Reviews in Pain 2011 Goebel 3 11
10
http://bjp.sagepub.com/ Reviews in Pain http://bjp.sagepub.com/content/5/2/3 The online version of this article can be found at: DOI: 10.1177/204946371100500202 2011 5: 3 Reviews in Pain Andreas Goebel Current Concepts in Adult CRPS Published by: http://www.sagepublications.com On behalf of: British Pain Society can be found at: Reviews in Pain Additional services and information for http://bjp.sagepub.com/cgi/alerts Email Alerts: http://bjp.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: http://bjp.sagepub.com/content/5/2/3.refs.html Citations: What is This? - Jun 1, 2011 Version of Record >> by guest on March 15, 2014 bjp.sagepub.com Downloaded from by guest on March 15, 2014 bjp.sagepub.com Downloaded from
Transcript of Reviews in Pain 2011 Goebel 3 11

http://bjp.sagepub.com/Reviews in Pain
http://bjp.sagepub.com/content/5/2/3The online version of this article can be found at:
DOI: 10.1177/204946371100500202
2011 5: 3Reviews in PainAndreas Goebel
Current Concepts in Adult CRPS
Published by:
http://www.sagepublications.com
On behalf of:
British Pain Society
can be found at:Reviews in PainAdditional services and information for
http://bjp.sagepub.com/cgi/alertsEmail Alerts:
http://bjp.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://bjp.sagepub.com/content/5/2/3.refs.htmlCitations:
What is This?
- Jun 1, 2011Version of Record >>
by guest on March 15, 2014bjp.sagepub.comDownloaded from by guest on March 15, 2014bjp.sagepub.comDownloaded from

R E VI E W S I N P }.I N
V O L . S - N O .2 - J U N E 20 1 1
Current Concepts in adult CRPS
l
Dr. Andreas Goebel MsC PhD FRCASenior Lecturer and Honorary Consultant in Pain Medicine, Pain Research Group and Centre for Immune Studies in Pain, Unil't'TSityU I't'rpool and the 'l'0tlton Centre NHS Trost, Liverpool Clinical Sciences Centre, Unnersity Hospiral Aimree; Lirerpoo!1..9 l AL0151 529 5822: [email protected]
CRr s d iagno sis, ep ide miology, recovery, heal th economics and
rare p re5<'ntations
C RPS is a pa infu l con d ition which usually dev elops after trauma
to a limb . It is chnracrerbed by l imb_confln~-d sensory, autonomic,
moto r, skin and bon e cha nges, btu the lead symptom is pain.
Earlier names for the condi tion are given in appendix A. 111e C Rrs
diagno stic crite ria have recently been up dated ('Budape sr Criteria",
appendi x B}, because earlier criteria were nor specific . These new
criteria, although widely used have nOI yet been formally ado pted
by rhe Int ernational Associati on for the Stud y of Pain ( I) . O ver
the past 10 years many investigators , scient ists an d clini cians alike
have jointl y ach ieved remarkable progress in understanding and
treating C RPS. These efforts have been enhanced by the success of
the 'TREN D" consort ium led by Prof. J.J. van Hilren from Leidenand Prof. van der Helm from Delft , who secured in the early 2000's
over 20 million Eurc in research suppo rr from the Durch M inisrry of
Econ omic Affairs to study CRPS and related cond itio ns.
As a result of the first ever. population based Europ ean
epidemiological study, we now unde rstand thai C RPS is more
commo n (incide nce: 26fJOO.OOO po pulation) than previou sly
thought (for comparison, the incide nce of Mul tiple Sclerosis in the
UK is estima ted at 4/100.000). It has its peak in people aged 55-75
years, bur may take a mor e benign co urse in this gro up, than in
younger partcnrs (2), Ck l'S is associated with migraines, osteoporosisand asthma (3). Overall 85% of patients will have substan tial pain
reduction within the flrst 1-2 years afier d isease onset. How ever only
30% of partenrs co nsider rhernselves fully recovered even 6 years afterdisease onset, and only 40% of people who worked before will return
10 their prior work. C RI'S which has not improved ear ly is less likely
10 improve later (4) .
A defin it ion of recovery from C RPS has not yet been achieved.
Auto no mic signs usually reduce with rime, even where pain persists
(5) . Wirhou l autonomi c signs, a diagnosis of C Rrs can often no t be
mad e (Append ix B), so that patients may 'lese' their init ial di agnosis
ali:er some years, but cont inue to suffer from pain", It is likely thar
we will in the future define a 'p<>st.CRPS syndrome' for patients who
have fulfilled the Buda pest c rite ria in the past. Similar as posrherperic
I An r"dirr 1,",10'1 u'<Ir mmed 'Omr"'-H"rdrn rrllrrid: but WI" S,rpl/{/tl Onlrh{tIIldNomu/II Hardor",M, Ih'/l Imtrad rhr 1/"'''' 'Blldtlprll mlrna"is usrd 10rtf /rrt Ihr /or"IIOII ofl"r rOJMI/! IIl «mft rtJJrr.
"'CRPS NOS '(1101 olhrr",I'r ,prdjird) I, ,hr now rtrom", ,,,drd '''1/1 fir dUMenm which ;'"d" fufJicirnt Ilumb" of,lg", ("pp",dlx A) In t!lrpmt. but kuksig'" 011 rXilt'lln"tlon.
neuralgia. bur unlik e lower back pain and fibromyalgia alrnosr all
CRPS is mon op hasic (once n uly disap peared it won't co me back),
wirh only 2% relapsing-remitting cases (6),
Because mo st cases ofCRPS get better early on, for clinical trial
pur poses it can make sense to separately conside r the difhculr-rotreat lon gsrand mg CRrs (wit h > 6 mom hs disease duration). Th is
co ncep t has received more att ention ove r the last J() years. Almost
all clinical stud ies in lon gstandin g C RPS have been co nducted after
2000. For health economic calculations, the Naricnallnstinue
for Clinical Excellence (N IC E) has assumed a 15 year estimated
average C RI'S durat ion for those cases oflongstanding CRI'S which
req uire spinal cord srim ularion (hn p:l/ www.nice.org.uk /ni cemcdiaJ
Iive/1108 2f42367/ 42367.pdf, page 2 1).
Similar as many other chro nic pain s (7), C RI'S is expensive.
Average an nual health -care costs (excluding physiotherapy) in the
Nethe rlands were £5700 in 1998. Bec ause paricurs with lon gstanding
e RPS almost never work (8) overall COStSare higher. Return to work
rates may remain low even in patient s who successfully rec eivedspinal cord stimulatio n (SCS) rrearr ncm (Prof. Kemler, perso nal
co mmunicatio n). Thae is in spi te of the fact that SCS treatment
Imp roves parknl5' qual ity ofli fe (9). The average quali ty of Hfeof
pa tients with lon gstanding C RPS is very low, with an Euroquol
score of 0.2 to I (8), For comparlson rhc average scores in multi ple
selerosis are0.4-0.5 -1 (10),
We all kn ow rhar patlc urs with CRPS can present in ma ny different
ways. For example, limb s can be hOI or cold, shiny, swollen or
thin. red o r blue, with scaling or with clammy skin . However
there are some rare presentations/complicati on s. which even pain
specialists may only enco unter every few years. These include CRrS
with spontaneous onset (no trauma), with a painful sho ulder and
auto no mic signs (but not pain) only in the ipsilateral hand (formerly
termed 'should er-hand synd rome'), rhe .lr reading of symptoms 10
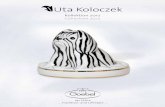
anothe r limb, ch ronic lymphedema, skin ulcerations (often withsecondary infections, Figure I), blister formation, dystoni a, severe
at rophy and myocl onus; the co mplica tio ns are more common in
you ng wo men ( I I) .
by guest on March 15, 2014bjp.sagepub.comDownloaded from

1l.!! V l f W S I N P A I N
4 V O L. S - ~O . 2 - J U ~ E 20 1 1
Ca uses and trearmenrs ofeRrs
There are currently seven major wn(;ept s about the CRPS etiology.
These co ncepts em also explain the rario nale for mosr clin ical
rrearmemsll1:
deemp hasize the impo rtance of sympathetic dysregulanon for C RPS
pain.
2) Cmmll trmititation 'II th, drivi1/g fim orfor CRPSCe nt ral sensmserton is the molecular process rhar corresponds to
the clinical observation that after a per iod of intense or repeated
noxious snmulanon, innocuous (non- noxiou s) stimul i become
painful and remain painfu l (for a wh ile ar least) even if rhe initial
noxious st imulation has subsided . Th is mechan ism is import ant in
most chro nic pains (19), Because Ncmcrhyl Dcaspanare (N M DA)
receptors play a crtrtcal role in central sensutsanon, the recent
observat ion in IWO rando r nired controlled trials that low-dose
intravenou s keta mine (an NM DA-anragonlst) can dramat ically
reduce C RPS pain indicates an lmportanr role for such central
senstdsado n (20). There is currently no RCT evide nce for high-
dose 'ketarnine-corna' und er lntenslve care conditions, which has
sometimes been discussed in rhe media (2 1). In the rwo publishedlow-dose RCT's, kcmmlne stro ngly reduced average pain intensity
for several weeks, independent of the CRI'S disease d uration. It is
un certa in whethe r these research find ings will translate into clinicalpractice. Side effects from repeale d keramine infusions are poorly
understood, with some experts expressing co ncern about potential
neurotoxicity (22). Curren t pro toco ls for Keta mine rreatrn enr are
expensive and cumbe rsome. In the published protocols either a S-dayhospital inparlenr stay, or 10 consecutive wo rking-days ourpanenr
treatments are required 10 achieve pain relief lasling several week>.
Recently a small pilot trial suggested efficacy of int raveno us
magnesium which , similar 10 Keraminc may work rc reduce central
scnsirlsarion (23) .
I
Figure I. LYII/phrdmltlofthe right UpP"rxlrrmity in a35 ymrold IIlIlI/. 7hisptlfinll had an IIlIdisplllad righl sidedfinelllrrof lhrfifih maacarpal. He drvrloprd ComplaRrgional Pain Sp Jdromecomp licated by/ymphednllaand recurrent rpiJod~ of((/lulitis. whirhUlfTr m'al£dwilh ansibioncs. AlI/pUlalioll ofthr 4frcud limbwm i atrr considered I/rcm flly. Chronic IymphrtUllulwilh rrllulitiJ isa rare complimtiollin CRPS(/romNE1tg/Mrd 2008; 359(5):508, withpermis sion},
l) CRPS asa sympathrtiml/ymrdiaud diJordrrSwearing and colo ur/temperature changes in rhe C RPS-affew:d
extremity are in pan rnedia red by sympathetic dysrcgulano n .
however the perman ent w id rcmpcrarure in some cases oflare C RPS
may be due ro endot helial dysfuncnon (13). Evans had int roduced
the. now superseded term ' Reflex Sympathetic Dyst r ophy' (RSD .
appenuh A) 10 Indlcare rhar the auronomk uysregularion CIl/ij~
the pat iem s' pain (14). Hanningron-Kiffla rer suggesrcd that agents
which deplet e rhe limb autonomic nerve endings of nora drenaline,
such as regional gua lll'thid ine (lr nraveno us rcgiOrt.l1 symp arhertc
block. IVRSB) sho uld be effective (15) . Unfortunately all four
Rei 'Sconducted to assess th is rrearm ent have been negative{I 2).
G iven the experience sha red by mOSI clin icians that this met hod
actuall y does red uce pain in some patients, one wonders whether it is
per haps the application of tou rniquet wh ich conveys that effect. Of
note, o ne study has shown that IVRSB with saline is more effective
than IVRSB with guanethidine (16). local anaesthetic appli cation to
the symparhenc ganglia e m relief pain sho rt ter m in selected pat ients
(17) , but repea t application does not prolon g that effect (18).
These trial resu lts have cont ributed 10 prompting CRPS expens to
III 7h, dlNI(lit 'ridl nJidm(t dud i" Ih,-, l«tioNII dm·r'rdfrom ,,/ I«lj/ ON(rm"wmlud eo"troll,d tn'''!;'1lIteh(Iii(. ""d wllh "0 conflicting muttl. UNUUlpreiftcaUy fIOud 71'(l' tri"ls hlll)( b' m idm liftrd i" ly<lmuUic rrt,I,W< byFOroU""Nf lr lt "I. (( 12). until 06.2(00). "Nd ,ht UK CRI'$ guid,!IN,group (uu·tilfrom 06.2()()(}-{)4.20fO. Coll;" !,1 "t 1'1p"pml/lon)
3) Autoimmul/itymay ram, CRPSThis is a novel concept which has recently bee n sugges ted bot h
by our and Franz Blacs's group . Borh groups fou nd eviden<:e for
ami -n euronal autoantibodies ill C RPS (24-26). We have shown in
a recent Re r ehar 10w--<;10se in traveno us lmmunogloh ulln (IY1G) is
efflX"live in longsrandi ng C RPS (27). Pain relief in responders lasted
for five week>on average. Mo S! llIedkal condiricns which respond
to IVIG rrearmen r are autoimmune in nature, and associated whh
fu nctionally lmpcrtanr autoantibodies. In our trial, patients ryplcally
respo nded with in 2 days, which is at}'Pk al, If auro anribodics arc
indeed respo nsible, rhen the nK,<:haniSlll of their lnrcractlon with
the nervous system sho uld be d ifferent from that des cribed in othe r
condino ns.
4) CRPS (/J a m ull of limb isrhemia oriJrh,mia-rt'prrjilSio1/ i I/jilT)
A recent pilot -tr ial showed that Tadalaf il a phosphodiesterase
inhibito r, red uces pain in some patients with C RpS who have
w id limbs (28). Tedalaf il is a vasod ilator and it may be that th e
vasodila rory property of thisd rug is responsible for pain relief,
however rhe affected limbs did nor gel warmer with treatment (limb
temp erature was rhe pr ima ry outcome}. No other tr ial has to date
demonsuared the success of a treatmen t which imp roves limb blood
flow (the working mec hanis m of symparheric block>could of cause
be explained rhar war ). In an imal model s, transient applicat ion of
limb ischemia produces a syndrome which resemb les CRPS (29) .
A possible prophylactic efficacy ofVitamin C in CRPS after dorsal
by guest on March 15, 2014bjp.sagepub.comDownloaded from

R E VI E W S I N P }.I N
V O L . S - N O.2 - J U N E 20 1 1
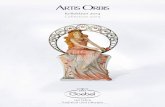
Figure 2, T!JI' follrpillars ojtrefllmmt in CRPS. !I/formatiol//
tdliCittiol/, physical ((h/fbi/itatiOlI, psyrhol"gim!mpport,a/ld drug/proadt/ I'll/ ;/Il(r/l(//li01l$ ht(V1' ('qM!
importill'((,for thl'trmtment ojCRPS. Emphasis is 011flIl ;ndil'id/ft1lisrd. inl(gml(d infrrdisciplitwyapp'Oftrh.
radiu s fract ure has been explained by the prod union of free radicals
after such injury (30).
5) Cortical r(orgfllliSrltioll is mpomib/(for thl'CRPSp{/ill
Th is is anoth er excmng clinical and research development.Functional MRI stud ies over the last 10 years have d early shown
rhar the sensor}' representa tio n of the C RPS affected limb is altered
(shrun k and shi fted), thar rhe degree of the alteratio n correspo nd,
10 the pain inten sity, and that pain reduction is associated with
normalis.ltion (31 ;321, There are also Important changes in rhc
moto r CO rtex. Wc do n't know whe ther these changes are secondary,
or whe the r th t')' relate to the C RrS pat hophysiology. Clin ically we
have learned That patients often feel alicnarlon with their affecwd
limb, which can feel strange and disfigured and OUl of place (33);
these feelings are often not commun ic:ned 10 avoid the SUSpl,<IOO
danger of not bein g believed. Some patients can't Stop thi nk ing
about amputating that limb . These feelings may be associated with
the altered co rt ical limb representation. although this has yet 10
be confi rmed . Co mputer- based 'graded motor imagery' (GMI),
which involves an exercise to tra in the brain in berrer recogn izing
the affected limb can red uce (34) pain and swelling (35) . Mirror
IherapyN was first applied 10 the rrearmene of CRPS by Candy
McCa be's group (36). h has been show n 10 reduce pain in C RPS
(borh early and late)after stroke (37) .
Pain Re lief(MedlCallCll &ProcedUres )
Physic al
& Vocational
aereomancn
PatientInformation &education tosupportselfmanaaement
PsyttnloglC ar
rntevereons
These therapeutic advances appear part icularly exciting since these
treatments have few adverse events (2). Unfort unately we and oth ers
were recently un able ro reproduce the published GM I findin gs in
a 2.hospi tal audit set tin g {johnson er al., un der review). GMI an d
mi rror treatment arc now widely practiced, and clinicians should beaware tha t many patients whh longstanding C RrS will not respond .
But even if no pain relief can be achieved, rhe clinician's antic ipatio n
and rcflccnon of his/her patient's 'strange ' limb feelings mar well
support a better und erstanding and acceptan ce of the co ndition.
Physkxhcrap y and occupational therapy (PTfOT) consti tu te one
pillar of CRrs rreann cm (Figu re 2). Th ere ale man y repo rted PT f
OT t reatment methods. We recenrl r found that rherapists in ou r
Liverpo ol region usc ove r 20 different methods. with pacrcrns grearly
varying between indi vidu al therapi sts. Important methods include
desensfrisarlon (rubbing the affected limb gently wirh d oth or
similar), gradual weight bearing, srretching and simple funnional
exercises.
6) CRPSmfly b( dllr to Ilml( J{/Jmtg(
This concepr stales that persistent dysfunction of small-diamete r
primary afferent noc icepto r axon s distal to the trauma ls causal 10
C RPS. Snuhes in CRPS amputated limb s and skin biopsies have
shown small fibre loss (38-40) . Th us it is postula ted that C RI'S-I
mar represent a neuropathic pain synd rome". a small-fibre-
IV MirrtJ'th(mPl rrquim thottht /,,1I;mt hiM. tht offiC/(dlimb bthi"d"mirrorwhkh ispositi/Jlltd pI'rpmditr<lttr to his body-midl;tlt. Whmlooki"g illlotht mirro' /mdptrjontlitlg Mlttltmf s) tI,hrotlistd gm(lr IIIO/I(/I/m/$, tIl( virlJl fll of[tC/(dlimb (~ III( rrjitcliolloftht wm!ftclI'dlimb ill tfJt mirro') Ik/. fl1/omlJlf 'Ip/ittmlll(( ItndItM mOlI(S "onn,dly. It rr"Mitt! I",knoumuJ)) fl>;s Immn(1lf u'V'*'.
V Nn,ro/",Ihk /",i1/ is dtfintd as/",in "'lsittg "." dirrri.:o"l(q"(1I(( of0 Inion ordi!rmt flffirting Iht IOn"lIOl('I!Ory s)#(",(41)
pred ominant mon o- or oligoneuroparhy (SF N), initialed by limb
trauma (42). The concer t shares some argumem s with rhae of a
'ne urogenic intlammalion' (see next section) and demands tha e CRPS
signs. symptoms and assodared tissue inflanllllation are caused by the
co nsequences of end-o rgan (includ ing swear gland s and small vessels)
partial dcnervarion , by malfunctioning of neighbouring survivors to
rhe dea d small fibres (' irdmhle noctccpror s'), and by result ing central
changes (4 2). The cause for rhe first srep in the proposed cascade of
events. the posrrraumatic death of small fibres is curre ntly unknown.
Of rhc recom mended first or secon d !inc treatments for neuropathic
pain (43), only Ga bape ntin ar a submaxlma l dose of 1800mglday has
yet been assessed, with negative result (44).
7) !lIjI'lmmaliOlI (till txplttill cliniml CRPS ,igmTh is was o riginally propo sed by Peter Sudec k ('Sudl:Ck's atrophy' )
(45). Th e painful C RPS·a ffl'Cled limb is often red , hor and swollen,
with reduced fun ction : the five card inal signs of inflammation (46).
And indeed recent research fou nd that inRammarory mar kers are
elevated in blister Huid from C RPS-alfecred limbs (47 ). However
rhe titre of these markers is nor related 10 rhe pain int ensity and
mark ers can rema in high even if the pain disappear s (48). One small
randomized control tria l has suggesred that ste roid treat ment is
effective in very early CRrs and some clinicians find this observano n
co nfirmed by their clinical experience (49) . In longstand ing CRI'S
intrathecal steroi ds are nat effective (50). TNf-alpha rrenmenr has
been prop osed, bur no RCT has been conducted. l .enalidomide, a
highly toxic anti-inflammatory thalidomide derivative W<lS rested
in one of the largest ever tr ials in CRPS, bur untonunarely the
co mpanr (Celge ne) has nOI published rhe results.
It remains unclear which cells lnltiate CRPS inflammation . One
possibility is that neuropepndes. antidromically released from
by guest on March 15, 2014bjp.sagepub.comDownloaded from

6
1l.!! V l f W S I N P A I N
V O L. S - ~ O. 2 - J U ~ E 20 1 1
sensory neuro ns cause skin reddenin g and swelling thus producmg
C RPS signs ('neuroge nic inflammation'); immune mediator release
may follow. In detailed experiments, Frank Birklein's team has
indeed confi rmed an abnormality uf the neuropepnde handl ing
in CRPS and termed what they fou nd 'facllirated neurogenic
inflamrnarion'(S I). They showed that when c-fibres in affecred {and
ro a lesser degree also unaffec ted (52» limbs are stimulated , CRPS
patients respon d with r nuch Stronger [neuropep ride-rned iared) skin
redd ening and swelling than control pat ient s. The cause is unclear.
It is possible tha t in C RrS these ncuropepddes. OIKe released are
not p roperly merabolbed. The Importance of neuropeprides for
the C Rrs pathophysiology hal gained furt her credence by the
recenr finding that C RPS is associated with intake of angjcrensicn
conve rting enzyme (ACE)-inhibiror medication (53). ACE
rnerabolises the neuropeprides substance P and brad ykinin to inact ive
fo rms, th us ACE- inh ibitol> may lead to higher t issue levels of both
neuropcpndes. Up until now, these interesting find ings have not
rranslared into clin ical treatments.
Alternative concep ts on the CRrs parhophysiclogy
Some auth ors have placed C Rrs broadly into the context of
somatofo rm disord ers or malingering. A few aut hors have also taken
the fact that CRI'S I ~'I is not associated with structuralles ions as
evidence that this prohlem should he,at k>;)st in part of psychological
origin (54). Recent more systematic investigations were not
corrobo rative (35 5). StrI.'SSful life events may hemor e common in
patients before developrn em of the cond ition (55). Some people self
indu ce injuries 10 resemble C RPS (56).
Although th is has not been systematically assessed, it is my clinical
impression that patients can feel srtgmarised by health professionals
who did nor believ e thnt their condition is ' real'. The sclcnrtfic
evidence in suppo n of somansauo n and malingering as causes for
C RPS is meagre at best. Interestin gly, almost hidd en from mose
d inidans there call he intense arguments in the medico- legal
contexts about the causes of C RPS. Stakes in the context of work
related injuries can be high, and 'psychogenic' concepts about the
C RPS pathophysiology may be cited more frequently tha n would be
in clinical situations.
In common with other chro nic pain s, CRPS should best be seen as a
bio psychosocial conditio n. Randomised controlled trials ofcognitive
behavioural ther apy in CRPS arc st ill missing. The UK guideline
group will recom mend cognitive behavioura l therapy as one of the
four pillars of treatment (Figure 2).
Genenc pred isposition is important in a wide range of medical
disorders. Several groups have examined genetic associations in
C RPS, but to dat e no robust association has been found (57) .
Ge nome-wide associat ion studies have nOI yet been accomplished .
VI CRPS 1/2 iJ d(finrd <ISwithlu'ifhol<1d.mJltg( to a maior ,,(rV(,
Recommend ations for t he treatmen t of e Rr s
(il patients should be educat ed about CRPS and be given simple
information on self-management such as advice to dtrec r attenti on 10
the limb and to stroke and use il frequently and gemly.
[ii) most pat ient s requ ire specialised physiotherapy delivered by
physiotherapists or occupatio nal therapists experienced in the
treatment of patients with chro nic pain (Figure 2). Th is should be
initiated as early as possible, recogntztng that advice to gently move
the frequendy red. swollen and painful limb of early CRPS can
sometimes appear counte rin tuitive to pat ients and pracnnoners.
lrnporranr met hods include desensirisarion (rubbing the affected
limb gently with cloth), gradual weight bearing, stretchin g and
funct ional and fine mutor exercises. Since the required expertise to
deliver these rrearmems is not universally available, the dev elopm ent
of a network app roach app eal>useful. where stakeholders in a region
kno w 10 locate th e regional expert cenrrets) and/or experienced
practitionerfs). More research is needed to better understand the
relation between early physioth erapy treat ment and prevention of
late complications (such as ankylosis and contractu re).
(iii) mult idisciplinary pain management treatment, guided by
princip les of cognitive behavioural therapy should be conside red
early for those patie nts who do not imp rove, and who show signs of
distress. Here again stakeholders should know of the nearest cent re
which offers such service.
[lv ) a number of novel drug or lnrcrvcmional trcarmenr s, which
may provide pain relief have been described. however confirmatory
tr ials are required for mOSI before recomme ndat ions can be given.
It is reasonable 10 Initially treat patients wirhdru gs developed for
neuropathic pain, although there is no C RPS-specific evidence for
any of thes e trcatnt entsVl1• In addition , a one off pamidro nate 60mg
lv infusion treatment should be conside red for those with less than 6
mon ths dura tion. Intravenous regional sym pathetic blocks (IVRSB)
should not rou tinely be used in the treannenr of C RI'S since four
randor nised cont rolled trials have not demonst rated any benefit.
Pragmati cally, in rhose rare patient s with early CRPS , for whom
101."<11annesrhedc tnjccnon 10 sympat hetic ganglia provides days or
weeks uf pain relief, th is treatment may bridge the lime untilthe
disorder gets better by itself, however more research is needed before
a recommendation can be made - imp ortantly repeat blocks will
nOI prolong the analgesic effecl. In the UK, spinal cord stimulator
(SCS) treatment is the only NIC E approved method 10 treat CRrS .
Wit h time, the SCS effect docs slowly d iminish, so rhar in the
Re T the SCS results d id not exceed those in the 'physical therapy'
control group from 3 years after implantat ion (58) . The authors of
the seminal RCT conclude that, altho ugh pat ient satisfactio n was
generally high, 'the unknown working mechanisms of the (SCS)
treatment app arentl y do not function indefinitely' (59). Spinal
cord stimulato r treatment may be appropriate where th ese other
treatment s do not provide benefit. Unfortunately, even with best
Vll f800"'gg(lb"fHwhiltL" is 1101(jJt(tiw (44)
by guest on March 15, 2014bjp.sagepub.comDownloaded from

V O L . S - N O .2 - J U N E 20 1 1
R E vr E W S r N p }.r N
7
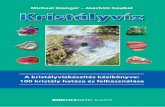
Figure 3. 7h1' m,ll/(/Kl'ml'''' ofe RPS in prinMrJ (/Jld $I'(()I/(imy((/T/' ( (/1/ i l/Vo/vl'sPl'Cilllisl$.from(/ witii' mlltl' ofhmlth(1Irt' profnsiom.
current treatment app roaches some patient s may not experience
sufficient pain relief.
(v)p"iOpmlfi~ Cllrt' ,md prt'Vl'lIIioli '1Ji" trauma: The risk of surge ry
causing a severe new C RPS episode in someo ne who had CRPS in
rhe pasr is probably neither high nor zero (60) . lr seems commo n
sense ro defer operating in an early case of C RPS umil acut e
symptoms have subsided . if at all possible, to reduce rhe risk of
aggravating rhe cond ition , though even for such recomme ndation no
RCf-derived evidence exists. 'Ih ere is no evidence for the supe rloriry
of any anaesthetic techniq ue ro prevent re-igniting or aggravating
CR I'S. 'Ihcrc is preliminary evidence in favour of giving oral vitamin
C after dorsal radius fracture (500 mg x 50 days), but more evidence
is needed before this can he recommended (30)
(vi) 101l[-trrl/l carer Nor a single publication ro dat e has described
how we should care for rhose who have rrialled available physical,
behavioural and pain relief treatments, but who still have ongoin g
pain and a reduced quali ty oflife. Any lon g-term approach shou ld hepatien t-centred and includ e facihrared wars for rhe patient 10 wques r
re p-up suppor t (e.g. by wa y ofoccasional on-demand cons ulration
with a named specialise physiotherapist . psychologist or doctor},
attendan ce of self-support groups under the umb rella of, or wit h
some link to the medical trearmenr centre, and access to informarion
about available suppo rt for dcvcloptn g adapted work, leisure and
social activities. In a recent series ofC RPS focus group discussions ar
our centre , paucms named rhc educat ion of healrhcare professionals,
particularly the ir GP's, about C RPS a 101' priority (in prepara tion).
In itiatives in the UK to enha nce rhe care of patients with CRrs
and research into Ihis co nd ition
Late d iagnosis ofC RPS may lead to unnecessary suffering from
nor knowing what is going on and , in some cases, inappropriate
treatment. In addition, where patients never reach pain management
specialists, research is not so easy to conduct. 'When we looked at
enro lling patients to our, now completed randornised contro lled
trial in cent ral Lond on, we saw only two suitab le patients wit h
longstanding CRPS within a 2.5 year period , in a busy pain clinicwith a direc t catchment area of 600 .000 populanon plus tertia ry
referrals, suggesting that patients in this area are nor referred to
specialist care. You could check rhis fur your own region: Assuming
the published incidence- and recovery rates, you should see every year
4 new patients with un -resolvln g C Rr s of", I year duration / loo.Ooo
of your catchme nt pop ulation; furth er, supposing an average 15 year
duratio n, you should have 60 C RPS parient s/JOO.OOO catchment
area pop ulation on your books . ls this number anywhere remotely
dose to the number of patie nt you see~ At least in some UK regions
it is not. 'Where are these pariems ? We susf'C'-"l: tha t they may either
remain undi agnosed, or that they do not reach pain services.
In order to address these issues, Chris Barker (Specialist in pain
medici ne, Sello n community pain services) and I initiated in 200 8
a mult idisciplinary UK guidance workshop series with an aim to
support the d iagnosis and appropriate management of pat ient s with
CRrS across the wide range of those health professional s who see
rhem (Figure 3). 111e guidance development process has lIOW been
adopted by the Royal College of Physician 'Concise G uidance series',
and {his process (but nor yet the produ cr) ha-s been suppor ted by 3
Royal Colleges and 8 UK professional organisations induding the
Faculty of Pain Ml-dicine with in {he Royal Co lleges of Anacsrhertsrs
and {he British O rthopaedic Association. We hope to complete
rhts process and distribute the guidance by summer 201 1. Chris
Barker has also led efforrs to revise {he G i' ' read codes ' fur C RPS.
Read codes appear when a GI' enters a certain med ical term into the
electronic records database. Up until lase year the term 'CRPS' 0 1
'Complex Regional Pain Synd rome' was not rec ognized , but rhis has
now been changed and Gl"s are given the oprion to link to a shn rr
explanatory lcatier abou r the condition.
Candy McCa be has previously reported in ' BPS's newsletter un rhe
foundation of the 'C RPS Network UK' , a mul tid isciplinary group
of currently 10 clinicians and researchers with a special interest in
e RpS (6 1). This group aims to enhance clin ical care for and research
into C RPS in the UK, and liaise with other European investigators.
We welcome interested clinicians to join the network. Should YO Il
be interested (membership is Informal and open ), please do comacr
our administ rator, Mrs . Yvette Hibb ert fur further information and
upcoming mecnn g dates (appendix C). As a first joint project we
have (in 2008 ) established the UK CRPS registry, supported by
the cancer services information techn ology unir at the University
Southampton. Parriciparing investigators ente r, after taking informed
conse nt con racr data fur C RPS panems un this web-based dat abase.
By giving consent , patien ts agree tha t they can later be contacted
by researchers for ethics-approved project s. Database access will be
by guest on March 15, 2014bjp.sagepub.comDownloaded from

8
1l.!! V l f W S I N P A I N
V O L. S - ~ O. 2 - J U~E 2 0 1 1
managed by a stee ring committee, which will be happy to receive
propos-lis fur access from late 20 11. 111e manage mem lead for the
registry is Dr. Nic k Shenker (appendix C ). Th e registry currently
hold s 140 entr ies of patients with longstanding CRPS, and
rec ruitment is going stro ng.
Fut ure developments: One never knows whnt is around the next
corner, however for my special area of aut oimmunity and imm une
mod ulation , I suspet;t that clini cians will event ually be offered
a seru m test for CRPS diagnosis, and that novel applicat ions of
imm unoglobuli n (such as low-dose home applicat ion) will he
assessed?'!',
SI//1//1/I/,YWe have learned a lot about C RPS in the Pa5t 10 years, and we have
even been given a glimpse upon some treatments which, for the first
tim e promise effective pain reduction fur those with lon gstanding
disease. To dal e all evidence is preliminar y, with the except ion of that
for Spinal Cord Stimulato r treatm ent and, potent ially, the treat ment
with bisphosphonares (12)'x. The quality of cl inical trials has mu ch
improved and the qua nt ity of research into the condition has
skyrocketed. Wh ile we still don't know what causes C RPS, one has
the sense that efforts to tackle thi s fascinating, debilitati ng co nd ition
are exemplary for the progress of the new field of Pain Med icine ro
come int o its own.
2
3
4
5
6
7
deMos M , De Bruijn AG, Huygen FJ, Die leman j R Stricker
BH , Sturkenboo m Me. The incidence of complex regional
pain syndro me: a popu lation -based study, Pain 200 7
May;129(1-2): 12-20.
de M M , H uygen FJ, Diele man Jp, Koopman JS, Stricker
BH , Sturkenboom Me. Medical histo ry and the ouse r of
co mplex regional pain syndrome (C RPS). Pain 2008 Del15;139(2):458-66.
de MM, H uygen FJ. Hoev en-Borgman M , Diek-man Jp, Ch
Str icker BH , Srurkenboom Me. O utcome of the complex
regional pa in syndrome. Clin J Pain 2009 Sep;25(7):5 90-7.
Birklein F. Co mplex regional pain synd rome. J Neurol 2005
Feb;252(2): 13 1-8.
Veldman PH , Reyncn H M , Arn tz IE, Goris RJ. Signs and
symptoms of reflex sympathetic dystro phy: prospective study of
829 pat ient s. lancet 1993 Ou 23;342( 8878) : 10 12-6.
Phillip s C, Main e. Buck R, AylwardM, Wynne-Jones G, Farr
A. Priorit ising pain in policy making: The need for a whole
s)'5tems perspect ive. Hcalrh Policy 2008 Occ:88 (2-3): 166 -75.
AckliOI/,kdgl'1l1l'11t
Dr. Goebel's work has bee n sup ported by the Pain RdiefFou/1darion,
Liverpool. M rs. Linda Cosslns for sup port of a recent systematic
review on treatmen ts for C RPS. 111e members of the UK C Rr S
guidelines group, the UK C RrS network, and the Liverpool CRPS
path way group for important suggcsrlons which underlay the
principles of treatm ent doc umented in thi s paper.
Confl ict ofimtrmDr. Goebel has received grant suppo rt from Talecds , SC, USA and
CSL- Behring, Bern, Ch, and a speaker honorarium from Baxter.
USA. T hese companies prod uce polyvalent immu noglobu lins.
R F.FF.R ENc r-s
Harde n RN , Bruehl S, Srar uon-Hicks M, Wilson PR. Propo sed
new diagnostic criteria for complex regional pain syndro me.
Pain Med 2007 May;8(4):326-3 1.
VH! 171t ui( ofimmunog!cbu/im iu tilt UK is mort tightly rtgukllrd dum inothrr cowll rin . bteauSf tllrrt had bun a lack ofmpply in Ihcpall. b,dk atioltJart
r,urgoriad illlo ltrvml CO/"Ul1"lid tltrrtllrfy e RPSil l/Otlisud til 'III i"dlmtion.An "!,!,/im lion I<> rtvilt thil to ·blut'I"" bu" IlIbmilud (bbu illdimln" diw lJtftr whim ,I,rrt iJ a rttIlOlI,tblr tl1idt1lctbalr but wlltl"rolhrr Irttlmlttlt optiom "rt1/l~lifablt
IX Bi>p/t(},pho"tl lt rrttllllltm um rif«tivt i" fOur'lIIa// ",,"wmiud contmllrdtn',,/.,i ll di',",r CRPSpop"t.lIiolil. 17,rworki"g mtel", ,,i, ,,, ofbi<pho,p!IlJIIllln ill
CRI'S i, ",i/",ow" . bill nlllJ br amNujltlll/lI/tI/I}ry. J,[o;t pati(lllf Irmlcd in I}mtftur tn'II/., !",d ((/r~y CRPS.
8 Kemler MA, Furnee CA . Economic evaluation of spinal
cord srimula rion for chro nic reflex sympa thetic dystrophy
Neurology 2002 O Ct 22;59(8 ); 1203"9.
9 Kemler MA, Bnrendse GA, van KM , de Vet HC, Rijks C P,
FIITIICC CA, er al. Spinal cord srhn ulanon in pati ent s with
chronic reflex sympathetic dystrophy. N Engl J Med 2000 Aug
3 1;343( 9) :6 18-24 .
10 Go rrberg K, Eina rsson U, Ynerbcrg C , de Pedro C], Fredriksen
S, von KL, er al. Health-related qu ality of life in a po pulation
based sample of peo ple with mul tiple sclerosis in Stoc kho lm
Co unty Muir Seier 2006 0a: 12(5),605·12.
11 van der LaanL. Veldman PH , Goris RJ. Severe complications
of reflex sympathetic dysrrophy infecdo n, ulcers, chronic
edema, dystonia, and myoclo nus. Arch Phys Med Rehabil 1998
Apr;79(4):424-9.
12 Foro uzanfar T, Koke AJ, van KM , Weber WE . Treatment
of co mplex regional pain synd rome type I. Eur J Pain
2002;6( 2):10 5-22.
13 Schansc hnelder J, Hartung K, Stengel M , Ludwig J , Binder A.
Wasner G, et al. Endo thelial dysfunct ion in cold type complex
regional pain synd rome. Neu rology 2006 Aug 22;67{4):673-5.
14 EVANS JA. Reflex sympathetic dystrop hy; repc« on 57 cases.
An n Intern Med 1947 Ma r;26 (3):417-26.
by guest on March 15, 2014bjp.sagepub.comDownloaded from

V O L . S - N O.2 - J U N E 20 1 1
R E VI E W S I N P }.I N
9
15 Hannington-KHf JG . Int ravenous regional sympat hetic block
with gua nethid ine. La ncer 1974 May 25;1(7865): 10 19-20.
16 Livingstone JA, Atkins RM . Intravenou s regional guanethidine
blockade in the treatment of pos t- traumatic complex region al
pain synd rome type I (algodysrrophyl of the hand. J Bon e
joint Surg fir 2002 Apr;84(3):380-6.
17 Price DO, Long S, Wilsey B, Rani A. Analysis of peak
magnitude and durat ion of analgesia produced by 10Cl1
anesth etics injected into sympat hetic ganglia ofcomplexwgional pain syndro me patients. Clin J Pain 1998
ScI':14(3):216-26.
18 Rod rigw_'l RF, Bravo I.E, Tovar MA, Castro F, Ramos G E,
Dazn P. Study of the anal gesic efficacy of stellate ganglion
nblock ade in the ma nageme:nt of the co mplex regional pain
synd rome: in patients with pain media ted by sym pathet ic
nervous syslem: preliminary study. Rev Soc Esp Do lor
2006;4:230-7.
19 Latremoliere A, Woolf CJ. Ce nt ral sensitization: a gencrator of
pain hypersensiriviry by central neural plasticity. J Pain 200 9
Sep: 10(9):895-926 .
20 Sigterrn.ms MJ , Van Hihen JJ, Bauer Me. Arbous MS,Marinus J, Sanon EY,et al. Keramine prod uces effective and
lon g-te:rm pain relief in paticnt s wilh Complex R~"gional Pain
Syndro me Type 1. Pain 2009 OCt;145(3):304-1J.
2 1 Kiefer RT, Rohr P, Ploppa A, Diererlch HJ , O rorhusen ] .
Koffler S, er al. Effica~y of Kcramine in Anesth et ic Do sage for
the Trearmcnr of Rcfr,KlOry Complex Regional Pain Syndrome:
An O pe n-Label Phase II Study. Pain M~'lI 200 8 Feb 5.
22 Bdl RF, Moore RA, lm ravenous ketarninc for C RPS: Ma king
tOO mu ch of100 little? Pain 20 10 Jul;150( I): 10- 1.
23 Co llins 5, Zu urmo nd WW, de Lange JJ, van Hllre n BJ,
Perez RS. Intravenous magnesium for co mplex wgio nal pa in
synd rome rypc I (C RPS I) pat ients: a pilot study, Pain Med
200 9 Jul ;1O(5l :930 -40 .
24 Goebel A, Vogel H . Ca ncrts O . Bajwa Z , Cl over L, Roewer
N . er al. Immune r~-spon ses to Campylobacrer and serum
autoant ibodi es in patient s with co mplex regional pain
synd rome. J Neuroimmunol 2005 May;162(1-2l:184-9.
25 Blaes F, Sch mitz K. Tschernarsch M . Kaps M. Krasenbrfnk
I, Hempd mann G , er al. Autoimmune enology of complexregional pain syndro me (M. Sudec k). Ne urology 2004 Nov
9;63(9): 1734 -6.
26 Kuhr D , Tschem atsch M. Schmitz K, Singh 1'. Kaps M.
Schafer KH , er al. Auto ant ibod ies in complex regional pain
syndrome bind to a differendado n-dep endenr neu ronal surface
auroan tlgen. Pain 200 9 Jun;143(3):246 -5 1.
27 Goebel A, Baranowski AP, Maurer K, Ghiai A, McC abe
C, Ambler G . Intravenous Immunoglubulin Trearrnenr of
Co mplex Regional Pain Syndro me: A Rand omized Trial. An n
Intern Med 20 10;152 (3): 152-8.
28 G roeneweg G, Huygcn FJ. NiehofSI'. Wesseldijk F, Bussmann
JB . Schasfoon Fe. et al. Effect of tadalafil on blood flow, pain,
and function in chronic cold co mplex regional pain synd rome:
a rand omized cont rolled trial . BMC M usculoskcle r DiSON
200 8;9 : 143.
29 Coderre TJ , Xanrhos ON, Francis l., Benn ett GJ . Chro nic
posr-ischc r nia pain (C PIP): a novel animal model of com plex
regional pain syndro me-type I (C RrS-I; reflex sympathe tic
dystrophy) prod uced by pro lon ged hlndpaw ischemia and
reperfusion in the rar. Pain 2004 Nov: 112(1-2):94-10').
30 Zo llinger PE. Tuinebreijer W E, Kreis RW; Breederveld
RS. Effect of vitamin C on frequency of reflex symparhenc
dystrophy in wrist fractures: a rando r nised trial. Lancer 199 9
D~'(; 11;354(919 5):2025-8.
3 1 Mai ho fner C, Handwerker H O , Neu ndo rfer B, Birklein F.Patterns of conical reorganiza rlon in co mplex regional pain
syndro me. Neuro logy 2003 Dec 23 ;6 1(12):1707-15.
32 Mai ho fner C, Hand werker H O , Neu ndorfer B. Birklein f.
Co nical rcorgar uaadon during recovery from complexregional
pa in synd rome. Neurology 2004 Aug 24;63(4):693-70 1.
33 Lewis JS, Kersten P, M~-cahe CS. Mc l' herson K.'vj, Blake
D R. Body perception disturban ce: a concrtbunon 10 pain in
complex regional pain syndro me (C Rrs). Pain 2007 Dec15;\ 33(1-3): 111-9.
34 M oseley GL 'Why do people with complex regional pain
syndrome lake longer to recognize their affected hand?
Neurology 2004 Jun 22 ;62{12):2182-6 .
35 M oseley G l. Grad ed motor imag ery is effective for lon g
standing complex regio nal pain synd rome: a randomised
controlled tri al. Pain 200 4 Mar ;108(1-2):I92-8.
36 Mc;Cabe C S, Haigh ac, Ring EF, Halligan PW; Wall
I'D . Blake D R. A co rurolled pilot stu dy of the utiliry of
mirror visual feedback in the rrearm enr of co mplex regional
pa in syndro me [rype I ). Rheu mato logy (Oxford) 2003
JanA2(I ):97-1OI.
by guest on March 15, 2014bjp.sagepub.comDownloaded from

1l.!! V l f W S I N P A I N
V O L. S - ~ O. 2 - J U~E 20 1 1
37 Cacchto A, De BE, Necoztone S, d i OF, Santilli V. Mirror
therapy for chronic complex regional pain syndrome rype I and
stroke. N Eng!J Med 2009 Aug 6;36 1(6):634-6.
38 van der LI.. rer Laak HJ, Gabrecls-Pesren A, Ca brecls F,Goris
R]. Complex regional pain syndrome lYpe I (RSD) : pathology
of skeletal muscle and peripheral nerve. Neurology 1998Jul;5 I (I ):20-5.
39 Albrecht PJ , Hines S, Eisenberg E, Pud D, Finlay D R,
Conno lly M K, er al. Pathologic alterat ions of cutaneo us
innervation and vasculature in affected limbs from
patients with complex regional pain syndro me. Pain 2006Feb;120(3);244-66.
40 Daklander AI.. Rissmiller JG , Gelman LB, Zheng L, Ch angY, Con R. Evidence of focal small-fiber axonal degeneration
in complex regional pain syndrome-I (reflex sympathet icdystrophy). Pain 2006 Feb;120 (3):235-43.
4 1 Treedc RIJ , Jensen TS, Campbell IN, C ruccu G, Dosreovsky
JO, Griffi n JW, et al. Neuropath ic pain: redefinition and a
grading system for clinical and research purposes. Neurology
2008 Apr 29;70 (18): 1630-5.
42 Oaklunder AL, Fields H L. Is reflex sympathetic dystrophyl
complex regional pain syndrome type I a small-fiber
neuropathy? Ann Neurol2oo9 Jun;65(6):629-38.
43 Dworkin RH , O 'Co nnor AB, Backonla M, Farrar JT.
Finnerup NB, Jensen TS, et al. Pharmacologic management of
neuropathic pain; evidence-based recommendations. Pain 2007
Dec 5;\32(3):237·51.
44 van de Vasse AC , Stomp -van den Berg SG, Kessels AH, Weber
WE. Randornised controlled trial of gabapcmtn in ComplexRegional Pain Syndro me type I [ISRCfN84 121379]. BMC
Neurol2004 Scp 29;4; 13.
45 Sudeck P. Ueber die anne enrzucndltche Kn<Xhenatrophie.Arch Klin Chir 1900;62;147-56.
46 Rather LJ. Disturbance of function (funcrio laesa): the
legendary filth cardinal sign of inf lammation, added by Galen
to the four cardinal signs of Celsus. Bull N Y Acad Med 1971Mar;47(3):303-22.
47 Huygcn FJ, De Bruijn AG, De Bruin MT, Grocneweg JG ,
Klein J , Zijistra FJ. Evidence for local inflammation in complex
regional pain synd rome type I . Mediators InAamm 2002Feb; I I(l ):47-51.
48 Wessdd ijk F, Huygen FJ. Heijmans-Anronisscn C, NiehofSP,
Zijlma FJ. Tumor necrosis factor-alpha and inrerleukin- f arenot correlated with the characteristics of Co mpk'X R~'8ional
Pain Syndrome type 1 in 66 pat ients. Eor J Pain 2008Aug;12(6);716-21.
49 Christensen K, jensen EM. Noer I. The reflex dystrophy
syndrome response to treatment with systemic curticosreroids.
Am Chir Scand 1982;148(8):653-5.
50 Munrs AG, van der Pb s AA, Ferrari MD, Tce pe-Twiss 1M ,
Martnus J. Van Hilren JJ. Efficacy and safelY of a single
intrathecal methylprednisolone bolus in chro nic complex
regional pain syndro me. Eur J Pain 2009 Dec 15.
51 Birklein F,Schmelz M , Schlfrer S, Webt:t M. 111e important
role of neurope pt ides in complex regional pain syndrome.
Neu rology 200 1 Dec 26:57(12):2179-84 .
52 Leis S, Weber M , Schmelz M , Birklein F. Facilitated
neurogenic inflammation in unaffected limbs of patients with
complex regional pain syndro me. Neuroscl Len 2004 Apr
15;359(3):163-6.
53 de MM , Hu yg en FJ , Stricker BH, Dieleman J P, Srurkenboom
Me. The association between ACE inhibitors and the complex
regional pain syndro me Suggestions for a neuro-Inflammarory
pathogenesis of CRPS. Pain 2009 Apr; 142(3):2 18.24.
54 Verd ugo RJ, Ochoa j l., Abnormal moverncnrs in complex
regional pain synd rome: assessment of their nature. Muscle
Nerve 2000 Feb;23(2);198-205.
55 Beerthuizen A, van 't SA, Huygcn FJ, Klc tn], de WR. Is
there an association between psychological factors and the
Complex Regional Pain Synd rome type 1 (C RPSI) in adults?A
systematic review. Pain 2009 Sep; 145(1·2 );52-9.
56 ,\-h ilis-Gagnon A, Nicholson K. Blumberger D. Zurowski
M. Characteristics and periodp r~'Val el\ce of self-induced
d isorder in patients referred to a pain clinic with the diagnosis
of complex regional pain syndrome. Clin J Pain 2008Feb;24 (2):176-85.
57 de Rooij AJ\-1 , de MM . Van Hilren j], Srurkenboom Me.Gosse ME van den Maagdenberg AJ\-1 , er al. Increased risk of
complex regional pain synd rome in siblings of patients! J Pain2009 D~'i:;10( 12): 1 250-5 .
58 Kemler MA, de Vet H C, Barendse GA, van den W ildenbt:rg
FA, van KM. Spinal COld stimulation for ch ronic retlex
sympathetic dys trophy-five-year follow-up. N Engl J Med2006 jun 1;354(22):2394-6.
by guest on March 15, 2014bjp.sagepub.comDownloaded from

R E VI E W S I N P }.I N
V O L . S - N O .2 - J U N E 20 1 1
59 Kemler :-'iA, de Vet He. Barendse GA, van den Wildenberg
FA, van KM. Effect of spinal cord stimulation for ch ronic
complex regional pain syndrome Type I: five-year final follow
up of patients in a randomized cont rolled trial. J Neurosurg2008 Feh;108(2):292-8.
60 Veldman PH, Gorts RJ, Surgery on extremities with reflex
sympathet icdystrophy Unfalk hirurg 1995 Jan;98(1):45-8.
61 McCabe C. The e RPS UK network. BPS Newsletter
2007;sp ring:17,
APP E NDI X
A) Now superseded old terms for CRP S:
Algodymophy
Shoulder-Hand Syndro me
Reflex Symparheric Dystroph y
Algodysreophy
Causalgia
Sudeck'satrophy
B} Budapest Diagnostic Criteria for C RrS
All of the following statements must bemel:
• The patienthas continuing painwhich isdisproportionate to the inciting event• The patient hasat leastone sign intwo ormore of the categories below• The patient reports at least one symptom inthree or more of the categories below• No other diagnosiscan better explain thesigns and symptoms
category SlgnlSymptom
1 'sensory' allodynia (painto light touch and/or temperature sensation and/or deep somatic pressure and/or joint movement')and/or hyperalgesia (topinprick)
2 'vasomotor' Temperature asymmetry (>t"C if counted as a sign) and/or skin colour changes ami/or skincolour asymmetry
3 'sudomotor/oedema' Oedema and/or sweating changes and/or sweating asymmetry
4 'motor/trophic ' Decreased range of motion and/ormotor dysfunction (weakness, tremor,dystonia) and/ortrophic changes (hair/naiVskin)
C) Co ntact de-tails and links
CAPS NetworkUK: Mrs. Yvette Hibberd Yvette,[email protected],uk
UK CRPS Registry: Dr,NickShenker nichotas.shenierwaooenorookes.nhs.uc
liverpool Centre forImmuneStudies inPain: httpJlwww,jiv,aC.uk!prilcisp/
X 7J~ J~" ")laud ulldmtt",ding o/"'/fody"i'" as!,"btji,1Irm"/ioll to" "umb(ro/.m,,-p"i"fi' [5timuli i5mrrmt!y .",&r l'(l'i(1lJ by tJ,( IASP ttlX(J/Jo",y gro"p.SOIl!( (X!' ( rtI 1II.fgl'll tl " " t f,( /(t'nl "lIody"in JllOuld b, m (nqd o,,/yftr brwh,trok, (/JOk,d !,,,i ,, rd,Y1l"mic m(r/"miml ,,//od.Y1lin).
by guest on March 15, 2014bjp.sagepub.comDownloaded from