Pediatrics 2011--aterosclerose
46
Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents: Summary Report 1. INTRODUCTION Atherosclerotic cardiovascular disease (CVD) remains the leading cause of death in North Americans, but manifest disease in childhood and ado- lescence is rare. By contrast, risk factors and risk behaviors that acceler- ate the development of atherosclerosis begin in childhood, and there is increasing evidence that risk reduction delays progression toward clinical disease. In response, the former director of the National Heart, Lung, and Blood Institute (NHLBI), Dr Elizabeth Nabel, initiated development of cardio- vascular health guidelines for pediatric care providers based on a formal evidence review of the science with an integrated format addressing all the major cardiovascular risk factors simultaneously. An expert panel was appointed to develop the guidelines in the fall of 2006. The goal of the expert panel was to develop comprehensive evidence-based guidelines that address the known risk factors for CVD (Table 1-1) to assist all primary pediatric care providers in both the promotion of cardio- vascular health and the identification and management of specific risk factors from infancy into young adult life. An innovative approach was needed, because a focus on cardiovascular risk reduction in children and adolescents addresses a disease process (atherosclerosis) in which the clinical end point of manifest CVD is remote. The recommen- dations, therefore, need to address 2 different goals: the prevention of risk-factor development (primordial prevention) and the prevention of future CVD by effective management of identified risk factors (primary prevention). The evidence review also required an innovative approach. Most sys- tematic evidence reviews include 1 or, at most, a small number of finite questions that address the impact of specific interventions on specific health outcomes, and a rigorous literature review often results in only a handful of in-scope articles for inclusion. Typically, evidence is limited to randomized controlled trials (RCTs), systematic reviews, and meta- analyses published over a defined time period. There is a defined for- mat for abstracting studies, grading the evidence, and presenting of results. The results of the review lead to the conclusions, independent of interpretation. By contrast, given the scope of the charge to the expert panel, this evidence review needed to address a broad array of questions con- cerning the development, progression, and management of multiple risk factors extending from birth through 21 years of age, including studies with follow-up into later adult life. The time frame extended back to 1985, 5 years before the review for the last NHLBI guideline addressing lipids in children published in 1992. 1 This evidence is largely available in the form of epidemiologic observational studies EXPERT PANEL ON INTEGRATED GUIDELINES FOR CARDIOVASCULAR HEALTH AND RISK REDUCTION IN CHILDREN AND ADOLESCENTS ABBREVIATIONS CVD—cardiovascular disease NHLBI—National Heart, Lung, and Blood Institute RCT—randomized controlled trial PDAY—Pathobiological Determinants of Atherosclerosis in Youth BP—blood pressure HDL—high-density lipoprotein DM—diabetes mellitus CIMT—carotid intima-media thickness LDL—low-density lipoprotein T1DM—type 1 diabetes mellitus T2DM—type 2 diabetes mellitus TC—total cholesterol AAP—American Academy of Pediatrics DGA—Dietary Guidelines for Americans NCEP—National Cholesterol Education Program DASH—Dietary Approaches to Stop Hypertension CHILD—Cardiovascular Health Integrated Lifestyle Die FLP—fasting lipid profile CDC—Centers for Disease Control and Prevention AMA—American Medical Association MCHB—Maternal and Child Health Bureau FDA—Food and Drug Administration AHA—American Heart Association www.pediatrics.org/cgi/doi/10.1542/peds.2009-2107C doi:10.1542/peds.2009-2107C Accepted for publication Sep 8, 2011 Address correspondence to Janet M. de Jesus, MS, RD, 31 Center Dr, Building 31, Room 4A17, MSC 2480, Bethesda, MD 20892. E-mail: [email protected] PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2011 by the American Academy of Pediatrics FINANCIAL DISCLOSURE: Dr Daniels has served as a consultant for Abbott Laboratories, Merck, and Schering-Plough and has received funding/grant support for research from the National Institutes of Health (NIH); Dr Gidding has served as a consultant for Merck and Schering-Plough and has received funding/grant support for research from GlaxoSmithKline; Dr Gillman has given invited talks for Nestle Nutrition Institute and Danone and has received funding/grant support for research from Mead Johnson, Sanofi-Aventis, and the NIH; Dr Gottesman has served on the Health Advisory Board, Child Development Council of Franklin County, was a consultant to Early Head Start for Region 5B, has written for iVillage and taught classes through Garrison (Continued on last page) SUPPLEMENT ARTICLES PEDIATRICS Volume 128, Supplement 5, December 2011 S213 by guest on April 30, 2015 pediatrics.aappublications.org Downloaded from
-
Upload
gisalegal -
Category
Art & Photos
-
view
37 -
download
4
Transcript of Pediatrics 2011--aterosclerose

Expert Panel on Integrated Guidelines forCardiovascular Health and Risk Reduction in Childrenand Adolescents: Summary Report
1. INTRODUCTIONAtherosclerotic cardiovascular disease (CVD) remains the leading causeof death in North Americans, but manifest disease in childhood and ado-lescence is rare. By contrast, risk factors and risk behaviors that acceler-ate the development of atherosclerosis begin in childhood, and there isincreasing evidence that risk reductiondelaysprogression towardclinicaldisease. In response, the former director of the National Heart, Lung, andBlood Institute (NHLBI), Dr Elizabeth Nabel, initiated development of cardio-vascular health guidelines for pediatric care providers based on a formalevidence review of the science with an integrated format addressing allthemajor cardiovascular risk factors simultaneously. An expert panelwasappointed to develop the guidelines in the fall of 2006.
Thegoalof theexpertpanelwas todevelopcomprehensiveevidence-basedguidelines that address theknownrisk factors forCVD (Table1-1) to assistall primary pediatric care providers in both the promotion of cardio-vascular health and the identification and management of specific riskfactors from infancy into young adult life. An innovative approach wasneeded, because a focus on cardiovascular risk reduction in childrenand adolescents addresses a disease process (atherosclerosis) inwhich the clinical end point of manifest CVD is remote. The recommen-dations, therefore, need to address 2 different goals: the prevention ofrisk-factor development (primordial prevention) and the prevention offuture CVD by effective management of identified risk factors (primaryprevention).
The evidence review also required an innovative approach. Most sys-tematic evidence reviews include 1 or, at most, a small number of finitequestions that address the impact of specific interventions on specifichealth outcomes, and a rigorous literature review often results in onlya handful of in-scope articles for inclusion. Typically, evidence is limitedto randomized controlled trials (RCTs), systematic reviews, and meta-analyses published over a defined time period. There is a defined for-mat for abstracting studies, grading the evidence, and presenting ofresults. The results of the review lead to the conclusions, independentof interpretation.
By contrast, given the scope of the charge to the expert panel, thisevidence review needed to address a broad array of questions con-cerning the development, progression, and management of multiplerisk factors extending from birth through 21 years of age, includingstudies with follow-up into later adult life. The time frame extendedback to 1985, �5 years before the review for the last NHLBI guidelineaddressing lipids in children published in 1992.1 This evidence islargely available in the form of epidemiologic observational studies
EXPERT PANEL ON INTEGRATED GUIDELINES FORCARDIOVASCULAR HEALTH AND RISK REDUCTION INCHILDREN AND ADOLESCENTS
ABBREVIATIONSCVD—cardiovascular diseaseNHLBI—National Heart, Lung, and Blood InstituteRCT—randomized controlled trialPDAY—Pathobiological Determinants of Atherosclerosis inYouthBP—blood pressureHDL—high-density lipoproteinDM—diabetes mellitusCIMT—carotid intima-media thicknessLDL—low-density lipoproteinT1DM—type 1 diabetes mellitusT2DM—type 2 diabetes mellitusTC—total cholesterolAAP—American Academy of PediatricsDGA—Dietary Guidelines for AmericansNCEP—National Cholesterol Education ProgramDASH—Dietary Approaches to Stop HypertensionCHILD—Cardiovascular Health Integrated Lifestyle DieFLP—fasting lipid profileCDC—Centers for Disease Control and PreventionAMA—American Medical AssociationMCHB—Maternal and Child Health BureauFDA—Food and Drug AdministrationAHA—American Heart Association
www.pediatrics.org/cgi/doi/10.1542/peds.2009-2107C
doi:10.1542/peds.2009-2107C
Accepted for publication Sep 8, 2011
Address correspondence to Janet M. de Jesus, MS, RD, 31Center Dr, Building 31, Room 4A17, MSC 2480, Bethesda, MD20892. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2011 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: Dr Daniels has served as a consultantfor Abbott Laboratories, Merck, and Schering-Plough and hasreceived funding/grant support for research from the NationalInstitutes of Health (NIH); Dr Gidding has served as a consultantfor Merck and Schering-Plough and has received funding/grantsupport for research from GlaxoSmithKline; Dr Gillman hasgiven invited talks for Nestle Nutrition Institute and Danone andhas received funding/grant support for research from MeadJohnson, Sanofi-Aventis, and the NIH; Dr Gottesman has servedon the Health Advisory Board, Child Development Council ofFranklin County, was a consultant to Early Head Start for Region5B, has written for iVillage and taught classes through Garrison
(Continued on last page)
SUPPLEMENT ARTICLES
PEDIATRICS Volume 128, Supplement 5, December 2011 S213 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

(rather than RCTs) that, therefore,must be included in the review. In ad-dition, the review required critical ap-praisal of the body of evidence that ad-dresses the impact of managing riskfactors in childhood on the develop-ment and progression of atherosclero-sis. Because of known gaps in the evi-dence base relating risk factors andrisk reduction in childhood to clinicalevents in adult life, the review must in-clude the available evidence that justi-fies evaluation and treatment of riskfactors in childhood. The process ofidentifying, assembling, and organiz-ing the evidence was extensive, the re-view process was complex, and theconclusions could only be developedby interpretation of the body of evi-dence. Even with inclusion of every rel-evant study from the evidence review,there were important areas in whichthe evidence was inadequate. Whenthis occurred, recommendations weremade on the basis of a consensus ofthe expert panel. The schema used ingrading the evidence appears in Ta-bles 1-2 and 1-3; expert consensusopinions are identified as grade D.
The NHLBI expert panel integratedguidelines for cardiovascular healthand risk reduction in children and ad-olescents contain recommendationsbased on the evidence review and aredirected toward all primary pediatriccare providers: pediatricians, familypractitioners, nurses and nurse prac-
titioners, physician assistants, andregistered dietitians. The full reportcontains complete background infor-mation on the state of the science,methodology of the evidence reviewand the guideline-development pro-cess, summaries of the evidence re-views according to risk factor, discus-sion of the expert panel’s rationale forrecommendations, and �1000 cita-tions from the published literature andis available at www.nhlbi.nih.gov/guidelines/cvd_ped/index.htm. Thecomplete evidence tables will be avail-able as a direct link from that site. Thissummary report presents the expertpanel’s recommendations for patientcare relative to cardiovascular healthand risk-factor detection and manage-ment with only the references cited inthe text provided. It beginswith a state-of-the-science synopsis of the evi-dence, which indicates that athero-sclerosis begins in childhood, and theextent of atherosclerosis is linked di-rectly to the presence and intensity ofknown risk factors. This is followed bya cardiovascular health schedule (Sec-tion 3), which summarizes the expertpanel’s age-based recommendationsaccording to risk factor in a 1-page pe-riodic table. Risk factor specific sec-tions follow, with the graded conclu-sions of the evidence review, normativetables, and age-specific recommenda-tions. These recommendations are oftenaccompanied by supportive actions,which represent expert consensus sug-gestions from the panel provided to sup-port implementation of the recommen-
dations. The summary report will bereleased simultaneously with onlineavailability of the full report with refer-ences for each section and the evidencetables at www.nhlbi.nih.gov/guidelines/cvd_ped/index.htm.
It is the hope of the NHLBI and the expertpanel that these recommendationswill beuseful for all thosewhoprovide cardiovas-cular health care to children.
2. STATE OF THE SCIENCE:CARDIOVASCULAR RISK FACTORSAND THE DEVELOPMENT OFATHEROSCLEROSIS IN CHILDHOOD
Atherosclerosis begins in youth, and thisprocess, from its earliest phases, is re-lated to the presence and intensity of theknown cardiovascular risk factorsshown in Table 1-1. Clinical events suchas myocardial infarction, stroke, pe-ripheral arterial disease, and rup-tured aortic aneurysm are the culmi-nation of the lifelong vascular processof atherosclerosis. Pathologically, theprocess begins with the accumulationof abnormal lipids in the vascular in-tima, a reversible stage, progresses toan advanced stage in which a core ofextracellular lipid is covered by a fibro-muscular cap, and culminates inthrombosis, vascular rupture, or acuteischemic syndromes.
Evidence Linking Risk Factors inChildhood to Atherosclerosis atAutopsy
Atherosclerosis at a young age wasfirst identified in Korean and Vietnam
TABLE 1-1 Evaluated Risk Factors
Family historyAgeGenderNutrition/dietPhysical inactivityTobacco exposureBPLipid levelsOverweight/obesityDiabetes mellitusPredisposing conditionsMetabolic syndromeInflammatory markersPerinatal factors
TABLE 1-2 Evidence Grading System: Quality Grades
Grade Evidence
A Well-designed RCTs or diagnostic studies performed on a population similar to the guideline’starget population
B RCTs or diagnostic studies with minor limitations; genetic natural history studies;overwhelmingly consistent evidence from observational studies
C Observational studies (case-control and cohort design)D Expert opinion, case reports, or reasoning from first principles (bench research or animal
studies)
Adapted from American Academy of Pediatrics, Steering Committee on Quality Improvement and Management. Pediatrics.2004;114(3):874–877.
S214 EXPERT PANEL by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

War casualties. Two major contempo-rary studies, the Pathobiological De-terminants of Atherosclerosis in Youth(PDAY) study2 and the Bogalusa HeartStudy,3 subsequently evaluated the ex-tent of atherosclerosis in children, ad-olescents, and young adults who diedaccidentally. The Bogalusa study3 mea-sured cardiovascular risk factors(lipid levels, blood pressure [BP], BMI,and tobacco use) as part of a compre-hensive school-based epidemiologicstudy in a biracial community. Theseresults were related to atherosclero-sis measured at autopsy after acciden-tal death. Strong correlations wereshown between the presence and in-tensity of risk factors and the extentand severity of atherosclerosis. In thePDAY study,2 risk factors and surro-gate measures of risk factors weremeasured after death in 15- to 34-yearolds who died accidentally of externalcauses. Strong relationships werefound between atherosclerotic sever-ity and extent, and age, non–high-density lipoprotein (HDL) choles-terol, HDL cholesterol, hypertension
(determined by renal artery thick-ness), tobacco use (thiocyanate con-centration), diabetes mellitus (DM)(glycohemoglobin), and (in men) obe-sity. There was a striking increase inboth severity and extent as age and thenumber of risk factors increased. Bycontrast, the absence of risk factorswas shown to be associated with a vir-tual absence of advanced atheroscle-rotic lesions, even in the oldest sub-jects in the study.
Evidence Linking Risk Factors inChildhood to AtherosclerosisAssessed Noninvasively
Over the last decade, measures of sub-clinical atherosclerosis have devel-oped, including the demonstration ofcoronary calcium on electron beamcomputed tomography imaging, in-creased carotid intima-media thick-ness (CIMT) assessed with ultrasound,endothelial dysfunction (reduced arte-rial dilation) with brachial ultrasoundimaging, and increased left ventricularmass with cardiac ultrasound. Thesemeasures have been assessed in
young people with severe abnormali-ties of individual risk factors:
● In adolescents with a marked eleva-tion of low-density lipoprotein (LDL)cholesterol level caused by familialheterozygous hypercholesterolemia,abnormal levels of coronary calcium,increased CIMT, and impaired endo-thelial function have been found.
● Children with hypertension havebeen shown to have increased CIMT,increased left ventricularmass, andeccentric left ventricular geometry.
● Childrenwith type 1 DM (T1DM) havesignificantly abnormal endothelialfunction and, in some studies, in-creased CIMT.
● Children and young adults with afamily history of myocardial infarc-tion have increased CIMT, higherprevalence of coronary calcium,and endothelial dysfunction.
● Endothelial dysfunction has beenshown by ultrasound and plethys-mography in association with ciga-rette smoking (passive and active)
TABLE 1-3 Evidence Grading System: Strength of Recommendations
Statement Type Definition Implication
Strong recommendation The expert panel believes that the benefits of the recommended approachclearly exceed the harms and that the quality of the supportingevidence is excellent (grade A or B). In some clearly definedcircumstances, strong recommendations may be made on the basis oflesser evidence when high-quality evidence is impossible to obtain andthe anticipated benefits clearly outweigh the harms.
Clinicians should follow a strong recommendationunless a clear and compelling rationale for analternative approach is present.
Recommendation The expert panel feels that the benefits exceed the harms but that thequality of the evidence is not as strong (grade B or C). In some clearlydefined circumstances, recommendations may be made on the basis oflesser evidence when high-quality evidence is impossible to obtain andwhen the anticipated benefits clearly outweigh the harms.
Clinicians should generally follow arecommendation but remain alert to newinformation and sensitive to patientpreferences.
Optional Either the quality of the evidence that exists is suspect (grade D) or well-performed studies (grade A, B, or C) have found little clear advantageto one approach versus another.
Clinicians should be flexible in their decision-making regarding appropriate practice,although they may set boundaries onalternatives; patient and family preferenceshould have a substantial influencing role.
No recommendation There is both a lack of pertinent evidence (grade D) and an unclearbalance between benefits and harms.
Clinicians should not be constrained in theirdecision-making and be alert to new publishedevidence that clarifies the balance of benefitversus harm; patient and family preferenceshould have a substantial influencing role.
Adapted from American Academy of Pediatrics, Steering Committee on Quality Improvement and Management. Pediatrics. 2004;114(3):874–877.
SUPPLEMENT ARTICLES
PEDIATRICS Volume 128, Supplement 5, December 2011 S215 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

and obesity. In obese children, im-provement in endothelial functionoccurs with regular exercise.
● Left ventricular hypertrophy at lev-els associated with excessmortalityin adults has been found in childrenwith severe obesity.
Four longitudinal studies have found re-lationships of risk factors measured inyouth (specifically LDL cholesterol, non-HDL cholesterol and serum apolipopro-teins, obesity, hypertension, tobaccouse, and DM) with measures of subclini-cal atherosclerosis in adulthood. Inmany of these studies, risk factors mea-sured in childhood and adolescencewere better predictors of the severity ofadult atherosclerosis thanwere risk fac-torsmeasured at the time of the subclin-ical atherosclerosis study.
Evidence Linking Risk Factors inChildhood to Clinical CVD
The most important evidence relatingrisk in youth to clinical CVD is the ob-served association of risk factors foratherosclerosis to clinically manifestcardiovascular conditions. Genetic dis-orders related to high cholesterol arethe biological model for risk-factor im-pact on the atherosclerotic process.With homozygous hypercholesterol-emia, in which LDL cholesterol levelsexceed 800mg/dL beginning in infancy,coronary events begin in the first de-cade of life and life span is severelyshortened. With heterozygous hyper-cholesterolemia, in which LDL choles-terol levels are minimally 160 mg/dLand typically �200 mg/dL and totalcholesterol (TC) levels exceed 250mg/dL beginning in infancy, 50% ofmen and 25% of women experienceclinical coronary events by the age of50. By contrast, genetic traits associ-ated with low cholesterol are associ-ated with longer life expectancy. In thePDAY study,2 every 30 mg/dL increasein non-HDL cholesterol level was asso-ciated with a visible incremental in-
crease in the extent and severity ofatherosclerosis. In natural-historystudies of DM, early CVDmortality is soconsistently observed that the pres-ence of DM is considered evidence ofvascular disease in adults. Consonantwith this evidence, in 15- to 19-yearolds in the PDAY study, the presence ofhyperglycemia was associated withthe demonstration of advanced ath-erosclerotic lesions of the coronaryarteries. In the PDAY study, there wasalso a strong relationship between ab-dominal aortic atherosclerosis and to-bacco use. Finally, in a 25-year follow-up, the presence of the metabolicsyndrome risk-factor cluster in child-hood predicted clinical CVD in adultsubjects at 30 to 48 years of age.4
The Impact of Racial/EthnicBackground and SocioeconomicStatus in Childhood on theDevelopment of Atherosclerosis
CVD has been observed in diverse geo-graphic areas and all racial and ethnicbackgrounds. Cross-sectional re-search in children has found differ-ences according to race and ethnicityand according to geography for preva-lence of cardiovascular risk factors;these differences are often partiallyexplained by differences in socioeco-nomic status. No group within theUnited States is without a significantprevalence of risk. Several longitudi-nal cohort studies referenced exten-sively in this report (Bogalusa HeartStudy,3 the PDAY study,2 and the Coro-nary Artery Risk Development in YoungAdults [CARDIA] study5) have includedracially diverse populations, and otherstudies have been conducted outsidethe United States. However, longitudi-nal data on Hispanic, Native American,and Asian children are lacking. Clini-cally important differences in preva-lence of risk factors exist according torace and gender, particularly with re-gard to tobacco-use rates, obesityprevalence, hypertension, and dyslipi-
demia. Low socioeconomic status inand of itself confers substantial risk.However, evidence is not adequate forthe recommendations provided in thisreport to be specific to racial or ethnicgroups or socioeconomic status.
The Impact of Risk-FactorClustering in Childhood on theDevelopment of Atherosclerosis
From a population standpoint, cluster-ing of multiple risk factors is the mostcommon association with prematureatherosclerosis. The pathologic stud-ies reviewed above clearly showedthat the presence of multiple risk fac-tors is associated with striking evi-dence of an accelerated atheroscle-rotic process. Among the mostprevalent multiple-risk combinationsare the use of tobacco with 1 other riskfactor and the development of obesity,which is often associated with insulinresistance, elevated triglyceride lev-els, reduced HDL cholesterol levels,and elevated BP, a combination knownin adults as the metabolic syndrome.There is ample evidence from bothcross-sectional and longitudinal stud-ies that the increasing prevalence ofobesity in childhood is associated withthe same obesity-related risk-factorclustering seen in adults and that itcontinues into adult life. This high-riskcombination is among the reasonsthat the current obesity epidemic withits relationship to future CVD and DM isconsidered one of the most importantpublic health challenges in contempo-rary society. One other prevalentmultiple-risk combination is the asso-ciation of low cardiorespiratory fit-ness (identified in 33.6% of adoles-cents in the National Health andNutrition Examination Surveys [NHANES]from 1999 to 20026) with overweightand obesity, elevated TC level and sys-tolic BP, and a reduced HDL cholesterollevel.
S216 EXPERT PANEL by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
Risk-Factor Tracking FromChildhood Into Adult Life
Tracking studies from childhood toadulthood have been performed for allthe major risk factors.
● Obesity tracks more strongly thanany other risk factor; among manyreports from studies that have dem-onstrated this fact, one of the mostrecent is from the Bogalusa study,7
in which �2000 children were fol-lowed from initial evaluation at 5 to14 years of age to adult follow-up ata mean age of 27 years. On the basisof BMI percentiles derived from thestudy population, 84% of those witha BMI in the 95th to 99th percentileas children were obese as adults,and all of those with a BMI at the�99th percentile were obese inadulthood. Increased correlation isseen with increasing age at whichthe elevated BMI occurs.
● For cholesterol and BP, trackingcorrelation coefficients in the rangeof 0.4 have been reported consis-tently from many studies, correlat-ing these measures in children 5 to10 years of age with results 20 to 30years later. These data suggest thathaving cholesterol or BP levels inthe upper portion of the pediatricdistribution makes having them asadult risk factors likely but not cer-tain. Those who develop obesityhave been shown to be more likelyto develop hypertension or dyslipi-demia as adults.
● Tracking data on physical fitnessare more limited. Physical activitylevels do track but not as stronglyas other risk factors.
● By its addictive nature, tobacco usepersists into adulthood, although�50% of those who have eversmoked eventually quit.
● T1DM is a lifelong condition.
● The insulin resistance of T2DM can bealleviated by exercise, weight loss, and
bariatricsurgery,but the long-termout-come of those with T2DM diagnosed inchildhood is not known.
● As already discussed, risk-factorclusters such as those seen withobesity and themetabolic syndromehave been shown to track fromchildhood into adulthood.
CVD Prevention Beginning in Youth
The rationale for these guidelinescomes from the following evidence.
● Atherosclerosis, the pathologic ba-sis for clinical CVD, originates inchildhood.
● Risk factors for the development ofatherosclerosis can be identified inchildhood.
● Development and progression ofatherosclerosis clearly relates tothe number and intensity of cardio-vascular risk factors, which begin inchildhood.
● Risk factors track from childhoodinto adult life.
● Interventions exist for the manage-ment of identified risk factors.
The evidence for the first 4 bulletpoints is reviewed in this section, andthe evidence surrounding interven-tions for identified risk factors is ad-dressed in the risk-factor–specificsections of the guideline to follow.
It is important to distinguish betweenthe goals of prevention at a young ageand those at older ages in which ath-erosclerosis is well established, mor-bidity may already exist, and the pro-cess is only minimally reversible. At ayoung age, there have historically been2 goals of prevention: (1) prevent thedevelopment of risk factors (primor-dial prevention); and (2) recognize andmanage those children and adoles-cents who are at increased risk as aresult of the presence of identified riskfactors (primary prevention). It is wellestablished that a population that en-ters adulthood with lower risk will
have less atherosclerosis and will col-lectively have lower CVD rates. Thisconcept is supported by research thathas found that (1) societies with lowlevels of cardiovascular risk factorshave low CVD rates and that changesin risk in those societies are associ-ated with a change in CVD rates, (2)in adults, control of risk factorsleads to a decline in morbidity andmortality from CVD, and (3) thosewithout childhood risk have minimalatherosclerosis at 30 to 34 years ofage, absence of subclinical athero-sclerosis as young adults, extendedlife expectancy, and a better qualityof life free from CVD.
The Pathway to RecommendingClinical Practice-Based Prevention
The most direct means of establishingevidence for active CVD prevention be-ginning at a young age would be to ran-domly assign young people withdefined risks to treatment of cardio-vascular risk factors or to no treat-ment and follow both groups oversufficient time to determine if cardio-vascular events are prevented withoutundue increase in morbidity arisingfrom treatment. This direct approachis intellectually attractive, becauseatherosclerosis prevention would be-gin at the earliest stage of the diseaseprocess and thereby maximize thebenefit. However, this approach is asunachievable as it is attractive, pri-marily because such studies would beextremely expensive and would be sev-eral decades in duration, a time periodin which changes in environment andmedical practice would diminish therelevance of the results.
The recognition that evidence fromthis direct pathway is unlikely to beachieved requires an alternative step-wise approach in which segments ofan evidence chain are linked in a man-ner that serves as a sufficiently rigor-ous proxy for the causal inference of a
SUPPLEMENT ARTICLES
PEDIATRICS Volume 128, Supplement 5, December 2011 S217 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

clinical trial. The evidence reviewed inthis section provides the critical ratio-nale for cardiovascular prevention be-ginning in childhood: atherosclerosisbegins in youth; the atheroscleroticprocess relates to risk factors that canbe identified in childhood; and thepresence of these risk factors in agiven child predicts an adult with riskif no intervention occurs. The remain-ing evidence links pertain to the dem-onstration that interventions to lowerrisk will have a health benefit and thatthe risk and cost of interventions toimprove risk are outweighed by the re-duction in CVD morbidity and mortal-ity. These issues are captured in theevidence reviews of each risk factor.The recommendations reflect a com-plex decision process that integratesthe strength of the evidence withknowledge of the natural history ofatherosclerotic vascular disease, esti-mates of intervention risk, and the phy-sician’s responsibility to provide bothhealth education and effective diseasetreatment. These recommendationsfor those caring for children will bemost effective when complemented bya broader public health strategy.
The Childhood Medical Office Visitas the Setting for CardiovascularHealth Management
One cornerstone of pediatric care isplacing clinical recommendations in adevelopmental context. Those whomake pediatric recommendationsmust consider not only the relation ofage to disease expression but the abil-ity of the patient and family to under-stand and implement medical advice.For each risk factor, recommenda-tionsmust be specific to age and devel-opmental stage. The Bright Futuresconcept of the American Academy ofPediatrics8 (AAP) is used to provide aframework for these guidelines withcardiovascular risk-reduction recom-mendations for each age group.
This document provides recommenda-tions for preventing the developmentof risk factors and optimizing cardio-vascular health, beginning in infancy,that are based on the results of theevidence review. Pediatric care provid-ers (pediatricians, family practitio-ners, nurses, nurse practitioners,physician assistants, registered dieti-tians) are ideally positioned to rein-force cardiovascular health behaviorsas part of routine care. The guidelinealso offers specific guidance on pri-mary prevention with age-specific,evidence-based recommendations forindividual risk-factor detection. Man-agement algorithms provide stagedcare recommendations for risk reduc-tion within the pediatric care settingand identify risk-factor levels that re-quire specialist referral. The guide-lines also identify specificmedical con-ditions such as DM and chronic kidneydisease that are associated with in-creased risk for accelerated athero-sclerosis. Recommendations forongoing cardiovascular health man-agement for children and adolescentswith these diagnoses are provided.
A cornerstone of pediatric care is theprovision of health education. In the UShealth care system, physicians andnurses are perceived as credible mes-sengers for health information. Thechildhood health maintenance visitprovides an ideal context for effectivedelivery of the cardiovascular healthmessage. Pediatric care providersprovide an effective team educated toinitiate behavior change to diminishrisk of CVD and promote lifelong car-diovascular health in their patientsfrom infancy into young adult life.
3. CARDIOVASCULAR HEALTHSCHEDULE (p. S219)
4. FAMILY HISTORY OF EARLYATHEROSCLEROTIC CVD
A family history of CVD represents thenet effect of shared genetic, biochemi-
cal, behavioral, and environmentalcomponents. In adults, epidemiologicstudies have found that a family his-tory of premature coronary heart dis-ease in a first-degree relative (heartattack, treated angina, percutaneouscoronary catheter interventional pro-cedure, coronary artery bypass sur-gery, stroke, or sudden cardiac deathin a male parent or sibling before theage of 55 years or a female parent orsibling before the age of 65 years) is animportant independent risk factor forfuture CVD. The process of atheroscle-rosis is complex and involves many ge-netic loci and multiple environmentaland personal risk factors. Nonethe-less, the presence of a positive paren-tal history has been consistently foundto significantly increase baseline riskfor CVD. The risk for CVD in offspring isstrongly inversely related to the age ofthe parent at the time of the indexevent. The association of a positivefamily history with increased cardio-vascular risk has been confirmed formen, women, and siblings and in dif-ferent racial and ethnic groups. The ev-idence review identified all RCTs, sys-tematic reviews, meta-analyses, andobservational studies that addressedfamily history of premature athero-sclerotic disease and the developmentand progression of atherosclerosisfrom childhood into young adult life.
Conclusions and Grading of theEvidence Review for the Role ofFamily History in CardiovascularHealth
● Evidence from observational stud-ies strongly supports inclusion of apositive family history of early coro-nary heart disease in identifyingchildren at risk for accelerated ath-erosclerosis and for the presence ofan abnormal risk profile (grade B).
● For adults, a positive family historyis defined as a parent and/or siblingwith a history of treated angina,
S218 EXPERT PANEL by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

3.INTEGRATEDCARDIOVASCULARHEALTHSCHEDULE
RiskFactor
Age
Birthto12mo
1–4y
5–9y
9–11y
12–17y
18–21y
Familyhistoryof
earlyCVD
—At3y,evaluatefamilyhistoryfor
earlyCVD:parents,grand-
parents,aunts/uncles,men
�55yold,women
�65yold;
reviewwithparentsandrefer
asneeded;positivefamily
historyidentifieschildrenfor
intensiveCVDRFattention
Updateateachnonurgenthealth
encounter
Reevaluatefamilyhistoryforearly
CVDinparents,grandparents,
aunts/uncles,men
�55yold,
women
�65yold
Updateateachnonurgenthealth
encounter
Repeatfamily-historyevaluationwith
patient
Tobacco
exposure
Advisesmoke-freehome;
offersmoking-cessation
assistanceorreferral
toparents
Continueactiveantismoking
advicewithparents;offer
smoking-cessationassistance
andreferralasneeded
Obtainsmokeexposurehistory
fromchildBeginactive
antismokingadvicewithchild
Assesssmokingstatusofchild;
activeantismokingcounseling
orreferralasneeded
Continueactiveantismoking
counselingwithpatient;offer
smoking-cessationassistanceor
referralasneeded
Reinforcestrongantismokingmessage;
offersmoking-cessationassistanceor
referralasneeded
Nutrition/dietSupportbreastfeedingas
optimalto12moofage
ifpossible;addformula
ifbreastfeeding
decreasesorstops
before12moofage
Atage12–24mo,maychangeto
cow’smilkwith2%
percentageoffatdecidedby
familyandpediatriccare
provider;after2yofage,
fat-freemilkforall;juice
�4
oz/d;transitiontoCHILD-1
dietbytheageof2y
ReinforceCHILD-1dietmessages
ReinforceCHILD-1dietmessages
asneeded
Obtaindietinformationfromchild
andusetoreinforcehealthydiet
andlimitationsandprovide
counselingasneeded
Reviewhealthydietwithpatient
Growth,
overweight/
obesity
Reviewfamilyhistoryfor
obesity;discussweight-
for-heighttracking,
growthchart,and
healthydiet
Chartheight/weight/BMI;
classifyweight-byBMIfrom
age2y;reviewwithparent
Chartheight/weight/BMIand
reviewwithparent;BMI�
85thpercentile,crossing
percentiles:Intensifydiet/
activityfocusfor6mo;ifno
change:RDreferral,manage
perobesityalgorithms
Chartheight/weight/BMIand
reviewwithparentandchild;
BMI�85thpercentile,
crossingpercentiles:Intensify
diet/activityfocusfor6mo;if
nochange:RDreferral,
manageperobesity
algorithms;BMI�95th
percentile:manageperobesity
algorithms
Chartheight/weight/BMIandreview
withchildandparent;BMI�85th
percentile,crossingpercentiles:
intensifydiet/activityfocusfor6
mo;ifnochange:RDreferral,
manageperobesityalgorithms;
BMI�95thpercentile,manage
perobesityalgorithms
Reviewheight/weight/BMIandnormsfor
healthwithpatient;BMI�85th
percentile,crossingpercentiles:
intensifydiet/activityfocusfor6mo;
ifnochange:RDreferral,manageper
obesityalgorithms;BMI�95th
percentile,manageperobesity
algorithms
BMI�95thpercentile,manage
perobesityalgorithms
Lipids
Noroutinelipidscreening
ObtainFLPonlyiffamilyhistory
forCVDispositive,parenthas
dyslipidemia,childhasany
otherRFsorhigh-risk
condition
ObtainFLPonlyiffamilyhistory
forCVDispositive,parent
hasdyslipidemia,childhas
anyotherRFsorhigh-risk
condition
Obtainuniversallipidscreenwith
nonfastingnon-HDL
�TC
�HDL,orFLP:manageperlipid
algorithmsasneeded
ObtainFLPiffamilyhistorynewly
positive,parenthas
dyslipidemia,childhasanyother
RFsorhigh-riskcondition;
manageperlipidalgorithmsas
needed
Measure1nonfastingnon–HDLorFLPin
all:reviewwithpatient;managewith
lipidalgorithmsperATPasneeded
BPMeasureBPininfantswith
renal/urologic/cardiac
diagnosisorhistoryof
neonatalICU
MeasureBPannuallyinallfrom
theageof3y;chartforage/
gender/heightpercentileand
reviewwithparent
CheckBPannuallyandchartfor
age/gender/height:review
withparent;workupand/or
managementperBP
algorithmasneeded
CheckBPannuallyandchartfor
age/gender/height:reviewwith
parent,workupand/or
managementperBPalgorithm
asneeded
CheckBPannuallyandchartfor
age/gender/height:reviewwith
adolescentandparent,workup
and/ormanagementperBP
algorithmasneeded
MeasureBP:reviewwithpatient;
evaluateandtreatperJNCguidelines
Physical
activity
Encourageparentsto
modelroutineactivity;
noscreentimebefore
theageof2y
Encourageactiveplay;limit
sedentary/screentimeto
�2
h/d;noTVinbedroom
RecommendMVPAof
�1h/d;
limitscreen/sedentarytime
to�2h/d
Obtainactivityhistoryfromchild:
recommendMVPAof
�1h/d
andscreen/sedentarytimeof
�2h/d
Useactivityhistorywithadolescent
toreinforceMVPAof
�1h/dand
leisurescreentimeof
�2h/d
Discusslifelongactivity,sedentarytime
limitswithpatient
Diabetes
——
—Measurefastingglucoselevelper
ADAguidelines;referto
endocrinologistasneeded
Measurefastingglucoselevelper
ADAguidelines;referto
endocrinologistasneeded
Obtainfastingglucoselevelifindicated;
refertoendocrinologistasneeded
Allalgorithmsandguidelinesinthisscheduleareincludedinthissummaryreport.RFindicatesriskfactor;RD,registereddietitian;ATP,AdultTreatmentPanelIII(“ThirdReportoftheExpertPanelonDetection,Evaluation,andTreatmentofHighBlood
CholesterolinAdults”);JNC,JointNationalCommitteeonPrevention,Detection,Evaluation,andTreatmentofHighBloodPressure;MVPA,moderate-to-vigorousphysicalactivity;ADA,AmericanDiabetesAssociation.
ThefullandsummaryreportsoftheExpertPanelonIntegratedGuidelinesforCardiovascularHealthandRiskReductioninChildrenandAdolescentscanalsobefoundontheNHLBIWebsite(www.nhlbi.nih.gov).
SUPPLEMENT ARTICLES
PEDIATRICS Volume 128, Supplement 5, December 2011 S219 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
myocardial infarction, percutane-ous coronary catheter interven-tional procedure, coronary arterybypass grafting, stroke, or suddencardiac death before 55 years inmen or 65 years in women. Becausethe parents and siblings of childrenand adolescents are usually youngthemselves, it was the panel con-sensus that when evaluating familyhistory of a child, history shouldalso be ascertained for the occur-rence of CVD in grandparents,aunts, and uncles, although the evi-dence supporting this recommen-dation is insufficient to date (gradeD).
● Identification of a positive familyhistory for cardiovascular diseaseand/or cardiovascular risk fac-tors should lead to evaluation ofall family members, especiallyparents, for cardiovascular riskfactors (grade B).
● Family history evolves as a child ma-tures, so regular updates are a nec-essary part of routine pediatriccare (grade D).
● Education about the importance ofaccurate and complete familyhealth information should be part ofroutine care for children and ado-lescents. As genetic sophisticationincreases, linking family history tospecific genetic abnormalities willprovide important new knowledgeabout the atherosclerotic process(grade D).
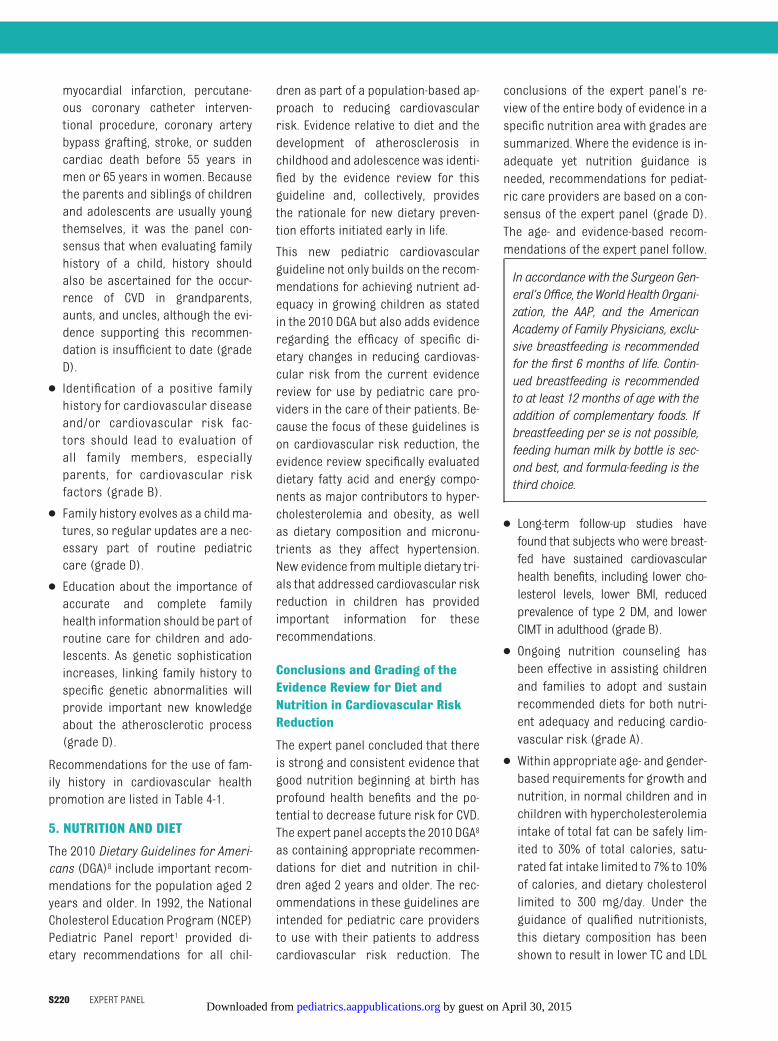
Recommendations for the use of fam-ily history in cardiovascular healthpromotion are listed in Table 4-1.
5. NUTRITION AND DIET
The 2010 Dietary Guidelines for Ameri-cans (DGA)8 include important recom-mendations for the population aged 2years and older. In 1992, the NationalCholesterol Education Program (NCEP)Pediatric Panel report1 provided di-etary recommendations for all chil-
dren as part of a population-based ap-proach to reducing cardiovascularrisk. Evidence relative to diet and thedevelopment of atherosclerosis inchildhood and adolescence was identi-fied by the evidence review for thisguideline and, collectively, providesthe rationale for new dietary preven-tion efforts initiated early in life.
This new pediatric cardiovascularguideline not only builds on the recom-mendations for achieving nutrient ad-equacy in growing children as statedin the 2010 DGA but also adds evidenceregarding the efficacy of specific di-etary changes in reducing cardiovas-cular risk from the current evidencereview for use by pediatric care pro-viders in the care of their patients. Be-cause the focus of these guidelines ison cardiovascular risk reduction, theevidence review specifically evaluateddietary fatty acid and energy compo-nents as major contributors to hyper-cholesterolemia and obesity, as wellas dietary composition and micronu-trients as they affect hypertension.New evidence frommultiple dietary tri-als that addressed cardiovascular riskreduction in children has providedimportant information for theserecommendations.
Conclusions and Grading of theEvidence Review for Diet andNutrition in Cardiovascular RiskReduction
The expert panel concluded that thereis strong and consistent evidence thatgood nutrition beginning at birth hasprofound health benefits and the po-tential to decrease future risk for CVD.The expert panel accepts the 2010 DGA8
as containing appropriate recommen-dations for diet and nutrition in chil-dren aged 2 years and older. The rec-ommendations in these guidelines areintended for pediatric care providersto use with their patients to addresscardiovascular risk reduction. The
conclusions of the expert panel’s re-view of the entire body of evidence in aspecific nutrition area with grades aresummarized. Where the evidence is in-adequate yet nutrition guidance isneeded, recommendations for pediat-ric care providers are based on a con-sensus of the expert panel (grade D).The age- and evidence-based recom-mendations of the expert panel follow.
In accordancewith the Surgeon Gen-eral’s Office, theWorldHealth Organi-zation, the AAP, and the AmericanAcademy of Family Physicians, exclu-sive breastfeeding is recommendedfor the first 6 months of life. Contin-ued breastfeeding is recommendedto at least 12 months of age with theaddition of complementary foods. Ifbreastfeeding per se is not possible,feeding human milk by bottle is sec-ond best, and formula-feeding is thethird choice.
● Long-term follow-up studies havefound that subjects who were breast-fed have sustained cardiovascularhealth benefits, including lower cho-lesterol levels, lower BMI, reducedprevalence of type 2 DM, and lowerCIMT in adulthood (grade B).
● Ongoing nutrition counseling hasbeen effective in assisting childrenand families to adopt and sustainrecommended diets for both nutri-ent adequacy and reducing cardio-vascular risk (grade A).
● Within appropriate age- and gender-based requirements for growth andnutrition, in normal children and inchildren with hypercholesterolemiaintake of total fat can be safely lim-ited to 30% of total calories, satu-rated fat intake limited to 7% to 10%of calories, and dietary cholesterollimited to 300 mg/day. Under theguidance of qualified nutritionists,this dietary composition has beenshown to result in lower TC and LDL
S220 EXPERT PANEL by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

cholesterol levels, less obesity, andless insulin resistance (grade A).Under similar conditions and withongoing follow-up, these levels of fatintake might have similar effectsstarting in infancy (grade B). Fatsare important to infant diets be-cause of their role in brain and cog-nitive development. Fat intake for in-fants younger than 12 monthsshould not be restricted withoutmedical indication.
● The remaining 20% of fat intakeshould comprise a combination ofmonosaturated and polyunsatu-rated fats (grade D). Intake of transfats should be limited as much aspossible (grade D).
● For adults, the current NCEP guide-lines9 recommend that adults con-sume 25% to 35% of calories fromfat. The 2010 DGA supports the Insti-tute of Medicine recommendationsfor 30% to 40% of calories from fatfor ages 1 to 3 years, 25% to 35% ofcalories from fat for ages 4 to 18years, and 20% to 35% of caloriesfrom fat for adults. For growing chil-dren, milk provides essential nutri-ents, including protein, calcium,magnesium, and vitamin D, that arenot readily available elsewhere inthe diet. Consumption of fat-freemilk in childhood after 2 years ofage and through adolescence opti-mizes these benefits without com-promising nutrient quality whileavoiding excess saturated fat andcalorie intake (grade A). Betweenthe ages of 1 and 2 years, as chil-dren transition from breast milk orformula, reduced-fat milk (rangingfrom 2%milk to fat-freemilk) can beused on the basis of the child’sgrowth, appetite, intake of othernutrient-dense foods, intake ofother sources of fat, and risk forobesity and CVD. Milk with reducedfat should be used only in the con-text of an overall diet that supplies
30% of calories from fat. Dietary in-tervention should be tailored toeach specific child’s needs.
● Optimal intakes of total protein andtotal carbohydrate in children werenot specifically addressed, but witha recommended total fat intake of30% of energy, the expert panel rec-ommends that the remaining 70% ofcalories include 15% to 20% fromprotein and 50% to 55% from carbo-hydrate sources (no grade). Theserecommended ranges fall withinthe acceptable macronutrient dis-tribution range specified by the2010 DGA: 10% to 30% of caloriesfrom protein and 45% to 65% of cal-ories from carbohydrate for chil-dren aged 4 to 18 years.
● Sodium intake was not addressed bytheevidencereview for this sectiononnutrition and diet. From the evidencereview for the “High BP” section,lower sodium intake is associatedwith lower systolic and diastolic BP ininfants, children, and adolescents.
● Plant-based foods are important low-calorie sources of nutrients includingvitamins and fiber in the diets of chil-dren; increasing access to fruits andvegetables has been shown to in-crease their intake (grade A). How-ever, increasing fruit and vegetableintake is an ongoing challenge.
● Reduced intake of sugar-sweetenedbeverages is associated with de-creased obesity measures (grade B).Specific information about fruit juiceintake is too limited for an evidence-based recommendation. Recommen-dations for intake of 100% fruit juiceby infants was made by a consensusof the expert panel (grade D) and arein agreement with those of the AAP.
● Per the 2010 DGA, energy intakeshould not exceed energy neededfor adequate growth and physicalactivity. Calorie intake needs tomatch growth demands and physi-
cal activity needs (grade A). Esti-mated calorie requirements ac-cording to gender and age group at3 levels of physical activity from thedietary guidelines are shown in Ta-ble 5-2. For children of normalweight whose activity is minimal,most calories are needed to meet nu-tritional requirements, which leavesonly �5% to 15% of calorie intakefrom extra calories. These caloriescan be derived from fat or sugaradded to nutrient-dense foods to al-low their consumptionassweets, des-serts, or snack foods (grade D).
● Dietary fiber intake is inversely as-sociated with energy density and in-creased levels of body fat and is pos-itively associated with nutrientdensity (grade B); a daily total di-etary fiber intake from food sourcesof at least age plus 5 g for youngchildren up to 14 g/1000 kcal forolder children and adolescents isrecommended (grade D).
● The expert panel supports the 2008AAP recommendation for vitamin Dsupplementationwith 400 IU/day forall infants and children.10 No othervitamin, mineral, or dietary supple-ments are recommended (grade D).The new recommended daily allow-ance for vitamin D for those aged 1to 70 years is 600 IU/day.
● Use of dietary patterns modeled onthose shown to be beneficial foradults (eg, Dietary Approaches toStop Hypertension [DASH] pattern)is a promising approach to improv-ing nutrition and decreasing cardio-vascular risk (grade B).
● All diet recommendations must beinterpreted for each child and fam-ily to address individual diet pat-terns and patient sensitivities suchas lactose intolerance and food al-lergies (grade D).
Graded, age-specific recommenda-tions for pediatric care providers to
SUPPLEMENT ARTICLES
PEDIATRICS Volume 128, Supplement 5, December 2011 S221 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
use in optimizing cardiovascularhealth in their patients are summa-rized in Table 5-1. The CardiovascularHealth Integrated Lifestyle Diet(CHILD-1) is the first stage in dietarychange for childrenwith identified dys-lipidemia, overweight and obesity,risk-factor clustering, and high-riskmedical conditions that might ulti-mately require more intensive dietarychange. CHILD-1 is also the recom-mended diet for children with a posi-tive family history of early cardiovas-cular disease, dyslipidemia, obesity,primary hypertension, DM, or expo-sure to smoking in the home. Any di-etary modification must provide nutri-ents and calories needed for optimalgrowth and development (Table 5-2).Recommended intakes are adequatelymet by a DASH-style eating plan, whichemphasizes fat-free/low-fat dairy andincreased intake of fruits and vegeta-bles. This diet has been modified foruse in children aged 4 years and older
on the basis of daily energy needs ac-cording to food group and is shown inTable 5-3 as an example of a heart-healthy eating plan using CHILD-1recommendations.
6. PHYSICAL ACTIVITY
Physical activity is any bodily move-ment produced by contraction of skel-etal muscle that increases energy ex-penditure above a basal level. Physicalactivity can be focused on strengthen-ing muscles, bones, and joints, but be-cause these guidelines address car-diovascular health, the evidencereview concentrated on aerobic activ-ity and on the opposite of activity: sed-entary behavior. There is strong evi-dence for beneficial effects of physicalactivity and disadvantageous effects ofa sedentary lifestyle on the overallhealth of children and adolescentsacross a broad array of domains. Ourreview focused on the effects of activ-ity on cardiovascular health, because
physical inactivity has been identifiedas an independent risk factor for cor-onary heart disease in adults. Over thelast several decades, there has been asteady decrease in the amount of timethat children spend being physicallyactive and an accompanying increasein time spent in sedentary activities. Theevidence review identified many studiesin youthranging inage from4 to21yearsthat strongly linked increased timespent in sedentary activities with re-duced overall activity levels, disadvanta-geous lipid profiles, higher systolic BP,higher levels of obesity, andhigher levelsof all the obesity-related cardiovascularrisk factors including hypertension, in-sulin resistance, and type 2 DM.
Conclusions and Grading of theEvidence Review for PhysicalActivity
The expert panel felt that the evidencestrongly supports the role of physicalactivity in optimizing cardiovascularhealth in children and adolescents.
● There is reasonably good evidencethat physical activity patterns estab-lished in childhood are carried for-ward into adulthood (grade C).
● There is strong evidence that in-creases in moderate-to-vigorousphysical activity are associated withlower systolic and diastolic BP, de-creased measures of body fat, de-creased BMI, improved fitness mea-sures, lower TC level, lower LDLcholesterol level, lower triglyceridelevel, higher HDL cholesterol level,and decreased insulin resistance inchildhood and adolescence (gradeA).
● There is limited but strong and con-sistent evidence that physical exer-cise interventions improve subclini-cal measures of atherosclerosis(grade B).
● Physical activity patterns, dietarychoices, and smoking behaviorscluster together (grade C).
TABLE 4-1 Evidence-Based Recommendations for Use of Family History in CardiovascularHealth Promotion
Birth to 18 y Take detailed family history of CVD at initial encounter and/or at 3,9–11, and 18 ya
Grade BRecommend
If positive family history identified, evaluate patient for othercardiovascular risk factors, including dyslipidemia, hypertension,DM, obesity, history of smoking, and sedentary lifestyle
If positive family history and/or cardiovascular risk factors identified,evaluate family, especially parents, for cardiovascular risk factors
Grade BRecommend
Update family history at each nonurgent health encounter Grade DRecommend
Use family history to stratify risk for CVD risk as risk profile evolves Grade DRecommend
Supportive action: educate parents about the importance of familyhistory in estimating future health risks for all family members
18 to 21 y Review family history of heart disease with young adult patient Grade BStrongly recommend
Supportive action: educate patient about family/personal risk forearly heart disease, including the need for evaluation for allcardiovascular risk factors
Grades reflect the findings of the evidence review; recommendation levels reflect the consensus opinion of the expertpanel; and supportive actions represent expert consensus suggestions from the expert panel provided to supportimplementation of the recommendations (they are not graded).a “Family” includes parent, grandparent, aunt, uncle, or sibling with heart attack, treated angina, coronary artery bypassgraft/stent/angioplasty, stroke, or sudden cardiac death at�55 y in males and�65 y in females.
S222 EXPERT PANEL by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
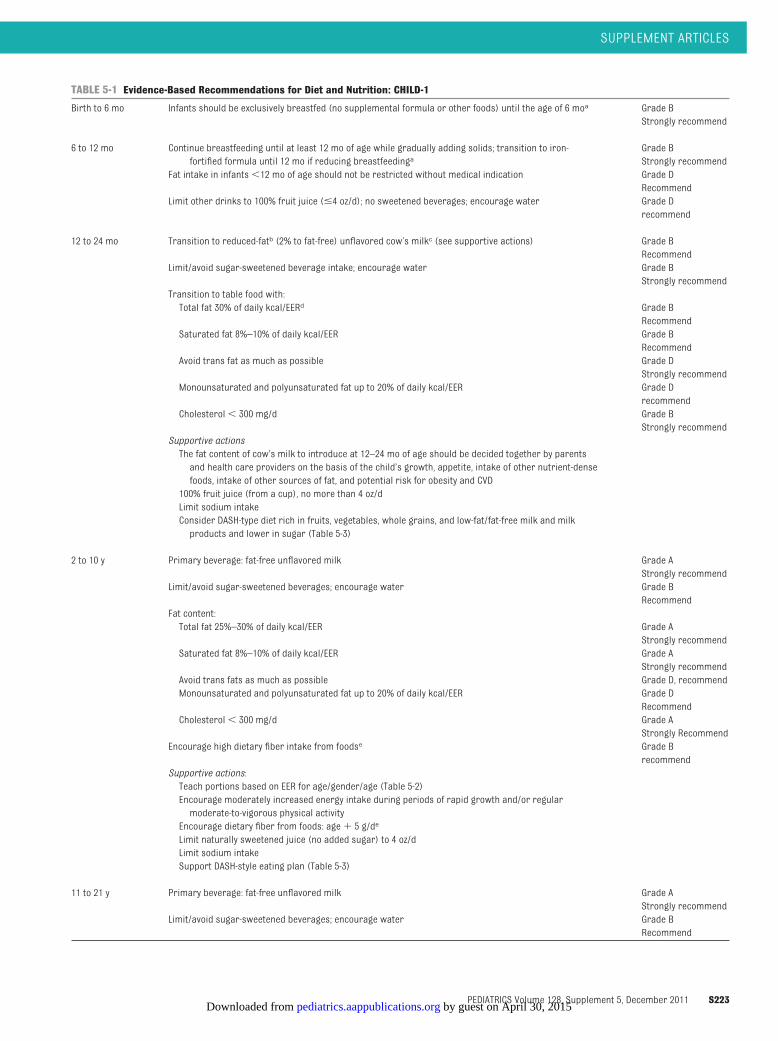
TABLE 5-1 Evidence-Based Recommendations for Diet and Nutrition: CHILD-1
Birth to 6 mo Infants should be exclusively breastfed (no supplemental formula or other foods) until the age of 6 moa Grade BStrongly recommend
6 to 12 mo Continue breastfeeding until at least 12 mo of age while gradually adding solids; transition to iron-fortified formula until 12 mo if reducing breastfeedinga
Grade BStrongly recommend
Fat intake in infants�12 mo of age should not be restricted without medical indication Grade DRecommend
Limit other drinks to 100% fruit juice (�4 oz/d); no sweetened beverages; encourage water Grade Drecommend
12 to 24 mo Transition to reduced-fatb (2% to fat-free) unflavored cow’s milkc (see supportive actions) Grade BRecommend
Limit/avoid sugar-sweetened beverage intake; encourage water Grade BStrongly recommend
Transition to table food with:Total fat 30% of daily kcal/EERd Grade B
RecommendSaturated fat 8%–10% of daily kcal/EER Grade B
RecommendAvoid trans fat as much as possible Grade D
Strongly recommendMonounsaturated and polyunsaturated fat up to 20% of daily kcal/EER Grade D
recommendCholesterol� 300 mg/d Grade B
Strongly recommendSupportive actionsThe fat content of cow’s milk to introduce at 12–24 mo of age should be decided together by parentsand health care providers on the basis of the child’s growth, appetite, intake of other nutrient-densefoods, intake of other sources of fat, and potential risk for obesity and CVD100% fruit juice (from a cup), no more than 4 oz/dLimit sodium intakeConsider DASH-type diet rich in fruits, vegetables, whole grains, and low-fat/fat-free milk and milkproducts and lower in sugar (Table 5-3)
2 to 10 y Primary beverage: fat-free unflavored milk Grade AStrongly recommend
Limit/avoid sugar-sweetened beverages; encourage water Grade BRecommend
Fat content:Total fat 25%–30% of daily kcal/EER Grade A
Strongly recommendSaturated fat 8%–10% of daily kcal/EER Grade A
Strongly recommendAvoid trans fats as much as possible Grade D, recommendMonounsaturated and polyunsaturated fat up to 20% of daily kcal/EER Grade D
RecommendCholesterol� 300 mg/d Grade A
Strongly RecommendEncourage high dietary fiber intake from foodse Grade B
recommendSupportive actions:Teach portions based on EER for age/gender/age (Table 5-2)Encourage moderately increased energy intake during periods of rapid growth and/or regularmoderate-to-vigorous physical activityEncourage dietary fiber from foods: age� 5 g/de
Limit naturally sweetened juice (no added sugar) to 4 oz/dLimit sodium intakeSupport DASH-style eating plan (Table 5-3)
11 to 21 y Primary beverage: fat-free unflavored milk Grade AStrongly recommend
Limit/avoid sugar-sweetened beverages; encourage water Grade BRecommend
SUPPLEMENT ARTICLES
PEDIATRICS Volume 128, Supplement 5, December 2011 S223 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
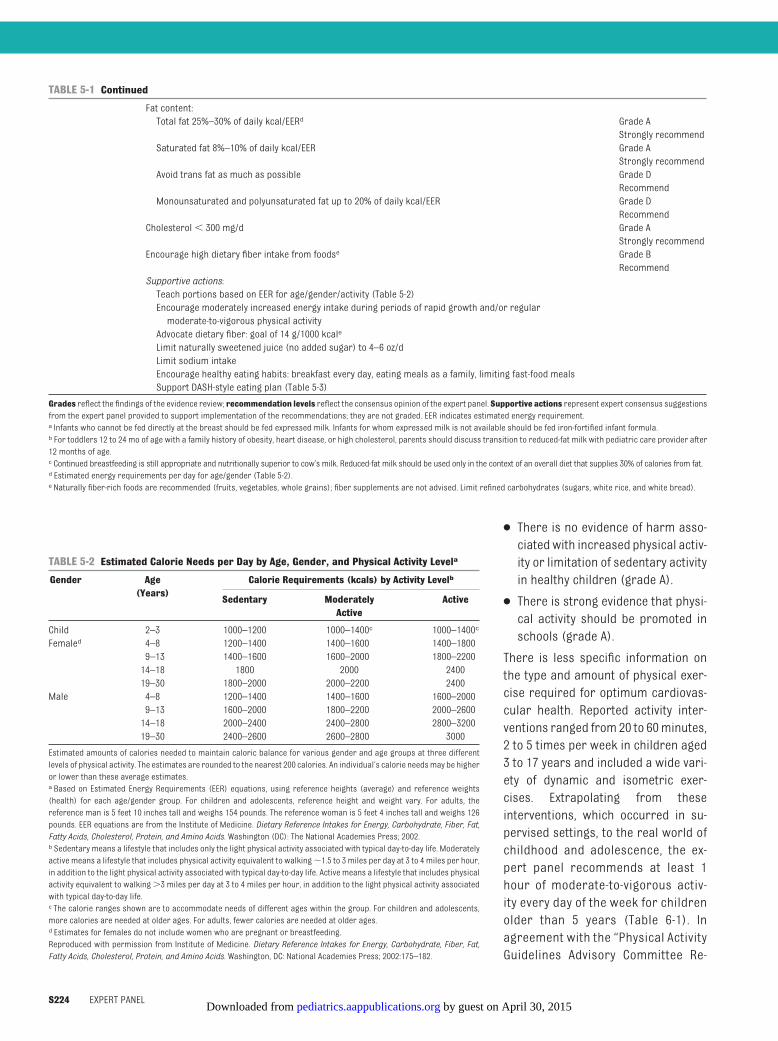
● There is no evidence of harm asso-ciatedwith increased physical activ-ity or limitation of sedentary activityin healthy children (grade A).
● There is strong evidence that physi-cal activity should be promoted inschools (grade A).
There is less specific information onthe type and amount of physical exer-cise required for optimum cardiovas-cular health. Reported activity inter-ventions ranged from 20 to 60minutes,2 to 5 times per week in children aged3 to 17 years and included a wide vari-ety of dynamic and isometric exer-cises. Extrapolating from theseinterventions, which occurred in su-pervised settings, to the real world ofchildhood and adolescence, the ex-pert panel recommends at least 1hour of moderate-to-vigorous activ-ity every day of the week for childrenolder than 5 years (Table 6-1). Inagreement with the “Physical ActivityGuidelines Advisory Committee Re-
TABLE 5-2 Estimated Calorie Needs per Day by Age, Gender, and Physical Activity Levela
Gender Age(Years)
Calorie Requirements (kcals) by Activity Levelb
Sedentary ModeratelyActive
Active
Child 2–3 1000–1200 1000–1400c 1000–1400c
Femaled 4–8 1200–1400 1400–1600 1400–18009–13 1400–1600 1600–2000 1800–220014–18 1800 2000 240019–30 1800–2000 2000–2200 2400
Male 4–8 1200–1400 1400–1600 1600–20009–13 1600–2000 1800–2200 2000–260014–18 2000–2400 2400–2800 2800–320019–30 2400–2600 2600–2800 3000
Estimated amounts of calories needed to maintain caloric balance for various gender and age groups at three differentlevels of physical activity. The estimates are rounded to the nearest 200 calories. An individual’s calorie needsmay be higheror lower than these average estimates.a Based on Estimated Energy Requirements (EER) equations, using reference heights (average) and reference weights(health) for each age/gender group. For children and adolescents, reference height and weight vary. For adults, thereference man is 5 feet 10 inches tall and weighs 154 pounds. The reference woman is 5 feet 4 inches tall and weighs 126pounds. EER equations are from the Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat,Fatty Acids, Cholesterol, Protein, and Amino Acids. Washington (DC): The National Academies Press; 2002.b Sedentary means a lifestyle that includes only the light physical activity associated with typical day-to-day life. Moderatelyactive means a lifestyle that includes physical activity equivalent to walking�1.5 to 3 miles per day at 3 to 4 miles per hour,in addition to the light physical activity associated with typical day-to-day life. Active means a lifestyle that includes physicalactivity equivalent to walking�3 miles per day at 3 to 4 miles per hour, in addition to the light physical activity associatedwith typical day-to-day life.c The calorie ranges shown are to accommodate needs of different ages within the group. For children and adolescents,more calories are needed at older ages. For adults, fewer calories are needed at older ages.d Estimates for females do not include women who are pregnant or breastfeeding.Reproduced with permission from Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat,Fatty Acids, Cholesterol, Protein, and Amino Acids. Washington, DC: National Academies Press; 2002:175–182.
TABLE 5-1 Continued
Fat content:Total fat 25%–30% of daily kcal/EERd Grade A
Strongly recommendSaturated fat 8%–10% of daily kcal/EER Grade A
Strongly recommendAvoid trans fat as much as possible Grade D
RecommendMonounsaturated and polyunsaturated fat up to 20% of daily kcal/EER Grade D
RecommendCholesterol� 300 mg/d Grade A
Strongly recommendEncourage high dietary fiber intake from foodse Grade B
RecommendSupportive actions:Teach portions based on EER for age/gender/activity (Table 5-2)Encourage moderately increased energy intake during periods of rapid growth and/or regularmoderate-to-vigorous physical activityAdvocate dietary fiber: goal of 14 g/1000 kcale
Limit naturally sweetened juice (no added sugar) to 4–6 oz/dLimit sodium intakeEncourage healthy eating habits: breakfast every day, eating meals as a family, limiting fast-food mealsSupport DASH-style eating plan (Table 5-3)
Grades reflect the findings of the evidence review; recommendation levels reflect the consensus opinion of the expert panel. Supportive actions represent expert consensus suggestionsfrom the expert panel provided to support implementation of the recommendations; they are not graded. EER indicates estimated energy requirement.a Infants who cannot be fed directly at the breast should be fed expressed milk. Infants for whom expressed milk is not available should be fed iron-fortified infant formula.b For toddlers 12 to 24 mo of age with a family history of obesity, heart disease, or high cholesterol, parents should discuss transition to reduced-fat milk with pediatric care provider after12 months of age.c Continued breastfeeding is still appropriate and nutritionally superior to cow’s milk. Reduced-fat milk should be used only in the context of an overall diet that supplies 30% of calories from fat.d Estimated energy requirements per day for age/gender (Table 5-2).e Naturally fiber-rich foods are recommended (fruits, vegetables, whole grains); fiber supplements are not advised. Limit refined carbohydrates (sugars, white rice, and white bread).
S224 EXPERT PANEL by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
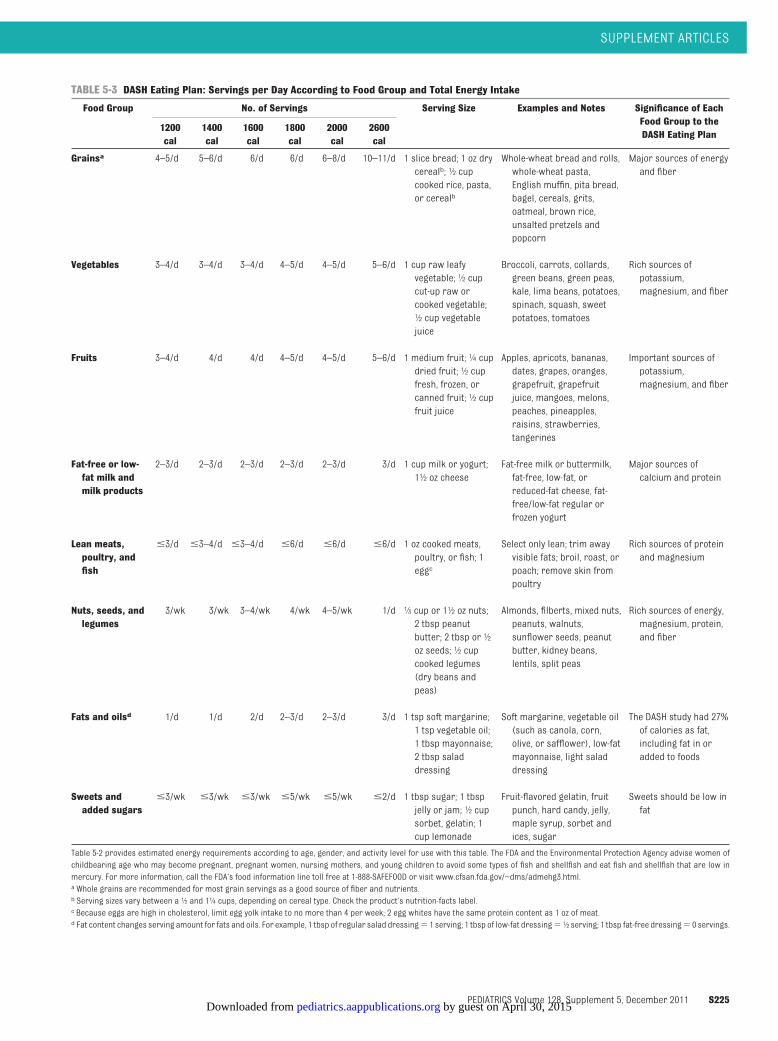
TABLE 5-3 DASH Eating Plan: Servings per Day According to Food Group and Total Energy Intake
Food Group No. of Servings Serving Size Examples and Notes Significance of EachFood Group to theDASH Eating Plan
1200cal
1400cal
1600cal
1800cal
2000cal
2600cal
Grainsa 4–5/d 5–6/d 6/d 6/d 6–8/d 10–11/d 1 slice bread; 1 oz drycerealb; 1⁄2 cupcooked rice, pasta,or cerealb
Whole-wheat bread and rolls,whole-wheat pasta,English muffin, pita bread,bagel, cereals, grits,oatmeal, brown rice,unsalted pretzels andpopcorn
Major sources of energyand fiber
Vegetables 3–4/d 3–4/d 3–4/d 4–5/d 4–5/d 5–6/d 1 cup raw leafyvegetable; 1⁄2 cupcut-up raw orcooked vegetable;1⁄2 cup vegetablejuice
Broccoli, carrots, collards,green beans, green peas,kale, lima beans, potatoes,spinach, squash, sweetpotatoes, tomatoes
Rich sources ofpotassium,magnesium, and fiber
Fruits 3–4/d 4/d 4/d 4–5/d 4–5/d 5–6/d 1 medium fruit; 1⁄4 cupdried fruit; 1⁄2 cupfresh, frozen, orcanned fruit; 1⁄2 cupfruit juice
Apples, apricots, bananas,dates, grapes, oranges,grapefruit, grapefruitjuice, mangoes, melons,peaches, pineapples,raisins, strawberries,tangerines
Important sources ofpotassium,magnesium, and fiber
Fat-free or low-fat milk andmilk products
2–3/d 2–3/d 2–3/d 2–3/d 2–3/d 3/d 1 cup milk or yogurt;11⁄2 oz cheese
Fat-free milk or buttermilk,fat-free, low-fat, orreduced-fat cheese, fat-free/low-fat regular orfrozen yogurt
Major sources ofcalcium and protein
Lean meats,poultry, andfish
�3/d �3–4/d �3–4/d �6/d �6/d �6/d 1 oz cooked meats,poultry, or fish; 1eggc
Select only lean; trim awayvisible fats; broil, roast, orpoach; remove skin frompoultry
Rich sources of proteinand magnesium
Nuts, seeds, andlegumes
3/wk 3/wk 3–4/wk 4/wk 4–5/wk 1/d 1⁄3 cup or 11⁄2 oz nuts;2 tbsp peanutbutter; 2 tbsp or 1⁄2oz seeds; 1⁄2 cupcooked legumes(dry beans andpeas)
Almonds, filberts, mixed nuts,peanuts, walnuts,sunflower seeds, peanutbutter, kidney beans,lentils, split peas
Rich sources of energy,magnesium, protein,and fiber
Fats and oilsd 1/d 1/d 2/d 2–3/d 2–3/d 3/d 1 tsp soft margarine;1 tsp vegetable oil;1 tbsp mayonnaise;2 tbsp saladdressing
Soft margarine, vegetable oil(such as canola, corn,olive, or safflower), low-fatmayonnaise, light saladdressing
The DASH study had 27%of calories as fat,including fat in oradded to foods
Sweets andadded sugars
�3/wk �3/wk �3/wk �5/wk �5/wk �2/d 1 tbsp sugar; 1 tbspjelly or jam; 1⁄2 cupsorbet, gelatin; 1cup lemonade
Fruit-flavored gelatin, fruitpunch, hard candy, jelly,maple syrup, sorbet andices, sugar
Sweets should be low infat
Table 5-2 provides estimated energy requirements according to age, gender, and activity level for use with this table. The FDA and the Environmental Protection Agency advise women ofchildbearing age who may become pregnant, pregnant women, nursing mothers, and young children to avoid some types of fish and shellfish and eat fish and shellfish that are low inmercury. For more information, call the FDA’s food information line toll free at 1-888-SAFEFOOD or visit www.cfsan.fda.gov/~dms/admehg3.html.a Whole grains are recommended for most grain servings as a good source of fiber and nutrients.b Serving sizes vary between a 1⁄2 and 11⁄4 cups, depending on cereal type. Check the product’s nutrition-facts label.c Because eggs are high in cholesterol, limit egg yolk intake to no more than 4 per week; 2 egg whites have the same protein content as 1 oz of meat.d Fat content changes serving amount for fats and oils. For example, 1 tbsp of regular salad dressing� 1 serving; 1 tbsp of low-fat dressing� 1⁄2 serving; 1 tbsp fat-free dressing� 0 servings.
SUPPLEMENT ARTICLES
PEDIATRICS Volume 128, Supplement 5, December 2011 S225 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

port, 2008”11 from the Department ofHealth and Human Services, the ex-pert panel recommends that activitybe vigorous on 3 days/week (www.health.gov/paguidelines). In workingwith children and families, the expertpanel suggested that moderate-to-vigorous activity could be comparedwith jogging or playing baseball and thatvigorous physical activity could be com-pared with running, playing singles ten-nis, or playing soccer. Similarly, reduc-ing sedentary time is convincinglyassociatedwitha favorable cardiovascu-lar profile, and the expert panel agreedwith the AAP recommendation for limit-ing leisure screen time to�2hours/day.
7. TOBACCO EXPOSURE
Tobacco dependence is responsible for�4 million deaths worldwide annually,and in utero exposure to tobacco prod-ucts, involuntary tobacco smoke expo-sure (secondhand smoke), and tobaccouse directly impair health in fetuses, in-fants, children, and adolescents. On thebasis of an analysis of published causesof death, tobacco use is the leading ac-tual cause of death in the United States.The evidence that cigarette use is harm-ful and addictive is unequivocal. In child-hood, nicotine is highly addicting;symptoms of tobacco dependencehave been found after brief intermit-tent use. Cigarette use among highschool students declined from 1997 to2003. Rates were stable from 2003 to2007 with �20% of high school stu-dents reporting daily smoking. From apublic health standpoint, the need toreduce tobacco exposure is compel-ling, and a role for pediatric healthcare providers is essential.
A clinical practice guideline updatefrom the US Public Health Service pub-lished in May 200812 systematically re-viewed almost 9000 publications andconcluded that smoking preventionand cessation interventions are effec-tive in adults. These same methods
should be safely applicable in child-hood and adolescence, because behav-ioral interventions to alter smoking be-haviors have little if any morbidity andbecause morbidity with pharmaco-logic treatment is limited. Physicianswho care for children are well posi-tioned to provide prevention and treat-ment interventions for their patients.Youth interventions must target par-ents as well as children, because pa-rental smoking is both a risk factor forchild smoking and provides second-hand smoke exposure to fetuses andchildren. The evidence review as-sessed prevention and treatment in-terventions in each of these areas.
Conclusions and Grading of theEvidence on Preventing TobaccoExposure
Among all the known risk factors forCVD, the dichotomy between known ben-efits of risk elimination and the paucityof evidence for effective interventions toachieve risk reduction in pediatric careprovider settings is greatest for tobaccoexposure. The quality of the evidence re-garding the harm of smoking and thebenefits of avoiding passive smoke expo-sure, smoking prevention, and smokingcessation is uniformly grade A. That evi-dence grades in the recommendationsare less than grade A reflects the lack ofexisting evidence on interventions thatimpact smokingbehaviors in specific pe-diatric age groups as opposed to the col-lective evidence.
● Good-quality interventions in pediatriccare settings to decrease children’s en-vironmental smoke exposure have hadmixed results (grade B).
● Intervention studies to preventsmoking initiation have had moder-ate success, although long-term re-sults are limited (grade B).
● Practice-based interventions to achievesmoking cessation in adolescents havehad moderate success with limitedlong-term follow-up (grade B).
● School-based smoking-preventionprograms have been moderatelysuccessful with limited long-termfollow-up (grade B).
Although the evidence base for effec-tive office-based approaches to to-bacco interventions is moderate andmixed, the evidence that cigarette useis harmful and addictive is unequivo-cal. The need to reduce tobacco expo-sure is so compelling that a role forpediatric health care providers is es-sential. The lack of harm associatedwith such interventions and the impor-tance of communicating the messageof risk associated with tobacco pro-vides the rationale for “strongly rec-ommend” despite the lack of conclu-sive evidence that office-basedinterventions reliably reduce tobaccoinitiation or smoking cessation. Physi-cians and nurses who care for chil-dren are well positioned to provide in-tervention to patients who smoke. Theexpert panel feels that such providersshould routinely identify patients whosmoke by using the medical history(Table 7-1). Patients should be explic-itly informed about the addictive andadverse health effects of tobacco use.By using the 5 A’s (ask, advise, assess,assist, and arrange), providers can as-sess readiness to quit and assist inproviding resources to supportsmoking-cessation efforts. Informa-tion about telephone quit lines (eg,1-800-QUIT-NOW), community cessationprograms, and pharmacotherapyshould also be made available.
As described, practice-based interven-tions to decrease environmentalsmoke exposure have had mixed re-sults. Nonetheless, the expert panelbelieves that pediatric care providersshould identify parents and othercaregivers who smoke and explicitlyrecommend that children not be ex-posed to tobacco smoke in the home,in automobiles, or in any other spacewhere exposure can occur. For the
S226 EXPERT PANEL by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

parent who smokes, information pro-vided should include statements abouthealth benefits to the individual, child,and/or fetus and referral to smoking-cessation care providers.
8. HIGH BP
In 2004, an NHLBI task force published“The Fourth Report on the Diagnosis,Evaluation, and Treatment of HighBlood Pressure in Children and Adoles-cents.”13 This report included a com-plete review of the current evidence onthis subject and detailed recommen-dations for managing BP throughoutchildhood. These recommendationswere used as the basis for these guide-lines, considered complete until 2003when the review for the report ended.Therefore, this evidence review for BPfor these guidelines was limited to stud-ies published between January 1, 2003,and June 30, 2007, with the addition ofselected studies through June 30, 2008,identified by the expert panel as havingmet all the criteria for inclusion. Repeat-ing the review performed by the taskforce was not felt to be necessary, giventhe short time since publication of thatreport, or a judicious use of the re-sources available for development ofthese guidelines. Recommendations re-gardingBPare all gradedas expert opin-ion (gradeD), because they arebasedonthe expert consensus conclusions of thisNHLBI task force.
Conclusions of the Evidence-ReviewUpdate for High BP (2003–2008)
● The evidence review for the definedtime period resulted in no majorchanges in the approach to BP eval-uation and management.
● According to epidemiologic surveysof children and adolescents overthe past 20 years, BP levels havebeen increasing, and the prevalenceof hypertension and prehyperten-sion are also increasing, explainedpartially by the rise in obesity rates.
TABLE 6-1 Evidence-Based Activity Recommendations for Cardiovascular Health
Newborn to12 mo
Parents should create an environment that promotes and modelsphysical activity and limits sedentary time
Grade DRecommend
Supportive actions:Discourage TV viewing altogether
1 to 4 y Allow unlimited active playtime in safe, supportive environments Grade DRecommend
Limit sedentary time, especially TV/video Grade DRecommend
Supportive actions:Limit total media time to no more than 1-2 hours of qualityprogramming per dayFor children�2 y old, discourage TV viewing altogetherNo TV in child’s bedroomEncourage family activity at least once per weekCounsel routine activity for parents as role models for children
5 to 10 y Moderate-to-vigorous physical activity every daya Grade AStrongly recommend
Limit daily leisure screen time (TV/video/computer) Grade BStrongly recommend
Supportive actions:Prescribe moderate-to-vigorous activity 1 h/da with vigorous-intensity physical activity 3 d/wkb
Limit total media time to no more than 1–2 h/d of qualityprogrammingNo TV in child’s bedroomTake activity and screen-time history from child once per yearMatch physical activity recommendations with energy intakeRecommend appropriate safety equipment relative to eachsportSupport recommendations for daily physical education inschools
11 to 17 y Moderate-to-vigorous physical activity every daya Grade AStrongly recommend
Limit leisure time TV/video/computer use Grade BStrongly recommend
Supportive actions:Encourage adolescents to aim for 1 h/d of moderate-to-vigorousdaily activitya with vigorous intense physical activityb 3 d/wk
Encourage no TV in bedroomLimit total media time to no more than 1–2 h/d of qualityprogrammingMatch activity recommendations with energy intakeTake activity and screen-time history from adolescent at healthsupervision visitsEncourage involvement in year-round physical activitiesSupport continued family activity once per week and/or familysupport of adolescent’s physical activity programEndorse appropriate safety equipment relative to each sport
18 to 21 y Moderate-to-vigorous physical activity every daya Grade AStrongly recommend
Limit leisure time TV/video/computer Grade BStrongly recommend
Supportive actions:Support goal of 1 h/d of moderate-to-vigorous activity withvigorous intense physical activity 3 d/wkRecommend that combined leisure screen time not exceed 2 h/dActivity and screen-time history at health supervision visitsEncourage involvement in year-round, lifelong physical activities
Grades reflect the findings of the evidence review; recommendation levels reflect the consensus opinion of the expertpanel; and supportive actions represent expert consensus suggestions from the expert panel provided to supportimplementation of the recommendations (they are not graded).a Examples of moderate-to-vigorous physical activities are jogging and playing baseball.b Examples of vigorous physical activities are running, playing singles tennis, and playing soccer.
SUPPLEMENT ARTICLES
PEDIATRICS Volume 128, Supplement 5, December 2011 S227 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

● Prehypertension progresses to hy-pertension at a rate of �7% peryear; hypertension persists in al-most one-third of boys and one-fourth of girls on 2-year longitudinalfollow-up.
● Breastfeeding and supplementationof formula with polyunsaturatedfatty acids in infancy are both asso-ciated with lower BP at follow-up.
● A DASH-style diet, which is rich infruits, vegetables, low-fat or fat-freedairy products, whole grains, fish,poultry, beans, seeds, and nuts andlower in sweets and added sugars,fats, and red meats than the typicalAmerican diet, is associated withlower BP. The CHILD-1 combinedwith the DASH eating plan describedin “Diet and Nutrition” is an appro-priate diet for children that meetsthe DASH study and 2010 DGA nutri-ent goals.
● Lower dietary sodium intake is as-sociated with lower BP levels in in-fants, children, and adolescents.
● Losartan, amlodipine, felodipine, fosi-nopril, lisinopril, metoprolol, and val-sartan canbeadded to the list ofmed-ications that are tolerated over shortperiodsandcan reduceBP in childrenfrom ages 6 to 17 years but are pre-dominantly effective in adolescents.For black children, greater doses offosinopril might be needed for effec-tive BP control. Medications areshown in Table 8-5.
●In 1 study of small-for-gestational-age infants, a nutrient-enriched dietthat promoted rapid weight gain wasassociated with higher BP onfollow-up in late childhood. This po-tential risk should be consideredwhen such diets are selected in theclinical setting.
● In another study, transcendentalmeditation effectively lowered BP innonhypertensive adolescents.
Recommendations
In “The Fourth Report on the Diagnosis,Evaluation, and Treatment of HighBlood Pressure in Children and Adoles-cents,”13 an NHLBI task force providedan algorithm and flow diagram to as-sist clinicians in identifying hyperten-sion in children. For these guidelines,the task force’s recommendations arestratified here to provide an age-appropriate approach congruent withother risk-factor recommendations inother sections, and this is also re-flected in a series of revised algo-rithms (Table 8-1 and Figs 8-1 and 8-2).Conditions under which childrenyounger than 3 years should have BPmeasured are shown in Table 8-2. TheBP norms for age, gender, and height
TABLE 7-1 Evidence-Based Recommendations to Prevent Tobacco Exposure
Prenatal Obtain smoking history from mothers; provide explicit smoking-cessation message beforeand during pregnancy
Grade AStrongly recommend
Supportive actions:Identify resources to support maternal smoking-cessation efforts.Advocate for school and community-based smoke-free interventionsSee “Perinatal Factors” section
0 to 4 y Smoke-free home environment Grade BStrongly recommend
Reinforce this message at every encounter, including urgent visits for respiratory problems Grade CRecommend
Supportive actions:Provide information about health benefits of a smoke-free home to parents and childrenAdvocate for school- and community-based smoke-free interventions
5 to 10 y Obtain smoke-exposure history from child, including personal history of tobacco use Grade CRecommend
Counsel patients strongly about not smoking, including providing explicit information aboutthe addictive and adverse health effects of smoking
Grade CRecommend
11 to 21 y Obtain personal smoking history at every nonurgent health encounter Grade BStrongly recommend
Explicitly recommend against smoking Grade BStrongly recommend
Provide specific smoking-cessation guidance Grade BStrongly recommend
Supportive actions:Use 5 A questions to assess readiness to quitEstablish your health care practice as a resource for smoking cessationProvide quit-line phone numberIdentify community cessation resourcesProvide information about pharmacotherapy for cessationAdvocate for school and community-based smoke-free interventions
Grades reflect the findings of the evidence review; recommendation levels reflect the consensus opinion of the expert panel; and supportive actions represent expert consensussuggestions from the expert panel provided to support implementation of the recommendations (they are not graded).
S228 EXPERT PANEL by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

are shown in Tables 8-3 and 8-4 andwere taken directly from the NHLBItask force’s report. Age-specific per-centiles of BP measurements frombirth to 12 months are provided in the“Report of the Fourth Task Force onBlood Pressure Control in Children.”
For all age groups the assessment ofleft ventricular mass by echocardiog-raphy is recommended as the bestmethod of assessing hypertensive tar-get organ disease; this testing shouldbe performed for patients with stage 2hypertension and those with persis-
tent stage 1 hypertension. Elevated leftventricular massmight be useful in es-tablishing the need for pharmacologictreatment of hypertension. In Table 8-5,the medications used to achieve BPcontrol in children and adolescentsare listed. At present, there are no datato support the use of specific antihy-pertensive agents for specific agegroups.
9. LIPIDS AND LIPOPROTEINS
Since the last NHLBI guidelines for lipidmanagement in children and adoles-cents were published in 1992,1 both theknowledge base surrounding dyslipi-demia in childhood and the clinical pic-ture have changed. A series of criticalobservational studies have found aclear correlation between lipoproteindisorders and the onset and severity ofatherosclerosis in children, adoles-cents, and young adults. A major in-crease in the prevalence of obesity hasled to a much larger population of chil-dren with dyslipidemia. At the time ofthe original guidelines, the focus wasalmost exclusively on identification ofchildren with an elevated LDL choles-terol level. Since then, the predomi-nant dyslipidemic pattern in childhoodis a combined pattern associated withobesity, moderate-to-severe elevationin triglyceride level, normal-to-mildelevation in LDL cholesterol level,and a reduced HDL cholesterol level.Both dyslipidemic patterns havebeen shown to be associated with ini-tiation and progression of athero-sclerotic lesions in children and ad-olescents as demonstrated bypathology and imaging studies. Iden-tification of children with dyslipi-demias, which place them at in-creased risk for accelerated earlyatherosclerosis, must include a com-prehensive assessment of serumlipid and lipoprotein levels.
The evidence review for lipids and lipo-proteins addressed the association
TABLE 8-1 Age-Specific Recommendations for BP Measurement and Diagnosis ofHypertension
Birth to 3 y No routine BP measurementMeasure BP if history (�) for neonatal complications, congenital heart disease, urinary/
renal abnormality, solid-organ transplant, malignancy, drug prescription, orcondition known to raise BP or increase intracranial pressure (Table 8-2)
If BP�90th percentile by oscillometry, confirm by auscultation¡ If BP confirmed�90thpercentile, initiate evaluation for etiology and treatment per algorithm (Figure8-2)
3 to 11 y Annual BP measurement in all, interpreted for age/gender/height per Tables 8-3 and 8-4If BP�90th percentile, repeat in 1 yIf BP�90th percentile:Repeat BP� 2 by auscultationAverage replicate measurements and reevaluate BP category (Fig 8-1)
If BP confirmed�90th percentile,�95th percentile� prehypertension (HTN):Recommend weight management if indicatedRepeat BP in 6 mo
If BP�95th percentile,�99th percentile� 5 mm Hg:Repeat BP in 1–2 wk, average all BP measurements and reevaluate BP category (Fig8-1)
If BP confirmed�95th percentile,�99th percentile� 5 mm Hg� stage 1 HTN:Basic work-up per Fig 8-2
If BP�99th percentile� 5 mm HgRepeat BP by auscultation� 3 at that visit, average all BP measurements andreevaluate BP category
If BP confirmed�99th percentile� 5 mm Hg� stage 2 HTN:Refer to pediatric HTN expert within 1 wk ORBegin BP treatment and initiate basic work-up, per Fig 8-2
12 to 17 y Annual BP measurement in all, interpreted for age/gender/height per Tables 8-3 and 8-4If BP�90th percentile, counsel on CHILD-1 diet, activity recommendations, and repeat BP
in 1 yIf BP�90th percentile or�120/80 mm Hg:
Repeat BP� 2 by auscultationAverage replicate measurements and reevaluate BP category (Fig 8-1)
If BP confirmed�90th percentile,� 95th percentile or�120/80� pre-HTN:CHILD-1 diet, activity recommendations, weight management if indicatedRepeat BP in 6 mo
If BP�95th percentile,�99th percentile� 5 mm HgRepeat BP in 1–2 wk, average all BP measurements and reevaluate BP category (Fig8-1)
If BP confirmed�95th percentile,�99th percentile� 5 mm Hg� stage 1 HTN:Basic workup per Fig 2
If BP�99th percentile� 5 mm Hg:Repeat BP by auscultation� 3 at that visit, average all BP measurements andreevaluate BP category
If BP confirmed�99th percentile� 5 mm Hg� stage 2 HTN:Refer to pediatric HTN expert within 1 wk ORBegin BP treatment and initiate work-up per Fig 8-2
18 to 21 y Measure BP at all health care visitsBP�120/80 to 139/89� pre-HTNBP�140/90 to 159/99� stage 1 HTNBP�160/100� stage 2 HTN
BP recommendations are based on the NHLBI’s “The Fourth Report on the Diagnosis, Evaluation and Treatment of High BloodPressure in Children and Adolescents” with the evidence review updated from 2003. Recommendations are all graded asexpert opinion (grade D) because they are based on the expert consensus conclusions of the Fourth Report.
SUPPLEMENT ARTICLES
PEDIATRICS Volume 128, Supplement 5, December 2011 S229 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

between dyslipidemia and atheroscle-rosis in childhood, lipid assessment inchildhood and adolescence with tablesof normative results provided, the dys-lipidemias, dietary treatment of dyslip-idemia, and medication therapy.
Conclusions and Grading of theEvidence Review for LipidAssessment in Childhood andAdolescence
● Combined evidence from autopsystudies, vascular studies, and co-hort studies strongly indicates thatabnormal lipid levels in childhoodare associated with increased evi-dence of atherosclerosis (grade B).
● The evidence review supports theconcept that early identification andcontrol of dyslipidemia throughoutyouth and into adulthood will sub-stantially reduce clinical CVD riskbeginning in young adult life. Pre-liminary evidence in children withheterozygous familial hypercholes-terolemia with markedly elevatedLDL cholesterol levels indicates thatearlier treatment is associated withreduced subclinical evidence of ath-erosclerosis (grade B).
● Multiple prospective screening co-hort studies have demonstrated thenormal lipid and lipoprotein distri-butions in childhood, adolescence,and young adult life (Tables 9-1 and9-2) (grade B). Cohort studies havealso demonstrated significanttracking of elevated lipid levels from
childhood into adulthood. Lipid andlipoprotein results in childhood arepredictive of future adult lipopro-tein profiles; the strongest statisti-cal correlation occurs between re-sults in late childhood and in thethird and fourth decades of life(grade B).
● TC and LDL cholesterol levels de-crease as much as 10% to 20% ormoreduringpuberty (gradeB).On thebasis of thisnormalpatternof changein lipid and lipoprotein levels withgrowth and maturation, 10 years ofage (range: 9–11 years) is a stabletime for lipid assessment in children(grade D). For most children, this agerange will precede the onset ofpuberty.
● Significant evidence exists to indicatethat using family history of prematureCVD or cholesterol disorders as theprimary factor in determining lipidscreening for children misses�30%to 60%of childrenwith dyslipidemias,and accurate and reliable measuresof family history are not available(grade B). In the absence of a clinicalor historic marker, identification ofchildren with lipid disorders that pre-dispose them to accelerated athero-sclerosis requires universal lipid as-sessment (grade B).
● Non-HDL cholesterol level has beenidentified as a significant predictorof the presence of atherosclerosis,as powerful as any other lipoprotein
cholesterol measure in childrenand adolescents. For both childrenand adults, non-HDL cholesterollevel seems to be more predictive ofpersistent dyslipidemia and, there-fore, atherosclerosis and futureevents than TC, LDL cholesterol, orHDL cholesterol levels alone. A ma-jor advantage of non-HDL choles-terol is that it can be accurately cal-culated in a nonfasting state and istherefore practical to obtain in clin-ical practice. The expert panel feltthat non-HDL cholesterol should beadded as a screening tool for iden-tification of a dyslipidemic state inchildhood (grade B).
● In terms of other lipid measure-ments, (1) most but not all studieshave found that measurement ofapolipoprotein B and apolipopro-tein A-1 for universal screening pro-vides no additional advantage overmeasuring non-HDL cholesterol, LDLcholesterol, and HDL cholesterol lev-els, (2) measurement of lipopro-tein(a) is useful in the assessmentof children with both hemorrhagicand ischemic stroke, (3) in offspringof a parent with premature CVD andno other identifiable risk factors, el-evations of apolipoprotein B, apoli-poprotein A-1, and lipoprotein(a)have been noted, and (4) measure-ment of lipoprotein subclasses andtheir sizes by advanced lipoproteintesting has not been found to havesufficient clinical utility in childrenat this time (grade B).
● Obesity is commonly associatedwith a combined dyslipidemia pat-tern with mild elevation in TC andLDL cholesterol levels, moderate-to-severe elevation in triglyceridelevel, and a low HDL cholesterollevel. This is the most common dys-lipidemic pattern seen in childhood,and lipid assessment in overweightand obese children identifies an im-portant proportion of those with
TABLE 8-2 Conditions Under Which Children <3 Years Old Should Have BP Measured
History of prematurity, very low birth weight, or other neonatal complication requiring intensive careCongenital heart disease (repaired or unrepaired)Recurrent urinary tract infections, hematuria, or proteinuriaKnown renal disease or urologic malformationsFamily history of congenital renal diseaseSolid-organ transplantMalignancy or bone marrow transplantTreatment with drugs known to raise BPOther systemic illnesses associated with hypertension (neurofibromatosis, tuberous sclerosis, etc)Evidence of increased intracranial pressure
Reproduced with permission from High Blood Pressure Education Program Working Group on High Blood Pressure inChildren and Adolescents. Pediatrics. 2004;114(2 suppl 4th report):556.
S230 EXPERT PANEL by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
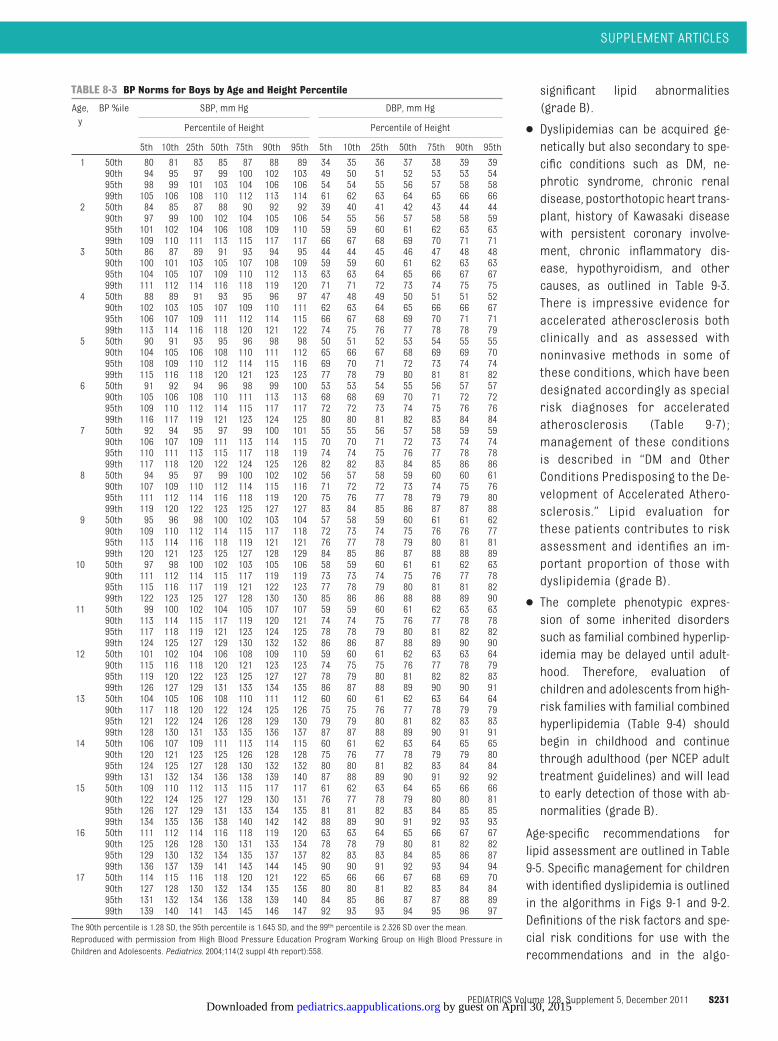
significant lipid abnormalities(grade B).
● Dyslipidemias can be acquired ge-netically but also secondary to spe-cific conditions such as DM, ne-phrotic syndrome, chronic renaldisease, postorthotopic heart trans-plant, history of Kawasaki diseasewith persistent coronary involve-ment, chronic inflammatory dis-ease, hypothyroidism, and othercauses, as outlined in Table 9-3.There is impressive evidence foraccelerated atherosclerosis bothclinically and as assessed withnoninvasive methods in some ofthese conditions, which have beendesignated accordingly as specialrisk diagnoses for acceleratedatherosclerosis (Table 9-7);management of these conditionsis described in “DM and OtherConditions Predisposing to the De-velopment of Accelerated Athero-sclerosis.” Lipid evaluation forthese patients contributes to riskassessment and identifies an im-portant proportion of those withdyslipidemia (grade B).
● The complete phenotypic expres-sion of some inherited disorderssuch as familial combined hyperlip-idemia may be delayed until adult-hood. Therefore, evaluation ofchildren and adolescents from high-risk families with familial combinedhyperlipidemia (Table 9-4) shouldbegin in childhood and continuethrough adulthood (per NCEP adulttreatment guidelines) and will leadto early detection of those with ab-normalities (grade B).
Age-specific recommendations forlipid assessment are outlined in Table9-5. Specific management for childrenwith identified dyslipidemia is outlinedin the algorithms in Figs 9-1 and 9-2.Definitions of the risk factors and spe-cial risk conditions for use with therecommendations and in the algo-
TABLE 8-3 BP Norms for Boys by Age and Height Percentile
Age,yBP %ile SBP, mm Hg DBP, mm Hg
Percentile of Height Percentile of Height
5th 10th 25th 50th 75th 90th 95th 5th 10th 25th 50th 75th 90th 95th
1 50th 80 81 83 85 87 88 89 34 35 36 37 38 39 3990th 94 95 97 99 100 102 103 49 50 51 52 53 53 5495th 98 99 101 103 104 106 106 54 54 55 56 57 58 5899th 105 106 108 110 112 113 114 61 62 63 64 65 66 66
2 50th 84 85 87 88 90 92 92 39 40 41 42 43 44 4490th 97 99 100 102 104 105 106 54 55 56 57 58 58 5995th 101 102 104 106 108 109 110 59 59 60 61 62 63 6399th 109 110 111 113 115 117 117 66 67 68 69 70 71 71
3 50th 86 87 89 91 93 94 95 44 44 45 46 47 48 4890th 100 101 103 105 107 108 109 59 59 60 61 62 63 6395th 104 105 107 109 110 112 113 63 63 64 65 66 67 6799th 111 112 114 116 118 119 120 71 71 72 73 74 75 75
4 50th 88 89 91 93 95 96 97 47 48 49 50 51 51 5290th 102 103 105 107 109 110 111 62 63 64 65 66 66 6795th 106 107 109 111 112 114 115 66 67 68 69 70 71 7199th 113 114 116 118 120 121 122 74 75 76 77 78 78 79
5 50th 90 91 93 95 96 98 98 50 51 52 53 54 55 5590th 104 105 106 108 110 111 112 65 66 67 68 69 69 7095th 108 109 110 112 114 115 116 69 70 71 72 73 74 7499th 115 116 118 120 121 123 123 77 78 79 80 81 81 82
6 50th 91 92 94 96 98 99 100 53 53 54 55 56 57 5790th 105 106 108 110 111 113 113 68 68 69 70 71 72 7295th 109 110 112 114 115 117 117 72 72 73 74 75 76 7699th 116 117 119 121 123 124 125 80 80 81 82 83 84 84
7 50th 92 94 95 97 99 100 101 55 55 56 57 58 59 5990th 106 107 109 111 113 114 115 70 70 71 72 73 74 7495th 110 111 113 115 117 118 119 74 74 75 76 77 78 7899th 117 118 120 122 124 125 126 82 82 83 84 85 86 86
8 50th 94 95 97 99 100 102 102 56 57 58 59 60 60 6190th 107 109 110 112 114 115 116 71 72 72 73 74 75 7695th 111 112 114 116 118 119 120 75 76 77 78 79 79 8099th 119 120 122 123 125 127 127 83 84 85 86 87 87 88
9 50th 95 96 98 100 102 103 104 57 58 59 60 61 61 6290th 109 110 112 114 115 117 118 72 73 74 75 76 76 7795th 113 114 116 118 119 121 121 76 77 78 79 80 81 8199th 120 121 123 125 127 128 129 84 85 86 87 88 88 89
10 50th 97 98 100 102 103 105 106 58 59 60 61 61 62 6390th 111 112 114 115 117 119 119 73 73 74 75 76 77 7895th 115 116 117 119 121 122 123 77 78 79 80 81 81 8299th 122 123 125 127 128 130 130 85 86 86 88 88 89 90
11 50th 99 100 102 104 105 107 107 59 59 60 61 62 63 6390th 113 114 115 117 119 120 121 74 74 75 76 77 78 7895th 117 118 119 121 123 124 125 78 78 79 80 81 82 8299th 124 125 127 129 130 132 132 86 86 87 88 89 90 90
12 50th 101 102 104 106 108 109 110 59 60 61 62 63 63 6490th 115 116 118 120 121 123 123 74 75 75 76 77 78 7995th 119 120 122 123 125 127 127 78 79 80 81 82 82 8399th 126 127 129 131 133 134 135 86 87 88 89 90 90 91
13 50th 104 105 106 108 110 111 112 60 60 61 62 63 64 6490th 117 118 120 122 124 125 126 75 75 76 77 78 79 7995th 121 122 124 126 128 129 130 79 79 80 81 82 83 8399th 128 130 131 133 135 136 137 87 87 88 89 90 91 91
14 50th 106 107 109 111 113 114 115 60 61 62 63 64 65 6590th 120 121 123 125 126 128 128 75 76 77 78 79 79 8095th 124 125 127 128 130 132 132 80 80 81 82 83 84 8499th 131 132 134 136 138 139 140 87 88 89 90 91 92 92
15 50th 109 110 112 113 115 117 117 61 62 63 64 65 66 6690th 122 124 125 127 129 130 131 76 77 78 79 80 80 8195th 126 127 129 131 133 134 135 81 81 82 83 84 85 8599th 134 135 136 138 140 142 142 88 89 90 91 92 93 93
16 50th 111 112 114 116 118 119 120 63 63 64 65 66 67 6790th 125 126 128 130 131 133 134 78 78 79 80 81 82 8295th 129 130 132 134 135 137 137 82 83 83 84 85 86 8799th 136 137 139 141 143 144 145 90 90 91 92 93 94 94
17 50th 114 115 116 118 120 121 122 65 66 66 67 68 69 7090th 127 128 130 132 134 135 136 80 80 81 82 83 84 8495th 131 132 134 136 138 139 140 84 85 86 87 87 88 8999th 139 140 141 143 145 146 147 92 93 93 94 95 96 97
The 90th percentile is 1.28 SD, the 95th percentile is 1.645 SD, and the 99th percentile is 2.326 SD over the mean.Reproduced with permission from High Blood Pressure Education Program Working Group on High Blood Pressure inChildren and Adolescents. Pediatrics. 2004;114(2 suppl 4th report):558.
SUPPLEMENT ARTICLES
PEDIATRICS Volume 128, Supplement 5, December 2011 S231 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
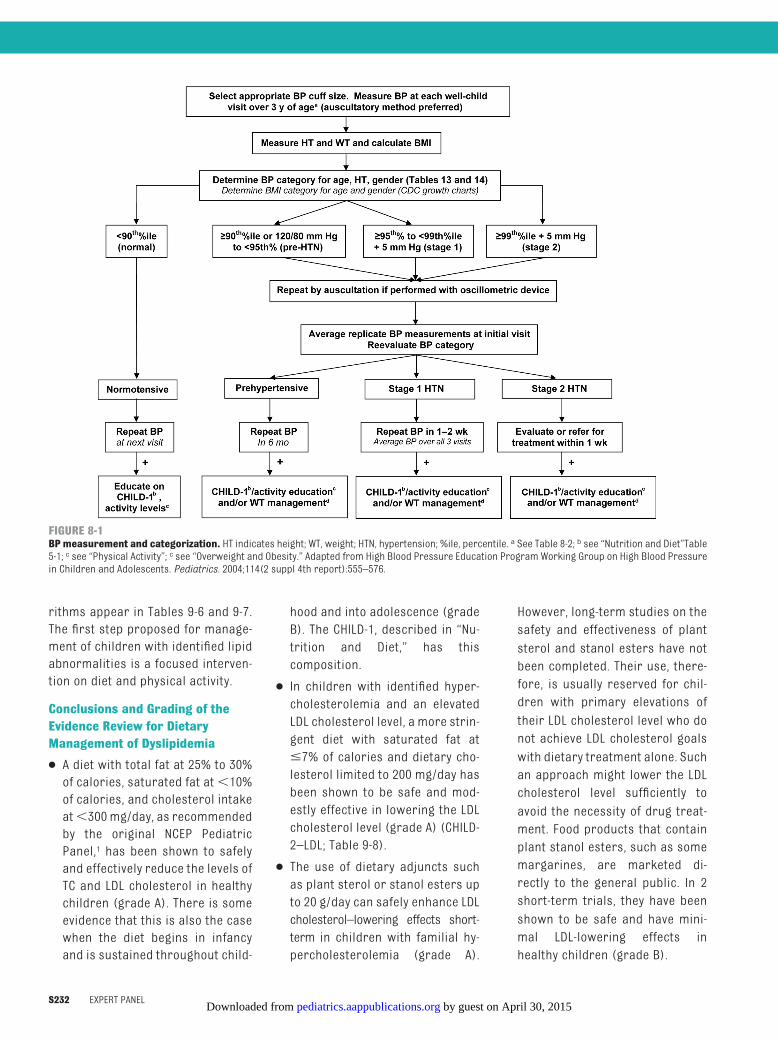
rithms appear in Tables 9-6 and 9-7.The first step proposed for manage-ment of children with identified lipidabnormalities is a focused interven-tion on diet and physical activity.
Conclusions and Grading of theEvidence Review for DietaryManagement of Dyslipidemia
● A diet with total fat at 25% to 30%of calories, saturated fat at�10%of calories, and cholesterol intakeat�300 mg/day, as recommendedby the original NCEP PediatricPanel,1 has been shown to safelyand effectively reduce the levels ofTC and LDL cholesterol in healthychildren (grade A). There is someevidence that this is also the casewhen the diet begins in infancyand is sustained throughout child-
hood and into adolescence (gradeB). The CHILD-1, described in “Nu-trition and Diet,” has thiscomposition.
● In children with identified hyper-cholesterolemia and an elevatedLDL cholesterol level, a more strin-gent diet with saturated fat at�7% of calories and dietary cho-lesterol limited to 200 mg/day hasbeen shown to be safe and mod-estly effective in lowering the LDLcholesterol level (grade A) (CHILD-2–LDL; Table 9-8).
● The use of dietary adjuncts suchas plant sterol or stanol esters upto 20 g/day can safely enhance LDLcholesterol–lowering effects short-term in children with familial hy-percholesterolemia (grade A).
However, long-term studies on thesafety and effectiveness of plantsterol and stanol esters have notbeen completed. Their use, there-fore, is usually reserved for chil-dren with primary elevations oftheir LDL cholesterol level who donot achieve LDL cholesterol goalswith dietary treatment alone. Suchan approach might lower the LDLcholesterol level sufficiently toavoid the necessity of drug treat-ment. Food products that containplant stanol esters, such as somemargarines, are marketed di-rectly to the general public. In 2short-term trials, they have beenshown to be safe and have mini-mal LDL-lowering effects inhealthy children (grade B).
FIGURE 8-1BP measurement and categorization. HT indicates height; WT, weight; HTN, hypertension; %ile, percentile. a See Table 8-2; b see “Nutrition and Diet”Table5-1; c see “Physical Activity”; c see “Overweight and Obesity.” Adapted from High Blood Pressure Education Program Working Group on High Blood Pressurein Children and Adolescents. Pediatrics. 2004;114(2 suppl 4th report):555–576.
S232 EXPERT PANEL by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
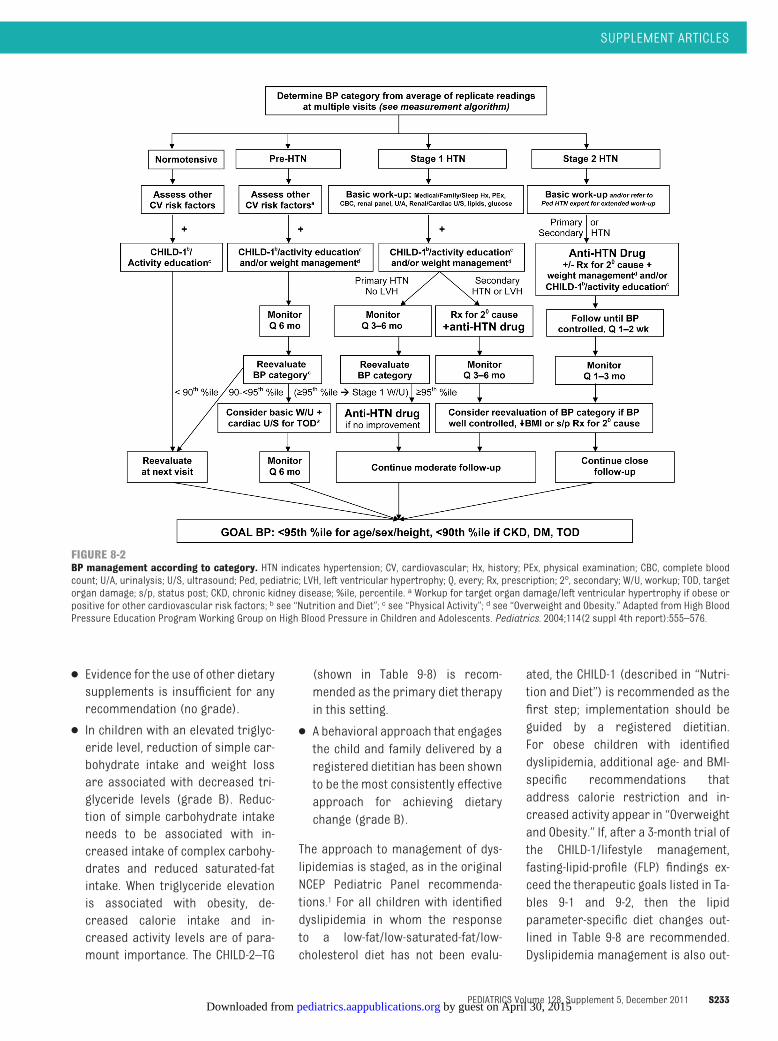
● Evidence for the use of other dietarysupplements is insufficient for anyrecommendation (no grade).
● In children with an elevated triglyc-eride level, reduction of simple car-bohydrate intake and weight lossare associated with decreased tri-glyceride levels (grade B). Reduc-tion of simple carbohydrate intakeneeds to be associated with in-creased intake of complex carbohy-drates and reduced saturated-fatintake. When triglyceride elevationis associated with obesity, de-creased calorie intake and in-creased activity levels are of para-mount importance. The CHILD-2–TG
(shown in Table 9-8) is recom-mended as the primary diet therapyin this setting.
● A behavioral approach that engagesthe child and family delivered by aregistered dietitian has been shownto be the most consistently effectiveapproach for achieving dietarychange (grade B).
The approach to management of dys-lipidemias is staged, as in the originalNCEP Pediatric Panel recommenda-tions.1 For all children with identifieddyslipidemia in whom the responseto a low-fat/low-saturated-fat/low-cholesterol diet has not been evalu-
ated, the CHILD-1 (described in “Nutri-tion and Diet”) is recommended as thefirst step; implementation should beguided by a registered dietitian.For obese children with identifieddyslipidemia, additional age- and BMI-specific recommendations thataddress calorie restriction and in-creased activity appear in “Overweightand Obesity.” If, after a 3-month trial ofthe CHILD-1/lifestyle management,fasting-lipid-profile (FLP) findings ex-ceed the therapeutic goals listed in Ta-bles 9-1 and 9-2, then the lipidparameter-specific diet changes out-lined in Table 9-8 are recommended.Dyslipidemia management is also out-
FIGURE 8-2BP management according to category. HTN indicates hypertension; CV, cardiovascular; Hx, history; PEx, physical examination; CBC, complete bloodcount; U/A, urinalysis; U/S, ultrasound; Ped, pediatric; LVH, left ventricular hypertrophy; Q, every; Rx, prescription; 2°, secondary; W/U, workup; TOD, targetorgan damage; s/p, status post; CKD, chronic kidney disease; %ile, percentile. a Workup for target organ damage/left ventricular hypertrophy if obese orpositive for other cardiovascular risk factors; b see “Nutrition and Diet”; c see “Physical Activity”; d see “Overweight and Obesity.” Adapted from High BloodPressure Education Program Working Group on High Blood Pressure in Children and Adolescents. Pediatrics. 2004;114(2 suppl 4th report):555–576.
SUPPLEMENT ARTICLES
PEDIATRICS Volume 128, Supplement 5, December 2011 S233 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
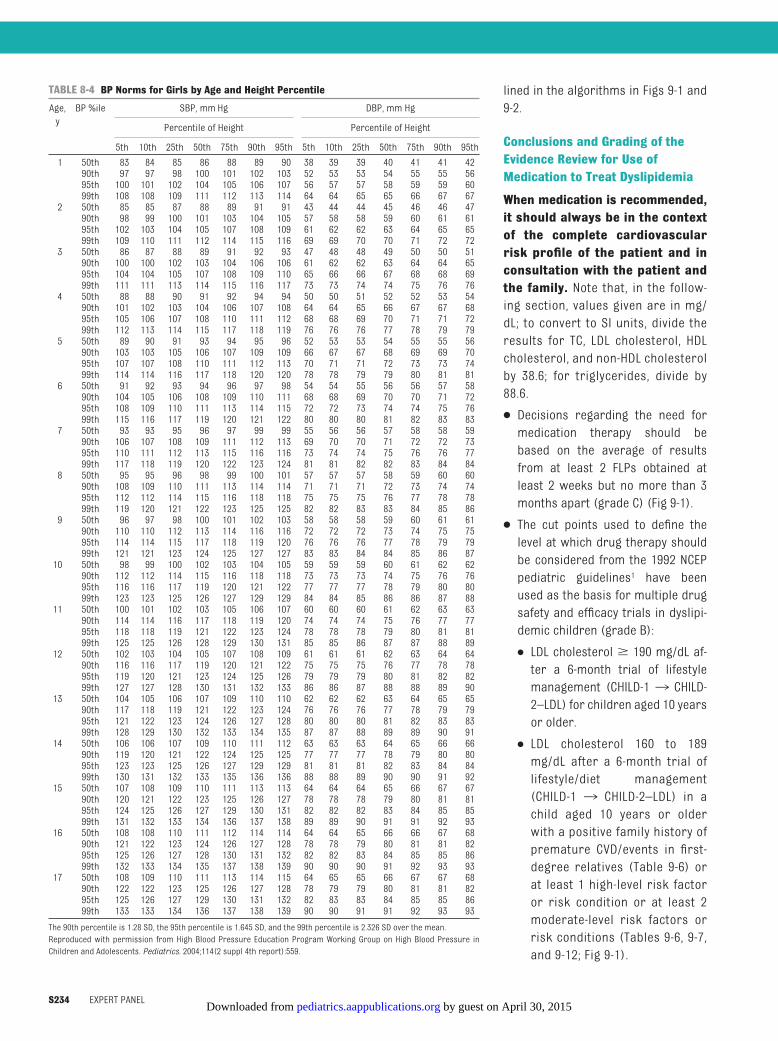
lined in the algorithms in Figs 9-1 and9-2.
Conclusions and Grading of theEvidence Review for Use ofMedication to Treat Dyslipidemia
When medication is recommended,it should always be in the contextof the complete cardiovascularrisk profile of the patient and inconsultation with the patient andthe family. Note that, in the follow-ing section, values given are in mg/dL; to convert to SI units, divide theresults for TC, LDL cholesterol, HDLcholesterol, and non-HDL cholesterolby 38.6; for triglycerides, divide by88.6.
● Decisions regarding the need formedication therapy should bebased on the average of resultsfrom at least 2 FLPs obtained atleast 2 weeks but no more than 3months apart (grade C) (Fig 9-1).
● The cut points used to define thelevel at which drug therapy shouldbe considered from the 1992 NCEPpediatric guidelines1 have beenused as the basis for multiple drugsafety and efficacy trials in dyslipi-demic children (grade B):
● LDL cholesterol � 190 mg/dL af-ter a 6-month trial of lifestylemanagement (CHILD-1 ¡ CHILD-2–LDL) for children aged 10 yearsor older.
● LDL cholesterol 160 to 189mg/dL after a 6-month trial oflifestyle/diet management(CHILD-1 ¡ CHILD-2–LDL) in achild aged 10 years or olderwith a positive family history ofpremature CVD/events in first-degree relatives (Table 9-6) orat least 1 high-level risk factoror risk condition or at least 2moderate-level risk factors orrisk conditions (Tables 9-6, 9-7,and 9-12; Fig 9-1).
TABLE 8-4 BP Norms for Girls by Age and Height Percentile
Age,yBP %ile SBP, mm Hg DBP, mm Hg
Percentile of Height Percentile of Height
5th 10th 25th 50th 75th 90th 95th 5th 10th 25th 50th 75th 90th 95th
1 50th 83 84 85 86 88 89 90 38 39 39 40 41 41 4290th 97 97 98 100 101 102 103 52 53 53 54 55 55 5695th 100 101 102 104 105 106 107 56 57 57 58 59 59 6099th 108 108 109 111 112 113 114 64 64 65 65 66 67 67
2 50th 85 85 87 88 89 91 91 43 44 44 45 46 46 4790th 98 99 100 101 103 104 105 57 58 58 59 60 61 6195th 102 103 104 105 107 108 109 61 62 62 63 64 65 6599th 109 110 111 112 114 115 116 69 69 70 70 71 72 72
3 50th 86 87 88 89 91 92 93 47 48 48 49 50 50 5190th 100 100 102 103 104 106 106 61 62 62 63 64 64 6595th 104 104 105 107 108 109 110 65 66 66 67 68 68 6999th 111 111 113 114 115 116 117 73 73 74 74 75 76 76
4 50th 88 88 90 91 92 94 94 50 50 51 52 52 53 5490th 101 102 103 104 106 107 108 64 64 65 66 67 67 6895th 105 106 107 108 110 111 112 68 68 69 70 71 71 7299th 112 113 114 115 117 118 119 76 76 76 77 78 79 79
5 50th 89 90 91 93 94 95 96 52 53 53 54 55 55 5690th 103 103 105 106 107 109 109 66 67 67 68 69 69 7095th 107 107 108 110 111 112 113 70 71 71 72 73 73 7499th 114 114 116 117 118 120 120 78 78 79 79 80 81 81
6 50th 91 92 93 94 96 97 98 54 54 55 56 56 57 5890th 104 105 106 108 109 110 111 68 68 69 70 70 71 7295th 108 109 110 111 113 114 115 72 72 73 74 74 75 7699th 115 116 117 119 120 121 122 80 80 80 81 82 83 83
7 50th 93 93 95 96 97 99 99 55 56 56 57 58 58 5990th 106 107 108 109 111 112 113 69 70 70 71 72 72 7395th 110 111 112 113 115 116 116 73 74 74 75 76 76 7799th 117 118 119 120 122 123 124 81 81 82 82 83 84 84
8 50th 95 95 96 98 99 100 101 57 57 57 58 59 60 6090th 108 109 110 111 113 114 114 71 71 71 72 73 74 7495th 112 112 114 115 116 118 118 75 75 75 76 77 78 7899th 119 120 121 122 123 125 125 82 82 83 83 84 85 86
9 50th 96 97 98 100 101 102 103 58 58 58 59 60 61 6190th 110 110 112 113 114 116 116 72 72 72 73 74 75 7595th 114 114 115 117 118 119 120 76 76 76 77 78 79 7999th 121 121 123 124 125 127 127 83 83 84 84 85 86 87
10 50th 98 99 100 102 103 104 105 59 59 59 60 61 62 6290th 112 112 114 115 116 118 118 73 73 73 74 75 76 7695th 116 116 117 119 120 121 122 77 77 77 78 79 80 8099th 123 123 125 126 127 129 129 84 84 85 86 86 87 88
11 50th 100 101 102 103 105 106 107 60 60 60 61 62 63 6390th 114 114 116 117 118 119 120 74 74 74 75 76 77 7795th 118 118 119 121 122 123 124 78 78 78 79 80 81 8199th 125 125 126 128 129 130 131 85 85 86 87 87 88 89
12 50th 102 103 104 105 107 108 109 61 61 61 62 63 64 6490th 116 116 117 119 120 121 122 75 75 75 76 77 78 7895th 119 120 121 123 124 125 126 79 79 79 80 81 82 8299th 127 127 128 130 131 132 133 86 86 87 88 88 89 90
13 50th 104 105 106 107 109 110 110 62 62 62 63 64 65 6590th 117 118 119 121 122 123 124 76 76 76 77 78 79 7995th 121 122 123 124 126 127 128 80 80 80 81 82 83 8399th 128 129 130 132 133 134 135 87 87 88 89 89 90 91
14 50th 106 106 107 109 110 111 112 63 63 63 64 65 66 6690th 119 120 121 122 124 125 125 77 77 77 78 79 80 8095th 123 123 125 126 127 129 129 81 81 81 82 83 84 8499th 130 131 132 133 135 136 136 88 88 89 90 90 91 92
15 50th 107 108 109 110 111 113 113 64 64 64 65 66 67 6790th 120 121 122 123 125 126 127 78 78 78 79 80 81 8195th 124 125 126 127 129 130 131 82 82 82 83 84 85 8599th 131 132 133 134 136 137 138 89 89 90 91 91 92 93
16 50th 108 108 110 111 112 114 114 64 64 65 66 66 67 6890th 121 122 123 124 126 127 128 78 78 79 80 81 81 8295th 125 126 127 128 130 131 132 82 82 83 84 85 85 8699th 132 133 134 135 137 138 139 90 90 90 91 92 93 93
17 50th 108 109 110 111 113 114 115 64 65 65 66 67 67 6890th 122 122 123 125 126 127 128 78 79 79 80 81 81 8295th 125 126 127 129 130 131 132 82 83 83 84 85 85 8699th 133 133 134 136 137 138 139 90 90 91 91 92 93 93
The 90th percentile is 1.28 SD, the 95th percentile is 1.645 SD, and the 99th percentile is 2.326 SD over the mean.Reproduced with permission from High Blood Pressure Education Program Working Group on High Blood Pressure inChildren and Adolescents. Pediatrics. 2004;114(2 suppl 4th report):559.
S234 EXPERT PANEL by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

TABLE 8-5 Antihypertensive Medications With Pediatric Experience
Class Drug Initial Dosea Maximal Dose DosingInterval
Evidenceb FDAc Commentsd
ACE inhibitors Benazepril 0.2 mg/kg per d up to10 mg/d
0.6 mg/kg per d upto 40 mg/d
QD RCT Yes 1. All ACE inhibitors are contraindicatedin pregnancy; women of childbearingage should use reliable contraception
Captopril 0.3–0.5 mg/kg perdose (�12 mo)
6 mg/kg per d TID RCT, CS No 2. Check serum potassium and creatinineperiodically to monitor forhyperkalemia and azotemia3. Cough and angioedema are reportedlyless common with newer members ofthis class than with captopril
Fosinoprile Children�50 kg:5–10 mg/d
40 mg/d QD RCT Yes 4. Benazepril, enalapril, and lisinoprillabels contain information on thepreparation of a suspension; captoprilmay also be compounded into asuspension
Lisinoprile 0.07 mg/kg per d upto 5 mg/d
0.6 mg/kg per d upto 40 mg/d
QD RCT Yes 5. FDA approval for ACE inhibitors withpediatric labeling is limited to children�6 y of age and to children withcreatinine clearance rate of�30 mL/min per 1.73 m2
Quinapril 5–10 mg/d 80 mg/d QD RCT, EO No 6. Initial dose of fosinopril of 0.1 mg/kgper d may be effective, although blackpatients might require a higher dose
ARBs Irbesartan 6–12 y: 75–150 mg/d;�13 y: 150–300mg/d
300 mg/d QD CS Yes 1. All ARBs are contraindicated inpregnancy; women of childbearing ageshould use reliable contraception
Losartane 0.7 mg/kg per d up to50 mg/d
1.4 mg/kg per d upto 100 mg/d
QD–BID RCT Yes 2. Check serum potassium and creatininelevels periodically to monitor forhyperkalemia and azotemia
Valsartane 5–10 mg/d; 0.4 mg/kgper d
40–80 mg/d; 3.4mg/kg per d
QD RCT No 3. Losartan label contains information onthe preparation of a suspension4. FDA approval for ARBs is limited tochildren�6 y of age and to childrenwith creatinine clearance rate of�30mL/min per 1.73 m2
�- and�-antagonist
Labetalol 1–3 mg/kg per d 10–12 mg/kg per dup to 1200 mg/d
BID CS, EO No 1. Asthma and overt heart failure arerelative contraindications2. Heart rate is dose-limiting3. May impair athletic performance inathletes4. Should not be used in insulin-dependent diabetic patients
�-antagonists Atenolol 0.5–1 mg/kg per d 2 mg/kg per d upto 100 mg/d
QD–BID CS No 1. Noncardioselective agents(propranolol) are contraindicated inasthma and heart failure
Bisoprolol/hydrochlorothiazide
2.5–6.25 mg/d 10/6.25 mg/d QD RCT No 2. Heart rate is dose-limiting
Metoprolole Children�6 y: 1 mg/kg per d (12.5–50mg/d)
2 mg/kg per d upto 200 mg/d
BID CS Yesf 3. May impair athletic performance inathletes
Propranolol 1–2 mg/kg per d 4 mg/kg per d upto 640 mg/d
BID–TID RCT, EO Yes 4. Should not be used in insulin-dependent diabetic patients5. A sustained-release, once-dailyformulation of propranolol is available
Calcium-channelblockers
Amlodipinee Children 6–17 y: 2.5mg/d
5 mg/d QD RCT Yes 1. Amlodipine and isradipine can becompounded into stableextemporaneous suspensions
Felodipine 2.5 mg/d 10 mg/d QD RCT, EO No 2. Felodipine and extended-releasenifedipine tablets must be swallowedwhole
SUPPLEMENT ARTICLES
PEDIATRICS Volume 128, Supplement 5, December 2011 S235 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
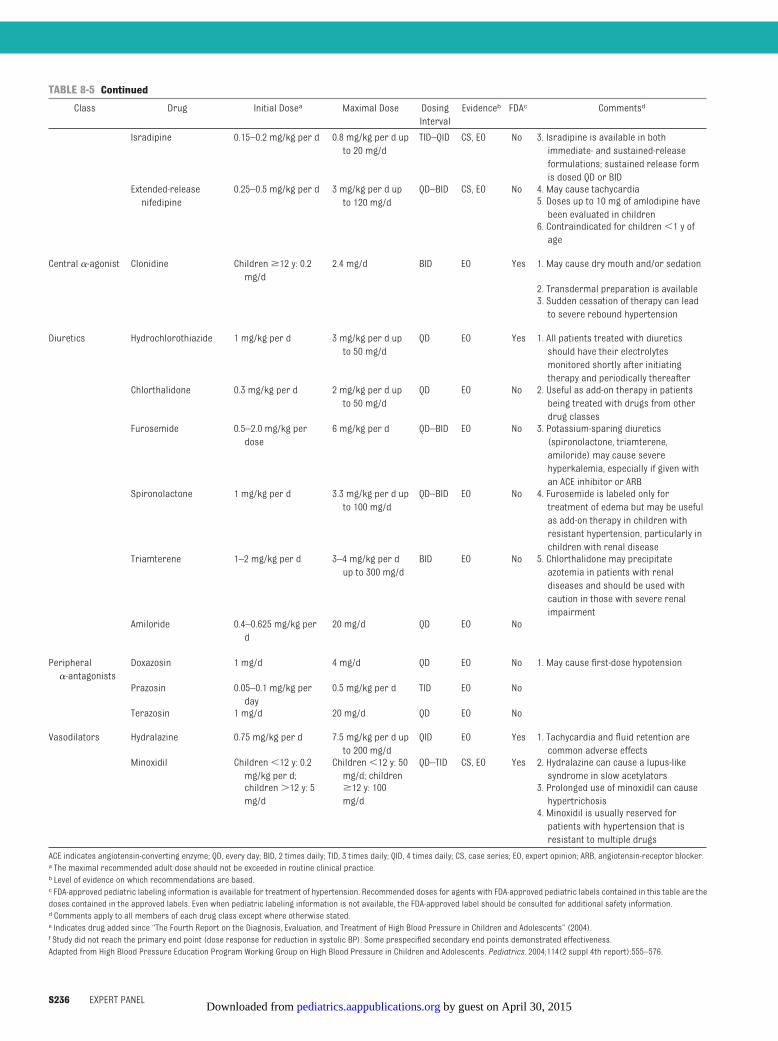
TABLE 8-5 Continued
Class Drug Initial Dosea Maximal Dose DosingInterval
Evidenceb FDAc Commentsd
Isradipine 0.15–0.2 mg/kg per d 0.8 mg/kg per d upto 20 mg/d
TID–QID CS, EO No 3. Isradipine is available in bothimmediate- and sustained-releaseformulations; sustained release formis dosed QD or BID
Extended-releasenifedipine
0.25–0.5 mg/kg per d 3 mg/kg per d upto 120 mg/d
QD–BID CS, EO No 4. May cause tachycardia5. Doses up to 10 mg of amlodipine havebeen evaluated in children6. Contraindicated for children�1 y ofage
Central �-agonist Clonidine Children�12 y: 0.2mg/d
2.4 mg/d BID EO Yes 1. May cause dry mouth and/or sedation
2. Transdermal preparation is available3. Sudden cessation of therapy can leadto severe rebound hypertension
Diuretics Hydrochlorothiazide 1 mg/kg per d 3 mg/kg per d upto 50 mg/d
QD EO Yes 1. All patients treated with diureticsshould have their electrolytesmonitored shortly after initiatingtherapy and periodically thereafter
Chlorthalidone 0.3 mg/kg per d 2 mg/kg per d upto 50 mg/d
QD EO No 2. Useful as add-on therapy in patientsbeing treated with drugs from otherdrug classes
Furosemide 0.5–2.0 mg/kg perdose
6 mg/kg per d QD–BID EO No 3. Potassium-sparing diuretics(spironolactone, triamterene,amiloride) may cause severehyperkalemia, especially if given withan ACE inhibitor or ARB
Spironolactone 1 mg/kg per d 3.3 mg/kg per d upto 100 mg/d
QD–BID EO No 4. Furosemide is labeled only fortreatment of edema but may be usefulas add-on therapy in children withresistant hypertension, particularly inchildren with renal disease
Triamterene 1–2 mg/kg per d 3–4 mg/kg per dup to 300 mg/d
BID EO No 5. Chlorthalidone may precipitateazotemia in patients with renaldiseases and should be used withcaution in those with severe renalimpairment
Amiloride 0.4–0.625 mg/kg perd
20 mg/d QD EO No
Peripheral�-antagonists
Doxazosin 1 mg/d 4 mg/d QD EO No 1. May cause first-dose hypotension
Prazosin 0.05–0.1 mg/kg perday
0.5 mg/kg per d TID EO No
Terazosin 1 mg/d 20 mg/d QD EO No
Vasodilators Hydralazine 0.75 mg/kg per d 7.5 mg/kg per d upto 200 mg/d
QID EO Yes 1. Tachycardia and fluid retention arecommon adverse effects
Minoxidil Children�12 y: 0.2mg/kg per d;
Children�12 y: 50mg/d; children
QD–TID CS, EO Yes 2. Hydralazine can cause a lupus-likesyndrome in slow acetylators
children�12 y: 5mg/d
�12 y: 100mg/d
3. Prolonged use of minoxidil can causehypertrichosis4. Minoxidil is usually reserved forpatients with hypertension that isresistant to multiple drugs
ACE indicates angiotensin-converting enzyme; QD, every day; BID, 2 times daily; TID, 3 times daily; QID, 4 times daily; CS, case series; EO, expert opinion; ARB, angiotensin-receptor blocker.a The maximal recommended adult dose should not be exceeded in routine clinical practice.b Level of evidence on which recommendations are based.c FDA-approved pediatric labeling information is available for treatment of hypertension. Recommended doses for agents with FDA-approved pediatric labels contained in this table are thedoses contained in the approved labels. Even when pediatric labeling information is not available, the FDA-approved label should be consulted for additional safety information.d Comments apply to all members of each drug class except where otherwise stated.e Indicates drug added since “The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents” (2004).f Study did not reach the primary end point (dose response for reduction in systolic BP). Some prespecified secondary end points demonstrated effectiveness.Adapted from High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. Pediatrics. 2004;114(2 suppl 4th report):555–576.
S236 EXPERT PANEL by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

● LDL cholesterol 130 to 190mg/dL ina child aged 10 years or older witha negative family history of prema-ture CVD in first-degree relativesand no high- ormoderate-level riskfactor or risk condition: manage-ment should continue to focus onlifestyle changes (CHILD-1¡CHILD-2–LDL) based on lipid-profile find-ings (Fig 9-1) plus weight manage-ment if the BMI is at the �85thpercentile.
● The goal of LDL-lowering therapyin childhood and adolescence isto decrease the LDL cholesterollevel to the �95th percentile(�130 mg/dL).
● Children with homozygous familialhypercholesterolemia and extremely
elevated LDL cholesterol levels (�500mg/dL) have undergone effective LDL-lowering therapy with biweekly LDLapheresis under the care of lipid spe-cialists in academic medical centers(grade C).
● Multiple cohort studies have foundthat the benefits of LDL-loweringtherapy in children at high risk foraccelerated atherosclerosis (suchas those with chronic kidney dis-ease, T1DM or T2DM, Kawasaki dis-ease with coronary aneurysms,or post–cardiac transplantation)should be considered for initiationof medication therapy (grade C)(see “DM and Other Conditions Pre-disposing to the Development of Ac-celerated Atherosclerosis”).
● Bile acid sequestrants are medica-tions that bind bile salts within theintestinal lumen and prevent theirenterohepatic reuptake in the ter-minal ileum, which results in a de-pletion of bile salts in the liver andsignals for increased production.Because bile salts are synthesizedfrom intracellular cholesterol in theliver, the intracellular pool of cho-lesterol becomes depleted, whichsignals increased production of LDL
TABLE 9-1 Acceptable, Borderline-High, and High Plasma Lipid, Lipoprotein, andApolipoprotein Concentrations for Children and Adolescents
Category Low, mg/dLa Acceptable, mg/dL Borderline-High, mg/dL High, mg/dLa
TC — �170 170–199 �200LDL cholesterol — �110 110–129 �130Non-HDL cholesterol — �120 120–144 �145Apolipoprotein B — �90 90–109 �110Triglycerides0–9 y — �75 75–99 �10010–19 y — �90 90–129 �130HDL cholesterol �40 �45 40–45 —Apolipoprotein A-1 �115 �120 115–120 —
Values for plasma lipid and lipoprotein levels are from the NCEP Expert Panel on Cholesterol Levels in Children. Non-HDLcholesterol values from the Bogalusa Heart Study are equivalent to the NCEP Pediatric Panel cut points for LDL cholesterol.Values for plasma apolipoprotein B and apolipoprotein A-1 are from the National Health and Nutrition Examination SurveyIII. Note that values shown are in mg/dL; to convert to SI units, divide the results for TC, LDL cholesterol, HDL cholesterol, andnon-HDL cholesterol by 38.6; for triglycerides, divide by 88.6.a Low cut points for HDL cholesterol and apolipoprotein A-1 represent approximately the 10th percentile. The cut points forhigh and borderline-high represent approximately the 95th and 75th percentiles, respectively.
TABLE 9-2 Recommended Cut Points for Lipid and Lipoprotein Levels in Young Adults
Category Low, mg/dL Borderline-Low,mg/dL
Acceptable,mg/dL
Borderline-High,mg/dL
High, mg/dL
TC — — �190 190–224 �225LDL cholesterol — — �120 120–159 �160Non-HDL cholesterol — — �150 150–189 �190Triglycerides — — �115 115–149 �150HDL cholesterol �40 40–44 �45 — —
Values provided are from the Lipid Research Clinics Prevalence Study. The cut points for TC, LDL cholesterol, and non-HDLcholesterol represent the 95th percentile for 20- to 24-year-old subjects and are not identical with the cut points used in themost recent NHLBI adult guidelines, Adult Treatment Panel III (“Third Report of the Expert Panel on Detection, Evaluation, andTreatment of High Blood Cholesterol in Adults”), which are derived from combined data on adults of all ages. The age-specificcut points given here are provided for pediatric care providers to use in managing this young adult age group. For TC, LDLcholesterol, and non-HDL cholesterol, borderline-high values are between the 75th and 94th percentiles, whereas accept-able value are at the �75th percentile. The high triglyceride cut point represents approximately the 90th percentile;borderline-high values are between the 75th and 89th percentiles, and acceptable values are at the�75th percentile. Thelow HDL cholesterol cut point represents approximately the 25th percentile; borderline-low values are between the 26th and50th percentiles, and acceptable values are at the�50th percentile.
TABLE 9-3 Causes of SecondaryDyslipidemia
ExogenousAlcoholDrug therapy: corticosteroidsIsoretinoin�-blockersSome oral contraceptivesSelect chemotherapeutic agentsSelect antiretroviral agents
Endocrine/metabolicHypothyroidism/hypopituitarismT1DM and T2DMPregnancyPolycystic ovary syndromeLipodystrophyAcute intermittent porphyriaRenalChronic renal diseaseHemolytic uremic syndromeNephrotic syndromeInfectiousAcute viral/bacterial infectiona
HIVHepatitisHepaticObstructive liver disease/cholestatic conditionsBiliary cirrhosisAlagille syndromeInflammatory diseaseSystemic lupus erythematosisJuvenile rheumatoid arthritisStorage diseaseGlycogen-storage diseaseGaucher diseaseCystine-storage diseaseJuvenile Tay-Sachs diseaseNiemann-Pick diseaseOtherKawasaki diseaseAnorexia nervosaPost–solid organ transplantationChildhood cancer survivorProgeriaIdiopathic hypercalcemiaKlinefelter syndromeWerner syndrome
a Delay measurement until�3 weeks after infection.
SUPPLEMENT ARTICLES
PEDIATRICS Volume 128, Supplement 5, December 2011 S237 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

receptors and increased clearanceof circulating LDL cholesterol to re-plenish the intracellular cholesterolpool for increased production ofbile salts. Studies of bile acid se-questrants in children and adoles-cents aged 6 to 18 years with LDLcholesterol levels from 131 to 190mg/dL have resulted in TC reductionof 7% to 17% and reduction of LDLcholesterol of 10% to 20%, some-times with a modest elevation in tri-glyceride level. Bile acid seques-trants commonly cause adversegastrointestinal effects that can sig-nificantly affect compliance. How-ever, they are safe and moderatelyeffective (grade A).
● Statin medications inhibit hydroxy-methylglutaryl coenzyme A reduc-tase, which is a rate-limiting enzymein the endogenous cholesterol-synthesis pathway. This inhibition re-sults in a decrease in the intracellularpool of cholesterol, which signals up-regulation of LDL receptors and in-creased clearance of circulating LDLcholesterol. As a group, statins havebeen shown to reduce LDL cholesterolin children and adolescents withmarked LDL cholesterol elevation or
familial hypercholesterolemia (de-fined as elevated LDL cholesterol inthe child in conjunction with a familyhistory of elevated LDL cholesteroland/or atherosclerosis or CAD) whenused from 8 weeks to 2 years for chil-dren aged 8 to 18 years. The lower LDLcholesterol level for eligibility into thestatin trials was �190 or �160mg/dLwith�2 additional risk factorsafter a trial period on diet. Trial sub-jects were monitored carefullythroughout treatment; adverse ef-fects on growth, development, or sex-ual maturation were not seen, andadverse-event profiles and efficacywere similar to those in studies ofadults (grade A).
● Adverse effects from statins arerare at standard doses but includemyopathy and hepatic enzyme eleva-tion. In ameta-analysis of statin use inchildren, evidence of hepatic enzymeelevation and muscle toxicity did notdiffer between the statin and placebogroups. Routinemonitoringof hepaticenzymes and clinical assessment formuscle toxicity are strongly recom-mended for children and adolescentsonstatin therapy (Table 9-12). The riskof adverse events increases with use
of higher doses and interactingdrugs; the latter occurs primarilywith drugs that are metabolized bythe cytochrome P-450 system, whichis the primary mode of metabolismfor the majority of statins. Drugs thatpotentially interact with statins in-clude fibrates, azole antifungalagents, macrolide antibiotics, antiar-rhythmic agents, and protease inhibi-tors (grade A).
● Bile acid–binding sequestrants maybe used in combination with a statinfor patients who fail to meet LDL cho-lesterol target levels with either med-ication alone. One pediatric study as-sessed this combinationand foundnoincrease in adverse effects. The effi-cacyof the2agents togetherseems tobe additive (grade B).
● There is limited published experiencein children of use of niacin and fi-brates, which have been useful intreating adult patientswith combineddyslipidemias. Efficacy and safetydataare limited, andnodataareavail-able regardingnewer formulations. Inadults, cholesterol absorption inhibi-tors have been advocated as an ad-junct to statin therapy for patientswho do not reach LDL cholesteroltherapeutic targets. Because their ac-tion is independent of and comple-mentary to that of statins, the LDL cho-lesterol–lowering effect is additive.No pediatric studies of monotherapywithcholesterol absorption inhibitorshad been published during the timeperiod for this evidence review. Theuseofniacin, fibrates, andcholesterolabsorption inhibitors should be insti-tuted only in consultation with a lipidspecialist (grade C).
● Medication therapy is rarely neededfor children with elevated triglycer-ide levels that respond well toweight loss and lifestyle changes(grade B) (Fig 9-2; Table 9-8). Whentriglyceride levels exceed 500 mg/dL, patients are at risk for pancre-
TABLE 9-4 Summary of Major Lipid Disorders in Children and Adolescents
Primary Lipid Disorders Lipid/Lipoprotein Abnormality
Familial hypercholesterolemiaHomozygous 11 LDL cholesterolHeterozygous 1 LDL cholesterola
Familial defective apolipoprotein B 1 LDL cholesterolFamilial combined hyperlipidemiaa
Type IIa 1 LDL cholesterolType IV 1 VLDL cholesterol,1 triglyceridesType IIb 1 LDL cholesterol,1 VLDL cholesterol,1
triglyceridesTypes IIb and IV 2 HDL cholesterol (often)
Polygenic hypercholesterolemia 1 LDL cholesterolFamilial hypertriglyceridemia (200–1000 mg/dL) 1 VLDL cholesterol,1 triglyceridesSevere hypertriglyceridemia (�1000 mg/dL) 1 chylomicrons,1 VLDL cholesterol,11
triglyceridesFamilial hypoalphalipoproteinemia 2 HDL cholesterolDysbetalipoproteinemia (TC: 250–500 mg/dL;triglycerides: 250–600 mg/dL)
1 IDL cholesterol,1 chylomicron remnants
1 indicates increased;2, decreased; IDL indicates intermediate-density lipoprotein; VLDL, very low density lipoprotein.a These are the 2 lipid and lipoprotein disorders seen most frequently in childhood and adolescence; familial combinedhyperlipidemia most often manifests with obesity.
S238 EXPERT PANEL by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

TABLE 9-5 Evidence-Based Recommendations for Lipid AssessmentBirth to 2 y No lipid screening Grade C
Recommend2 to 8 y No routine lipid screening Grade B
RecommendMeasure fasting lipid profile twice,a average results if:Parent, grandparent, aunt/uncle, or sibling with Grade BMI, angina, stroke, CABG/stent/angioplasty at�55 y in males,�65 y in females Strongly recommendParent with TC� 240 mg/dL or known dyslipidemia Grade BParent with TC� 240 mg/dL or known dyslipidemia Strongly recommendChild has diabetes, hypertension, BMI� 95th percentile or smokes cigarettes Grade B
Strongly recommendChild has a moderate- or high-risk medical condition (Table 5-2) Grade B
Strongly recommend
Use Table 9-1 for interpretation of results, algorithms in Figs 9-1 and 9-2 for management.
9 to 11 y Universal screening Grade BStrongly recommend
Non-FLP: Calculate non–HDL cholesterol:Non–HDL cholesterol � TC � HDL cholesterolIf non-HDL� 145 mg/dL� HDL� 40 mg/dLb:Obtain FLP twice,a average resultsORFLP:If LDL cholesterol� 130 mg/dL� non-HDL cholesterol� 145 mg/dL� HDL cholesterol� 40 mg/dL� triglycerides� 100 mg/dLif�10 y,�130 mg/dL if�10 y:
Repeat FLP, average resultsUse Table 9-1 for interpretation of results, algorithms in Figs 9-1 and 9-2 for management.
12 to 16 y No routine screeningc Grade BRecommend
Measure FLP twice,a average results, if new knowledge of:Parent, grandparent with MI, angina, stroke, CABG/stent/angioplasty, sudden death at�55 y in male,�65 y in female Grade B
Strongly recommendParent with TC� 240 mg/dL or known dyslipidemia Grade B
Strongly recommendPatient has diabetes, hypertension, BMI� 85th percentile or smokes cigarettes Grade B
Strongly recommendPatient has a moderate- or high-risk medical condition (Table 5-2) Grade B
Strongly recommend
Use Table 9-1 for interpretation of results, algorithms in Figs 9-1 and 9-2 for management.
17 to 21 y Universal screening once in this time period: Grade BRecommend
Non-FLP: Calculate non–HDL cholesterol:Non–HDL cholesterol � TC � HDL cholesterol*17–19 y:If non–HDL cholesterol�145 mg/dL� HDL cholesterol� 40 mg/dLb
Measure FLP twice,a average resultsORFLP:If LDL cholesterol� 130 mg/dL� non–HDL cholesterol� 145 mg/dL� HDL cholesterol� 40 mg/dL� triglycerides� 130 mg/dLRepeat FLP, average results
Use Table 9-1 for interpretation of results, algorithms in Figs 9-1 and 9-2 for management.
20–21 y:Non–HDL cholesterol� 190 mg/dL� HDL cholesterol� 40 mg/dLMeasure FLP twice, average resultsORFLP:If LDL cholesterol� 160 mg/dL� non–HDL cholesterol� 190 mg/dL� HDL cholesterol� 40 mg/dL� triglycerides� 150 mg/dLRepeat FLP, average results
Use Table 9-2 for interpretation of results, Adult Treatment Panel (ATP III) algorithm for management.
Grades reflect the findings of the evidence review, recommendation levels reflect the consensus opinion of the expert panel. Note that the values given are in mg/dL. To convert to SI units,divide the results for TC, LDL cholesterol, HDL cholesterol, and non-HDL cholesterol by 38.6; for triglycerides, divide by 88.6. MI indicates myocardial infarction; CABG, coronary artery bypassgraft; ATP III, Adult Treatment Panel III.a Interval between FLP measurements: after 2 weeks but within 3 months.b Use Table 9-1 for interpretation of results; use lipid algorithms in Figs 9-1 and 9.2 for management of results.c Disregard triglyceride and LDL cholesterol levels in nonfasting sample.d Lipid screening is not recommended for those aged 12 to 16 years because of significantly decreased sensitivity and specificity for predicting adult LDL cholesterol levels and significantlyincreased false-negative results in this age group. Selective screening is recommended for those with the clinical indications outlined.e Use Table 9-1 for interpretation of results of 7- to 19-year-olds and lipid algorithms in Figs 9-1 and 9-2 for management. Use Table 17 for interpretation of results of 20- to 21-year-olds andATP III algorithms for management.
SUPPLEMENT ARTICLES
PEDIATRICS Volume 128, Supplement 5, December 2011 S239 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

atitis and require care in consulta-tion with a lipid specialist (grade B).In adults, use of�-3 fish oil has beenshown to lower the triglyceride levelby 30% to 40% and to raise the HDLlevel by 6% to 17%. Experience withfish oil in children has been limited tosmall case series, and no safety con-cerns identified; there have been noRCTs of fish oil in children (grade D).
Age-Based Recommendations forMedication Therapy of Childrenwith Dyslipidemia
The age-specific recommendations forpharmacologic management ofdyslipidemia are summarized in Table9-9. Children Younger Than 10 Years
● Children younger than 10 yearsshould not be treated with a medica-tion unless they have a severe pri-mary hyperlipidemia or a high-riskcondition that is associated with seri-ous medical morbidity (homozygoushypercholesterolemia/LDL choles-
terol level of�400 mg/dL; primaryhypertriglyceridemia with a tri-glyceride level of �500 mg/dL; ev-ident CVD in the first 2 decades oflife; post– cardiac transplanta-tion) (grade C).
Children Aged 10 to 21 Years
● Decisions regarding the need formedication therapy should bebased on the average of resultsfrom at least 2 FLPs obtained atleast 2 weeks but no more than 3months apart (grade C) (Fig 9-1).
● Children with an average LDL cho-lesterol level of �250 mg/dL or av-erage triglyceride level of �500mg/dL should be referred directly toa lipid specialist (grade B).
● Children with lipid abnormalitiesshould have a detailed family historytaken and be assessed for causes ofhyperlipidemia, additional risk fac-tors, and risk conditions (grade C)(Tables 9-3, 9-6, and 9-7).
● Children with lipid abnormalities(other than an LDL cholesterol levelof �250 mg/dL or triglyceride levelof�500 mg/dL) should be managedinitially for 3 to 6 months with dietchanges (CHILD-1¡ CHILD-2–LDL orCHILD-2–TG) (Table 9-8) on the basisof specific lipid profile findings (Figs9-1 and 9-2); if the BMI is at the�85th percentile, add increasedphysical activity, reduced screentime, and calorie restriction. As-sessment for associated secondarycauses (Table 9-3), additional riskfactors, or high-risk conditions (Ta-bles 9-6 and 9-7) is recommended.Children at high risk who are un-likely to achieve lipid targets withthis strategy alone (severe primarydyslipidemia, post–cardiac trans-plantation) should concomitantly beconsidered for initiation of medica-tion therapy (grade C) (see “DM andOther Conditions Predisposing tothe Development of AcceleratedAtherosclerosis”).
Treatment for children with severe el-evation of LDL cholesterol is based onassessment of lipid levels and associ-ated risk factors or risk conditions (Ta-bles 9-6 and 9-7; Figs 9-1 and 9-2):
● Children with an average LDL cho-lesterol level of�250 mg/dL shouldbe referred directly to a lipid spe-cialist (grade B).
● If the LDL cholesterol level remains�190 mg/dL after a 6-month trial oflifestyle/diet management (CHILD-1¡ CHILD-2–LDL) for children aged10 years and older, statin therapyshould be considered (grade A) (Fig9-1; Table 9-11 and 9-12).
● If the LDL cholesterol level remains�130 to�190mg/dL in a child aged10 years or older with a negativefamily history of premature CVD infirst-degree relatives and no high-or moderate-level risk factor or riskcondition (Tables 9-6 and 9-7), man-
TABLE 9-6 Risk-Factor Definitions for Dyslipidemia Algorithms
Positive family history: myocardial infarction, angina, coronary artery bypass graft/stent/angioplasty,sudden cardiac death in parent, grandparent, aunt, or uncle at�55 y for males,�65 y for females
High-level RFsHypertension that requires drug therapy (BP� 99th percentile� 5 mm Hg)Current cigarette smokerBMI at the�97th percentilePresence of high-risk conditions (Table 9-7)(DM is also a high-level RF, but it is classified here as a high-risk condition to correspond with AdultTreatment Panel III recommendations for adults that DM be considered a CVD equivalent.)
Moderate-level RFsHypertension that does not require drug therapyBMI at the�95th percentile,�97th percentileHDL cholesterol� 40 mg/dLPresence of moderate-risk conditions (Table 9-7)
RF indicates risk factor.
TABLE 9-7 Special Risk Conditions
High riskT1DM and T2DMChronic kidney disease/end-stage renal disease/post–renal transplantPost–orthotopic heart transplantKawasaki disease with current aneurysmsModerate riskKawasaki disease with regressed coronary aneurysmsChronic inflammatory disease (systemic lupus erythematosus, juvenile rheumatoid arthritis)HIV infectionNephrotic syndrome
S240 EXPERT PANEL by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
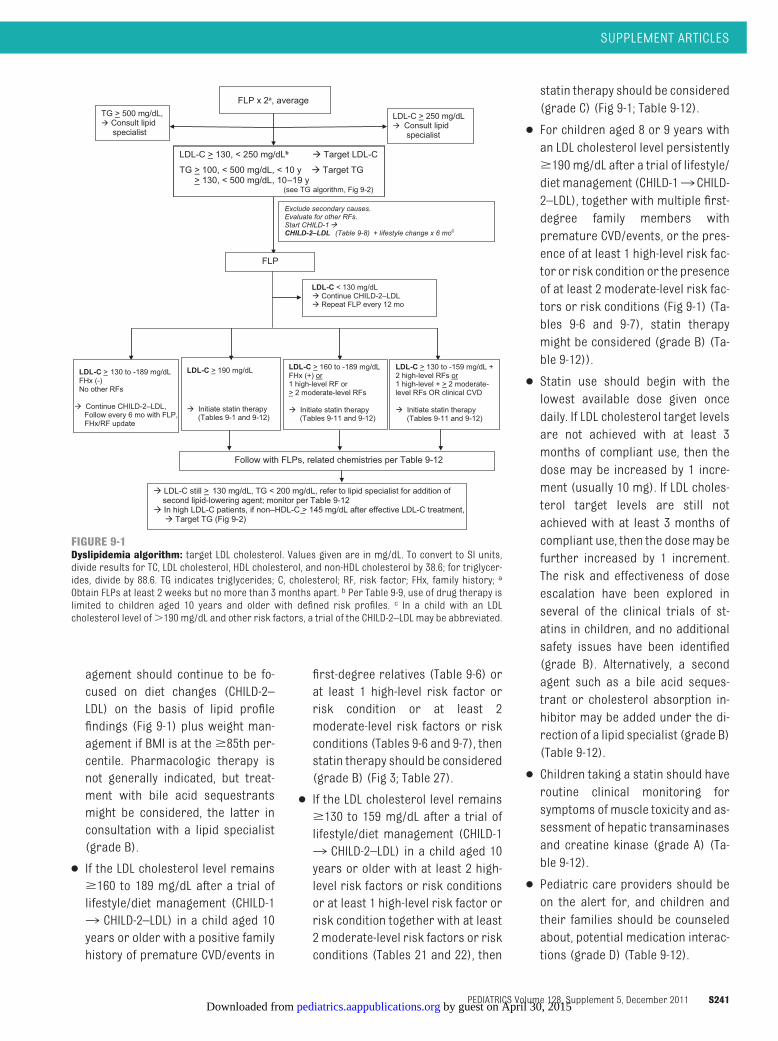
agement should continue to be fo-cused on diet changes (CHILD-2–LDL) on the basis of lipid profilefindings (Fig 9-1) plus weight man-agement if BMI is at the�85th per-centile. Pharmacologic therapy isnot generally indicated, but treat-ment with bile acid sequestrantsmight be considered, the latter inconsultation with a lipid specialist(grade B).
● If the LDL cholesterol level remains�160 to 189 mg/dL after a trial oflifestyle/diet management (CHILD-1¡ CHILD-2–LDL) in a child aged 10years or older with a positive familyhistory of premature CVD/events in
first-degree relatives (Table 9-6) orat least 1 high-level risk factor orrisk condition or at least 2moderate-level risk factors or riskconditions (Tables 9-6 and 9-7), thenstatin therapy should be considered(grade B) (Fig 3; Table 27).
● If the LDL cholesterol level remains�130 to 159 mg/dL after a trial oflifestyle/diet management (CHILD-1¡ CHILD-2–LDL) in a child aged 10years or older with at least 2 high-level risk factors or risk conditionsor at least 1 high-level risk factor orrisk condition together with at least2 moderate-level risk factors or riskconditions (Tables 21 and 22), then
statin therapy should be considered(grade C) (Fig 9-1; Table 9-12).
● For children aged 8 or 9 years withan LDL cholesterol level persistently�190 mg/dL after a trial of lifestyle/dietmanagement (CHILD-1¡ CHILD-2–LDL), together with multiple first-degree family members withpremature CVD/events, or the pres-ence of at least 1 high-level risk fac-tor or risk condition or the presenceof at least 2 moderate-level risk fac-tors or risk conditions (Fig 9-1) (Ta-bles 9-6 and 9-7), statin therapymight be considered (grade B) (Ta-ble 9-12)).
● Statin use should begin with thelowest available dose given oncedaily. If LDL cholesterol target levelsare not achieved with at least 3months of compliant use, then thedose may be increased by 1 incre-ment (usually 10 mg). If LDL choles-terol target levels are still notachieved with at least 3 months ofcompliant use, then the dosemay befurther increased by 1 increment.The risk and effectiveness of doseescalation have been explored inseveral of the clinical trials of st-atins in children, and no additionalsafety issues have been identified(grade B). Alternatively, a secondagent such as a bile acid seques-trant or cholesterol absorption in-hibitor may be added under the di-rection of a lipid specialist (grade B)(Table 9-12).
● Children taking a statin should haveroutine clinical monitoring forsymptoms of muscle toxicity and as-sessment of hepatic transaminasesand creatine kinase (grade A) (Ta-ble 9-12).
● Pediatric care providers should beon the alert for, and children andtheir families should be counseledabout, potential medication interac-tions (grade D) (Table 9-12).
LDL-C > 190 mg/dL
� Initiate statin therapy(Tables 9-1 and 9-12)
Exclude secondary causes.Evaluate for other RFs.Start CHILD-1�CHILD-2–LDL (Table 9-8) + lifestyle change x 6 moc
FLP
FLP x 2a, average
LDL-C > 130, < 250 mg/dL ** � Target LDL-C
TG > 100, < 500 mg/dL, < 10 y � Target TG> 130, < 500 mg/dL, 10-19 y
(see TG algorithm, Figure 9-2)
LDL-C > 250 mg/dL� Consult lipid
specialist
TG > 500 mg/dL,� Consult lipid
specialist
LDL-C < 130 mg/dL� Continue CHILD-2–LDL� Repeat FLP every 12 mo
LDL-C > 130 to -189 mg/dLFHx (-)No other RFs
� Continue CHILD-2–LDL,Follow every 6 mo with FLP, FHx/RF update
LDL-C > 160 to -189 mg/dLFHx (+) or1 high-level RF or> 2 moderate-level RFs
� Initiate statin therapy(Tables 9-11 and 9-12)
LDL-C > 130 to -159 mg/dL +2 high-level RFs or1 high-level + > 2 moderate-level RFs OR clinical CVD
� Initiate statin therapy(Tables 9-11 and 9-12)
Follow with FLPs, related chemistries per Table 9-12
� LDL-C still > 130 mg/dL, TG < 200 mg/dL, refer to lipid specialist for addition of second lipid-lowering agent; monitor per Table 9-12
� In high LDL-C patients, if non–HDL-C > 145 mg/dL after effective LDL-C treatment,� Target TG (Fig 9-2)
LDL-C > 130, < 250 mg/dLb � Target LDL-C
TG > 100, < 500 mg/dL, < 10 y � Target TG> 130, < 500 mg/dL, 10–19 y
(see TG algorithm, Fig 9-2)
FIGURE 9-1Dyslipidemia algorithm: target LDL cholesterol. Values given are in mg/dL. To convert to SI units,divide results for TC, LDL cholesterol, HDL cholesterol, and non-HDL cholesterol by 38.6; for triglycer-ides, divide by 88.6. TG indicates triglycerides; C, cholesterol; RF, risk factor; FHx, family history; a
Obtain FLPs at least 2 weeks but no more than 3 months apart. b Per Table 9-9, use of drug therapy islimited to children aged 10 years and older with defined risk profiles. c In a child with an LDLcholesterol level of�190 mg/dL and other risk factors, a trial of the CHILD-2–LDL may be abbreviated.
SUPPLEMENT ARTICLES
PEDIATRICS Volume 128, Supplement 5, December 2011 S241 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
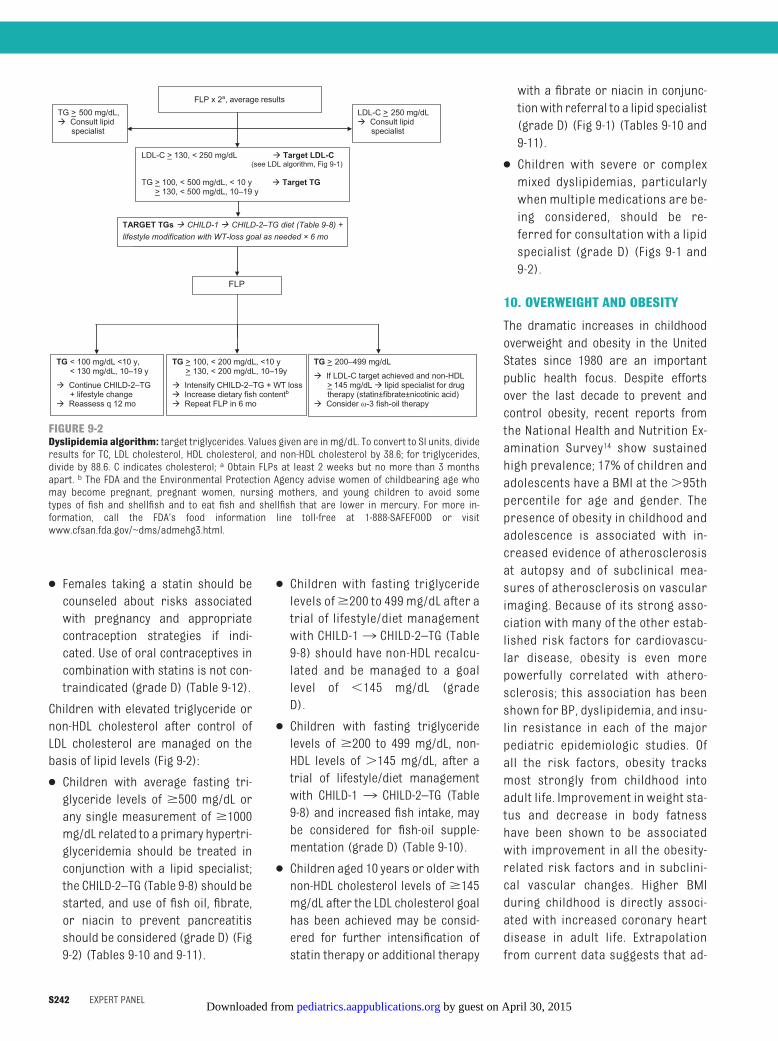
● Females taking a statin should becounseled about risks associatedwith pregnancy and appropriatecontraception strategies if indi-cated. Use of oral contraceptives incombination with statins is not con-traindicated (grade D) (Table 9-12).
Children with elevated triglyceride ornon-HDL cholesterol after control ofLDL cholesterol are managed on thebasis of lipid levels (Fig 9-2):
● Children with average fasting tri-glyceride levels of �500 mg/dL orany single measurement of �1000mg/dL related to a primary hypertri-glyceridemia should be treated inconjunction with a lipid specialist;the CHILD-2–TG (Table 9-8) should bestarted, and use of fish oil, fibrate,or niacin to prevent pancreatitisshould be considered (grade D) (Fig9-2) (Tables 9-10 and 9-11).
● Children with fasting triglyceridelevels of�200 to 499 mg/dL after atrial of lifestyle/diet managementwith CHILD-1¡ CHILD-2–TG (Table9-8) should have non-HDL recalcu-lated and be managed to a goallevel of �145 mg/dL (gradeD).
● Children with fasting triglyceridelevels of �200 to 499 mg/dL, non-HDL levels of �145 mg/dL, after atrial of lifestyle/diet managementwith CHILD-1 ¡ CHILD-2–TG (Table9-8) and increased fish intake, maybe considered for fish-oil supple-mentation (grade D) (Table 9-10).
● Children aged 10 years or older withnon-HDL cholesterol levels of �145mg/dL after the LDL cholesterol goalhas been achieved may be consid-ered for further intensification ofstatin therapy or additional therapy
with a fibrate or niacin in conjunc-tionwith referral to a lipid specialist(grade D) (Fig 9-1) (Tables 9-10 and9-11).
● Children with severe or complexmixed dyslipidemias, particularlywhen multiple medications are be-ing considered, should be re-ferred for consultation with a lipidspecialist (grade D) (Figs 9-1 and9-2).
10. OVERWEIGHT AND OBESITY
The dramatic increases in childhoodoverweight and obesity in the UnitedStates since 1980 are an importantpublic health focus. Despite effortsover the last decade to prevent andcontrol obesity, recent reports fromthe National Health and Nutrition Ex-amination Survey14 show sustainedhigh prevalence; 17% of children andadolescents have a BMI at the�95thpercentile for age and gender. Thepresence of obesity in childhood andadolescence is associated with in-creased evidence of atherosclerosisat autopsy and of subclinical mea-sures of atherosclerosis on vascularimaging. Because of its strong asso-ciation with many of the other estab-lished risk factors for cardiovascu-lar disease, obesity is even morepowerfully correlated with athero-sclerosis; this association has beenshown for BP, dyslipidemia, and insu-lin resistance in each of the majorpediatric epidemiologic studies. Ofall the risk factors, obesity tracksmost strongly from childhood intoadult life. Improvement in weight sta-tus and decrease in body fatnesshave been shown to be associatedwith improvement in all the obesity-related risk factors and in subclini-cal vascular changes. Higher BMIduring childhood is directly associ-ated with increased coronary heartdisease in adult life. Extrapolationfrom current data suggests that ad-
FLP
LDL-C > 130, < 250 mg/dL ** � Target LDL-C(see LDL algorithm, Figure 9-1)
TG > 100, < 500 mg/dL, < 10 y � Target TG > 130, < 500 mg/dL, 10-19 y
TARGET TGs --> Cardiovascular Health Integrated Lifestyle Diet (CHILD 1) � CHILD 2 TG diet (Table 9–needed × 6 months
TG < 100 mg/dL <10 y,< 130 mg/dL, 10–19 y
� Continue CHILD-2–TG+ lifestyle change
� Reassess q 12 mo
TG > 100, < 200 mg/dL, <10 y> 130, < 200 mg/dL, 10–19y
� Intensify CHILD-2–TG + WT loss� Increase dietary fish contentb� Repeat FLP in 6 mo
TG > 200–499 mg/dL
� If LDL-C target achieved and non-HDL > 145 mg/dL � lipid specialist for drugtherapy (statin±fibrate±nicotinic acid)
� Consider ω-3 fish-oil therapy
FLP x 2a, average resultsTG > 500 mg/dL,� Consult lipid
specialist
LDL-C > 250 mg/dL� Consult lipid
specialist
TARGET TGs � CHILD-1 � CHILD-2–TG diet (Table 9-8) +lifestyle modification with WT-loss goal as needed × 6 mo
LDL-C > 130, < 250 mg/dL � Target LDL-C(see LDL algorithm, Fig 9-1)
TG > 100, < 500 mg/dL, < 10 y � Target TG > 130, < 500 mg/dL, 10–19 y
FIGURE 9-2Dyslipidemia algorithm: target triglycerides. Values given are in mg/dL. To convert to SI units, divideresults for TC, LDL cholesterol, HDL cholesterol, and non-HDL cholesterol by 38.6; for triglycerides,divide by 88.6. C indicates cholesterol; a Obtain FLPs at least 2 weeks but no more than 3 monthsapart. b The FDA and the Environmental Protection Agency advise women of childbearing age whomay become pregnant, pregnant women, nursing mothers, and young children to avoid sometypes of fish and shellfish and to eat fish and shellfish that are lower in mercury. For more in-formation, call the FDA’s food information line toll-free at 1-888-SAFEFOOD or visitwww.cfsan.fda.gov/~dms/admehg3.html.
S242 EXPERT PANEL by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

olescent obesity will likely increaseadult coronary heart disease by 5%to 16% over the next 25 years with�100 000 excess cases of coronaryheart disease attributable to in-creased obesity in childhood. Theevidence review included RCTs, sys-tematic reviews, meta-analyses, andobservational studies that assessedthe prevention and treatment ofoverweight and obesity in childhoodand adolescence.
Identification of Overweight andObese Children and Adolescents
To identify overweight and obesity inchildren living in the United States, BMIpercentile distributions relative togender and age on the Centers for Dis-ease Control and Prevention (CDC)2000 growth charts15 are now the pre-ferred reference. The CDC growthcharts were not developed as a health-related standard. Instead, the growth
charts present percentiles of the BMIdistribution derived from measure-ments taken during several NationalHealth and Nutrition Examination Sur-veys as points of reference. Althoughthe chartswere published in 2000, theyinclude selected data from the 1963through 1980 surveys and, thus, arenot representative of the US popula-tion in 2000. These BMI percentilegrowth charts provide the best refer-ence data available for describing nor-mal growth in US children. They are,however, a screening tool and not aninstrument for the diagnosis of over-weight and obesity.
An expert committee jointly convenedby the American Medical Association(AMA), the CDC, and the Maternal andChild Health Bureau (MCHB) of theHealth Resources and Services Admin-istration (US Department of Health andHuman Services)16 recently recom-mended that BMI be used to assessweight-for-height relationships in chil-dren. This conclusion was reached be-cause BMI can be easily calculatedfrom height and weight, correlatesstrongly with direct measures of bodyfat (especially at higher BMI values),associates only weakly with height,and identifies those with the highestbody fat correctly with acceptable ac-curacy, particularly above the 85th BMIpercentile. Pediatric care providersneed a feasible standard for identify-ing overweight and obesity in theirpatients, because parents recognizea child’s overweight status in fewerthan half of the cases. The AMA/CDC/MCHB expert committee16 defined aBMI at the�95th percentile as obeseand a BMI between the 85th and 94thpercentiles as overweight; childrenin the latter BMI category have agreat deal of variation with respectto prediction of future risk. The ex-pert panel for these guidelines con-cluded that BMI is a sufficient mea-sure for screening children and
TABLE 9-8 Evidence-Based Recommendations for Dietary Management of Elevated LDLCholesterol, Non-HDL Cholesterol, and Triglyceride Levels
2 to 21 y Elevated LDL cholesterol: CHILD-2–LDLRefer to a registered dietitian for family medical nutrition therapy Grade B
Stronglyrecommend
25%–30% of calories from fat,�7% from saturated fat,�10%from monounsaturated fat;�200 mg/d of cholesterol;avoid trans fats as much as possible
Grade ARecommend
Supportive actions:Plant sterol esters and/or plant stanol estersa up to 2 g/d asreplacement for usual fat sources can be used after 2 y ofage in children with familial hypercholesterolemia
Plant stanol esters as part of a regular diet are marketeddirectly to the public; short-term studies have found noharmful effects in healthy children
The water-soluble fiber psyllium can be added to a low-fat, low-saturated-fat diet as cereal enriched with psyllium at adose of 6 g/d for children 2–12 y of age and 12 g/d forthose�12 y of age
As for all children, 1 h/d of moderate-to-vigorous physicalactivity and�2 h/d of sedentary screen time arerecommended.
Elevated triglycerides or non-HDL cholesterol: CHILD-2–TGRefer to a registered dietitian for family medical nutrition
therapybGrade BStronglyrecommend
25%–30% of calories from fat,�7% from saturated fat,�10%from monounsaturated fat;�200 mg/d of cholesterol;avoid trans fats as much as possible
Grade ARecommend
Decrease sugar intake Grade BRecommend
Replace simple with complex carbohydratesNo sugar-sweetened beveragesIncrease dietary fish to increase �-3 fatty acidsc Grade D
Recommend
Grades reflect the findings of the evidence review; recommendation levels reflect the consensus opinion of the expertpanel; and supportive actions represent expert consensus suggestions from the expert panel provided to supportimplementation of the recommendations (they are not graded). Values given are in mg/dL. To convert to SI units, divide theresults for TC, LDL cholesterol, HDL cholesterol, and non-HDL cholesterol by 38.6; for triglycerides, divide by 88.6.a Can be found added to some foods, such as some margarines.b If the child is obese, nutrition therapy should include calorie restriction, and increased activity (beyond that recommendedfor all children) should be prescribed. See “Overweight and Obesity” for additional age-specific recommendations.c The FDA and the Environmental Protection Agency advise women of childbearing age whomay become pregnant, pregnantwomen, nursingmothers, and young children to avoid some types of fish and shellfish and eat fish and shellfish that are lowin mercury. For more information, call the FDA’s food information line toll-free at 1-888-SAFEFOOD or visitwww.cfsan.fda.gov/~dms/admehg3.html.
SUPPLEMENT ARTICLES
PEDIATRICS Volume 128, Supplement 5, December 2011 S243 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

adolescents to identify those whoneed evaluation for cardiovascularrisk factors associated with body ad-iposity. The expert panel also con-cluded that the scientific evidencelinking elevated BMI to cardiovascu-lar risk factors and morbidity isstrong and well supported.
The expert panel therefore recom-mends that children and adolescentsaged 2 to 18 years with a BMI at the�95th percentile be described as“obese” and identified as needing as-sessment for cardiovascular risk fac-tors. For children with a BMI that fallsbetween the 85th and 95th percen-
tiles, the term “overweight” shouldbe used, and the position of thechild’s BMI on the growth chartshould be used to express concernregarding weight-for-height dispro-portion. It is important to follow thepattern of growth over time by usingthese cut points to identify children
TABLE 9-9 Evidence-Based Recommendations for Pharmacologic Treatment of Dyslipidemia
Birth to 10y
Pharmacologic treatment is limited to children with severe primary hyperlipidemia (homozygous familialhypercholesterolemia, primary hypertriglyceridemia [triglycerides� 500 mg/dL]), a high-risk condition(Tables 9-6 and 9-7), or evident cardiovascular disease, all under the care of a lipid specialist
Grade CRecommend
�10 to 21 y Detailed family history and RF assessment required before initiation of drug therapya (high- to moderate-level RFsand RCs are listed in Tables 9-6 and 9-7)
Grade CStrongly recommend
LDL cholesterolIf average LDL cholesterol� 250 mg/dLa, consult lipid specialist Grade B
Strongly recommendIf average LDL cholesterol� 130–250 mg/dL, or non-HDL� 145 mg/dL:Refer to dietitian for medical nutrition therapy with CHILD-1¡ CHILD-2–LDL (Table 9-8) for 6 mo; repeatFLP
Grade AStrongly recommend
Repeat FLPLDL cholesterol� 130 mg/dL, continue CHILD-2–LDL, reevaluate in 12 mo Grade A
Strongly recommendLDL cholesterol� 190 mg/dL,b consider initiation of statin therapy per Tables 9-11 and 9-12 Grade A
Strongly recommendLDL cholesterol� 130–189 mg/dL, negative family history, no other RF or RC, continue CHILD-2–LDL,reevaluate every 6 mo
Grade BRecommend
LDL cholesterol� 160–189 mg/dL� positive family history or�1 high-level RF/RC or�2 moderate-levelRFs/RCs, consider statin therapy per Tables 9-11 and 9-12
Grade BRecommend
LDL cholesterol� 130–159 mg/dL� �2 high-level RFs/RCs or 1 high-level� 2 moderate-level RFs/RCs,consider statin therapy per Tables 9-11 and 9-12
Grade BRecommend
Children on statin therapy should be counseled and carefully monitored per Table 9-12 Grade AStrongly recommend
�10 to 21 y Detailed family history and RF/RC assessment required before initiation of drug therapya (high- and moderate-level RFs/RCs in Tables 9-6 and 9-7c)
Grade CStrongly recommend
TriglyceridesIf average triglycerides� 500 mg/dL, consult lipid specialist Grade B
RecommendIf average triglycerides� 100 mg/dL in a child aged�10 y,�130 mg/dL in a child aged 10–19 y, or�500mg/dL:Refer to dietitian for medical nutrition therapy with CHILD-1¡ CHILD-2–TG (Table 9-8) for 6 mo Grade B
Strongly recommendRepeat FLPTriglycerides� 100 (130) mg/dL, continue CHILD-2–TG, monitor every 6–12 mo Grade B
Strongly recommendTriglycerides� 100 (130) mg/dL, reconsult dietitian for intensified CHILD-2–TG diet counseling Grade C
RecommendTriglycerides� 200–499 mg/dL, non-HDL� 145 mg/dL, consider fish oil� consult lipid specialist Grade D
RecommendNon-HDL cholesterolChildren aged�10 y with non-HDL cholesterol� 145 mg/dL after LDL cholesterol goal is achieved may beconsidered for additional treatment with statins, fibrates, or niacin in conjunction with a lipid specialistconsultation
Grade DOptional
Grades reflect the findings of the evidence review, and recommendation levels reflect the consensus opinion of the expert panel. When medication is recommended, it should always bein the context of the complete cardiovascular risk profile of the patient and in consultation with the patient and the family. Values given are in mg/dL. To convert to SI units, divide the resultsfor TC, LDL cholesterol, HDL cholesterol, and non-HDL cholesterol by 38.6; for triglycerides, divide by 88.6. RF indicates risk factor; RC, risk condition.a Consideration of drug therapy is based on the average of�2 FLPs, obtained at least 2 weeks but no more than 3 months apart.b If average LDL cholesterol� 190 mg/dL after CHILD-2–LDL and child is 8 to 9 years old with a positive family history or�1 high-level risk factor/risk condition or�2 moderate-level riskfactors/risk conditions, statin therapy may be considered.c If the child is obese, nutrition therapy should include calorie restriction and increased activity beyond that recommended for all children. See “Overweight and Obesity” for additionalage-specific recommendations.
S244 EXPERT PANEL by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
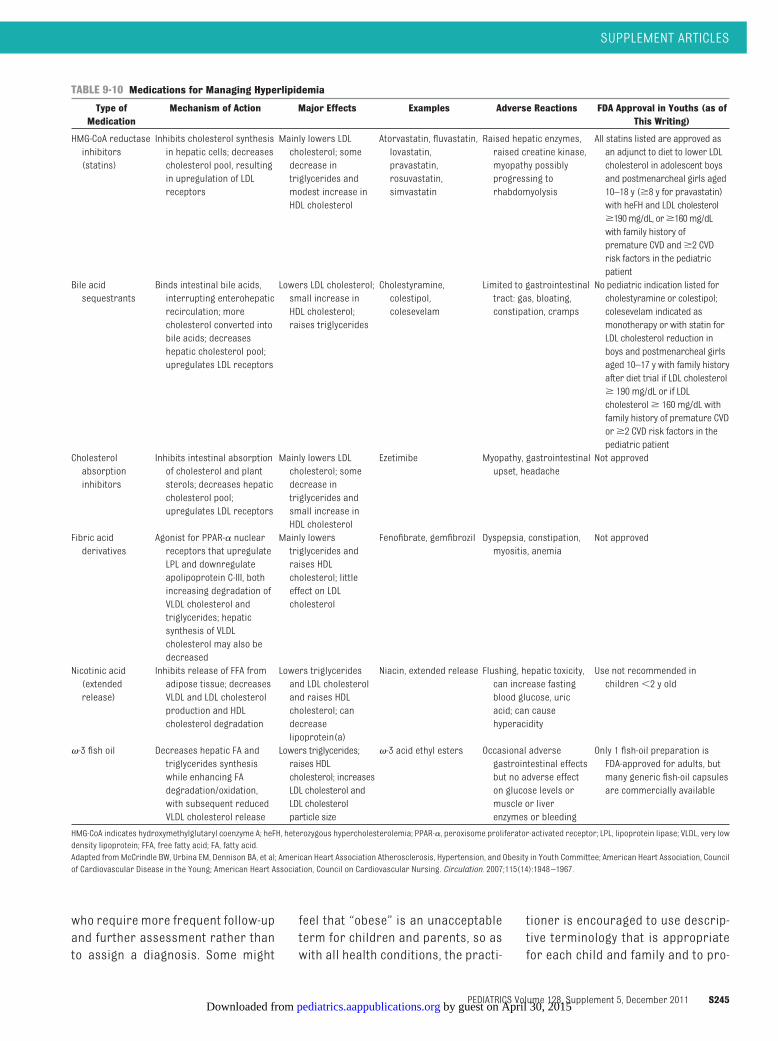
who require more frequent follow-upand further assessment rather thanto assign a diagnosis. Some might
feel that “obese” is an unacceptableterm for children and parents, so aswith all health conditions, the practi-
tioner is encouraged to use descrip-tive terminology that is appropriatefor each child and family and to pro-
TABLE 9-10 Medications for Managing Hyperlipidemia
Type ofMedication
Mechanism of Action Major Effects Examples Adverse Reactions FDA Approval in Youths (as ofThis Writing)
HMG-CoA reductaseinhibitors(statins)
Inhibits cholesterol synthesisin hepatic cells; decreasescholesterol pool, resultingin upregulation of LDLreceptors
Mainly lowers LDLcholesterol; somedecrease intriglycerides andmodest increase inHDL cholesterol
Atorvastatin, fluvastatin,lovastatin,pravastatin,rosuvastatin,simvastatin
Raised hepatic enzymes,raised creatine kinase,myopathy possiblyprogressing torhabdomyolysis
All statins listed are approved asan adjunct to diet to lower LDLcholesterol in adolescent boysand postmenarcheal girls aged10–18 y (�8 y for pravastatin)with heFH and LDL cholesterol�190mg/dL, or�160mg/dLwith family history ofpremature CVD and�2 CVDrisk factors in the pediatricpatient
Bile acidsequestrants
Binds intestinal bile acids,interrupting enterohepaticrecirculation; morecholesterol converted intobile acids; decreaseshepatic cholesterol pool;upregulates LDL receptors
Lowers LDL cholesterol;small increase inHDL cholesterol;raises triglycerides
Cholestyramine,colestipol,colesevelam
Limited to gastrointestinaltract: gas, bloating,constipation, cramps
No pediatric indication listed forcholestyramine or colestipol;colesevelam indicated asmonotherapy or with statin forLDL cholesterol reduction inboys and postmenarcheal girlsaged 10–17 y with family historyafter diet trial if LDL cholesterol� 190 mg/dL or if LDLcholesterol� 160 mg/dL withfamily history of premature CVDor�2 CVD risk factors in thepediatric patient
Cholesterolabsorptioninhibitors
Inhibits intestinal absorptionof cholesterol and plantsterols; decreases hepaticcholesterol pool;upregulates LDL receptors
Mainly lowers LDLcholesterol; somedecrease intriglycerides andsmall increase inHDL cholesterol
Ezetimibe Myopathy, gastrointestinalupset, headache
Not approved
Fibric acidderivatives
Agonist for PPAR-� nuclearreceptors that upregulateLPL and downregulateapolipoprotein C-III, bothincreasing degradation ofVLDL cholesterol andtriglycerides; hepaticsynthesis of VLDLcholesterol may also bedecreased
Mainly lowerstriglycerides andraises HDLcholesterol; littleeffect on LDLcholesterol
Fenofibrate, gemfibrozil Dyspepsia, constipation,myositis, anemia
Not approved
Nicotinic acid(extendedrelease)
Inhibits release of FFA fromadipose tissue; decreasesVLDL and LDL cholesterolproduction and HDLcholesterol degradation
Lowers triglyceridesand LDL cholesteroland raises HDLcholesterol; candecreaselipoprotein(a)
Niacin, extended release Flushing, hepatic toxicity,can increase fastingblood glucose, uricacid; can causehyperacidity
Use not recommended inchildren�2 y old
�-3 fish oil Decreases hepatic FA andtriglycerides synthesiswhile enhancing FAdegradation/oxidation,with subsequent reducedVLDL cholesterol release
Lowers triglycerides;raises HDLcholesterol; increasesLDL cholesterol andLDL cholesterolparticle size
�-3 acid ethyl esters Occasional adversegastrointestinal effectsbut no adverse effecton glucose levels ormuscle or liverenzymes or bleeding
Only 1 fish-oil preparation isFDA-approved for adults, butmany generic fish-oil capsulesare commercially available
HMG-CoA indicates hydroxymethylglutaryl coenzyme A; heFH, heterozygous hypercholesterolemia; PPAR-�, peroxisome proliferator-activated receptor; LPL, lipoprotein lipase; VLDL, very lowdensity lipoprotein; FFA, free fatty acid; FA, fatty acid.Adapted fromMcCrindle BW, Urbina EM, Dennison BA, et al; American Heart Association Atherosclerosis, Hypertension, and Obesity in Youth Committee; American Heart Association, Councilof Cardiovascular Disease in the Young; American Heart Association, Council on Cardiovascular Nursing. Circulation. 2007;115(14):1948–1967.
SUPPLEMENT ARTICLES
PEDIATRICS Volume 128, Supplement 5, December 2011 S245 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
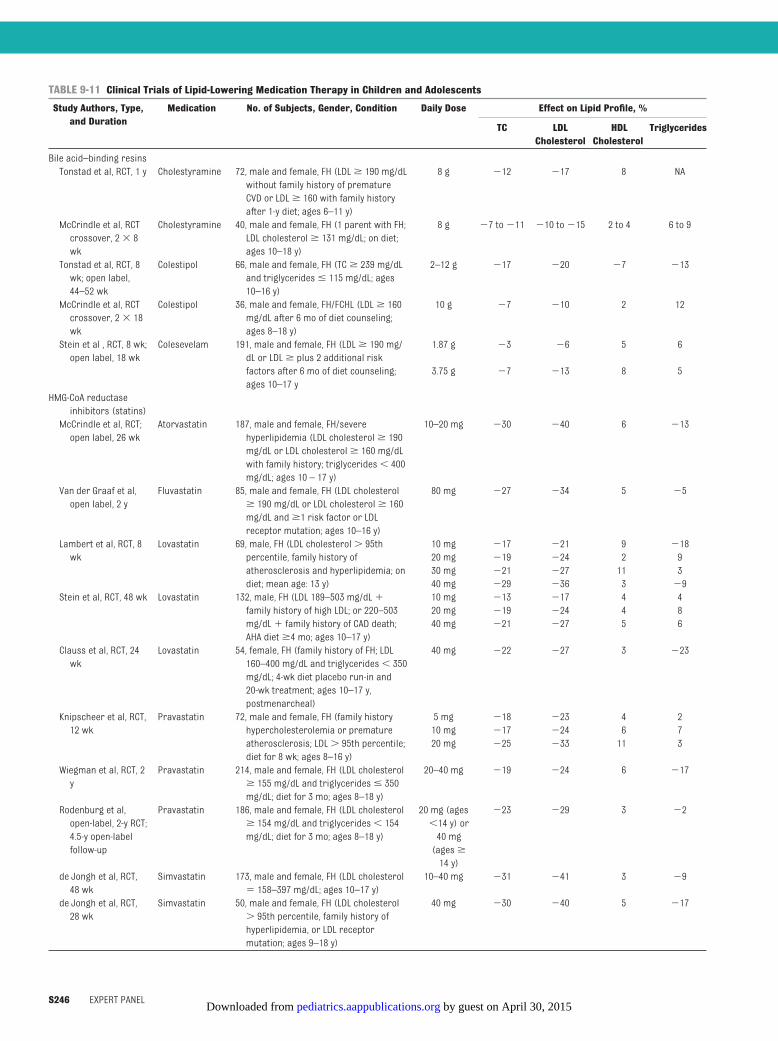
TABLE 9-11 Clinical Trials of Lipid-Lowering Medication Therapy in Children and Adolescents
Study Authors, Type,and Duration
Medication No. of Subjects, Gender, Condition Daily Dose Effect on Lipid Profile, %
TC LDLCholesterol
HDLCholesterol
Triglycerides
Bile acid–binding resinsTonstad et al, RCT, 1 y Cholestyramine 72, male and female, FH (LDL� 190 mg/dL
without family history of prematureCVD or LDL� 160 with family historyafter 1-y diet; ages 6–11 y)
8 g �12 �17 8 NA
McCrindle et al, RCTcrossover, 2� 8wk
Cholestyramine 40, male and female, FH (1 parent with FH;LDL cholesterol� 131 mg/dL; on diet;ages 10–18 y)
8 g �7 to�11 �10 to�15 2 to 4 6 to 9
Tonstad et al, RCT, 8wk; open label,44–52 wk
Colestipol 66, male and female, FH (TC� 239 mg/dLand triglycerides� 115 mg/dL; ages10–16 y)
2–12 g �17 �20 �7 �13
McCrindle et al, RCTcrossover, 2� 18wk
Colestipol 36, male and female, FH/FCHL (LDL� 160mg/dL after 6 mo of diet counseling;ages 8–18 y)
10 g �7 �10 2 12
Stein et al , RCT, 8 wk;open label, 18 wk
Colesevelam 191, male and female, FH (LDL� 190 mg/dL or LDL� plus 2 additional riskfactors after 6 mo of diet counseling;ages 10–17 y
1.87 g �3 �6 5 6
3.75 g �7 �13 8 5
HMG-CoA reductaseinhibitors (statins)McCrindle et al, RCT;open label, 26 wk
Atorvastatin 187, male and female, FH/severehyperlipidemia (LDL cholesterol� 190mg/dL or LDL cholesterol� 160 mg/dLwith family history; triglycerides� 400mg/dL; ages 10 – 17 y)
10–20 mg �30 �40 6 �13
Van der Graaf et al,open label, 2 y
Fluvastatin 85, male and female, FH (LDL cholesterol� 190 mg/dL or LDL cholesterol� 160mg/dL and�1 risk factor or LDLreceptor mutation; ages 10–16 y)
80 mg �27 �34 5 �5
Lambert et al, RCT, 8wk
Lovastatin 69, male, FH (LDL cholesterol� 95thpercentile, family history ofatherosclerosis and hyperlipidemia; ondiet; mean age: 13 y)
10 mg �17 �21 9 �1820 mg �19 �24 2 930 mg �21 �27 11 340 mg �29 �36 3 �9
Stein et al, RCT, 48 wk Lovastatin 132, male, FH (LDL 189–503 mg/dL�family history of high LDL; or 220–503mg/dL� family history of CAD death;AHA diet�4 mo; ages 10–17 y)
10 mg �13 �17 4 420 mg �19 �24 4 840 mg �21 �27 5 6
Clauss et al, RCT, 24wk
Lovastatin 54, female, FH (family history of FH; LDL160–400 mg/dL and triglycerides� 350mg/dL; 4-wk diet placebo run-in and20-wk treatment; ages 10–17 y,postmenarcheal)
40 mg �22 �27 3 �23
Knipscheer et al, RCT,12 wk
Pravastatin 72, male and female, FH (family historyhypercholesterolemia or prematureatherosclerosis; LDL� 95th percentile;diet for 8 wk; ages 8–16 y)
5 mg �18 �23 4 210 mg �17 �24 6 720 mg �25 �33 11 3
Wiegman et al, RCT, 2y
Pravastatin 214, male and female, FH (LDL cholesterol� 155 mg/dL and triglycerides� 350mg/dL; diet for 3 mo; ages 8–18 y)
20–40 mg �19 �24 6 �17
Rodenburg et al,open-label, 2-y RCT;4.5-y open-labelfollow-up
Pravastatin 186, male and female, FH (LDL cholesterol� 154 mg/dL and triglycerides� 154mg/dL; diet for 3 mo; ages 8–18 y)
20 mg (ages�14 y) or40 mg(ages�
14 y)
�23 �29 3 �2
de Jongh et al, RCT,48 wk
Simvastatin 173, male and female, FH (LDL cholesterol� 158–397 mg/dL; ages 10–17 y)
10–40 mg �31 �41 3 �9
de Jongh et al, RCT,28 wk
Simvastatin 50, male and female, FH (LDL cholesterol� 95th percentile, family history ofhyperlipidemia, or LDL receptormutation; ages 9–18 y)
40 mg �30 �40 5 �17
S246 EXPERT PANEL by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
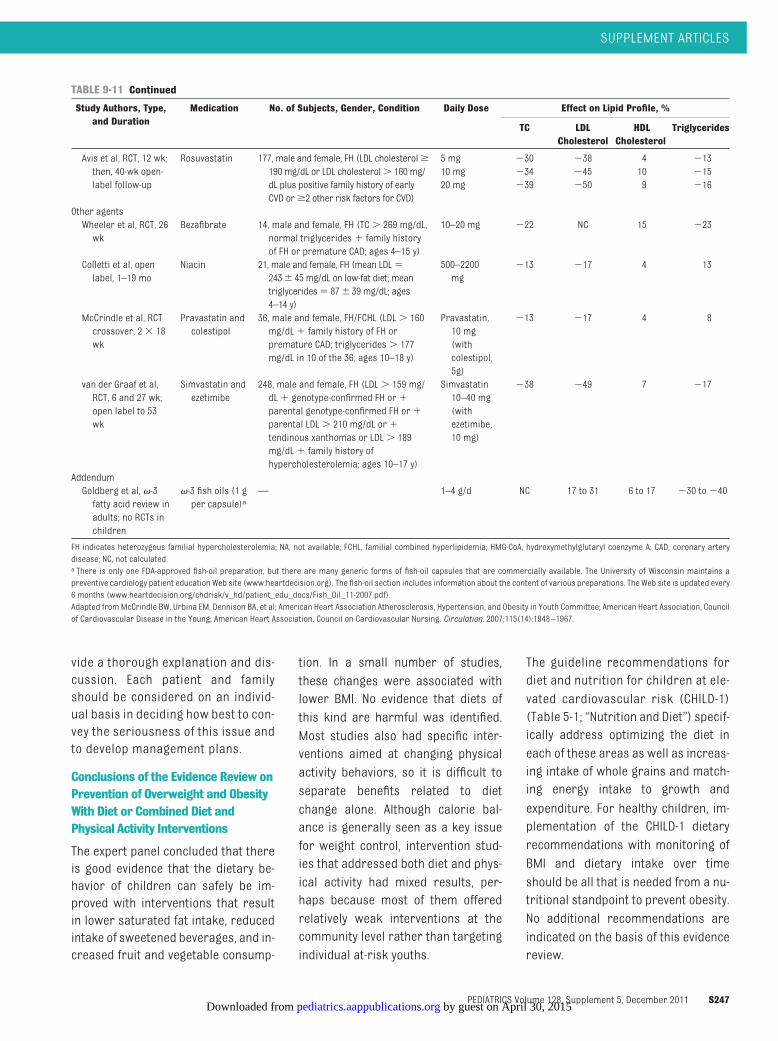
vide a thorough explanation and dis-cussion. Each patient and familyshould be considered on an individ-ual basis in deciding how best to con-vey the seriousness of this issue andto develop management plans.
Conclusions of the Evidence Review onPrevention of Overweight and ObesityWith Diet or Combined Diet andPhysical Activity Interventions
The expert panel concluded that thereis good evidence that the dietary be-havior of children can safely be im-proved with interventions that resultin lower saturated fat intake, reducedintake of sweetened beverages, and in-creased fruit and vegetable consump-
tion. In a small number of studies,these changes were associated withlower BMI. No evidence that diets ofthis kind are harmful was identified.Most studies also had specific inter-ventions aimed at changing physicalactivity behaviors, so it is difficult toseparate benefits related to dietchange alone. Although calorie bal-ance is generally seen as a key issuefor weight control, intervention stud-ies that addressed both diet and phys-ical activity had mixed results, per-haps because most of them offeredrelatively weak interventions at thecommunity level rather than targetingindividual at-risk youths.
The guideline recommendations fordiet and nutrition for children at ele-vated cardiovascular risk (CHILD-1)(Table 5-1; “Nutrition and Diet”) specif-ically address optimizing the diet ineach of these areas as well as increas-ing intake of whole grains and match-ing energy intake to growth and
expenditure. For healthy children, im-plementation of the CHILD-1 dietaryrecommendations with monitoring ofBMI and dietary intake over timeshould be all that is needed from a nu-tritional standpoint to prevent obesity.No additional recommendations areindicated on the basis of this evidencereview.
TABLE 9-11 Continued
Study Authors, Type,and Duration
Medication No. of Subjects, Gender, Condition Daily Dose Effect on Lipid Profile, %
TC LDLCholesterol
HDLCholesterol
Triglycerides
Avis et al, RCT, 12 wk;then, 40-wk open-label follow-up
Rosuvastatin 177, male and female, FH (LDL cholesterol�190 mg/dL or LDL cholesterol� 160 mg/dL plus positive family history of earlyCVD or�2 other risk factors for CVD)
5 mg �30 �38 4 �1310 mg �34 �45 10 �1520 mg �39 �50 9 �16
Other agentsWheeler et al, RCT, 26wk
Bezafibrate 14, male and female, FH (TC� 269 mg/dL,normal triglycerides� family historyof FH or premature CAD; ages 4–15 y)
10–20 mg �22 NC 15 �23
Colletti et al, openlabel, 1–19 mo
Niacin 21, male and female, FH (mean LDL�243� 45 mg/dL on low-fat diet; meantriglycerides� 87� 39 mg/dL; ages4–14 y)
500–2200mg
�13 �17 4 13
McCrindle et al, RCTcrossover, 2� 18wk
Pravastatin andcolestipol
36, male and female, FH/FCHL (LDL� 160mg/dL� family history of FH orpremature CAD; triglycerides� 177mg/dL in 10 of the 36; ages 10–18 y)
Pravastatin,10 mg(withcolestipol,5g)
�13 �17 4 8
van der Graaf et al,RCT, 6 and 27 wk;open label to 53wk
Simvastatin andezetimibe
248, male and female, FH (LDL� 159 mg/dL� genotype-confirmed FH or�parental genotype-confirmed FH or�parental LDL� 210 mg/dL or�tendinous xanthomas or LDL� 189mg/dL� family history ofhypercholesterolemia; ages 10–17 y)
Simvastatin10–40 mg(withezetimibe,10 mg)
�38 �49 7 �17
AddendumGoldberg et al, �-3fatty acid review inadults; no RCTs inchildren
�-3 fish oils (1 gper capsule)a
— 1–4 g/d NC 17 to 31 6 to 17 �30 to�40
FH indicates heterozygous familial hypercholesterolemia; NA, not available; FCHL, familial combined hyperlipidemia; HMG-CoA, hydroxymethylglutaryl coenzyme A; CAD, coronary arterydisease; NC, not calculated.a There is only one FDA-approved fish-oil preparation, but there are many generic forms of fish-oil capsules that are commercially available. The University of Wisconsin maintains apreventive cardiology patient education Web site (www.heartdecision.org). The fish-oil section includes information about the content of various preparations. The Web site is updated every6 months (www.heartdecision.org/chdrisk/v_hd/patient_edu_docs/Fish_Oil_11-2007.pdf).Adapted fromMcCrindle BW, Urbina EM, Dennison BA, et al; American Heart Association Atherosclerosis, Hypertension, and Obesity in Youth Committee; American Heart Association, Councilof Cardiovascular Disease in the Young; American Heart Association, Council on Cardiovascular Nursing. Circulation. 2007;115(14):1948–1967.
SUPPLEMENT ARTICLES
PEDIATRICS Volume 128, Supplement 5, December 2011 S247 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

Conclusions of the EvidenceReview on Prevention ofOverweight and Obesity WithPhysical Activity
A moderate number of RCTs have eval-uated the effect of interventions thataddressed only physical activityand/or sedentary behavior on preven-tion of overweight and obesity. In asmall number of these studies, the in-tervention was effective. It should benoted that these successful interven-tions often addressed reduction insedentary behavior rather than at-
tempts to increase physical activity. Ina majority of the studies there was nosignificant difference in body-sizemea-sures. Sample sizes were often small,and follow-up was often short (fre-quently �6 months). It is suggestedthat gender-specific programs mightbe more successful in changing activitybehavior. Overall, the expert panel con-cluded that on the basis of the evidencereview, increasing activity in isolationis of little benefit in preventing obesity.By contrast, the review suggests thatreducing sedentary behavior might be
beneficial in preventing the develop-ment of obesity. The activity recom-mendations in the guideline specifi-cally address limiting sedentarybehavior and increasing physical ac-tivity in all children. Guidance onamounts and intensity of physical ac-tivity and limitations on sedentaryscreen time are provided in the recom-mendations in “Physical Activity.” Onthe basis of this evidence review, noadditional specific recommendationsaddressing physical activity in pre-venting obesity are indicated.
TABLE 9-12 Recommendations for Use of 3-Hydroxy-3-Methylglutaryl-Coenzyme A Reductase Inhibitors (Statins) in Children and Adolescents
Patient selection1. Use algorithm (Fig 9-1) and risk-factor categories (Tables 9-6 and 9-7) to select statin therapy for patients.2. Include preferences of patient and family in decision-making.3. In general, do not start treatment with statins before the age of 10 y (patients with high-risk family history, high-risk conditions, or multiple risk factors[Tables 9-6 and 9-7] might be considered for medication initiation at age�10 y).
4. Precaution/contraindication with potentially interactive medications (cyclosporine, niacin, fibric acid derivatives, erythromycin, azole antifungal agents,nefazodone, many HIV protease inhibitors); check for potential interaction with all current medications at baseline.
5. Conduct baseline hepatic panel and CK before initiating treatment.Initiation and titration1. Choice of particular statin is a matter of preference. Clinicians are encouraged to develop familiarity and experience with one of the statins, includingdosage regimen and potential drug-drug interactions.
2. Start with the lowest dose once daily, usually at bedtime. Atorvastatin and rosuvastatin can be taken in the morning or evening because of their longhalf-lives.
3. Measure baseline CK, ALT, and AST.4. Instruct the patient to report all potential adverse effects, especially muscle cramps, weakness, asthenia, and more diffuse symptoms suggestive ofmyopathy.
5. Advise female patients about concerns with pregnancy and the need for appropriate contraception.6. Advise about potential future medication interactions, especially cyclosporine, niacin, fibric acid derivatives, erythromycin, azole antifungal agents,nefazodone, and HIV protease inhibitors.
Check for potential interaction whenever any new medication is initiated.1. Whenever potential myopathy symptoms are present, stop medication and assess CK; determine relation to recent physical activity. The threshold forworrisome level of CK is 10 times above the upper limit of reported normal, considering the impact of physical activity. Monitor the patient for resolutionof myopathy symptoms and any associated increase in CK level. Consideration can be given to restarting the medication once symptoms and laboratoryabnormalities have resolved.
2. After 4 wk, measure FLP, ALT, and AST and compare with laboratory-specific reported normal values.The threshold for worrisome levels of ALT or AST is�3 times the upper limit of reported normal.Target levels for LDL cholesterol: minimal,�130 mg/dL; ideal,�110 mg/dL.3. If target LDL cholesterol levels are achieved and there are no potential myopathy symptoms or laboratory abnormalities, continue therapy and recheck FLP,ALT, and AST in 8 wk and then in 3 mo.
4. If laboratory abnormalities are noted or symptoms are reported, temporarily withhold the medication and repeat the blood work in 2 wk. Whenabnormalities resolve, the medication may be restarted with close monitoring.
5. If target LDL cholesterol levels are not achieved, increase the dose by 1 increment (usually 10 mg) and repeat the blood work in 4 wk. If target LDLcholesterol levels are still not achieved, dose may be further increased by 1 increment, or another agent (bile acid sequestrant or cholesterol absorptioninhibitor) may be added under the direction of a lipid specialist.
Maintenance monitoring1. Monitor growth (height, weight, and BMI relative to normal growth charts), sexual maturation, and development.2. Whenever potential myopathy symptoms present, stop medication and assess CK.3. Monitor FLP, ALT, and AST every 3–4 mo in the first year, every 6 mo in the second year and beyond, and whenever clinically indicated.4. Monitor and encourage compliance with lipid-lowering dietary and medication therapy. Serially assess and counsel for other risk factors such as weightgain, smoking, and inactivity.
5. Counsel adolescent girls about statin contraindications in pregnancy and the need for abstinence or use of appropriate contraceptive measures. Use of oralcontraceptives is not contraindicated if medically appropriate. Seek referral to an adolescent medicine or gynecologic specialist as appropriate.
CK indicates creatine kinase; ALT, alanine aminotransferase; AST, aspartate aminotransferase.
S248 EXPERT PANEL by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
Summary of the Evidence Reviewof Children at Increased Risk forOverweight and Obesity
Certain populations of children whoare of normal weight are at risk fordeveloping overweight and obesity asthey grow older. Observational studieshave identified risk factors that putthese children at greater risk; how-ever, research is lacking regarding anappropriate intervention. Despite thatfact, epidemiologic associations sug-gest that primary care providersshould be alert to increasing BMItrends and excessive weight gain be-yond what is anticipated for height in-crease when dealing with these chil-dren and consider intervention beforethe child becomes overweight.
Observational studies have identifiedsample populations that are at specialrisk for obesity:
● children with a BMI between the85th and 95th percentiles;
● children in whom there is a positivefamily history of obesity in 1 or bothparents;
● early onset of increasing weight be-yond that appropriate for increase inheight, which can be identified early(beginning in the first year of life);
● excessive increase in weight duringadolescence, particularly in blackgirls; and
● children who have been very activeand then become inactive or adoles-cents who are inactive in general(an example would be a child whopreviously participated in organizedsports and has stopped, particu-larly in adolescence).
No RCTs that addressed these popula-tions were identified. Despite this fact,the expert panel believes that lifestylerecommendations with a goal of pre-vention of excessive weight gain areneeded for normal-weight childrenwith characteristics consistent withspecial risk for development of over-
weight and obesity. The diet and activ-ity recommendations proposed forchildren at elevated cardiovascularrisk (“Nutrition and Diet”; “Physical Ac-tivity”) should be vigorously reinforcedin these children. In any child, the de-velopment of a BMI between the 85thand 95th percentile should be taken asa sign that increased attention to dietand activity as well as BMI-specificfollow-up is indicated.
Conclusions and Grading of theEvidence Review on Treatment ofObesity
● There is good evidence for the effec-tiveness of combined weight-lossprograms that included behavior-change counseling, negative energybalance through diet, and increasedphysical activity in addressing obe-sity in children older than 6 yearswith a BMI at the �95th percentileand no comorbidities (grade A).However, such programs have beeneffective primarily in a comprehen-sive weight-loss program or in re-search settings; only a small numberhave been shown to be effective in pri-mary care settings.
● No data were identified on weight-loss programs for children youngerthan 6 years.
● No single negative-energy diet planwas identified from the evidence re-view. Dietary plans should be deter-mined for each child on the basis ofbaseline body size, energy require-ments for growth, and physical activitylevel (grade D).
● Increasing dietary fiber from cornbran, wheat flour, wheat bran, oatflakes, corn germ meal, or gluco-mannan does not significantly im-prove weight loss (grade A).
● Various diets, including low-glycemic-load diets, low-carbohydrate diets, fi-ber supplements, and protein-sparing modified fasts, have notbeenadequately studiedas to their ef-
fects on obesity in children andadolescents.
● For children aged 6 to 12 years:● Family-based programs in re-search settings that addressedboth diet and activity have beenshown to be effective at initiatingand sustaining weight loss over afollow-up of 10 years (grade A).
● The greatest weight loss is achievedwhenparents are the focus of the in-tervention (grade A).
● For adolescents:
● Comprehensive programs in re-search settings were effective atachieving weight loss in theshort-term (grade A).
● The greatest weight change wasachieved when the adolescentwas the primary focus of the in-tervention (grade B).
● Behavior-change programs thatinvolved peers resulted in moresustained weight loss (grade B).
● In overweight and obese youth, thecombination of diet and a specificphysical activity intervention thatreduced sedentary activity and/orincreased physical activity was uni-versally more effective at achievingdecreases in weight and BMI as wellas decreases in body fat comparedwith an isolated diet intervention:
● In both children and adolescents,exercise training improved weightloss and body composition (de-creasing fat mass and reducingvisceral fat), decreased insulin re-sistance, reduced BP, normalizeddyslipidemia, and normalized sub-clinical measures of atherosclero-sis (grade A).
● In children aged 7 to 12 years, re-duction in sedentary activity inde-pendent of increasing physicalactivity produced weight loss(grade B). In this age group, re-ductions in sedentary activity
SUPPLEMENT ARTICLES
PEDIATRICS Volume 128, Supplement 5, December 2011 S249 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
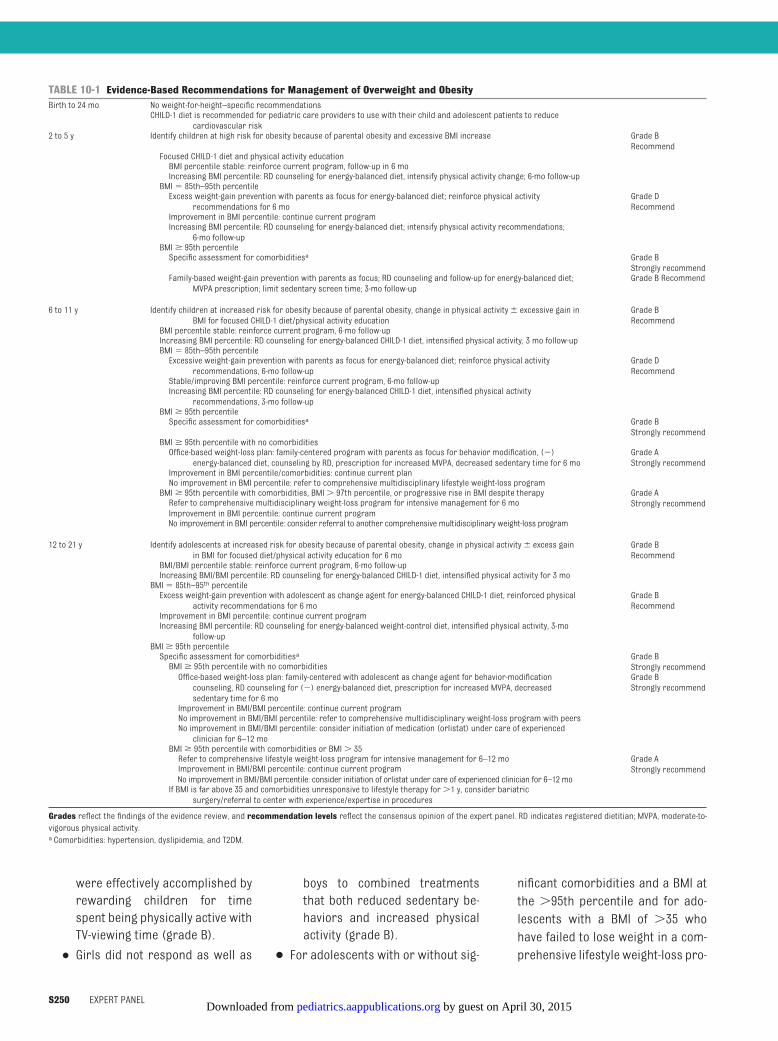
were effectively accomplished byrewarding children for timespent being physically active withTV-viewing time (grade B).
● Girls did not respond as well as
boys to combined treatmentsthat both reduced sedentary be-haviors and increased physicalactivity (grade B).
● For adolescents with or without sig-
nificant comorbidities and a BMI atthe �95th percentile and for ado-lescents with a BMI of �35 whohave failed to lose weight in a com-prehensive lifestyle weight-loss pro-
TABLE 10-1 Evidence-Based Recommendations for Management of Overweight and ObesityBirth to 24 mo No weight-for-height–specific recommendations
CHILD-1 diet is recommended for pediatric care providers to use with their child and adolescent patients to reducecardiovascular risk
2 to 5 y Identify children at high risk for obesity because of parental obesity and excessive BMI increase Grade BRecommend
Focused CHILD-1 diet and physical activity educationBMI percentile stable: reinforce current program, follow-up in 6 moIncreasing BMI percentile: RD counseling for energy-balanced diet, intensify physical activity change; 6-mo follow-upBMI� 85th–95th percentileExcess weight-gain prevention with parents as focus for energy-balanced diet; reinforce physical activity
recommendations for 6 moGrade DRecommend
Improvement in BMI percentile: continue current programIncreasing BMI percentile: RD counseling for energy-balanced diet; intensify physical activity recommendations;
6-mo follow-upBMI� 95th percentileSpecific assessment for comorbiditiesa Grade B
Strongly recommendFamily-based weight-gain prevention with parents as focus; RD counseling and follow-up for energy-balanced diet;
MVPA prescription; limit sedentary screen time; 3-mo follow-upGrade B Recommend
6 to 11 y Identify children at increased risk for obesity because of parental obesity, change in physical activity� excessive gain inBMI for focused CHILD-1 diet/physical activity education
Grade BRecommend
BMI percentile stable: reinforce current program, 6-mo follow-upIncreasing BMI percentile: RD counseling for energy-balanced CHILD-1 diet, intensified physical activity, 3 mo follow-upBMI� 85th–95th percentileExcessive weight-gain prevention with parents as focus for energy-balanced diet; reinforce physical activity
recommendations, 6-mo follow-upGrade DRecommend
Stable/improving BMI percentile: reinforce current program, 6-mo follow-upIncreasing BMI percentile: RD counseling for energy-balanced CHILD-1 diet, intensified physical activity
recommendations, 3-mo follow-upBMI� 95th percentileSpecific assessment for comorbiditiesa Grade B
Strongly recommendBMI� 95th percentile with no comorbiditiesOffice-based weight-loss plan: family-centered program with parents as focus for behavior modification, (�)
energy-balanced diet, counseling by RD, prescription for increased MVPA, decreased sedentary time for 6 moGrade AStrongly recommend
Improvement in BMI percentile/comorbidities: continue current planNo improvement in BMI percentile: refer to comprehensive multidisciplinary lifestyle weight-loss programBMI� 95th percentile with comorbidities, BMI� 97th percentile, or progressive rise in BMI despite therapy Grade A
Strongly recommendRefer to comprehensive multidisciplinary weight-loss program for intensive management for 6 moImprovement in BMI percentile: continue current programNo improvement in BMI percentile: consider referral to another comprehensive multidisciplinary weight-loss program
12 to 21 y Identify adolescents at increased risk for obesity because of parental obesity, change in physical activity� excess gainin BMI for focused diet/physical activity education for 6 mo
Grade BRecommend
BMI/BMI percentile stable: reinforce current program, 6-mo follow-upIncreasing BMI/BMI percentile: RD counseling for energy-balanced CHILD-1 diet, intensified physical activity for 3 moBMI� 85th–95th percentileExcess weight-gain prevention with adolescent as change agent for energy-balanced CHILD-1 diet, reinforced physical
activity recommendations for 6 moGrade BRecommend
Improvement in BMI percentile: continue current programIncreasing BMI percentile: RD counseling for energy-balanced weight-control diet, intensified physical activity, 3-mo
follow-upBMI� 95th percentileSpecific assessment for comorbiditiesa Grade B
Strongly recommendBMI� 95th percentile with no comorbiditiesOffice-based weight-loss plan: family-centered with adolescent as change agent for behavior-modificationcounseling, RD counseling for (�) energy-balanced diet, prescription for increased MVPA, decreasedsedentary time for 6 mo
Grade BStrongly recommend
Improvement in BMI/BMI percentile: continue current programNo improvement in BMI/BMI percentile: refer to comprehensive multidisciplinary weight-loss program with peersNo improvement in BMI/BMI percentile: consider initiation of medication (orlistat) under care of experiencedclinician for 6–12 mo
BMI� 95th percentile with comorbidities or BMI� 35Refer to comprehensive lifestyle weight-loss program for intensive management for 6–12 mo Grade A
Strongly recommendImprovement in BMI/BMI percentile: continue current programNo improvement in BMI/BMI percentile: consider initiation of orlistat under care of experienced clinician for 6–12 moIf BMI is far above 35 and comorbidities unresponsive to lifestyle therapy for�1 y, consider bariatric
surgery/referral to center with experience/expertise in procedures
Grades reflect the findings of the evidence review, and recommendation levels reflect the consensus opinion of the expert panel. RD indicates registered dietitian; MVPA, moderate-to-vigorous physical activity.a Comorbidities: hypertension, dyslipidemia, and T2DM.
S250 EXPERT PANEL by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

gram, addition of medication underthe care of a physician experiencedin managing weight loss with medi-cation can be safe and effective inachieving weight loss with follow-upof 4 to 12 months. However, long-term safety and efficacy data arenot available:
● In adolescents with severe obe-sity and insulin resistance, theaddition of metformin to a com-prehensive lifestyle weight-lossprogram improved fasting insu-lin levels and significantly re-duced weight and BMI (grade B).(Metformin is currently approvedby the US Food and Drug Adminis-tration [FDA] for pediatric pa-tients aged 10 years or older withT2DM but is not approved forweight loss for either children oradults.)
● For obese adolescents older than12 years, the addition of orlistatto a comprehensive lifestyleweight-loss program improvedweight loss and BMI (grade A);however, use of this medicationhad a high rate of adverse gastro-intestinal effects. (Orlistat [underthe trade name Xenical (RochePharmaceuticals, Nutley, NJ)] isapproved by the FDA for weightloss in pediatric patients 12 yearsof age and older in conjunctionwith a reduced-calorie diet. In Au-gust 2009, the FDA released anearly communication about anongoing safety review regardingreports of liver-related adverseevents in some patients takingorlistat. In May 2010, the orlistatlabeling was updated to incorpo-rate safety information pertain-ing to the occurrence of rarepostmarketing cases of severeliver injury, including hepatic fail-ure that resulted in liver trans-plant or death.)
● Dropout rates are substantial for allweight-treatment programs.
● No studies defining an appropriaterate forweight loss in any age groupwere identified by the guidelines ev-idence review. The 2010 DGA8 recom-mends slowing weight gain whileallowing normal growth and devel-opment. For those with a BMI at the�95th percentile without comor-bidities, both the AMA/CDC/MCHB ex-pert committee and the AAP16 recom-mend weight maintenance resultingin decreasing BMI as age increases.With a BMI at the �95th percentilewith comorbidities, the AMA/CDC/MCHBexpert committee and the AAP16
recommend gradual weight loss notto exceed 1 lb/month in children aged2 to 11 years or 2 lb/week in adoles-cents (no grade).
● For adolescents with a BMI farabove 35 and associated comorbidi-ties, bariatric surgery on a researchprotocol in conjunction with a com-prehensive lifestyle weight-loss pro-gram improved weight loss, BMI,and other outcomes such as insulinresistance, glucose tolerance, andcardiovascular measures in smallcase series (grade D).
The recommendations for manage-ment of overweight and obesity arelisted in Table 10-1.
11. DM AND OTHER CONDITIONSPREDISPOSING TO THEDEVELOPMENT OF ACCELERATEDATHEROSCLEROSIS
DM is an established risk factor forearly CVD. Metabolically, DM is charac-terized by hyperglycemia caused bydefects in insulin secretion (T1DM)and insulin function and/or secretion(T2DM). Both T1DM and T2DM are asso-ciated with vascular disease. Resultsof autopsy and noninvasive imagingstudies suggest that the extent of vas-cular involvement reflects the dura-tion of the disease and the severity of
the chronic metabolic derangement.The epidemiologies of the 2 types differsignificantly. T1DM presents at ayounger age; 25% of patients are diag-nosed between the ages of 5 and 10years and another 40% between theages of 10 and 15 years. If not treatedadequately, the degree of hyperglyce-mia is severe, and patients are highlysymptomatic. By contrast, with T2DM,the majority of patients present inadult life, but a small and growingnumber present in adolescence, andmost are relatively asymptomatic withonly mild-to-moderate hyperglycemiain combination with obesity. Regard-less of these differences, children withDM, type 1 or 2, are at significantly in-creased risk for accelerated athero-sclerosis and early CVD.
In certain other pediatric diseasestates, the process of atherosclerosisis dramatically accelerated with clini-cal coronary events occurring in child-hood and very early adult life. Theseconditions were the subject of a recentguideline from the American Heart As-sociation (AHA).17 The expert panelelected to use the AHA guideline as atemplate for developing recommenda-tions for children with conditions suchas DM that predispose them to very ac-celerated atherosclerosis, becausethe evidence review identified only asmall number of studies that ad-dressed these conditions in an RCT.
Conclusions of the EvidenceReview for DM and OtherPredisposing Conditions
Children with DM, T1DM or T2DM, repre-sent the prototype of the child at specialrisk for accelerated atherosclerosis andearly clinical CVD. Tomaximize identifica-tion of T2DM in childhood and adoles-cence, the screening algorithm from theAmerican Diabetes Association18 is rec-ommended for screening in all children(Table 11-1).
Limited high-quality studies that ad-
SUPPLEMENT ARTICLES
PEDIATRICS Volume 128, Supplement 5, December 2011 S251 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

dressed cardiovascular risk reductionin children with conditions predispos-ing them to accelerated atherosclero-sis were found, so the expert panelelected to modify the recommenda-tions of an expert pediatric panel con-vened by the AHA that published itsrecommendations for risk-factor man-agement in 2006; these recommenda-tions have been endorsed by the AAPand are included in the guideline data-base for these guidelines.17
The authors of the AHA statement rec-ommended specific risk identificationand management stratified accordingto risk on the basis of defined otherconditions that parallel the recom-mendations for adults with DM or
other CVD equivalents. For those in thehigh-risk category (Table 11-2), the dis-ease process has been associatedwith clinical coronary disease before30 years of age. For those in themoderate-risk category, the diseaseprocess has been shown to be associ-ated with pathologic, physiologic, orsubclinical evidence of acceleratedatherosclerosis.
The expert panel believes that theserecommendations should be used forthe management of children and ado-lescents with DM and other predispos-ing conditions as outlined in the algo-rithm in Fig 11-1 and in Tables 11-2 and11-3. With the growing evidence of vas-cular disease in children with T2DM,
the expert panel felt that it was pru-dent to include both T1DM and T2DM inthe high-risk category. With increasingevidence of vascular dysfunction inchildren with HIV infection and ne-phrotic syndrome, these 2 conditionshave been added to the selected dis-ease settings in the moderate-risk cat-egory. Patients in the high-risk cate-gory require intensive managementwith more aggressive goals for ther-apy than those in the moderate-riskcategory, as outlined in the algorithm.
12. RISK-FACTOR CLUSTERING ANDTHE METABOLIC SYNDROME
Traditional cardiovascular risk factorssuch as obesity, hypertension, and dys-lipidemia demonstrate clustering inyouth. Risk behaviors such as smok-ing, suboptimal diet, and sedentary be-havior also demonstrate clustering, asdo advantageous diet and exercisehabits. Becoming obese increases theprevalence of the risk-factor cluster inadults called the metabolic syndrome.The metabolic syndrome is defined as�3 of the following risk factors: elevatedwaist circumference, triglyceride levels,BP, and/or fasting glucose level and re-ducedHDL cholesterol level. In theUnitedStates, themetabolic syndrome issaid toaffect between 34% and 39% of adults,including 7%ofmenand 6%ofwomen inthe 20- to 30-year-old age group. The ex-pert panel reviewed all the RCTs, system-atic reviews, meta-analyses, and obser-vational studies that addressed thechildhood association between the risk-factor cluster known as the metabolicsyndrome and the development of ath-erosclerosis, and the identification andmanagement of the cluster in childrenand adolescents.
There is a lack of consensus on how todefine metabolic syndrome in youth,which has led to widely varying esti-mates of its frequency. A recent analysisofNationalHealthandNutritionExamina-tion Survey data from 1999 to 200219
TABLE 11-1 American Diabetes Association (ADA) Screening Recommendations for Type 2DM in Childhood
Criteria:● Overweight, defined by:–BMI� 85th percentile for age and gender, or–Weight for height� 85th percentile, or–Weight� 120% of ideal for height
Plus any two of the following risk factors:● Family history of type 2 DM in first- or second-degree relative● Race/ethnicity (Native American, African-American, Latino, Asian-American, Pacific Islander)● Signs of insulin resistance or conditions associated with insulin resistance (acanthosis nigricans,hypertension, dyslipidemia, or polycystic ovary syndrome)
Screening procedure:Age of initiation:�10 y, or at onset of puberty, if puberty occurs at a younger ageFrequency:Every 2 yTest:Fasting plasma glucose
Reproduced with permission from American Diabetes Association. Diabetes Care. 2000;23(3):386.
TABLE 11-2 Special Risk Pediatric Conditions: Stratification by Risk Category
High riskManifest coronary artery disease at�30 y of age: clinical evidenceT1DM or T2DMChronic kidney disease/end-stage renal disease/post–renal transplantPost–orthotopic heart transplantationKawasaki disease with current coronary aneurysms
Moderate riskAccelerated atherosclerosis: pathophysiologic evidenceKawasaki disease with regressed coronary aneurysmsChronic inflammatory disease (systemic lupus erythematosus, juvenile rheumatoid arthritis)HIV infectionNephrotic syndrome
Adapted from Kavey RE, Allada V, Daniels SR, et al; American Heart Association, Expert Panel on Population and PreventionScience; American Heart Association, Council on Cardiovascular Disease in the Young; American Heart Association, Councilon Epidemiology and Prevention; American Heart Association, Council on Nutrition, Physical Activity and Metabolism;American Heart Association, Council on High Blood Pressure Research; American Heart Association, Council on Cardiovas-cular Nursing; American Heart Association, Council on the Kidney in Heart Disease; Interdisciplinary Working Group onQuality of Care and Outcomes Research. Circulation. 2006;114(24):2710–2738.
S252 EXPERT PANEL by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

yielded prevalence estimates for allteens from 2.0% to 9.4% and for obeseteens from12.4% to44.2%.Regardlessofthe definition used, the prevalence of themetabolic syndrome risk-factor clusteris higher in older (12- to 14-year-old)compared with younger (8- to 11-year-old) children. The specific etiology of
metabolic syndrome is unknown; how-ever, it is most likely caused by the ex-pression of various genotypes modifiedby environmental interactions andmedi-ated through abdominal obesity and in-sulin resistance. Longitudinal studies ofcohorts in which the metabolic syn-drome cluster was present in childhood
identified an increased incidence of bothT2DM and clinical cardiovascular eventsover a follow-up period of 25 years.4 Astrong association between obesity withor without elevated insulin levels and/orhypertension in early childhood and sub-sequent development of the metabolicsyndromeconstellation inadulthoodhas
Directions: Step 1: Risk stratification by disease process (Table 11-2). Step 2: Assess all cardiovascular risk factors. If there are >2 comorbidities,
move tier II patient to tier I for subsequent management. Step 3: Tier-specific treatment goals/cut points defined. Step 4: Initial therapy: For tier I, initial management is therapeutic lifestyle
change PLUS disease-specific management (Table 11-3). For tier II, initial management is therapeutic lifestyle change.
Yes
Tier I: High Risk
� T1DM and T2DM � Chronic kidney disease/end stage
renal disease/ post–kidney transplant � Post–heart transplant � Kawasaki disease with current
coronary artery aneurysms
Intensive lifestyle management CHILD-1a, Activity Rxb
Weight loss as neededc
Tier II: Moderate Risk� BMI ≤ 90%ile for age/gender � BP ≤ 95%ile for age/gender/HT%ile � Lipids (mg/dL): LDL-C ≤ 130,
TG < 130, non–HDL-C < 140 � FG < 100 mg/dL, HgbA1c < 7%
CV RISK FACTORS/ COMORBIDITIES� Family history of early CVD in expanded first-degree pedigree (♂ ≤55 y;
♀ ≤65 y)� FLP� Smoking history � BP (3 separate occasions), interpreted for age/gender/HT percentile (%ile)� HT, WT, BMI � FG� Diet, physical activity/exercise history
Tier II: Moderate Risk
� Kawasaki disease with regressed coronary aneurysms
� Chronic inflammatory disease � HIV � Nephrotic syndrome
Condition-specific management – Table 11-3
If goals not met, considermedication per risk-specific guideline recommendations
PPLLUUSS
Intensive lifestyle management CHILD-1a, Activity Rxb WT loss as neededc
Tier 1: High Risk� BMI < 85th%ile for age/gender. � BP < 90th %ile for age/gender/HT%ile � Lipids (mg/dL): LDL-C < 100,
TG < 90, non–HDL-C < 120 � FG < 100 mg/dL, HgbA1c < 7%
No
Step 1. RISK
STRATIFICATIONBY DISEASE
PROCESS
Step 2. ASSESSCV RFs
(> 2 RFs �Move to tier 1)
Step 3. TIER-
SPECIFIC CUT POINTS/
TREATMENTGOALS
Step 4: LIFESTYLE CHANGE
Step 5: DRUG
THERAPY
FIGURE 11-1Risk stratification and management for children with conditions predisposing to accelerated atherosclerosis and early CVD. CV indicatescardiovascular; RF, risk factor; HT, height; WT, weight; TG, triglycerides; %ile, percentile; C, cholesterol; FG, fasting glucose; Rx, recommendation. a See“Nutrition and Diet”; b see “Physical Activity”; c see “Overweight and Obesity.” Adapted from Kavey RE, Allada V, Daniels SR, et al; American Heart Association,Expert Panel on Population and Prevention Science; American Heart Association, Council on Cardiovascular Disease in the Young; American HeartAssociation, Council on Epidemiology and Prevention; American Heart Association, Council on Nutrition, Physical Activity and Metabolism; American HeartAssociation, Council on High Blood Pressure Research; American Heart Association, Council on Cardiovascular Nursing; American Heart Association, Councilon the Kidney in Heart Disease; Interdisciplinary Working Group on Quality of Care and Outcomes Research. Circulation. 2006;114(24):2710–2738.
SUPPLEMENT ARTICLES
PEDIATRICS Volume 128, Supplement 5, December 2011 S253 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

been consistently demonstrated. Treat-ment of cardiovascular risk-factor clus-tering in youth has not been thoroughlyevaluated, butmaintenance of low levelsof cardiovascular risk factors starting inchildhood is associated with a lowerprevalence of CVD and increased longev-ity in adult life.
RECOMMENDATIONS FORMANAGEMENT OF RISK-FACTORCLUSTERING AND THE METABOLICSYNDROMEThe metabolic-syndrome concept is im-portant, because it identifies a commonmultiple cardiovascular-risk phenotypein pediatrics. However, the absence of adefined etiology, the lack of consensuson definition, and the paucity of high-
level evidence addressing managementin childhood led the expert panel to con-clude that the metabolic syndromeshould not be considered as a separaterisk factor in childhood and adoles-cence. Prevention of obesity is the mostimportant strategy for lowering theprevalence of metabolic syndrome inadults, and this seems strongly applica-ble in childhood (see “Overweight andObesity”). Given the strong relationshipof obesity and physical inactivity to themetabolic syndrome and insulin resis-tance, the expert panelmakes the follow-ing recommendations. Because of thepaucity of evidence available, the recom-mendations are a consensus of the ex-pert panel (grade D).
● The presence of any combination ofmultiple risk factors should prompt in-tensification of therapy with an empha-sis on lifestyle modification to addressindividual metabolic syndrome risk-factor levels.
● The presence of obesity shouldprompt specific evaluation for allother cardiovascular risk factors in-cluding family history of prematureCVD, hypertension, dyslipidemia,DM, and tobacco exposure.
● The coexistence of obesity with anyothermajor cardiovascular risk fac-tor should be recognized by clini-cians as a setting in which:
● intensive weight reduction shouldbe undertaken per the recommen-dations in “Overweight and Obe-sity,” along with management ofidentified risk factors including ini-tiation of pharmacologic therapy,per the risk-factor–specific sec-tions in theseguidelines (“HighBP”;“Lipids and Lipoproteins”; “DM andOther Conditions Predisposing tothe Development of AcceleratedAtherosclerosis”; “Tobacco Expo-sure”); and
● prompt evaluation for DM, liver-function abnormalities, left ven-tricular hypertrophy, and sleepapnea should be undertaken.
These recommendations are supportedby the knowledge that cardiovascu-lar morbidity has a continuous rela-tionship across the risk-distributionspectrum and that a youth with multi-ple borderline risk factors might, infact, have risk equivalent to a personwith extreme abnormality of a singlemajor risk factor. A presentation suchas this should lead to intense nutritionand exercise management with closefollow-up, and if lifestyle interventionis unsuccessful, consideration shouldbe given to endocrine referral. Table12-1 provides definitions of componentrisk-factor levels for evaluating chil-
TABLE 11-3 Condition-Specific Treatment Recommendations for High-Risk Conditions
Rigorous age-appropriate education in diet, activity, smoking cessation for allSpecific therapy as needed to achieve BP, LDL cholesterol, glucose, and HbA1c goals indicated for eachtier, as outlined in algorithm; timing individualized for each patient and diagnosis
DM regardless of type:For T1DM, intensive glucose management per endocrinologist with frequent glucose monitoring/insulintitration to maintain optimal plasma glucose and HbA1c levels for ageFor T2DM, intensive weight management and glucose control in consultation with an endocrinologist asneeded to maintain optimal plasma glucose and HbA1c levels for ageAssess BMI and fasting lipid levels: step 4 lifestyle management of weight and lipid levels for 6 moIf LDL goals are not achieved, consider statin therapy if age is�10 y to achieve tier 1 treatment goalsfor LDL cholesterolInitial BP� 90th percentile: step 4 lifestyle management plus no added salt, increased activity for 6 moIf BP is consistently at the�95th percentile for age/gender/height, initiate angiotensin-convertingenzyme inhibitor therapy with a BP goal of�90th percentile for gender/height or�120/80 mm Hg,whichever is lower
Chronic kidney disease/end-stage renal disease/post–renal transplant:Optimization of renal-failure management with dialysis/transplantation per nephrologyAssess BMI, BP, and lipid and FG levels: step 4 lifestyle management for 6 moIf LDL goals are not achieved, consider statin therapy if age is�10 y to achieve tier 1 treatment goalsfor LDL cholesterolIf BP is consistently at the�95th percentile for age/gender/height, initiate angiotensin-convertingenzyme inhibitor therapy with a BP goal of�90th percentile for gender/height or�120/80 mm Hg,whichever is lower
After heart transplantation:Optimization of antirejection therapy, treatment for cytomegalovirus infection, routine evaluation byangiography/perfusion imaging per transplant physicianAssess BMI, BP, and lipid and FG levels: initiate step 5 therapy, including statins, immediately for allpatients aged�1 y to achieve tier 1 treatment goals
Kawasaki disease with current coronary aneurysms:Antithrombotic therapy, activity restriction, ongoing myocardial perfusion evaluation per cardiologistAssess BMI, BP, and lipid and FG levels: step 4 lifestyle management for 6 moIf goals are not achieved, consider pharmacologic therapy for LDL cholesterol and BP if age is�10 y toachieve tier 1 treatment goals
FG indicates fasting glucose.Adapted from Kavey RE, Allada V, Daniels SR, et al; American Heart Association, Expert Panel on Population and PreventionScience; American Heart Association, Council on Cardiovascular Disease in the Young; American Heart Association, Councilon Epidemiology and Prevention; American Heart Association, Council on Nutrition, Physical Activity and Metabolism;American Heart Association, Council on High Blood Pressure Research; American Heart Association, Council on Cardiovas-cular Nursing; American Heart Association, Council on the Kidney in Heart Disease; Interdisciplinary Working Group onQuality of Care and Outcomes Research. Circulation. 2006;114(24):2710–2738.
S254 EXPERT PANEL by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

dren with multiple cardiovascular riskfactors.
13. PERINATAL FACTORSIncreasing evidence links prenatal expo-sures to adverse health outcomes. Peri-natal risk reduction is an area in whichpediatric care providers can potentiallybe effective, because they are often theonly physicians whom amother sees be-tween pregnancies. The expert panelidentified 3 potential areas for consider-ation: maternal obesity; choice of neona-tal feeding method; and maternal smok-ing cessation. Maternal obesity isassociated with gestational DM, higherbirth weight, childhood obesity mea-sured by increased BMI, and increasedrisk of the metabolic syndrome and
T2DM in offspring. However, the expertpanel could not identify any prepreg-nancy or postpartum studies that ad-dressed maternal obesity in a pediatriccare setting, and more general ap-proaches to preventing or treating obe-sity in women of reproductive age arebeyond the scope of this report. A de-tailed discussion of childhood obesity it-self is the subject of “Overweight andObesity.” With regard to choice of neona-tal feeding method, the cardiovascularadvantages of breastfeeding as the pri-mary source of nutrition for infants areemphasized in “Nutrition and Diet.”Therefore, the evidence review for thissection is focused on maternal smokingcessation.
Conclusions and Grading of theEvidence Review on MaternalSmoking Cessation
● The expert panel found that strongevidence supports a benefit for in-terventions directed at maternalsmoking cessation during pregnancy(grade A). Weaker evidence suggeststhat these interventions do not pre-vent relapse after delivery. Trials ofcessation in the postpartum period,whichwouldbe themostapplicable topediatric providers, havebeen limitedin number and suggest that for ma-ternal smoking cessation to be sus-tained, specific continued support inthe pediatric care setting is required.
● No smoking-cessation interventionshave resulted in any reported ad-verse effects related to the interven-tions (no grade).
● The expert panel believes that pediat-ric care providers can play a role inhelping mothers to remain smoke-free or to quit smoking in the inter-pregnancy interval. For most women,this interval will extend to the earlyfirst trimester of any subsequentpregnancy. The pediatric well-childschedule calls for �10 visits in thefirst 2 years of life, and mothers at-tend most of those visits, so the pedi-atric care provider usually seeswomen in this period more than anyother health care professional. Pedi-atric care providers often have a sus-tained relationship with the motherand her infant, and many already ad-vocate for parental smoking cessa-tion in their efforts to promote asmoke-free environment for chil-dren. Pediatric providers and/ortheir staff need to be trained to ei-ther deliver or refer to a long-termmaternal smoking-cessation pro-gram (no grade).
Recommendations for maternal smok-ing cessation are listed in Table 13-1.
TABLE 12-1 Metabolic Syndrome Component Levels for Evaluation of Children With MultipleCardiovascular Risk Factors
Risk Factor Cut Point Reference
Obesity, percentileBMI �85th to�95th CDC growth chartsWaist circumference �90th to�95th NHANESBP, percentile �90th to�95th “The Fourth Report on the Diagnosis,
Evaluation and Treatment of HighBlood Pressure in Children andAdolescents”
Dyslipidemia, mg/dL See “Lipids and Lipoproteins” fornormative values
HDL cholesterol �40 to�45Triglycerides0–9 y �75 to�100�10 y �90 to�130Non-HDL cholesterol �120 to�144Glycemia, mg/dL ADA screening recommendationsFasting glucose �100 to�126Fasting insulin Elevated fasting insulin level, above
normal for gender, race, andpubertal status, is consideredevidence of insulin resistance
NHANES indicates National Health and Nutrition Examination Survey; ADA, American Diabetes Association.
TABLE 13-1 Evidence-Based Recommendations for Maternal Smoking Cessation
Smoking-cessation guidance during pregnancy is strongly advised Grade A, strongly recommendSupportive action:Pediatric care providers should be provided with appropriatetraining and materials to deliver, or refer to, a smoking-cessation program in the postpartum period for all smokingwomen of childbearing ageThis intervention should be directly linked to ongoing smoke-free home recommendations directed at all young mothers andfathers as described in the “Tobacco Exposure” section
Grades reflect the findings of the evidence review; recommendation levels reflect the consensus opinion of the expertpanel; and supportive actions represent expert consensus suggestions from the expert panel provided to supportimplementation of the recommendations (they are not graded).
SUPPLEMENT ARTICLES
PEDIATRICS Volume 128, Supplement 5, December 2011 S255 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

REFERENCES
1. NCEP Expert Panel of Blood Cholesterol Levelsin Children and Adolescents. National Choles-terol Education Program (NCEP): highlights ofthe report of the Expert Panel on Blood Cho-lesterol Levels in Children and Adolescents.Pediatrics. 1992;89(3):495–501
2. Strong JP, Malcom GT, McMahan CA, et al;Prevalence and extent of atherosclerosis inadolescents and young adults: implicationsfor prevention from the Pathobiological De-terminants of Atherosclerosis in YouthStudy. JAMA. 1999;281(3):495–501
3. Berenson GS, Srinivasan SR, Bao W, New-man WP III, Tracy RE, Wattigney WA. Associ-ation between multiple cardiovascular riskfactors and atherosclerosis in children andyoung adults. The Bogalusa Heart Study. NEngl J Med. 1998;338(23):1650–1656
4. Morrison JA, Friedman LA, Gray-McGuire C.Met-abolicsyndromeinchildhoodpredictsadultcar-diovascular disease 25 years later: the Prince-ton Lipid Research Clinics Follow-up Study.Pediatrics. 2007;120(2):340–345
5. McMahan CA, Gidding SS, Malcolm GT, et al.Pathobiological Determinants of Atherosclero-sis in Youth (PDAY) Research Group. Compari-sonof coronaryheartdiseaserisk factors inau-topsied young adults from the PDAY Study withliving young adults from the CARDIA study. Car-diovasc Pathol. 2007;16(3):151–158
6. Carnethon MR, Gulati M. Prevalence andcardiovascular disease correlates of lowcardiorespiratory fitness in adolescentsand adults. JAMA. 2005;294(23):2981–2988
7. Freedman DS, Mei Z, Srinivasan SR, BerensonGS,DietzWH.Cardiovascular risk factorsandex-cess adiposity among overweight children andadolescents: the Bogalusa Heart Study. J Pedi-atr. 2007;150(1):12–17
8. US Department of Agriculture; US Depart-ment of Health and Human Services. DietaryGuidelines for Americans, 2010. 7th ed.Washington, DC: US Government PrintingOffice; 2011
9. Expert Panel on Detection, Evaluation, andTreatment of High Blood Cholesterol inAdults. Executive summary of the Third Re-port of the National Cholesterol EducationProgram (NCEP) Expert Panel on Detection,Evaluation, and Treatment of High BloodCholesterol in Adults (Adult TreatmentPanel III). JAMA. 2001;285(19):2486–2497
10. Abrams SA. Dietary guidelines for calciumand vitamin D: a new era. Pediatrics. 2011;127(3):566–568
11. US Department of Health and Human Ser-vices. 2008 physical activity guidelines forAmericans. Available at: www.health.gov/paguidelinesAccessed November 2, 2011
12. US Department of Health and Human Ser-v ices . Treat ing tobacco use anddependence: 2008 update. Available at:www .ahrq . gov /pa th / tobacco .h tm#Accessed November 2, 2011
13. High Blood Pressure Education ProgramWorking Group on High Blood Pressure inChildren and Adolescents. The fourth reporton the diagnosis, evaluation, and treatmentof high blood pressure in children and ado-lescents. Pediatrics. 2004;114(2 suppl 4thReport):555–576
14. Ogden CL, Carroll MD, Flegal KM. Prevalence ofhighbodymass index inUSchildrenandadoles-cents, 2007–2008. JAMA. 2010;303(3):242–249
15. Kuczmarski RJ, Ogden CL, Grummer-StrawnLM, et al. CDC growth charts: United States.Adv Data. 2000;314: 1–27
16. Barlow SE; Expert Committee. Expert com-
mittee recommendations regarding theprevention, assessment, and treatment ofchild and adolescent overweight andobesity: summary report. Pediatrics. 2007;120(suppl 4):S164–S192
17. Kavey RE, Allada V, Daniels SR, et al; AmericanHeart Association Expert Panel on PopulationandPreventionScience; AmericanHeart Asso-ciation Council on Cardiovascular Disease inthe Young; American Heart Association Coun-cil on Epidemiology and Prevention; AmericanHeart Association Council on Nutrition, Physi-cal Activity and Metabolism; American HeartAssociation Council on High Blood PressureResearch; American Heart Association Coun-cil on Cardiovascular Nursing; AmericanHeart Association Council on the Kidney inHeart Disease; Interdisciplinary WorkingGroup on Quality of Care and Outcomes Re-search. Cardiovascular risk reduction in high-risk pediatric patients: a scientific statementfrom the American Heart Association ExpertPanel on Population and Prevention Science;the Councils on Cardiovascular Disease in theYoung, Epidemiology and Prevention, Nutri-tion, Physical Activity and Metabolism, HighBlood Pressure Research, CardiovascularNursing, and the Kidney in Heart Disease; andthe InterdisciplinaryWorkingGrouponQualityof Care and Outcomes Research: endorsed bythe American Academy of Pediatrics. Circula-tion. 2006;114(24):2710–2738
18. Type 2 diabetes in children and adoles-cents. Diabetes Care. 2000;23(3):381–389
19. Cook S; Auinger P; Li C; Ford ES. Metabolicsyndrome rates in United States adoles-cents, from the National Health and Nutri-tion Examination Survey, 1999–2002. J Pedi-atr. 2008;152(2):165–170
(Continued from first page)
Associates for the State of Ohio, Bureau of Early Intervention Services and Help Me Grow program, and has received funding/grant support for research from theNIH; Dr Kwiterovich has served as a consultant or advisory board member for Merck, Schering-Plough, Pfizer, Sankyo, LipoScience, and Astra Zeneca, has servedon speaker’s bureaus for Merck, Schering-Plough, Pfizer, Sankyo, Kos, and Astra Zeneca, and has received funding/grant support for research from Pfizer,Merck, GlaxoSmithKline, Sankyo, and Schering-Plough; Dr McBride has served as a consultant or advisory board member for Bristol-Myers Squibb and Merckand has served on speaker’s bureaus for Kos, Merck, and Pfizer but declares no relevant relationships since July 2007; Dr McCrindle has been a consultant forAbbott, Bristol-Myers Squibb, Daichii Sankyo, and Roche, owns stock in CellAegis and reports funding/grant support for research from Astra Zeneca, Sankyo,Merck, Schering-Plough, and the NIH; Dr Urbina reports funding/grant support for research from Merck, Schering-Plough, Sankyo, and the NIH; and Dr VanHornhas provided advice to Chartwells School Food Service and has received funding/grant support for research from General Mills and the NIH. Drs Benuck,Christakis, Dennison, O’Donnell, Rocchini, and Washington have indicated they have no financial relationships relevant to this article to disclose.
Funded by the National Institutes of Health (NIH).
S256 EXPERT PANEL by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2009-2107C; originally published online November 14, 2011; 2011;128;S213Pediatrics
HEALTH AND RISK REDUCTION IN CHILDREN AND ADOLESCENTSEXPERT PANEL ON INTEGRATED GUIDELINES FOR CARDIOVASCULAR
Reduction in Children and Adolescents: Summary ReportExpert Panel on Integrated Guidelines for Cardiovascular Health and Risk
ServicesUpdated Information &
_5/S213.full.htmlhttp://pediatrics.aappublications.org/content/128/Supplementincluding high resolution figures, can be found at:
References
_5/S213.full.html#ref-list-1http://pediatrics.aappublications.org/content/128/Supplementat:This article cites 16 articles, 5 of which can be accessed free
Citations
_5/S213.full.html#related-urlshttp://pediatrics.aappublications.org/content/128/SupplementThis article has been cited by 61 HighWire-hosted articles:
Subspecialty Collections
_subhttp://pediatrics.aappublications.org/cgi/collection/cardiologyCardiologythe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
mlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhttables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2011 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
DOI: 10.1542/peds.2009-2107C; originally published online November 14, 2011; 2011;128;S213Pediatrics
HEALTH AND RISK REDUCTION IN CHILDREN AND ADOLESCENTSEXPERT PANEL ON INTEGRATED GUIDELINES FOR CARDIOVASCULAR
Reduction in Children and Adolescents: Summary ReportExpert Panel on Integrated Guidelines for Cardiovascular Health and Risk
http://pediatrics.aappublications.org/content/128/Supplement_5/S213.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2011 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from


![Aterosclerose [ETEC KK]](https://static.fdocuments.net/doc/165x107/55b198a6bb61eb667f8b4748/aterosclerose-etec-kk.jpg)