Notes Webb
69
NOTES ON “INTRODUCTION TO BIOMEDICAL IMAGING” BY ANDREW WEBB SANDRO NUNES TÉCNICAS DE IMAGIOLOGIA Prof. Patrícia Figueiredo
-
Upload
alex-souza -
Category
Documents
-
view
249 -
download
0
Transcript of Notes Webb
NOTES ON “INTRODUCTION TO BIOMEDICAL IMAGING”
BY ANDREW WEBB
SANDRO NUNES TÉCNICAS DE IMAGIOLOGIA
Prof. Patrícia Figueiredo

1
1. X-Ray Imaging and Computed Tomography
1.1. General Principles of Imaging with X-Rays
X-Ray Imaging – transmission-based technique in which X-rays from a source pass through
the patient and are detected either by film or an ionization chamber on the opposite side of the
body. Contrast in the image between different tissues arises from differential attenuation of X-
rays in the body.
Computed Tomography – the source and detectors rotate together around the patient,
producing a series of one-dimensional projections at a number of different angles. This data is
reconstructed to give a two-dimensional image. The x-ray source is collimated to interrogate a
thin slice through the patient. It has a very high spatial resolution (~1mm).

2
1.2. X-ray Production
The x-ray source is the most important component in determining the image quality:
1.2.1. X-ray Source
The main structure of the X-ray source (also called tube) is shown below:
Production of X-rays involves accelerating a beam of electrons to strike the surface of a
metal target. The X-ray tube has 2 electrodes: a negatively charged cathode (electron source) –
filament of coiled tungsten wire - and a positively charged anode (metal target).
An electric current passes through the cathode, heating it (~2200ºC) and causing electrons
to move away from the metallic surface (thermionic emission). The tube potential causes the
free electrons to accelerate towards the anode. Since the spatial resolution is determined by the
effective focal spot size, the cathode is designed to produce a tight, uniform beam of electrons.
To do this, a negatively charged focusing cup is placed around the cathode:
Moreover, the anode is beveled in order to produce a small effective focal spot size:
𝑓 = 𝐹𝑠𝑖𝑛(𝜃)
3
The electrons striking the anode lose their kinetic energy, which is converted into X-rays.
The anode must be made of a metal with high melting point and good thermal conductivity
(usually tungsten).
1.2.2. X-ray tube current, tube output and beam intensity
Tube potential: 15-150kV (rectified alternating voltage, characterized by the maximum
value, kilovolts peak or accelerating voltage - kVp).
Tube current: 50-1000mA (depends on kVp)
Tube output: tube current × tube potential. We need a high tube output in order to
decrease the exposure time. It depends on:
- kVp
- Vacuum in the tube (reduces interactions between electrons and molecules and
increase electrons’ velocity)
Tube power rating: maximum power dissipated in an exposure of 0.1s. Limited by anode
heating, which can be reduced by causing it to rotate at roughly 3000 rpm.
Intensity of the X-ray beam: power incident per unit area (J/m2). It depends on the
number (𝛼 current) and energy of the X-rays (𝛼 kVp2)
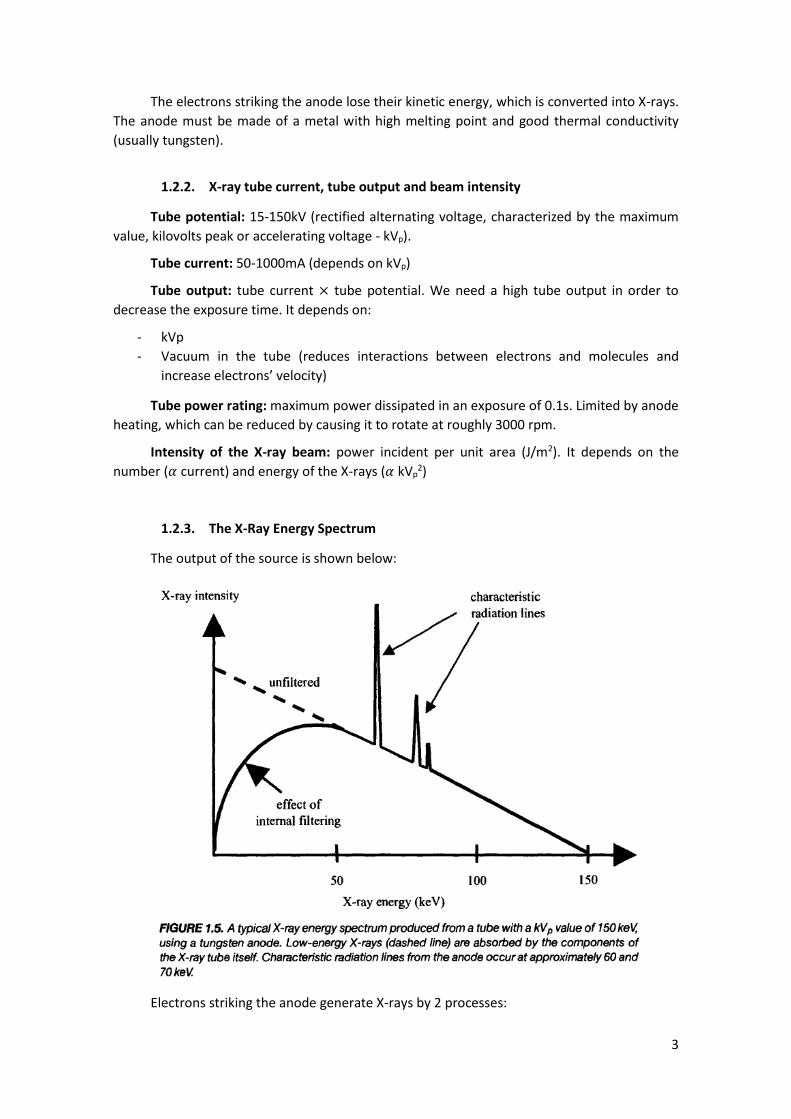
1.2.3. The X-Ray Energy Spectrum
The output of the source is shown below:
Electrons striking the anode generate X-rays by 2 processes:
4
-Bremsstrahlung: generated when an electron is deflected by the tungsten nucleus, losing
kinetic energy which is emitted as an X-ray. The Bremsstrahlung radiation has a wide range of
energies, with a maximum corresponding to the case where all the electron’s kinetic energy is
converted into a single X-ray (with energy kVp). It is characterized by a linear decrease in X-ray
intensity with increasing X-ray energy, however many low energy X-rays are absorbed within the
tube (additional external filters are used because low energy X-rays would be incapable of
passing through the patient, adding to the dose unnecessarily).The efficiency, 𝜂, of the
Bremsstrahlug is given by:
𝜂 = 𝑘(𝑘𝑉𝑝)𝑍
k – constant related to the target material
Z – atomic number of the target material
-Characteristic Radiation: shown as sharp peaks. It is emitted when an accelerated
electron hits an electron in the inner shell of the tungsten atom, causing it to be ejected. An
electron from the outer shell fills the hole, which causes a loss in potential, emitted as an X-ray.
Only happens for incoming electrons with energy > 70 keV.
1.3. Interactions of X-rays with tissue
The X-ray can be classified according to the type of interaction:
- Primary interaction: passes through the body with no interaction.
- Secondary interaction: scattered radiation, whose trajectory between source and
detector was altered. Caused by coherent and Compton scattering.
- Absorbed radiation: absorbed radiation that does not reach the detector. Caused by
photoelectric interactions.
1.3.1. Coherent Scattering
Also called Rayleigh scattering. The radiation is absorbed by the tissue’s atoms and then
emitted in a random direction. Reduces the quantity of X-rays reaching the detectors and alters
their trajectory.
1.3.2. Compton Scattering
Refers to the interaction between an incident X-ray and a loosely bound electron in an
outer shell of an atom in tissue. A fraction of the X-ray energy is transferred to the electron, the
electron is ejected and the X-ray is deflected from its original path. The difference in energy is
very small, which means that this radiation is detected with approximately the same efficiency
as primary radiation. Also, it does not depend on atomic number, thus it is absorbed the same
way in different tissues.
1.3.3. Photoelectric Effect
The energy of the incident X-ray is absorbed by an atom, with a tightly bound electron
being emitted from the K or L shells. A second electron with a higher energy level then fills the
hole, emitting a characteristic X-ray with very low range that does not reach the detector. For
an incident energy just higher than K-shell, the probability of photoelectric interactions is very
high and is given by:

5
1.4. Linear and mass attenuation coefficients of X-rays in tissue
Attenuation of the X-ray beam through tissue is given by:
𝜇 – linear attenuation coefficient
The value of 𝜇 is given by:
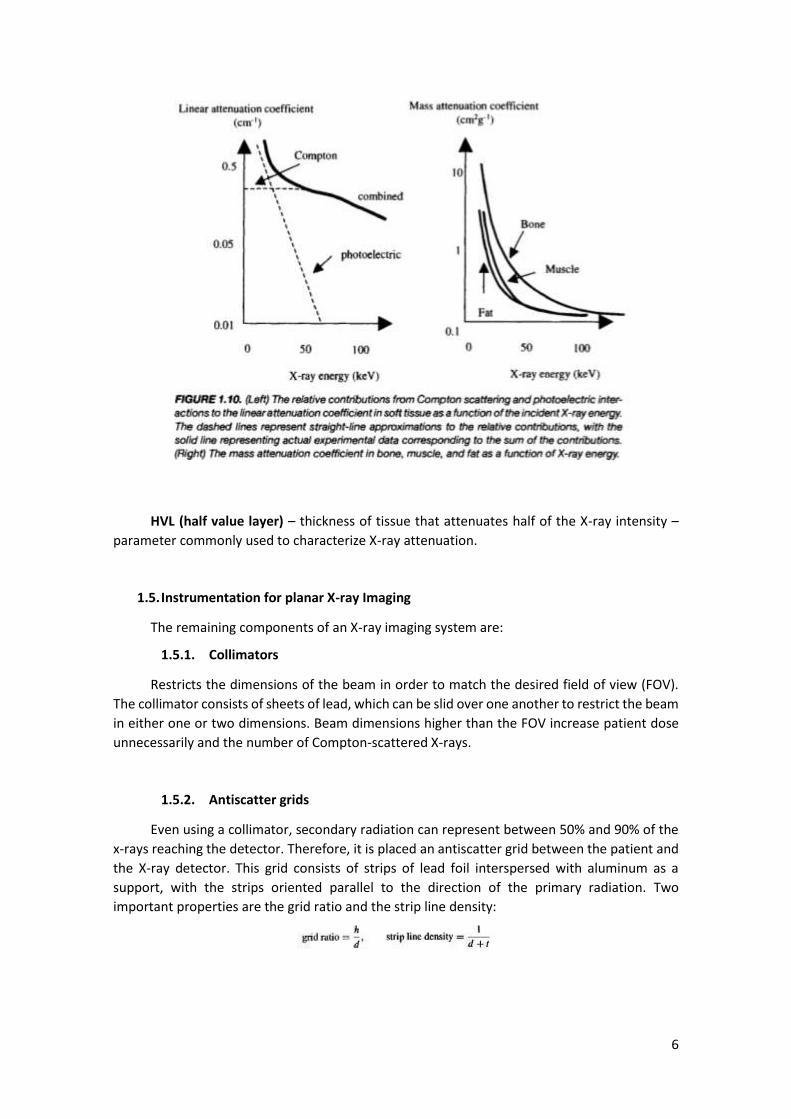
Contributions of photoelectric interactions dominate at lower energies, whereas
Compton scattering is more important at higher energies. X-ray attenuation is often
characterized by mass attenuation coefficient which is equal to the linear attenuation coefficient
divided by the density of the tissue. We can see from the graph below (right) that, at higher
energies, little differentiation is possible because the number of photoelectric interactions
decreases.
6
HVL (half value layer) – thickness of tissue that attenuates half of the X-ray intensity –
parameter commonly used to characterize X-ray attenuation.
1.5. Instrumentation for planar X-ray Imaging
The remaining components of an X-ray imaging system are:
1.5.1. Collimators
Restricts the dimensions of the beam in order to match the desired field of view (FOV).
The collimator consists of sheets of lead, which can be slid over one another to restrict the beam
in either one or two dimensions. Beam dimensions higher than the FOV increase patient dose
unnecessarily and the number of Compton-scattered X-rays.
1.5.2. Antiscatter grids
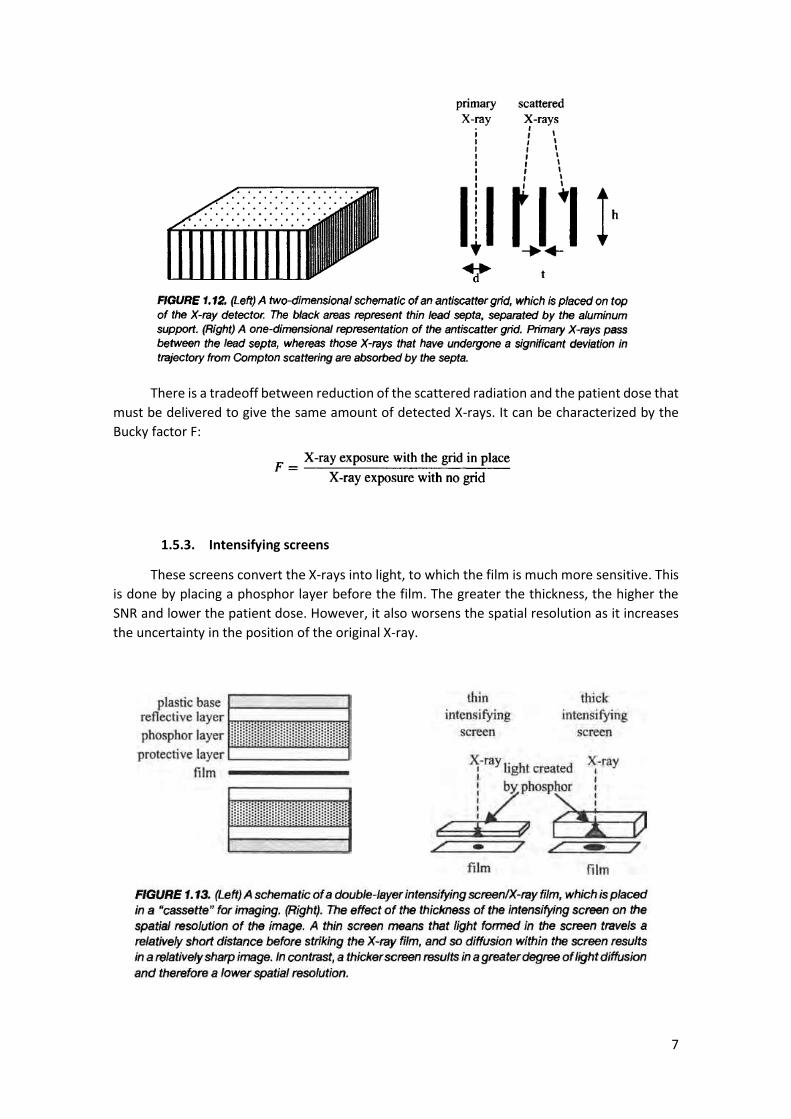
Even using a collimator, secondary radiation can represent between 50% and 90% of the
x-rays reaching the detector. Therefore, it is placed an antiscatter grid between the patient and
the X-ray detector. This grid consists of strips of lead foil interspersed with aluminum as a
support, with the strips oriented parallel to the direction of the primary radiation. Two
important properties are the grid ratio and the strip line density:
7
There is a tradeoff between reduction of the scattered radiation and the patient dose that
must be delivered to give the same amount of detected X-rays. It can be characterized by the
Bucky factor F:
1.5.3. Intensifying screens
These screens convert the X-rays into light, to which the film is much more sensitive. This
is done by placing a phosphor layer before the film. The greater the thickness, the higher the
SNR and lower the patient dose. However, it also worsens the spatial resolution as it increases
the uncertainty in the position of the original X-ray.

8
1.5.4. X-ray film
The presence of lighter regions is due to a chemical reaction of silver particles in the film
to metallic silver. This reaction is reduced in the areas where light hits the film, so the degree of
“blackening” depends on the intensity and time of the light hitting a specific area. This
blackening is measured by the optical density (OD):
Ii – intensity of the light incident on.
It – intensity of the light transmitted through the X-ray film.
1.6. X-Ray image characteristics
1.6.1. Signal to Noise Ratio
SNR is proportional to the statistical variance in the number of X-rays per unit area
(quantum mottle). Since this variance is characterized by a Poisson distribution, SNR is
proportional to the square root of the number of detected X-rays per unit area (N). It is affected
by:
- X-ray tube voltage: the higher the kVp, the higher high-energy X-rays produced and
thus, the number of X-rays reaching the film (↑1)
- X-ray tube current (↑)
- X-ray exposure time (↑)
- Intensifying screen thickness (↑)
- X-ray filtration (↓)
- Object thickness (↓)
- Antiscatter grid ratio (↓)
1.6.2. Spatial Resolution
The main factors affecting it are:
- Effective focal spotsize (↑2)
- Magnification factor (↑)
- Film speed (↑)
- Intensifying screen thickness (↑)
The resultant spatial resolution is given by:
1 The arrows represent what happens to SNR if we increase the value of each given factor. 2 ↑ means higher R, the minimum distance which can be resolved, this is, worse resolution.

9
1.6.3. Contrast to Noise Ratio
Refers to the difference in signal intensity from various regions of the body (for example
the difference between the SNR of bone and soft tissue). It is affected by all the factors that
affect SNR and R, in addition to:
- Energy of the X-ray: if high energies are used, Compton scattering dominates (↓)
- FOV: for values between 10cm and 30cm, the proportion of Compton scattering
reaching the detector increases linearly. After that, it is constant.
- Geometry of the antiscatter grid
1.7. X-ray contrast agents
X-ray contrast agents are chemicals that are introduced in the body to increase image
contrast. Some examples are the barium sulfate and the iodine-based X-ray contrast agents.
These chemicals have a particular K-edge energy that can be used to distinguish the tissues on
which they accumulate from the surroundings.
1.8. X-Ray Imaging methods
The main imaging techniques that use X-rays are:
1.8.1. X-ray angiography
Angiography techniques produce images that show selectively the blood vessels in the
body. Iodine-based contrast agents are injected into the bloodstream to improve contrast. A
related imaging technique called digital subtraction angiography consists on taking an image
before the agent is administered and one after, and then compute the difference (yielding very
high contrast).
1.8.2. X-ray fluoroscopy
X-ray fluoroscopy is a continuous imaging technique using X-rays with very low energies
(used, for example, for placement of stents and catheters). Since very low energies cause low
SNR because of the quantum mottle, a fluoroscopic image intensifier (CsI:Na) is used to improve
the SNR. A fluorescent screen is used to continuously monitor the area of interest.
1.8.3. Dual-Energy Imaging
Technique that produces two separate images corresponding to soft tissue and bone
(used for imaging the chest region). There are 2 ways of performing dual-energy imaging:
- Two X-ray exposures, one applied immediately after the other, with different values of
kVp;
- Single exposure and 2 detectors. The detector placed directly beneath the patient
absorbs low energy X-rays and hardens the beam detected by the second detector.
Therefore, the image from the first detector corresponds to a low energy x-ray, high

10
contrast image, and that from the second, to a high energy x-ray, low contrast image. If
more beam hardening is required, a copper filter can be put in front of the second
detector.
1.9. Clinical applications of X-ray imaging
Apart from the ones described above, there are additional applications of X-ray imaging:
1.9.1. Mammography
X-ray mammography is used to detect small lesions in the breasts. It requires very high
spatial resolution and CNR to detect the microcalcifications (<1mm).
- A low dosage is also important to avoid tissue damage (a molybdenum filter is used to
remove high energies, which also improves CNR);
- Fast intensifying screen/film combinations are necessary to allow the use of low Kvp to
optimize SNR;
- Large source to detector distance and small focal spot size to increase resolution.
1.10. Computed Tomography
CT enables the acquisition of 2D thin slices, which can be obtained in order to reconstruct
a 3D volume. These 2D slices are reconstructed from a series of 1 dimensional projections of the
object acquired at different angles. The detectors, which are situated opposite to the x-ray
source, detect the total number of x-rays transmitted through the patient, producing a one
dimensional projection. The signal intensities in this projection are dictated by the two
dimensional distribution of the tissue attenuation coefficients within the slice. The X-ray source
and the detectors are then rotated by a certain angle and the measurements are repeated. The
image is reconstructed by a process termed backprojection.
1.10.1. Scanner instrumentation
The basic operation of a 1st generation scanner is shown below:
11
The image acquired this way has M X N points. The spatial resolution could be increased
by using finer translational steps or the angular increments, up to a value limited by the effective
x-ray focal spot size.
The 2nd generation replaced the single beam by a fan beam and used multiple detectors,
which reduced the scanning time. It required the development of fan-beam backprojection.
The 3rd generation uses a much wider x-ray fan beam (45º) and an increased number of
detectors (between 512 and 768). Two collimators are used to restrict the fan beam and the
slice thickness (1-5mm). The rotation covers 360º.
In the 4th generation detectors, a complete ring of detectors surrounds the patient. No
decrease in scanning time.
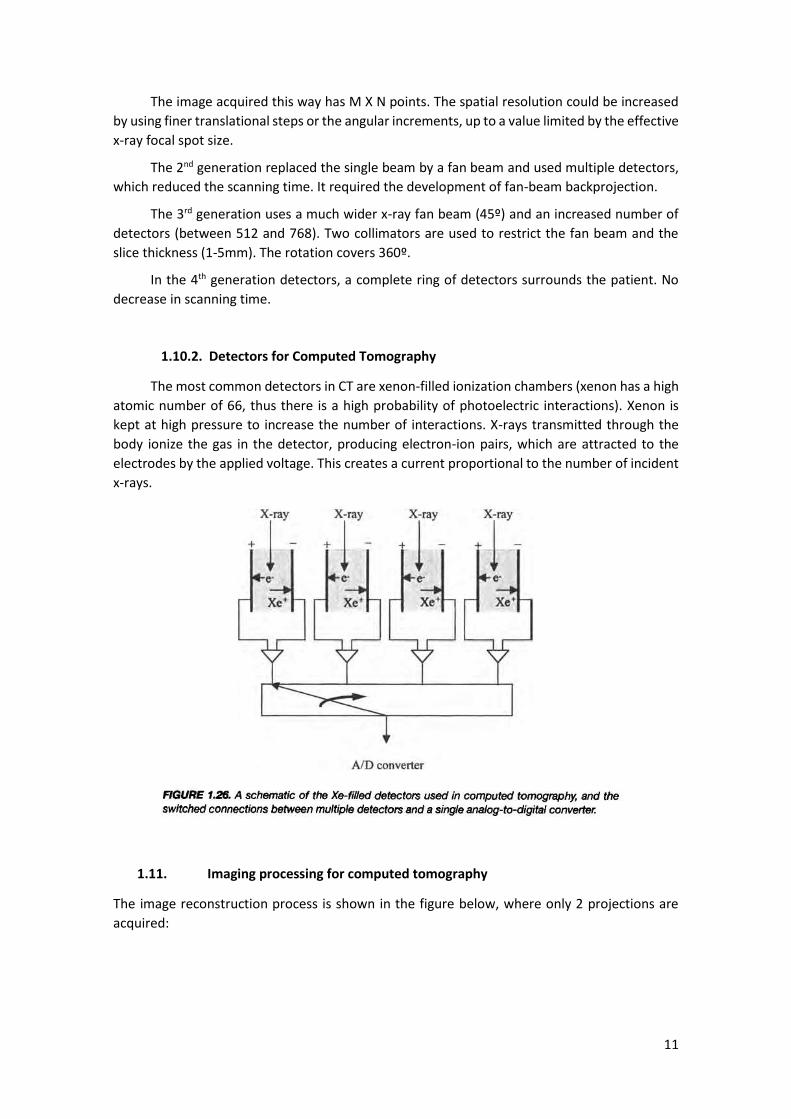
1.10.2. Detectors for Computed Tomography
The most common detectors in CT are xenon-filled ionization chambers (xenon has a high
atomic number of 66, thus there is a high probability of photoelectric interactions). Xenon is
kept at high pressure to increase the number of interactions. X-rays transmitted through the
body ionize the gas in the detector, producing electron-ion pairs, which are attracted to the
electrodes by the applied voltage. This creates a current proportional to the number of incident
x-rays.
1.11. Imaging processing for computed tomography
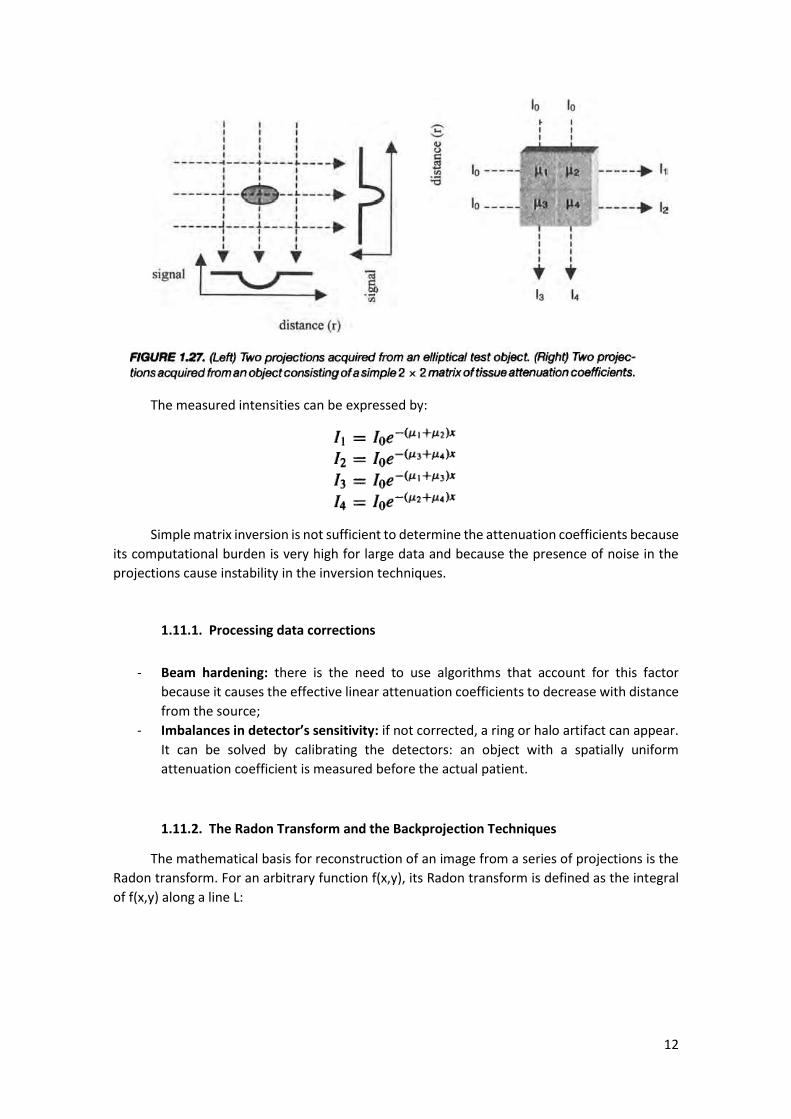
The image reconstruction process is shown in the figure below, where only 2 projections are
acquired:
12
The measured intensities can be expressed by:
Simple matrix inversion is not sufficient to determine the attenuation coefficients because
its computational burden is very high for large data and because the presence of noise in the
projections cause instability in the inversion techniques.
1.11.1. Processing data corrections
- Beam hardening: there is the need to use algorithms that account for this factor
because it causes the effective linear attenuation coefficients to decrease with distance
from the source;
- Imbalances in detector’s sensitivity: if not corrected, a ring or halo artifact can appear.
It can be solved by calibrating the detectors: an object with a spatially uniform
attenuation coefficient is measured before the actual patient.
1.11.2. The Radon Transform and the Backprojection Techniques
The mathematical basis for reconstruction of an image from a series of projections is the
Radon transform. For an arbitrary function f(x,y), its Radon transform is defined as the integral
of f(x,y) along a line L:

13
Each X-ray projection, 𝑝(𝑟, 𝜃), can therefore be expressed as a function of the Radon
transform of the object:
To obtain the reconstructed image we need to compute the inverse Radon transform by
using filtered backprojection. The image is displayed as a map of the tissue CT number, defined
by:
𝜇0- linear attenuation coefficient of the tissue
1.11.3. Fan-beam reconstructions
The 2nd, 3rd and 4th generation scanners use fan-beams, which are not parallel to one
another, thus the backfiltered algorithms need some modifications. The simplest way is to re-
sort the acquired data in order to form sets of parallel X-ray paths, such as S1D1 and S2D3 in the
following picture:

14
This way, the standard backprojection algorithms can be used.
1.12. Spiral/helical computed tomography
To avoid the time delay and the spatial misregistrations between slices due to the patient
movement, a technique called spiral or helical CT was developed. This technique acquires data
as the table moves continuously through the scanner. This allows 10 times faster scan times and
the acquisition of very fast 3D vascular imaging datasets just after injection of an iodinated
contrast agent, resulting in significant increase in SNR of the angiograms.
In terms of instrumentation, the main difficulty is that X-rays must be produced
continuously, without the cooling period. Therefore, the X-ray source must be designed to have
a high heat capacity and a very efficient cooling. Moreover, detectors must be very efficient in
order to reduce the tube current and alleviate the anode heating (for example, scintillation
crystals, made of BGO, are used since they have a high efficiency – 75-85% in converting X-rays
to light).
The most important acquisition parameter in helical CT is the spiral pitch:
Where d is the table feed per rotation and S is the slice thickness.
p typically lies between 1 and 2, thus the radiation dose is lower than in single-slice CT.
For values of p less than 1, the x-ray beams of adjacent spirals overlap, resulting in high tissue
radiation dose. For values of p greater than 2, gaps appear in the data sampled along the
longitudinal axis and image blurring happens due to the patient movement.
Due to the helical trajectory, modifications of the backprojection reconstruction must be
made. The modified algorithms use linear interpolation of data 180º apart on the spiral
trajectory to estimate the data that would be obtained with a stationary table.
1.13. Multislice spiral computed tomography
Multislice spiral CT incorporates an array of detectors in the z direction (direction of table
motion). It improves efficiency by allowing higher values of the table feed to be used and, thus,
lower scan times. The spiral pitch 𝑝𝑚𝑠 is defined slightly different:
Where Ssingle is the single-slice collimated beam width
In a multislice system, the focal-spot-to-isocenter and the focal-spot-to-detector
distances are shortened compared to the single-slice scanner and the number of detectors in
the longitudinal direction is increased from one long element to a number of shorter elements.
There are 2 types of detector arrangements:
- Fixed – consists of 16 elements with a total length of 2 cm. Signals from sets of 4
individual elements are typically combined. Only fixed values of pitch can be chosen.
15
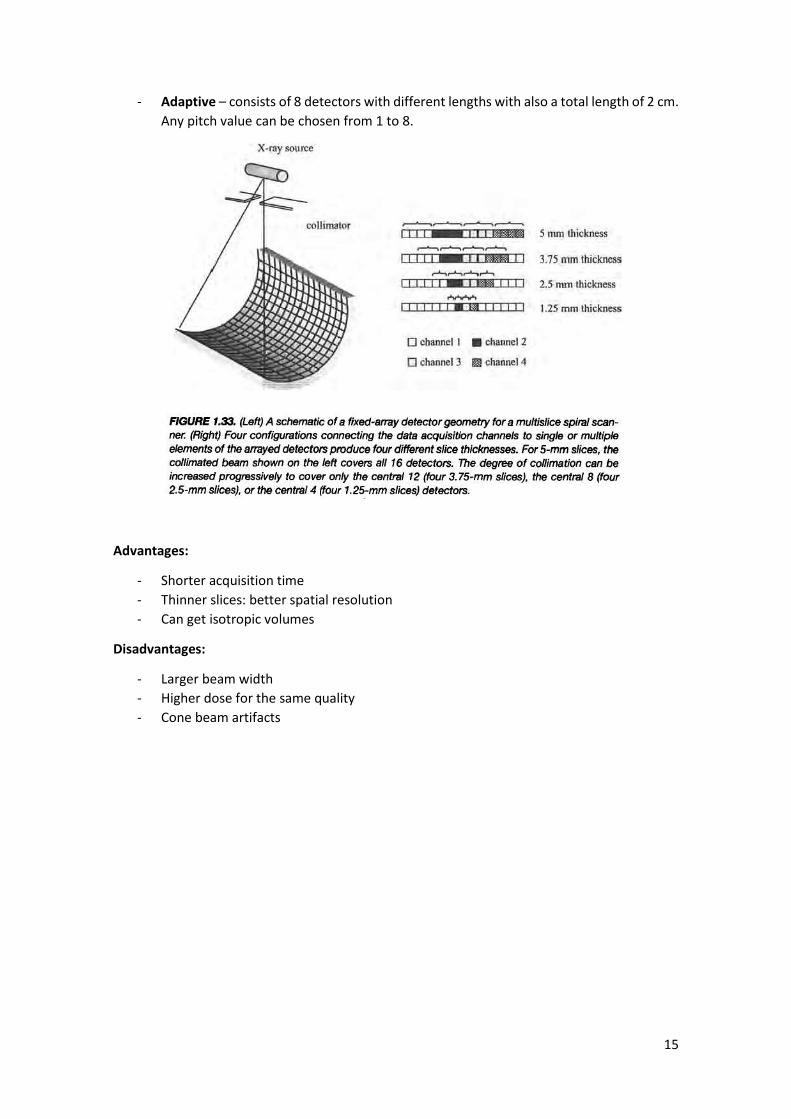
- Adaptive – consists of 8 detectors with different lengths with also a total length of 2 cm.
Any pitch value can be chosen from 1 to 8.
Advantages:
- Shorter acquisition time
- Thinner slices: better spatial resolution
- Can get isotropic volumes
Disadvantages:
- Larger beam width
- Higher dose for the same quality
- Cone beam artifacts

16
2. Nuclear Medicine
2.1. General principles of nuclear medicine
Nuclear medicine images the spatial distribution of radiopharmaceuticals introduced in
the body. It can detect biochemical changes in tissue, serving as a diagnostic to pathological
conditions such as formation of edema, tumor enlargement or metastasis, and changes in the
tissue morphology. These radiopharmaceuticals, termed radiotracers, are compounds linked to
a radioactive element, whose structure determines its distribution in the body. Radiation,
usually in the form of 𝛾-rays, is detected using a gamma camera. The following picture shows
the basic principles and instrumentation involved:
Decay of the radioactive element produces 𝛾-rays, which emanate in all directions.
Attenuation of 𝛾-rays occurs the same way as in X-rays. In order to determine the position of
the source of the 𝛾-rays, a collimator is placed between the patient and the detector so that
only those components of radiation that have a trajectory at an angle close to 90º to the
detector plane are recorded. A scintillation crystal is used to convert the 𝛾-rays into light. These
light photons are in turn converted into an electrical signal by photomultiplier tubes (PMTs). The
image is formed by analyzing the spatial distribution and the magnitude of the electrical signals
from each PMT. Planar nuclear images are characterized as having poor SNR and low spatial
resolution (~5 mm), but extremely high specificity because there is no background radiation in
the body.

17
3D nuclear images can be produced using the principle of tomography. A rotating gamma
camera is used in a technique called single photon emission computed tomography (SPECT). The
most recently developed technique is positron emission tomography (PET), which is based on
positron-emitting radiotracers. This technique has a sensitivity advantage over SPECT of 2 to 3
orders of magnitude.
2.2. Radioactivity
Radioactivity is an intrinsic property of particular isotopes that have unstable nuclei. The
phenomenon of radioactivity refers to the process whereby various forms of radiation are
emitted as result of spontaneous change in the composition of the nucleus. The stability of a
nucleus is dictated by the relationship between Z (nº protons) and A (nº protons +neutrons).
Strong neutron-neutron, proton-neutron and proton-proton forces are attractive over very
short distances, whereas electromagnetic forces between protons are repulsive, and so the
nucleus stability is determined by the balance between these forces. For A<50, the stable
configuration corresponds to a 1:1 ratio, whereas for A>50, the ratio of neutrons increases:
The radioactivity, or activity, Q, of a radionuclide is defined as the nº of disintegrations
per unit time (in Curies, Ci=3.7X1010 N/s) where 𝜆 is the decay constant:
It can be solved to give:
The half-life corresponds to the time required for the radioactivity to drop one-half of its
current value:
When calculating the time dependence of radioactivity within the body for a nuclear
medicine scan, the biological half-life of the radionuclide must be considered:
18
2.3. Production of radionuclides
There are 4 basic methods for producing radionuclides:
- Neutron capture
- Nuclear fission (uses fast high energy neutrons to create 99Mo 133Xe and 131I)
- Charged particle bombardment (uses a cyclotron to accelerate ionized hydrogen or
deuterium gas and create 201Ti, 67Ga, 111In or 123I)
- Radionuclide generators (most common method, via on-site generator)
2.4. Types of radioactive decay
Radioactive elements can decay via a number of mechanisms, of which the most
important in nuclear medicine are:
- 𝛼-particle decay
- 𝛽-particle emission
- 𝛾-ray emission
- Electron emission
The most useful radionuclides are the ones that emit 𝛾-rays or X-rays because these forms
of radiation can pass through tissue and reach the detector. A useful parameter to quantify
attenuation is the HVL.
An 𝛼-particle consists of a helium nucleus. It has a tissue HVL of only a few mm and, thus,
it is not directly related to nuclear medicine. This form of radioactive decay occurs mainly for
radionuclides with Z>150.
A 𝛽-particle is an electron. Radioactive decay occurs via conversion of a neutron into a
proton, with emission of a high energy 𝛽-particle and an antineutrino. Kinetic energy is shared
in a random manner between the 𝛽-particle and the neutrino, and hence the electron has a
continuous range of energies (e.g.: a 1MeV 𝛽-particle has a HVL=0.4 mm while a 5MeV 𝛽-particle
has a HVL=4 mm).
Due to their low HVL, radionuclides that produce 𝛼 and 𝛽 particles cannot be used for
imaging.
No radionuclide can decay solely by 𝛾-ray emission, but certain decay schemes result in
formation of an intermediate species that exists in a metastable state. This is the case of 99mTc,
which is the most widely used:
The energy of the emitted 𝛾-ray for the 99mTc is 140 keV. Below an energy of 100 keV most
𝛾-rays are absorbed in the body via photoelectric interactions. Above 200 keV, 𝛾-rays penetrate
the thin collimator septa, thus the ideal energy range lies between 100 and 200 keV.

19
The final mechanism of radioactive decay is the electron capture (with subsequent 𝛾-ray
or X-ray emission), in which an orbital electron from the K or L shell is captured by the nucleus,
leaving a hole that is occupied by an outer electron. This process produces characteristic X-rays.
For clinical imaging, an ideal radionuclide should have a half-life short enough to limit the
dose to the patient but long enough such that the radioactivity is not exhausted by the time the
nuclide has distributed within the body. The radioactive decay should be via monochromatic 𝛾-
ray emission to a stable nuclear state, without 𝛼 or 𝛽-particle emission.
2.5. Technetium generator
99mTc is the most used radionuclide because:
- Can be produced from an on-site generator
- Half-life of 6.02h
- Very minor 𝛽-particle emission
- HVL of 4.6 cm
The generator consists of an alumina ceramic column with 99Mo on its surface. The 99mTc
is obtained by flowing an eluting solution through the generator, which washes out the 99mTc,
leaving behind the 99Mo. Typically, the technetium is eluded every 24h and the generator is
replaced once a week.
2.6. Biodistribution of the technetium-based agents within the body
The majority of radiopharmaceuticals uses ionic technetium (TC4+), which is bind to a
metal ion according to the target organ.
2.7. Instrumentation: the gamma camera
20
The roles of each component of the gamma camera are listed below:
2.7.1. Collimator
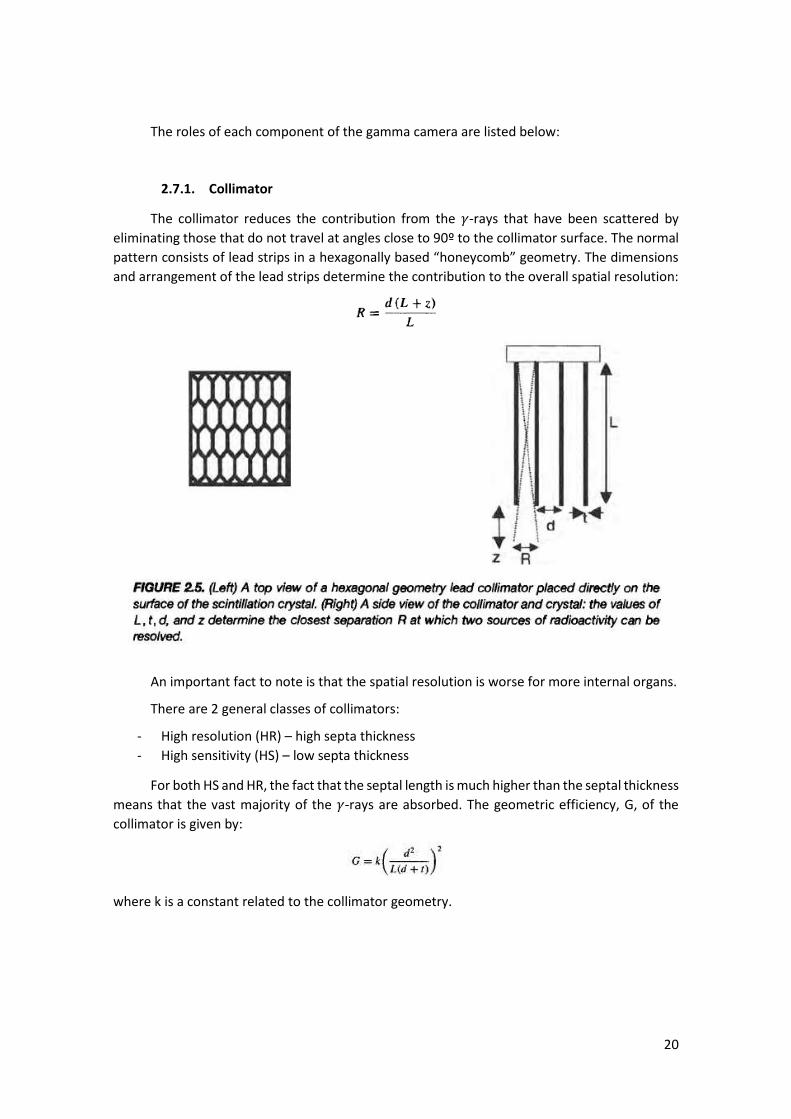
The collimator reduces the contribution from the 𝛾-rays that have been scattered by
eliminating those that do not travel at angles close to 90º to the collimator surface. The normal
pattern consists of lead strips in a hexagonally based “honeycomb” geometry. The dimensions
and arrangement of the lead strips determine the contribution to the overall spatial resolution:
An important fact to note is that the spatial resolution is worse for more internal organs.
There are 2 general classes of collimators:
- High resolution (HR) – high septa thickness
- High sensitivity (HS) – low septa thickness
For both HS and HR, the fact that the septal length is much higher than the septal thickness
means that the vast majority of the 𝛾-rays are absorbed. The geometric efficiency, G, of the
collimator is given by:
where k is a constant related to the collimator geometry.
21
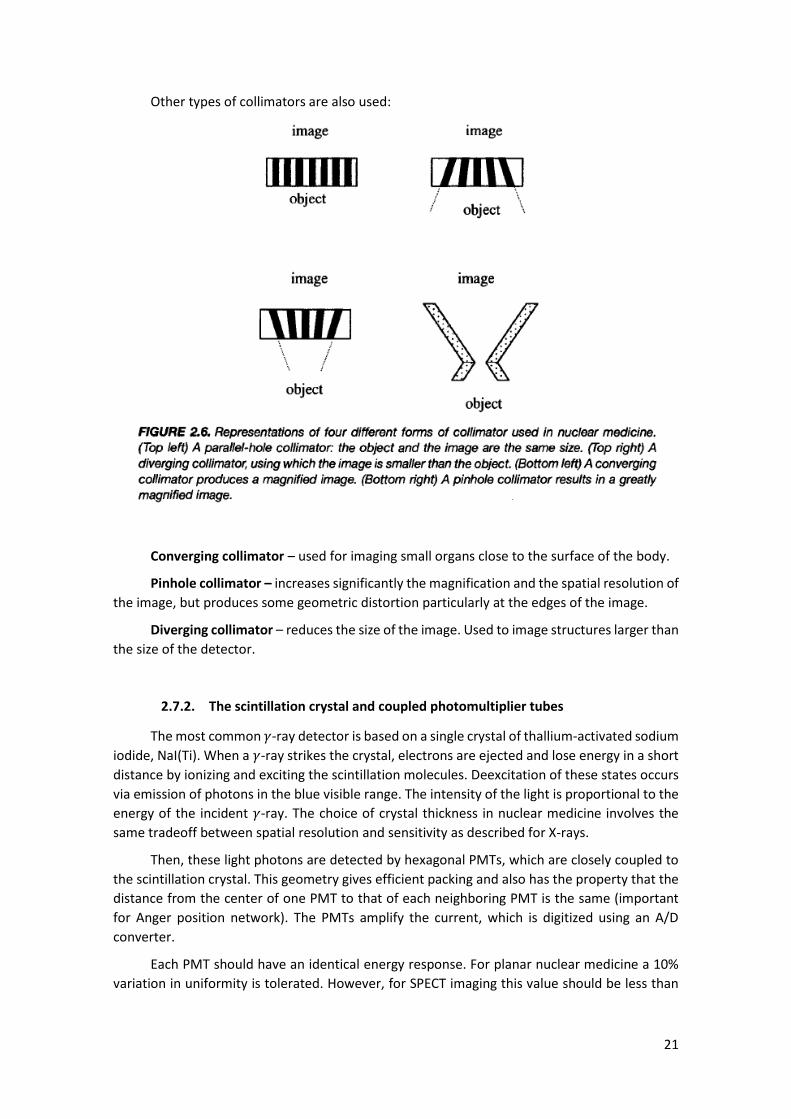
Other types of collimators are also used:
Converging collimator – used for imaging small organs close to the surface of the body.
Pinhole collimator – increases significantly the magnification and the spatial resolution of
the image, but produces some geometric distortion particularly at the edges of the image.
Diverging collimator – reduces the size of the image. Used to image structures larger than
the size of the detector.
2.7.2. The scintillation crystal and coupled photomultiplier tubes
The most common 𝛾-ray detector is based on a single crystal of thallium-activated sodium
iodide, NaI(Ti). When a 𝛾-ray strikes the crystal, electrons are ejected and lose energy in a short
distance by ionizing and exciting the scintillation molecules. Deexcitation of these states occurs
via emission of photons in the blue visible range. The intensity of the light is proportional to the
energy of the incident 𝛾-ray. The choice of crystal thickness in nuclear medicine involves the
same tradeoff between spatial resolution and sensitivity as described for X-rays.
Then, these light photons are detected by hexagonal PMTs, which are closely coupled to
the scintillation crystal. This geometry gives efficient packing and also has the property that the
distance from the center of one PMT to that of each neighboring PMT is the same (important
for Anger position network). The PMTs amplify the current, which is digitized using an A/D
converter.
Each PMT should have an identical energy response. For planar nuclear medicine a 10%
variation in uniformity is tolerated. However, for SPECT imaging this value should be less than
22
1%. In practice, calibration is done using samples of uniform and known radioactivity or, more
recently, through a LED calibration source for each PMT in real time.
2.7.3. The Anger position network and the Pulse Height Analyzer
By comparing the magnitudes of the currents from all of the PMTs, the location of
individual scintillations within the crystal can be estimated. This calculation is done by using an
Anger logic circuit. This network produces four output signals, X+, X-, Y+ and Y-, the relative
magnitudes and signs of which define the location of the scintillation in the crystal. The summed
signal, termed the z-signal, is sent to a pulse-height analyzer (PHA), which compares the z-signal
to a threshold value to determine if it was originated by a scattered 𝛾-ray (for a 99mTC scan, it
corresponds to that produced by a 𝛾-ray with energy 140 keV). The z-signal is accepted if its
energy is inside a certain interval given by the full-width half-maximum (FWHM) of the
photopeak: the narrower the FWHM, the better it is at discriminating between scattered and
unscattered 𝛾-rays. Typically, a 15% interval is used.
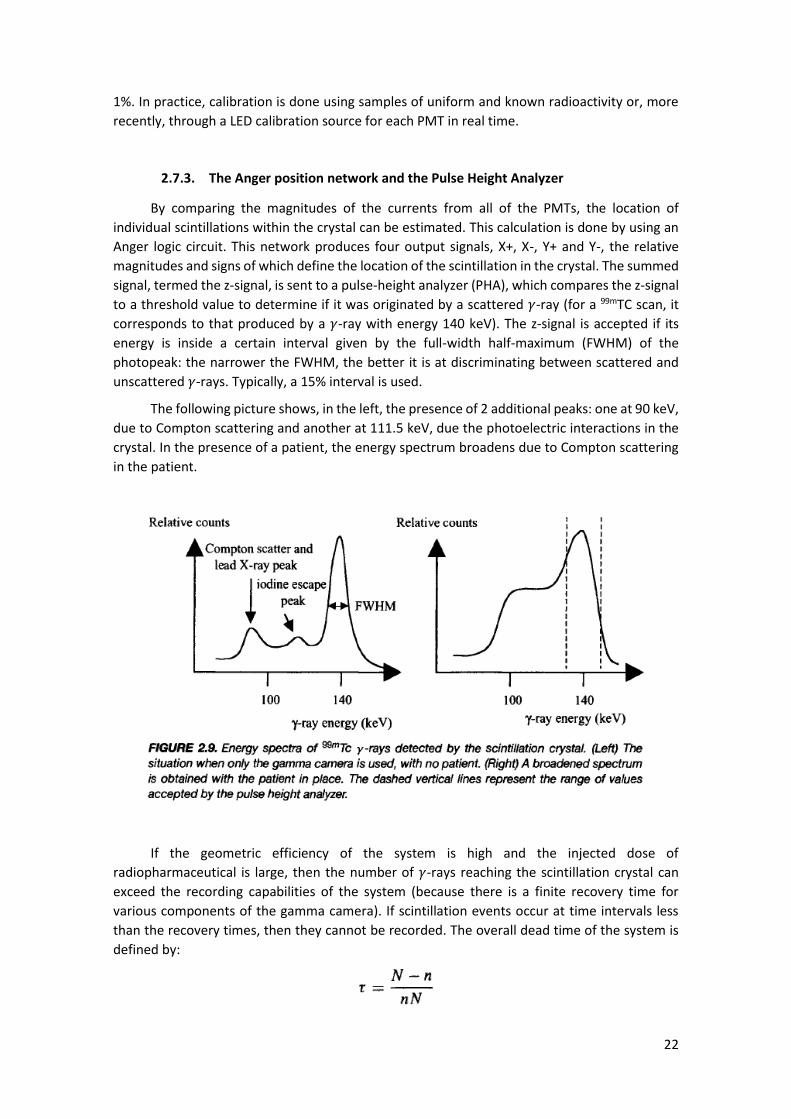
The following picture shows, in the left, the presence of 2 additional peaks: one at 90 keV,
due to Compton scattering and another at 111.5 keV, due the photoelectric interactions in the
crystal. In the presence of a patient, the energy spectrum broadens due to Compton scattering
in the patient.
If the geometric efficiency of the system is high and the injected dose of
radiopharmaceutical is large, then the number of 𝛾-rays reaching the scintillation crystal can
exceed the recording capabilities of the system (because there is a finite recovery time for
various components of the gamma camera). If scintillation events occur at time intervals less
than the recovery times, then they cannot be recorded. The overall dead time of the system is
defined by:
23
where N in the true count rate and n is the observed count rate. Standard gamma cameras
typically have a 20% loss in the number of counts.
2.8. Image characteristics
Nuclear medicine images are characterized by low SNR and poor spatial resolution, but an
extremely high CNR. Postprocessing is used to increase the image SNR, although this further
degrades the spatial resolution.
2.8.1. Signal to Noise Ratio
The number of disintegrations per unit time fluctuates around an average value described
by a Poisson distribution and, thus, SNR is proportional to the square root of the number of
counts (√𝑁). The factors that affect SNR are:
- Radioactive dose administered (↑) – comparing to X-rays, the number of counts is
10000 times lower
- Effectiveness of the radiopharmaceutical at targeting a specific organ (↑)
- Time over which the image is acquired (↑) – limited by radioactive and biological half-
lives
- Sensitivity of the gamma camera (↑) – related to the collimator geometry and the
thickness of the scintillation crystal
- Postacquisition image filtering (↑) – by applying low pass filters (however causes blur)
2.8.2. Spatial Resolution
There are 4 major contributions to the spatial resolution of a nuclear medicine scan:
- Intrinsic spatial resolution of the gamma camera, excluding the collimator (↑) – reflects
the uncertainty in the exact location at which light is produced in the scintillation crystal
due to thickness of the crystal and the Anger position encoder (~3-5 mm).
- Geometry of the collimator
- Degree of Compton scattering (↑) – goes up with depth of the radiopharmaceutical
within the body
- Postacquisition image filtering (↑)
Considering the first 3 terms, the overall spatial resolution is given by:
Typical values are approximately 1-2 cm and 5-8 mm for organs in depth and close to the
surface of the collimator, respectively.
2.8.3. Contrast to Noise Ratio
If there’s no background signal (due to the fact that the radiopharmaceutical did not
distribute out of the targeted area), then CNR ~ SNR. It is affected by:

24
- Compton scattering (↓)
- Partial volume effects (↓) – depends on R
- Postprocessing filtering
2.9. Single photon emission computed tomography
SPECT applies tomographic principles to produce a series of 2D images. Its main image
characteristics are:
- CNR: improved by up to a factor of 5 to 6 times because sources of radioactivity are not
superimposed.
- R: not changed. Approximately Gaussian PSF with FWHM ~1 cm
- SNR: it needs about 5 times as many counts to obtain an equivalent SNR as in planar
scintigraphy (~500,000 counts in brain and ~100,000 counts in myocardium)
It is the standard acquisition modality for myocardial and brain perfusion and for
oncological investigations.
2.9.1. Instrumentation for SPECT
SPECT can be performed using either multidetector or rotating gamma camera systems.
The former has higher sensitivity and spatial resolution but is very complex and expensive,
making it a rare technique in clinic environment. The latter is preferred for routine clinical
imaging because it can also be used for planar scintigraphy. Data is collected from multiple views
as the detector rotates around the patient. An improvement to this setup is to increase the
number of cameras in the system as the sensitivity per slice is proportional to the number of
cameras. Thus, two and three camera systems are commonly used. A 360º rotation is generally
needed in SPECT because the effects of 𝛾-ray scatter and tissue attenuation and the dependence
of the spatial resolution on the source to detector distance all mean that projections acquired
at 180º to one another are not identical. A focused collimator is used to improve sensitivity,
which requires increased complexity of data reconstruction.
The data matrix acquired is usually 64x64 or 128x128 with first allowing better SNR and
the second allowing better spatial resolution. Projections can be acquired in a “stop-and-go”
mode or in a continuous rotation.
2.9.2. Scatter and attenuation correction
In SPECT, scatter correction is needed because we do not have a well-defined 𝛾-ray
geometry due the lack of tight source collimation. Moreover, tissue attenuation has here a
different role: in CT, the reconstructed image is an estimate of the spatial distribution of X-ray
attenuation coefficients, while in SPECT the reconstructed image is an estimate of the spatial
distribution of injected radiopharmaceutical. Thus, spatially dependent 𝛾-ray attenuation gives
rise to artifacts and need to be corrected. If tissue attenuation is not included, a measured SPECT
projection can be represented as:
25
If we add tissue attenuation, then:
This equation is extremely difficult to solve analytically and, thus, it is an important part
of SPECT data processing.
The scatter correction is done by using a dual-energy window detection method: the main
window contains contributions from both scattered and unscatterd 𝛾-rays (fractional width of
20% around 140keV); the subwindow is set to a lower energy (7% around 121keV). The true
primary 𝛾-rays count can be calculated from:
The attenuation correction can be done using 2 different methods. The first assumes that
𝛾-ray attenuation is uniform throughout the entire body. Thus assumption works well for the
brain, but introduces artifacts in cardiac imaging, for example. The second measures the
attenuation distribution using transmission of a reference activity to make a calibration.
2.10. Clinical applications of nuclear medicine
The major clinical applications are the measurement of blood perfusion in the brain, the
diagnosis of tumors in various organs and the assessment of cardiac function.
2.10.1. Brain Imaging
- Planar scintigraphy using DTPA or 99tTc-glucoheptonate, which do not cross the blood
brain barrier (BBB), can be used to determine a rupture of the BBB as there will be a
high concentration of these radiotracers in the brain.
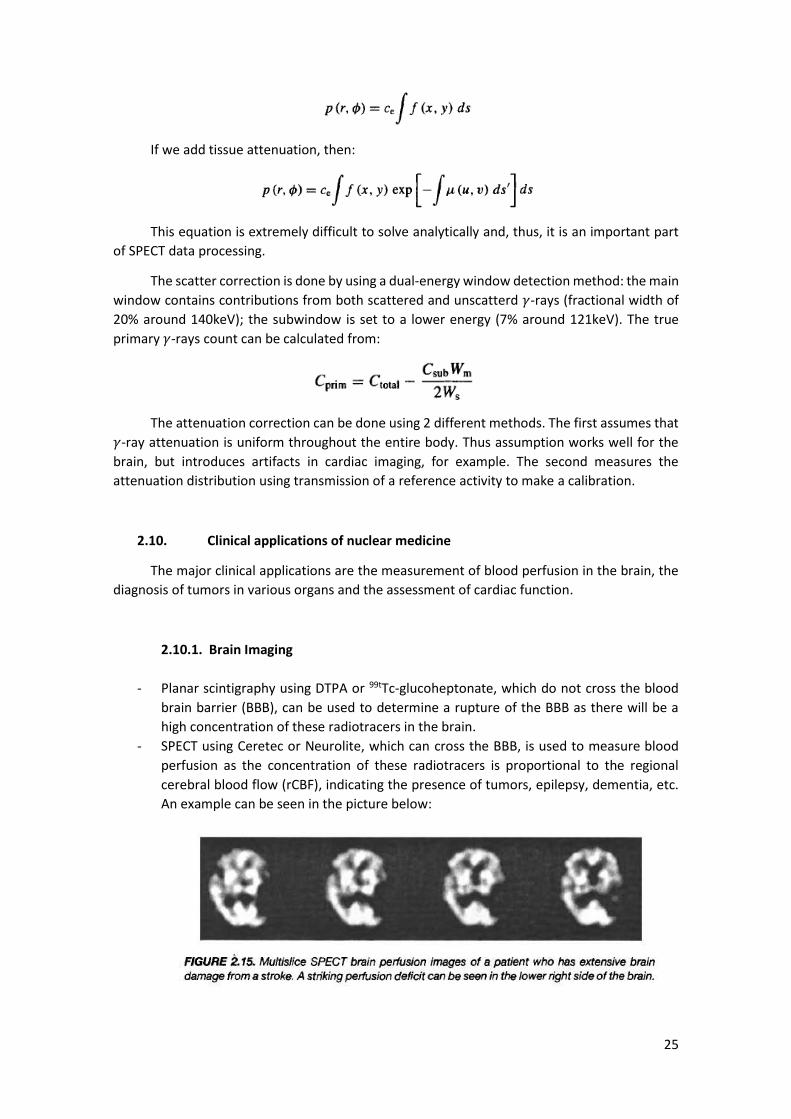
- SPECT using Ceretec or Neurolite, which can cross the BBB, is used to measure blood
perfusion as the concentration of these radiotracers is proportional to the regional
cerebral blood flow (rCBF), indicating the presence of tumors, epilepsy, dementia, etc.
An example can be seen in the picture below:

26
2.10.2. Cardiac Imaging
Cardiac SPECT scans are performed to measure blood flow pattern in the heart and to
detect coronary artery disease and myocardial infarcts. The most common test is the stress test,
used to measure myocardial perfusion and diagnose myocardial ischemia and infarct.
2.11. Positron Emission Tomography
PET, as SPECT, is also a tomographic technique used to measure physiology and function,
rather than gross anatomy. The fundamental difference is that now the radiotracer emits
positrons, which, after annihilation with an electron in the tissue, result in the formation of 2 𝛾-
rays. This fact makes it possible to produce images with much higher SNR and spatial resolution
as we will see.
PET is mainly used in oncology, cardiology and neurology. The main disadvantage is its
high cost and the need to have a cyclotron on-site to produce positron-emitting nuclides.
2.11.1. General principles
The radiotracers used in PET are structural analogs of a biologically active molecule, such
as glucose, in which one or more atoms have been replaced by a radioactive atom. An important
example is the FDG, which contains 18F and [11C]palmitate. Isotopes such as 18F undergo
radioactive decay by emitting a positron, that is, a positively charged electron, and a neutrino:
The positron then annihilates with an electron, resulting in 2 𝛾-rays, each with an energy
of 511 keV, which travel in opposite directions an angle of 180º to one another. Because 2
antiparallel 𝛾-rays are produced and both must be detected, a PET system consists of a complete
ring of scintillation crystals surrounding the patient. Since they are created simultaneously, both
are detected within a certain time window with the 2 crystals that detected them defining a line
along which the annihilation occurred. This process of line definition is called annihilation
coincidence detection (ACD). This difference in localization method is the major reason for the
much higher detection efficiency in PET than in SPECT (moreover, the fact that the 𝛾-ray energy
is much higher means less attenuation, increasing further the sensitivity). The spatial resolution
depends upon a number of factors including the number and size of the individual crystal
detectors (R~3-5 mm).
2.11.2. Radionuclides used for PET
All the radionuclides used in PET are produced by a cyclotron. The most common are 18F, 11C, 15O and 13N.

27
2.11.3. Instrumentation for PET
The major differences are the scintillation crystals needed to detect the 511 keV 𝛾-rays
efficiently and the additional circuitry needed for coincidence detection.
2.11.3.1. Scintillation crystals
They are in large number and are usually formed from bismuth germinate (BGO). The
crystals are coupled to a smaller number PMTs (for cost reasons). Typically, each “block” of
scintillation crystals consists of an 8X8 array cut from a single BGO crystal. Each block is coupled
to 4 PMTs. Four of these blocks are arranged to form a bucket. The full detector ring may have
up to 32 of such buckets. The ideal detector must have a high density and a large effective atomic
number in order to increase the 𝛾-rays detection efficiency by increasing Compton and
photoelectric interactions. The size of the crystal is also important as it affects spatial resolution
(however, crystals too small can cause scatter to adjacent crystals, which reduces resolution;
width for BGO ~1 cm).
2.11.3.2. Annihilation coincidence detection circuitry
The ACD circuitry is designed to maximize the ratio of true-to-false recorded coincidences.
Considered the example in left picture:
A positron is emitted and annihilates with an electron, producing 2 anti-parallel 𝛾-rays.
The first is detected by the crystal number 2 and produces a number of photons. These photons
are converted into an amplified electrical signal at the output of the PMT, which is fed into a
PHA. If the voltage is inside a predefined range, than the PHA generates a logic pulse, which is
sent to the coincidence detector. When the second 𝛾-ray is detected (by the crystal number 10)

28
and produces a voltage that is accepted by the associated PHA, a second logic pulse is sent to
the coincidence detector. This detector sums the 2 logic pulses and passes it through another
PHA, which has a threshold set just under the sum value. If the logic pulses overlap in time, then
the system accepts the 2 𝛾-rays as having evolved from one annihilation and record a line
integral between the 2 crystals.
2.11.4. Image Reconstruction
The process is basically the same as in SPECT, however, prior to reconstruction,
corrections to attenuation and accidental coincidences must be made.
2.11.4.1. Attenuation Correction
The 2 methods available are very similar to the ones described for SPECT.
2.11.4.2. Correction for accidental, multiple and scattered coincidences
The main sources of noise in PET are accidental and scattered coincidences:
The accidental coincidences term is usually much higher. An event of this type is shown
below:
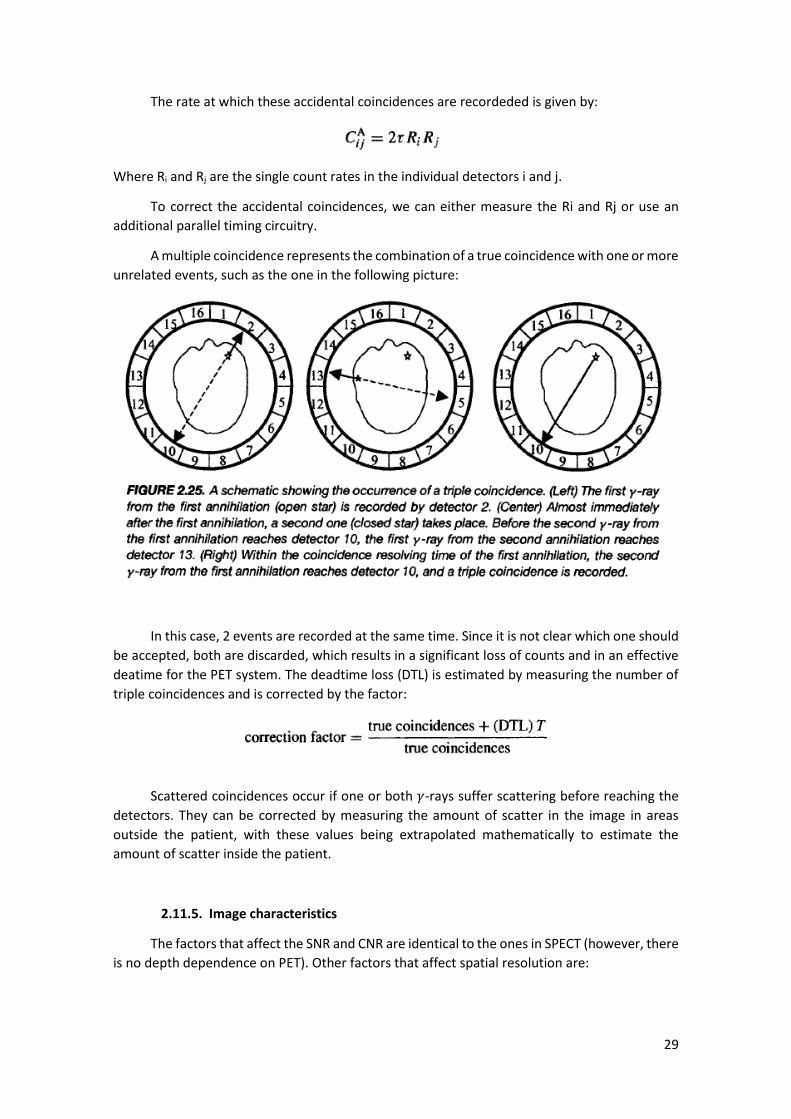
29
The rate at which these accidental coincidences are recordeded is given by:
Where Ri and Rj are the single count rates in the individual detectors i and j.
To correct the accidental coincidences, we can either measure the Ri and Rj or use an
additional parallel timing circuitry.
A multiple coincidence represents the combination of a true coincidence with one or more
unrelated events, such as the one in the following picture:
In this case, 2 events are recorded at the same time. Since it is not clear which one should
be accepted, both are discarded, which results in a significant loss of counts and in an effective
deatime for the PET system. The deadtime loss (DTL) is estimated by measuring the number of
triple coincidences and is corrected by the factor:
Scattered coincidences occur if one or both 𝛾-rays suffer scattering before reaching the
detectors. They can be corrected by measuring the amount of scatter in the image in areas
outside the patient, with these values being extrapolated mathematically to estimate the
amount of scatter inside the patient.
2.11.5. Image characteristics
The factors that affect the SNR and CNR are identical to the ones in SPECT (however, there
is no depth dependence on PET). Other factors that affect spatial resolution are:
30
- Finite distance which the positron travels before annihilation;
- Slight deviation from a nominal angle of 180º due to the motion of the center mass of
the annihilation (non-colinearity)
- Size of the crystal
The overall spatial resolution is given by:
Where krecon is the degradation due to the reconstruction algorithm
2.11.6. Multislice and 3D PET Imaging
Multislice capability can be introduced into PET as for CT by having a number of detector
rings stacked alongside one another. Retractable septa are positioned between each ring: these
are kept in position for multislice operation and retracted for 3D imaging. Sensitivity is about 10
times higher for 3D due to absence of the septa.
2.11.7. Clinical applications of PET
PET is used to provide quantitative information on metabolic and physiological changes in
3 major areas: brain imaging, cardiac studies and tumor imaging.
2.11.7.1. Brain Imaging
In the body, FDB is metabolized in the same way as glucose. Thus, it can cross the BBB.
Inside the cell, FDG is phosphorylated and, unlike glucose, it is trapped inside the cell. The
amount of FDG is therefore proportional to both the initial glucose transport and subsequent
phosphorylation, providing data about the presence of tumors (high metabolic rate) or epilepsy
(low metabolic rate), for example.

31
3. Ultrasonic Imaging
3.1. General principles of ultrasonic imaging
Ultrasound imaging operates at frequencies between 1 and 10 MHz, producing images
based on backscattering of mechanical energy from boundaries between tissues and from small
structures within tissue. It can be used to obtain anatomical information (either at surface, using
higher frequencies, or deep in the body, using lower frequencies) or to measure blood flow (via
Doppler shift).
Advantages: Noninvasive, easily portable, inexpensive diagnostic modality, allowing real-
time imaging and high spatial resolution.
Disadvantages: relatively poor soft-tissue contrast and the fact that gas and bone impede
the passage of ultrasound waves.
Basic principle: A short pulse, typically 1-5 𝜇𝑠, of energy is transmitted into the body,
using an ultrasound transducer. The transducer is focused to produce a narrow ultrasound
beam, which propagates as a pressure wave. When the ultrasound wave encounters boundaries
between tissues or structures within organs, a part of the energy is scattered in all directions,
with a certain fraction being backscattered along the original transmission path and returning
to the transducer, which converts it to a potential (later amplified and digitized). The direction
of the beam is then changed to acquire a second line of data adjacent to the first one and so on.

32
3.2. Wave propagation and characteristic acoustic impedance
A useful model of tissue is that of a lattice of small particles held together by elastic forces:
As the ultrasound energy passes through the tissue, the particles move very short
distances (W) about a fixed mean position, whereas the ultrasonic energy propagates over much
larger distances. The directions of particle vibration and wave propagation are the same
(longitudinal wave). Assuming a planar wavefront and no loss of energy, the particle
displacement W can be described as a function of the sound velocity by:
The value c depends on the tissue density 𝜌 and compressibility 𝜅:
The particle velocity (much slower than c) in the z direction, 𝑢𝑧, is given by
The pressure, p, of the wave is given by:
Because the transducer undergoes sinusoidal motion, 𝑝(𝑡) and 𝑢𝑧(𝑡) can be described as:
The mean intensity is given by
An important parameter in ultrasonic imaging is the characteristic acoustic impedance Z
of the tissue (analog to Ohm’s Law):
33
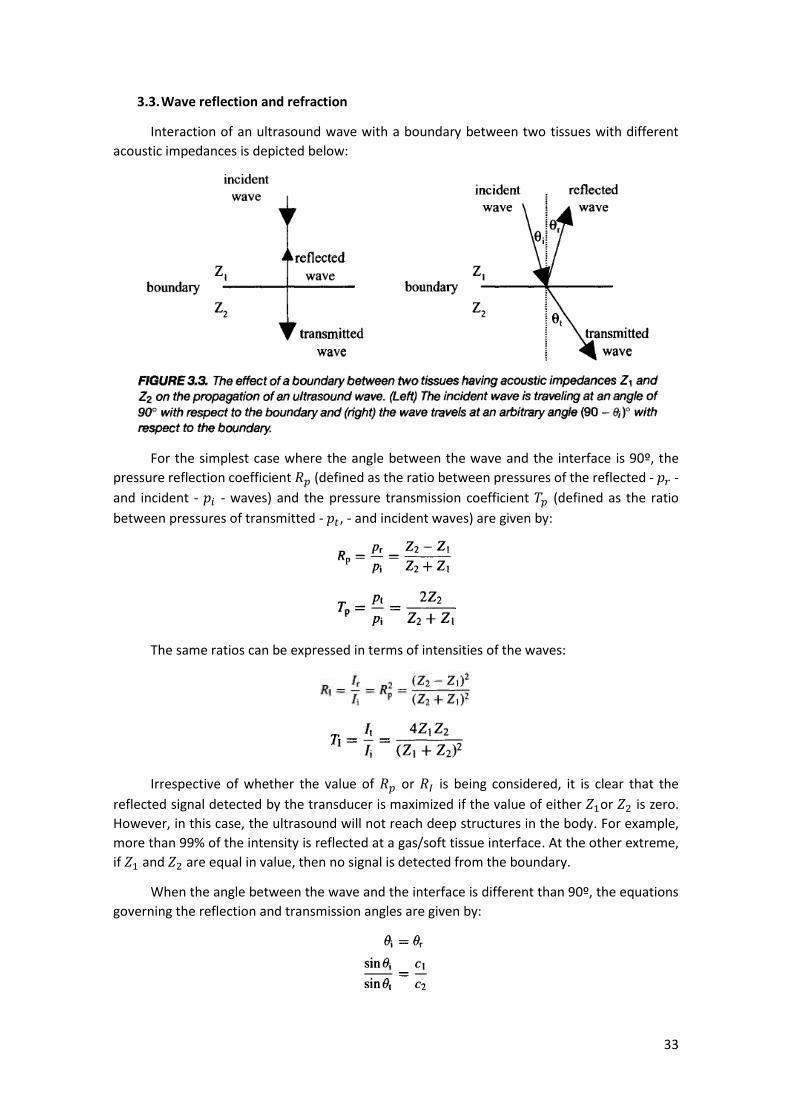
3.3. Wave reflection and refraction
Interaction of an ultrasound wave with a boundary between two tissues with different
acoustic impedances is depicted below:
For the simplest case where the angle between the wave and the interface is 90º, the
pressure reflection coefficient 𝑅𝑝 (defined as the ratio between pressures of the reflected - 𝑝𝑟 -
and incident - 𝑝𝑖 - waves) and the pressure transmission coefficient 𝑇𝑝 (defined as the ratio
between pressures of transmitted - 𝑝𝑡, - and incident waves) are given by:
The same ratios can be expressed in terms of intensities of the waves:
Irrespective of whether the value of 𝑅𝑝 or 𝑅𝐼 is being considered, it is clear that the
reflected signal detected by the transducer is maximized if the value of either 𝑍1or 𝑍2 is zero.
However, in this case, the ultrasound will not reach deep structures in the body. For example,
more than 99% of the intensity is reflected at a gas/soft tissue interface. At the other extreme,
if 𝑍1 and 𝑍2 are equal in value, then no signal is detected from the boundary.
When the angle between the wave and the interface is different than 90º, the equations
governing the reflection and transmission angles are given by:

34
If 𝑐1 ≠ 𝑐2, then the transmitted signal is refracted, which leads to misregistration artifacts.
The pressure and intensity coefficients are given by:
3.4. Energy loss mechanism in tissue
In addition to reflection, ultrasound waves can be attenuated by absorption and
scattering.
3.4.1. Absorption
Absorption refers to the conversion of mechanical energy into heat, which can occur
either by:
- Classical absorption: due to friction between particles as they are displaced by the
passage of the ultrasound wave. Proportional to the square of the wave frequency.
- Relaxation: due to the time 𝜏 taken for a molecule to return to its original position. If
the relaxation time of the tissue is of the same order of the wave period, then the
relaxation mechanism can act against the compression/rarefaction cycle, which leads to
loss of energy.
3.4.2. Scattering
Scattering occurs when the beam encounters tissue irregularities or particles that are the
same size or smaller than the ultrasound wavelength. If the size of the scattering body is small
compared to the wavelength, then scattering is relatively uniform in direction with slightly more
energy being scattered towards the transducer (Rayleigh scattering). It is characterized in terms
of scattering cross section 𝜎𝑠, which depends on the fourth power of wave frequency.
3.4.3. Attenuation
Attenuation is the sum of the scattering and absorption processes. It is characterized by
an exponential decrease in both pressure and intensity of the ultrasound as a function of
propagation distance z:
35
Where the intensity attenuation coefficient 𝜇 and the pressure attenuation coefficient 𝛼
depend linearly on the wave frequency.
3.5. Instrumentation
The instrumentation for ultrasounds consists of:
- Transducer (single-crystal or, more commonly, an array of crystals): converts oscillating
voltage into mechanical vibrations and vice-versa
- Detection electronics: modules for time-gain compensation and beam forming;
- Computer: data processing, image display and data storage
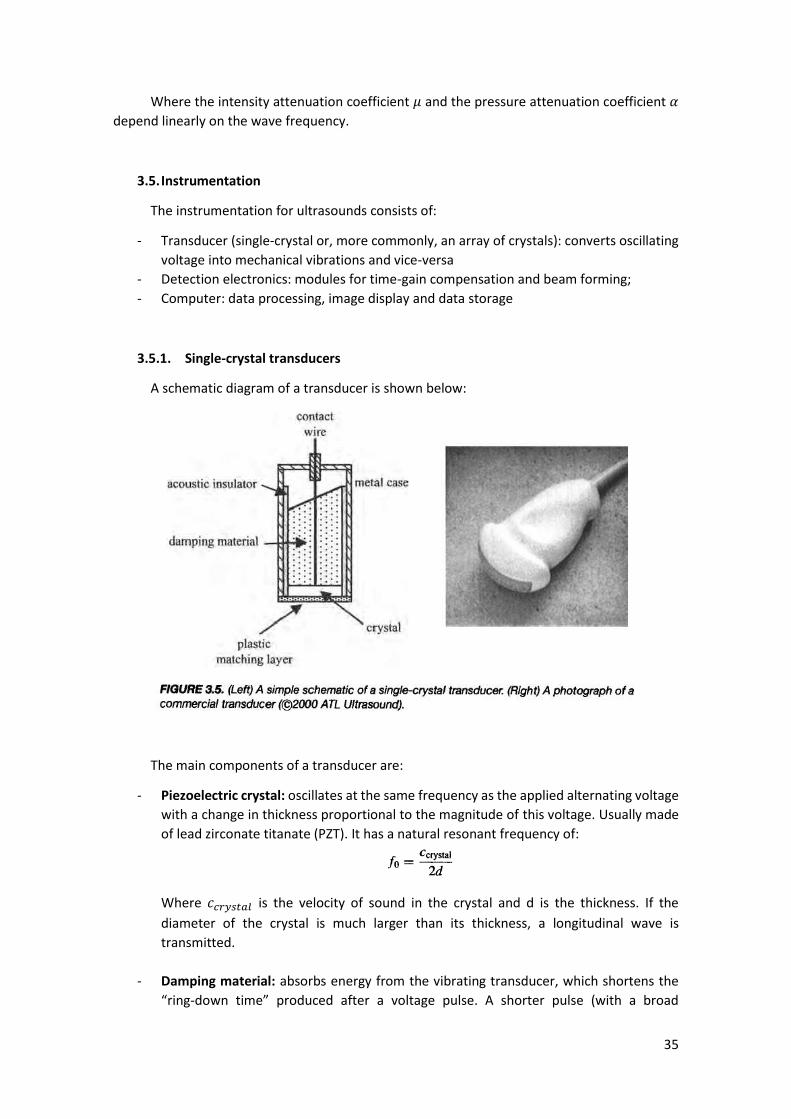
3.5.1. Single-crystal transducers
A schematic diagram of a transducer is shown below:
The main components of a transducer are:
- Piezoelectric crystal: oscillates at the same frequency as the applied alternating voltage
with a change in thickness proportional to the magnitude of this voltage. Usually made
of lead zirconate titanate (PZT). It has a natural resonant frequency of:
Where 𝑐𝑐𝑟𝑦𝑠𝑡𝑎𝑙 is the velocity of sound in the crystal and d is the thickness. If the
diameter of the crystal is much larger than its thickness, a longitudinal wave is
transmitted.
- Damping material: absorbs energy from the vibrating transducer, which shortens the
“ring-down time” produced after a voltage pulse. A shorter pulse (with a broad

36
bandwidth – BW – in the frequency domain) gives a better spatial resolution. It is often
specified the quality factor Q which, in a well damped material, is between 1 and 2.
Since the acoustic impedance of PZT is about 15 times that of skin, there is a huge amount
of energy reflected. Thus, a layer of material with an acoustic impedance 𝑍𝑀𝐿 is placed to
maximize energy transmission:
3.5.1.1. The beam geometry of a single transducer
Considering a plane-piston (flat face) transducer, made up of a large number of point
sources, the total pressure wave emitted is the superposition of the spherical waves emitted by
these point sources:

37
The near-field boundary (NFB) corresponds to the last maximum and separates the near-
field (where the wavefront if not well defined), or Fresnel zone, from the far-field, or Fraunhofer
zone (where the wavefront is well approximated as planar):
Where a is the diameter of the transducer and 𝜆 is the wavelength of the ultrasound.
Beyond this point, the beam diverges and its intensity decreases smoothly. In addition to
the main beam, side lobes may be present due to the transducer acting as a diffraction grating,
which is undesirable since they remove energy from the main beam and can introduce artifacts.
The greater the ratio wavelength/transducer diameter, the fewer the number of side lobes but
the closer the NFB lies to the face of the transducer.
3.5.1.2. Lateral resolution and depth of focus
In the far-field region, the lateral beamwidth can be well approximated by a Gaussian
function, which has a FWHM:
Where 𝜎 is the standard deviation.
Since the diameter of the single-crystal is typically between 1 and 5 cm, the lateral
resolution is usually very poor and a concave lens is used to focus the beam. Lowering the lens
curvature (R) lowers the focal distance F (distance from the face of the transducer at which the
lateral beam width is narrowest). The plane perpendicular to the beam axis at F distance is called
focal plane.

38
For a spherical focusing lens, the FWHM at the focal point is given by
Therefore, decreasing the lens curvature (R) and increasing the diameter of the crystal (a)
improves lateral resolution. The wavelength (𝜆) dependence arises from the appearance of side
lobes as discussed previously.
However, there is a tradeoff: the better the lateral resolution (small FWHM), the lower
the depth of focus as the beam diverges much more at locations away from the focal plane.
3.5.1.3. Axial resolution
Axial resolution is defined as the closest separation, in the direction of the propagating
wave, of two scatterers that result in two backscattered signals. This distance can be expressed
as:
Where PD is the pulse duration. Therefore, axial resolution can be improved by reducing
PD (either by using a higher frequency ultrasound – which also increases attenuation – or
improving the transducer damping).

39
3.5.2. Transducer arrays
There are several problems regarding single crystal transducers:
- Require manual or mechanical steering of the beam;
- Tradeoff between lateral resolution and DOF
- Large distance between the face of the transducer and the NFB
One way of avoiding these problems is to use an array of small piezoelectric crystals. There are
three types of arrays:
3.5.2.1. Linear sequential arrays
A linear sequential array consist of a large number (64-512) of rectangular piezoelectric
crystals, each having a width of the order of the ultrasound wavelength. The width of the
ultrasound is determined by the number of elements that are excited simultaneously. A planar
wavefront is produced by exciting a number of elements (3 for example), which corresponds to
the first line. The process is repeated for the adjacent set (2nd, 3rd and 4th elements), displacing
laterally the focus point, and so on. Additional lines can be acquired by performing again the
same process but with an even number of elements (4 for example).
It is particularly used when a large FOV is required close to the surface of the array.
3.5.2.2. Linear phased arrays
The layout of a linear phased array is very similar to that of a linear sequential array, but
operates in a different way. A much larger number of elements is excited for each line with the
voltage pulses exciting each one being delayed in time in order to produce a curved wavefront
similar to that produced by a focused single crystal transducer. The elements are smaller than
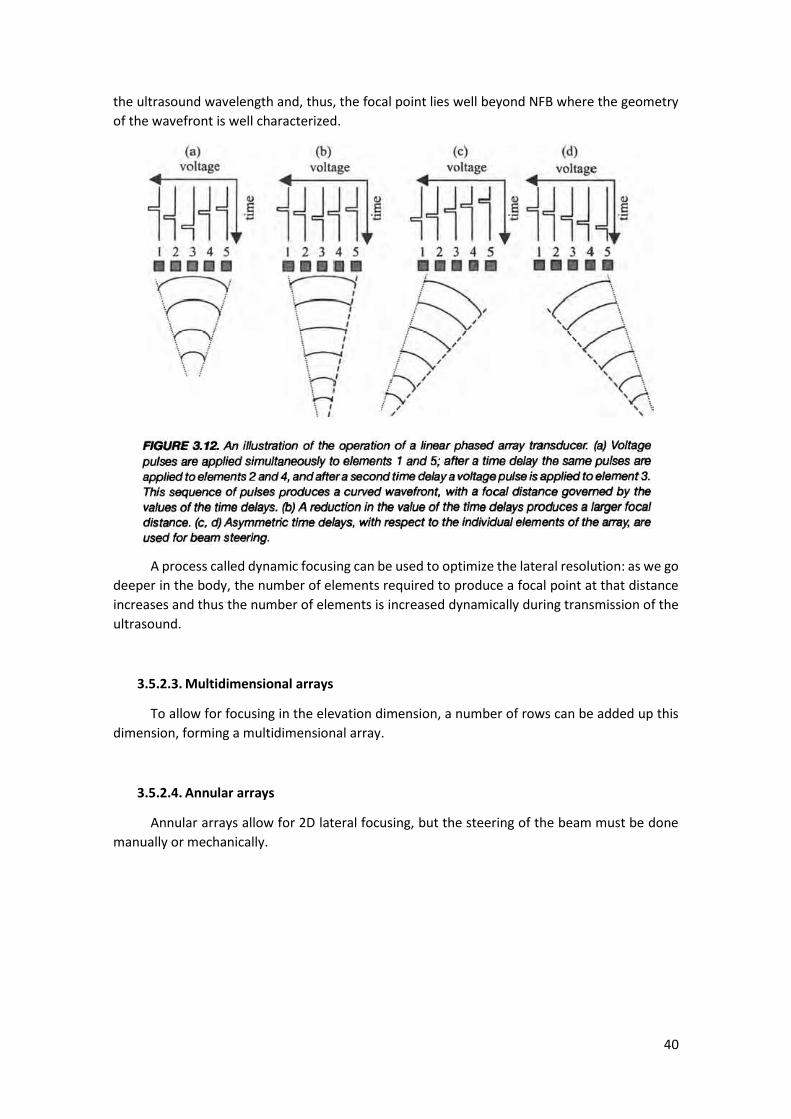
40
the ultrasound wavelength and, thus, the focal point lies well beyond NFB where the geometry
of the wavefront is well characterized.
A process called dynamic focusing can be used to optimize the lateral resolution: as we go
deeper in the body, the number of elements required to produce a focal point at that distance
increases and thus the number of elements is increased dynamically during transmission of the
ultrasound.
3.5.2.3. Multidimensional arrays
To allow for focusing in the elevation dimension, a number of rows can be added up this
dimension, forming a multidimensional array.
3.5.2.4. Annular arrays
Annular arrays allow for 2D lateral focusing, but the steering of the beam must be done
manually or mechanically.

41
3.5.3. Beam forming and time-gain compensation
Time-gate compensation (TGC): signal amplification is dependent on the time that the
signal takes to reach the transducer. Signals arising from structures close to the transducer
(faster to arrive) are amplified by a smaller factor than those from greater depths (which
suffered more attenuation). Various linear or nonlinear functions can be used and adjusted
online by the operator.
3.6. Diagnostic scanning modes
There are three basic modes of diagnostic anatomical imaging: A-mode, M-mode and B-
mode. Recent technical advances include the use of compound and 3D imaging.
3.6.1. A-mode, M-mode and B-mode scans
Amplitude (A)-mode: refers to the acquisition of a 1D scan, that is, a plot of the amplitude
of the backscattered echo versus the time after transmission of the ultrasound pulse. Used for
measuring distances for example in ophthalmology (assuming constant velocity of the sound).
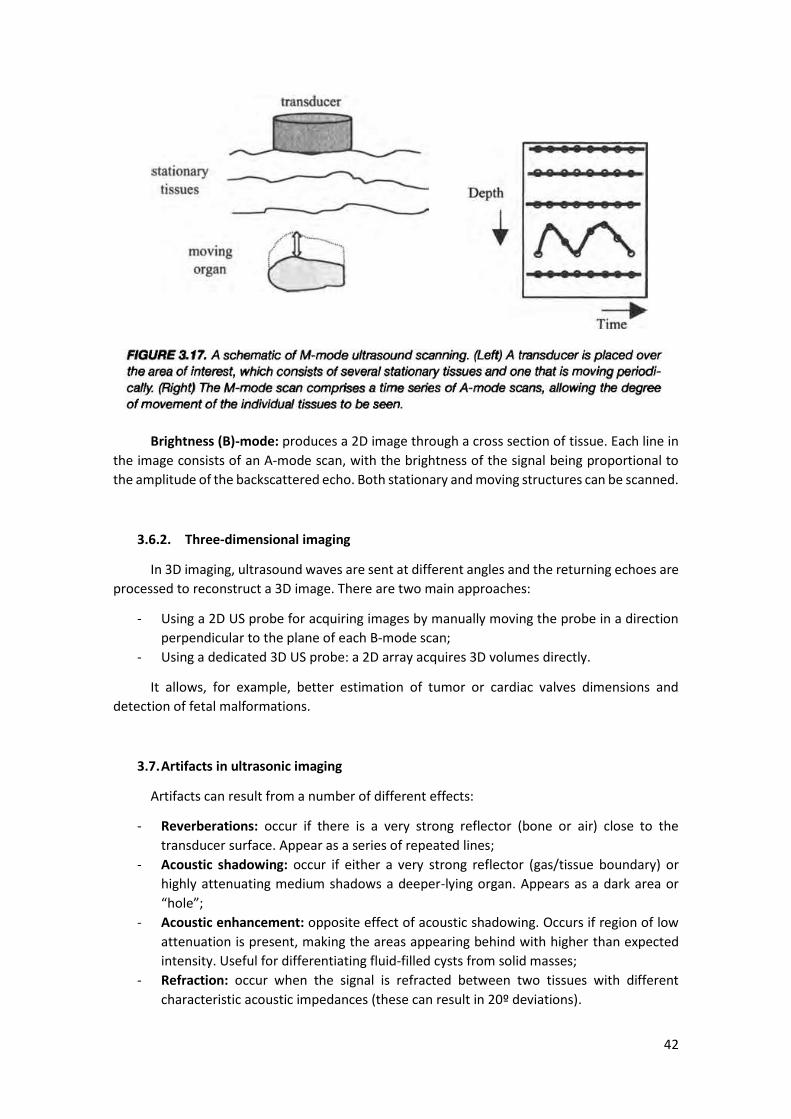
Motion (M)-mode: consists of a series of A-mode scans to detect motion of a moving
structure. The brightness of the displayed signal is proportional to the amplitude of the
backscattered echo.
42
Brightness (B)-mode: produces a 2D image through a cross section of tissue. Each line in
the image consists of an A-mode scan, with the brightness of the signal being proportional to
the amplitude of the backscattered echo. Both stationary and moving structures can be scanned.
3.6.2. Three-dimensional imaging
In 3D imaging, ultrasound waves are sent at different angles and the returning echoes are
processed to reconstruct a 3D image. There are two main approaches:
- Using a 2D US probe for acquiring images by manually moving the probe in a direction
perpendicular to the plane of each B-mode scan;
- Using a dedicated 3D US probe: a 2D array acquires 3D volumes directly.
It allows, for example, better estimation of tumor or cardiac valves dimensions and
detection of fetal malformations.
3.7. Artifacts in ultrasonic imaging
Artifacts can result from a number of different effects:
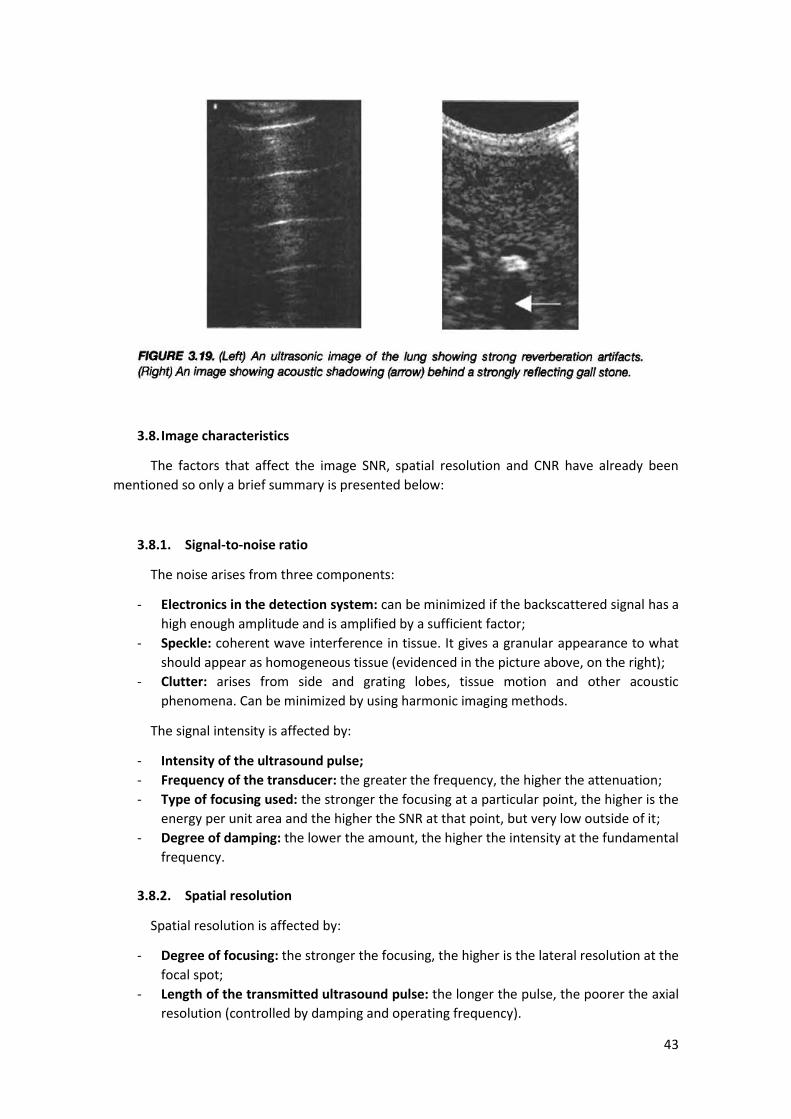
- Reverberations: occur if there is a very strong reflector (bone or air) close to the
transducer surface. Appear as a series of repeated lines;
- Acoustic shadowing: occur if either a very strong reflector (gas/tissue boundary) or
highly attenuating medium shadows a deeper-lying organ. Appears as a dark area or
“hole”;
- Acoustic enhancement: opposite effect of acoustic shadowing. Occurs if region of low
attenuation is present, making the areas appearing behind with higher than expected
intensity. Useful for differentiating fluid-filled cysts from solid masses;
- Refraction: occur when the signal is refracted between two tissues with different
characteristic acoustic impedances (these can result in 20º deviations).
43
3.8. Image characteristics
The factors that affect the image SNR, spatial resolution and CNR have already been
mentioned so only a brief summary is presented below:
3.8.1. Signal-to-noise ratio
The noise arises from three components:
- Electronics in the detection system: can be minimized if the backscattered signal has a
high enough amplitude and is amplified by a sufficient factor;
- Speckle: coherent wave interference in tissue. It gives a granular appearance to what
should appear as homogeneous tissue (evidenced in the picture above, on the right);
- Clutter: arises from side and grating lobes, tissue motion and other acoustic
phenomena. Can be minimized by using harmonic imaging methods.
The signal intensity is affected by:
- Intensity of the ultrasound pulse;
- Frequency of the transducer: the greater the frequency, the higher the attenuation;
- Type of focusing used: the stronger the focusing at a particular point, the higher is the
energy per unit area and the higher the SNR at that point, but very low outside of it;
- Degree of damping: the lower the amount, the higher the intensity at the fundamental
frequency.
3.8.2. Spatial resolution
Spatial resolution is affected by:
- Degree of focusing: the stronger the focusing, the higher is the lateral resolution at the
focal spot;
- Length of the transmitted ultrasound pulse: the longer the pulse, the poorer the axial
resolution (controlled by damping and operating frequency).
44
3.8.3. Contrast-to-noise ratio
Affected by the same factors as SNR. It can be greatly improved by using contrast agents
and pulse inversion techniques, discussed in the next sections.
3.9. Compound Imaging
Also called sonoCT, it consists in acquiring multiple coplanar B-mode scans and combining
them into a single image. Although it presents blurring due to movement across multiple
acquisitions, it has the following advantages:
- Improved SNR (especially in the center, where the lines overlap)
- Reduced speckle and clutter
- Reduced acoustic shadowing
3.10. Blood velocity measurements using ultrasound
Two techniques are used to estimate blood velocity:
- Doppler shift based techniques (used in either continuous – CW – , pulsed or duplex
modes);
- Time-domain signal correlation techniques.
3.10.1. The Doppler Effect
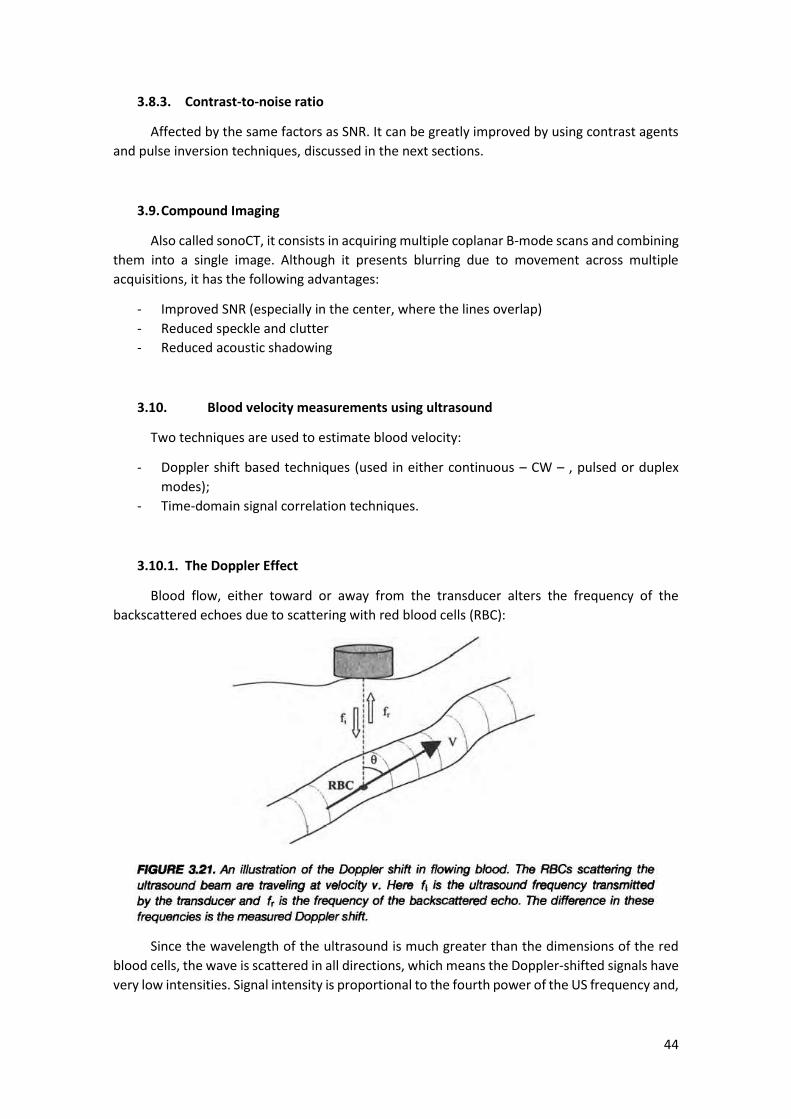
Blood flow, either toward or away from the transducer alters the frequency of the
backscattered echoes due to scattering with red blood cells (RBC):
Since the wavelength of the ultrasound is much greater than the dimensions of the red
blood cells, the wave is scattered in all directions, which means the Doppler-shifted signals have
very low intensities. Signal intensity is proportional to the fourth power of the US frequency and,
45
thus, higher operating frequencies are used (however, maximum measuring depth decreases
with higher frequencies because of the beam attenuation).
The overall Doppler shift ∆𝑓 is given by:
3.10.2. Continuous wave Doppler measurements
CW Doppler uses a continuous pulse transmitted by one transducer and the backscattered
signal is detected by the second one, with the region of overlap of the sensitive regions of the
transducers defining the area in which blood flow is detected (it is often large and the existence
of more than one blood vessel can lead to misinterpretations). It is used when there is no need
to localize exactly the source of Doppler shifts. Its advantages are:
- No maximum depth limitation;
- No maximum measurable velocity limitation.
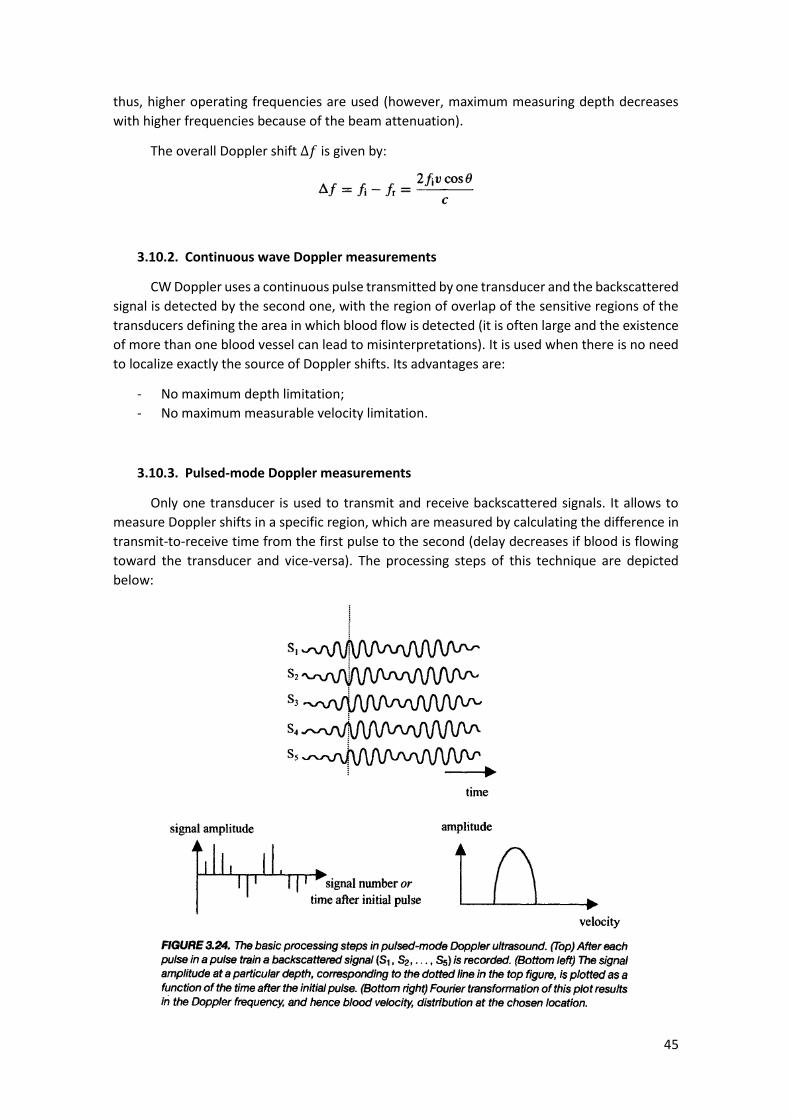
3.10.3. Pulsed-mode Doppler measurements
Only one transducer is used to transmit and receive backscattered signals. It allows to
measure Doppler shifts in a specific region, which are measured by calculating the difference in
transmit-to-receive time from the first pulse to the second (delay decreases if blood is flowing
toward the transducer and vice-versa). The processing steps of this technique are depicted
below:

46
Contrary to CW Doppler, there is a limit to the highest velocity 𝑣𝑚𝑎𝑥which can be
measured imposed by the Nyquist theorem (sampling frequency – in this case, the pulse
repetition rate PRR – must be at least twice the measured frequency). It is given by:
It is also limited to a maximum depth 𝑑𝑚𝑎𝑥:
𝑑𝑚𝑎𝑥 =𝑐
2𝑃𝑅𝑅
3.10.4. Color Doppler/B-mode Duplex Imaging
Duplex imaging consists in interlacing Doppler flow measurements with B-mode imaging
in order to impose the flow maps onto high-resolution anatomical images. Only the mean value
of the velocity and not the full velocity distribution is determined. The mean velocity, its sign
and its variance are represented by the hue, saturation and luminance respectively (red and blue
represents flow towards and away from the transducer, respectively).
When a vessel lies parallel to the face of the transducer array, directly below the center
of the transducer array there is a signal void, which can be solved by using power Doppler mode.
It consists in integrating the area under the frequency vs amplitude plot, allowing to:
- Remove angle dependence (power depends only on the number of RBC scatters);
- Reduce aliasing artifacts at high flow rates.
The main disadvantage of Doppler power is the loss of directional information.
3.11. Ultrasound contrast agents, harmonic imaging and pulse inversion techniques
Contrast agents are used to increase the intensity of backscattered signals and consist of
gas-filled microspheres or microbubbles injected into the bloodstream. They act by two
mechanisms:
- Large increase of the difference in acoustic properties (higher compressibility and lower
density) between gas-filled particles and the surroundings;
- Resonance: gas-filled microspheres expand and contract when the US travels through
them, acting as harmonic oscillators.
These mechanisms results in a much larger effective scattering cross section.
Harmonic Imaging: the backscattered signal consists of a fundamental frequency and its
harmonics. Although these harmonics have lower intensities, they can have higher SNR because
of the very low contributions from clutter and tissue motion. The most common implementation
uses the second harmonic using a pulse inversion technique, which combines two scans. In the
first scan, both the returning fundamental and its harmonic are stored. In the second scan, the
fundamental signal is inverted, but the harmonic has the same phase. Summation of both scans
thus results in the elimination of the fundamental component.

47
4. Magnetic Resonance Imaging
4.1. General principles of Magnetic Resonance Imaging
Magnetic Resonance Imaging (MRI) – nonionizing technique with full 3D capabilities,
excellent soft-tissue contrast and high spatial resolution (~1mm), although expensive and
subject to patient motion due to high scanning times (typically 3-10 mins).
Brief description of the technique – MRI signal arises from protons in the body (mainly
water), which act as small magnets. After the patient is placed inside the scanner, a strong
magnet causes the protons to precess either in a parallel or antiparallel configuration regarding
the direction of the static magnetic field. The frequency of precession is proportional to the
strength of the field. Application of a weak radiofrequency (RF) field causes protons to precess
coherently and the sum of their number is detected as an induced voltage in a tuned detector
coil. Spatial information is encoded into the image using magnetic field gradients (one in each
direction). These gradients cause variations in the magnetic field, which, in turn, causes the
precessional frequencies to vary depending on their spatial location. Frequency and phase is
measured by the RF coil and the signal is then digitized. Finally, an inverse 2D Fourier transform
is performed to convert the signal into the spatial domain.
4.2. Nuclear magnetism
MRI arises from the interaction between the magnetic field and the hydrogen nuclei,
which can be described from a quantum mechanical or classical approach.
4.2.1. Quantum mechanical description
The spin of a proton can be viewed as a rotation around an internal axis, giving the proton
a certain angular momentum P. Since a proton is a charged particle, it gives the proton a
magnetic moment 𝜇, which, in turn, produces a magnetic field. In the absence of an external
magnetic field, the orientation of the individual magnetic moments is random.

48
The magnitude of P is quantized:
For protons, the spin quantum number l is equal to ½, and thus:
The magnetic momentum 𝜇 is related with P by the gyromagnetic ratio 𝛾:
In the presence of a strong magnetic field 𝐵0, the z component (along 𝐵0) of 𝜇 can only
have the values given by:
The nuclear magnetic quantum number 𝑚𝑙 takes values l, l-1,…,-l so, in the case of a
proton, 𝑚𝑙 takes +1/2 and -1/2, yielding:
𝜇𝑧 = ±𝛾ℎ/4𝜋
The magnetic field only interacts with the z component, thus:
The two possible interaction energies correspond to the parallel (negative E) and
antiparallel (positive E) configurations. The energy difference between the 2 levels is given by:
Using the Boltzmann distribution, we find the relative number of nuclei in each
configuration:
The magnitude of the MRI signal is proportional to the difference in populations between
the 2 energy levels:
Where 𝑁𝑠is the total number of protons in the body.
49
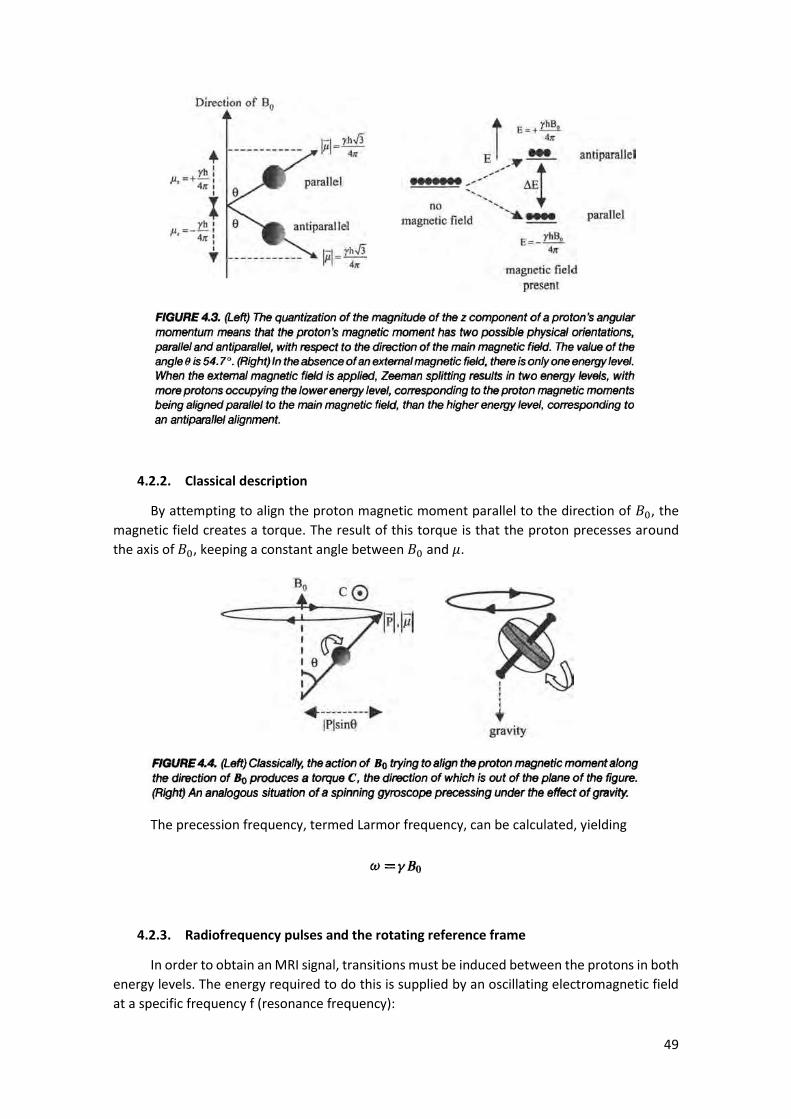
4.2.2. Classical description
By attempting to align the proton magnetic moment parallel to the direction of 𝐵0, the
magnetic field creates a torque. The result of this torque is that the proton precesses around
the axis of 𝐵0, keeping a constant angle between 𝐵0 and 𝜇.
The precession frequency, termed Larmor frequency, can be calculated, yielding
4.2.3. Radiofrequency pulses and the rotating reference frame
In order to obtain an MRI signal, transitions must be induced between the protons in both
energy levels. The energy required to do this is supplied by an oscillating electromagnetic field
at a specific frequency f (resonance frequency):

50
If we refer to the expression in the previous section, we notice that this resonance
frequency is the Larmor frequency.
The electromagnetic energy is provided as a single or series of radiofrequency (RF) pulses.
To analyse the effect of a given sequence of pulses, we will consider the net effect of all of the
protons in the body, thus we define the net magnetization as:
Since the distribution of magnetic momenta in the transverse plane is random, the net
magnetization in x and y directions is zero:
As we will see, a detectable signal can only be produced by 𝑀𝑥 and 𝑀𝑦, so it is necessary
to rotate the net magnetization from z to xy plane by applying a second magnetic field 𝐵1 aligned
along x at the Larmor frequency (much slower than the frequency of 𝐵0). The nuclei are now
said to be phase coherent as all the vectors are pointing in the same direction. The tip angle 𝛼
is defined as the angle through which the net magnetization is rotated. It depends on the
strength and time during which the RF is applied:
To simplify the visualization, we will use a rotating reference frame in which xy plane
rotates around z at the Larmor frequency:
The signal is detected by an RF coil in the form of a voltage E across the ends of the coil
loop, created by the change of the magnetic flux (Faraday’s law):
51
This is the reason why only the xy plane gives rise to a nuclear magnetic resonance (there
is no time change in z). The higher 𝐵0, the higher is the signal detected.
4.2.4. Spin-Lattice and Spin-Spin Relaxation
After the application of an RF pulse, the magnetization components must return to their
equilibrium value over time. The time evolution of each component is given by the Bloch
equations.
The return of 𝑀𝑧 to its equilibrium value 𝑀0 is governed by the spin-lattice relaxation time
𝑇1 (arises from the loss of proton energy to the surrounding lattice) and it is given by the
expression:
Different tissues have different values of 𝑇1, therefore 𝑇1 is one source of contrast in MRI
imaging.
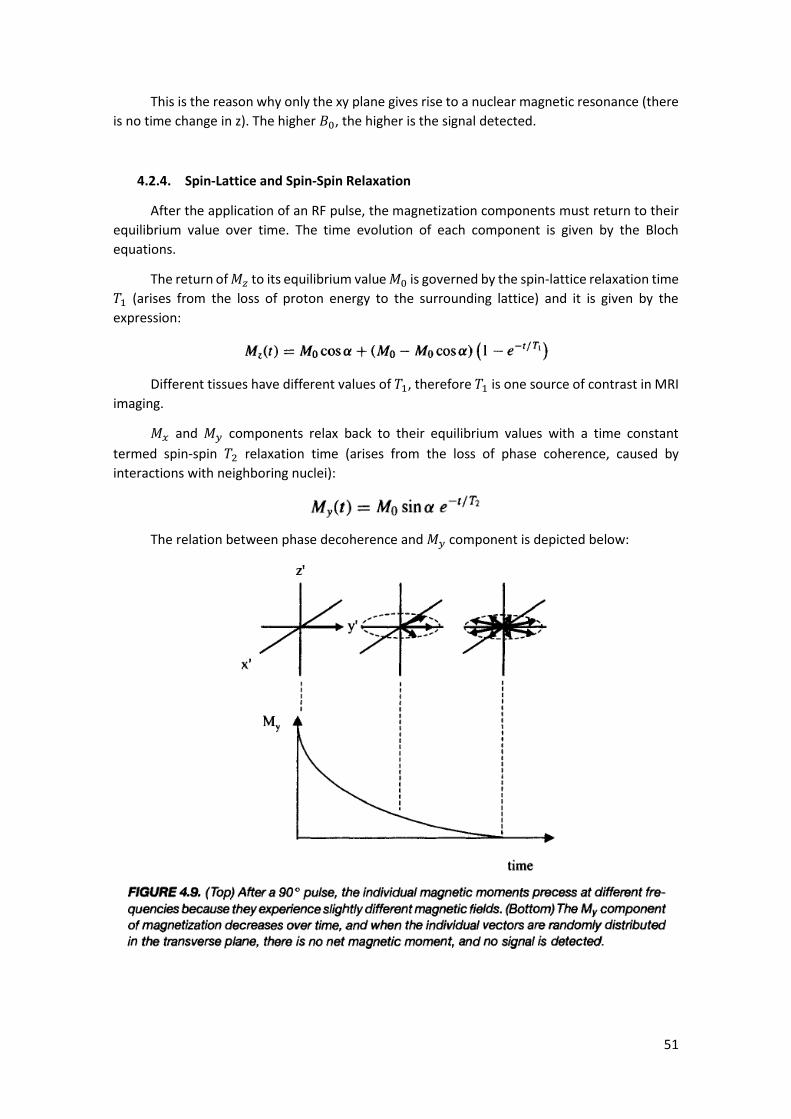
𝑀𝑥 and 𝑀𝑦 components relax back to their equilibrium values with a time constant
termed spin-spin 𝑇2 relaxation time (arises from the loss of phase coherence, caused by
interactions with neighboring nuclei):
The relation between phase decoherence and 𝑀𝑦 component is depicted below:

52
Aside from the nuclei-nuclei interaction, phase decoherence is also affected by spatial
variations of the magnetic field (due to non-uniformities in the magnet design or different
magnetic susceptibilities of different tissues). The overall relaxation of transverse magnetization
is given by 𝑇2∗, a combination of both effects:
Different tissues have different 𝑇2 and, thus, 𝑇2is used as a contrast source as well.
4.2.5. Measurements of 𝑻𝟏 and 𝑻𝟐: inversion recovery and spin-echo sequences
The value of 𝑇1 is measured using an inversion recovery sequence, which consists of a
180º pulse, a variable delay 𝜏 and a 90º pulse, followed immediately by data acquisition. This
sequence is repeated n times, each with a different 𝜏. The detected signal is given by:
A plot of ln (𝑆(𝜏𝑛)) versus 𝜏𝑛 gives a straight line with a slope of −𝑇1.
The measurement of 𝑇2 involves a spin-echo setup, where a 90º is applied, followed by a
variable delay 𝜏, a 180º pulse (in the xy plane), an identical 𝜏 and then the signal acquisition. To
see how the spin-echo sequence works, consider a single proton which, due to spatial
inhomogeneities in the magnetic field, resonates at a frequency Δ𝜔, less than the nominal
Larmor frequency. At 𝜏 after the 90º pulse, the precessing magnetization has accumulated a
phase 𝜙 = Δωτ. By applying the 180º pulse, we convert 𝑀𝑦to −𝑀𝑦 and +𝜙 to −𝜙. During the
second 𝜏 interval, the precessing magnetization accumulates a further phase +𝜙. Thus, at 2𝜏,
the precessing magnetization has 0 phase, which eliminates the 𝑇2+ contribution, yielding 𝑇2
∗ =
𝑇2:
53
A plot of ln (𝑆(𝜏𝑛)) versus 2𝜏𝑛 gives a straight line with a slope of −1/𝑇2.
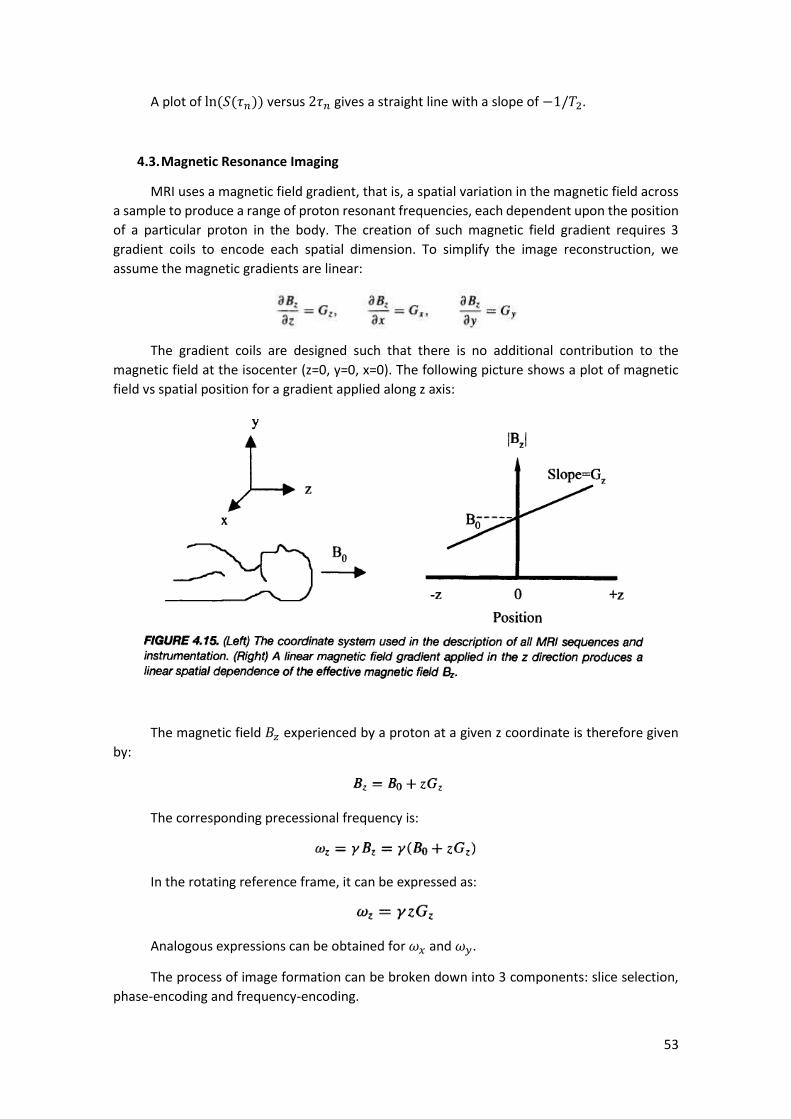
4.3. Magnetic Resonance Imaging
MRI uses a magnetic field gradient, that is, a spatial variation in the magnetic field across
a sample to produce a range of proton resonant frequencies, each dependent upon the position
of a particular proton in the body. The creation of such magnetic field gradient requires 3
gradient coils to encode each spatial dimension. To simplify the image reconstruction, we
assume the magnetic gradients are linear:
The gradient coils are designed such that there is no additional contribution to the
magnetic field at the isocenter (z=0, y=0, x=0). The following picture shows a plot of magnetic
field vs spatial position for a gradient applied along z axis:
The magnetic field 𝐵𝑧 experienced by a proton at a given z coordinate is therefore given
by:
The corresponding precessional frequency is:
In the rotating reference frame, it can be expressed as:
Analogous expressions can be obtained for 𝜔𝑥 and 𝜔𝑦.
The process of image formation can be broken down into 3 components: slice selection,
phase-encoding and frequency-encoding.
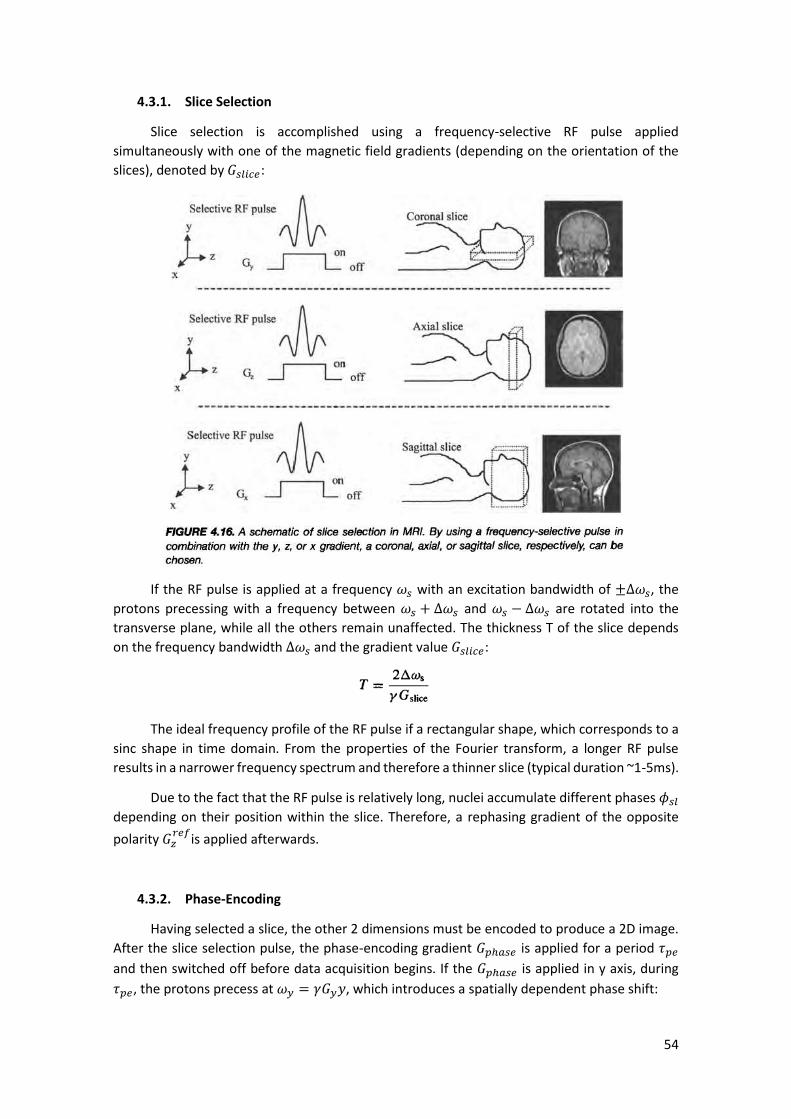
54
4.3.1. Slice Selection
Slice selection is accomplished using a frequency-selective RF pulse applied
simultaneously with one of the magnetic field gradients (depending on the orientation of the
slices), denoted by 𝐺𝑠𝑙𝑖𝑐𝑒:
If the RF pulse is applied at a frequency 𝜔𝑠 with an excitation bandwidth of ±Δ𝜔𝑠, the
protons precessing with a frequency between 𝜔𝑠 + Δ𝜔𝑠 and 𝜔𝑠 − Δ𝜔𝑠 are rotated into the
transverse plane, while all the others remain unaffected. The thickness T of the slice depends
on the frequency bandwidth ∆𝜔𝑠 and the gradient value 𝐺𝑠𝑙𝑖𝑐𝑒:
The ideal frequency profile of the RF pulse if a rectangular shape, which corresponds to a
sinc shape in time domain. From the properties of the Fourier transform, a longer RF pulse
results in a narrower frequency spectrum and therefore a thinner slice (typical duration ~1-5ms).
Due to the fact that the RF pulse is relatively long, nuclei accumulate different phases 𝜙𝑠𝑙
depending on their position within the slice. Therefore, a rephasing gradient of the opposite
polarity 𝐺𝑧𝑟𝑒𝑓
is applied afterwards.
4.3.2. Phase-Encoding
Having selected a slice, the other 2 dimensions must be encoded to produce a 2D image.
After the slice selection pulse, the phase-encoding gradient 𝐺𝑝ℎ𝑎𝑠𝑒 is applied for a period 𝜏𝑝𝑒
and then switched off before data acquisition begins. If the 𝐺𝑝ℎ𝑎𝑠𝑒 is applied in y axis, during
𝜏𝑝𝑒, the protons precess at 𝜔𝑦 = 𝛾𝐺𝑦𝑦, which introduces a spatially dependent phase shift:

55
4.3.3. Frequency-Encoding
The frequency-encoding is encoded by the nuclei precessing at different frequencies
under the influence of a gradient 𝐺𝑓𝑟𝑒𝑞 , which is applied during data acquisition. The time
between successive acquisitions is referred to as dwell time 𝑡𝑑𝑤, being the reciprocal of the
acquisition bandwidth.
A graphical representation of the slice, frequency and phase encoding processes is
depicted below:
4.3.4. The k-Space formalism
To understand how the acquired 𝑁𝑟 × 𝑁𝑝 data matrix is transformed into the final image,
we will look into the k-space formalism. First, we define two variables:
With x and y being the frequency and phase encoding directions respectively. The signal
can then be expressed as:
The 𝑁𝑟 × 𝑁𝑝 acquisition points can be visualized as a 2D data set in k-space. Consider the
𝑁𝑟 points collected when the minimum value of the phase encoding 𝐺𝑦 is applied. Referring to

56
the 𝑘𝑦 expression, all these 𝑁𝑟 have the minimum 𝑘𝑦 value. When the frequency-encoding
gradient is turned on, the first data point collected corresponds to a small positive value of 𝑘𝑥,
the second data point to a slightly more positive value of 𝑘𝑥 and so forth, and so these 𝑁𝑟 points
correspond to the first (bottom) line in k-space. The second line corresponds to the next value
of the phase encoding gradient and so on. The spacing between k-space points is dictated by the
required FOV of the image:
A 2D inverse Fourier transform of the k-space data 𝑆(𝑘𝑥 , 𝑘𝑦) gives an estimation of
𝜌(𝑥, 𝑦), that is, an image corresponding to the spatial variation in proton density. In the previous
example only the positive half of the 𝑘𝑥 was acquired. In full k-space coverage, the SNR and
spatial resolution (determined by the maximum values of 𝑘𝑥 and 𝑘𝑦) would be increased. This
can be achieved by a gradient-echo imaging sequence, which adds a negative gradient 𝐺𝑑𝑒𝑝ℎ𝑎𝑠𝑒
before data acquisition.
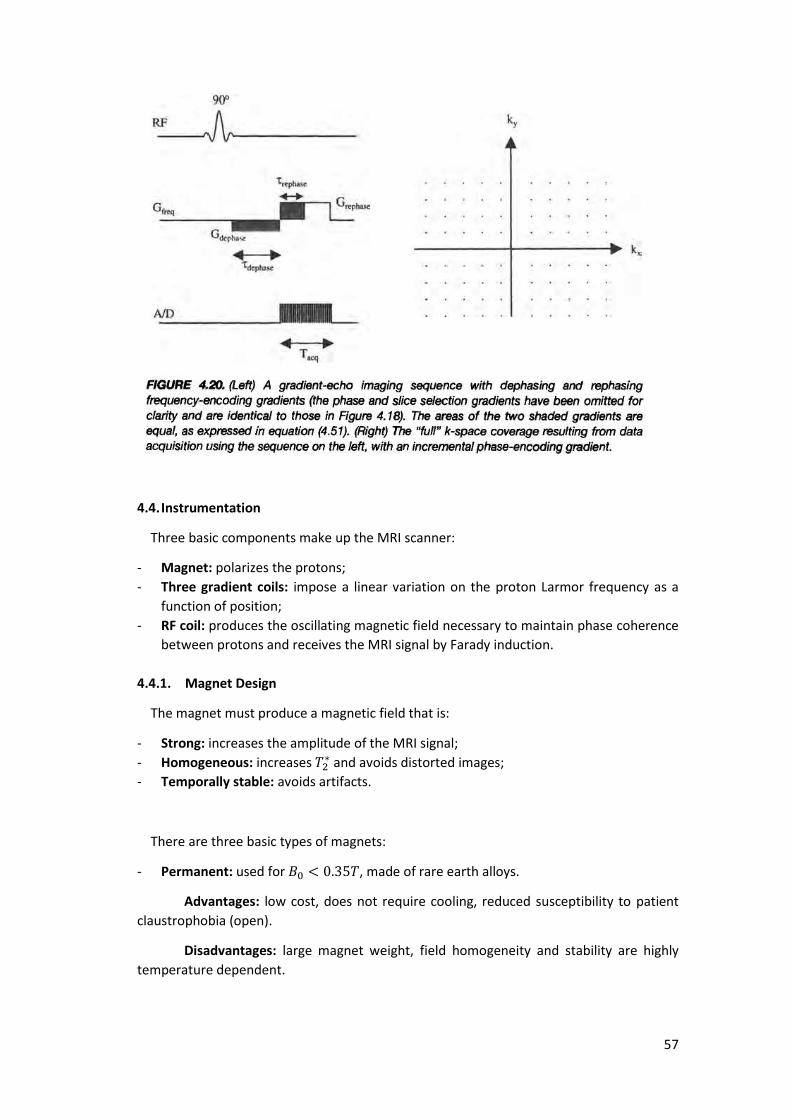
57
4.4. Instrumentation
Three basic components make up the MRI scanner:
- Magnet: polarizes the protons;
- Three gradient coils: impose a linear variation on the proton Larmor frequency as a
function of position;
- RF coil: produces the oscillating magnetic field necessary to maintain phase coherence
between protons and receives the MRI signal by Farady induction.
4.4.1. Magnet Design
The magnet must produce a magnetic field that is:
- Strong: increases the amplitude of the MRI signal;
- Homogeneous: increases 𝑇2∗ and avoids distorted images;
- Temporally stable: avoids artifacts.
There are three basic types of magnets:
- Permanent: used for 𝐵0 < 0.35𝑇, made of rare earth alloys.
Advantages: low cost, does not require cooling, reduced susceptibility to patient
claustrophobia (open).
Disadvantages: large magnet weight, field homogeneity and stability are highly
temperature dependent.

58
- Resistive: used for 𝐵0 < 0.35𝑇, magnetic field strength is proportional to a constant
current passing through a conductor such as copper. Power dissipated as heat is
proportional to the resistance of the conductor and the square of the current.
Disadvantages: requires cooling, maximum magnetic field strength is limited by the
maximum current, homogeneity and stability highly dependent on temperature.
- Superconducting: used for 𝐵0 > 0.35𝑇 (typically 1.5T or 3T). It minimizes the problem
of cooling by using superconductors which have 0 resistance at very low temperatures
and allows stronger magnetic fields to be used. The superconductor is housed in a can
containing liquid helium at 4.2K, surrounded by radiation shields, vacuum vessels and a
liquid nitrogen chamber. Because heat losses are not avoidable, liquid nitrogen and
helium must be replenished on a regular basis. Additional correction and shim coils are
added to correct uniformity of the magnetic field.
4.4.2. Magnetic field gradient coils
Gradient coils have three basic requirements:
- Production of linear gradients over the imaged region: their geometry is optimized to
produce a linear gradient, rather than a uniform field. Since the value of the gradient is
relatively small, chilled water cooling is sufficient. The z coil consists of a “Maxwell pair”
(two separate loops, with current flowing in opposed directions). The x and y coils have
a “saddle coil” arrangement (four arcs each). The gradient strength is proportional to
the number of turns.
- Production of high gradient strengths per unit current: achieved by minimizing
resistance;
- Fast switching times: achieved by minimizing inductance; important to reduce the time
which must be allowed for gradients to stabilize in imaging techniques.
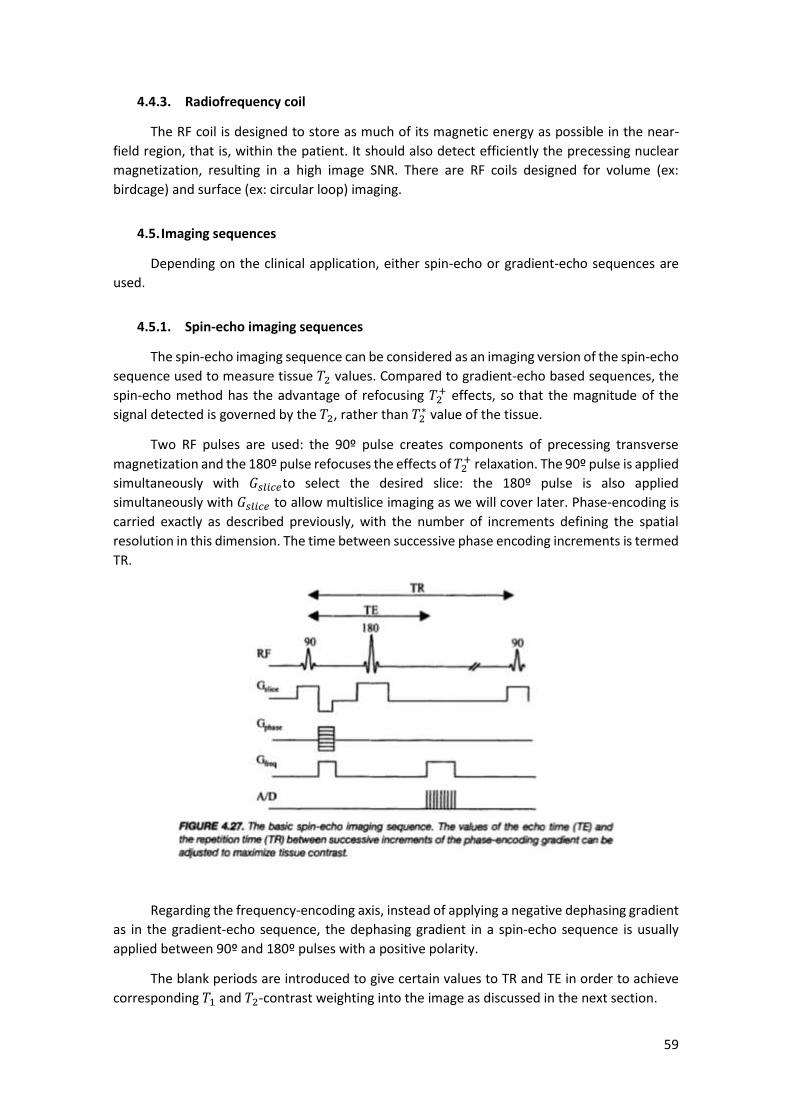
59
4.4.3. Radiofrequency coil
The RF coil is designed to store as much of its magnetic energy as possible in the near-
field region, that is, within the patient. It should also detect efficiently the precessing nuclear
magnetization, resulting in a high image SNR. There are RF coils designed for volume (ex:
birdcage) and surface (ex: circular loop) imaging.
4.5. Imaging sequences
Depending on the clinical application, either spin-echo or gradient-echo sequences are
used.
4.5.1. Spin-echo imaging sequences
The spin-echo imaging sequence can be considered as an imaging version of the spin-echo
sequence used to measure tissue 𝑇2 values. Compared to gradient-echo based sequences, the
spin-echo method has the advantage of refocusing 𝑇2+ effects, so that the magnitude of the
signal detected is governed by the 𝑇2, rather than 𝑇2∗ value of the tissue.
Two RF pulses are used: the 90º pulse creates components of precessing transverse
magnetization and the 180º pulse refocuses the effects of 𝑇2+ relaxation. The 90º pulse is applied
simultaneously with 𝐺𝑠𝑙𝑖𝑐𝑒to select the desired slice: the 180º pulse is also applied
simultaneously with 𝐺𝑠𝑙𝑖𝑐𝑒 to allow multislice imaging as we will cover later. Phase-encoding is
carried exactly as described previously, with the number of increments defining the spatial
resolution in this dimension. The time between successive phase encoding increments is termed
TR.
Regarding the frequency-encoding axis, instead of applying a negative dephasing gradient
as in the gradient-echo sequence, the dephasing gradient in a spin-echo sequence is usually
applied between 90º and 180º pulses with a positive polarity.
The blank periods are introduced to give certain values to TR and TE in order to achieve
corresponding 𝑇1 and 𝑇2-contrast weighting into the image as discussed in the next section.

60
4.5.2. 𝑻𝟏 and 𝑻𝟐-weighted imaging sequences
The intensity of an axial image acquired using a spin-echo sequence is given by:
The term 1 − 𝑒−𝑇𝑅/𝑇1 determines the 𝑇1 weighting of the sequence. If the TR value (which
can be set by the operator) is set to a value much greater than 𝑇1, then the image has no 𝑇1-
weighting as the term 1 − 𝑒−𝑇𝑅/𝑇1 is very similar for all tissues. If the TR value is set closer to
the tissue 𝑇1 then the image becomes more 𝑇1-weighted. As the TR values becomes smaller, the
SNR decreases, although the total imaging time (𝑁𝑝 × 𝑇𝑅) also decreases (the goal is to decrease
imaging time while maintaining sufficient SNR for accurate diagnosis).
The same considerations apply to the term 𝑒−𝑇𝐸/𝑇2, which determines the degree of 𝑇2-
weighting: if the value of TE is set much shorter than the tissue 𝑇2, then no 𝑇2 contrast is present;
if the value of TE is too long, then the contrast is high, but the SNR is low (the goal is to have the
highest CNR).
4.5.2.1. Which physical properties influence 𝑻𝟏 and 𝑻𝟐?
The mechanism of 𝑇1 relaxation involves the protons losing their excess energy via
interactions with oscillating magnetic fields, produced by nuclei in surrounding molecules as
they execute random Brownian motion. When these randomly fluctuating magnetic fields have
a component at the Larmor frequency, they can stimulate transitions between the antiparallel
and parallel states, and thereby cause the 𝑀𝑧 component to return to 𝑀0. Thus, slowly moving
molecules (low frequency) in a viscous media have higher contributions to 𝑇1 at low magnetic
field strengths, while rapidly moving molecules (high frequency) in mobile liquids produce
fluctuating magnetic fields over a wide frequency range. The spectral density 𝐽(𝜔) is a measure
of the number of nuclei capable of producing magnetic fields at the Larmor frequency, thus the
greater 𝐽(𝜔), the shorter is 𝑇1:
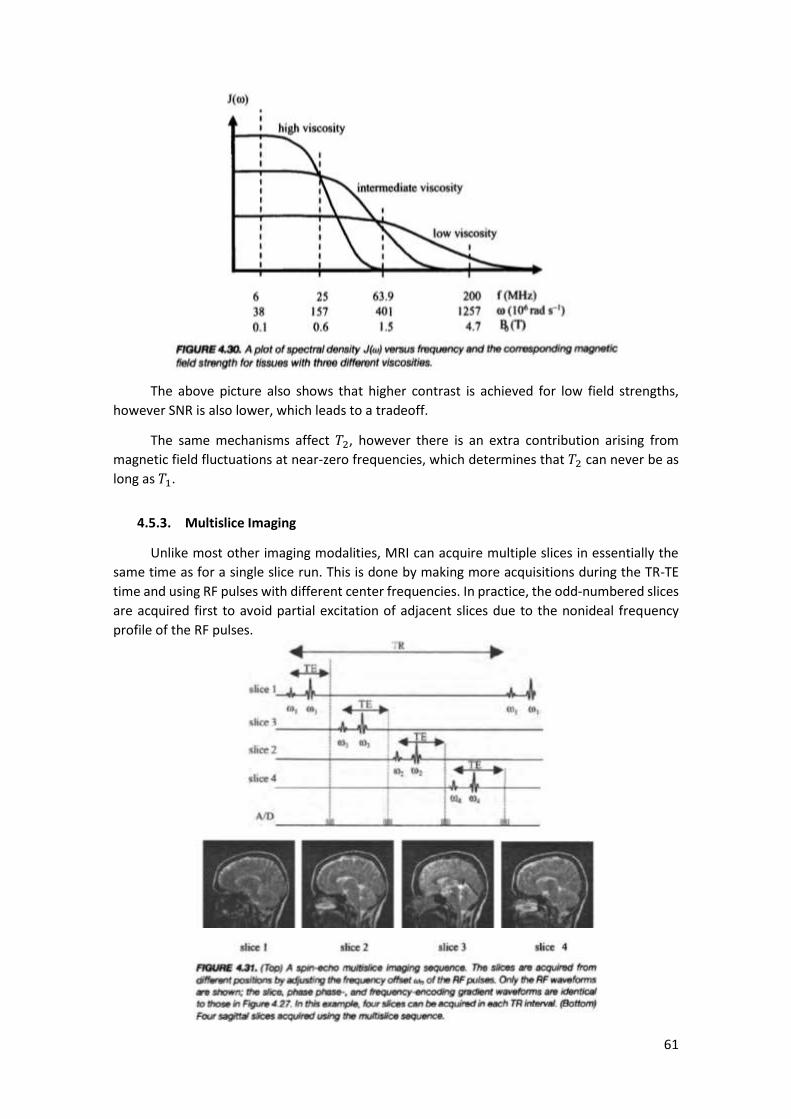
61
The above picture also shows that higher contrast is achieved for low field strengths,
however SNR is also lower, which leads to a tradeoff.
The same mechanisms affect 𝑇2, however there is an extra contribution arising from
magnetic field fluctuations at near-zero frequencies, which determines that 𝑇2 can never be as
long as 𝑇1.
4.5.3. Multislice Imaging
Unlike most other imaging modalities, MRI can acquire multiple slices in essentially the
same time as for a single slice run. This is done by making more acquisitions during the TR-TE
time and using RF pulses with different center frequencies. In practice, the odd-numbered slices
are acquired first to avoid partial excitation of adjacent slices due to the nonideal frequency
profile of the RF pulses.
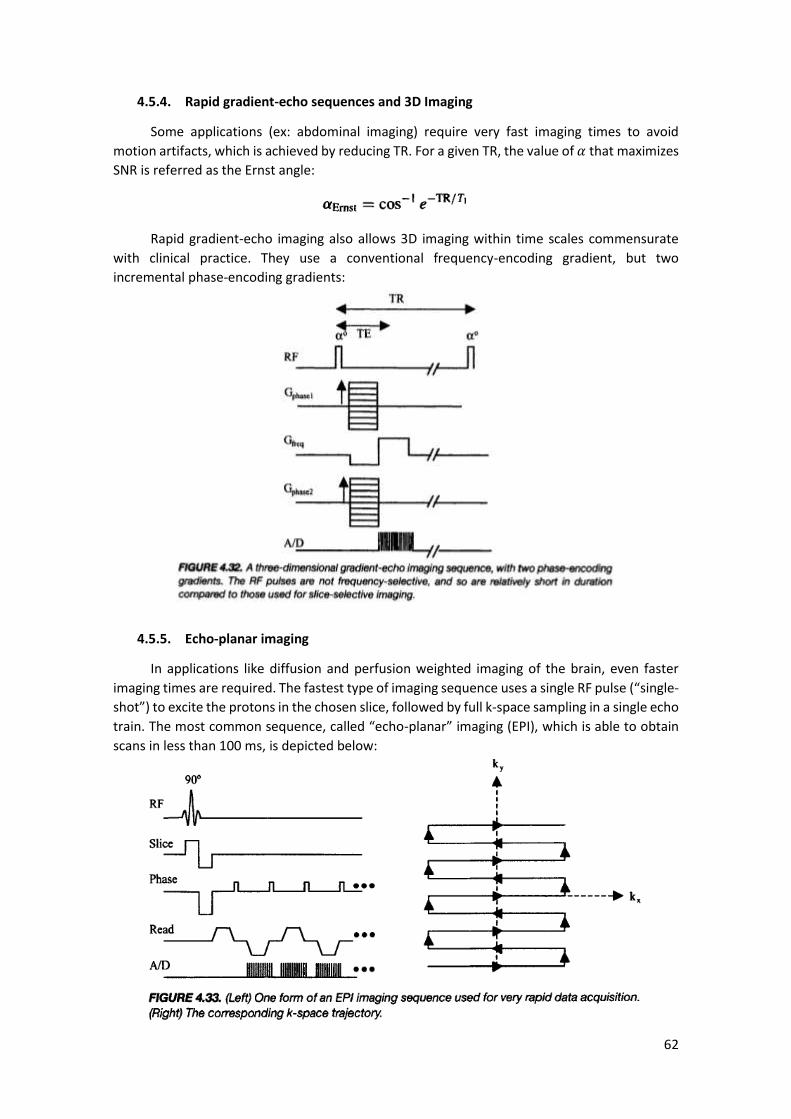
62
4.5.4. Rapid gradient-echo sequences and 3D Imaging
Some applications (ex: abdominal imaging) require very fast imaging times to avoid
motion artifacts, which is achieved by reducing TR. For a given TR, the value of 𝛼 that maximizes
SNR is referred as the Ernst angle:
Rapid gradient-echo imaging also allows 3D imaging within time scales commensurate
with clinical practice. They use a conventional frequency-encoding gradient, but two
incremental phase-encoding gradients:
4.5.5. Echo-planar imaging
In applications like diffusion and perfusion weighted imaging of the brain, even faster
imaging times are required. The fastest type of imaging sequence uses a single RF pulse (“single-
shot”) to excite the protons in the chosen slice, followed by full k-space sampling in a single echo
train. The most common sequence, called “echo-planar” imaging (EPI), which is able to obtain
scans in less than 100 ms, is depicted below:

63
This sequence can introduce an unacceptable level of image blurring due to the broad
PSF, which arises from 𝑇2∗ relaxation during the sequence. To overcome this, a segmented mode
can be used, where, for instance, only every fourth data point is acquired and the process is
repeated 4 times.
4.5.6. Spiral imaging
Instead of a rectangular k-space trajectory, “spiral imaging” uses a spiral trajectory, which
presents two basic advantages:
- Low spatial frequencies are sampled more densely, because the spiral is tightest close
to the origin of the k-space axis. This results in higher SNR and compensation for patient
motion;
- The gradient “slew rate” (rate at which strength is changed) is slower.
Prior to the 2D inverse Fourier transform, an interpolation onto a rectangular grid must
be performed. A segmented mode is also commonly used.
4.6. Image characteristics
The tradeoffs and factors that affect SNR, spatial resolution and CNR are discussed below.
4.6.1. Signal-to-noise ratio
The main factors affecting SNR are:
- Magnetic field 𝐵0 strength: improves nuclear polarization and voltage measured by
Faraday induction (↑)
- RF coil sensitivity: defined as the 𝐵1 field produced per unit current (↑)
- Noise contributions from the RF coil and the sample: random voltage fluctuations (↓)
- Number of phase encoding steps 𝑁𝑝(↓)
- Number of frequency encoding steps 𝑁𝑟(↓)
- Slice thickness (↑)

64
4.6.2. Spatial resolution
The image PSF is different in each spatial dimension. In the slice-select direction, the PSF
is simply related to the RF pulse frequency profile (slice thickness). In the frequency and phase
encoding directions, three factors affect the PSF:
- Digital resolution: defined as FOV/Number of data points acquired.
- Data truncation: because only a finite number of frequency and phase encoding data
points are taken, the data are effectively truncated and the corresponding PSF is a sinc
function. The width of the sinc function in each dimension is inversely proportional to
the number of data points acquired;
- 𝑻𝟐∗ relaxation time: the exponential decay corresponds to a Lorentzian PSF, which
FWHM decreases when 𝑇2∗ increases:
4.6.3. Contrast-to-noise ratio
CNR is essentially dependent on the difference between the relaxation times and proton
density and the values of TR and TE. There is also a dependence on the strength of 𝐵0 since 𝑇1-
weighted contrast is higher for lower 𝐵0. Since CNR between two tissues depends on the
respective SNRs, CNR is also affected by the factors listed for SNR.
4.7. MRI contrast agents
In certain situations such as the detection of very small lesions, where the signal from the
lesion is effectively averaged with that of healthy tissue, the CNR can be very low. In this case,
one of two basic types of MRI contrast agents can be used:
- Paramagnetic agents: shorten 𝑇1; tissues on which it accumulate appear bright;
- Superparamagnetic (or ferromagnetic): shorten 𝑇2 and 𝑇2∗, accumulate primarily in
healthy tissues.
4.7.1. Paramagnetic agents
Paramagnetic agents are based on metal ions such as gadolinium that have a large number
of unpaired electrons (with high magnetic moments). The interactions between the unpaired
electrons and the water molecules cause the proton 𝑇1 to be shortened, with the effect being
quantified by the relaxivity of the agent:
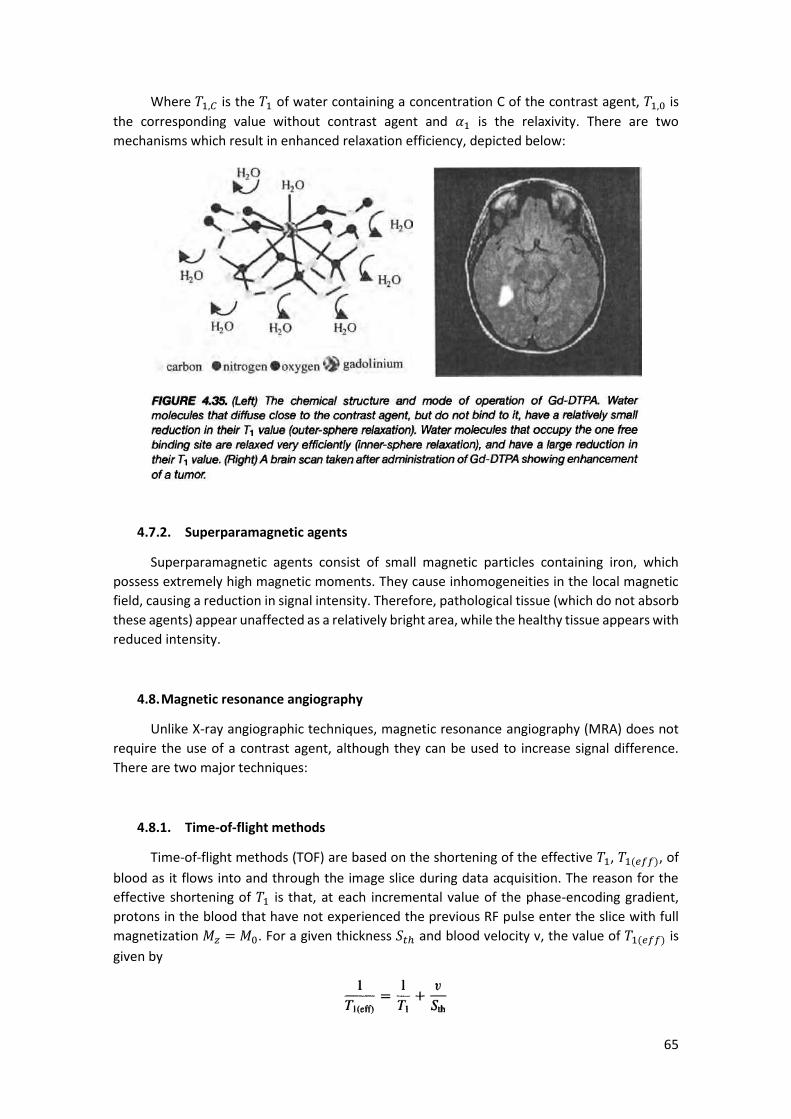
65
Where 𝑇1,𝐶 is the 𝑇1 of water containing a concentration C of the contrast agent, 𝑇1,0 is
the corresponding value without contrast agent and 𝛼1 is the relaxivity. There are two
mechanisms which result in enhanced relaxation efficiency, depicted below:
4.7.2. Superparamagnetic agents
Superparamagnetic agents consist of small magnetic particles containing iron, which
possess extremely high magnetic moments. They cause inhomogeneities in the local magnetic
field, causing a reduction in signal intensity. Therefore, pathological tissue (which do not absorb
these agents) appear unaffected as a relatively bright area, while the healthy tissue appears with
reduced intensity.
4.8. Magnetic resonance angiography
Unlike X-ray angiographic techniques, magnetic resonance angiography (MRA) does not
require the use of a contrast agent, although they can be used to increase signal difference.
There are two major techniques:
4.8.1. Time-of-flight methods
Time-of-flight methods (TOF) are based on the shortening of the effective 𝑇1, 𝑇1(𝑒𝑓𝑓), of
blood as it flows into and through the image slice during data acquisition. The reason for the
effective shortening of 𝑇1 is that, at each incremental value of the phase-encoding gradient,
protons in the blood that have not experienced the previous RF pulse enter the slice with full
magnetization 𝑀𝑧 = 𝑀0. For a given thickness 𝑆𝑡ℎ and blood velocity v, the value of 𝑇1(𝑒𝑓𝑓) is
given by
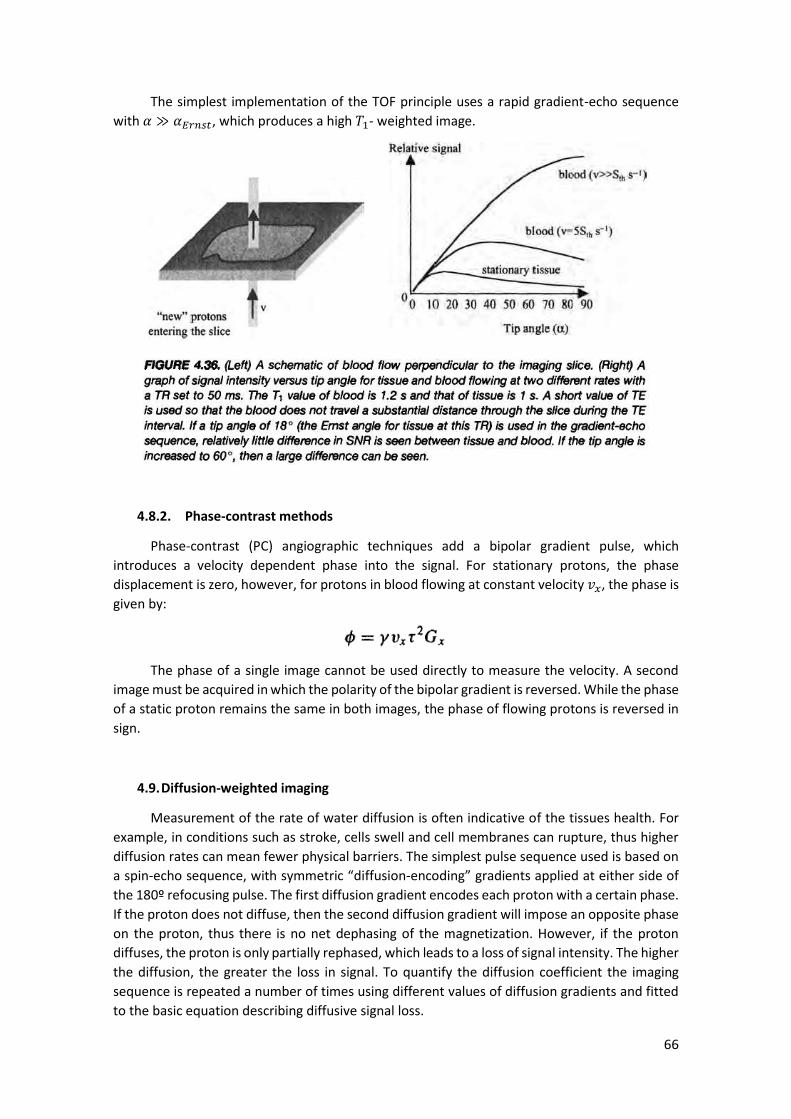
66
The simplest implementation of the TOF principle uses a rapid gradient-echo sequence
with 𝛼 ≫ 𝛼𝐸𝑟𝑛𝑠𝑡, which produces a high 𝑇1- weighted image.
4.8.2. Phase-contrast methods
Phase-contrast (PC) angiographic techniques add a bipolar gradient pulse, which
introduces a velocity dependent phase into the signal. For stationary protons, the phase
displacement is zero, however, for protons in blood flowing at constant velocity 𝑣𝑥, the phase is
given by:
The phase of a single image cannot be used directly to measure the velocity. A second
image must be acquired in which the polarity of the bipolar gradient is reversed. While the phase
of a static proton remains the same in both images, the phase of flowing protons is reversed in
sign.
4.9. Diffusion-weighted imaging
Measurement of the rate of water diffusion is often indicative of the tissues health. For
example, in conditions such as stroke, cells swell and cell membranes can rupture, thus higher
diffusion rates can mean fewer physical barriers. The simplest pulse sequence used is based on
a spin-echo sequence, with symmetric “diffusion-encoding” gradients applied at either side of
the 180º refocusing pulse. The first diffusion gradient encodes each proton with a certain phase.
If the proton does not diffuse, then the second diffusion gradient will impose an opposite phase
on the proton, thus there is no net dephasing of the magnetization. However, if the proton
diffuses, the proton is only partially rephased, which leads to a loss of signal intensity. The higher
the diffusion, the greater the loss in signal. To quantify the diffusion coefficient the imaging
sequence is repeated a number of times using different values of diffusion gradients and fitted
to the basic equation describing diffusive signal loss.

67
4.10. Functional MRI
fMRI makes use of the sensitivity of the MRI signal intensity to the level of oxygen in the
blood in the brain (oxygen-level-dependent – BOLD – effect) to determine which areas of the
brain are involved in specific cognitive tasks. In gray matter in the brain, a modest increase in
the cerebral metabolic rate of oxygen (MCRO2) and of glucose occurs in areas involved in neural
activation, which leads to the release of vasodilatory compounds and increase of blood flow in
the capillary bed. The rate of delivery of oxygen increases, but to a much lesser extent than the
increase in blood flow, which leads to an oxygenation of blood. This, in turn, increases the level
of oxyhemoglobin and decreases the level of deoxyhemoglobin. The decrease in
deoxyhemoglobin reduces the local magnetic field gradients between the blood in the capillary
bed and tissue, which leads to an increase of 𝑇2 and 𝑇2∗ in areas of the brain associated with
neural activation.
The most common sequence used is the multislice EPI because it is fast enough to obtain
whole brain coverage in a few seconds. The changes in image intensity in activated areas are
very small, thus the experiments are repeated a number of times and the data is subjected to
statistical analysis and filtering.
The changing in MRI signal intensity at sites associated with neuronal activation has three
components:
- Small signal decrease immediately after the onset of the stimulation, which corresponds
to the total deoxyhemoglobin increasing for the first 3 s due to an initial increase in
oxygen extraction before the increase in blood flow;
- Increase in signal intensity, which reaches a maximum at about 7 s after the onset of the
stimulus (hemodynamic response time);
- Signal undershoot which can last up to 1 min and corresponds to the blood volume in
the venules.
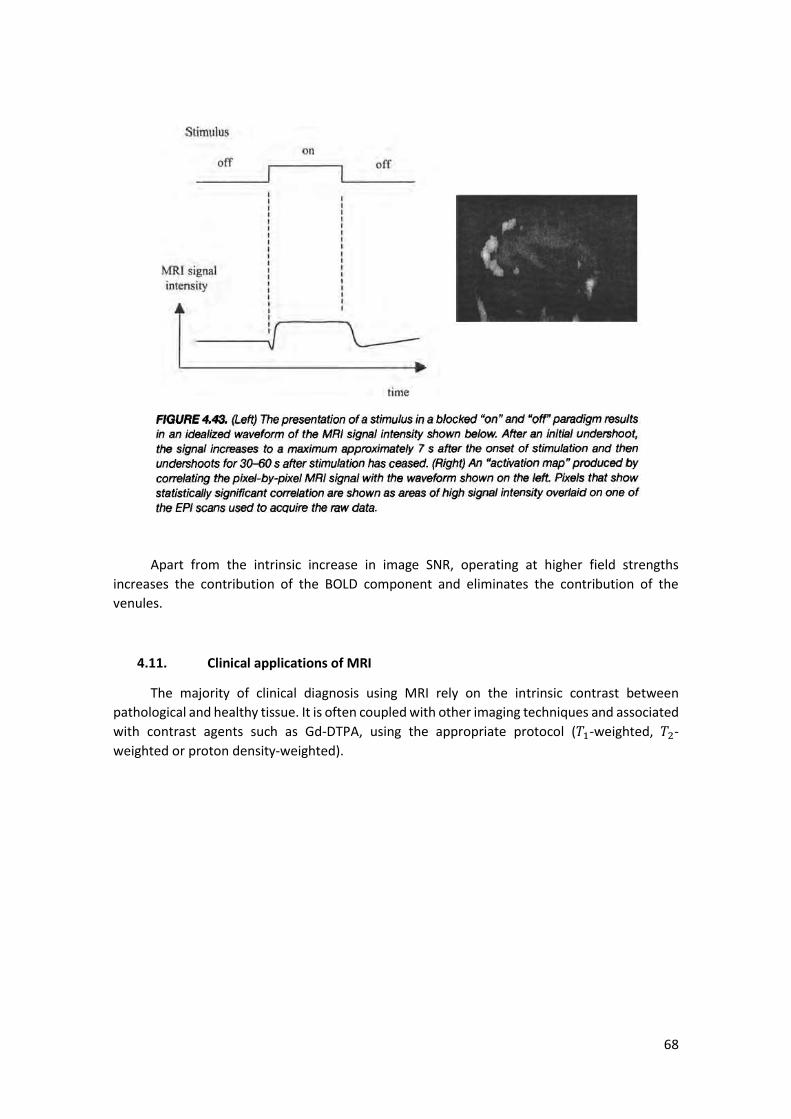
68
Apart from the intrinsic increase in image SNR, operating at higher field strengths
increases the contribution of the BOLD component and eliminates the contribution of the
venules.
4.11. Clinical applications of MRI
The majority of clinical diagnosis using MRI rely on the intrinsic contrast between
pathological and healthy tissue. It is often coupled with other imaging techniques and associated
with contrast agents such as Gd-DTPA, using the appropriate protocol (𝑇1-weighted, 𝑇2-
weighted or proton density-weighted).