Senior Case Presentation Armi Azad, M.D.. Introduction S.R. is a 4 y/o HF transferred from MVCH for...
41
Senior Case Presentation Armi Azad, M.D.
-
Upload
neil-daniels -
Category
Documents
-
view
215 -
download
1
Transcript of Senior Case Presentation Armi Azad, M.D.. Introduction S.R. is a 4 y/o HF transferred from MVCH for...

Senior Case Presentation
Armi Azad, M.D.

Introduction
• S.R. is a 4 y/o HF transferred from MVCH for higher level of care
• Chief Complaint:
Intermittent fever x 1 month (ranging from 100.4 to 103º) and R hip pain for the past couple of weeks; no hx. of trauma

Review of Systems
• On further questioning:
+occasional abdominal pain
generalized weakness and fatigue
?decreased appetite
• ROS otherwise negative

PMHx
Strep Throat x 1 month ago, tx’d w/ PO Abx. x10 dys.

PSHx
No Surgical History
Birth Hx
Full Term
C/S 2/2 failure to progress
Birth Wt= 8 lbs.

Family History
Mother Denies

Social History
Lives with both parents
2 older siblings
No sick contacts
No pets
No tobacco exposure
Pre-school waiting List
History Cont’d.
• Development- Appropriate
• Diet- Regular
• Meds- Motrin
• Allergies- Amoxicillin rash
• Immunizations- Up to date

Physical Exam
Vital Signs:
T=101.5
P=115
R=24
BP=84/59
Wt= 17 kg
Height= 103 cm
Physical Exam
• Gen- pale, scared/anxious
• HEENT- normocephalic, PERRLA
neck supple
no lymphadenopathy
throat clear
TM’s clear B/L

Physical Exam
• CV- RRR, 2/6 systolic murmur
• Resp- CTA B/L
• Abd- Soft, ND, +BS
+tenderness to deep palpation RLQ
no CVA tenderness

Physical Exam
• MS- Decreased abduction R hip 2/2 pain,
+TTP R lower back (no bony TTP),
5/5 motor strength x 4 extremities
+sensation intact B/L
DTR’s intact B/L
• Neuro- AAOx3, CN’s II-XII grossly intact,
gait WNL

What tests do you want to order?

Diagnostic Testing
• CBC w/ peripheral smear
• CMP
• UA, UCx/Blood Cx.
• Pelvis and R hip x-rays
• ESR, CRP, ASO titer

Laboratory Results
7.8
6.8 423
23.1
MCV= 76.3
ESR= >140
CRP= 13.7
ASO= 15 (<150)
• Segs= 19 (37-80%)• Lymphs= 57 (25-35%)• Mono= 5 (0-12%)• Eos= 1 (0-7%)• Bands= 17 (0-6%)

Laboratory Results
137 103 12
86
5.0 28 0.4
Albumin= 3.3 Ca= 9.6
Total Protein= 7.0 BiliT= 0.2
AST= 54 AlkPhos= 150
ALT= 14 Retic= 2.4%

Urine Analysis
• Color yellow• Glucose negative• Bili negative• Blood negative• Nitrite moderate• LE 2+• WBC 5-10• RBC 0-2

Laboratory Results
• Urine Cx- negative
• Blood Cx’s- negative x2

X-ray
• Pelvis and R hip x-rays: unremarkable

Any Thoughts?
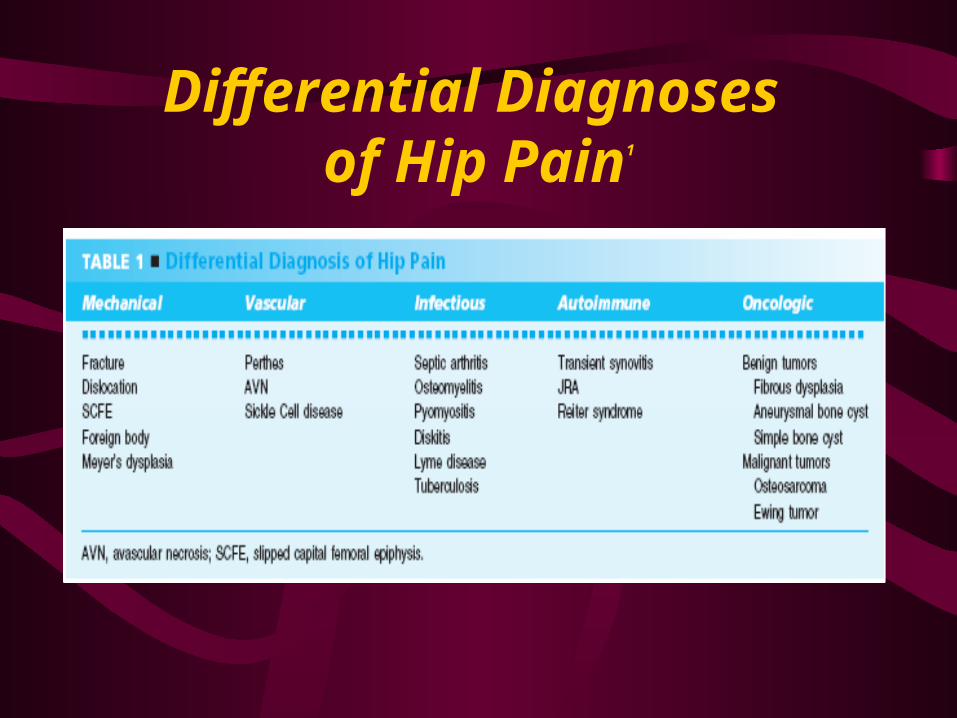
Differential Diagnoses of Hip Pain1

Now What?

Radiology
• CT Pelvis:– Large fecal collection in rectum– Thickening of urinary bladder– No evidence of acute osteo or a pelvic abscess

Update
• Continued fevers despite IV Abx• Migratory bone pain (i.e. L shoulder, mid
back)• Intermittent RLQ abdominal tenderness to
deep palpation 6.7
8.0 372 19.9

3- Phase Bone Scan
• Vascular Flow Study-No abn. Increased vascular flow in lower abdomen,
pelvis, and thighs
• Blood Pool Phase-
Slight hyperemia in the right medial ilium

3- Phase Bone Scan
• 3-hr Delayed Static Images-
Abn. accumulation in R mastoid and clivus
Abn. accumulation in body of C2/C3
Mild generalized accumulation in bodies of L3/L4 and multiple levels of the thoracic vertebrae
Non-functional R kidney
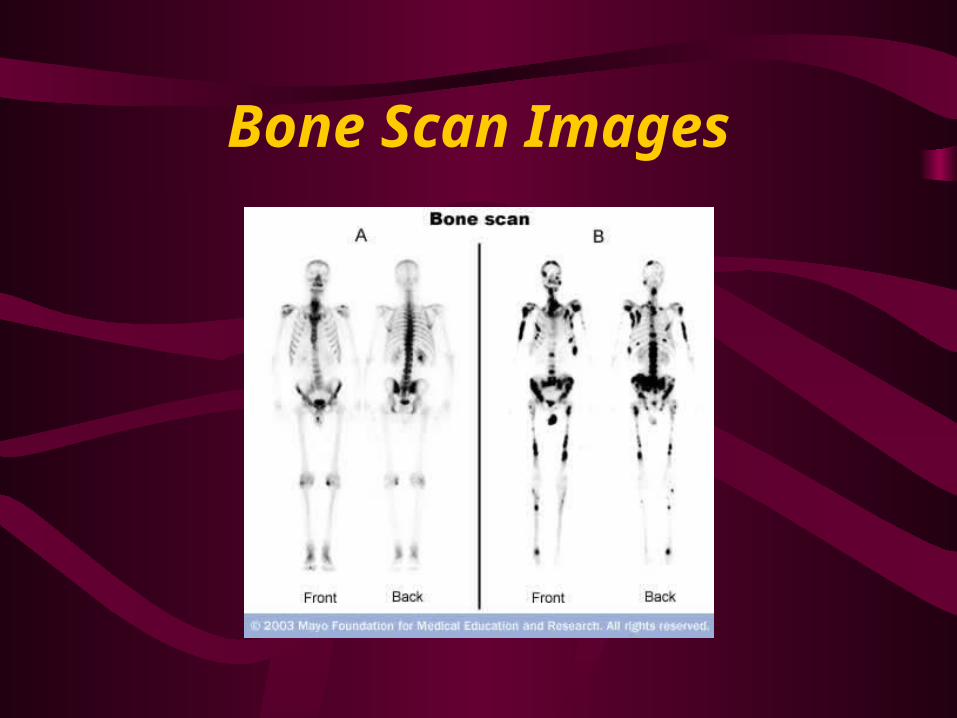
Bone Scan Images

Impression
Metastases
vs.
Extensive Diffuse Osteomyelitis
More Radiology
• CT Chest w/ contrast-
Multiple osteolytic and osteoblastic lesions in the thoracic spine
• CT Abd/Pelvis w/ contrast-
3.6 cm L adrenal mass
No ascites or adenopathy
Osteolytic lesion in R posteromedial ilium w/ sclerotic rim

Neuroblastoma
• What is it?– 4th most common malignancy of childhood– Cancerous tumor that begins in nerve tissue of
infants and very young children– Usually begins in tissues of adrenal gland
(sometimes in neck, chest, and/or pelvis)

Neuroblastoma
• Metastasizes quickly (i.e. LN’s, liver, lungs, bones, CNS, bone marrow)
• 70% of all children diagnosed have some metastatic disease

Frequency3
• Approx. 650 new cases dx’d in U.S./year
• More common in whites
• Male-to-Female ratio 1.3:1
• 79% of children diagnosed by age 4
• 97% of cases diagnosed before age 10
Etiology4
• Chromosome #1
• Deletion/rearrangement on short arm of C’some 1
• Amplification of n-myc oncogene
• Inherited mutation + 2nd mutation after birth
vs.
2 acquired mutations after birth
Symptoms
• Abdominal mass/distention• Uncontrolled eye movement if facial
involvement• Changes in urination, diarrhea• Pain, limping, paralysis, weakness if bone
marrow involvement• Fever• High BP and increased HR

Staging5

Treatment
• Surgery
• Chemotherapy
• Radiation
• Bone marrow transplant
• Antibiotics
• Supportive care
• Continuous follow-up

Prognosis6
• Depends on a variety of factors including age of pt. and stage of disease
• Survival significantly better for children less than 1 year of age
• N-myc amplification confers worse prognosis
• Increased ploidy has better prognosis

Survival6
• Patients risk stratified into 3 groups
• 5-year survival by risk group:
1) Low Risk- 95%
2) Intermediate Risk- 85-90%
3) High Risk- 30-50%

Back to S.R.
• Chemotherapy: completing 4 of 6 cycles today
• Surgery to remove tumor
• Bone marrow transplant

References
1. An Evidence-Based Approach to the Evaluation and Management of Hip Pain in Children. Pediatric Case Reviews, Volume 2:1; January 2002
2. http://www.emedicine.com/med/topic2836.htm
3. http://www.okstate.edu/artsci/zoology/ravdb/3024.htm
4. Staging of Neuroblastoma at Imaging. Report of the Radiology Oncology Diagnostic Group 2002; Volume 223:1 (p. 168-175)
5. http://www.cancer.org/docroot/cri/content/cri_2_4_3x_how_is_neuroblastoma_staged_31.asp