Meconium aspiration syndrome (MAS)
17
MECONIUM ASPIRATION SYNDROME Written by: Dr. Prithwiraj Maiti, R.G.Kar Medical College Resources used: Nelson’s Pediatrics, Rudolph’s Pediatrics, CMDT of Pediatrics and IAP Textbook of Pediatrics
-
Upload
rgkar-medical-college -
Category
Health & Medicine
-
view
1.497 -
download
7
Transcript of Meconium aspiration syndrome (MAS)

MECONIUM ASPIRATION SYNDROMEWritten by: Dr. Prithwiraj Maiti, R.G.Kar Medical College
Resources used: Nelson’s Pediatrics, Rudolph’s Pediatrics, CMDT of Pediatrics and IAP Textbook of Pediatrics

CONTENTS
• INTRODUCTION
• RISK FACTORS
• PATHOPHYSIOLOGY
• CLINICAL PRESENTATION
• DIAGNOSTIC TOOLS
• DIFFERENTIAL DIAGNOSIS
• COMPLICATIONS
• MANAGEMENT
• PREVENTION
• PROGNOSIS

INTRODUCTION
• Meconium aspiration syndrome (MAS) is one of the most common causes of severe respiratory failure in infants born at term/ post-term gestation.
• Meconium is the first stool of an infant, composed of materials ingested during the period of gestation.
• Meconium is normally stored in the infant's intestines until after birth, but sometimes (often in response to fetal distress and hypoxia) it is expelled into the amniotic fluid prior to birth, or during labor. If the baby then inhales the meconium, MAS may occur.
• Meconium is present in the amniotic fluid in approximately 10-15% of all term deliveries, but MAS occurs in fewer than 1/3rd of these infants.

RISK FACTORS
Maternal risk factors includes all which induce fetal distress and hypoxia:
1. Preeclampsia,
2. Hypertension,
3. Oligohydramnios,
4. Maternal infections,
5. Maternal drug use,
6. Placental insufficiency,
7. Intrauterine growth restriction.

PATHOPHYSIOLOGY

CLINICAL PRESENTATION
HISTORY:
MAS occurs most frequently in term/ post-term infants who:
1. Have a history of fetal distress
2. Have a low APGAR score at birth and
3. Have meconium stained amniotic fluid at birth.

CLINICAL PRESENTATION
SIGNS AND SYMPTOMS:
1. Meconium stained skin, nails and umbilical cord
2. Signs of respiratory distress develop usually within the 1st hour of birth:
A. Tachypnoea,
B. Intercostal retractions,
C. Coarse bronchial sounds,
D. Expiratory grunting, and/or
E. Cyanosis.
3. Chest may be overinflated/ barrel shaped, with a protruding sternum (due to obstructive emphysema).

DIAGNOSTIC TOOLS
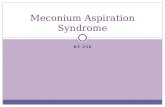
• CXR: Often reveals-
1. Bilateral patchy areas of increased density,
2. Sometimes confluent and alternating with hyperlucent areas;
3. Increased anteroposterior diameter, and
4. Flattening of the diaphragm.
• ABG in first hour of birth: Often reveals evidences of perinatal asphyxia-
1. Hypoxemia and
2. Some degree of metabolic acidosis.

DIAGNOSTIC TOOLS
CXR from an infant with
severe MAS showing bilateral
patchy areas of increased
density

DIFFERENTIAL DIAGNOSIS
• A normal CXR in an infant with severe hypoxemia and no cardiac malformation suggests the diagnosis of pulmonary hypertension.

COMPLICATIONS
• Pneumothorax
• Persistent pulmonary hypertension of the newborn
• Secondary bacterial infection of the lungs
• Subglottic stenosis (secondary to the extended presence of the endotracheal tube in patients requiring mechanical ventilation).

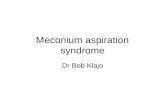
COMPLICATIONS
Development of a left tension
pneumothorax in an infant with MAS

MANAGEMENT
• Treatment of MAS includes supportive care and standard management for respiratory distress
• Endotracheal intubation and suction to remove meconium from the airway before the 1st breath in the delivery room is essential
• In infants with clinical signs of respiratory failure; oxygen saturation by pulse oximetry, ABG and a CXR should be obtained as soon as possible
• These infants often require high peak inspiratory pressures to maintain adequate ventilation and oxygenation
• In infants with MAS who develop complications (like pneumothorax) require mechanical ventilation
• Patients with MAS who are refractory to conventional mechanical ventilation may benefit from HFV (High frequency ventilation) or ECMO (Extracorporeal membrane oxygenation)

MANAGEMENT
• Administration of exogenous surfactant/ inhaled NO to infants with MAS and hypoxemic respiratory failure/ pulmonary hypertension requiring mechanical ventilation decreases the need for ECMO support
• Because meconium aspiration can inactivate alveolar surfactant, the administration of exogenous surfactant or even pulmonary lavage with a surfactant solution sometimes can be beneficial
• Inhaled nitric oxide is the pulmonary vasodilator of choice
• Because of the difficulty in diagnosing a superimposed infection, many clinicians elect to treat these infants with antibiotics until the acute respiratory failure subsides
• Most of these infants are hyperactive and restless, it is often necessary to use sedation or even neuromuscular blockade, at least during the first 24-48 hours of mechanical ventilation, until the infant is stable and the peak airway pressure can be reduced.

PREVENTION
• When meconium appears in the amniotic fluid or is present in the upper airway at the time of birth, the first concern should be to reduce the risk of aspiration of the meconium into the more distal air spaces and thereby prevent the subsequent pulmonary involvement
• The recommended approach is to suction the nasopharynx with a large catheter or a suction bulb
• Infants with previous intrapartum asphyxia and meconium aspiration should receive 100% oxygen immediately after birth in order to increase arterial oxygenation and reverse the pulmonary hypertension that accompanies hypoxemia and acidosis
• Most clinicians still recommend early suctioning of the nasopharynx when there is any evidence of meconium in the amniotic fluid with the purpose of reducing the risk of aspiration of this material into the lower airways.

PROGNOSIS
• The mortality rate of meconium-stained infants is considerably higher than that of non-stained infants. The decline in neonatal deaths due to MAS during the last decades is related to improvements in obstetric and neonatal care.
• Although most infants with MAS survive without sequelae, long-term follow-up studies have demonstrated an increased prevalence of neurologic sequelae most likely associated with perinatal asphyxia.