Koors, massaverlies en vergrote klierelearning.ufs.ac.za/INTERNAL_MEDICINE_ON/Resources/3....
61
Koors, massaverlies en vergrote kliere Interne Geneeskunde – Aansteeklike siektes – Pulmonologie – Sub dissiplines Kindergeneeskunde Huisartskunde Dermatologie Farmakologie Obstertrie en Ginekologie Radiologie Onkoterapie
Transcript of Koors, massaverlies en vergrote klierelearning.ufs.ac.za/INTERNAL_MEDICINE_ON/Resources/3....

Koors, massaverlies en
vergrote kliereInterne Geneeskunde
– Aansteeklike siektes
– Pulmonologie
– Sub dissiplines
Kindergeneeskunde
Huisartskunde
Dermatologie
Farmakologie
Obstertrie en Ginekologie
Radiologie
Onkoterapie

Davidson’s
• Bladsye 377 tot 402
– Kliniese Ondersoek – 378
– Epidemiologie en Virologie – 380
– Natuurluke verloop en klassifikasie – 383
– Voorkoming – 384
– Opp Infeksies en Maligniteiete – 384 –
– Hantering – 379 –
– HTLV - 401


Risiko vir Infeksie p 380 Davidson’s
• Bloed oortapping
• Moeder na Kind
• Naalde (dwelms)
• Mukosale membrane
– Genitaal
– Non genitaal
• 90%
• 15 – 40%
• 0,5 – 1,0%
• 0,2% - 0,5%
• < 0,1%

Differensiële diagnose van
Limfadenopatie – T 24.11 Davidson
1. Infektief– Virusse: MIV, EBV,
Rubella
– Bakterie: TB, NTBMB, Kat-krap siekte, Brusellose, Siffilis, Strep, Staf, LGV van chlamydia
– Parasiete:Toksoplasmose, tripanosomiase
– Fungi: Histoplasmose
2. Bindweefsel siektes– RA, SLE
3. Neoplasma– Hematologies:
• Limfoom, ALL, CLL
– Metastases• Long, tiroied, maag,
mamma
4. Infiltrasie– Sarkoiedose, Amiloiedose
5. Middels– Phenytoin, allopurinol,
carbamasepien, hidralasien

Geskiedenis –
Simptome van MIV infeksie
• Primêre MIV infeksie (A)
• 2-4 weke : 70-80% – p383 Davidson’s
– Koors (80%)
– Makulo-papulêre veluitslag (60%)
– Moegheid (80%)
– Faringittes met servikale kliere (50%)
– Mialgie en atralgie (50%)
– Hoofpyn en retro-orbitale pyn (40%)
– Mukosale ulserasie (mond 20%, genitaal 10%)
– Aseptiese meningites, enkefalites, miëlittes, polineurites)


Tabel 14.6
P 384
Davidson’s

ELISA
Antibody
testing
are nearly
• 100 % sensitive
(unless a person is
in the window
period)
and about
• 99 % specific

Window period
Window period

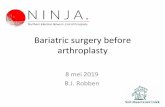
CD4 count
• > 500 /mm3 ( > 29%)
– Mild immune deficiency
– Asymptomatic + unlikely to develop OI
• 200 – 500 / mm3 (14-28%)
– Moderate immune deficiency
– some OI
• < 200 / mm3 (<14%)
– Severe immune deficiency
– Opportunistic infections
Surrogaat
• Lotale limfosiettelling
• < 1,25 x 109/l =
– CD4 < 200
• < 0,75 x 109/l =
– CD4 < 50


> 500
200
100
50
Oral thrush, TB, Shingles
PCP, HSV, Candida esophagitis
Toxoplasmosis, Cryptococcosis
MAC, CMV
Time
CD4
Opp Infections
Tabel 14.7
Davidson’s


Lymphadenopathy
Differential diagnosis
• HIV
• Lymphoma
• Kaposi sarcoma
• TB
– Asymmetrical
– > 2 cm
– Skin involvement
– unexplained fever or
– weight loss


Parotid enlargement and
dry mouth
Pictures taken from booklet: Common oral lesions in Children and Adults
University of Stellenbosch

Oral Hairy Leukoplakia
Etiologie?

Aphthous ulcers
• Extremely painful
– 2% lidocaine gel
– Systemic pain killers
• Topical Hibident mouth rises with Kenalog in orabase 3 x per day
• Systemic prednisone if no response
From Common oral lesions
in Children and Adults
University of Stellenbosch




Treatment of esophageal
candidiasis
•14 day
fluconazole
(200mg/d orally)





Prophylaxis for PCP
Indication BactrimR
• CD4
< 200/mm3
•Stage 3 or 4
infection
Co-trimoxazole
1 DS /day
2 SS /day

When to stop
BACTRIM?
IF CD4 has recovered to
> 200 on ARVs

BACTRIM ALLERGY?
Alternative– Dapsone 100 mg /d

PCP TreatmentBactrimR x 21 d
• PO2 < 70 mmHg
– Prednisone
• 40mg b.d x 5 days
• 40mg/ d x 5days
• 20 mg/d x 11 days

Waarvan sal die pasient kla?

Presenterende Simptoom
• A – Hoes
• B – Koors
• C - Epilepsie
• D - Hoofpyn

D- HEADACHE• Common symptom in HIV
• Serious causes
Common side effect of ARVs
1st 6 weeks
resolve spontaneously
• Breakthrough meningitis complicating
immune recovery

Severe Headache• new onset or different
• unable to sleep
• vomiting
• temp > 38
• neck stiffness
• confusion
• visual changes
• seizure
• weakness on one side

Cryptococcal meningitis
Indian ink
stain

Cryptococcal Meningitis
1.) Acute therapy
– Amphotericin B ivi
+ Fluconazole
– Fluconazole monotherapy

Cryptococcal Meningitis
2.) Maintenance therapy
– Fluconazole
200mg/d po

Raised
Intracranial pressure
• Remove 20 ml - 30 ml of
CSF daily, till normal

Toxoplasmosis p 392 Davidsons
– Pyrimethamine +
• 100 – 200 mg stat
• Then 50 – 100mg /d
– Folinic acid +
• 10 mg/d
– Sulfadiazine
• 4-8 g/d
– or Clindamycin
• 900 – 1200 mg/d ivi q 6 hourly or
• 300 – 450 mg po q 6 hourly
– suppressive therapy
• Pyr + FA + Sd or Cl

Toxoplasmosis prophylaxis
Indication Preferred Alternatives
• positive IgG
serology
and
• CD4
< 100/mm3
• TMP-SMX
1 DS per day
2 SS per day
Dapsone +
pyrimethamine
+ folinic acid

CNS lymphoma


Tabel 14.16
Davidson’s

Severe Eye problems
Same day referral:
– Shingles – face
– One painful red eye
– Sudden change in vision

CMV retinitis
- sudden loss
of vision in
one or both
eyes

• Most days x 1/12 = stage 3 disease
Bactrim prophylaxis
• Wasting disease: weight loss + diarrhoea / fever > 1/12
= AIDS defining illness
- ARVs regardless of CD4
P 33

Diarrhoea
Not on ARVs
usually caused by organisms
which respond poorly to
antibiotics
– best treatment = ARVs

Diarrhoea on ARVs
• d4T and AZT
usually resolves in 1st 6 weeks
• ddI and Kaletra
can cause loose stools


Shingles
SAME DAY REFERAL– Eye / Meningitis /< 72 hours
Acyclovir (ZoviraxR)
800mg, 5 x /d
Systemic analgesics– Paracetamol, Ibuprofen, Codein
– Amitriptyline

HIV+ persons with Chikenpox
are at risk for:
• prolonged new lesion formation and
• extensive cutaneous involvement
• secondary bacterial infection
• life-threatening visceral dissemination

Varicella pneumonia
• varicella in HIV is
more commonly
associated with severe
disease
• varicella pneumonia
has a mortality of up
to 40%

Management of varicella in HIV
• Acyclovir: 800mg orally 5 x per day for 7 days
• HIV or AIDS patients with pneumonia, encephalitis, haemorrhagic manifestations or multi-organ involvement
– IV acyclovir -10mg/kg 3 x per day for 7 days

Herpes Simplex
• Painful – Lignocaine gel + paracetamol
• Gargle with salt water
• Acyclovir


Antiviral Therapy
• Limited salvage regimes
• First regimen = best change of success
• Once failure
– limited fall back options
– evolution of triple-class resistance can occur
rapidly after the second regimen fails

Wie moet HAART kry?
Tabel 14.25 Davidson’s
– CD4: < 200 /mm3
of
– WHO stadium 4 siekte

Failure of therapy – 400plasma HIV RNA levels not > 1 log drop at 6-8 weeks
> 0.6 increase in VL from its lowest levels
• non-adherence
• inadequate potency of drugs
• suboptimal levels of antiretroviral agents
• Drug interactions or toxicity
• Previous ARVT or resistance
• Very high baseline VL
• other factors that are poorly understood