Oral cavity oropharynx esophagus stomach liver Gallbladder Small intestine Large intestine rectum...
63
Oral cavity oropharynx esophagus stomach liver Gallbladder Small intestine Large intestine rectum pancreas Anal canal Salivary glands Accessory Organs Alimentary Canal
-
Upload
marvin-lewis -
Category
Documents
-
view
227 -
download
1
Transcript of Oral cavity oropharynx esophagus stomach liver Gallbladder Small intestine Large intestine rectum...

Oral cavity
oropharynx
esophagus
stomachliver
GallbladderSmall intestine
Large intestine
rectum
pancreas
Anal canal
Salivary glands
Accessory OrgansAlimentary Canal

The Alimentary Canals

DIGESTIVE SYSTEM FUNCTIONS
• Obtain nutrients for cells• Nutrients are needed/used for:
– Energy source (break down of nutrients can generate ATP)
– Building materials for:• Cell Growth• Cell Repair• Cell Maintenance• Production of hormones, enzymes, etc….
– Elements for normal cell function• Coenzymes, ions, etc…

D.S. processes• Ingestion—bring nutrients/ food it into our alimentary
canal• Mechanical Digestion
– breaking big into small—no chemical changes– Facilitates chemical digestion
• Chemical Digestion– breaking of covalent bonds by enzymes to turn large molecules
into small molecules (molecules small enough for absorption)
• Absorption:– nutrients cross epithelial tissue of alimentary canal and enter
circulation—cardiovascular or lymphatic systems
• Propulsion—peristalsis– Movement of ingested material made possible by muscle—
mostly smooth—lining digestive tract
• Elimination of material that was not digested or absorbed

Macromolecule Review:these are the major nutrients (i.e., macronutrients)
• Carbohydrates: – monosaccharides < disaccharides < polysaccharides– Amylase = enzymes that break down carbs
• Proteins: – amino acids– Protease = enzymes that break down proteins
• Lipids: – Fatty Acids + Glycerol/monoglycerides– Lipase = enzyme that breaks down lipids

Figure 24.1


1. Liver – Break down and synthesize (interconvert) most carbs, lipids, and
amino acids/proteins– Stores glycogen– ONLY TISSUE THAT CAN RELEASE GLUCOSE*
• When glucose enters non-liver tissue it is phosphoylated preventing it from crossing back out across the PM
• Only the liver can de-phosphorylate
2. Adipose tissue – Stores lipids primarily as triglycerides– Can release lipids as fatty acids and glycerol
*as far as we are concerned.
five metabolic components/tissues

3. Skeletal muscle (close to half your body mass)– Creates substantial glycogen reserves– Proteins in myofibrils can be broken down as source of
releasable amino acids– Uses mostly glucose and triglycerides for energy
4. Neural tissue--BRAIN– Requires glucose* and has high glucose demand– canNOT store energy reserves
5. Other tissues – Insignificant energy reserves– Variable use of carbs, lipids, and amino acids (and
others) substrates.
five metabolic components/tissues
Absorptive State
• 0-4 hrs after feeding• Period of increase blood nutrient levels• Period of increased nutrient availability• Characterized by nutrient uptake by cells• Cells use plasma nutrients as source of energy• Cells generate nutrient stores from uptake of
nutrients• Promoted by insulin

Insulin• Released from beta cells in pancrease• Promotes cell uptake of nutrients from plasma• Reduces blood glucose (lipids & amino acid)• Production of glyocogen (glycogenisis)• Stimulates adipocytes to synthesize triglycerides (with glucose)• Stimulates protein synthesis
Insulin release is stimulated by:• High blood glucose levels• High amino acids levels• Digestive activity

Fate of Nutrients: Absorptive State
* Resting skeletal muscle uses triglycerides for ATP, but
uptakes glucose and stores it as glycogen
*

Absorptive State
LiverG.I. Tract
(small intestines)
Other cells
blood

Stored Substrates
1-2 months of ATP
~4 hrs – overnight worth of ATP -- only liver can release glucose -- muscle glucose cannot be released
Mostly in skeletal muscle
Proteins (amino acids)
14.46%
Mostly in adipose tissue

Post-Absorptive State
• >4 hrs after a meal• Cells use own stored energy reserves• Release of stored reserves into blood• Formation of glucose from non-carbs (gluconeogenisis)
• Glucose sparing • Ensures adequate blood glucose for the brain• Promoted primarily by Glucagon
– Also glucocorticoids, epinephrine, and other hormones
Glucagon
• Released by alpha cells in pancrease• Breakdown of glycogen (glycogenolysis) in liver
and relase of glucose into blood• Stimulates gluconeogenisis in liver and release of
glucose into blood• Stimulates adipocytes to release lipids• Blood fatty acid levels rise
• Glucagon release is stimulated by low blood sugar
Post-Absorptive State & the Brain
• The brain is primarily dependent on glucose• The brain does not store glucose or glycogen• Brain is dependent on constant supply of blood
glucose to function
• Many post-absorptive activities ensure brain has adequate glucose

Post-Absorptive State & the liver
• The liver is the only* organ that has cells which can release glucose
• The liver is the major metabolic organ that can interconvert major macromolecules
• The liver can release stored glucose into blood• The liver can uptake non-carbs, convert them to
glucose (gluconeogenisis), and then release that glucose

Post Absorptive Substrate Fate

Post-absorptive State
LiverG.I. Tract
(small intestines)
blood
Other cells Brain

ATP
Adipose Tissue
MuscleTissue
Liver
Interconversion of substrates:Common source organs/tissues

Insulin release and action

Insulin, Glucagon and Blood Sugar


• Negative Feedback control of blood glucose by insulin and glucagon

Diabetes Mellitus:high blood sugar/inability to regulate blood glucose levels
Types:Type 1 Diabetes (10-15% of diabetes)• usually appears by early adulthood• autoimmune disorder that destroys beta cells• most commonly treated with supplemental insulin and blood glucose
monitoringType 2 Diabetes (85-90% of diabetes)• Cells of body stop responding to insulin (insulin resistance).• Caused largely by lifestyle (poor diet and lack of exercise)• Some ethnicities are more genetically susceptible (will get it faster/easier
and easier in light of poor diet and lack of exercise)– Thrifty Gene Hypothesis
• largely a preventable disorder• Treated with drugs, change in diet, and exercise
Gestational Diabetes:• Can happen during pregnancy

More on Type 2 Diabetes
leading cause of:– amputations– blindness– impotence– heart/cardiovascular disease– hypertension– strokes– renal/kidney failure– slow healing wound/increased risk of infection
• 7th leading cause of death, but contributes to death by renal failure and CV disease (70% of deaths due to diabetes related deaths also had heart disease) (CDC)
• Rate of Type 2 doubled between 1990 and 2005 in the U.S. (CDC)
• Currently 23.2 million in US have it—7.5% of the population….and growing (CDC)
• estimated $1 out of every $8 healthcare dollars spent are diabetes related• $174 billion in diabetes related costs, 116 billion were DIRECT costs. (NIH)
• WITH “typical” health insurance Type 2 diabetes will cost you an average of $1900/yr—with no serious complications (NIH)

Diabetes S/Sx
Primary• Frequent urination• Increase thirst• Increase hunger
other• blurred/diminished vision• acetone/fruity breath• acidosis/metabolic problems with deep labored
breathing….primarily in Type 1


Glucocorticoids (e.g. cortisol)• Released from the andrenal cortex• Increase glucose synthesis in liver (gluconeogenisis)• Causes adipose cells to release fatty acids into blood• Promotes protein breakdown and amino acid release into blood• Inhibits glucose use by organs/tissues other than the brain (spares
glucose for brain)• Causes other tissues to metabolize fatty acids and proteins rather than
glucose for their own needs to “spare” glucose for the brain.• Also anti-inflammatory and inhibits WBC, release of histimine and
reduce the movement of phagocytes to the site generally reducing inflammation but slowing the healing and increasing risk of infection.
Increased levels released in response to stress
(e.g., fasting and physical activity)

Oral Cavity


Oral CavityKey Processes• mastication = mechanical digestion by teeth• chemical digestion
– salivary amylase • Complex carbs disaccharides
– Salivary lipase breaks down lipids
Saliva (from salivary glands)• salivary amylase: breaks down carbohydrates• mucus: holds food together, lubricates• stimulated by parasympathetic ANS
pH of oral cavity is near 7 (more or less neutral)
Esophagus
• A muscular tube that conducts/propells food (bolus) to the stomach.

Stomach Anatomy• Cardiac/Lower Esophageal
Sphincter– prevents movement of stomach
contents back into the esophagus
– heart burn/acid reflux/GERD caused by failure of valve to do its job
• Pyloric Sphincter– regulates the passage of food
into small intestine (emptying of stomach)
• Lined by simple columnar tissue– Thin enough to be readily
permeable– Cells have enough volume to
contain necessary machinery (organelles to make proteins and process energy/ATP)
– Mucus=protects lining of stomach

Hiatal Hernia: the stomach slips up into the thoracic cavity through an
opening in the diaphragm. Promotes reflux.

Stomach Function
• Chemical Digestion of Proteins
• destruction of ingested pathogens
• Minimal absorption – (lipid soluble substances, water, alcohol, some ions)
Gastric Juice

Stomach lining and gastric pits/glands

Gastric JuiceSecreted by Gastric Glands and Contains:• Pepsinogen=inactive enzyme that digests
proteins• Hydrochloric Acid (HCl)
– activates pepsinogen• pepsinogen + HCl pepsin (digestive enzyme)
– creates low pH ~ 2.5 - 4.5• denatures protiens and kills pathogens
• Intrinsic factor (helps absorb B12)• Gastrin a regulatory hormone

Peptic Ulcers:either in stomach (gastric) or duodenum (duodenal)
• 70-90% involve the bacteria Helicobacter pylori
• can be treated with antibiotics
• founders won nobel prize (but not without effort and unconventional demonstrations)
• But 80% of individuals harboring H. pylori are a symptomatic. – Why do only some individuals get ulcers?


Acid Reflux and Hiatal Hernias• Failure of the L.E.S. to work correctly can lead to
acid reflux• Displacement of the L.E.S. relative to the
diaphragm—hiatal hernia--promotes acid reflux because the diaphragm no longer reinforces the L.E.S.– Can also cause breathing difficulty in some settings
• Acid reflux is uncomfortable, can cause histological changes in esophagus, increases likelihood of esophageal cancer, can even cause pneumonia if acids are aspirated

Small Intestines
• THE PRIMARY SITE OF DIGESTION AND ABSORPTION
• Lined with simple columnar cells– thin enough to be
permeable, – big enough to perform
active process such as secretion and absorption
• pH ~ 8 (slightly alkaline/basic)
S.I. Processes
• Chemical Digestion– Receives digestive enzymes from pancreas
and produces own
• Absorption– nutrients cross intestinal wall and enter
circulation
• features that increase absorption– villi, microvilli, length of intestines



Absorption of Nutrients
• monosaccharides blood/capillaries• amino acids blood/capillaries• glycerol/monoglycerides blood capillaries• fatty acids lymph/lacteals
• Hepatic Portal System: nutrients that are absorbed into blood are delivered directly to liver where the liver can remove many nutrients for storage and/or conversion and toxins can be neutralized.

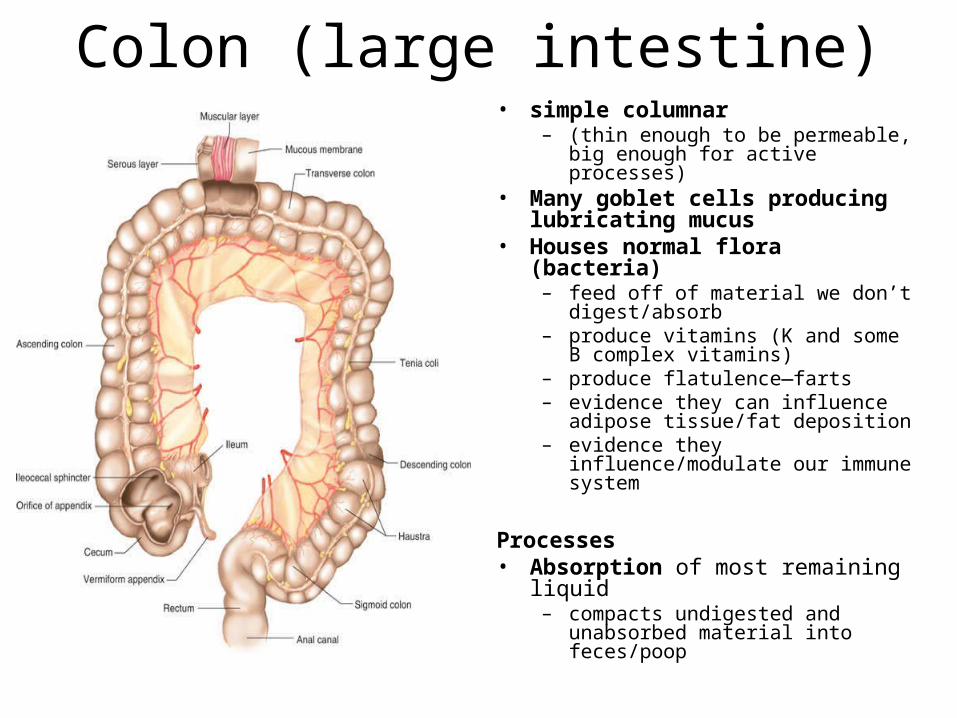
Colon (large intestine)• simple columnar
– (thin enough to be permeable, big enough for active processes)
• Many goblet cells producing lubricating mucus
• Houses normal flora (bacteria)– feed off of material we don’t
digest/absorb– produce vitamins (K and some B
complex vitamins)– produce flatulence—farts– evidence they can influence
adipose tissue/fat deposition– evidence they influence/modulate
our immune system
Processes• Absorption of most remaining
liquid– compacts undigested and
unabsorbed material into feces/poop


Liver Functions• Stores and Releases glucose (only organ/tissue that
can release glucose)– to stabilize blood glucose
• Synthesizes and stores lipids (chlosterol, …..) also regulates circulating lipids– foie gras anyone?
• Amino Acid interconversion and breakdown (gluconeogenisis)
• Detoxify absorbed toxins• Removes old RBC’s• Produces Bile
– bile emulsifies fat (mechanically breaks it up and allows it to mix with water)
– eliminates cholesterol and bilirubin• Bile is stored in gallbladder and enters duodeum
through a system of ducts (biliary ducts)


Pancreas
• Digestive Function– Creates Pancreatic Juice that enters
duodenum– digestive enzymes that breakdown carbs,
lipids, and proteins– alkaline to neutralize stomach acid
• Endocrine Function– releases insulin and glucagon (more later)

Substrate Use:molecules broken down to generate ATP
Two primary molecules used for energy are:• Glucose (carbohydrate)
• can be stored as glycogen by various cells• once glucose enters a cell it cannot leave (except liver)• produces 4 kilocalories of energy per gram• Brain is highly dependent on glucose but can’t store it
• Fats (triglyercides = Fatty acids + glycerol)• Occurs mainly in adipose and liver tissues • Yields 9 kilocalories/g
• Proteins are typically not a primary source of energy
5-35

Uses of Different Energy Sources• Different cells have different preferred energy substrates• Brain uses glucose as its major source of energy
5-48

Interconversion of energy substrates:
excess intake/storage • Excess glucose enters cells and is stored
as glycogen• Once glyocogen stores are maximized
glucose is converted into fats for storage• glucose can even be used to create amino
acids• If you intake more amino acids then
needed they can be converted into glucose and fats/triglycerides

Essential and Non-essential Amino Acids• 20 amino acids are used to build proteins• 12 can be produced by body• 8 must come from diet (= essential amino acids)
5-42
can be synthesized by our body

various intermediate molecules
from diet and absorbed by
digestive system
ATP

Substrate Interconversion
When energy is needed:• Glucose and Fats (both stored and circulating)
can be broken down through cellular respirationIf more glucose is needed:• stored glycogen is broken downWhen cells use up their stored substrates:• adipocytes and release lipids into blood• liver can release its stored carbohydrates• fats and amino acids can be converted into the
carbs (gluconeogenisis)– Particularly important to keep the brain functioning

various intermediate molecules
sources of energy for a
cell
ATP
Insulin and Glucagon:Hormones release by Pancreas
Insulin:• released by beta cells in pancreas in response to high
blood glucose
• lowers blood glucose levels by stimulating liver to remove glucose and create glycogen
• promotes uptake (by facilitated diffusion) of glucose by cells of body)
• Also stimulates update of amino acids and production of proteins and uptake and synthesis of fats (including by adipocytes)

Insulin and Glucagon:Hormones release by Pancreas
Glucagon• released by alpha cells in pancreas in response to low
blood glucose
• Promotes glucose synthesis (from glycogen and other) and release by the liver
• stimulates the breakdown and release of fats/lipids by adipocytes