AssociationJSM Joint Strategic MeetingKANCO Kenya AIDS NGOs ConsortiumKAPTLD Kenya Association for Prevention of TB and Lung DiseasesKIT Royal Tropical Institute KNCV KNCV Tuberculosis FoundationLED Light Emitting Diode (microscopy)LPA Line Probe AssayMDR Multi Drug ResistanceMDR-TB Multi Drug Resistant Tuberculosis M&E Monitoring and EvaluationMOA Memorandum of AgreementMoH Ministry of HealthMOST Management & Organizational Sustainability ToolMSF Médecins sans Frontières (Doctors without Borders)MSH Management Sciences for HealthNAP National Aids ProgramNCE No-Cost ExtensionNGO Non-Governmental OrganizationNIHE National Institute of Health and Epidemics (Vietnam)NTP National TB ProgramNRL National Reference LaboratoryNTRL National Tuberculosis Reference LaboratoryOPD Out-patient DepartmentOR Operations ResearchPCA Patient Centered ApproachPITC Provider-Initiated Treatment and CounselingPHCC Primary Health Care CenterPLHIV People Living with HIVPMDT Programmatic Management of Drug-resistant TuberculosisPMU Program Management UnitPPM Private Public MixPPP Public Private PartnershipRIF Rifampicin

5
QMR Quarterly Monitoring ReportSANAS South Africa National Accreditation SystemSLD Second Line DrugSNRL Supra National Reference LaboratorySOP Standard Operating ProceduresSS+ Sputum Smear positiveSS- Sputum Smear negativeTA Technical AssistanceTB TuberculosisTB CAP Tuberculosis Control Assistance ProgramTBCTA Tuberculosis Coalition for Technical AssistanceTB IC TB Infection ControlTBIS TB Information SystemTOT Training of TrainersTFM Transitional Funding MechanismTWG Technical Working GroupUSAID United States Agency for International DevelopmentUVGI Ultraviolet Germicidal IrradiationWHO World Health Organization

6
1. Introduction TB CARE I is happy to present USAID with the quarterly monitoring report for the January-March 2012 quarter of the TB CARE I program. This timeframe covers the second quarter of Year 2, including also some projects with an approvedextensionfromYear1.FifteencountriesbeganorcontinuedimplementingYear2workplanswhilefivecountries continued Year 1 activities. One new country was added to TB CARE I’s portfolio (Uganda), where the Year 2 workplan has started.
Ten Year 1 core projects were completed or continued this quarter. In addition, 22 Year 2 core projects continued and13newYear2coreprojectswerelaunched.Ofthefiveregionalprojects,fourreceivedapprovaloftheirYear2workplansinJanuary(oneprojectremainsjustYear1funding).Thisreportprovidesatechnicalandfinancialupdate on progress made during the quarter for TB CARE I core, regional and country projects. Below is a brief summary of TB CARE I’s main achievements to date and challenges for the next quarter.
Main Achievements: • GeneXpert use continues to gain momentum. Eight TB CARE I countries have procured a total of 41 Xpert
machines to date and 26 more machines are expected to be purchased in Year 2. Testing has begun in Cambodia, Indonesia, Kenya and Nigeria where a total of 933 Xpert tests have been conducted as of March 2012.
• The Pakistan TB prevalence survey was completed. Preliminary results have been presented, which indicate that theprevalenceofdefinitepulmonaryTBcasesinPakistanis295/100,000adultpopulation.
• In Afghanistan, TB CARE I interventions (SOPs for case detection implementation, TBIC and innovative approachessuchCB-DOTSandUrbanDOTS,etc.)resultedinsustainingahighercasenotificationtrendinAfghanistan. Thus, in 2011, in TB CARE I intervention provinces there was a 5% (700 cases) increase in all TB casenotificationcomparedto2010.Conversely,therewasa7%(762cases)declineinnon-TBCAREIprovincesfor the same period.
• InCambodia,WHO/TBCAREIassistedtheNTPtosuccessfullyadvocateforandsecureathree-yearadultTB drug grant from the Global Drug Facility (GDF) and continue the current grant for children’s drugs for one more year. TB CARE I also conducted a vulnerability analysis of the National TB Program (NTP) following the cancellation of Global Fund (GF) Round 11.
• In Indonesia, four GeneXpert machines started full operations in March 2012, while one other machine will be operational starting in April. As of March, 116 suspects have been examined using GeneXpert; 84 were confirmedasTBpositive,andamongthem43wereconfirmedrifampicinresistant.Allconfirmedrifampicinresistant cases were referred to the local PMDT treatment center; 27 have already been put on treatment (63%), 7 are still in the pre-enrollment phase, 1 died before treatment could be started and the remaining 8 were lost to follow-up or refused treatment.
• TB CARE I-Dominican Republic together with the NTP initiated a partnership with the Government´s Hotline to incorporate information on TB services, diagnosis and treatment. TB CARE I provided training and technical assistance (TA) to the Government’s Hotline to guarantee the dissemination of high quality information.
• In Mozambique, 8,751 TB suspects were referred to health facilities as a result of community volunteer activities.Ofthese,755werepositivelydiagnosedthroughsmearmicroscopyashavingactiveTB,299asTB/HIVco-infectedand230asmalariapositive.TheexistenceofmalariaconfirmedcaseshighlightsthepositiveresultsoftheTBCAREIintegratedTB/malariaapproachinthecountry.
• World TB Day (WTBD) was commemorated with support from TB CARE I in numerous project countries. Highlights include celebrating WTBD in Afghanistan in 320 public and private health facilities, launching a TB CARE I-renovated prison health post in Cambodia and an MDR-TB ward in Nigeria, organizing radio programs in Ethiopia and supporting a walk-a-thon and fun-bike that was attended by over 8,000 people in Indonesia. Four cured TB or MDR-TB patients from TB CARE I countries (Ethiopia, Kenya, Namibia and Vietnam) visited Washington DC to speak at a USAID-sponsored event for World TB Day.
• The Guide on Electronic Recording and Reporting for TB Care and Control has now been published and is available on the TB CARE I and WHO websites.
• The Ndola district TB IC demonstration site project was launched in January in Zambia. Baseline assessments of the 15 health facilities were completed and 13 of these facilities developed TB IC implementation plans using the CDC assessment and analysis tools.
Main Challenges and Next Steps: • Although many projects have made gains in accelerating workplan implementation after delayed starts to Year
2 workplans, this pace needs to be maintained or further accelerated to ensure timely and thorough completion of Year 2 workplans, particularly for country projects. Spending is not keeping pace with technical activity completion, resulting in a growing pipeline for the program. Financial reporting will be closely examined to identify savings and accruals; accelerated spending and activity completion will be encouraged. A new system for tracking and reprograming country project savings has been implemented, which will hopefully help to remedy the country pipelines.
• The ongoing security situation in Nigeria resulted in the TB CARE I Country Director resigning. The Senior Technical Advisor for Program Management (Dr. Mustapha Gidado) has been acting Director since her departure. Activities continue to be negatively impacted by the security situation as well.

7
2. Project Management Unit (PMU)
A USAID-hosted Joint Strategic Meeting (JSM) between TB CARE I and TB CARE II was conducted in February 2012 in Washington DC. The meeting provided the projects with an opportunity to present and discuss the progress/resultsofkeyYear1coreandcountryprojectstodate.TheAdvisoryGroupsforeachtechnicalareaalsomet to discuss the strategic direction of each technical component and priority areas for future core projects. The meeting proved to be very productive in focusing on the larger strategies and technical approaches of the projects, while also providing an opportunity to strengthen collaboration between the two projects. The salary of Advisory Group members’ participation in the JSM and follow-up discussions was supported with Year 2 core funds.
Following the JSM, TB CARE I held a partners meeting, which focused more on the managerial aspects of the program as opposed to the technical strategy. A list of action points was generated during the meeting and the PMU is following up to ensure all items are addressed by the appropriate parties.
TheTBCAREIOperationalManualhasbeensignificantlyrewrittenandupdatedthisquarter.Thiswasdonetobetter describe and update program policies, procedures and guidelines.
Anewsystemfortrackingandreprogramingcountryprojectsavingshasbeenimplemented.Themodificationtracker (MoT) has been developed to speed up the process of identifying savings, reallocating these funds and obtaining approval for the changes.
Technical Assistance (TA) visits by PMU staff this quarter included:
Country: Purpose:
Cambodia GeneXpert
Ethiopia Infection control
Indonesia Infection control; GeneXpert
Kenya Program management
Mozambique Workplanning/programmanagement
Nigeria Joint International Monitoring Mission; GeneXpert
Switzerland PMDT/totaldrugresistance
Uganda Workplanning
Washington DC, USA TB CARE Joint Strategic Meeting and TBCARE I Partners Meeting
2.1 Knowledge Exchange
The TB CARE I website has continued to gain traction, with a 33% increase in visitors this quarter (Table 1).
Table 1: Summary of visitors to the TB CARE I website:
Number of visitors October-December 2011 January-March 2012
Percent that were new visits 2,700 3,604
Number of countries visitors came from 100 110
Number of Pages Viewed 7,940 10,612
Percentage of new visitors 67% 70%
Most Popular Downloads 1. TB-IC at Community Level Training Handbook (60)2. TB-IC Facilitators Guide (46)3. TB CARE I Year 1 QMR 3 April 2010 June 2011 (45)4. TB CARE Brochure (43)5. Rapid Implementation of Xpert MTB-RIF Diagnostic Test 406. TB CARE I Newsletter April 2011 (37)7. TB CARE I Newsletter February 2012 (32)8. A Guide to Monitoring and Evaluation for Collaborative 9. TB/HIVActivities(27)10. TB CARE I Year 2 QMR Oct 2011-Dec 2011 (25) 11. Compendium of Indicators for Monitoring and Evaluating National
TB Programs (24)
The second TB CARE I newsletter was released in February 2012 in a new 4-page PDF format. The newsletter has so far been viewed 745 times (12% higher than the average for similar organisations who use the same electronic distributor) and 8.8% higher than previous mailings.
http://www.tbcare1.org/publications/toolbox/recent/TB_CARE_Newsletter_February2012.pdfWorld TB Day 2012

8
World TB Day was celebrated in many TB CARE I countries with events ranging from community meetings to races. Four cured TB or MDR-TB patients from TB CARE I countries (Ethiopia, Kenya, Namibia and Vietnam) visited Washington DC to speak at a USAID-sponsored event for World TB Day. A slideshow of some of the events can be seen here:http://www.tbcare1.org/wtbd/
New TB CARE I Tools:A number of new TB CARE I publications have been released this quarter:
Electronic Recording and Reporting for TB Care and ControlThis guide provides practical advice for countries planning to introduce electronic recording and reporting systems, or to enhance existing systems. It is intended for people likely to be involved in the design and implementation of electronicrecordingandreportingsystemsforTBcareandcontrolsuchasNTPManagers,ProcurementOfficers,LegalOfficers,ProjectManagers,SoftwareDevelopers,HealthInformationSystemManagers,ConsultantsandTechnical Agencieshttp://www.tbcare1.org/publications/toolbox/tools/me/Electronic_recording_and_reporting_for_tb_care_and_control.pdf
TB CARE I Newsletter February 2012http://www.tbcare1.org/publications/toolbox/recent/TB_CARE_Newsletter_February2012.pdf
TB-IC at Community Level Training Handbook Thehandbookisdesignedtofacilitatetheunderstandinganduseofthe‘SimplifiedChecklistforTBInfectionControl’,withaparticularemphasisonsettingswhereTB,HIVandTB/HIVareprevalenthasnowbeentranslatedin two new languages (Portuguese and French):
Controle de Infeccao por TB no Nivel Comunitario Um Manual de Treinamento (Portuguese)http://www.tbcare1.org/publications/toolbox/tools/ic/Controle_de_Infeccao_por_TB_no_Nivel_Comunitario_Um_Manual_de_Treinamento.pdf
Lutte contre la tuberculose au niveau communautaire manuel de formation (French)http://www.tbcare1.org/publications/toolbox/tools/ic/Lutte_contre_la_tuberculose_au_niveau_communautaire_manuel_de_formation.pdf
3. Core projects
As of March 31, 2012, 21 of the 28 Year 1 core projects (75%) have been completed and tangible deliverables are published on the website. Two Year 2 core projects have been completed (6%). Figure 1 summarizes the status of Year 1 and Year 2 core project completion as of this quarter. Table 2 lists all completed Year 1 core projects and their respective deliverables as of March 2012.
Figure 1: Status of Approved Core Projects by Fiscal Year, as of March 2012
0
5
10
15
20
25
30
35
75%
Ongoing
Year 1 Year 2
Completed
6%
7 33
221
Num
ber
of A
ppro
ved
Proj
ects

9
Table 2: Completed Year 1 Core Projects and Deliverables, through March 2012(all tangible deliverables are available on the TB CARE I website unless otherwise indicated; projects highlighted in orange have deliverables that were completed between January-March 2012)
Technical Areas
Code Lead Project Title Type of Deliverable
Outcome/Deliverables
Universal and Early Access
C1.1.1 KNCV Tool to identify TB most at risk and vulnerable populations Tool A compendium was generated detailing over 100 strategies linking key tools
and guidance to pertinent at-risk and vulnerable populations.
C1.1.5 KNCV Adapt and pilot patient centered package
Workshops Tworegionalworkshopswereimplementedwherethefivetoolsofthepatient-centered approach package were introduced. Cambodia, Indonesia, Mozambique, Nigeria and Zambia selected 2-3 tools each to implement in Year 2.
Laboratories
C6.1.1 KNCV Practical handbook for the development of a national laboratory strategy
Handbook A practical handbook for the development of a national laboratory strategy was developed.
C6.1.2 Union Tool for laboratory network assessment
Tool A draft tool for conducting lab network assessments was developed; piloting and training will take place in Year 2.
C6.2.1 KNCV Laboratory accreditation tools and roadmap
Toolbox Laboratory accreditation roadmap and toolbox have been developed (available on the GLI website: www.GLIquality.org).
C6.3.1 WHO Guiding and coordinating Xpert MTB/RIFimplementation
Guide ThedocumentRapidImplementationoftheXpertMTB/RIFdiagnostictest - Technical and Operational ‘How-to’ Practical considerations has been developed.
C6.4.1 WHO Assess quality of WHO-GLI SRLN and individual SRLs using GLI assessment tool
Tool The GLI assessment tool has been revised and is available on the GLI and TB CARE I websites.
C6.4.2 Union Develop Benin NRL in Africa to join SRLN
SRL candidate status
WHO has accepted the Benin NRL as a candidate SRL.
Infection Control
C3.1.1 WHO Develop a tool to measure TB incidence in HCWs
Guide Guides on monitoring active TB incidence among health care workers (HCWs) and conducting TB prevalence surveys among HCWs were drafted and will be finalizedinYear2.
C3.2.1 PMU Core Package of IC Interventions
Strategy AcoreTB-ICpackagewasagreedtoandfinalized(TBCAREIandIIcollaboration).
C3.3.2 KNCV Training and mentoring on TB-IC
Training & mentoredfield
visits
Twelveparticipantsweretrainedandnine(target)completedmentoredfieldvisits; three became TB-IC consultants and were registered on the TB TEAM website.
PMDT
C2.1.1 PMU Strengthening of regional and local technical collaboration centers (TCC) for PMDT
Assessment report
An inventory of strengths, weaknesses and challenges of existing TCCs was conducted. Technical assistance needs and possible scale-up approaches ofTCCswereidentifiedthroughdiscussionwithcurrentTCCsandotherstakeholders.

10
TB/HIV
C4.1.1 FHI 360 TB Infection Control at Community Level
Curriculum and guide
The TB Infection Control at the Community Level training handbook and the SimplifiedChecklistforTBInfectionControlweredeveloped.
C4.3.1 KNCV AssessmentofTB/HIVmortality data
Assessment report & tool
Assessment report "Learning from Loss" available. A new tool for the Patient-Centered Approach (PCA) on conducting a "Death Audit" has been developed.
Health Systems
Strengthening
C7.4.1 MSH Training national leaders on HRD Tools
Action plans Action plans on HRD are in place for six NTPs that participated in a virtual HRD training program (Afghanistan (2), Ghana, Indonesia, Pakistan, and Uganda).
C7.5.1 KNCV Build capacity of civil society in TB Control
Workplans Civil society organizations (CSOs) in Nigeria (4) and Indonesia (4) have developed and are implementing their TB control activity plans (continuing in Year 2).
M&E, OR and Surveillance
C5.1.1 WHO Guide on electronic recording and reporting for TB care and control
Guide The Guide on Electronic Recording and Reporting for TB Care and Control has been published and is available on the WHO and TB CARE I websites.
C5.2.1 MSH Develop M&E COP for NTPs Training A workshop "Using TB Information for Decision Making" was attended by 31 participants from 16 countries. Participants developed mini M&E plans for their countries, which will be implemented in Year 2.
Overarching Elements
C0.0.2 KNCV Support to CSHGP and CORE Group
Evaluation reports
Two evaluation missions for CORE Group (a coordinating body of US-borne private voluntary organizations) were implemented in India and Malawi.
C6.1.3 WHO Advisory Group members LOE Outcome indicators
TB CARE themes and outcome indicators were established for all technical areas with guidance from the Advisory Groups.
C6.1.4 WHO Training for Global Fund Round 11 Consultants
Training 42 consultants (36 TB CARE I-funded) were trained to provide quality technical assistance for Global Fund Round 11 proposal development.
Table 3 provides detailed information on the progress of the Year 1 core projects that are not yet complete. Table 4 summarizes progress on the Year 2 core projects that have been approved before or during the quarter (22 in total). Twelve Year 2 core projects are either still under review for approval or were approved after this reporting period.

11
Table 3: Overview of Extended Year 1 Core Projects, January 2012 to March 2012
Technical Area Code Lead Title Expected Year 1 Deliverables Progress to date %
completeLevel of
spending
TB/HIV C4.2.2 ATSWHO
Guidelines for evaluations of contacts to infectious cases of tuberculosis
•WHO-approvedset of guidelines developed
Thedraftdocumentisbeingfinalizedand will be submitted to the WHO Guideline Review Committee in February. Editing & printing will take place in March. A workshop with selected countries to outline and prepare national guidelines based ontheWHO/ATSguidelinesisthenplanned. A no-cost extension through June 2012 is being requested (March no-cost extension (NCE) already approved).
75% 84%
M&E, OR and Surveillance C5.1.2 WHO
JATA
Guide on inventory studies to assess the level of TB under-reporting
•Guideoninventory studies developed
The scope of the guidelines was broadened to make them more useful in a greater variety of contexts. The peer-review process will take place inAprilandthefinaltextisexpectedin June. A no-cost extension (NCE) is being requested through June 2012.
90% 45%
Laboratories C6.4.3
WHOKNCV,MSH,
The Union
Meeting of the SRLN
•MeetingofSRLN convened and consensus workplan and strategy developed
The meeting of the SRLN is planned and taking place April 17-19, 2012 in France as part of a three-day meeting on the SRL network, laboratory strengthening activities of the GLI partnersandXpertMTB/RIF.
75% 89%

12
Health System Strengthening
C7.1.1 WHOATS, FHI 360
Increased and sustained political andfinancialcommitment to TB prevention, care and control
•ImprovedTBplans, indicators and budget embedded within national health plansand/orstrategies.
The assessment of plans is ongoing. Spending will happen between May - September 2012. A NCE is requested through September 2012 25% 24%
C7.1.2 MSHMSH, WHO
Create political commitment and financingdatabase
•Politicalcommitment (measured by domesticfinancingfor TB) increased
The assessment of plans is ongoing. Spending will happen between May - September 2012. NCE is requested through September 2012.
25% 7%
C7.1.3 WHO
Meeting of the SRLN
•MeetingofSRLN convened and consensus workplan and strategy developed
The meeting of the SRLN is planned and taking place April 17-19, 2012 in France as part of a three-day meeting on the SRL network, laboratory strengthening activities of the GLI partnersandXpertMTB/RIF.
75% 89%
Overarching elements C0.0.1 WHO
The Union
Support to the Sub Working Groups of the Stop TB Partnership
•Strategicareasof work discussed and agreed on in seven groups•Reportsfromallmeetings available
The 4th GLI meeting is taking place April 17-19, 2012 in France. It is a three-day meeting on the SRL network, laboratory strengthening activities of the GLI partners, and progress with the implementation of theXpertMTB/RIF.
75% 96%

13
Table 4: Overview of Approved Year 2 Core Projects, January 2012 to March 2012
Technical Areas Code Lead Title Expected Year 2 Deliverables Progress to date %
completeLevel of
spending
Universal and Early Access
C1.1PMU, ATS, MSH
World TB Day Patient Panel
World TB Day Patient Panel Completed.100% 0%
C1.2
WHOKNCV, The
Union
Engaging pharmacists in TB care and control
- baseline assessment - documentation of working models- preparation of a tool to engage pharmacists in TB care and control
A site visit to Cambodia was undertaken in March and the report is being prepared. A visit to Ghana is planned for mid-May. The tool on engaging pharmacists will be prepared this summer with plans to present the tool at the PPM workshop in Dhaka in September.
50% 19x%
C1.4
WHOATS,
KNCV, The
Union
PPM Toolkit workshop
A multi-country global workshop of selected countries on the PPM toolkit
The PPM workshop will be organized in mid-September 2012 in Dhaka, Bangladesh. The technical content of the workshop is being designed and key speakers and facilitators are beingidentified.
40% 0%
C1.5WHO, The
Union
Update of WHO guidelines on Childhood TB management
Updated WHO Guidelines on Childhood TB Management
Thefirstdraftoftheupdatedguidelinesiscurrently being edited. Further WHO input will be sought in May followed by a formal guideline review and panel discussion in July.
10% 6%
C1.9 The Union
Childhood TB training
- ToT for 10 people - Training in 4 Districts in both countries
Progress slow. Training materials and evaluation tools are ready. Namibia NTP interested but prefers implementation in 2013. Indonesia also interested but wants some clarificationsofcontent.Ano-costextensionwill be requested.
10% 5%
C1.12 WHO
Guidelines on screening for active TB
Guidelines on TB screening Several systematic reviews of active TB screening questions are in progress with results due in May. A meeting will take place in May to review these results and draft recommendations.
50% 25%
C1.13
ATS, KNCV, MSH, WHO
ISTC ed. 2 review
Review of ISTC ed. 2. Decision made on the topics that need to be updated and/orrenewed
The Steering Committee is being formed.
10% 0%
C1.15 KNCV
Adapt and pilot PCA package
- Complete regional workshops from Year 1- Final report of pilot with results & recommendations for next steps, scale up and adaptation.
Cambodia & Mozambique have received ethical approval for the research component of the project and have begun data collection. Nigeria is delayed due to civil unrest in country and Indonesia is awaiting Year 2 approval. The coordination team will support Indonesia to coordinate the start-up of planned activities.
10% 0%

14
14
Universal Access
C1.16ATS
FHI 360, WHO
Develop contact investigation guidelines*
Development of WHO approved set of guidelines for evaluations of contacts to infectious cases of TB and enhancedexistingintensifiedactiveTBcasefindingstrategiesinPLHIVandchildren.
No updated provided this quarter
0% 40%
C1.17KNCV,
FHI 360, WHO
Scaling up engagement of prisons
- Regional workshop for 7 countries - Action plans to scale up engagement of prisons in TB control
Preparations have begun for the international workshop that is provisionally planned for October 2012. A NCE is needed to accommodate this October workshop date.
10% 2%
C2.1KNCV,
The Union
Lab strategic plan handbook
Practical laboratory strategic handbook,pilotedandfinalized
A visit was conducted to set-up the second pilot in Botswana, planned for June. The handbook and budgeting tool are being further developed for this pilot.
60% 16%
C2.2
The Union, KNCV, WHO
Tool for lab network assessment
A consensus tool for assessment and accreditation of microscopy laboratory networks is available, pilot tested by trained assessors and endorsed by GLI
Aworkshopwithallpartnersledtofinalizationof the tool. Pilot testing has started in Pakistan. 33% 24%
Laboratories
C2.3
KNCVMSH, The
Union
Lab management training of NRL staff
A 2-week laboratory training of 12 NRL lab staff from sub-Saharan Africa in Nairobi, Kenya
The workshop is being developed with participants and venue selected for the May 28-June 8 workshop in Nairobi. 20% 11%
C2.4KNCVMSH, WHO
Lab accreditation tools and roadmap
Improved, functional implementation guide (version 2.0) available for use by NTRLs for the implementation of a total quality management system leading to ISO 15189 accreditation
A performance indicator workshop was conducted related to the tool in January at KIT. The tool has been presented at the GLI meeting and is further being piloted in Benin.
70% 11%
C2.6
PMU-PEPFAR,
KNCV, WHO
GeneXpert phase 2
Workshop, document and tool A TA mission to Indonesia was done to assess six sites for Xpert readiness; 5 TB CARE I machines are now operational. A TA mission to Nigeria was done to perform supervision visits and set up the M&E system for impact evaluation; 9 TB CARE I machines are now operational. Generic training and implementation documents to guide NTPs were improved. The African Regional workshop for early implementers will be held May 21-25; the Asian Regional workshop for advanced implementers is planned for early September. A TA mission to Kazakhstan is planned for June to perform a TOT and set up the Xpert M&E system.
40% 14%

15
Laboratories
C2.7The
UnionKNCV
Develop Benin NRL to SNRL
- A functional supra-national TB reference laboratory (SNRL) in Benin- The Benin NRL accreditation process is advanced
ThefirstjointvisitwasmadetotheNigerNRL, which agreed to be linked to the Benin SRL. Negative pressure was installed at the Cotonou NRL. The accreditation activities were supported and three staff members were trained in internal auditing according to ISO15189. Data collection tools and map prototypes were developed for GIS.
50% 15%
C2.8 The Union
Uganda TB Supra National Reference Lab
The Uganda NRL has started functioning as a SRL, integrated in the network (SRLN) as designated SRL, and actively linked with 2 countries in its area
Further contacts were made to identify SRL links. Joint visits and training were planned.
25% 15%
Infection Control
C3.1
PMUJATA,
FHI 360, KNCV, MSH, The
Union, WHO
Testing of guide for TB among HCWs
field-testedguideline After the selection of three countries in different regions (Cambodia, Ghana, and Kyrgyzstan), FHI 360, KNCV and URC will beresponsibleforfieldtestingtheguideinCambodia, MSH and PIH in Ghana, and Project Hope and KNCV in Kyrgyzstan. Field testing in Cambodia and Ghana are planned for April; Kyrgyzstan is planned for May.
25% 9%
C3.2
PMUFHI 360, KNCV, MSH
TB-IC Core package
TB-IC 'core package' strategy has been adapted and adopted in 15 health facilities of Ndola district (Zambia)
Project preparations progressing, including planning of a TA visit, identifying local counterparts at all levels of the Ministry of Health (MoH) and sharing draft IEC materials.
20% 9%
C3.3KNCVMSH, WHO
TB-IC training - Organize and conduct training and workshop in TB-IC for 12-20 participants from EMRO & Asia, in Indonesia participants from EMRO & Asia, in Indonesia Providementoredfieldvisitsto8consultants from the workshop Provide distance support to consultants
A refresher course on infection control was conducted in late January in Jakarta, Indonesia. The training was attended by 16 participants from 14 different countries. Based on selection criteria and observation of the facilitators, the eight most promising participants were selected formentoredfieldvisits.Sincethetraining,twomentoredfieldvisitshavetakenplaceandanother three are in preparation. KNCV has created an e-portal to connect all trained IC consultants for further distant support.
80% 64%
C3.5
PMU-PEPFARFHI 360,
KNCV
TB-IC demonstration Ndola district
End-evaluation study reports to describe approaches and demonstrate results
With the project launched in January, baseline assessments of the 15 health facilities (HFs) were completed. Key HF staff were trained inTBIC.Affiliatedcommunityvolunteerswere trained in community-based TB IC & administeringtheSimplifiedChecklist.13outof 15 facilities developed their implementation plans using the CDC assessment and analysis tools.
25% 29%

16
PMDT
C4.3MSHATS, WHO
Cost effectiveness modeling for MDR-TB treatment
- Tool completed- Advocacy materials
The design work has started and the tool development and testing will start in Indonesia in May. 25% 7%
C4.4
KNCVJATA, MSH, WHO
Assessing the costs faced by MDR -TB patients
- Development and validation of tool- Validation of tool -Consensusworkshoptodefinepolicyrecommendations (2013)
The scope of the tool has changed to include non-MDR-TB patients. The protocol and questionnaireareinfinaldraftstage.Countrieshave been approached to start planning for implementationofthetool.Pre-testing/piloting planned for Ethiopia in July.
20% 6%
C4.6TB CARE
II-4.3KNCV
DR TB Learning site
On-line PMDT training program for clinicians and program managers
The site for online case series is developed and functioningathttp://tbta.co/cases.The online functionality and the format of the “discussion” is being updated. Jacques van den Broek and Ieva Leimane (KNCV) joined the expert panel. TB CARE II and I experts will provide comprehensive responses to case discussions.
50% 61%
C4.7TB CARE
II-4.1KNCV
PMDT management training course
A training of three days around the WHO Guide, Management of MDR-TB: Afieldguide
The 3-day training course on the management ofMDR-TB/HIVco-infectionwillfocusondistrict-level practitioners, will include basic clinical protocols dealing with MDR-TB and ART and will include cases from the TB CARE clinical case discussion series. A draft version of the coursewillbecirculatedinJunewiththefinalproduct planned for early September.d.
0% 0%
C4.8
TB CARE II-4.6
The Union
Tools for tracking DR-TB suspects
Review of existing tools AfirstdraftforreviewisexpectedinMay.TBCARE II will then pilot it in Bangladesh. 0% 0%
Health Systems
Strengthening
C6.8 ATSMSH
Improved domestic financing
Technical assistance and mentoring will be provided to selected workshop participants
The workshop has not yet been scheduled--see Year 1 (7.1.1 and 7.1.2). 0% 19%
C6.9KNCV,
ATS, FHI 360
Build capacity of civil society in TB control
Revised training curricula, Post graduate curriculum Union conference, M&E framework including project results
Training curricula have been reviewed for utilization in Ethiopia and distance support has been provided to Ethiopia and Nigeria. A reporting tool has been developed and the M&Etoolwassimplifiedduetoinsufficientand complex reporting in Year 1. The Ethiopia training course will take place next quarter.
25% 59%

17
Health Systems
StrengtheningC6.11 PMU
Support to CSHGP and CORE group
Evaluationreportformid-termorfinalevaluations of selected CORE Group fieldprojects
Two mid-term evaluations are planned for this year to Zambia and Mozambique in the third quarter of Year 2. An external consultant has been contracted and preparations are taking place.
10% 0%
M&E, OR and Surveillance
C7.2 KNCV
Finalization of Prevalence Survey report Pakistan
Prevalencesurveyfinalized The Data Management Unit received support from Nico Kalisvaart. Jeroen van Gorkom attend the project close out and TB prevalence survey preliminary report sharing ceremony in March. Data analysis backstopping support was provided. Discussions underway on publication of survey results.
30% 21%
C7.5MSHKNCV, WHO
Support M&E efforts of NTPs
-A community of practice (CoP) will be established -Test and pilot in 2 TB CARE countries (one each in Asia and Africa) virtual and in-person training materials on TB data management
The eRoom CoP has been set up and access grantedtoparticipants.Thefirsttrainingsareplanned for February and March. Following the workshop in The Hague (Year 1), 13 country teamsfinalizedmini-M&Eworkplans,whichare being implemented. The data management training materials outline has been developed.
20% 5%
C7.6 MSH
GIS for managing human resources
A GIS tool which can be used for managing HR requirements, identify and visually display HR gaps and training needs, and develop training plans based on disease burden, and facilitiesformanagingTBinadefinedarea. People trained in the use of the GIS tool
After recent approval, Ethiopia was selected for implementation of the pilot. An initial visit is being planned to meet with stakeholders and definetheend-userrequirementsfortheGIStool. 10% 2%
C7.7WHO, The
Union
Improving the estimates of childhood TB
A featured in-depth analysis of childhoodTBcasenotificationsinthe2012 WHO Global TB Control Report. An approach for countries to identify gaps in the childhood TB activities of their surveillance systems that need to be addressed.
Thein-depthanalysisofnotificationdatafromthe WHO Global TB Database is advancing wellwiththeproductionofafirstsetofglobalestimates for childhood TB mortality, incidence and associated limitations. A questionnaire is being drafted for targeted countries to allow for the further collection of childhood TB activities and surveillance data not reported to WHO.
25% 4%
Overarching
C0.1 PMUPrinting of report to Congress
Reports printed and distributed. Completed.100% 100%
C0.2 PMU
Advisory Group member LOE
Advisory groups met during the Joint Strategic Meeting in Washington DC in February to discuss priorities for core projects in Year 3. Follow-up calls are also being held as needed.
50% 0%

18
4. Country projects
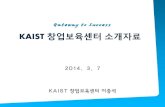
A new country was added to the TB CARE I portfolio this quarter (Uganda), bringing the total number of countries to21.Senegal’sworkplanisstillindevelopment.Basedonapprovedextensions,fivecountriesarereportingon Year 1 workplans while the remaining 15 are reporting on Year 2 activities. Figure 2 displays the geographic distribution of TB CARE I countries.
Figure 2: Map of TB CARE I countries, as of March 2012
Afghanistan
KazakhstanKyrgyzstan
Uzbekistan
Nigeria
Botswana
Pakistan
Ghana
Dominican Republic
Senegal
Cambodia
Djibouti
Ethiopia
IndonesiaNamibia
KenyaUgandaMozambique
South Sudan
Vietnam
Zambia
Zimbabwe
PMDT
PMDT scale-up at country level continues to be a priority for TB CARE I. Therefore, national data on MDR-TB cases that were diagnosed and put on treatment are collected each quarter. Table 5 summarizes the available information for 2010, 2011 and Jan-Mar 2012 by country. In total, 10,441 MDR-TB cases were diagnosed in TB CARE I-supported countries and 8,017 were put on treatment in 2010. In 2011, 9,693 cases were diagnosed and 8,044 were started on treatment. However, the reporting of Uzbekistan MDR data in 2010 and not in 2011 affects these totals. When Uzbekistan numbers are removed from the sum (new totals of 9,418 diagnosed cases and 7,389 cases initiating treatment in 2010), a 3% increase in MDR-TB diagnosis and a 9% increase in treatment initiation between 2010 and 2011 for TB CARE I countries is seen. In fact, 12 countries show an increase in the number of MDR patients put on treatment from 2010 to 2011 (Afghanistan, Cambodia, Djibouti, Ethiopia, Indonesia, Kenya, Mozambique, Nigeria, Pakistan, Uganda, Vietnam, and Zimbabwe), while six countries show a decline in MDR-TB treatment (Botswana, Dominican Republic, Ghana, Kazakhstan, Kyrgyzstan and Namibia). Another positive trend is the proportion of diagnosed patients put on treatment. While the cohorts for ‘diagnosed’ and ‘put on treatment’ are not equal, doing a rough comparison shows treatment coverage improving from about 77%in2010to83%in2011(89%forthefirstquarter2012).
TheavailabledataindicatesapositivetrendinPMDTscale-up,howeversignificantworkstillneedstobedoneto diagnose more MDR-TB cases and to close the gap between diagnosis and treatment. A continuing problem is the timeliness, completeness and reliability of reporting; as seen in Table 5, most countries do not yet have data available for the current quarter.

19
Table 5: MDR-TB cases diagnosed by drug sensitivity testing (DST) and put on second-line drug treatment during 2010, 2011 or 2012 by country, as of March 2012
Countries
Jan - Dec 2010 Jan - Dec 2011 Jan - March 2012
CommentsNumber Diagnosed
Number put on
Treament
Number Diagnosed
Number put on
Treament
Number Diagnosed
Number put on
Treament
Afghanistan 19 0 22 22 5 5
Botswana 106 92 46 44 N/A N/A
Cambodia 31 41 56 83 N/A N/A# put on treatment includesconfirmedandsuspected cases
Djibouti 8 8 73 12 N/A N/A
Dominican Republic 108 108 85 85 N/A N/A
Ethiopia 140 85 136 214 16 91
Ghana 14 2 10 1 0 0
Indonesia 182 142 326 248 131 72Jan-Mar 2012 cases include those diagnosed with Xpert
Kazakhstan 7,336 5,740 7,386 5,311 1,902 1,342
Kenya 112 59 130 130 21 21All diagnosed MDT-TB cases on treatment according to NTP
Kyrgystan 441 441 423 423 N/A 160
Only MDT-TB cases on treatment are registered. About 700 MDR-TB cases ar not on treatment and are not registered.
Mozambique 165 86 184 146 N/A 58
Namibia 222 222 198 198 N/A N/A
Diagnosed MDR-TB case unavailable due to electronic system which captures the number of samples tested rather than cases. TB CARE I is working with NTP and CDC to modify the R&R system.
Nigeria - OP U 23 92 61 54 12
Pakistan 203 203 344 344 N/A N/A
South Sudan 3 0 3 0 0 0
The NTP will only provide data once registration is complete
Uzbekistan
Vietnam 202 101 N/A 578 N/A 128
Zambia N/A N/A N/A N/A N/A N/A
R&R tools for PMDT are not yet available. TheNTPhasfinalizedthe tools and TB CARE I plans to make them available to the teo PMDT treatment sites in the next quarter.
Zimbabwe 40 27 108 73 37 38
Total 10,441 8,017 9,693 8,044 2,173 1,927
Total Excluding Uzbekistan
9,418 7,389 9,693 8,044 2,173 1,927
3% increase in diagnosis and 9 % increase in treatment initiation between 2010 and 2011

20
GeneXpert
GeneXpert is used in the routine diagnosis of HIV positive TB suspects and MDR-TB suspects. TB CARE I is helping to introduce and scale-up GeneXpert use in several countries. Testing has begun in Cambodia, Indonesia, Kenya and Nigeria; Table 6 summarizes Xpert testing to date in these four countries. Implementation is expected in Djibouti, Kazakhstan, Mozambique, Vietnam, Zambia and Zimbabwe in the near future.
Table 6: Number of Xpert tests performed through March 2012
Country # Xpert tests performed
Nigeria 129
Indonesia 116
Kenya 531
Cambodia 157
Total 933
More detail on Xpert progress can be found in each respective country section. Below is a summary of GeneXpert instruments and cartridges procured through March 2012 and planned for Year 2 with TB CARE I funds.
Table 7: TB CARE I-funded procurements of GeneXpert instruments and cartridges (completed and planned in Year 2) as of March 2012
Countries # Instruments Procured
# Cartridges Procured
# Instruments Planned
# Cartridges Planned
Afghanistan 0 0 0
Botswana 0 0 0
Cambodia 2 2,000 1 3,000
CAR - Kazakhstan 4 3,120 0 2,880
CAR - Kyrgyzstan 0 0 0 0
CAR - Uzbekistan 0 0 0 0
Djibouti 0 0 1 2,060
Dominican Republic 0 0 1 0
Ethiopia 0 0 0 0
Ghana 0 0 0 0
Indonesia 17 1,700 0 0
Kenya 3 1,000 0 1,450
Mozambique 3 1,500 0 0
Namibia 0 0 0 0
Nigeria - OP 9 7,600 6 7,500
Pakistan 0 0 0 0
South Sudan 0 0 0 0
Uganda 0 0 0 0
Vietnam 2 2,700 15 10,000
Zambia 1 400 2 560
Zimbabwe 0 0 1 250
Total 41 20,020 26 27,700
Each TB CARE I country will now be briefly discussed in turn.
4.1 Afghanistan
MSH is the lead partner in Afghanistan with collaboration from WHO and KNCV; community-based DOTS activities are subcontracted to BRAC. The project works in universal and early access (UA), infection control (IC), health system strengthening (HSS) and monitoring & evaluation (M&E). Implementation of the Year 2 workplan began in January 2012.
TBCAREIinterventionsresultedinsustainingahighercasenotificationtrendinAfghanistan.Theinterventionssuch as SOPs for case detection implementation, TB IC and innovative approaches such CB-DOTS and Urban DOTS resulted in increased access to TB services. Thus, in 2011, in TB CARE I intervention provinces there was a 5%

21
(700cases)increaseinallTBcasenotificationcomparedto2010.Conversely,therewasa7%(762cases)declinein Non-TB CARE I provinces for the same period.
TB CARE I assisted the NTP to rapidly expand the TB information system (TBIS) database across the country. TB CARE I with TA from MSH (Tech Serve) unit trained eight individuals from NTP M&E and surveillance department as master trainers and focal points for TBIS database management, maintenances and trainers. From Jan-Feb 2012, a total of 111 individuals including provincial TB coordinators, provincial Health Management Information Systems (HMIS)officersandNGOHMISofficers,weretrainedonTBISdatabaseutilizationanddataentry.NTPAfghanistanimplementedthefirsteverelectronicreportingsystemin32outof34provincesandasaresultNTPreceivedthefirstelectronicreportsfrom27/32provinces.
TBCAREIprovidedtechnicalandfinancialassistancetotheNTPforcelebrationofWorldTBDayatprovincialandhealthfacility/communitylevels.WorldTBDaywascelebratedin320healthfacilitiesandfourprovinceswithassistancefromTBCAREIAfghanistanandforthefirsttimeprivatehealthfacilitieswereinvolvedintheWorldTBDay celebrations.
The TB IC initiative was introduced to the NTP during TB CAP and was continued under TB CARE I. During the quarter, 22 health facilities were newly covered by TBIC. Currently, there are 55 health facilities covered by TB IC committees.
Supervisory/monitoringvisitswereconductedbyTBCAREIduringJan-Mar2012toall13USAIDsupportedprovinces to ensure CB-DOTS implementation and CHWs performance. In addition, during sub-national review workshops, feedback on CB-DOTS performance is provided to BPHS implementers, action plans are made and community health workers’ performances are monitored.
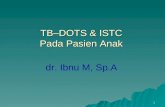
DOTSwasexpandedtosevenadditionalprivate/publichealthfacilities,includingorientationandtrainingof36staff. The NTP recording and reporting system was introduced and DOTS packages were delivered to them. 36 visits were conducted to ensure appropriate DOTS implementation. (Figure: Increase in examined TB suspects, 2008-2011.)
The Global Fund Round 8 Phase I was completed at the end of Sep 2011 and so far Phase II has not been approved. This put NTP and partners in challenging circumstances (i.e. delay in implementation and reduced motivation of NTP staff). Phase II approval is anticipated for late April 2012, however further delay will result in shortages of essential activities of the NTP including shortages of drugs, commodities, reagents and staff. Global Fund Round 10 for Afghanistan (PR: JICA) was approved and activities began late March 2012.
Figure 2: Results of SOP Implementation in Afghanistan
0
50000
100000
150000
200000
85,105
2008 2009 2010 2011
98,443
154,500
195,275
Num
ber
of T
B S
uspe
cts
Years
4.2 Botswana
KNCV is the lead partner and sole implementer in Botswana. In Year 2 the project focuses on universal and early access and laboratories. TB CARE I supported the development of a costed Global Fund Transitional Funding Mechanism (TFM) proposal through in country and international TA. A regional budget expert hired by TB CARE I supported the costing of the TFM proposal.

22
TheBotswanaNTRLreceiveditscertificateforaccreditationfromtheSouthAfricaNationalAccreditationSystem(SANAS). TB CARE I will support continued maintenance of accreditation status.
The in-country TB CARE I Senior Technical Advisor has provided technical support to the TB program focusing onthekeytechnicalareas:communityTBcare,PMDT,TB/HIV,TBIC,PPMDOTSandM&E.Hefacilitatedthedevelopment of a comprehensive annual performance plan for 2012-2013, supported the development of promotional materials and helped organize the commemoration of World TB Day 2012.
4.3 Cambodia
JATA is the lead partner in Cambodia, with collaboration from FHI 360, KNCV, MSH and WHO. In Year 2, the project hasactivitiesinsevenTBCAREItechnicalareas(UA,laboratories,IC,PMDT,TB/HIV,HSSandM&E).
TB CARE I organized an event in Correctional Center 3 (CC3) prison to mark World TB Day and inaugurate the prison health post renovated with TB CARE I funds. Around 560 prisoners from CC3 prison, various government institutions, USAID Cambodia and development partners attended this event. (Photos: The CC3 prison health post before (left) and after (right) TB CARE I-funded renovations).
TB CARE I continued expansion the of childhood TB activities to cover 15 operational districts (ODs). During the quarter 7,526 children were referred by health centers and CB-DOTS partners to referral hospitals for a complete diagnostic work up such as clinical examination, tuberculin skin test, and x-ray examination. Of those, 973 were diagnosed as childhood TB (42% female).
Theprojectfacilitatedthefirstoperationalresearch(OR)trainingcourse.ParticipantsidentifiedfourORtopicsanddeveloped protocols with assistance from the course facilitators and local mentors.
The e-TB manager tool customization process was initiated in January. Initial versions of the tool began being tested during the quarter.
TB CARE I assisted the NTP to successfully advocate for and secure a three-year adult TB drug grant from the Global Drug Facility (GDF) and continue the current grant for children’s drugs for one more year. TB CARE I also conducted a vulnerability analysis of the NTP following the cancellation of Global Fund (GF) Round 11. The prolonged negotiations for GF Round 7 Phase 2, have delayed the disbursement of funds by more than a year (start date of April 2011 with funds expected in April 2012).
4.4 CAR-Kazakhstan
KNCV is the lead and sole implementer of TB CARE I activities in all three Central Asian Republic (CAR) countries: Kazakhstan, Kyrgyzstan and Uzbekistan. There is also a small CAR regionally-funded project which is discussed on page 40. All three CAR country projects have activities in the eight technical areas (UA, laboratories, IC, PMDT, TB/HIV,HSS,M&Eanddrugsupplyandmanagement).EachofthesecountriesalsohadanapprovedNCEthroughMarch 2012 for the Year 1 workplans.
An assessment of facilities for selection of Xpert sites was conducted in Akmola oblast. Kokshetau City of Akmola oblast was selected as a pilot site for Xpert introduction. A draft MoU on implementation of Xpert in Kazakhstan was developed to clarify the NTP’s responsibility for implementation, supply and maintenance of Xpert, as well astheprovisionofadequatetreatmentfordetectedTBandMDR-TBcases.TheXpertMTB/RIFimplementationplan and clinical laboratory protocols have been approved by the NTP. Four 4-module Xpert machines are being procured.
ATB/HIVprotocolhasbeendevelopedandsenttoMoHforapproval.TheORprotocolontheeffectivenessofpatient support in East Kazakhstan was drafted.

23
4.5 CAR-Kyrgyzstan
A draft NTP «Tuberculosis IV» for 2012-2016 (a strategic plan) was discussed with the NTP and key partners, and submitted totheNTPforapproval.TheTB/HIVstrategicplanwasdrafted,discussed and submitted for revision to health care providers and partners.(Photo:AworkingmeetingforfinaldiscussionoftheNational Program «Tuberculosis IV», 2012-2016.)
Recording and reporting forms, the schedule of reporting, the chainofdatatransmissionandtheelectronicdatabaseonTBpatientswerediscussedandfinalizedinaworkingmeeting attended by numerous stakeholders. Guidelines on TB in children were discussed at a meeting in the Center of Development of Health Care under the MoH.
4.6 CAR-Uzbekistan
DuetothedelayedregistrationoftheKNCVbranchoffice,TBCAREIsecuredUSAID’sapprovaltoimplementactivities in Year 2 through WHO. Year 2 activities are expected to begin in May 2012.
4.7 Djibouti
WHO is the lead and sole implementer of activities in Djibouti. The Year 2 workplan focuses on UA, laboratories, PMDT, HSS, M&E and drug management. New TB treatment regimens in line with the new WHO guidelines were developed and were submitted for the approval of national stakeholders during a workshop organized by the NTP. While the workshop was organized by the MOH with funding from the World Bank, TB CARE I provided full TA locally.ThetreatmentrevisionwasdecidedbytheMoHuponrecommendationfromWHO/TBCAREI.
With TB CARE I TA, World TB Day materials were developed (health education messages, slogan, technical material for the media, a brochure on TB, address of the Minister of Health, address of the WHO Representative, analysis of the TB epidemiological situation and TB control activities).
In coordination with FIND experts responsible for the introduction of new rapid diagnostic technologies in the NRL, namely line probe assay (LPA), liquid culture and Strip Speciation, TB CARE I initiated the procurement of one 4-module GeneXpert instrument and test cartridges.
4.8 Dominican Republic
KNCV is the lead partner and sole implementer in Dominican Republic. Activities are conducted in UA, IC, PMDT, HSS and M&E. The project continues to implement the Year 1 workplan, which will run through April 2012. A new Country Director, Dr. Luis Alberto Rodriguez Reyes, began in January 2012.
The “Invisibles” Exhibition at the National Congress was attended by seven congresspersons, congressional staff, representatives of the press and over 150 students from a public high school. The exhibition was widely disseminated through TV channels, radio and print media across the country. The activity raised public awareness andincreasedthelevelofcommitmentamonghighlevelpoliticianstofightTB.Asaresultofthisitwasdecided
to send the exhibition on a tour around the country to contribute to higher community involvement and urge provincial political leaders to invest money in health care and TB in particular.
TB CARE I together with the NTP initiated a partnership with the Government´s Hotline to incorporate information on TB services, diagnosisandtreatment.Allcurrentandfutureprintedorfilmedmaterials for promotion, education or information produced by partners will be available through the TB Hotline. The Hotline can be reached free of charge from any landline or cellphone. This allows TB related information to be easily accessible to the general population. TB CARE I provided training and TA the Government’s Hotline to guarantee the dissemination of high quality information. (Photo: Call center operators after TB training during Hotline launch on World TB Day, 2012.)
Based on the example of the Community Stop TB Committee in Area 4, which was initiated by TB CARE I, over 35 Community Stop TB Committees are now operating in project selected provinces. Through capacity building, TB CARE I has encouraged people to form these committees that contribute to the increased access to health care services at the community level. The Community Stop TB Committees are particularly successful in the provinces in the south of the country and on the border with Haiti, which are among the poorest zones in the Dominican Republic. In addition, TB CARE I supported the creation of a Hospital Stop TB Committee within the biggest public

24
hospital in the country (Hospital José Ma. Cabral y Báez), which also has the most reported TB cases among health care staff (17 cases among HCWs in 2011). The Hospital Stop TB Committee has led to the refurbishment of TB services at this site including improved infection control. This mobilization has led to the inclusion of a TB CARE I IC Expert in the National Technical Group for Infections Control.
4.9 Ethiopia
KNCV is the lead partner in Ethiopia, working closely with collaborating partners MSH and WHO, as well as subcontractor German Leprosy and TB Relief Association (GLRA). The Year 2 workplan has activities in all eight technical areas. Mekele University hosted the 7th National TB Research Conference in March organized by the TB Research Advisory Committee (TRAC) under the theme “Effective partnership to combat TB: Rallying the forces in Ethiopia”. Morethanfiftyresearchpaperswerepresentedandpaneldiscussionswereheldonmaximizingthebenefitofthe TB control program through a Health Development Army, health system strengthening through the Stop TB partnership and the role of OR in TB control in Ethiopia. Like previous years, TB CARE I supported the conference bothtechnicallyandfinancially.SomeoftheTBCAREIsupportincluded:activityparticipationasamemberofthe national organizing Task Force, covering the cost of a video clip on TB produced in the local language which wasinauguratedonthefirstdayoftheconference,andsponsoringparticipantswhoattendedtheconference.TBCAREIwasawardedacertificateofappreciationfortheunreservedsupportoftheevent,aswellasrecognitionfrom USAID-Ethiopia for collaborating with the other USAID-funded programs (HEAL TB and Private Health Sector Project) to organize a successful event.
On the occasion of the 7th National TB Conference, a satellite session was conducted on OR, which was sponsored by TB CARE I. The objective was to set national OR priorities and design a road map to scale up OR in TB control. The main issues addressed included: current status of OR, opportunities & challenges, a priority agenda and future direction.
TB CARE I in collaboration with the Federal MoH organized a TB IC training for Engineers and Architects of MoH and Regional Health Bureaus. The training was tailored to address health facility design challenges of Ethiopia. Seventeen participants from Health Bureaus attended the February training workshop; at the end of the training, all participants agreed to consider air borne infection control issues during the health facility design stage and re-consider ways to improve the already built health facilities in their respective regions. They showed commitment to improve the national standard on the design of health facilities in Ethiopia.
The 2012 World TB Day commemoration was highly effective in conveying key messages to the public via electronic and print media. The role of the TB Media Forum (established with support from TB CAP) was crucial in disseminating these important messages in this commemoration through arranging a special booth on the role of Media in TB control. The TB Media Forum’s awareness on the basics of TB, TB DOTS, MDR-TB and IC is being refreshed continuously by TB CARE I. In effect, TB has become an issue of discussion among the public at large due to various ACSM activities such as the national weekly half an hour TB program of Radio Fana 98.1. (Photo: Awareness Walk on World TB Day.)
4.10 Ghana
MSH is the lead partner in Ghana with support from KNCV and WHO as collaborating partners. The Year 2 workplanfocusesonUA,laboratories,IC,TB/HIV,HSSandM&E.
As a part of data validation to address reported data inaccuracies and inconsistencies, TB CARE I demonstrated the systematic approach for conducting Regional TB Quarterly Review Meetings in the Eastern Region. TB CARE I introduced an innovative approach that involves TB Treatment Registers swapped among District TB Coordinators thus permitting them to review and validate each other’s data. This method of conducting review meetings exposedsomedifferencesbetweenthenumberofTBcasescompiledthroughregisterswapsandfiguresreportedto the regional level. This approach also revealed that most of District TB Coordinators have limited knowledge on thebasicprinciplesofTBcontrol(i.e.declaringSS+curedwithoutnegativesputumresultsattwomonths,fivemonths & end of treatment). Most differences were in TB-HIV data such as number of TB patients offered CPT and ART.ThesefindingshighlysuggesttheneedfortheNTPandTBCAREItofinalizethedevelopmentofthenationalTB guidelines and ensure that they are disseminated across the country. The NTP Central Unit has now made it a policy that all 10 regions should adopt this approach of conducting Regional TB quarterly Review meetings.
At the request of the Regional Health Management Team, TB CARE I supported the Eastern Region to perform a bottleneckanalysistoidentifythekeyreasonsforthedecliningcasenotificationandtreatmentsuccessrateinthe region over the last few years. One of the frequently mentioned reasons for the low TB case detection in the

25
region was the late presentation of TB suspects to health facilities. Many TB suspects preferred seeking care in Prayer/Regionscampsorshrinesbeforecomingtothehospital.TheNTPandTBCAREIneedtodevelopaclearstrategy for the referral of TB suspects from prayers camps to the hospital for early diagnosis and treatment.
TB CARE I has started supporting the Eastern Region to demonstrate the systematic approach for improving health facility TB case detection by scaling up the use of the SOPs for TB case detection developed under TB CAP. Two districts(LowerManyaKroboandKwaebibirim)havebeenidentifiedasthefirstdistrictstobesupportedduetothe presence of numerous large hospitals and microscopy sites. The implementation of systematic health facility TB case detection has started and TB CARE I is introducing TB suspect registers. Functional referral mechanisms for TB patients are being established. All hospital departments including out-patient and in-patients wards are being oriented to conduct early TB case detection.
4.11 Indonesia
IndonesiaisthelargestoftheTBCAREIcountriesintermsoffinancialobligations($10millionperyear);KNCVis the lead partner with close collaboration from ATS, FHI 360, JATA (as of Year 2), MSH, The Union and WHO. TB CARE I-Indonesia works in all eight technical areas. The project began implementation of the Year 2 workplan during this quarter.
FiveexistingC/DSTlaboratoriesforfirstlineandsecondlinedrugshavemaintainedtheirexcellentperformanceovertime.WithsupportofTBCAREI,fivenewC/DSTreferrallaboratoriesarepreparingtobecertifiedandamong them, three laboratories are doing panel testing under guidance of SNRL SA Pathology, Adelaide. Quality assurance results will be available at the end of Quarter 3.
Five GeneXpert machines have now been successfully installed after a comprehensive site assessment by CGAT (Country GeneXpert Advisory Team) with support from TB CARE I. In this quarter, on-site training was conducted to ensure the smooth functioning of the machines and implementation guidelines. Four machines started full operations in March 2012, while one machine beginning operation in April 2012. As of the end of March 2012, the totalnumberofsuspectsexaminedusingGeneXpertwas116;84ofthemwereconfirmedasTBpositive,andamongthem43wereconfirmedrifampicinresistant.Allconfirmedrifampicinresistantcaseswerereferredtothelocal PMDT treatment center and GeneXpert results were used to start PMDT immediately. 27 have already been put on treatment (63%), 7 are still in the pre-enrollment phase, 1 died before treatment could be started and the remaining 8 were lost to follow-up or refused treatment. After introducing this new technology, DR-TB case detectionincreasedsignificantlyinallimplementingsites.
Two new PMDT sites (Sanglah Hospital in Denpasar, Bali and Hasan Sadikin Hospital in Bandung) started operation this quarter. Screening of suspects started in January 2012. These two new sites will also be supported by GeneXpert implementation.
Two successful events related to the celebration of World TB Day were supported by TB CARE I. A national TB symposium, organized by the University of Indonesia, was attended by around 1,000 participants. A major public event was organized in Jakarta with about 8,000 people participants. TB CARE I supported a variety of activities including a walkathon, fun-bike, etc. The event was attended by the Coordinating Minister for Social Welfare, the Vice Minister of Health, the US Ambassador and several other partners. (Photo: TB Day Commemoration, Fun Bike and Walkathon, Jakarta.)
TBCAREIhassuccessfullysupportedtheengagementofhealthinsurancecompaniesinthefightagainstTB.Twolarge health insurance companies (PT. ASKES, mainly covering government employees and their families, and PT. Jamsostek, mainly covering private employees and families) now include insurance coverage for TB patients, consisting of support for TB diagnostics and TB treatment.
As a result of intensive efforts supported by TB CARE I, the main elements of the DOTS strategy and Hospital DOTS Linkage standards are now included in the national standards for hospital accreditation. These new accreditationstandardswereofficiallylaunchedbytheMinisterofHealthinFebruary2012.DOTSandHDLstandards are also included in the instrument for assessment of hospital accreditation.
4.12 Kenya
KNCV is the lead partner in Kenya; the collaborating partners are ATS, FHI 360 and MSH, and subcontracts are in place with the Kenya Association for Prevention of TB and Lung Diseases (KAPTLD) and Kenya AIDS NGOs Consortium (KANCO). As of Year 2, the project conducts activities in all eight technical areas; Year 2 workplan implementation began in January 2012.
ThethreeGeneXpertmachinesandaccompanyingequipmentthatTBCAREIprocuredwerethefirstGeneXpert

26
machines in the public sector. Installed in Coast Provincial Genera Hospital (Coast PGH), Port Reitz District Hospital and Likoni District Hospital, all within the Coast region, laboratory personnel were trained and clinicians sensitized to fully utilize the machines. There is good progress so far in the use of the GeneXpert machines although there is a need to sensitize more clinicians in the region.
The algorithm for GeneXpert testing was developed with TB CARE I support. From October 2011 to February 2012, a total of 531 samples have been tested. Out of these, 223 cases were MTB positive. 39 of these were new TB cases and 10 were Rifampicin (Rif) resistant (all of which were previously treated TB cases). All the 10 Rif resistant caseswereputonstandardizedsecondlineTBtreatment.SixofthetenwereconfirmedMDR-TBcasesbyHAINMTBDRplus;outofthe6,2havebeenconfirmedbyMGIT960DSTwhileconfirmationfortherestisongoing.
TB CARE I is supporting the Division of TB, Leprosy and other Lung Diseases to provide accessible, quality laboratory services in the country. TB CARE I procured 17 LED microscopes to be distributed to high volume TB diagnostic facilities countrywide in addition to the previous 20 already-procured instruments (37 in total).
TB CARE I continues to support TB supervision at all levels of the health system. Monthly district supervision coverage improved in January 2012 (81%) compared to October 2011 (76%), November 2011 (74%) and December 2011 (64%). February and March 2012 supervision will be reported next quarter.
MDR-TB contact tracing has started. This quarter, 17 contacts of MDR-TB patients were traced and screened for TB. 21MDR-TBcaseswereconfirmedthisquarterresultinginanestimated84contacts(fourpercase)thatshouldbescreened.
4.13 Mozambique
FHI 360, the lead partner for Mozambique, managed two separate TB CARE I workplans in Year 1: one for malaria activities,andoneforTBactivities.TheTBworkplanfocusesonUA,laboratories,IC,PMDT,TB/HIV,HSSanddrugmanagement. FHI 360 works with collaborating partners KNCV, MSH and WHO on the TB workplan. The Year 1 workplans had a NCE through March 2012.
TB workplan:
All 36 target districts for Year 1 have been covered by nine implementing partners for CB-DOTS implementation. TA was provided to World Relief, Kulima, AMODEFA Gaza and Zambezia, CUAMM, and ADPP Sofala and Manica. The support was focused on building their capacity to implement CB-DOTS as well as monitoring of activities including data collection, documentation and reporting. Through the partnership with the nine implementing NGOs, a total of 549 volunteers, 21 health practitioners and 75 traditional healers were trained in CB-DOTS management this quarter.Inaddition,19healthstaffatperipheralhealthfacilitiesweretrainedonslidefixation.Fromactivitiesimplemented by community volunteers, 8,751 TB suspects were referred to health facilities. Of these, 755 were positively diagnosed through smear microscopy as having active TB, 303 were diagnosed with sputum smear negativeTB,59diagnosedashavingextrapulmonaryTB,299asTB/HIVco-infectedand230asmalariapositive.TheexistenceofmalariaconfirmedcaseshighlightseffortsbeingtakenaspartoftheTBCAREIintegratedapproach in addressing TB and Malaria. The planning exercise for CB-DOTS expansion to new districts in Year 2 was also completed and an additional nine districts were selected in close collaboration with provincial health directorates and NTP, resulting in a total of 45 districts providing CB-DOTS services by the end of March. The selection process for implementing agencies was also concluded for these three provinces: Damien Foundation will implement CB-DOTS as a new partner in Tete province while existing agencies Amodefa Zambezia and Kulima will expand to the new districts in their respective provinces. To increase the capacity of traditional healers and involve them in case detection and community awareness activities, the project supported a training of trainers for traditional healers at central level. The training focused on the capacity building of a selected group of traditional healers from all provinces and focal points in CB-DOTS, malariaandHIV/AIDStoactasprovincialtrainersintheirrespectiveprovinces(31participantsintotal).Afterthetraining, a step down training will be organized by CB-DOTS implementing partners in TB CARE I provinces to train traditional healers in TB suspect and malaria case detection as well as suspect referral.
The Mozambican Patient Centered Approach (PCA) core team (5 members) elaborated and attained approval from the NTP to implement 3 PCA tools (Quote TB light, The Patient’s Charter and the TB Literacy Toolkit). The tools wereeditedtofittheMozambicancontextandabaselinesurveywascarriedoutintwodistricts(ruralChibutoand urban Nampula) to assess knowledge and practices related to the PCA tools. A total of 226 patients were interviewed, 6 focus groups discussions with TB patients were conducted, and 43 in-depth interviews with TB patients, key informants and NTP staff were done in six health facilities. A baseline report has been completed and will be shared with the lead team while preparation for materials (printing and dissemination) is in process to implement the PCA activities.
TBCAREIisprocuringtwoGeneXpertmachines,onefive-headedmicroscope,onenegativepressuremachineand20 LED microscopes. Procurement was conducted under Year 1 but delivery and site installation will be done in

27
Year 2.
As part of TB laboratory strengthening, the biosafety, quality assurance and AFB microscopy manuals are being finalized.Thesemanualswillbeusedtotrainlaboratorytechniciansinordertoimprovethebiosafetyintheirworking place and ensure quality assured TB laboratory diagnosis.
Supervision visits have been conducted in nine districts of two provinces (Manica and Nampula).Themainfindingsidentifiedincludedalackofpreventivemaintenanceofmicroscopes,alackoftrainingingoodlaboratory practices, a lack of data in the laboratory registry, weak stock management capacity, a lack of SOPs and a functional quality control system and the existence of a weak MDR-TB sample referral system. The project will reinforce technical assistance in these areas in Year 2. The NTP held a meeting with major stakeholders to develop a national sub strategy on PMDT. An external consultant drafted the strategy, which was subsequently reviewed by the technical working group and is now being reviewedbystakeholders.Thestrategywillbefinalizednextquarter. The renovation of the MDR-TB Ward at Mocuba Clinic (Zambezia) has been completed. The ward has a capacity to accommodate eight patients and will be the main internal MDR-TB ward for Zambezia province.
InNiassa,TBCAREIsupportedaTB/HIVtraining(24participants)conductedbytheNTPinclosecoordinationwith the Provincial Directorate for Health in Niassa. After the training, an increase in TB screening services among HIV patients, as well an increase in TB contact tracing and pediatric TB services within health facilities is expected.
TB CARE I also supported the NTP to develop the National Tuberculosis Control Program Strategy (2013 to 2017). AdraftstrategyhasbeenproducedandwillbefinalizedinMay.ThestrategieswillalsoincludeanM&Eplan,whichwas not included in the previous strategy.
Work continued on the development of the District Information Health System (DIHS) database and training manuals in M&E. Two local consultants are leading the process with support from NTP and TB CARE I. Development of the manuals and DIHS database has been completed and these will be used in training provincial supervisors and their deputies in M&E. This activity will increase the capacity of monitoring activities at provincial and district level as well as information management and data analysis (disaggregate TB patients by gender and age). The training will be done in Year 2.
Malaria workplan:
TB CARE I supported the training of clinicians in Cabo Delgado province on the clinical diagnosis and treatment of malaria. A total of 400 clinicians from 15 districts in the province participated. Similar trainings will be conducted in three provinces and will be conducted with funds from Year 2. An international consultant from CDC Atlanta was contracted to establish the malaria quality assurance system. The system will contribute to the improvement of malaria diagnosis in the country and is directly linked to the renovation of the NRL. Draft guidelines have been completed and will be distributed for review in April 2012.
The National Malaria Reference laboratory that was renovated and equipped during TB CAP and under PMI funding wasofficiallyinauguratedinMarch2012.
4.14 Namibia
KNCV is the lead partner and sole implementer in Namibia under TB CARE I. Activities are implemented in UA, IC, PMDT,TB/HIV,HSSandM&E.ImplementationoftheYear2workplanbeganinJanuary2012.
TB National Steering Committee meeting was held in Windhoek with TB CARE I support. This important meeting was very helpful in bringing together various stakeholders in TB control in the country to share experiences and challenges. A meeting of all local and international NGOs involved in community-based TB care (CBTBC) services was successfully conducted as well. One of the outcomes of the meeting was to analyze the various CBTBC models and come up with a model that best suits the country.
TB CARE I continued to provide TA to the NTP in coordinating and participating in management of DR-TB patients through the weekly Central Clinical Review Council meetings along with provision of technical support to regions and districts in DR-TB management through telephone and on-site visits.
Afour-dayretreattofinalizethefirst-everdrug-resistancesurvey(DRS)reportaswellasplanningthenextroundofDRSwasconductedwithfinancialandtechnicalsupportfromTBCAREI.Thepre-finalDRSreportwassubmitted to the Deputy Permanent Secretary for inputs and possible signing off for printing and distribution.
RegularKNCVfieldofficestaffmeetingsaswellasweeklyTBCAREImeetingsforCountryRepresentativeOfficers(through Skype) have brought about an improvement in project follow-up and the monitoring of annual workplans. Weekly meetings with the NTP have also increased levels of cooperation between the two entities. Recruitment

28
and training of Field Promoters engaged in CBTBC services in Karas and Erongo region (where TB CARE I provides directfinancialandtechnicalsupport)wereconductedthisquarter(22participants).
Programmanagementanddataqualitysupportvisitstoidentifieddistricts and regions was done with support from TB CARE I. Khomas Region was supported this quarter through targeted supportive supervision aiming to improve data quality and other aspects of program management. In line with improvement of data quality, SOPs for conducting Zonal Review Meetings were developed and distributed. Also done this quarter was the revision of the quarterly reporting formats for community based TB care which will form part of the reporting forms to be used quarterly.
World TB Day was successfully commemorated in Windhoek in MarchthroughtechnicalandfinancialsupportfromTBCAREI. (Photo: A group of Afro-beat dancers during World TB Day commemorations.)
All planned (5) Zonal Review Meetings were held with support from TB CARE I; these meetings are important in ensuring improved data quality through peer reviews and data cleaning. Writing of the NTP annual report for 2011 beganandwillbefinalizedinthethirdquarter.
4.15 Nigeria
KNCV, the lead partner for Nigeria, works closely with collaborating partners, FHI 360, MSH and WHO. These partnersareimplementingtwoworkplans:oneforTBandtheotherforTB/HIV-fundedactivitiesthroughPEPFAR.
TB Workplan:The TB workplan focuses on UA, laboratories, PMDT, HSS and M&E. The Year 1 workplan was given a NCE through the end of December. An important achievement was that seven out of nine GeneXpert machines (including inverter systems) were installed in the selected health facilities. The health facilities were given 120 cartridges each to start testing. In addition all earlier developed training materials, SOPs and recording and reporting forms wereprintedanddistributedtothefacilities.Thefirstdataarecurrentlybeingreported.DuringthequartertheUSG Department of Defense (DoD) contacted TB CARE I to be briefed on the ongoing activities. The materials as developedunderTBCAREIweresharedforfurtheruseinthefield.InadditiontheDoDwillbeinvitedtothenextCountry GeneXpert Advisory Team Meeting.
The Regional Kick-off Workshop for a Year 1 core project on Patient Centered Approach (PCA) was organized. Nineteen participants from Nigeria and Mozambique were in attendance. The Nigerian Country Team selected three tools from the PCA Package: the Quote Light Tool, the Patient Charter and the TB Costing Tool. A workplan andbudgetwerepreparedbytheCountryTeams.Thenextstepsarefinalizingtheworkplanandbudget(tobeincluded in Year 2 Country Plans), establishing a baseline analysis, submitting a proposal for ethical clearance and planning the follow up activities.
TB CARE I participated in the end term evaluation of the National TB & Leprosy Training Institute in Zaria in December. The team (consisting of staff from NTBLTC, Netherlands Leprosy Relief, KNCV and Ahmadu Bello UniversityZaria)visitedtheTrainingInstituteanddidadeskreview,hospital/traininginstitutetourandconductedafieldvisittotheKadunaStateTBControlProgrammebeforea‘StrategicThinkingSession’wasorganizedwithdifferent stakeholders. The end-term evaluation precedes the development of a new strategic plan for the training institute.Thereportiscurrentlybeingfinalized.
During the quarter, community TB care (CTBC) meetings were held in Udi, AMAC and Bauchi Local Government Areas. Major issues discussed during these meetings included the review of the CTBC activities for the month ofOctober,theneedformoreadvocacyandsensitizationofthecommunities/stakeholdersbytheCVs/CBOstocreate demand for and increase access to CTBC services, and motivation of the community volunteers. In addition, mentoring and supervisory visits held in the month of October in Udi and Bauchi LGAs where an emphasis was putontheneedforup-to-datedocumentationintheCBO/CVregistersbytheengagedCBOs,andtheCV/facilityregisters by facility staff in supported sites.
SignificantprogresswasbeenmadetowardsexpansionofaccesstoMDR-TBdiagnosisandtreatmentasthePhase 1 for upgrade of the MDR-TB treatment centers at IDH, Kano was completed. The completed sections include the waiting room, consulting rooms, bathrooms, nurses’ station, pediatric ward, male ward, audiometer room, pharmacy, and the praying ground. In the same vein, contractors mobilized to the NIMR lab to commence renovation and upgrade to a BSL-3 lab. Sub-structure and framework demolition were completed, and external walls, casting, electrical installation, and plumbing works were also done. The 3-day advocacy, sensitization and orientation training for community and religious leaders as well as training of general health workers was conducted in 16 out of the 18 WHO USAID focus states during the quarter under reporting. A total of 388 community and religious leaders and 364 GHWs were orientated from 17 LGAs in 62

29
communities. The community and religious leaders who participated in the sensitization and orientation training include the pastors, Imams, market women, and the youth leaders.
The challenges Nigeria has faced during the quarter are of social unrest (including bombings), imposed state of emergencies and curfews. The project will discuss the pending activities with the NTP and ensure implementation of the outstanding activities in the coming quarter.
4.16 Pakistan
KNCV is the lead and sole implementer of TB CARE I activities in Pakistan. The Pakistan Year 1 workplan, which ran through March 2012, focuses solely on the National Prevalence Survey (M&E, OR and surveillance). There is no Year 2 workplan for Pakistan, however USAID has approved the re-appropriation for TB CARE I. The project has a NCE through April 2012 for project audit and close out.
Themostsignificantachievementoftheprojectwasthecompletionofthesurveyfieldworkin95countrywideclustersfollowedbydataentry/validationandsharingofthepreliminaryresultswiththestakeholdersinMarch.ThepreliminarysurveyreportshowsthattheprevalenceofdefinitepulmonaryTBcasesinPakistanis295/100,000adultpopulation.
The NTP with support from TB CARE I organized a TOT and planning workshop on LED microscopy in February. Dr. Sang Jae Kim, Director Emeritus, Korean Institute of Tuberculosis, Korean National TB Association, facilitated theworkshop.HealsosupportedthedevelopmentoftheNationalguidelinesfortheEQAschemeforflorescentmicroscopy, as well as supporting preparation of the implementation plan. The event was attended by 14 participantsfromtheNationalReferencelaboratoryandtheProvincialreferenceLabs/PTPs.
4.17 South Sudan
MSH is the lead partner in South Sudan and works closely with collaborating partners KNCV and WHO. TB CARE I-SouthSudanimplementsactivitiesinUA,laboratories,PMDT,TB/HIVandHSS.TheYear2workplanactivitiesbegan in January 2012.
TB CARE I supported the NTP to improve the quality of TB services by strengthening the capacity of health workers to diagnose and treat TB. Twenty health workers were trained on TB diagnosis and treatment in Kwajok, Warrap State.
AmosKutwa,KNCVRegionalAdvisor,providedTAtofinalizetheTBStrategicPlan2013–2017.TheTBStrategicPlan was revised to be in line with the health sector development plan. This will ensure that TB control is embeddedasaprioritydiseaseinthecountrywithcommensuratedomesticfinancingandengagementofpartners. The Senior Laboratory Advisor is on board and a TB Internal Quality Control (IQC) and EQA plan has been developed for the next six months. Baseline data on the laboratories services has been collected and a monitoring tool developed. IQC has been established in three laboratories in Juba County. On-the-job training and mentorship on IQC and EQA of the lab focal persons at Central level and Juba Teaching Hospital is on-going. Assessments have been completed in three out of seven laboratories that require refurbishment. Procurement of the lab equipment and supplies is on-going. MDR-TBhasbeenconfirmedinsixpatientsoutofthe66fromwhomsamplesweresenttotheCRLinNairobi,Kenya. TB CARE I through coalition partner (WHO) continues to support the NTP to send samples to Nairobi for culture and DST. Although treatment is not yet available for MDR-TB cases, surveillance was started in order to fulfillGFtargets(GFR5).USAID,theNTPandWHOareexploringwaystosecuretreatmentfor10patients. TB CARE I supported World TB Day, which was observed in Torit, Eastern Equatoria State. TB CARE I supported radiotalkshowstodisseminateTB/HIVmessagesnationallyandlocallyusinglocalFMstations. The framework for integrating TB services developed through TB CARE I has been used to assess primary health care centers (PHCCs) for refurbishment. The tool has been used to identify three PHCCs that will be refurbished in the coming quarter. The tool will be shared with partners through the NGO Health Forum. This will help to identify health facilities for integration of TB services and those that require refurbishment.
A GF Transitional Funding Mechanism proposal was developed through high level TA provided by the MSH Regional Advisor (Eliud Wandwalo), lead consultant for the process, the TB CARE I country team and WHO EMRO. Stakeholders implementing TB services were also involved. The proposal was successfully submitted to the Global Fund. (Photo: The South Sudan CCM sending off a soft copy of the TFM proposal by email.)
4.19 Uganda
TB CARE I-Uganda is a new project as of this quarter. KNCV is the lead and sole implementing partner in Uganda.

30
TheYear2workplanwasapprovedinFebruary2012andfocusesonUA,PMDT,TB/HIVandHSS.
Thepriorityforthequarterwasthestart-upofthisnewproject.TheTBCAREI-UgandaofficeislocatedattheNationalTB/LeprosyProgram.TheChiefOfPartyandPMDTConsultantstartedworkinJanuary2012whiletheFinanceandOperationsOfficerbeganworkinMarch2012.Therestofthestaffwillbestartingorhiredinthenext quarter (April-June). In March, the Head for the KNCV Regional Team in Africa (Dr. Rene L’Herminez) visited Uganda to ensure project start up, as well as to visit key partners and the USAID Mission.
Initial meetings to introduce TB CARE I and KNCV to the Program Manager of the NTP were conducted. Meetings with different partners such as USAID, Uganda Stop TB Partnership (USTP), Regional Centre for Quality of Health Care in Africa, TB REACH, WHO and Kampala City Council Authority (KCCA) were carried out.
Scopes of Work (SOW) for the renovation of the MDR-TB Ward for Mulago National Referral Hospital were developed and shared with stakeholders. Renovation will begin next quarter.
In line with World TB Day activities, TB CARE I supported the Uganda STOP TB Partnership (USTP) to hold an MDR-TB symposium. About 150 people attended the symposium, mainly health workers from Mulago Hospital and partners of the USTP. The symposium was meant to increase awareness among health workers about MDR-TB management.
4.20 Vietnam
KNCV is the lead partner TB CARE I activities in Vietnam; as of Year 2, MSH began implementing activities as well.TheYear2workplanhasactivitiesinUA,laboratories,IC,PMDT,TB/HIV,HSSandM&E.TheMoHofVietnamofficiallyapprovedTBCAREI-Vietnamasaprojectfortheperiodof2011-2015.ThisisthelegalbasisfortheimplementationofTBCAREIinVietnam.TheYear2workplanwasofficiallyapprovedinMarch.
AnexposurevisittoIndonesiaisbeingplannedonTB,TB/HIVandMDR-TBcontrolinprisonsforhighlevelofficialsfrom the Ministry of Public Security, the MoH and the National Assembly. Planning is being coordinated with KNCV Indonesia, FHI 360 Indonesia, KNCV Vietnam and the NTP.
The proposal and data collection tools for the initial childhood TB assessment in three provinces have been developed by the NTP\Child TB Group for further review. The draft training materials have been developed for furtherdiscussionandfinalization.
Trainingcurriculumandmaterialsonlaboratorybio-safetyandmanagementforlabstaffinfiveMDR-TBlaboratories have been developed and are ready for training next quarter.
Theupgradingofbio-safetyandTB-ICstatusinfiveMDR-TBlaboratoriesinK74,Thanhhoa,BinhDinh,BinhThuan and Tien Giang is underway. Field visits to several laboratories were conducted. The diagnostic algorithms for using GeneXpert and the training curriculum and materials are being developed. The procurement is underway for nine GeneXpert machines and 14 LED microscopes.IECmaterial(flipbook)onMDR-TBhasbeendevelopedand is under review.
The research framework on assessing the screening of PLHIVforTBhasbeenfinalizedandtheproposalfordeveloping the research protocol is available. Terms of reference and preparatory working sessions with NTP were conducted for the visit of an operational research consultant in April. The consultant will support capacity enhancementinthefieldsofoperationalresearchonMTB/RifXpert,LEDmicroscopy,HIV/TBreferral,TBcontrol in children and TB IC.
(Photo: Singing festival of NTP staff (central and provincial levels) to respond to the Month of National Action for TB Control.)
4.21 Zambia
FHI 360 is the lead partner in Zambia and works closely with collaborating partners KNCV, WHO, and as of Year 2, MSH. Activities are implemented in all eight technical areas. Implementation of Year 2 activities began in January 2012.
A kick-off workshop for the Patient Centered Approach (PCA) package was held in February 2012 with nine participants. An implementation plan was drafted for implementation in three districts in the North Western province of Zambia. During the training, discussions and agreements were also made with the ACSM consultant for scale up of ACSM activities planned for the third quarter of project implementation. Planning meetings were held

31
forACSMwiththehealthpromotionofficerandTBCAREIandagreementshavebeenmadeonhowactivitieswillbe implemented in the next quarter. Activities include a situation analysis on ACSM in target provinces; orientation of stakeholders, community and civic leaders on ACSM with support of a consultant from KNCV; design of an ACSM strategy and operational plan; and training of health care workers in ACSM.
TB CARE I procured two Xpert MTBRIF machines in February that have been delivered. One machine will be placed in a facility in the Copperbelt province with high HIV and TB burden and one will be placed in a facility in Central province. TA will be provided by KNCV for the effective utilization of the new diagnostic tools. TB CARE I also provided support for training of six laboratory staff in advanced tuberculosis techniques at Makerere University in Uganda. The participants were trained in the use of Xpert MTBRIF, in-house PCR IS6110, HAIN molecular test and equipment validation. (Photo: Laboratory staff undergoing a practical training session at Makerere University.)
EQA was conducted in all target provinces this quarter. EQA was scaled up to 68 new health facilities this quarter (112 health facilities in total). TB CARE I staff participated in the EQA visits to the Copperbelt and North Western provinces. Follow-up visits were also conducted after observation of high false results recorded by three laboratoriesinLuapulaandfivelaboratoriesintheCopperbeltprovinces.Visitswereconductedinthesetwoprovinces in March and corrective actions were made.
TwoTB/HIVdistrictmeetingswereheldunderTBCAREIsupportinMarch;68participantsattendedthemeetingin two Copperbelt districts. The meetings provided a forum for exchange of information, plans and agreements amongtheTBandHIVprogram.TBCAREIsupportedtrainingof54nursesandclinicalofficersworkinginCopperbelt TB clinics on provider initiated HIV counseling and testing. TB CARE I also received a visit from USGpartnersincludingOGAC,CDCAtlantaandUSAIDWashingtontoplanforthescale-upofthethreeTB/HIVinitiatives(3Is).ItisanticipatedthatTBCAREIwillreceive$4.6milliontoimplementactivitiesinCentraland Copperbelt provinces in partnership with the Centre for Infectious Diseases Research in Zambia (CIDRZ), which will support activities in Lusaka and Southern provinces for an equivalent amount. A national proposal was developed by TB CARE I and CIDRZ and submitted to the USG partners for approval. Implementation is anticipated from June 2012.
The Ndola district TB IC demonstration site project was launched in January. Between January and March, three project interventions were completed and (summary) mission reports for the three interventions were submitted. 116 community volunteers representing 12 of the 15 facilities Health facilities under the Ndola Demonstration site project(TBIC)weretrainedinTBIC.AProjectManagerpositionwasalsofilledandthestaffmemberwillstartinApril.
The NTP began hosting planning meetings for the prevalence survey projected for 2012-2013. A protocol was prepared with local and international partner support and is being reviewed by both local and international consultants and partners.
4.22 Zimbabwe
Zimbabwe is led by The Union and has KNCV and WHO as collaborating partners. The Year 2 workplan, which beganinJanuary,focusesonUA,laboratories,IC,PMDT,TB/HIV,HSSandM&E.
The program continued to support Harare, Chitungwiza and Bulawayo cities with the transport system for sputum specimens. An evaluation of the sputum transport system in the three cities covering the period July 2010 to June 2011 was received during the quarter and showed less patients were diagnosed with pulmonary TB without a smear result in the three cities than in the provinces. Continued monitoring has shown that the same trend was maintaineduptoDecember2011.Intheruralexpansion,transportroutesweremappedoutinthefiveselected
districts-oneineachofthefiveprovincesofManicaland,Masvingo,Midlands,Matabeleland North and Matabeleland South. Motorcycles have been procured, training for the motorcycle riders is due to start in April 2012 and sputum transport soon after.
A job aid for use by TB treatment supporters was drafted and awaits NTP approval. Ten meetings in ten districts were conducted with existing community TB treatment supporters, reaching 1,036 community workers. The meetings revealed that most of the DOT supporters are unable to visit assigned patients at their homes daily due to the long distances and the number of patients involved. The information obtained from the meetings will facilitate the on-going NTP process of formulating community DOT policy. (Photo: Community TB supporters n Manicaland province) Development of PMDT guidelines was completed, paving the way for the

32
development of training materials, which has commenced. The DRS protocol is ready and will be submitted to the Zimbabwe Medical Research Council for expedited review. The pilot run is planned to start in early June.
Eachofthefiveprovincesconductedsupportsupervisiontoatotalof16districtsand129ruralhealthcentresduringthequarter.ThesupportvisitsfocusedmainlyonTBcasefindingathealthfacilitylevel,TBmanagementandcaseholding,TB/HIVcollaborativeactivities,aswellasrecordingandreporting.ThethrustwasonuseofTBdata at local level. Districts conducted nine visits to the periphery, reaching 71 rural health centres.
A total of seven general TB training workshops were conducted. The trainings focused on TB case detection, TB treatment,ChildhoodTB,CommunityTBsupport,caseholding,patienteducation,TB/HIVcollaborativeactivities,TB medicines and supplies, recording and reporting and MDR-TB. A total of 245 health workers were trained.
Threeoutofthefiveprovincialperformancereviewandplanningmeetingsplannedforthequarter(oneforeachsupported province) were held. The main areas covered during the review meetings were assessing data for the year2011bydistrict,focusingonnotificationtrends,treatmentoutcomesandTB/HIVinrelationtonationaltargets,andthewayforward.ThemostsignificantfindingwaswidespreaddeclineinTBnotificationsinallfiveprovinces - a development also noted nationally. TB CARE I is currently working with the NTP to determine whether the decline represents an epidemiological change, is due to recording and reporting challenges or other causes.Draft data collection, analysis and utilisation guidelines were developed to facilitate quality data analysis and use atlocallevel.Threepilotdistrictswereidentifiedandsensitisationmeetingswereconductedwithprovincialhealthexecutives and district health executives.
Three studies are on-going from Year 1, and are ready to be submitted to the Zimbabwe Medical Research Council for research authorisation. The studies are 1) ART uptake in TB patients in Midlands province, 2) TB mortality in Mat South province, 3) The maximum time a sputum sample can be kept at room temperature and still be useful for MTB culture. The other eight studies previously reported have not progressed. One Year 2-funded study on “HowthetypeofDOTinfluencedtuberculosistreatmentoutcomesinonedistrictinZimbabwe”isinprogress.
With the support of TB CARE I, the NTP re-applied for Phase 2 of Global Fund Round 8 (USD 25 million for three years) and is waiting for the results of the application. In the meantime, a NCE of Phase 1 was granted until June 2012.

33
5. Regional Projects
Inadditiontotheaforementionedcountryandcoreprograms,TBCAREIalsomanagesfiveregionalprojects,four of which receive Year 2 funding (CAR regional funding being Year 1 only). The four Year 2 funded project workplans were approved in January 2012.
5.1 Center of Excellence (CoE) for PMDT
TheCoEforPMDTprojectisimplementedbyKNCV.Thisquarter,anMoUwasofficiallysignedbetweentheSchoolof Public Health (SPH) of the National University of Rwanda and KNCV. This resulted in the MoH (NTP) successfully handingovertherunningoftheCoEtoSPHandthefirsttrancheoffundsbeingtransferredtoSPHfromKNCVinMarch 2012.
SPH appointed Dr. Francine Birugi as CoE Coordinator and recruitment of an Assistant CoE Coordinator is inprocess.ThefirstCoEsteeringcommitteemeetingwasheldatSPHinMarch,resultinginarevisedandsubsequently approved training calendar for 2012 (TB IC training in June, PMDT training in July & laboratory training in September). Fee levels were introduced and the training calendar was advertised to TB CARE I country coordinators and NTP program managers. Although implementation appears slow, all trainings are planned for later in the year (June-Sepetmber 2012) so this project remains on track.
5.2 East Africa Supranational Reference Laboratory (SNRL)
TheUnion,theleadpartner,workscloselywithKNCV/KITontheSNRLproject.Activitieshavebeendelayeddueto the project’s late start and the head of the Uganda lab’s recovery from an accident. The NTRL has applied for accreditation according to ISO15189 by SANAS. A KIT consultant visited the NTRL in March. Special attention was paid to occurrence management, resolution of complaints and a customer satisfaction survey, trend analysis for non-conformities and the policy cycle.
AvisitbyaUnionconsultantisplannedforMaytofinalizestrategicplanninganddraftabusinessplan.TrainingofonestaffatAntwerpSRLforDSTproficiencytestingisalsoplannedforMay.LinkswithsurroundingNRLswill be discussed with WHO and other SRLs during the GLI meeting in April; so far countries or other SRLs have been reluctant to give up their current links. WHO involvement will be vital to establishing new SRL links. Joint visits could not yet be conducted due to unavailability of WHO SRL funds for Uganda, but are foreseen for July-September 2012.
5.3 ECSA (East, Central and Southern Africa)
The ECSA project is carried out by KNCV. One TA mission was conducted to the ECSA secretariat during which all TB resolutions from 1999 to 2011 were reviewed and a summary tool was made to monitor implementation progress in the member states.
A country mission was also done to Malawi to monitor implementation of the ECSA Health Ministers resolutions. Progress has been made, including initiation of a PMDT program that predominantly uses a community-based ambulatory model and continuation of a high HIV testing & counseling rate among TB suspects (88% in 2010). Challenges do persist though, such as limited funding and human resources impacting the monitoring of the ambulatory model of care and the implementation of CB-DOTS. A second country mission will be done in the next quarter to Zambia. The workshop on WHO guidelines is also planned for the next quarter.
5.4 Central Asian Republic (CAR) Regional Funding
In addition to the three CAR country workplans, KNCV is the lead implementer of two regional CAR activities: a CAR/PMDTWorkshopandahighlevelmeetingoncrossborderTBcontrol.ThereiscurrentlyonlyYear1fundingfor these small projects. The PMDT workshop is planned and prepared for April 2012. The cross border TB control meeting was completed in November 2011.
5.5 Central Asian Republic (CAR) Regional Funding
KNCV coordinated this small project to support the travel and lodging for 18 participants from the East African regiontoattendtheSecondInternationalScientificLungHealthConferenceinKenyainOctober2011.Furtherdetails on the conference can be found in the Kenya section of the October-December 2011 QMR.

34