Meconium stained amniotic fluid with meconium aspiration syndrome by uma
Upload
kaylynn-rollCategory
view
249download
1
Meconium Happens:Meconium Aspiration Syndrome
Meconium Happens:Meconium Aspiration Syndrome
John Salyer RRT-NPS, FAARC, MBA
Director Respiratory Therapy
Seattle Children’s Hospital and Research Institute

The CulpritThe Culprit

What is meconium aspiration?What is meconium aspiration?
Meconium is the first intestinal discharge of the newborn
Epithelial cells, fetal hair, mucus, bile
Intrauterine stress may cause in utero passage of
meconium
Aspirated by the fetus when fetal gasping or deep
breathing occurs stimulated by hypoxia and hypercarbia
Warning sign of fetal distress

Frequency of meconium stained amniotic fluid = 8-19 %
Of MEC stained infants:
30 % depressed at birth
10 % meconium aspiration syndrome (range 5-33 %)
Of infants with MEC aspiration syndrome
17 % deliver through thin meconium (range 7-35 %)
35 % need mechanical ventilation (range 25-60 %)
12 % die (range 5-37 %)
Meconium: The StatsMeconium: The Stats


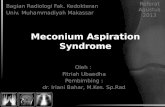
PO2
L --> R ductus arteriosus
shunt
Ventilation
Remove Placenta
Ductus Venosus Closes
Systemic Vascular Resistance
ß Umbilical Venous Return
ß IVC Return
ß RA Pressure
Ý Pulmonary Venous Return
Ý LA Pressure
Foramen Ovale Closes
Pulmonary Vascular Resistance


Goldsmith JP. J Perinatology 2008:28;S49-S55

Ventilation Strategy for MAS
Settings
1. Relatively Rapid Respiratory Rates• 40-60 breaths/min
2. Lowest PIP sufficient for chest excursion• Start at 16/5 and institute HFOV for
PIP>25• target VT 4-6 mL/kg BW• ECLS for mPaw>14• Heavy sedation for gas trapping
3. Short Inspiratory Times• 0.3-0.5 s• Longer Expiratory Times and lower
PEEP for gas trapping4. Nitric Oxide works well in this
population
Blood Gases
1. No pulmonary hypertension• pCO2 levels 40-50• pH > 7.30• Pa02 70-80
2. Pulmonary hypertension• pCO2 levels 30-35• pH > 7.35• Pa02 80-100

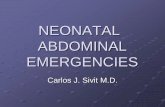
Airflow Scalars in a patient with MAS

OHSU Experience: Inborn + TransfersOHSU Experience: Inborn + Transfers
# Mecpassed
DRintub
MAS MAS+ vent
ECMO Died
1992-94 146 88 44 28 4 3*1995-97 154 92 39 25 1 1*
Total 300 180 83 53 5 4
MAS = Meconium aspiration syndrome as primary pulmonary diagnosisNo pulmonary hypoplasia or major congenital anomalies
MAS+ vent = ventilated with pulmonary diagnosis of MAS or PPHNECMO = MAS infants transferred for ECMO Died : * 1 infant in each of the years died with a diagnosis of severe HIE

Risk Factors for Meconium PassageRisk Factors for Meconium Passage
Postterm pregnancy
Preeclampsia-eclampsia
Maternal hypertension
Maternal diabetes mellitus
Abnormal fetal heart rate
IUGR
Abnormal biophysical profile
Oligohydramnios
Maternal heavy smoking

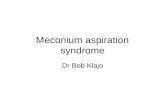
Infant ActiveInfant Depressed
Intrapartum suctioning of mouth, nose, pharynx
Intubate and suction trachea
Other resuscitation as indicated
Observe
Meconium in Amniotic Fluid

Meconium Aspiration SyndromePathophysiology
Meconium Aspiration SyndromePathophysiology
Airway obstruction of large and small airways
Inflammation and edema Protein leak
Inflammatory Mediators
Direct toxicity of meconium constituents = chemical
pneumonitis
Surfactant dysfunction or inactivation
Effects of in utero hypoxemia and acidosis
Altered pulmonary vasoreactivity (PPHN)

Meconium Aspiration SyndromeDiagnosis
Meconium Aspiration SyndromeDiagnosis
Known exposure to meconium stained amniotic fluid
Respiratory symptoms not explained by other cause
R/O pneumonia, RDS, spontaneous air leak
CXR changes - diffuse, patchy infiltrates, consolidation,
atelectasis, air leaks, hyperinflation



Meconium Aspiration SyndromeTreatment
Meconium Aspiration SyndromeTreatment
Ventilation strategies Avoid air leak, check CXR with acute
deterioration Prevent pulmonary hypertension - generous O2 HFOV if unable to maintain on conventional vent
Steroids (no human data, controversial)
ROS, Antibiotics (ampicillin, gentamicin)
Surfactant
Inhaled Nitric Oxide
ECMO

Other Things to Watch ForOther Things to Watch For
Hypoxia
Acidosis
Hypoglycemia
Hypocalcemia
End-organ damage due to perinatal
asphyxia

Fox WW,. Pediatrics 1975; 56:214–217.

Meconium Aspiration SyndromeSurfactant Treatment
Meconium Aspiration SyndromeSurfactant Treatment
Methods < 6 hours old with MAS
20 infants randomized to receive 150 mg/kg surfactant
by 20 minute infusion, q6h x4 doses maximum
On ventilator - FiO2 > 50%, MAP > 7, a:A PO2 < 0.22
Endpoint = improvement in OI and a:A PO2
No difference in groups
Findlay et al. Pediatrics 97 (1): 48, 1996.

Meconium Aspiration SyndromeSurfactant Treatment
Meconium Aspiration SyndromeSurfactant Treatment
Results
No infant received more than 3 doses
Significant improvement in OI, MAP, FiO2
within 3-6 hours after 2nd dose of surfactant
Significant improvement in a:A PO2 within 1
hour of 1st dose of surfactant
Findlay et al. Pediatrics 97 (1): 48, 1996.

Control Surf P valueAir leak 5 0 0.024ECMO 6 1 0.037Days MV 11 (1) 8 (1) 0.047Days O2 20 (3) 13 (1) 0.031LOS (days) 24 (2) 16 (1) 0.003D/C on O2 8 6 NSMortality (< 28 d) 0 0 NS
Meconium Aspiration SyndromeSurfactant Treatment
Meconium Aspiration SyndromeSurfactant Treatment
Findlay et al. Pediatrics 97 (1): 48, 1996.

Meconium Aspiration SyndromeOutcome
Meconium Aspiration SyndromeOutcome
High incidence long term pulmonary problems At 6 months - 23% MAS with regular bronchodilator
therapy*
FRC was higher in symptomatic infants
IPPV and O2 were not predictors of problems
Increased risk of poor neurologic outcome due
to perinatal insult - seizures, CP, mental
retardation*Yuksel et al. Pediatric Pulmonology 16:358, 1993