Gallbladder polyps and neoplasia - SUNY Downstate … polyps.pdfB-GALLBLADDER: -CHRONIC...
28
Gallbladder polyps and neoplasia Volodymyr Labinskyy MD, Brooklyn VA Hospital August 16, 2012 www.downstatesurgery.org
Transcript of Gallbladder polyps and neoplasia - SUNY Downstate … polyps.pdfB-GALLBLADDER: -CHRONIC...
Gallbladder polyps and neoplasia
Volodymyr Labinskyy MD, Brooklyn VA Hospital August 16, 2012
www.downstatesurgery.org
64 year old male referred for evaluation of incidentally found asymptomatic gallbladder polyp 1.1 cm on screening abdominal CT for HCC surveillance PMH: Obesity, GERD, Dislipidemia, Hep C, DM II, Hypothyroidism PSH: Vasectomy, TURP 4/2012 Home meds: Finasteride, metformin, omeprazole, levothyroxine, simvastatin, HTZ, gemfibrozil, orlistat Physical exam: BMI 35, liver 2+ cm below costal margin Labs: within normal limits
www.downstatesurgery.org

RUQ US
www.downstatesurgery.org
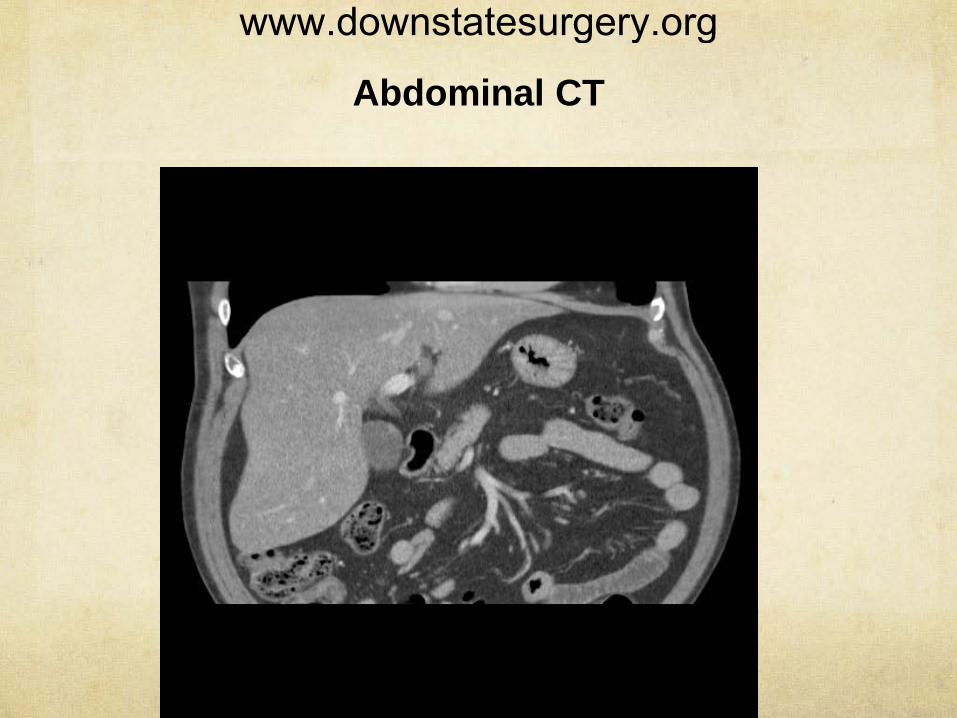
Abdominal CT
www.downstatesurgery.org
7/23/12 Lap cholecystectomy. Uneventful postoperative course.
7/24/12 Discharged home
Pathology: Specimen A is labeled as "gallbladder mass". It consists of multiple yellow soft stones in aggregate measuring 0.8 x 0.6 x 0.4 cm.
B-GALLBLADDER: -CHRONIC CHOLECYSTITIS WITH CHOLELITHIASIS.
www.downstatesurgery.org
Gallbladder polyps and neoplasia
www.downstatesurgery.org
Epidemiology The highest incidence of gallbladder cancer is found in women living in India, Pakistan, and Ecuador.
Approximately 9760 cases of gallbladder and other biliary cancers are diagnosed annually in the United States, with 3320 deaths annually
In North America, high incidence rates are found among Native Americans and Hispanic women
(Jemal et al, 2010). (Barakat et al, 2006)
www.downstatesurgery.org
Etiology
Cholelithiasis and chronic inflammation.
Calcification in the wall of the gallbladder otherwise known as porcelain gallbladder. Incidence of cancer <10%
Chronic inflammatory conditions of the gallbladder (cholecystoenteric fistula)
Anomalous Pancreatico-Biliary Duct Junction
Chemical carcinogens: methyldopa, isoniazid, occupational exposure in the rubber industry
8% incidence of gallbladder cancer in gallbladder specimens with polyps, all more than 1 cm in size.
www.downstatesurgery.org
Preneoplastic Lesions
Progression from dysplasia to carcinoma in situ to frank invasive carcinoma is seen in gallbladder epithelium
Progression of precursor lesions to invasive carcinoma was estimated to be approximately 15 years
Gallbladder polyps have been noted in 3% to 6% of patients undergoing ultrasonography (US).
(Albores-Saavedra et al, 1986) (Roa et al, 1996)
(Zielinski et al, 2009)
www.downstatesurgery.org
The incidence of carcinoma in nonadenomatous polyps—cholesterol polyps, inflammatory polyps, and hyperplastic polyps—is close to zero
Risk of malignancy was associated with: increasing age >50 size greater than 1 cm the presence of a single polyp
(Choi et al, 2008, Ito et al, 2009)
www.downstatesurgery.org
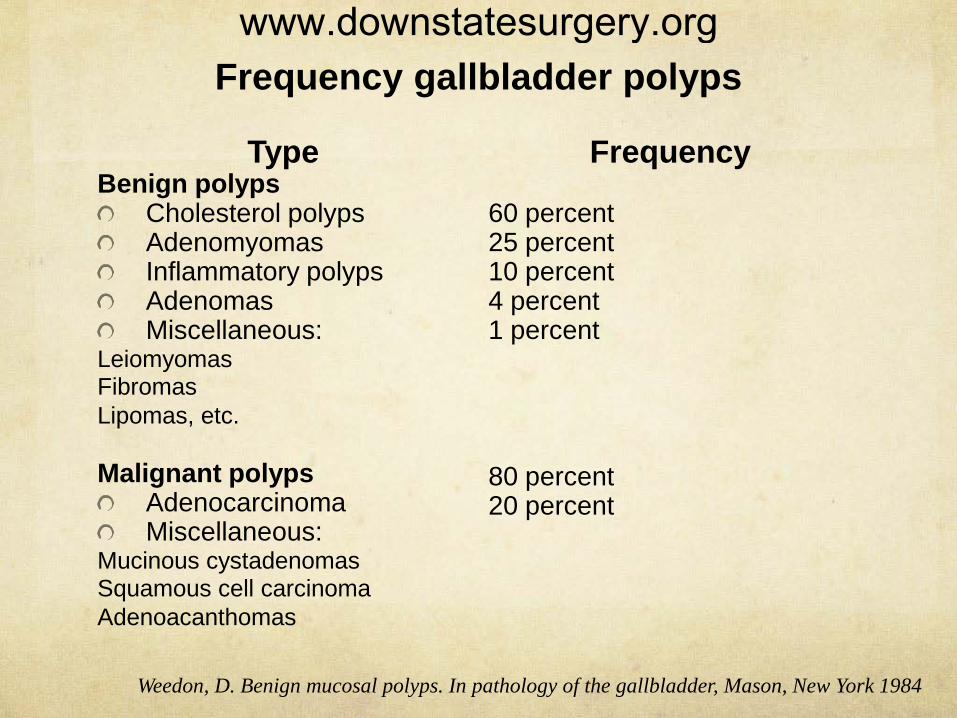
Frequency gallbladder polyps
Type Benign polyps
Cholesterol polyps Adenomyomas Inflammatory polyps Adenomas Miscellaneous:
Leiomyomas Fibromas Lipomas, etc. Malignant polyps
Adenocarcinoma Miscellaneous:
Mucinous cystadenomas Squamous cell carcinoma Adenoacanthomas
Frequency 60 percent 25 percent 10 percent 4 percent 1 percent 80 percent 20 percent
Weedon, D. Benign mucosal polyps. In pathology of the gallbladder, Mason, New York 1984
www.downstatesurgery.org
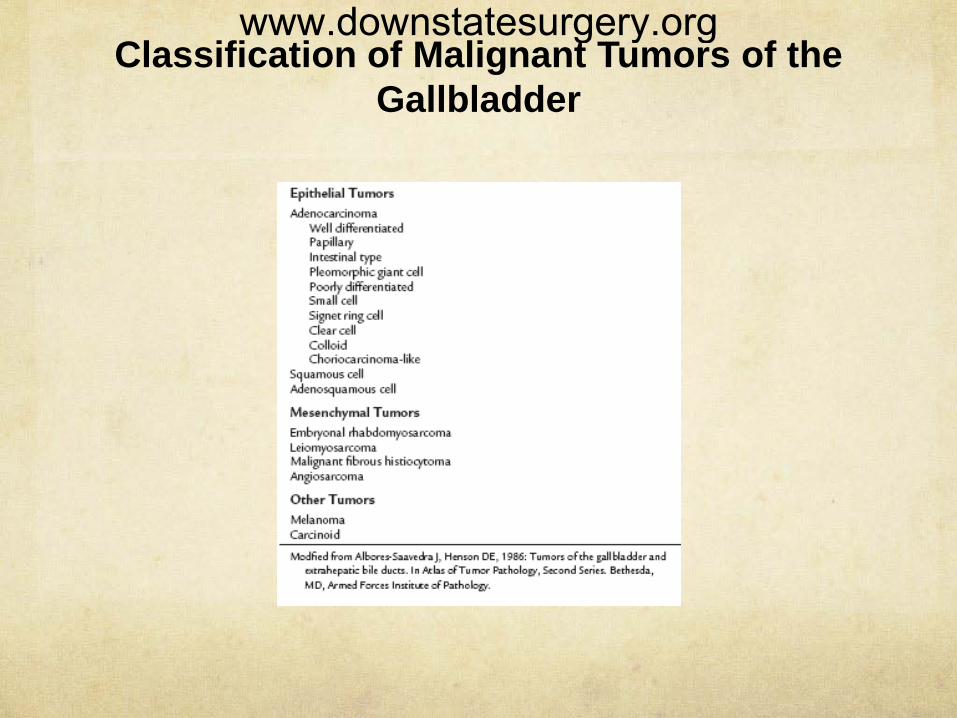
Classification of Malignant Tumors of the Gallbladder
www.downstatesurgery.org
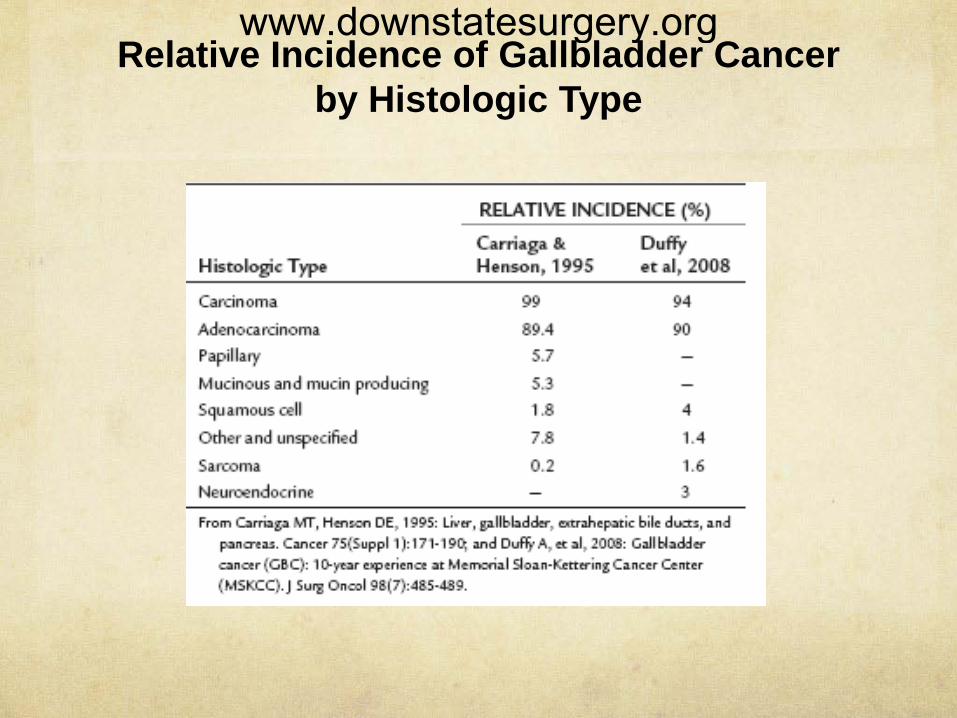
Relative Incidence of Gallbladder Cancer by Histologic Type
www.downstatesurgery.org
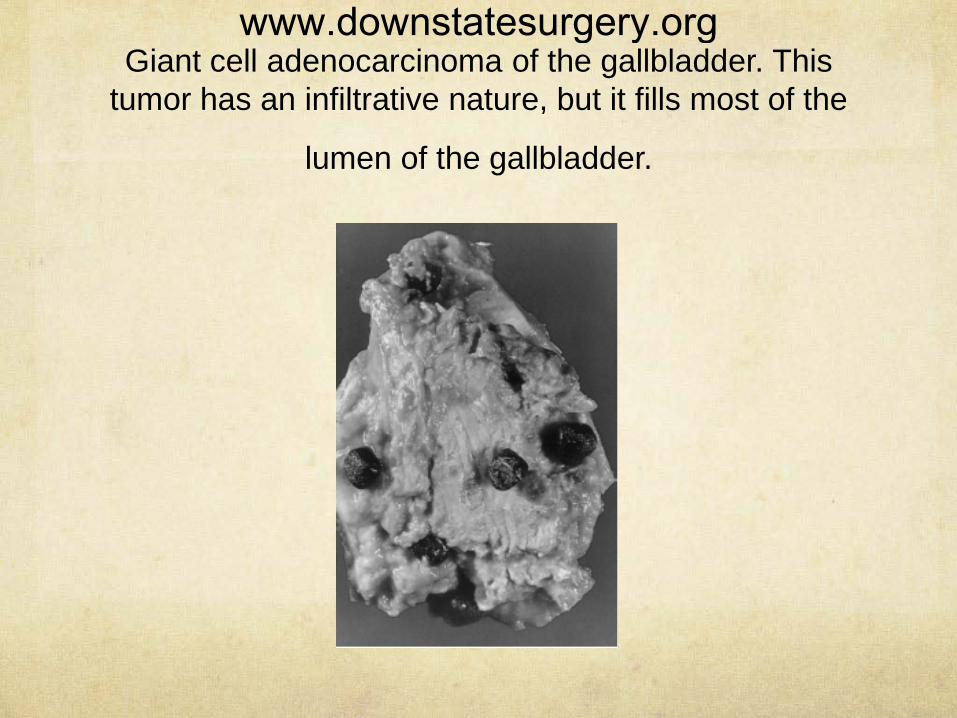
Giant cell adenocarcinoma of the gallbladder. This
tumor has an infiltrative nature, but it fills most of the
lumen of the gallbladder.
www.downstatesurgery.org
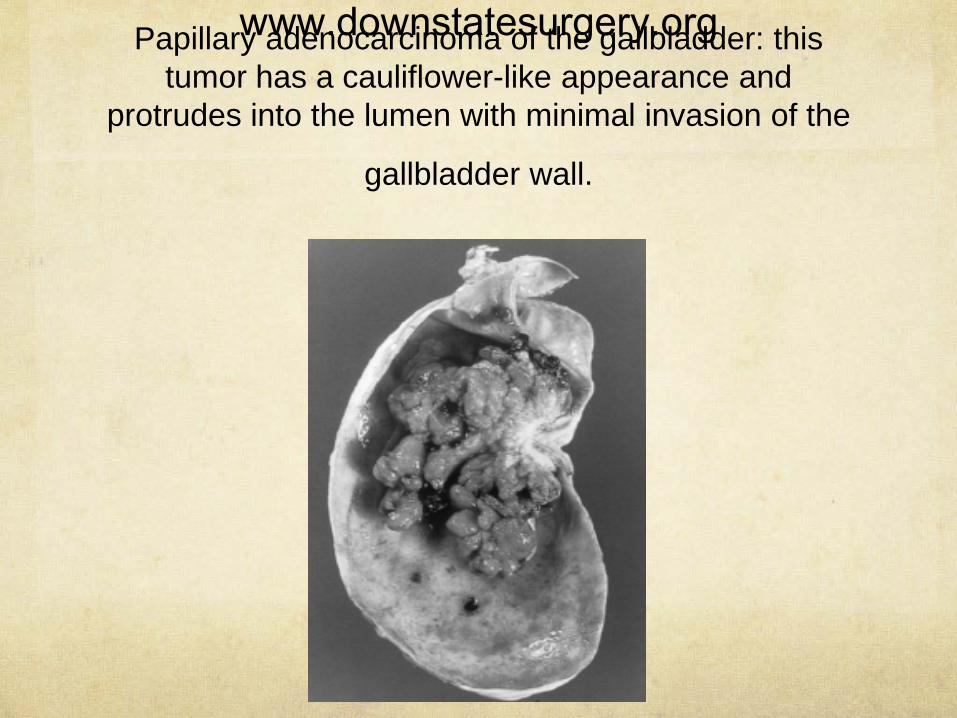
Papillary adenocarcinoma of the gallbladder: this
tumor has a cauliflower-like appearance and protrudes into the lumen with minimal invasion of the
gallbladder wall.
www.downstatesurgery.org
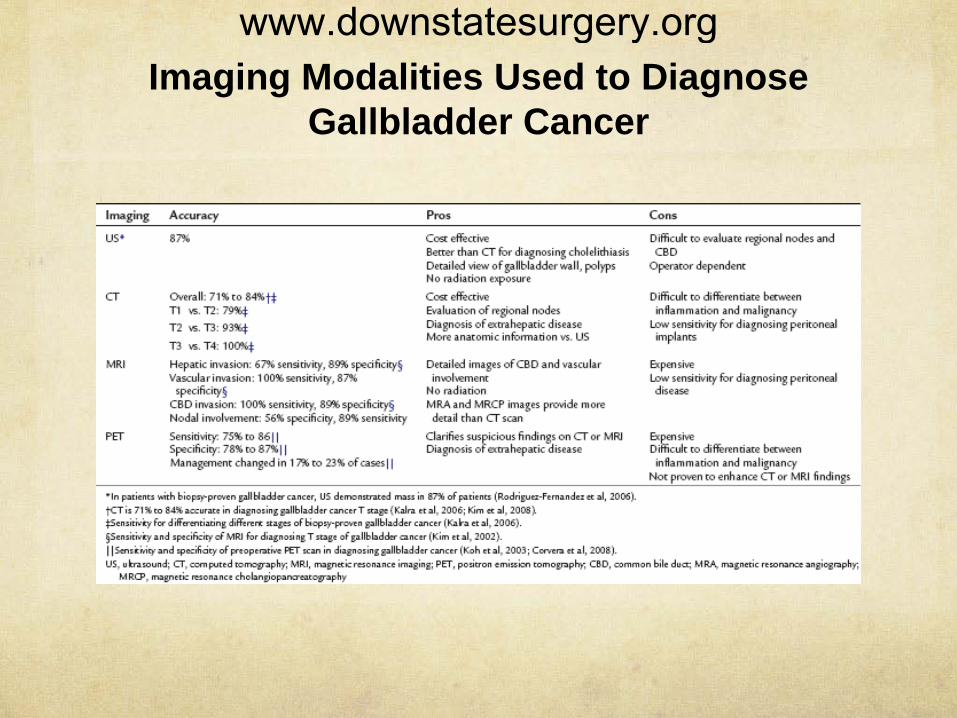
Imaging Modalities Used to Diagnose Gallbladder Cancer
www.downstatesurgery.org
Benign Polyps
Some clinicians have recommended cholecystectomy for any patient with fewer than three polyps
Cholecystectomy recommended for any polyp greater than 1 cm
The exception to this recommendation is for those arising in the setting of primary sclerosing cholangitis
(Shinkai et al, 1998) (Ito et al, 2009) (Buckles et al, 2002)
www.downstatesurgery.org
A prevalence of gallbladder cancer with polypoid lesions of the gallbadder equal to 0.08% was reported in white patients
On periodic US 4 to 12 months after the original US, polyps grew 1.4 to 4 times larger
US follow-up at 6- to 12-month intervals for 2 years; if polyp size is stable, routine survelliance can be stopped
(Aldouri et al, 2009) (Kubota at al, 1995)
www.downstatesurgery.org
Incidentally Discovered Gallbladder Carcinoma During or After Routine
Cholecystectomy
Gallbladder cancer is found in 0.27% to 2.1% of all laparoscopic cholecystectomies
Outcomes after prior noncurative resection were similar to outcomes from primary curative resections
Re-resection is recommended for all patients who are medically fit with T1b or greater level of invasion
Resection of the bile duct required for a complete resection in cases with a positive cystic duct stump margin
(Darmas et al, 2007; Kwon et al, 2008). (Fong et al, 2000). (Pawlik et al, 2007)
www.downstatesurgery.org
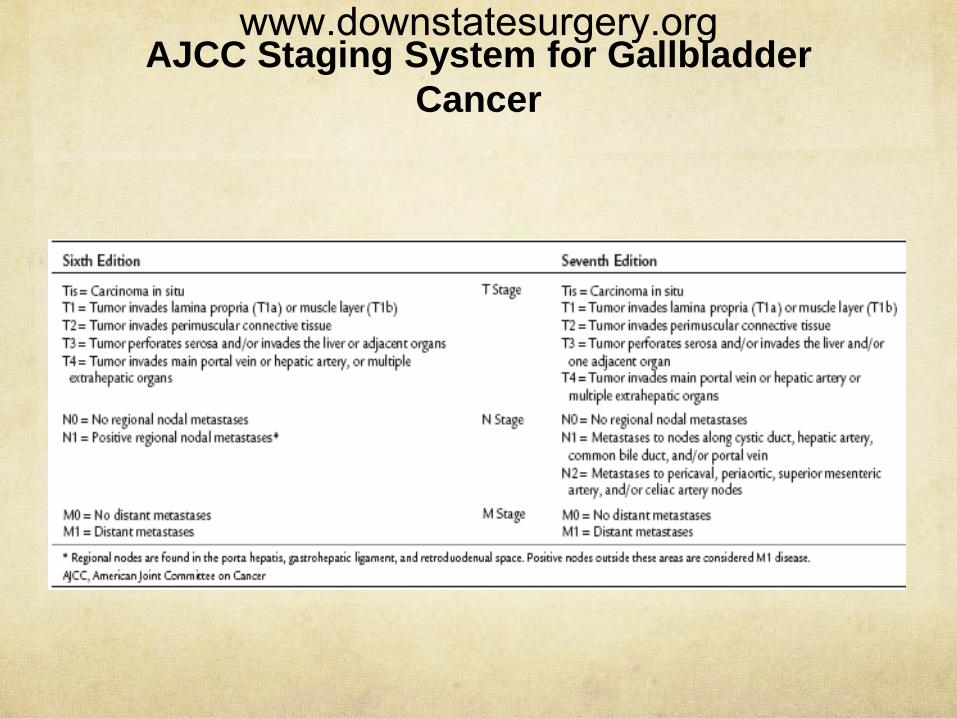
AJCC Staging System for Gallbladder Cancer
www.downstatesurgery.org
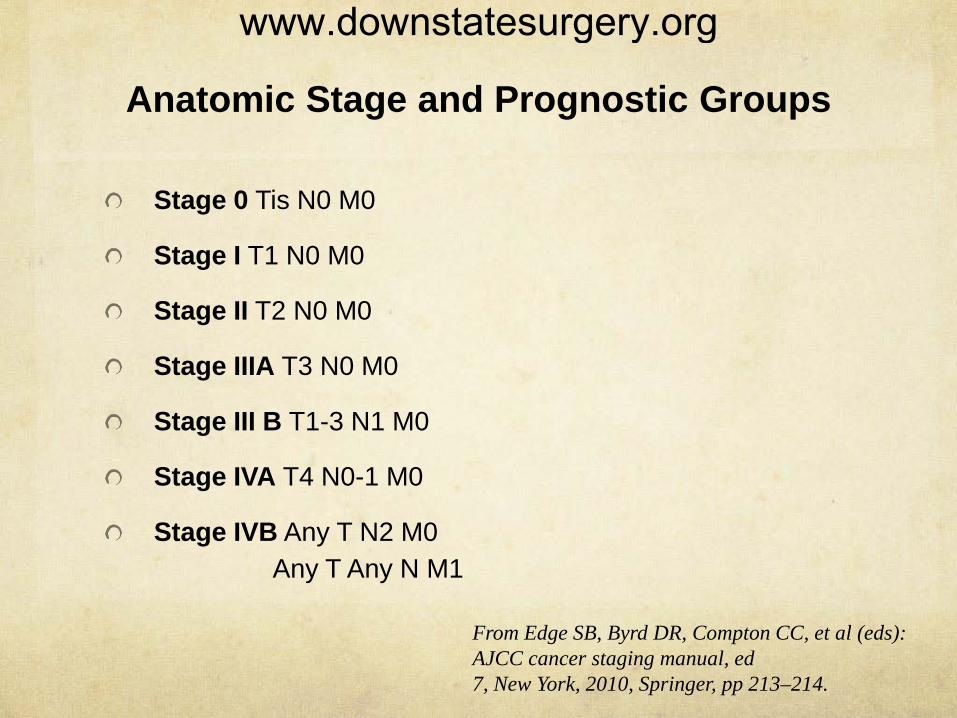
Anatomic Stage and Prognostic Groups
Stage 0 Tis N0 M0
Stage I T1 N0 M0
Stage II T2 N0 M0
Stage IIIA T3 N0 M0
Stage III B T1-3 N1 M0
Stage IVA T4 N0-1 M0
Stage IVB Any T N2 M0 Any T Any N M1
From Edge SB, Byrd DR, Compton CC, et al (eds): AJCC cancer staging manual, ed 7, New York, 2010, Springer, pp 213–214.
www.downstatesurgery.org
PORT SITE RECURRENCES There is a theoretical risk of port site seeding after
laparoscopic cholecystectomy for what is eventually diagnosed as gallbladder cancer
It is rare for port site recurrences to occur as the sole site of disease
General practice does not include empirically resecting prior port sites during reexploration for gallbladder cancer
(Winston et al, 1999) (Povoski et al, 2004; Shoup & Fong, 2002)
www.downstatesurgery.org
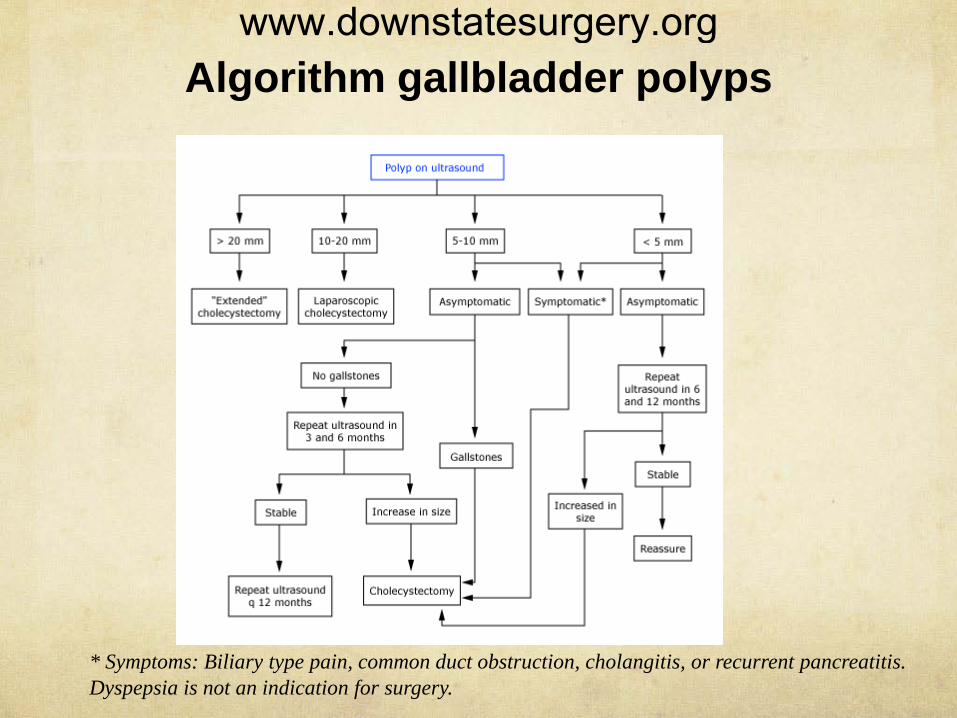
Algorithm gallbladder polyps
* Symptoms: Biliary type pain, common duct obstruction, cholangitis, or recurrent pancreatitis. Dyspepsia is not an indication for surgery.
www.downstatesurgery.org
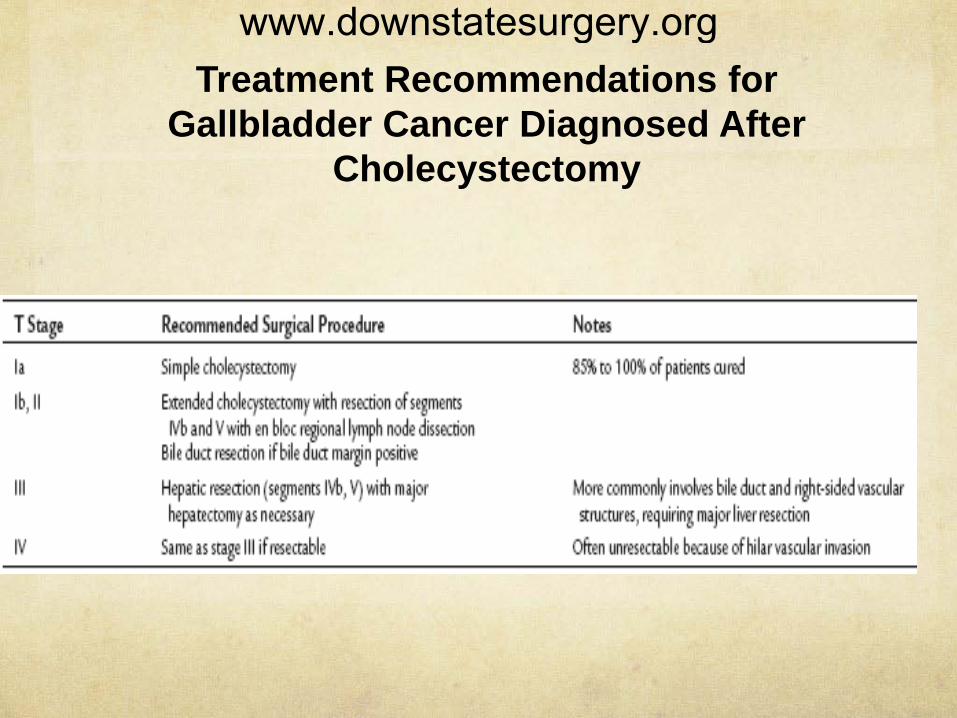
Treatment Recommendations for Gallbladder Cancer Diagnosed After
Cholecystectomy
www.downstatesurgery.org
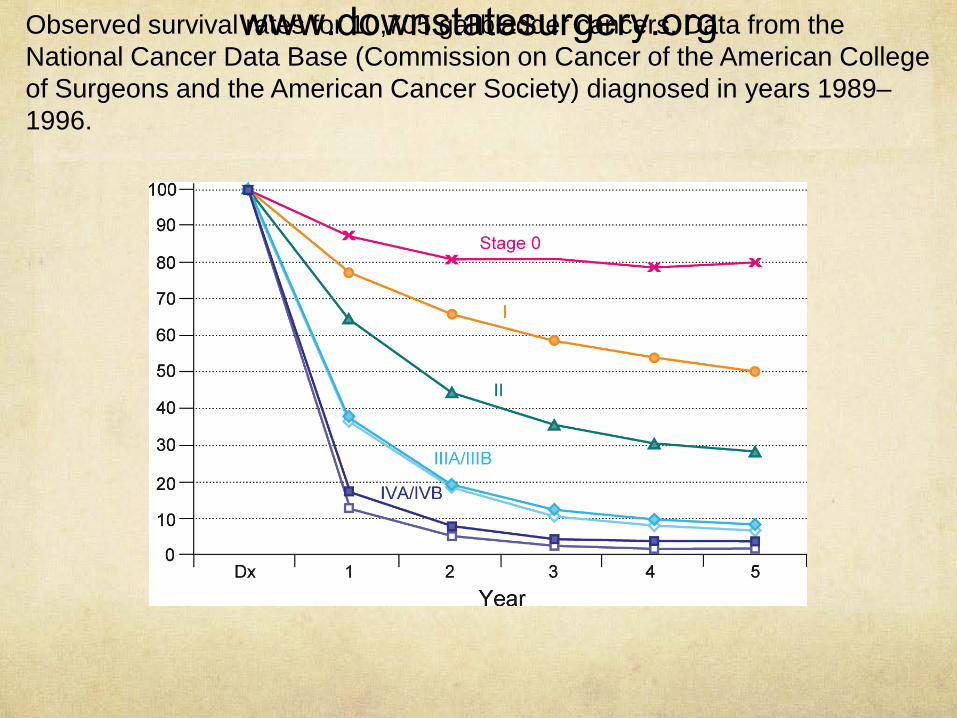
Observed survival rates for 10,705 gallbladder cancers. Data from the National Cancer Data Base (Commission on Cancer of the American College of Surgeons and the American Cancer Society) diagnosed in years 1989–1996.
www.downstatesurgery.org
Following cholecystectomy, an adenocarcinoma of the gallbladder extending into the subserosa
is discovered incidentally. The recommended treatment includes which of the following?
A. Nothing further at this time
B. External beam radiation therapy
C. Radiation therapy and chemotherapy
D. Reoperation for liver resection and lymphadenectomy
E. Reoperation for performance of pancreatoduodenectomy
www.downstatesurgery.org
Ultrasound imaging demonstrates a 15-mm polypoid lesion in the gallbladder of an
asymptomatic 60-year-old patient. Which of the following best describes the recommended
treatment?
A. Observation with repeat ultrasound studies in 6 months
B. Cholecysectomy
C. Cholecysectomy if the patient is female
D. Cholecysectomy only if symptoms develop
E. Cholecysectomyonly if the patient also has gallstones
www.downstatesurgery.org
Which of the following is a contraindication to resection of an adenocarcinoma of the bile duct?
A. Tumor location in the distal common bile duct
B. Tumor location at the bifurcation of the bile duct
C. Peritoneal metastases
D. Invasion of the right portal vein and right hepatic artery
E. None of above
www.downstatesurgery.org