Promoting integrated tB/HiV SerViceS tHrougH one-StoP-SHoP ... · death among people living with...
2
SEPTEMBER 2014 This fact sheet has been developed by the TB CARE II project and is made possible by the generous support of the American people through the United States Agency for International Development. The contents of this fact sheet are the sole responsibility of University Research Co., LLC and do not necessarily reflect the views of USAID or the United States Government. M alawi has an HIV prevalence rate of 10.3% and a TB incidence rate of 163 per 100,000. Nearly 60% of TB patients are co-infected with HIV. TB is the leading cause of death among people living with HIV/AIDS. HIV-positive TB patients have worse treatment outcomes than HIV-negative TB patients, and TB-related mortality among TB/HIV co-infected patients is particularly high during the first two to three months of TB treatment. Early initiation of ART during TB treatment has been shown to improve survival. Despite high levels of TB/HIV co-infection in Malawi and Southern Africa in general, these two diseases have been traditionally treated separately under separate vertical programs. Lack of coordination between National TB Control Program (NTP) and HIV/AIDS Department negatively impacts TB/HIV prevention, care and treatment, as patients are forced to travel to different clinics, make and wait in line for different appointments, and see different health care providers. Studies from Malawi have proven the integrated TB/HIV service delivery model to be more effective in terms of higher percentages of TB patients counseled and tested for HIV, as well as started on ART. 1 In Malawi, TB CARE II is working with the NTP and the Ministry of Health to improve care and treatment outcomes for TB/HIV co-infected patients through a one-stop-shop model of integrated TB/HIV services. Under the one-stop-shop model, TB, HIV, and co-infected patients are able to access a full package of services at one location, managed by one health care worker or health care team. For example, TB patients coming for TB treatment are offered HIV counselling and testing, and HIV patients coming for ART are routinely screened for TB. TB/HIV co- infected patients are able to get both TB treatment and ART at once, from staff who are able to more closely monitor their dual treatment outcomes. Health care teams are trained and equipped to provide TB screening and treatment, HTC, ART, as well as other services, including treatment for opportunistic infections and STIs. Patient data, as well as screening, monitoring, and reporting tools, are integrated to ensure high quality and comprehensive care. PROMOTING INTEGRATED TB/HIV SERVICES THROUGH ONE-STOP-SHOP MODEL 1 “K.Chifundo, et al. What is the best model of TB/HIV service delivery? Experience from Malawi. : AIDS 2010 - XVIII International AIDS Conference: Abstract no. MOPE0858 “ TB CARE II is a five-year cooperative agreement from the United States Agency for International Development (USAID) led by University Research Co., LLC (URC) designed to provide global leadership and assist National Tuberculosis Programs (NTP) in high burden countries around the world to accelerate the implementation of programs for TB DOTS, TB/HIV and Programmatic Management of Drug Resistant (DR) TB (PMDT). TB CARE II currently operates field-based programs in Bangladesh, Malawi, South Africa, and Vietnam. One-Stop-Shop Model for TB/HIV Services One patient record: Integrated patient records and monitoring tools, data sharing among TB/HIV services One care team: Health worker capacity to deliver both TB and HIV services TB patients: • TB Treatment • HTC TB/HIV patients: • ART • TB Treatment • CPT HIV patients: • ART • TB screening and diagnosis TB and HIV Services Offered Under One Roof
Transcript of Promoting integrated tB/HiV SerViceS tHrougH one-StoP-SHoP ... · death among people living with...

september 2014
This fact sheet has been developed by the TB CARE II project and is made possible by the generous support of the American people through the United States Agency for International Development. The contents of this fact sheet are the sole responsibility of University Research Co., LLC and do not necessarily reflect the views of USAID or the United States Government.
Malawi has an HIV prevalence rate of 10.3% and a TB incidence rate of 163 per 100,000. Nearly 60% of TB
patients are co-infected with HIV. TB is the leading cause of death among people living with HIV/AIDS. HIV-positive TB patients have worse treatment outcomes than HIV-negative TB patients, and TB-related mortality among TB/HIV co-infected patients is particularly high during the first two to three months of TB treatment. Early initiation of ART during TB treatment has been shown to improve survival. Despite high levels of TB/HIV co-infection in Malawi and Southern Africa in general, these two diseases have been traditionally treated separately under separate vertical programs. Lack of coordination between National TB Control Program (NTP) and HIV/AIDS Department negatively impacts TB/HIV prevention, care and treatment, as patients are forced to travel to different clinics, make and wait in line for different appointments, and see different health care providers. Studies from Malawi have proven the integrated TB/HIV service delivery model to be more effective in terms of higher percentages of TB patients counseled and tested for HIV, as well as started on ART.1 In Malawi, TB CARE II is working with the NTP and the Ministry of Health to improve care and treatment outcomes for TB/HIV co-infected patients through a one-stop-shop model of integrated TB/HIV services.
Under the one-stop-shop model, TB, HIV, and co-infected patients are able to access a full package of services at one location, managed by one health care worker or health care team. For example, TB patients coming for TB treatment are offered HIV counselling and testing, and HIV patients coming for ART are routinely screened for TB. TB/HIV co-infected patients are able to get both TB treatment and ART at once, from staff who are able to more closely monitor their dual treatment outcomes. Health care teams are trained and equipped to provide TB screening and treatment, HTC, ART, as well as other services, including treatment for opportunistic infections and STIs. Patient data, as well as screening, monitoring, and reporting tools, are integrated to ensure high quality and comprehensive care.
Promoting integrated tB/HiV SerViceS tHrougH one-StoP-SHoP model
1 “K.Chifundo, et al. What is the best model of TB/HIV service delivery? Experience from Malawi. : AIDS 2010 - XVIII International AIDS Conference: Abstract no. MOPE0858 “
TB CARE II is a five-year cooperative agreement from the United States Agency for International Development (USAID) led by University Research Co., LLC (URC) designed to provide global leadership and assist National Tuberculosis Programs (NTP) in high burden countries around the world to accelerate the implementation of programs for TB DOTS, TB/HIV and Programmatic Management of Drug Resistant (DR) TB (PMDT). TB CARE II currently operates field-based programs in Bangladesh, Malawi, South Africa, and Vietnam.
One-stop-shop model for tb/HIV services
One patient record: Integrated patient records and monitoring tools, data sharing among TB/HIV services
One care team: Health worker capacity to deliver both TB and HIV services
TB patients:• TBTreatment• HTC
TB/HIV patients:• ART• TBTreatment• CPT
HIV patients:• ART• TBscreening
and diagnosis
TB and HIV Services
OfferedUnderOneRoof

University Research Co., LLC • 7200 Wisconsin Avenue • Bethesda, Maryland 20814-4811 • USA • 301-654-8338 • www.urc-chs.com
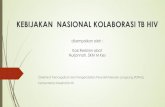
Mangochi District Hospital RenovationsIn 2014, TB CARE II funded the renovation of a one stop shop TB/HIV facility at Mangochi District Hospital. Previously, the environment at the hospital was not conducive to integration. TB and HIV services were offered in rooms far apart from one another, and patients were forced to stand in multiple lines to access multiple services. Some patients unfamiliar with the hospital were often confused where to go to access which services. The District Health Officer reported that many times, patients would simply give up before accessing the full array of necessary services. Now, the joint TB/HIV facility will be able to offer the full range of services to TB, HIV, and co-infected patients at one convenient location. The newly renovated facility was officially handed over to the district health office in September 2014.
To further improve the quality of services provided, TB CARE II supported and intensified TB case finding in HIV settings in order to identify TB patients among HIV-positive patients. Death audits are also being conducted to improve the clinical management of co-infected patients.
In the coming year, TB CARE II will work with the NTP and the HIV Department to establish five new TB/HIV one-stop-shop service centers in selected health facilities.
A waiting bay near an open window provides good airflow to reduce the spread of TB.
A new storeroom, to ensure the clinic has adequate stock of both TB and HIV testing materials and medications.
A new coughing booth, installed just outside the TB/HIV clinic, provides a place for patients to give sputum samples without risking spreading TB to others.
Before (top) and after (bottom) pictures of Mangochi District Hospital joint TB/HIV center. New windows permit greater air flow to reduce the spread of TB.