Partial sublingual glandectomy with ranula excision: a · PDF file160 Partial sublingual...
6
160 Partial sublingual glandectomy with ranula excision: a new conservative method for treatment In-Kyo Chung 1 , Hyo-Ji Lee 1 , Dae-Seok Hwang 1 , Yong-Deok Kim 1 , Hae-Ryoun Park 2 , Sang-Hun Shin 1 , Uk-Kyu Kim 1 , Jae-Yeol Lee 1 Departments of 1 Oral and Maxillofacial Surgery, 2 Oral and Maxillofacial Pathology, School of Dentistry, Pusan National University, Yangsan, Korea Abstract (J Korean Assoc Oral Maxillofac Surg 2012;38:160-5) Objectives: This study evaluated the clinical results of partial sublingual glandectomy accompanying the excision of ranula as new treatment modality. Materials and Methods: A total of 43 patients who were treated between 1999 and 2007 for oral or plunging ranula were reviewed. All patients were treated surgically by various methods with a total of 55 different procedures performed. Ten cases of partial sublingual glandectomy with excision of the ranula were conducted. All excised specimens were examined. We compared the clinical outcomes resulting from each treatment method. Results: The recurrence rates for marsupialization, excision of ranula, marsupialization with gauze packing, total excision of sublingual gland and ranula, and partial sublingual glandectomy with excision of ranula were 50%, 25%, 25%, 0% and 10%, respectively. Of the 10 patients treated by partial sublingual glandectomy with ranula excision, only one experienced recurrence (10%), i.e., plunging ranula. None of the ranulas contained an epithelial lining, and the excised portion of the feeding sublingual glands showed degenerative changes. Conclusion: In removal of ranulas, we found that excision of the attached sublingual gland, which removed the feeding portion and degenerative acinar cells, yielded good outcomes. Thus, as a new conservative method for treatment, we recommend partial sublingual glandectomy to accompany excision of the ranula. Key words: Ranula, Sublingual gland, Treatment outcome [paper submitted 2012. 2. 6 / revised 2012. 3. 15 / accepted 2012. 3. 16] of Rivini and Wharton ducts have been reported 1 . In this case, a true epithelial lining made of the epithelium of the duct was detected. When a ranula spreads out from the posterior inferior area of the mylohyoid muscle to the submental area or cervical area, it is known as a plunging ranula. In general, ranulas appear as a bluish dome-shaped swelling on the floor of the mouth. When mucoceles accumulate in the subcutaneous area or near the epidermis area, a ranula appears as a light bluish color because of epidermal cyanosis and retained saliva in the subcutaneous area. When a ranula exists in the deeper areas, however, the mucosa appears as an ordinary pinkish color. A ranula does not cause serious symptoms of pain except some discomfort, and it hardly gives rise to any severe clinical manifestation. According to Baurmash 1 , clinical findings such as discomfort in speech, mastication, and swallowing and external swelling differ depending on the size and location of the ranula. In the case of a very large mucocele in the sublingual gland, the tongue may compress I. Introduction A ranula is a mucocele occurring on the floor of the mouth and is derived either from the extravasation of saliva out of the salivary ducts or retention of saliva inside the salivary ducts, originating in the minor salivary gland or the sublingual gland as one of the major salivary glands 1,2 . In general, a ranula is known as an extravasation phenomenon of the sublingual gland 3-6 . It looks like a cystic lesion, but it is a pseudocyst without epithelial lining 3,7-12 . Note, however, that there have been few cases wherein mucus retention cysts Jae-Yeol Lee Department of Oral and Maxillofacial Surgery, Pusan National University Hospital, 179 Gudeok-ro, Seo-gu, Busan 602-739, Korea TEL: +82-51-240-7432 FAX: +82-51-231-7429 E-mail: id9753153@gmail.com This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. CC ORIGINAL ARTICLE http://dx.doi.org/10.5125/jkaoms.2012.38.3.160 pISSN 2234-7550 · eISSN 2234-5930
Transcript of Partial sublingual glandectomy with ranula excision: a · PDF file160 Partial sublingual...

160
Partial sublingual glandectomy with ranula excision: a new conservative method for treatment
In-Kyo Chung1, Hyo-Ji Lee1, Dae-Seok Hwang1, Yong-Deok Kim1,
Hae-Ryoun Park2, Sang-Hun Shin1, Uk-Kyu Kim1, Jae-Yeol Lee1
Departments of 1Oral and Maxillofacial Surgery, 2Oral and Maxillofacial Pathology, School of Dentistry, Pusan National University, Yangsan, Korea
Abstract (J Korean Assoc Oral Maxillofac Surg 2012;38:160-5)
Objectives: This study evaluated the clinical results of partial sublingual glandectomy accompanying the excision of ranula as new treatment modality.Materials and Methods: A total of 43 patients who were treated between 1999 and 2007 for oral or plunging ranula were reviewed. All patients were treated surgically by various methods with a total of 55 different procedures performed. Ten cases of partial sublingual glandectomy with excision of the ranula were conducted. All excised specimens were examined. We compared the clinical outcomes resulting from each treatment method.Results: The recurrence rates for marsupialization, excision of ranula, marsupialization with gauze packing, total excision of sublingual gland and ranula, and partial sublingual glandectomy with excision of ranula were 50%, 25%, 25%, 0% and 10%, respectively. Of the 10 patients treated by partial sublingual glandectomy with ranula excision, only one experienced recurrence (10%), i.e., plunging ranula. None of the ranulas contained an epithelial lining, and the excised portion of the feeding sublingual glands showed degenerative changes.Conclusion: In removal of ranulas, we found that excision of the attached sublingual gland, which removed the feeding portion and degenerative acinar cells, yielded good outcomes. Thus, as a new conservative method for treatment, we recommend partial sublingual glandectomy to accompany excision of the ranula.
Key words: Ranula, Sublingual gland, Treatment outcome[paper submitted 2012. 2. 6 / revised 2012. 3. 15 / accepted 2012. 3. 16]
ofRiviniandWhartonductshavebeenreported1.Inthiscase,
a trueepithelial liningmadeof theepitheliumoftheduct
wasdetected.Whenaranulaspreadsoutfromtheposterior
inferiorareaof themylohyoidmuscle to the submental
areaorcervicalarea, it isknownasaplungingranula.In
general, ranulasappearasabluishdome-shapedswelling
onthefloorofthemouth.Whenmucocelesaccumulatein
thesubcutaneousareaorneartheepidermisarea,aranula
appearsasalightbluishcolorbecauseofepidermalcyanosis
andretainedsalivainthesubcutaneousarea.Whenaranula
existsinthedeeperareas,however,themucosaappearsasan
ordinarypinkishcolor.
Aranuladoesnotcauseserioussymptomsofpainexcept
somediscomfort, and ithardlygives rise toanysevere
clinicalmanifestation.According toBaurmash1,clinical
findingssuchasdiscomfort in speech,mastication,and
swallowingandexternalswellingdifferdependingonthe
sizeandlocationoftheranula.Inthecaseofaverylarge
mucoceleinthesublingualgland,thetonguemaycompress
I. Introduction
Aranula is amucoceleoccurringon the floorof the
mouthandisderivedeitherfromtheextravasationofsaliva
outof thesalivaryductsor retentionofsaliva inside the
salivaryducts,originatingintheminorsalivaryglandorthe
sublingualglandasoneof themajorsalivaryglands1,2. In
general,aranulaisknownasanextravasationphenomenon
ofthesublingualgland3-6.Itlookslikeacysticlesion,butit
isapseudocystwithoutepitheliallining3,7-12.Note,however,
thattherehavebeenfewcaseswhereinmucusretentioncysts
Jae-Yeol LeeDepartment of Oral and Maxillofacial Surgery, Pusan National University Hospital, 179 Gudeok-ro, Seo-gu, Busan 602-739, KoreaTEL: +82-51-240-7432 FAX: +82-51-231-7429E-mail: [email protected]
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
CC
ORIGINAL ARTICLEhttp://dx.doi.org/10.5125/jkaoms.2012.38.3.160
pISSN 2234-7550·eISSN 2234-5930

Partial sublingual glandectomy with ranula excision: a new conservative method for treatment
161
52surgical treatmentswereperformedonthe43patients.
(Table1)Mucoceles inareasother than the floorof the
mouthandoccurrencesontheWharton’sductwereexcluded.
Basedonthemedicalrecords,weinvestigatedthediagnosis,
treatment,statusofrelapse,andcomplications.Theresults
ofeachsurgicalprocedurewerereviewed,andweassessed
theclinicalresultsofpartialsublingualglandectomywith
theexcisionof the ranula incomparisonwith theother
methodsused.Histologicalexaminationswereperformedon
allexcisedspecimens.Eachranulawascompletelyexcised,
exceptinthecaseofmarsupialization.Thefollow-upperiod
wasfromatleastsixmonthsuptotwoyears.
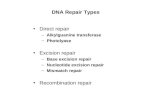
Among the43patients, 10were treatedwithpartial
sublingualglandectomywithexcisionoftheranula.Surgery
wasperformedundergeneralanesthesia.Ellipticalincision
wasmadeonthemucosaof theranula.Meticulous,blunt
dissectionwasperformedalongwiththepseudocystupto
thesublingualgland.Whendissectionreachedthebodyof
thesublingualglandsecretingtheranula,thelocationofthe
attachmentportionof thesublingualglandwasconfirmed
andexcisedfor1-1.5cm.(Fig.1)Theresectedmarginofthe
sublingualglandwassuturedwith4-0non-absorbablesilk,
andtheincisedmucosawasclosedusingageneralmethod.
Theotherproceduresused-exceptpartialglandectomy-
werecarriedoutusingordinarymethods.
III. Results
Atleast39and4patientswerediagnosedwithranulason
thefloorof themouthandplungingranulas,respectively.
theranuladuringeatingandswallowingsuchthat thereis
interferencewith thesalivaryflowof thesubmandibular
gland.Whenaplunging ranula increases insize, itmay
causedyspneaanddysphagiaandmayexpandasfarasthe
mediastinum13.Thereareseveralsurgicalmethodsfor the
treatmentofranulas,withvaryingcurerate7,8,14.Although
asimpletechnique,marsupializationhasbeenreportedto
haveahighrecurrencerate.Tominimizeanyrecurrence,
Baurmash2proposedmarsupializationwithgauzepacking
andsuggestedthattheremovaloftheentiresublingualgland
couldbeovertreatment insomecases. Incontrast, there
havebeenseveral reportsof theextirpationof theentire
sublingualgland,recordingarelativelyhighcurerate.Thus,
theremovalof theentiresublingualgland isproposed to
minimizeanyrecurrence7,8,11,14-16.Note,however, that the
completeremovalofthesublingualglandmayinvolvethe
functionaldeteriorationofthesalivaryglandsandincrease
thepossibilityofdamage to theWharton’sduct, lingual
nerves,andbloodvessels6,16.
Inthisresearch,wehaveinvestigatedtheusefulnessofa
procedureinvolvingthesimultaneouspartialremovalofa
damagedareaofthesublingualglandwiththeexcisionofthe
ranula.Thismethodmaintainsthefunctionofthesublingual
glandandminimizestherecurrencerate.Here,wedescribe
partialsublingualglandectomywiththeexcisionoftheranula
asanewtreatmentmodelandcompareitwithothersurgical
procedures.
II. Materials and Methods
Retrospectiveevaluationwasperformedon43consecutive
patientsdiagnosedwith ranulasduring theperiod1999-
2007at theauthors’ institution.Thepatients’agesranged
from3to75years,withaverageageof21years.Atotalof
Table 1. Surgical methods and recurrence rates
OperationtypeNumberof
operationcasesNumberofrecurrences
Recurrencerate(%)
ExcisionofranulaMarsupializationMarsupializationwithgauzepackingTotalexcisionofsublingualglandandranulaPartialsublingualglandectomywithexcisionofranulaTotal
24104
4
10
52
651
0
1
13
25.050.025.0
0
10.0
25.0
In-Kyo Chung et al: Partial sublingual glandectomy with ranula excision: a new conser-vative method for treatment. J Korean Assoc Oral Maxillofac Surg 2012
Fig. 1. Partial sublingual glandectomy with excision of ranula.In-Kyo Chung et al: Partial sublingual glandectomy with ranula excision: a new conser-vative method for treatment. J Korean Assoc Oral Maxillofac Surg 2012

J Korean Assoc Oral Maxillofac Surg 2012;38:160-5
162
ranula,andtheconditionwasresolved.
Inonecaseofexcisionoftheranula,thepatientcomplained
ofparethesiaontheipsilateralsideofthetongueimmediately
afterthesurgery,butthesymptomswereresolvedtwoweeks
laterwithnofurther treatment.Other thanpost-operative
swellingordiscomfort,noothercomplicationswerefound.
Accordingto thehistological tests,nolesionswith true
epithelial liningwerefound.Themucuscavitywas lined
withlooseconnectivetissueandgranulationtissue.These
showedfibroustissue,inflammatorycells,foamyhistiocytes,
andlymphocytesintheconnectivetissue.Degenerationof
aciniccells frompartiallyexcisedsublingualglandsand
dilationoftheductwereobserved.(Fig.3)Inflammationand
degenerationweredetectedinthesublingualglandadjacent
totheranula.
IV. Discussion
Ranulaisaclinicaltermdenotingamucoceleoccurringon
thefloorofthemouth.Theetiologyofaranulaisdiscussed
Therewere24casesofexcisionoftheranula,10casesof
marsupialization,4casesofmarsupializationwithgauze
packing,4casesoftotalexcisionofthesublingualglandand
ranula,and10casesofpartialsublingualglandectomywith
excisionoftheranula.Therecurrencerateswere25%,50%,
25%,0%,and10%,respectively.
Eightpatientsunderwentpartialsublingualglandectomy
withexcisionoftheranulaasthefirstoperation,andoneof
thepatientssufferedfromrecurrence.(Table2)Thismale
patientwas3yearsoldandwasdiagnosedwitharanulaat
thefirstvisit.Onemonthafterthesurgery,thepatienthada
recurrentlesion.Thepatientwasrediagnosedwithaplunging
ranulaandsubsequently treatedwith totalexcisionof the
sublingualglandandranula.
Intwoofthepatientswhowereeachtreatedwithexcision
oftheranulaandmarsupializationinthefirstsurgery,ranulas
recurredonemonthlater.Thesepatientswereoperatedon
usingpartialsublingualglandectomy(Fig.2),andneither
sufferedfromrecurrence.Therecurrentlesionsweretreated
withpartialsublingualglandectomywithexcisionof the
Table 2. Partial sublingual glandectomy with excision of ranula
Case Gender/age Dx. Site 1stoperation 2ndoperation1 Result
12345678910
Male/3Male/5Male/6Male/8Female/8Female/8Female/14Female/75Female/22Female/30
PlungingranulaRanulaRanulaRanulaRanulaRanulaRanulaRanulaRanulaRanula
Lt.Lt.Rt.Rt.Lt.Rt.Rt.Rt.Rt.Lt.
PSGPSGPSGPSGPSGPSGPSGPSGEM
TENNNNNNNPSGPSG
N
NN
(Dx.:diagnosis,Lt.:left,Rt.:right,PSG:partialsublingualglandectomywithexcisionofranula,E:excisionofranula,M:marsupialization,TE:totalexcisionofsublingualglandandranula,N:norecurrence)1inrecurrencecasesafterthe1stoperation.In-Kyo Chung et al: Partial sublingual glandectomy with ranula excision: a new conservative method for treatment. J Korean Assoc Oral Maxillofac Surg 2012
Fig. 2. Gross findings of excised ranula and excised portion of sublingual gland. Solid arrow: ranula, hollow arrow: atta-ched sublingual gland.In-Kyo Chung et al: Partial sublingual glandectomy with ranula excision: a new conservative method for treatment. J Korean Assoc Oral Maxillofac Surg 2012

Partial sublingual glandectomy with ranula excision: a new conservative method for treatment
163
thelesionisalsosmall8.Thecommonformofaranulaisa
pseudocystderivedfromtheextravasationofthesublingual
gland3-17.Thereasonfortheextravasationisconsideredto
betraumatothesublingualglandandrelatedstructure1,7,8.
in termsofductalobstructionanddamageof thesalivary
duct17.The retentionofmucusandductaldilationoccur
withtheobstructionofthisduct.Theresultisanepithelial-
linedcyst.Observationof thesecases is rare; thesizeof
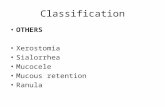
Fig. 3. Histopathologic features of ranula. A, B. A cystic cavity is surrounded by loose connective tissue or granulation tissue (H&E staining, A: ×50, B: ×120). Adjacent feeding sublingual gland (arrow) is seen near the cavity. C. The cystic wall is composed of numerous inflammatory cells, foamy histiocytes, lymphocytes, and fibrous tissue (H&E staining, ×150). D, E. In the sublingual gland, acinic cells show degenerative change (H&E staining, ×400). F. Ducts (arrows) are dilated and degenerated (H&E staining, ×500). In-Kyo Chung et al: Partial sublingual glandectomy with ranula excision: a new conservative method for treatment. J Korean Assoc Oral Maxillofac Surg 2012

J Korean Assoc Oral Maxillofac Surg 2012;38:160-5
164
of thesublingualgland.Baurmash5 insists that the total
excisionofthesublingualglandisnotappropriateforsmall-
sizedranulasandsuggestsamodifiedmarsupializationwith
gauzepacking.Baurmashused thismethodon12cases,
with1caseofrecurrencereported.AccordingtoBaurmash,
however,marsupializationcannotresolveranulasassociated
with thedeeppartof the sublingualgland. Inaddition,
marsupialization(eitheronceorrepeated)cancausefibrosis
oftheupperside;thus,mucuscanbeinducedinthelower
partofthelesion,resultinginaplungingranulaincaseof
recurrence15.
Tosummarizetheviewpointof thehealingprocess, the
previouslyreviewedtreatmentmethodcanbecategorized
asfollows:chronicfistulizationofthelesion;sealingofthe
feederbase;excisionof theranulaonly,and; removalof
thesublingualsalivaryglandastheorigin.Marsupialization
formsachronicfistulabetween themucussecretionpart
andtheoralcavity.Note,however,thatmostranulasdonot
haveatrueepithelial lining;thus,achronicfistulacannot
beestablished8,11.Consequently,thereisrecurrencewiththe
healingoftheoralepithelium.Thetechniqueofsealingthe
feederbaseinducesatrophyandfibrosisofthedamagedpart
ofthesublingualgland.Marsupializationwithgauzepacking,
cauterizationusingCO2laser20,21,andinjectionofpicibanil(OK-
432)22,23fallunderthiscategory.Marsupializationaccompanied
bygauzepackingmaintainsachanneltotheoralcavityand
allowstimeforfibrosisofthemucussecretionarea;henceits
lowerrecurrenceratethansimplemarsupialization.Similarly,
fibrosisandsclerosisofthemucussecretionpartareinduced
byCO2laserandinjectionofOK-432.Inthistrial,however,
thepossibilityofrecurrencestillexistsbecausethedamaged
partof thesublingualglandisnotexcised.Theprocedure
fortheexcisionoftheranulaonlyremovesthecyst,soithas
ablindpoint,i.e.,itcanmissthefeedergland.Theremoval
ofthesublingualglandasthesourceofthepseudocystisa
radicaltreatment;henceitspotentialcomplications.
Partialsublingualglandectomywithexcisionoftheranula
Whentheaciniccellsaredamagedbytrauma,salivaleaks
into adjacent tissueand formsa cystic cavity linedby
granulation tissuesurroundedby looseconnective tissue.
Manystudieshaveconfirmedthattheexcisedranulahasno
trueepithelial lining3,7-11.Theetiologyforaranula isstill
notclear,however1,18.Inthisresearch,nolesionswithtrue
epithelialliningwereobserved;thus,ranulasarethoughtto
beanextravasationphenomenonofthesublingualgland.
Therehavebeenseveralmethodsusedforthetreatment
ofranulas,butpropermodalityisstillasubjectofdebate
becauseofthetendencytowardrecurrence.Therecurrence
ratesinliteraturearesummarizedinTable3,decreasingin
thefollowingorder:marsupialization,excisionofranula,and
excisionofthesublingualgland.Zhaoetal.14statedthatthe
recurrenceratesofranulaswerenotrelatedtothepatternsof
lesionbutwerecloselyrelatedtothemethodofthesurgical
procedureused.Crysdaleetal.8suggestedexcisionof the
sublingualgland for ranulas>1cm.Catoneet al.11 and
Bridgeretal.15proposedexcisionofthesublingualglandas
theprimarytreatmentforallranulasregardlessofsize.
Becauseof its simplicityandcomplicationsafter the
excisionof thesublingualgland,manycliniciansprefer
marsupializationas thefirst treatment16,19.Complications
associatedwith thesurgicalmanagementof ranulashave
beeninvestigatedbyZhaoetal.16.Accordingtothem,the
mostfrequentcomplicationsaretherecurrenceoflesionand
numbnessofthetongueduetodamagetothelingualnerve.
Damage to theWhartonduct,hemorrhaging,hematoma,
wounddehiscence,andinfectionhavebeenreportedaswell.
Recurrencewasfrequentinthemarsupializationandexcision
of theranula.Injurytoadjacent tissuewasrelatedmainly
totheexcisionofthesublingualgland.Note,however,that
thesecomplicationsafter theexcisionof theranulawere
temporaryandwereresolvedwithinagiventimeframe.Thus,
tominimizerecurrenceasthemostcommoncomplication,
theremovalofthesublingualglandhasbeensuggested.
Somecliniciansarestillskepticalastothetotalremoval
Table 3. Recurrence rates (%) and number of cases inliterature
I&D M MP E ESG
Crysdaleetal.8
Yoshimuraetal.7
Zhaoetal.14
ChidzongaandMahomva19
100(4)---
61(19)36.4(22)66.67(9)
20(10)
0(2)---
0(4)25(4)
57.69(26)-
0(11)0(9)
1.05-1.55(415)0(73)
(I&D:incisionanddrainage,M:marsupialization,MP:marsupializationwithgauzepacking,E:excisionofranula,ESG:excisionofsublingualgland)Valuesarepresentedas%(number).In-Kyo Chung et al: Partial sublingual glandectomy with ranula excision: a new conservative method for treatment. J Korean Assoc Oral Maxillofac Surg 2012

Partial sublingual glandectomy with ranula excision: a new conservative method for treatment
165
TetsumuraA,etal.MRIofranulas.Neuroradiology2000;42:917-22.
4. ShelleyMJ,YeungKH,BowleyNB,SneddonKJ.Ararecaseofanextensiveplungingranula:discussionofimaging,diagnosis,andmanagement.OralSurgOralMedOralPatholOralRadiolEndod2002;93:743-6.
5. BaurmashHD.Marsupializationfor treatmentoforalranula:asecondlookat theprocedure.JOralMaxillofacSurg1992;50:1274-9.
6. BaurmashHD.Treatingoralranula:anothercaseagainstblanketremovalof the sublingualgland.Br JOralMaxillofacSurg2001;39:217-20.
7. YoshimuraY,ObaraS,KondohT,NaitohS.Acomparisonofthreemethodsusedfortreatmentofranula.JOralMaxillofacSurg1995;53:280-2.
8. CrysdaleWS,MendelsohnJD,ConleyS.Ranulas--mucocelesof theoral cavity: experience in26children.Laryngoscope1988;98:296-8.
9. GallowayRH,GrossPD,ThompsonSH,PattersonAL.Pathogenesisandtreatmentofranula:reportofthreecases.JOralMaxillofacSurg1989;47:299-302.
10. MoritaY,SatoK,KawanaM,TakahasiS,IkarashiF.Treatmentofranula--excisionofthesublingualglandversusmarsupialization.AurisNasusLarynx2003;30:311-4.
11. CatoneGA,MerrillRG,HennyFA.Sublingualglandmucus-escapephenomenon--treatmentbyexcisionofsublingualgland.JOralSurg1969;27:774-86.
12. BarnesL.Surgicalpathologyoftheheadandneck.1sted.NewYork:MarcelDekker;1985:1297-301.
13. MarxRE,SternD.Oralandmaxillofacialpathology. Illinois:QuintessencePublishing;2003:511.
14. ZhaoYF,JiaY,ChenXM,ZhangWF.Clinicalreviewof580ranulas.OralSurgOralMedOralPatholOralRadiolEndod2004;98:281-7.
15. BridgerAG,CarterP,BridgerGP.Plungingranula: literaturereviewandreportofthreecases.AustNZJSurg1989;59:945-8.
16. ZhaoYF,JiaJ, JiaY.Complicationsassociatedwithsurgicalmanagementofranulas.JOralMaxillofacSurg2005;63:51-4.
17. QuickCA,LowellSH.Ranulaandthesublingualsalivaryglands.ArchOtolaryngol1977;103:397-400.
18. HarrisonJD,GarrettJR.Anultrastructuralandhistochemicalstudyofanaturallyoccurringsalivarymucoceleinacat.JCompPathol1975;85:411-6.
19. ChidzongaMM,MahomvaL.Ranula:experiencewith83casesinZimbabwe.JOralMaxillofacSurg2007;65:79-82.
20. FrameJW.Removaloforalsoft tissuepathologywiththeCO2laser.JOralMaxillofacSurg1985;43:850-5.
21. MintzS,BarakS,Horowitz I.Carbondioxide laserexcisionandvaporizationofnonplungingranulas:acomparisonof twotreatmentprotocols.JOralMaxillofacSurg1994;52:370-2.
22. WooJS,HwangSJ,LeeHM.RecurrentplungingranulatreatedwithOK-432.EurArchOtorhinolaryngol2003;260:226-8.
23. FukaseS,OhtaN,InamuraK,AoyagiM.TreatmentofranulawthintracysticinjectionofthestreptococcalpreparationOK-432.AnnOtolRhinolLaryngol2003;112:214-20.
24. MartisC.Parotidbenigntumors:commentsonsurgicaltreatmentof263cases.IntJOralSurg1983;12:211-20.
25. MilsteinBB.Regenerationinthesubmaxillaryglandoftherat.BrJExpPathol1950;31:664-9.
26. HanksCT,ChaudhryAP.Regenerationofratsubmandibularglandfollowingpartialextirpation.Alightandelectronmicroscopicstudy.AmJAnat1971;130:195-207.
cansatisfymanyoftherequirementsdiscussedabove.First,
itremovestheranulalesionaswellastheoriginofthelesion
byexcisingthemucus-supplyingpartofthesublingualgland.
Suturingof theexcisedmarginof thesublingualglandis
intendedtosealthefeederbase.Furthermore,thesublingual
glandhasseveralsecretionductsthatopenindependently;
thus, functional recoveryof thesublingualglandcanbe
expectedevenafter theexcisionofpartof thesublingual
gland.Inaddition, it isnoninvasivecomparedtothetotal
extirpationofthesublingualgland,andsoitisexpectedto
havefewercomplications.
Partialglandectomyismainlyapplied tooperationson
theparotidgland,andsuperficialparotidectomyispracticed
widely.Partialsuperficialparotidectomyhasbeenintroduced
as amoreconservativemethod than superficialparoti-
dectomy24.Thispartialsalivaryglandectomyisbasedonthe
regenerativeabilityofthesalivaryglands,andthehealing
procedureofdamagedsalivaryglandsofrodentshasbeen
reported25,26.Note,however,thattherehavebeennoreports
onpartialsublingualglandectomy.Similartotheregeneration
ofparotidglands, sublingualglandsareexpected togo
throughasimilarhealingprocedure.
V. Conclusion
Inthisstudy,wehaveshownthatpatientswhounderwent
partialsublingualglandectomywiththeexcisionofaranula
recoveredwithoutanynoticeablecomplicationandwithlow
recurrencerate.
Therefore,partialsublingualglandectomywithexcisionof
theranulahasvalueinclinicalpracticeasanewconservative
method.Nonetheless,thenumberofcasesinthisresearchis
stillsmall,sofurtherinvestigationsareneeded.Moreover,
furtherresearchonfactorssuchastheamountofexcision,
functionalrecovery,andchangeinthepatternofsublingual
glandsafterpartialexcisionisrequired.
References
1. BaurmashHD.Mucocelesandranulas.JOralMaxillofacSurg2003;61:369-78.
2. BaurmashHD.Acaseagainstsublingualglandremovalasprimarytreatmentofranulas.JOralMaxillofacSurg2007;65:117-21.
3. KurabayashiT,IdaM,YasumotoM,OhbayashiN,YoshinoN,