Pancreatitis v2.0: Initial Management - Seattle Children's · For questions concerning this...
13
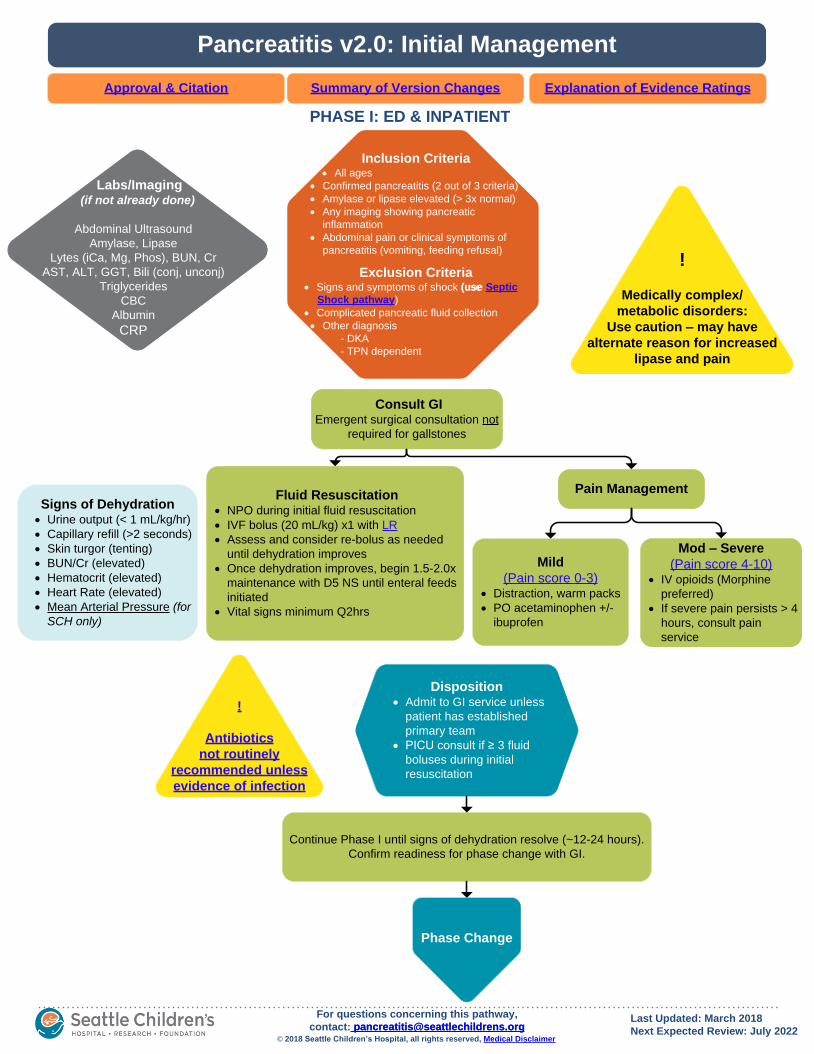
Pain Management PHASE I: ED & INPATIENT Inclusion Criteria · All ages · Confirmed pancreatitis (2 out of 3 criteria) · Amylase or lipase elevated (> 3x normal) · Any imaging showing pancreatic inflammation · Abdominal pain or clinical symptoms of pancreatitis (vomiting, feeding refusal) Exclusion Criteria · Signs and symptoms of shock (use · Complicated pancreatic fluid collection · Other diagnosis - DKA - TPN dependent Pancreatitis v2.0: Initial Management Explanation of Evidence Ratings Summary of Version Changes Last Updated: March 2018 Next Expected Review: July 2022 © 2018 Seattle Children’s Hospital, all rights reserved, Medical Disclaimer For questions concerning this pathway, contact: [email protected] Approval & Citation Fluid Resuscitation · NPO during initial fluid resuscitation · IVF bolus (20 mL/kg) x1 with LR · Assess and consider re-bolus as needed until dehydration improves · Once dehydration improves, begin 1.5-2.0x maintenance with D5 NS until enteral feeds initiated · Vital signs minimum Q2hrs Mild (Pain score 0-3) · Distraction, warm packs · PO acetaminophen +/- ibuprofen Mod – Severe (Pain score 4-10) · IV opioids (Morphine preferred) · If severe pain persists > 4 hours, consult pain service Phase Change Disposition · Admit to GI service unless patient has established primary team · PICU consult if ≥ 3 fluid boluses during initial resuscitation Labs/Imaging (if not already done) Abdominal Ultrasound Amylase, Lipase Lytes (iCa, Mg, Phos), BUN, Cr AST, ALT, GGT, Bili (conj, unconj) Triglycerides CBC Albumin CRP Consult GI Emergent surgical consultation not required for gallstones Signs of Dehydration · Urine output (< 1 mL/kg/hr) · Capillary refill (>2 seconds) · Skin turgor (tenting) · BUN/Cr (elevated) · Hematocrit (elevated) · Heart Rate (elevated) · Mean Arterial Pressure (for SCH only) ! Antibiotics not routinely recommended unless evidence of infection Continue Phase I until signs of dehydration resolve (~12-24 hours). Confirm readiness for phase change with GI. ! Medically complex/ metabolic disorders: Use caution – may have alternate reason for increased lipase and pain · IVF bolus (20 mL/kg) x1 with LR [email protected] (use Septic Shock pathway)
Transcript of Pancreatitis v2.0: Initial Management - Seattle Children's · For questions concerning this...
Pain Management
PHASE I: ED & INPATIENT
Inclusion Criteria· All ages
· Confirmed pancreatitis (2 out of 3 criteria)
· Amylase or lipase elevated (> 3x normal)
· Any imaging showing pancreatic
inflammation
· Abdominal pain or clinical symptoms of
pancreatitis (vomiting, feeding refusal)
Exclusion Criteria· Signs and symptoms of shock (use
· Complicated pancreatic fluid collection
· Other diagnosis
- DKA
- TPN dependent
Pancreatitis v2.0: Initial Management
Explanation of Evidence RatingsSummary of Version Changes
Last Updated: March 2018
Next Expected Review: July 2022© 2018 Seattle Children’s Hospital, all rights reserved, Medical Disclaimer
For questions concerning this pathway,
contact: [email protected]
Approval & Citation
Fluid Resuscitation· NPO during initial fluid resuscitation
· IVF bolus (20 mL/kg) x1 with LR
· Assess and consider re-bolus as needed
until dehydration improves
· Once dehydration improves, begin 1.5-2.0x
maintenance with D5 NS until enteral feeds
initiated
· Vital signs minimum Q2hrs
Mild
(Pain score 0-3)· Distraction, warm packs
· PO acetaminophen +/-
ibuprofen
Mod – Severe
(Pain score 4-10)· IV opioids (Morphine
preferred)
· If severe pain persists > 4
hours, consult pain
service
Phase Change
Disposition· Admit to GI service unless
patient has established
primary team
· PICU consult if ≥ 3 fluid
boluses during initial
resuscitation
Labs/Imaging(if not already done)
Abdominal Ultrasound
Amylase, Lipase
Lytes (iCa, Mg, Phos), BUN, Cr
AST, ALT, GGT, Bili (conj, unconj)
Triglycerides
CBC
Albumin
CRP
Consult GIEmergent surgical consultation not
required for gallstones
Signs of Dehydration· Urine output (< 1 mL/kg/hr)
· Capillary refill (>2 seconds)
· Skin turgor (tenting)
· BUN/Cr (elevated)
· Hematocrit (elevated)
· Heart Rate (elevated)
· Mean Arterial Pressure (for
SCH only)
!
Antibiotics
not routinely
recommended unless
evidence of infection
Continue Phase I until signs of dehydration resolve (~12-24 hours).
Confirm readiness for phase change with GI.
!
Medically complex/
metabolic disorders:
Use caution – may have
alternate reason for increased
lipase and pain
· IVF bolus (20 mL/kg) x1 with LR
(use Septic
Shock pathway)
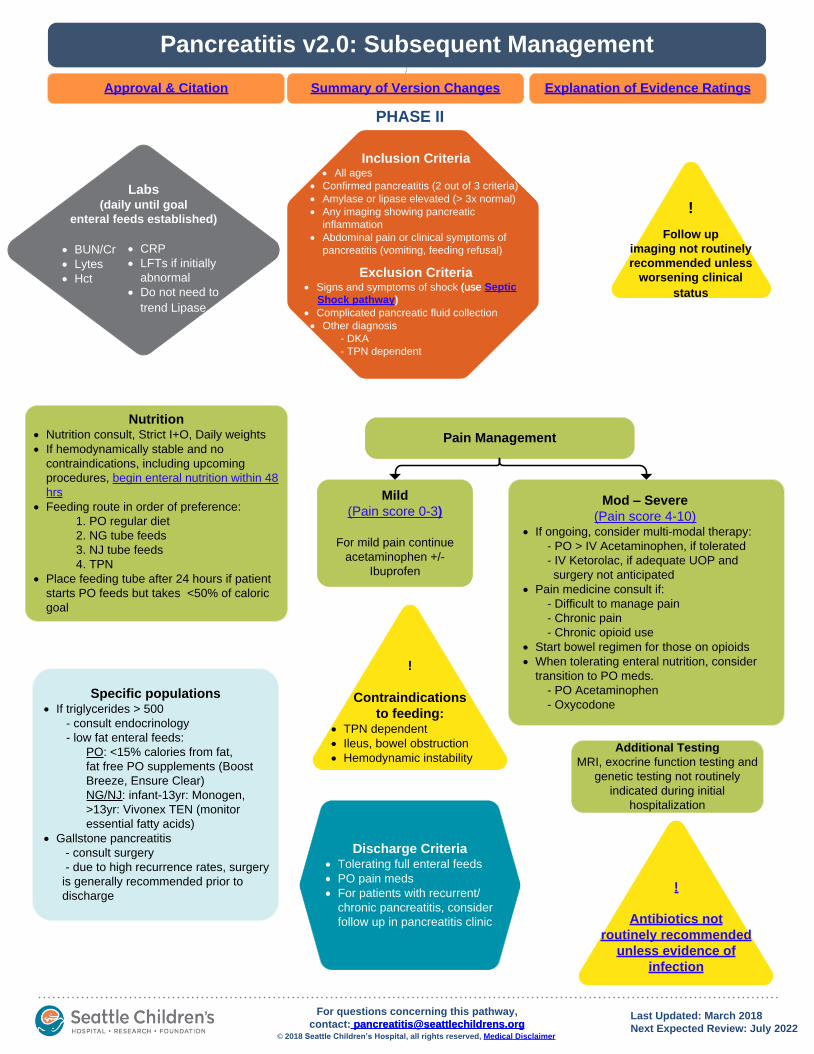
PHASE II
Pancreatitis v2.0: Subsequent Management
Explanation of Evidence RatingsSummary of Version ChangesApproval & Citation
Nutrition· Nutrition consult, Strict I+O, Daily weights
· If hemodynamically stable and no
contraindications, including upcoming
procedures, begin enteral nutrition within 48
hrs
· Feeding route in order of preference:
1. PO regular diet
2. NG tube feeds
3. NJ tube feeds
4. TPN
· Place feeding tube after 24 hours if patient
starts PO feeds but takes <50% of caloric
goal
Pain Management
!
Antibiotics not
routinely recommended
unless evidence of
infection
Discharge Criteria· Tolerating full enteral feeds
· PO pain meds
· For patients with recurrent/
chronic pancreatitis, consider
follow up in pancreatitis clinic
Last Updated: March 2018
Next Expected Review: July 2022© 2018 Seattle Children’s Hospital, all rights reserved, Medical Disclaimer
For questions concerning this pathway,
contact: [email protected]
Specific populations· If triglycerides > 500
- consult endocrinology
- low fat enteral feeds:
PO: <15% calories from fat,
fat free PO supplements (Boost
Breeze, Ensure Clear)
NG/NJ: infant-13yr: Monogen,
>13yr: Vivonex TEN (monitor
essential fatty acids)
· Gallstone pancreatitis
- consult surgery
- due to high recurrence rates, surgery
is generally recommended prior to
discharge
Additional Testing
MRI, exocrine function testing and
genetic testing not routinely
indicated during initial
hospitalization
!
Contraindications
to feeding:· TPN dependent
· Ileus, bowel obstruction
· Hemodynamic instability
Mild
(Pain score 0-3)
For mild pain continue
acetaminophen +/-
Ibuprofen
Mod – Severe
(Pain score 4-10)· If ongoing, consider multi-modal therapy:
- PO > IV Acetaminophen, if tolerated
- IV Ketorolac, if adequate UOP and
surgery not anticipated
· Pain medicine consult if:
- Difficult to manage pain
- Chronic pain
- Chronic opioid use
· Start bowel regimen for those on opioids
· When tolerating enteral nutrition, consider
transition to PO meds.
- PO Acetaminophen
- Oxycodone
!
Follow up
imaging not routinely
recommended unless
worsening clinical
status
Labs (daily until goal
enteral feeds established)
· BUN/Cr
· Lytes
· Hct
· CRP
· LFTs if initially
abnormal
· Do not need to
trend Lipase
Inclusion Criteria· All ages
· Confirmed pancreatitis (2 out of 3 criteria)
· Amylase or lipase elevated (> 3x normal)
· Any imaging showing pancreatic
inflammation
· Abdominal pain or clinical symptoms of
pancreatitis (vomiting, feeding refusal)
Exclusion Criteria· Signs and symptoms of shock (use
· Complicated pancreatic fluid collection
· Other diagnosis
- DKA
- TPN dependent
(use Septic
Shock pathway)
Lactated Ringers
Isotonic fluid type for fluid resuscitation:
Lactated ringers (LR) is recommended as the initial infusion solution for AP
based on 2 randomized controlled trials (pediatrics not specified) favoring
reduction of inflammation versus normal saline (NS). [LOE: Low
quality] (#45 Yokoe 2015) (#152 Working Group IAP/APA 2013)
Conditional recommendation made in favor of LR vs NS given in large volumes
may lead to non-anion gap, hyperchloremic metabolic acidosis. (# 157 Tenner
2013) A Spanish multidisciplinary society guideline commented on benefit of
LR over NS for control of inflammatory states, but did not make a
recommendation. (#178 Poma 2013)
Retrospective pediatric cohort study was not willing to recommend best type of
fluid due to lack of evidence in children. (#62 Szabo 2015).
Return to Initial
Management
Return to Subsequent
Management

Nutrition
Recommendations:
A nutrition consult should be placed for all patients admitted with pancreatitis.
Enteral nutrition is preferred in patients with pancreatitis and should begin
within 48 hours of hospital admission when the patient is hemodynamically
stable unless there are contraindications such as ileus or bowel obstruction.
Feeding route (in order of preference):
Oral Diet: Advance diet to goal of regular
Nasogastric feeds (NG): If unable to take PO due to pain, poor appetite,
other underlying cause impairing ability to eat, first line treatment should
be NG tube placement with initiation of continuous polymeric formula
unless contraindicated by protein allergy. Conversion to bolus feeds
should be attempted when clinical status allows.
Nasojejunal (NJ): If NG-feeds are poorly tolerated due to vomiting,
diarrhea, post-pyloric tube placement and trial of NJ continuous polymeric
feedings is recommended.
Parenteral nutrition: IV nutrition should be considered if there are
contraindications to enteral feeds or if severe feeding intolerance persists
despite attempts at enteral feeds.
Return to Initial
Management
Return to Subsequent
Management

Empiric Antibiotics for Patients with Pancreatitis
Return to Initial
Management
Return to Subsequent
Management
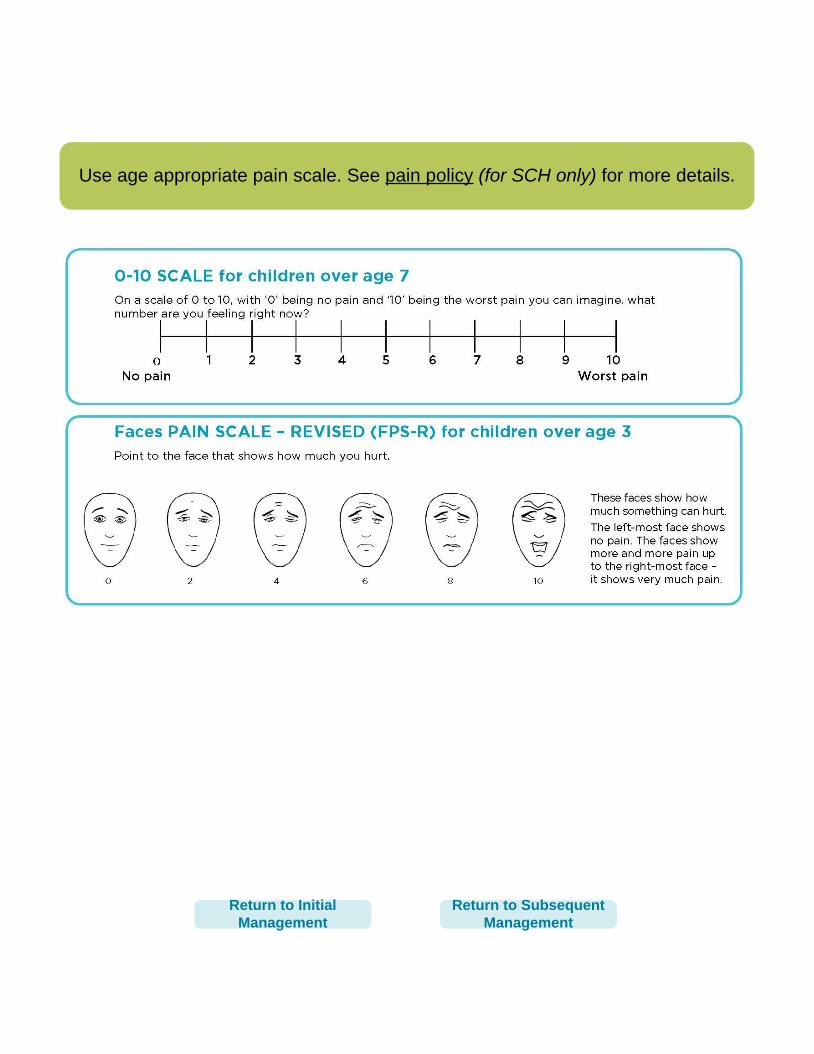
Use age appropriate pain scale. See pain policy (for SCH only) for more details.
Return to Initial
Management
Return to Subsequent
Management
Pancreatitis Approval & Citation
Approved by the CSW Pancreatitis team for July 26, 2017 go live.
CSW Pancreatitis Team:
Owner, GI Matt Giefer, MD, FAAP
Medical Clinical Nurse Specialist Anjanette Allard, RN
Medical Clinical Nurse Specialist Rebecca Engberg, RN, BSN,CPN
ED Clinical Nurse Specialist Sara Fenstermacher, RN
Clinical Dietitian Kim Leaf Braly, RD
Endocrinology Helen Dichek, MD
Clinical Pharmacy Jennifer Nguyen, PharmD
Pharmacy Informatics Rebecca Ford, PharmD
Anesthesia & Pain See Tham, MD
Clinical Effectiveness Team:
Consultant: Sara Vora, MD, MPH
Consultant: Lori Rutman, MD, MPH
Project Manager: Asa Herrman
CE Analyst: Maria Jerome
CIS Informatician: Carlos Villavicencio, MD, MS-MI
CIS Analyst: James Johnson
Librarian: Sue Groshong, MLIS
Program Coordinator: Kristyn Simmons
Executive Approval:
Sr. VP, Chief Medical Officer Mark Del Beccaro, MD
Sr. VP, Chief Nursing Officer Madlyn Murrey, RN, MN
Surgeon-in-Chief Bob Sawin, MD
Retrieval Website: http://www.seattlechildrens.org/pdf/pancreatitis-pathway.pdf
Please cite as:
Seattle Children’s Hospital, Giefer M, Allard A, Braly K, Dichek H, Fenstermacher S, Herrman A,
Rutman L, Tham S, Vora S, 2017 July. Pancreatitis Diagnosis Pathway. Available from: http://
www.seattlechildrens.org/pdf/pancreatitis-pathway.pdf
Return to Initial
Management
Return to Subsequent
Management
Evidence Ratings
To Bibliography
This pathway was developed through local consensus based on published evidence and expert
opinion as part of Clinical Standard Work at Seattle Children’s. Pathway teams include
representatives from Medical, Subspecialty, and/or Surgical Services, Nursing, Pharmacy, Clinical
Effectiveness, and other services as appropriate.
When possible, we used the GRADE method of rating evidence quality. Evidence is first assessed
as to whether it is from randomized trial or cohort studies. The rating is then adjusted in the
following manner (from: Guyatt G et al. J Clin Epidemiol. 2011;4:383-94.):
Quality ratings are downgraded if studies:
· Have serious limitations
· Have inconsistent results
· If evidence does not directly address clinical questions
· If estimates are imprecise OR
· If it is felt that there is substantial publication bias
Quality ratings are upgraded if it is felt that:
· The effect size is large
· If studies are designed in a way that confounding would likely underreport the magnitude
of the effect OR
· If a dose-response gradient is evident
Guideline – Recommendation is from a published guideline that used methodology deemed
acceptable by the team.
Expert Opinion – Our expert opinion is based on available evidence that does not meet GRADE
criteria (for example, case-control studies).
Return to Initial
Management

Summary of Version Changes
· Version 1.0 (7/26/2017): Go live
· Version 2.0 (3/16/2018): Added feeding tube parameters to algorithm
Return to Initial
Management
Return to Subsequent
Management
Medical Disclaimer
Medicine is an ever-changing science. As new research and clinical experience broaden our
knowledge, changes in treatment and drug therapy are required.
The authors have checked with sources believed to be reliable in their efforts to provide information
that is complete and generally in accord with the standards accepted at the time of publication.
However, in view of the possibility of human error or changes in medical sciences, neither the
authors nor Seattle Children’s Healthcare System nor any other party who has been involved in the
preparation or publication of this work warrants that the information contained herein is in every
respect accurate or complete, and they are not responsible for any errors or omissions or for the
results obtained from the use of such information.
Readers should confirm the information contained herein with other sources and are encouraged to
consult with their health care provider before making any health care decision.
Return to Initial
Management
Return to Subsequent
Management
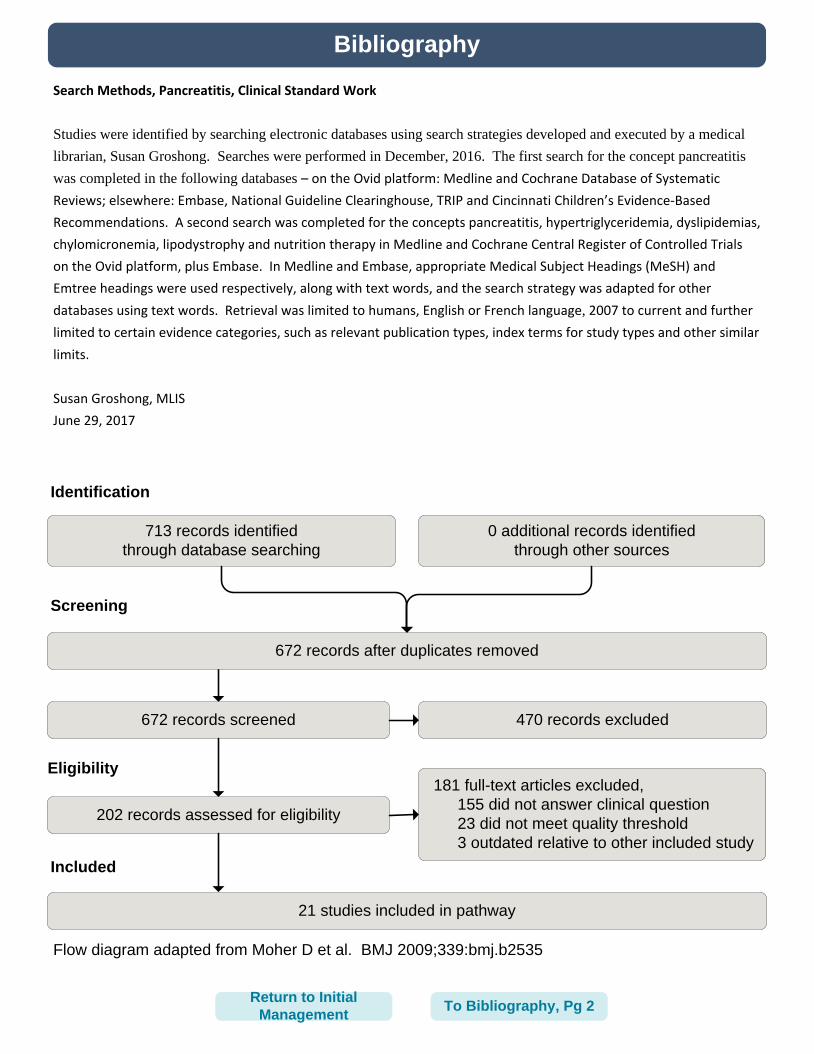
Bibliography
Identification
Screening
Eligibility
Included
Flow diagram adapted from Moher D et al. BMJ 2009;339:bmj.b2535
Search Methods, Pancreatitis, Clinical Standard Work
Studies were identified by searching electronic databases using search strategies developed and executed by a medical
librarian, Susan Groshong. Searches were performed in December, 2016. The first search for the concept pancreatitis
was completed in the following databases – on the Ovid platform: Medline and Cochrane Database of Systematic
Reviews; elsewhere: Embase, National Guideline Clearinghouse, TRIP and Cincinnati Children’s Evidence-Based
Recommendations. A second search was completed for the concepts pancreatitis, hypertriglyceridemia, dyslipidemias,
chylomicronemia, lipodystrophy and nutrition therapy in Medline and Cochrane Central Register of Controlled Trials
on the Ovid platform, plus Embase. In Medline and Embase, appropriate Medical Subject Headings (MeSH) and
Emtree headings were used respectively, along with text words, and the search strategy was adapted for other
databases using text words. Retrieval was limited to humans, English or French language, 2007 to current and further
limited to certain evidence categories, such as relevant publication types, index terms for study types and other similar
limits.
Susan Groshong, MLIS
June 29, 2017
To Bibliography, Pg 2
713 records identified
through database searching
0 additional records identified
through other sources
672 records after duplicates removed
672 records screened 470 records excluded
181 full-text articles excluded,
155 did not answer clinical question
23 did not meet quality threshold
3 outdated relative to other included study
202 records assessed for eligibility
21 studies included in pathway
Return to Initial
Management
Bibliography
Basurto Ona X, Rigau Comas D, Urrutia G. Opioids for acute pancreatitis pain. Cochrane Database of
Systematic Reviews [Pancreatitis]. 2013;7.
Carr RA, Rejowski BJ, Cote GA, Pitt HA, Zyromski NJ. Systematic review of hypertriglyceridemia-induced acute
pancreatitis: A more virulent etiology? Pancreatology [Pancreatitis]. 2016;16(4):469-476.
Greenberg JA, Hsu J, Bawazeer M, et al. Clinical practice guideline: Management of acute pancreatitis. Can J
Surg [Pancreatitis]. 2016;59(2):128-140. Accessed 20160324.
Haffar S, Bazerbachi F, Garg S, Lake JR, Freeman ML. Frequency and prognosis of acute pancreatitis
associated with acute hepatitis E: A systematic review. Pancreatology [Pancreatitis]. 2015;15(4):321-326.
Accessed 20150724. http://dx.doi.org/10.1016/j.pan.2015.05.460.
Hoffmeister A, Mayerle J, Beglinger C, et al. English language version of the S3-consensus guidelines on
chronic pancreatitis: Definition, aetiology, diagnostic examinations, medical, endoscopic and surgical
management of chronic pancreatitis. Z Gastroenterol [Pancreatitis]. 2015;53(12):1447-1495. Accessed
20151215. http://dx.doi.org/10.1055/s-0041-107379.
Italian Association for the Study of the Pancreas (AISP), Pezzilli R, Zerbi A, et al. Consensus guidelines on
severe acute pancreatitis. Dig Liver Dis [Pancreatitis]. 2015;47(7):532-543. Accessed 20150622. http://
dx.doi.org/10.1016/j.dld.2015.03.022.
Lim CLL, Lee W, Liew YX, Tang SSL, Chlebicki MP, Kwa AL. Role of antibiotic prophylaxis in necrotizing
pancreatitis: A meta-analysis. J Gastrointest Surg [Pancreatitis]. 2015;19(3):480-491. Accessed 20150218.
http://dx.doi.org/10.1007/s11605-014-2662-6.
Maravi Poma E, Zubia Olascoaga F, Petrov MS, et al. SEMICYUC 2012. recommendations for intensive care
management of acute pancreatitis. Med Intensiva [Pancreatitis]. 2013;37(3):163-179. Accessed 20130423.
http://dx.doi.org/10.1016/j.medin.2013.01.007.
Márta K, Farkas N, Szabó I, et al. Meta-analysis of early nutrition: The benefits of enteral feeding compared to
a nil per os diet not only in severe, but also in mild and moderate acute pancreatitis. Int J Mol Sci
[Pancreatitis]. 2016;17(10).
Mekitarian Filho E, Carvalho WBd, Silva FD. Acute pancreatitis in pediatrics: A systematic review of the
literature. J Pediatr (Rio J) [Pancreatitis]. 2012;88(2):101-114. Accessed 20120430. http://dx.doi.org/
10.2223/JPED.2163.
Melody GB, Varsha MA, Bharmal S, Landy MW, John AW, Maxim SP. Incidence and predictors of oral feeding
intolerance in acute pancreatitis: A systematic review, meta-analysis, and meta-regression. Clinical nutrition
(Edinburgh, Scotland) [Pancreatitis]. 2016.
To Bibliography, Pg 3Return to Initial
Management
Bibliography
Meng W, Yuan J, Zhang C, et al. Parenteral analgesics for pain relief in acute pancreatitis: A systematic review.
Pancreatology [Pancreatitis]. 2013;13(3):201-206. Accessed 20130530. http://dx.doi.org/10.1016/
j.pan.2013.02.003.
Okazaki K, Kawa S, Kamisawa T, et al. Amendment of the japanese consensus guidelines for autoimmune
pancreatitis, 2013 I. concept and diagnosis of autoimmune pancreatitis. J Gastroenterol [Pancreatitis].
2014;49(4):567-588. Accessed 20140421. http://dx.doi.org/10.1007/s00535-014-0942-2.
Szabo FK, Fei L, Cruz LA, Abu-El-Haija M. Early enteral nutrition and aggressive fluid resuscitation are
associated with improved clinical outcomes in acute pancreatitis. J Pediatr [Pancreatitis]. 2015;167(2):397-
402.e1. Accessed 20150727. http://dx.doi.org/10.1016/j.jpeds.2015.05.030.
Tenner S, Baillie J, DeWitt J, Vege SS, American College of Gastroenterology. American college of
gastroenterology guideline: Management of acute pancreatitis. Am J Gastroenterol. 2013;108(9):1400-15;
1416.
Tenner S, Baillie J, DeWitt J, Vege SS, American College of Gastroenterology. American college of
gastroenterology guideline: Management of acute pancreatitis. Am J Gastroenterol [Pancreatitis].
2013;108(9):1400-1415. Accessed 20130905. http://dx.doi.org/10.1038/ajg.2013.218.
Working Group IAP/APA Acute Pancreatitis Guidelines. IAP/APA evidence-based guidelines for the management
of acute pancreatitis. Pancreatology [Pancreatitis]. 2013;13(4 Suppl 2):e1-15. Accessed 20130923. http://
dx.doi.org/10.1016/j.pan.2013.07.063.
Yokoe M, Takada T, Mayumi T, et al. Japanese guidelines for the management of acute pancreatitis: Japanese
guidelines 2015. J Hepatobiliary Pancreat Sci [Pancreatitis]. 2015;22(6):405-432. Accessed 20150527. http://
dx.doi.org/10.1002/jhbp.259.
Yong L, Lu Q, Liu S, Fan H. Efficacy of glutamine-enriched nutrition support for patients with severe acute
pancreatitis: A meta-analysis. JPEN J Parenter Enteral Nutr [Pancreatitis]. 2016;40(1):83-94.
Yuan X, Wang H. Lack of association between CD14-159 C/T polymorphism and acute pancreatitis: A meta-
analysis. Int J Clin Exp Med [Pancreatitis]. 2015;8(3):4134-4139.
Zhu Y, Yin H, Zhang R, Ye X, Wei J. Nasogastric
Return To Bibliography,
Pg 1
Return to Initial
Management