Case Report A Rare Case of Meconium Periorchitis Diagnosed...
3
Case Report A Rare Case of Meconium Periorchitis Diagnosed in Utero Daigo Ochiai, 1 Sayu Omori, 2 Toshiyuki Ikeda, 1 Kazumi Yakubo, 1 and Tatsuro Fukuiya 1 1 Department of Obstetrics & Gynecology, Saitama City Hospital, 2460 Mimuro, Midori-ku, Saitama-shi, Saitama 336-8522, Japan 2 Department of Pediatrics, Saitama City Hospital, 2460 Mimuro, Midori-ku, Saitama-shi, Saitama 336-8522, Japan Correspondence should be addressed to Daigo Ochiai; [email protected] Received 26 June 2015; Revised 2 September 2015; Accepted 7 September 2015 Academic Editor: Giovanni Monni Copyright © 2015 Daigo Ochiai et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Meconium periorchitis is a rare disorder caused by fetal meconium peritonitis, with subsequent passage of meconium into the scrotum via a patent processus vaginalis. To date, clinical significance of meconium periorchitis for the prenatal diagnosis of meconium peritonitis and prediction for postnatal surgery remains to be determined. We present a clinical course of a fetus presenting with meconium periorchitis induced by meconium peritonitis. At 28 weeks’ gestation, fetal ultrasonography indicated fetal ascites associated with bilateral hydrocele and peritesticular calcification without other signs of meconium peritonitis. e pregnancy was uneventful until delivery and the infant was delivered at 37 weeks’ gestation. No abdominal distension was observed at birth, and radiography did not reveal any abdominal calcification except for scrotal calcification. Abdominal distension was observed 3 days aſter birth and laparotomy was performed. e diagnosis of meconium peritonitis was confirmed at surgery. Our case illustrated that careful examination of the scrotum during fetal life was helpful for prenatal diagnosis of meconium peritonitis as well as postnatal management. 1. Introduction Meconium periorchitis (MPO) is a rare disorder caused by fetal meconium peritonitis, with subsequent passage of meco- nium into the scrotum via a patent processus vaginalis [1]. To date, clinical significance of MPO for the prenatal diagnosis of meconium peritonitis and prediction for postnatal surgery remains to be determined. Herein, we present the clinical course of a fetus presenting with MPO induced by meconium peritonitis. 2. Case Report A 35-year-old gravida 1, para 1 woman was referred to our facility for evaluation at 28 weeks’ gestation. Fetal ultra- sonography indicated fetal ascites associated with bilateral hydrocele and peritesticular calcification (Figure 1(a)), lead- ing to a diagnosis of MPO induced by meconium peritonitis, although other characteristic signs such as calcification in the abdomen, dilated bowel, and intra-abdominal cystic mass were not evident at that time. e fetal ascites disappeared within 1 week, and the bilateral hydrocele disappeared in 2 weeks. However, the peritesticular calcification persisted. At 30 weeks’ gestation, a dilated bowel sign appeared, but it disappeared in 2 weeks. Viral infections including TORCH were negative. e baby was spontaneously delivered at 37 weeks’ gestation, weighing 2545 g with Apgar scores of 8 and 9 at 1 min and 5 min, respectively. No abdominal distension was observed at birth, and radiography did not reveal any abdominal calcification, but it revealed a scrotal calcification (Figure 1(b)), which was also demonstrated via ultrasonography. Abdominal distension was observed 3 days aſter birth; therefore, laparotomy was performed for the treatment of a bowel perforation. e diagnosis of meconium peritonitis was confirmed at surgery owing to the presence of a perforation of the small bowel 25cm from the distal end of the ileum. e infant’s scrotum remained asymptomatic and did not enlarge; therefore, the area was monitored carefully. e infant was subsequently discharged in good health. 3. Discussion In the present case, fetal ascites was the isolated manifes- tation unaccompanied by other exudates such as cutaneous oedema, pericardial or pleural effusion, or polyhydramnios. Hindawi Publishing Corporation Case Reports in Obstetrics and Gynecology Volume 2015, Article ID 606134, 2 pages http://dx.doi.org/10.1155/2015/606134
Transcript of Case Report A Rare Case of Meconium Periorchitis Diagnosed...

Case ReportA Rare Case of Meconium Periorchitis Diagnosed in Utero
Daigo Ochiai,1 Sayu Omori,2 Toshiyuki Ikeda,1 Kazumi Yakubo,1 and Tatsuro Fukuiya1
1Department of Obstetrics & Gynecology, Saitama City Hospital, 2460 Mimuro, Midori-ku, Saitama-shi, Saitama 336-8522, Japan2Department of Pediatrics, Saitama City Hospital, 2460 Mimuro, Midori-ku, Saitama-shi, Saitama 336-8522, Japan
Correspondence should be addressed to Daigo Ochiai; [email protected]
Received 26 June 2015; Revised 2 September 2015; Accepted 7 September 2015
Academic Editor: Giovanni Monni
Copyright © 2015 Daigo Ochiai et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Meconium periorchitis is a rare disorder caused by fetal meconium peritonitis, with subsequent passage of meconium into thescrotum via a patent processus vaginalis. To date, clinical significance of meconium periorchitis for the prenatal diagnosis ofmeconium peritonitis and prediction for postnatal surgery remains to be determined. We present a clinical course of a fetuspresenting with meconium periorchitis induced by meconium peritonitis. At 28 weeks’ gestation, fetal ultrasonography indicatedfetal ascites associated with bilateral hydrocele and peritesticular calcification without other signs of meconium peritonitis. Thepregnancy was uneventful until delivery and the infant was delivered at 37 weeks’ gestation. No abdominal distension was observedat birth, and radiography did not reveal any abdominal calcification except for scrotal calcification. Abdominal distension wasobserved 3 days after birth and laparotomy was performed. The diagnosis of meconium peritonitis was confirmed at surgery. Ourcase illustrated that careful examination of the scrotum during fetal life was helpful for prenatal diagnosis of meconium peritonitisas well as postnatal management.
1. Introduction
Meconium periorchitis (MPO) is a rare disorder caused byfetalmeconiumperitonitis, with subsequent passage ofmeco-nium into the scrotum via a patent processus vaginalis [1]. Todate, clinical significance of MPO for the prenatal diagnosisof meconium peritonitis and prediction for postnatal surgeryremains to be determined. Herein, we present the clinicalcourse of a fetus presenting withMPO induced bymeconiumperitonitis.
2. Case Report
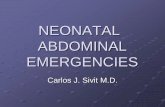
A 35-year-old gravida 1, para 1 woman was referred to ourfacility for evaluation at 28 weeks’ gestation. Fetal ultra-sonography indicated fetal ascites associated with bilateralhydrocele and peritesticular calcification (Figure 1(a)), lead-ing to a diagnosis of MPO induced by meconium peritonitis,although other characteristic signs such as calcification inthe abdomen, dilated bowel, and intra-abdominal cysticmasswere not evident at that time. The fetal ascites disappearedwithin 1 week, and the bilateral hydrocele disappeared in 2weeks. However, the peritesticular calcification persisted. At
30 weeks’ gestation, a dilated bowel sign appeared, but itdisappeared in 2 weeks. Viral infections including TORCHwere negative. The baby was spontaneously delivered at 37weeks’ gestation, weighing 2545 g with Apgar scores of 8 and9 at 1min and 5min, respectively.
No abdominal distension was observed at birth, andradiography did not reveal any abdominal calcification, but itrevealed a scrotal calcification (Figure 1(b)), which was alsodemonstrated via ultrasonography. Abdominal distensionwas observed 3 days after birth; therefore, laparotomy wasperformed for the treatment of a bowel perforation. Thediagnosis of meconium peritonitis was confirmed at surgeryowing to the presence of a perforation of the small bowel25 cm from the distal end of the ileum. The infant’s scrotumremained asymptomatic and did not enlarge; therefore, thearea was monitored carefully. The infant was subsequentlydischarged in good health.
3. Discussion
In the present case, fetal ascites was the isolated manifes-tation unaccompanied by other exudates such as cutaneousoedema, pericardial or pleural effusion, or polyhydramnios.
Hindawi Publishing CorporationCase Reports in Obstetrics and GynecologyVolume 2015, Article ID 606134, 2 pageshttp://dx.doi.org/10.1155/2015/606134

2 Case Reports in Obstetrics and Gynecology
(a) (b) (c)
Figure 1: Prenatal ultrasonographic and postnatal radiographic findings. Prenatal ultrasonography revealed bilateral hydrocele withperitesticular calcification at 28 weeks’ gestation (a), while postnatal radiography demonstrated scrotal calcification without abdominalcalcification (b, c). (c) was an enlarged view of the dotted circle in (b). Arrow indicated calcification.
Although the differential diagnosis of fetal ascites is diversebecause of various possible causes including immune andnonimmune hydrops, isolated fetal ascites associated withscrotal hydrocele and peritesticular calcification are sufficientsigns for the prenatal diagnosis of meconium peritonitis [2].Prenatal characteristic findings of meconium peritonitis areabdominal calcification, ascites, dilated bowel, and intra-abdominal cystic mass [3, 4], but it is sometimes difficultto make a definite diagnosis because these signs vary inshort periods. In fact, the fetal ascites disappeared within 1week and no abdominal calcification was detected prenatally.In case of meconium peritonitis, Zerhouni et al. reportedthat fetal intra-abdominal calcification and dilated bowelon prenatal ultrasonograms predicted a need for postnatalsurgery [4]. Since MPO is a complication derived frommeconium peritonitis and not the other way around, carefulexamination of the scrotum during fetal life is helpful for theearly and simple prenatal diagnosis of meconium peritonitisas well as its postnatal management.
A detailed evaluation of the scrotum during fetal life issignificant to avoid an orchiectomy in the neonatal period.Jeanty et al. reported the radiologic findings of 48 patientswith MPO diagnosed after birth [2], in which classical radio-logical findings inMPO, which are both abdominal and scro-tal calcification, were detected only in 42% (20 patients). Inthe present case, scrotal calcification was prenatally detected,but abdominal calcification was not. Although MPO can bemanaged with either surgical or conservative treatment, mostauthors recommended that surgery be performed when ascrotal neoplasm is suspected [2, 5]. As MPO is known tospontaneously resolve, expectant management is acceptable.Therefore, careful examination of the scrotum starting in thefetal period is essential for noninvasive treatment of MPO inthe neonatal period.
Thus, the present case highlights the clinical significanceof a detailed evaluation of the scrotum in a case of isolatedfetal ascites.
Conflict of Interests
The authors have no conflict of interests to declare.
References
[1] W. E. Berdon, D. H. Baker, J. Becker, and P. De Sanctis, “Scrotalmasses in healed meconium peritonitis,” The New EnglandJournal of Medicine, vol. 277, no. 11, pp. 585–587, 1967.
[2] C. Jeanty, A. Bircher, and C. Turner, “Prenatal diagnosis ofmeconium periorchitis and review of the literature,” Journal ofUltrasound in Medicine, vol. 28, no. 12, pp. 1729–1734, 2009.
[3] S. H. Nam, S. C. Kim, D. Y. Kim et al., “Experience withmeconium peritonitis,” Journal of Pediatric Surgery, vol. 42, no.11, pp. 1822–1825, 2007.
[4] S. Zerhouni, C. Mayer, and E. D. Skarsgard, “Can we selectfetuses with intra-abdominal calcification for delivery in neona-tal surgical centres?” Journal of Pediatric Surgery, vol. 48, no. 5,pp. 946–950, 2013.
[5] L. P. Dehner, D. Scott, and J. T. Stocker, “Meconiumperiorchitis:a clinicopathologic study of four cases with a review of theliterature,” Human Pathology, vol. 17, no. 8, pp. 807–812, 1986.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com