

Lung Transplantation Biology Robert Padera, M.D., Ph.D. HBTM 235 September 23, 2015...
31
Lung Transplantation Biology Robert Padera, M.D., Ph.D. HBTM 235 September 23, 2015 [email protected]
-
Upload
chastity-skinner -
Category
Documents
-
view
216 -
download
2
Transcript of Lung Transplantation Biology Robert Padera, M.D., Ph.D. HBTM 235 September 23, 2015...

Lung Transplantation Biology
Robert Padera, M.D., Ph.D.
HBTM 235
September 23, 2015

Goal
• To teach you everything something about the many facets of lung transplantation

Outline
• Introduction• The recipient• The donor• The transplant• The complications• Outcomes

NUMBER OF LUNG TRANSPLANTS REPORTED BY YEAR AND PROCEDURE TYPE
5 7 36 78190
419
704
921
10881223
1336145214621490
16291693
188219322071
23842448
2769
1357
2716
0
250
500
750
1000
1250
1500
1750
2000
2250
2500
2750
3000
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
Nu
mb
er
of
Tra
ns
pla
nts
Bilateral/Double LungSingle Lung
NOTE: This figure includes only the lung transplants that are reported to the ISHLT Transplant Registry. As such, this should not be construed as representing changes in the number of lung transplants performed worldwide.
2010ISHLTJ Heart Lung Transplant. 2010 Oct; 29 (10): 1083-1141

AGE DISTRIBUTION OF ADULT LUNG TRANSPLANT RECIPIENTS (1/1985-6/2009)
0
5
10
15
20
25
18-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-65 66+
Recipient Age
% o
f tr
an
sp
lan
ts
2010ISHLTJ Heart Lung Transplant. 2010 Oct; 29 (10): 1083-1141

Outline
• Introduction• The recipient• The donor• The transplant• The complications• Outcomes

The Recipient
• Respiratory failure of lung origin– Idiopathic pulmonary fibrosis/UIP– COPD/Emphysema– Cystic fibrosis– Primary pulmonary hypertension– Alpha-1 antitrypsin deficiency– Others
• All other options exhausted

ADULT LUNG TRANSPLANTATIONMajor Indications By Year (Number)
0
10
20
30
40
50
60
70
Myopathy
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
19940
250
500
750
1000
1250
1500
1750
2000
2250
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
Transplant Year
Nu
mb
er
of
Tra
ns
pla
nts
CF IPF COPD Alpha-1 IPAH Re-Tx
2010ISHLTJ Heart Lung Transplant. 2010 Oct; 29 (10): 1083-1141

Usual Interstitial Pneumonia• Also known as idiopathic pulmonary fibrosis• UIP adds cells and fibrous tissue (scar) to the lung,
thickening and stiffening it and restricting the elastic stretching, making inspiration harder
• Manifestations include:
Decreased compliance – stiff lung
Decreased lung volumes – spirometry measurements
Impaired diffusion - DLCO measurement
Abnormal small airway function
Pulmonary hypertension

UIP - Gross• Honeycombing, most severe/earliest in lower zones, subpleural areas

End-stage lung Normal lung
Fibroblastic foci
UIP - Microscopic

Emphysema

Cystic Fibrosis

Evaluation of Candidacy• Blood tests
– Nicotine/cotine (6 months)– Blood type (ABO)– Tissue typing (HLA – major histocompatibility complex)– Infection/immunity– General hematology/chemistry
• Imaging tests– Chest X-ray, chest computed tomography (CT)
• Pulmonary function tests– Spirometry, 6 minute walk
• Cardiac tests– EKG, coronary angiography, echocardiography

Outline
• Introduction• The recipient• The donor• The transplant• The complications• Outcomes
Donor Characteristics
• Brain death• Medical history
– Transmissible entities: infections, malignancy
• Willingness to be organ donor
• Imaging– Pneumonia, hemorrhage, underlying lung
disease, pulmonary emboli, etc.
• Function?
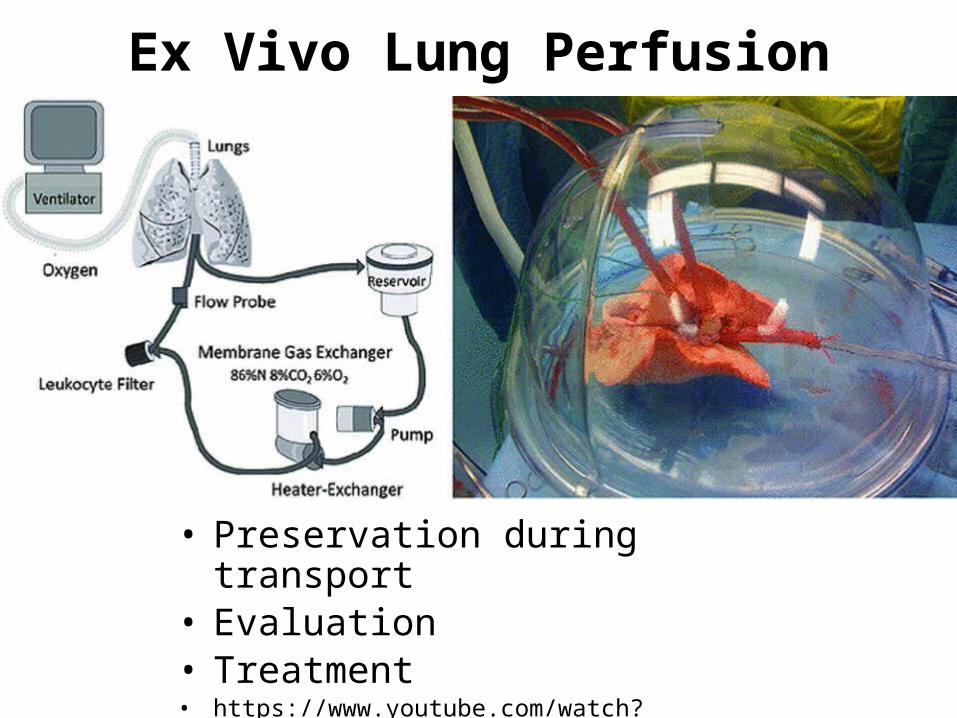
Ex Vivo Lung Perfusion
• Preservation during transport• Evaluation• Treatment• https://www.youtube.com/watch?v=emP9vrsdPwo

Outline
• Introduction• The recipient• The donor• The transplant• The complications• Outcomes

Procedure
• Multiorgan harvest• Removed from donor• Transport to recipient• Implantation and
anastomosis– Bronchus– Pulmonary artery– Pulmonary veins

Lung Anatomy
Vasculature

Outline
• Introduction• The recipient• The donor• The transplant• The complications• Outcomes

Rejection
• Hyperacute– ABO mismatch
• Acute cellular– HLA mismatch
• Antibody mediated– Developed
• Chronic

Acute RejectionVascular
Airway

Chronic RejectionVascular Airway

Post-transplant Medications
• 30-40 pills/day• Immunosuppressants
– Cyclosporine– Mycophenolate– Prednisone
• Antibiotics– PCP, CMV
• Vitamins/minerals

Infection• Increased risk from
– Immunosuppression– Cough reflex diminished– Mucociliary clearance impaired
• Opportunistic infections common
Aspergillus Pneumocystis jiroveci
Cytomegalovirus

Outline
• Introduction• The recipient• The donor• The transplant• The complications• Outcomes
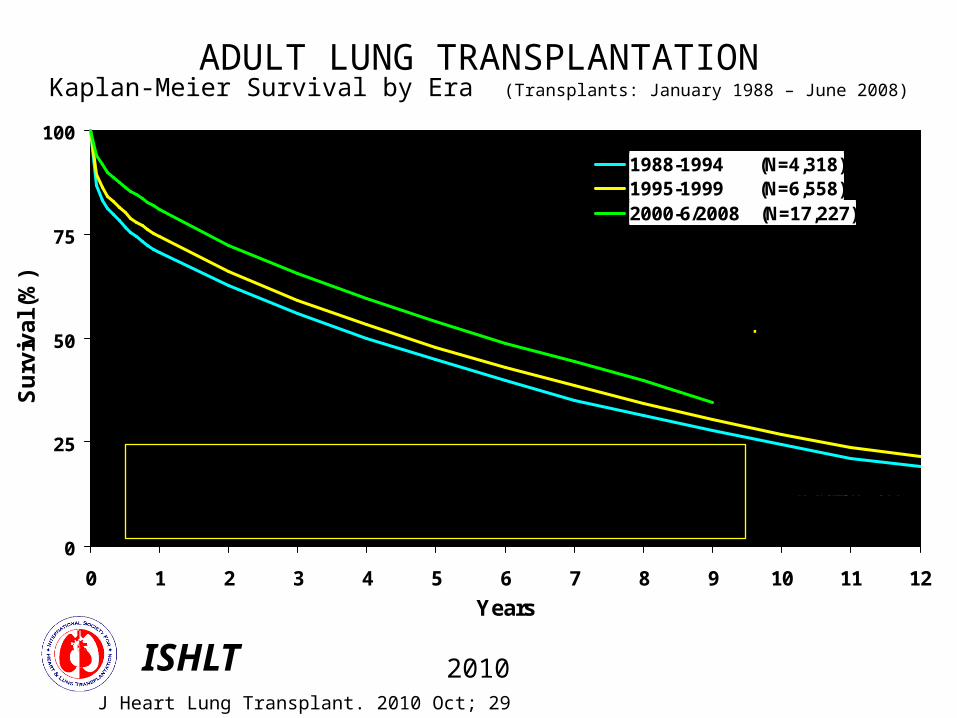
ADULT LUNG TRANSPLANTATIONKaplan-Meier Survival by Era (Transplants: January 1988 – June 2008)
0
25
50
75
100
0 1 2 3 4 5 6 7 8 9 10 11 12
Years
Su
rviv
al (
%)
1988-1994 (N=4,318)1995-1999 (N=6,558)2000-6/2008 (N=17,227)
1988-1994: 1/2-life = 4.0 Years; Conditional 1/2-life = 7.0 Years1995-1999: 1/2-life = 4.6 Years; Conditional 1/2-life = 7.3 Years2000-6/2008: 1/2-life = 5.7 Years; Conditional 1/2-life = 7.9 Years
N at risk = 129
N at risk = 406
N at risk = 577
Survival comparisons by era1988-94 vs. 1995-99: p = 0.00021988-94: vs. 2000-6/08: p <0.0001 1995-99 vs. 2000-6/08: p <0.0001
2010ISHLTJ Heart Lung Transplant. 2010 Oct; 29 (10): 1083-1141

ADULT LUNG RECIPIENTSEmployment Status of Surviving Recipients
(Follow-ups: April 1994 – June 2009)
0%
20%
40%
60%
80%
100%
1 Year (N=9,787) 3 Year (N=6,090) 5 Year (N=3,777) 10 year (N=702)
Working (FT/PTStatus unknown)
Working Part Time
Working Full Time
Retired
Not Working
2010ISHLTJ Heart Lung Transplant. 2010 Oct; 29 (10): 1083-1141

ADULT LUNG TRANSPLANT RECIPIENTS: Relative Incidence of Leading Causes of Death
(Deaths: January 1992 - June 2009)
0
10
20
30
40
50
0-30 Days (N=1,966)
31 Days – 1Year
(N=3,387)
>1 Year – 3Years
(N=3,073)
>3 Years – 5Years
(N=1,737)
>5 Years – 10Years
(N=2,014)
>10 Years (N=483)
Bronchiolitis Malignancy (non-Lymph/PTLD)
Infection (non-CMV) Graft Failure
Cardiovascular
Pe
rce
nta
ge
of
De
ath
s
2010ISHLTJ Heart Lung Transplant. 2010 Oct; 29 (10): 1083-1141


















