
Keith Dawkins MD FRCP FACC FSCAI Chief Medical Officer Senior Vice President Boston Scientific...
38
Keith Dawkins MD FRCP FACC FSCAI Keith Dawkins MD FRCP FACC FSCAI Chief Medical Officer Chief Medical Officer Senior Vice President Senior Vice President Boston Scientific Corporation Boston Scientific Corporation Boston Scientific Boston Scientific Programme Update Programme Update London – January 26, 2011 London – January 26, 2011
-
Upload
elaina-evens -
Category
Documents
-
view
220 -
download
0
Transcript of Keith Dawkins MD FRCP FACC FSCAI Chief Medical Officer Senior Vice President Boston Scientific...
Keith Dawkins MD FRCP FACC FSCAIKeith Dawkins MD FRCP FACC FSCAIChief Medical OfficerChief Medical OfficerSenior Vice PresidentSenior Vice PresidentBoston Scientific CorporationBoston Scientific Corporation
Boston ScientificBoston ScientificProgramme UpdateProgramme Update
London – January 26, 2011London – January 26, 2011
Conflicts of InterestConflicts of Interest
EmployeeBoston Scientific Corporation
StockholderBoston Scientific Corporation
Element Stent Platform
Next Generation DES
BSC Structural Heart ProgrammeSadra Lotus™ Valve
Atritech Watchman Device
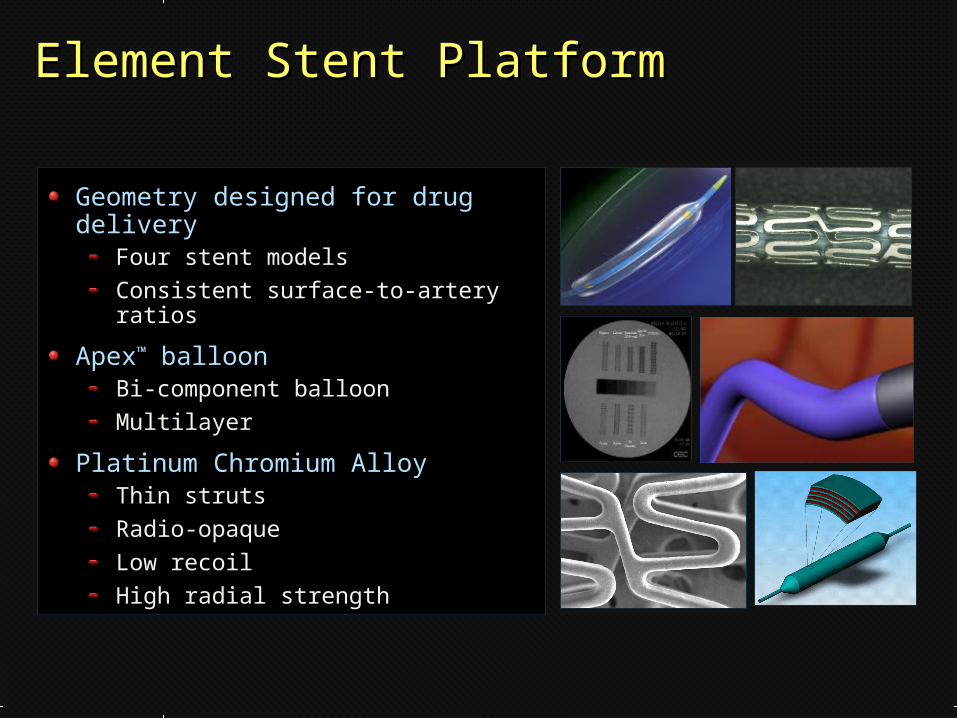
Element Stent PlatformElement Stent Platform
Geometry designed for drug delivery
Four stent modelsConsistent surface-to-artery ratios
Apex™ balloonBi-component balloonMultilayer
Platinum Chromium AlloyThin strutsRadio-opaqueLow recoilHigh radial strength
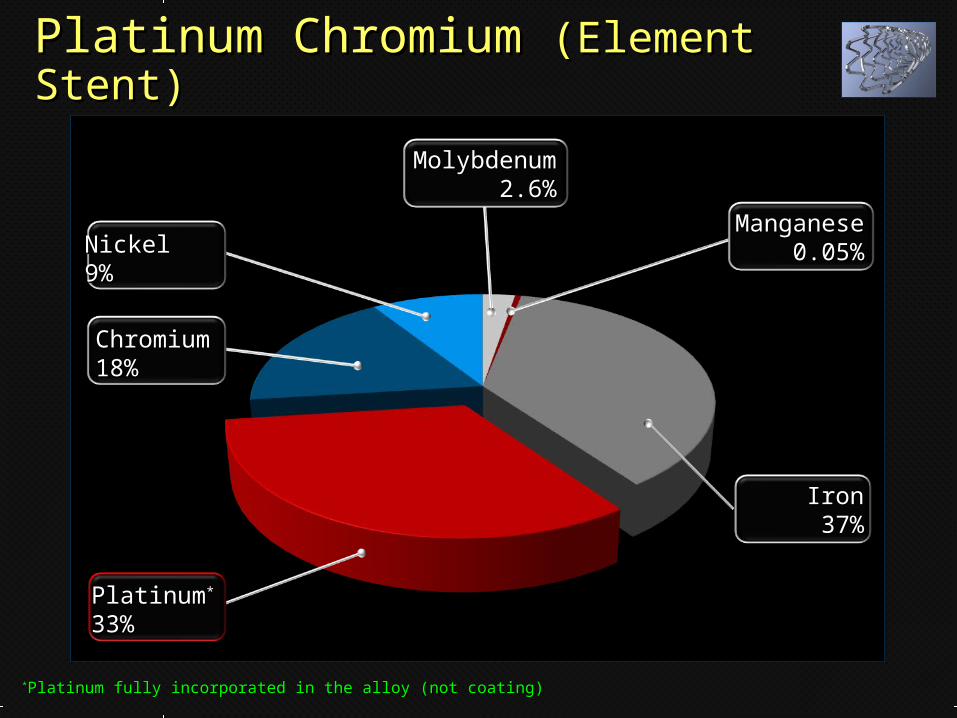
Platinum Chromium Platinum Chromium (Element Stent)(Element Stent)
ChromiumChromium18%18%
PlatinumPlatinum**
33%33%
IronIron37%37%
NickelNickel9%9%
ManganeseManganese0.05%0.05%
MolybdenumMolybdenum2.6%2.6%
**Platinum fully incorporated in the alloy (not coating)Platinum fully incorporated in the alloy (not coating)
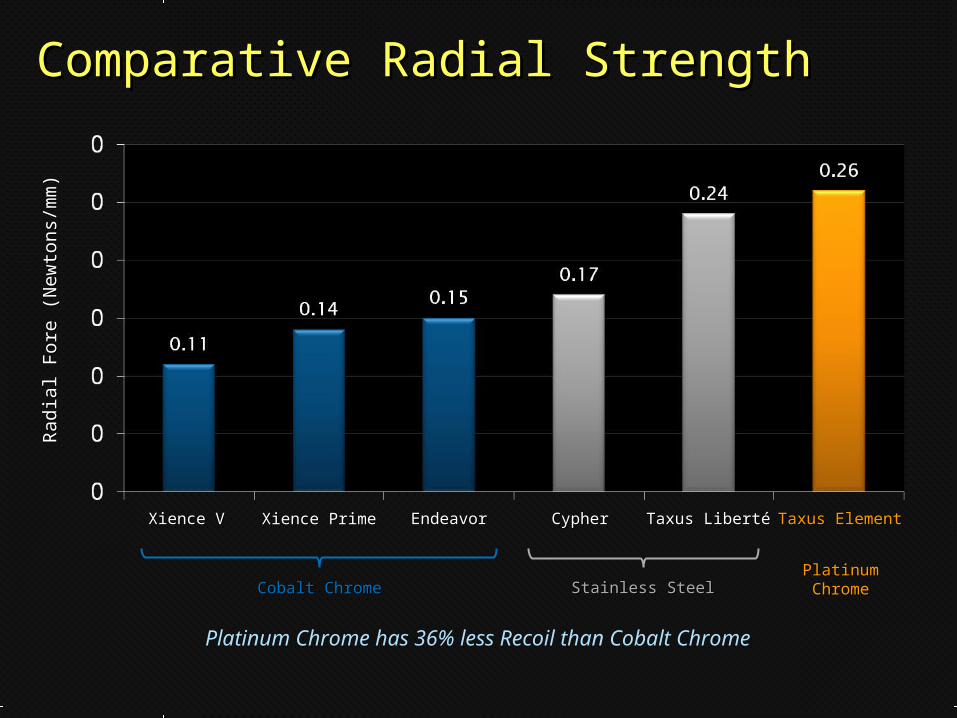
Comparative Radial StrengthComparative Radial StrengthR
adia
l Fo
re (
New
tons/
mm
)R
adia
l Fo
re (
New
tons/
mm
)
Xience VXience V EndeavorEndeavorXience PrimeXience Prime CypherCypher Taxus LibertéTaxus Liberté Taxus ElementTaxus Element
Cobalt ChromeCobalt Chrome Stainless SteelStainless SteelPlatinumPlatinumChromeChrome
Platinum Chrome has 36% less Recoil than Cobalt Chrome
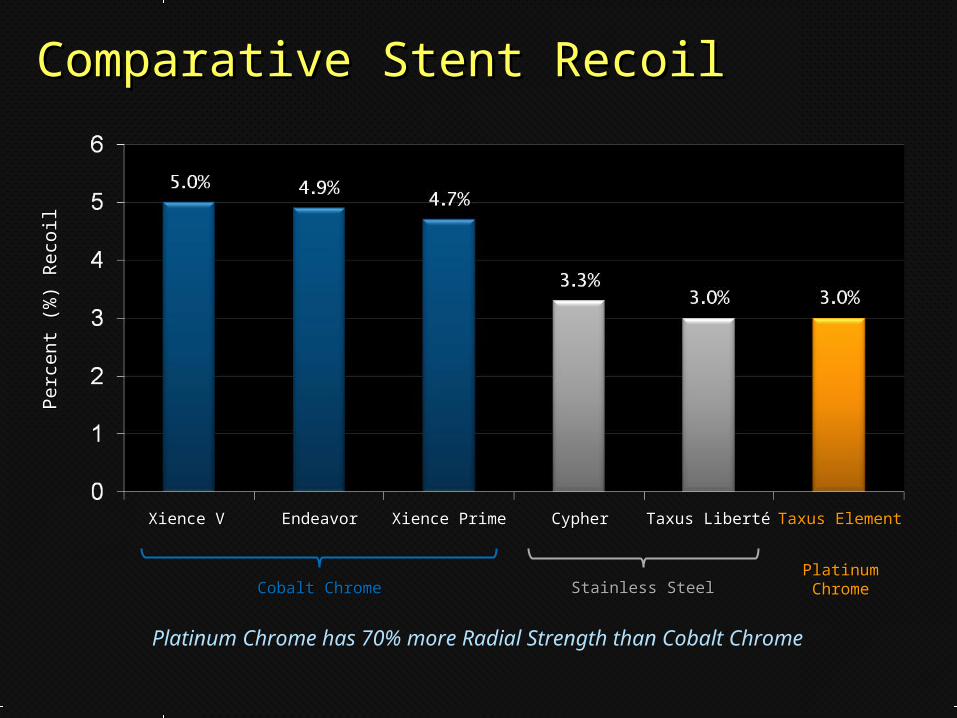
Comparative Stent RecoilComparative Stent RecoilPerc
en
t (%
) R
eco
ilPerc
en
t (%
) R
eco
il
Xience VXience V EndeavorEndeavor Xience PrimeXience Prime CypherCypher Taxus LibertéTaxus Liberté Taxus ElementTaxus Element
Cobalt ChromeCobalt Chrome Stainless SteelStainless SteelPlatinumPlatinumChromeChrome
Platinum Chrome has 70% more Radial Strength than Cobalt Chrome
Taxus LibertéTaxus Liberté
Ste
nt S
trut T
hickn
ess (µ
m)
Ste
nt S
trut T
hickn
ess (µ
m)
Taxus ExpressTaxus Express Taxus ElementTaxus Element
Avera
ge B
end C
ycl
es
Avera
ge B
end C
ycl
es
befo
re F
ract
ure
(m
illio
n)
befo
re F
ract
ure
(m
illio
n)
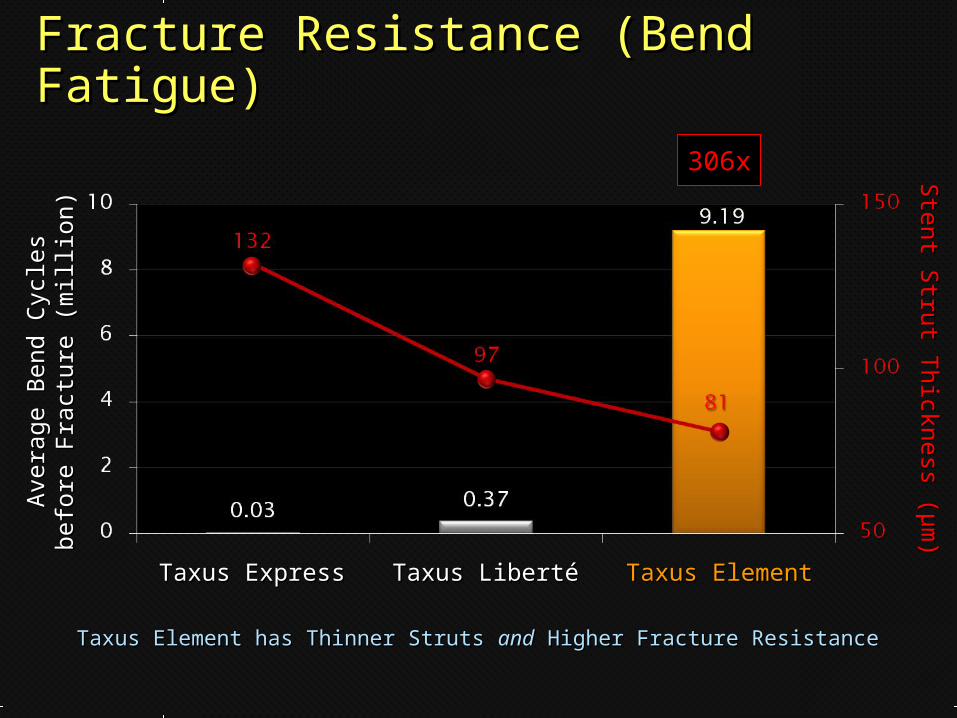
Fracture Resistance (Bend Fracture Resistance (Bend Fatigue)Fatigue)
Taxus Element has Thinner Struts Taxus Element has Thinner Struts andand Higher Fracture Resistance Higher Fracture Resistance
306x306x
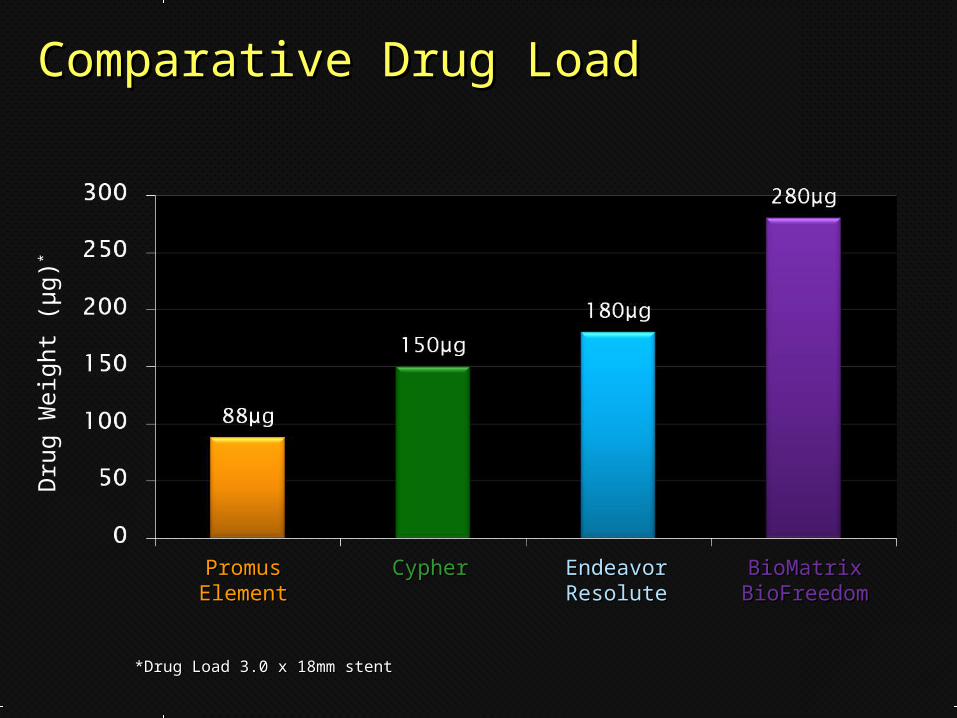
Comparative Drug LoadComparative Drug LoadD
rug W
eig
ht
(μg)*
PromusPromusElementElement
CypherCypher EndeavorEndeavorResoluteResolute
BioMatrixBioMatrixBioFreedomBioFreedom
*Drug Load 3.0 x 18mm stent*Drug Load 3.0 x 18mm stent
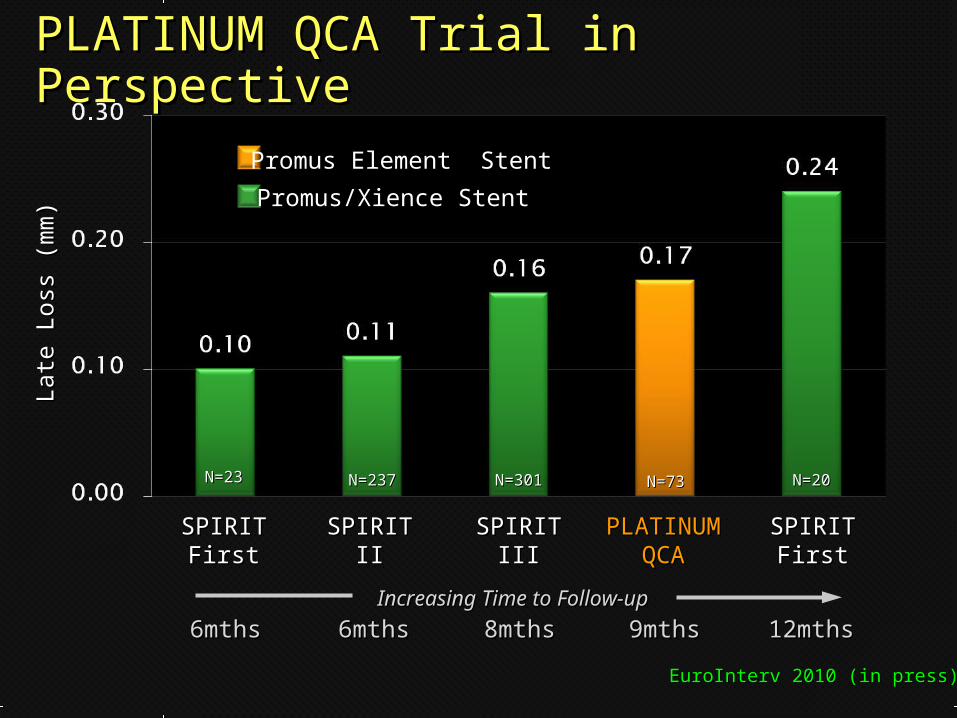
PLATINUM QCA Trial in PerspectivePLATINUM QCA Trial in PerspectiveLa
te L
oss
(m
m)
Late
Loss
(m
m)
SPIRITSPIRITFirstFirst
SPIRITSPIRITFirstFirst
PLATINUMPLATINUMQCAQCA
SPIRITSPIRITIIII
SPIRITSPIRITIIIIII
Increasing Time to Follow-upIncreasing Time to Follow-up
N=23N=23 N=237N=237 N=301N=301 N=73N=73 N=20N=20
6mths6mths 6mths6mths 8mths8mths 9mths9mths 12mths12mths
Promus Element Stent
Promus/Xience Stent
EuroInterv 2010 (in press)EuroInterv 2010 (in press)
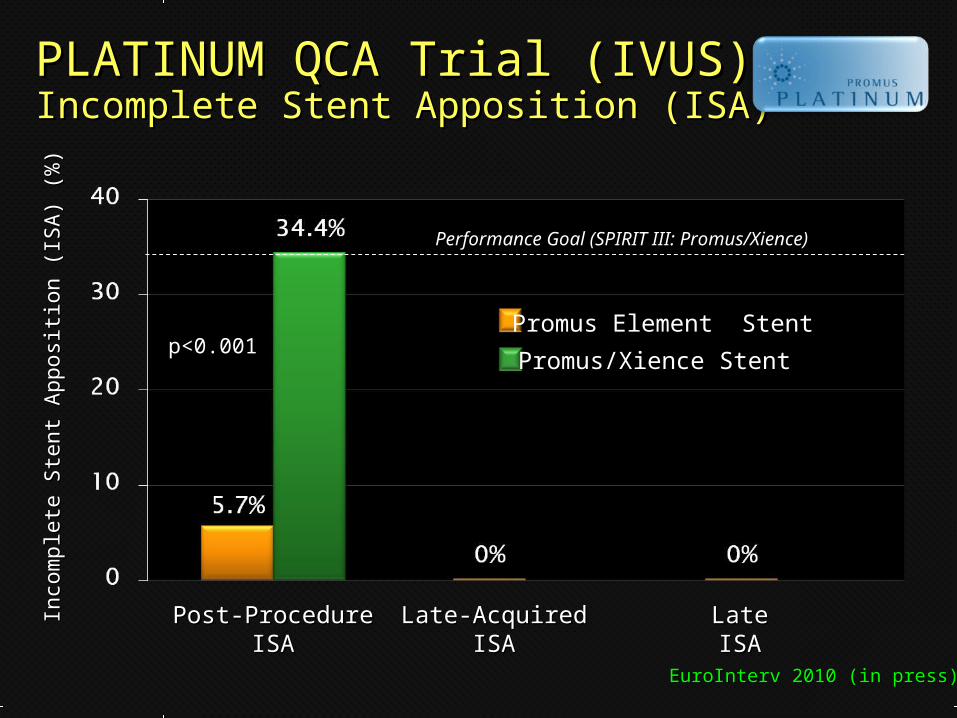
PLATINUM QCA Trial (IVUS)PLATINUM QCA Trial (IVUS)Incomplete Stent Apposition (ISA)Incomplete Stent Apposition (ISA)
Performance Goal (SPIRIT III: Promus/Xience)Performance Goal (SPIRIT III: Promus/Xience)
Post-ProcedurePost-ProcedureISAISA
Late-AcquiredLate-AcquiredISAISA
LateLateISAISA
Inco
mple
te S
tent
Apposi
tion (
ISA
) (%
)In
com
ple
te S
tent
Apposi
tion (
ISA
) (%
)
p<0.001p<0.001Promus Element Stent
Promus/Xience Stent
EuroInterv 2010 (in press)EuroInterv 2010 (in press)
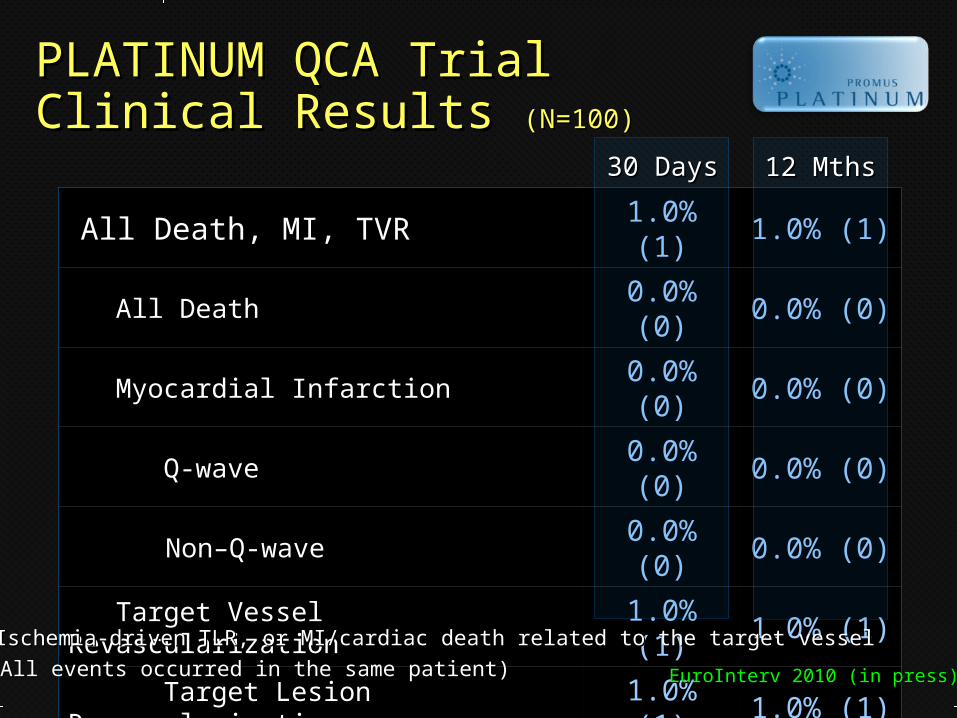
All Death, MI, TVRAll Death, MI, TVR 1.0% (1)1.0% (1) 1.0% (1)1.0% (1)
All DeathAll Death 0.0% (0)0.0% (0) 0.0% (0)0.0% (0)
Myocardial InfarctionMyocardial Infarction 0.0% (0)0.0% (0) 0.0% (0)0.0% (0)
Q-waveQ-wave 0.0% (0)0.0% (0) 0.0% (0)0.0% (0)
Non–Q-waveNon–Q-wave 0.0% (0)0.0% (0) 0.0% (0)0.0% (0)
Target Vessel RevascularizationTarget Vessel Revascularization 1.0% (1)1.0% (1) 1.0% (1)1.0% (1)
Target Lesion RevascularizationTarget Lesion Revascularization 1.0% (1)1.0% (1) 1.0% (1)1.0% (1)
Target Lesion FailureTarget Lesion Failure** 1.0% (1)1.0% (1) 1.0% (1)1.0% (1)
Stent Thrombosis Stent Thrombosis (ARC Def/Prob)(ARC Def/Prob) 1.0% (1)1.0% (1) 1.0% (1)1.0% (1)
30 Days30 Days 12 Mths12 Mths
PLATINUM QCA TrialPLATINUM QCA TrialClinical Results Clinical Results (N=100)(N=100)
**Ischemia-driven TLR, or MI/cardiac death related to the target vesselIschemia-driven TLR, or MI/cardiac death related to the target vessel
(All events occurred in the same patient)(All events occurred in the same patient) EuroInterv 2010 (in press)EuroInterv 2010 (in press)
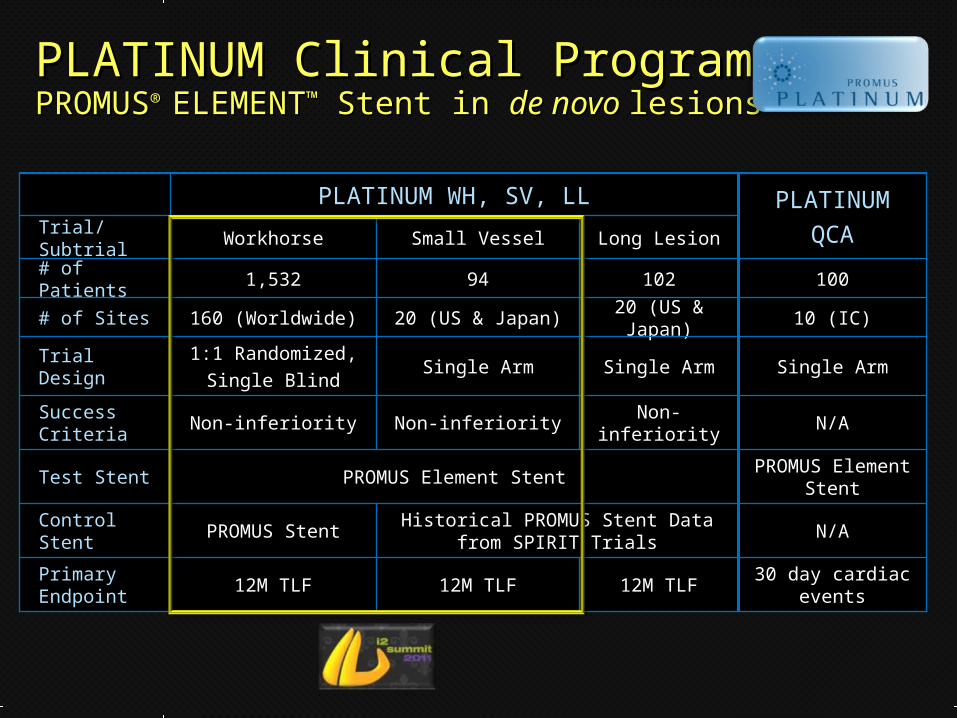
PLATINUMPLATINUM
QCAQCA
PLATINUM WH, SV, LLPLATINUM WH, SV, LL
12M TLF12M TLF
Non-inferiorityNon-inferiority
Single ArmSingle Arm
20 (US & Japan)20 (US & Japan)
102102
Long LesionLong Lesion
12M TLF12M TLF
Historical PROMUS Stent Data from Historical PROMUS Stent Data from SPIRIT TrialsSPIRIT Trials
Non-inferiorityNon-inferiority
Single ArmSingle Arm
20 (US & Japan)20 (US & Japan)
9494
Small VesselSmall Vessel
12M TLF12M TLF
PROMUS StentPROMUS Stent
PROMUS Element StentPROMUS Element Stent
Non-inferiorityNon-inferiority
1:1 Randomized,1:1 Randomized,
Single BlindSingle Blind
160 (Worldwide)160 (Worldwide)
1,5321,532
WorkhorseWorkhorse
10 (IC)10 (IC)# of Sites# of Sites
100100# of Patients# of Patients
30 day cardiac 30 day cardiac eventsevents
Primary Primary EndpointEndpoint
N/AN/AControl StentControl Stent
N/AN/ASuccess Success CriteriaCriteria
PROMUS Element PROMUS Element StentStentTest StentTest Stent
Single ArmSingle ArmTrial DesignTrial Design
Trial/SubtrialTrial/Subtrial
PLATINUM Clinical Program PLATINUM Clinical Program PROMUSPROMUS® ® ELEMENTELEMENT™™ Stent in Stent in de novo de novo lesionslesions
Next Next Generation Generation DESDES
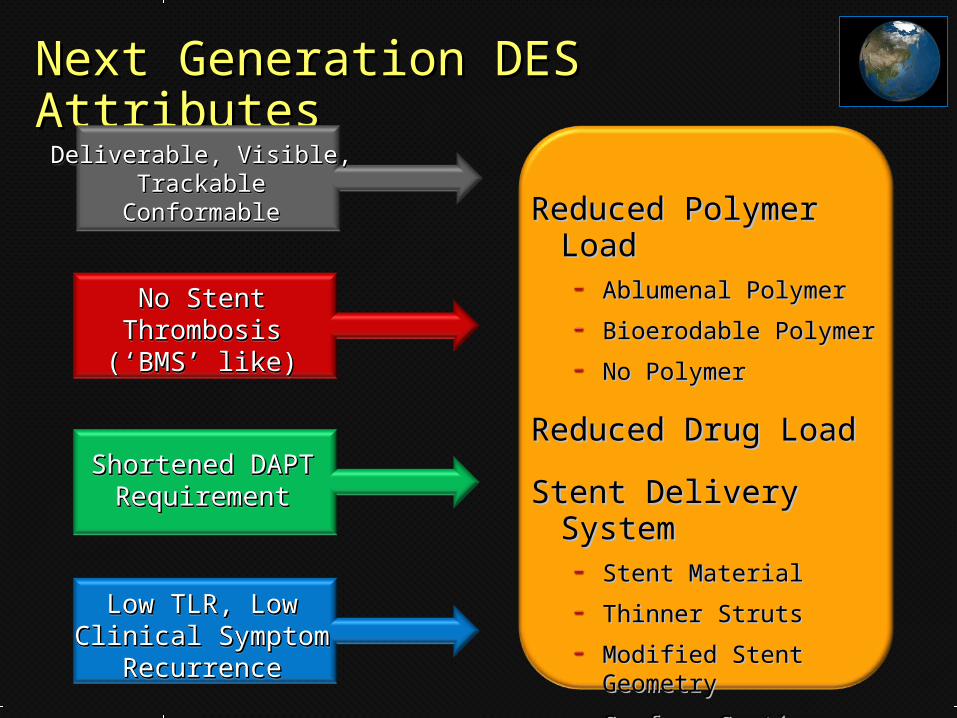
Next Generation DES AttributesNext Generation DES Attributes
No StentNo StentThrombosisThrombosis(‘BMS’ like)(‘BMS’ like)
No StentNo StentThrombosisThrombosis(‘BMS’ like)(‘BMS’ like)
Shortened DAPT Shortened DAPT RequirementRequirement
Shortened DAPT Shortened DAPT RequirementRequirement
Low TLR, Low Low TLR, Low Clinical Symptom Clinical Symptom
RecurrenceRecurrence
Low TLR, Low Low TLR, Low Clinical Symptom Clinical Symptom
RecurrenceRecurrence
Reduced Polymer Reduced Polymer LoadLoad
Ablumenal PolymerAblumenal Polymer
Bioerodable PolymerBioerodable Polymer
No PolymerNo Polymer
Reduced Drug LoadReduced Drug Load
Stent Delivery SystemStent Delivery SystemStent MaterialStent Material
Thinner StrutsThinner Struts
Modified Stent Modified Stent GeometryGeometry
Surface CoatingSurface Coating
Deliverable, Visible, Deliverable, Visible, TrackableTrackable
ConformableConformable
Deliverable, Visible, Deliverable, Visible, TrackableTrackable
ConformableConformable
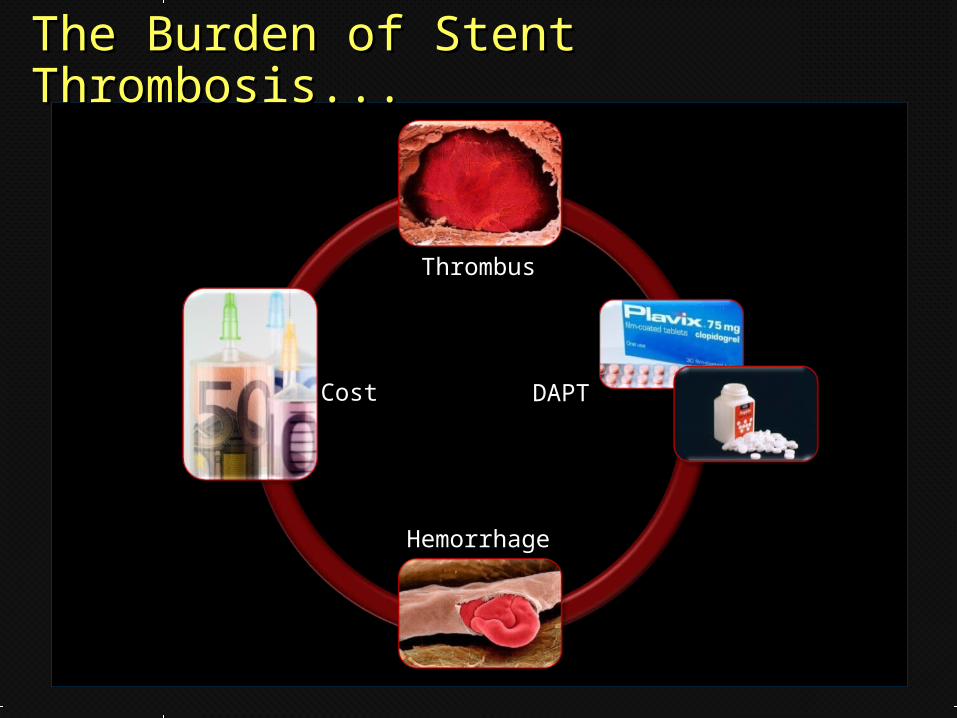
CostCost
ThrombusThrombus
HemorrhageHemorrhage
DAPTDAPT
The Burden of Stent The Burden of Stent Thrombosis...Thrombosis...
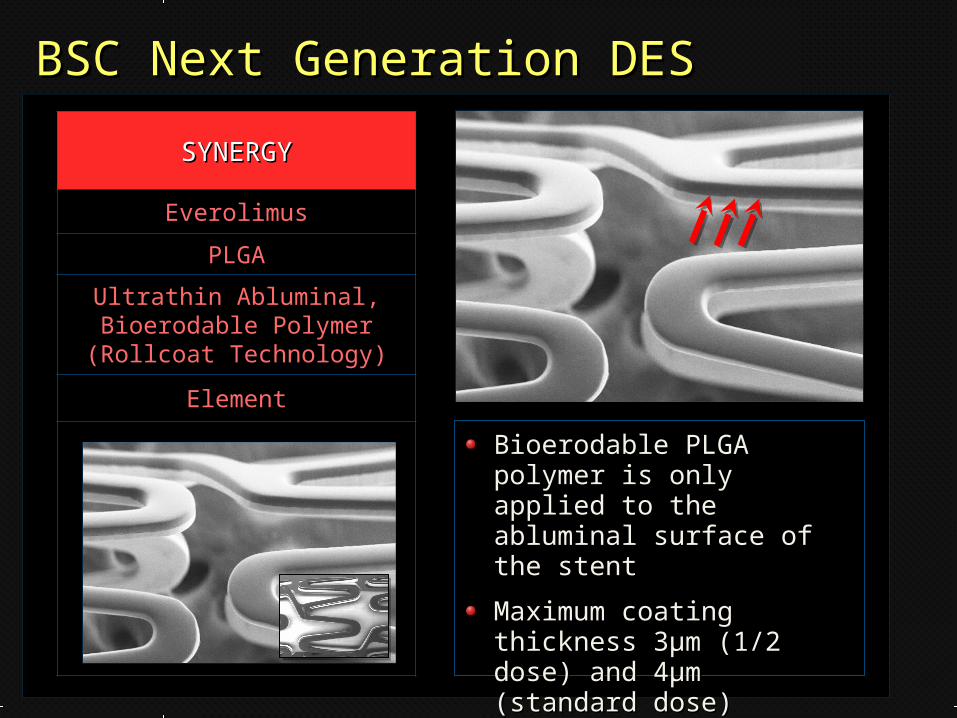
BSC Next Generation DESBSC Next Generation DES
SYNERGYSYNERGY
Everolimus
PLGA
Ultrathin Abluminal, Bioerodable Polymer (Rollcoat Technology)
Element
Bioerodable PLGA polymer Bioerodable PLGA polymer is only applied to the is only applied to the abluminal surface of the abluminal surface of the stentstent
Maximum coating Maximum coating thickness 3thickness 3μμm (1/2 dose) m (1/2 dose) and 4and 4μμm (standard dose)m (standard dose)
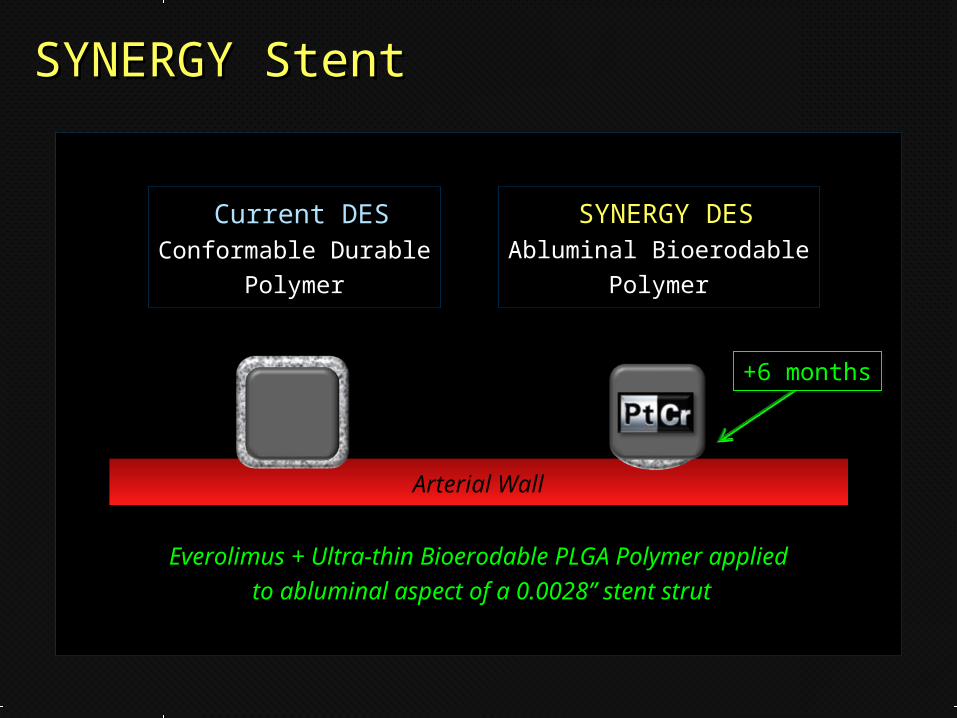
SYNERGY StentSYNERGY Stent
Arterial Wall
Current DESCurrent DESConformable DurableConformable Durable
PolymerPolymer
SYNERGY DESSYNERGY DESAbluminal BioerodableAbluminal Bioerodable
PolymerPolymer
Everolimus + Ultra-thin Bioerodable PLGA Polymer appliedEverolimus + Ultra-thin Bioerodable PLGA Polymer applied
to abluminal aspect of a 0.0028” stent strutto abluminal aspect of a 0.0028” stent strut
+6 months+6 months

SYNERGY Relative Polymer ThicknessSYNERGY Relative Polymer Thickness
SYNERGYPolymer(Thickness)
E. Coli(Length)
Red Cell(Diameter)
T. LibertéPolymer(Thickness)
Neutrophil(Diameter)
Mic
ron (
µ)
SYNERGY = Minimal Drug + Ultrathin Bioerodable Abluminal PolymerSYNERGY = Minimal Drug + Ultrathin Bioerodable Abluminal Polymer
μ

Relative Drug Coating WeightsRelative Drug Coating Weights
0 50 100 150 200 250 300 350 500 685 1267
l l l l l l l l l l l
Bare
Meta
lB
are
Meta
l
Coating Weight (Drug + Polymer) (µg/16mm Stent)Coating Weight (Drug + Polymer) (µg/16mm Stent)
//// //
½D½D SDSD
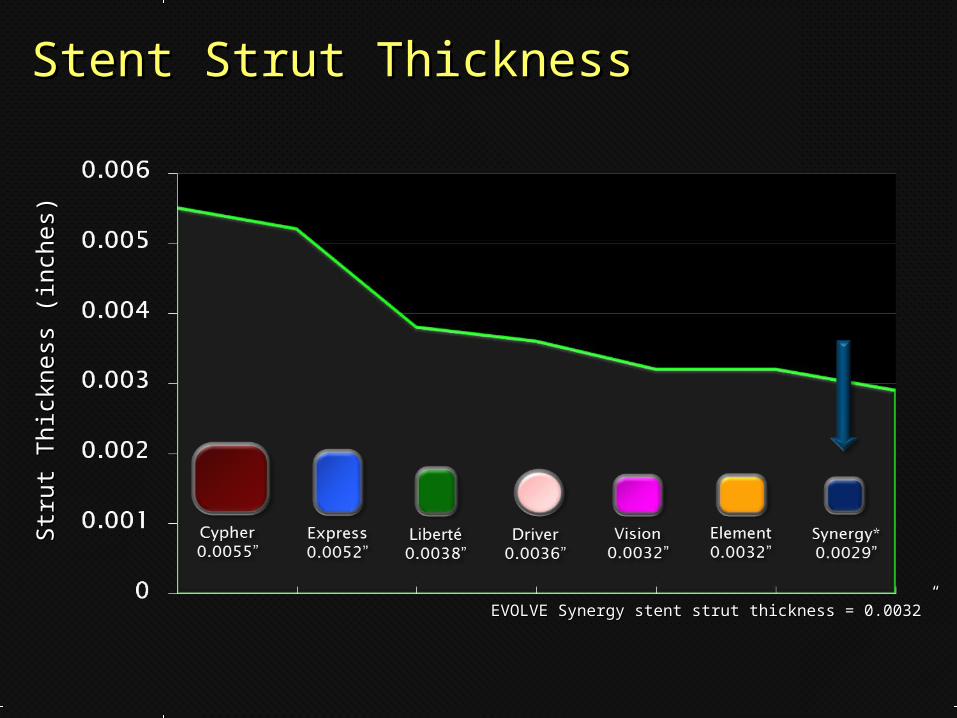
Stent Strut ThicknessStent Strut ThicknessStr
ut
Thic
kness
(in
ches)
Str
ut
Thic
kness
(in
ches)
EVOLVE Synergy stent strut thickness = 0.0032”EVOLVE Synergy stent strut thickness = 0.0032”
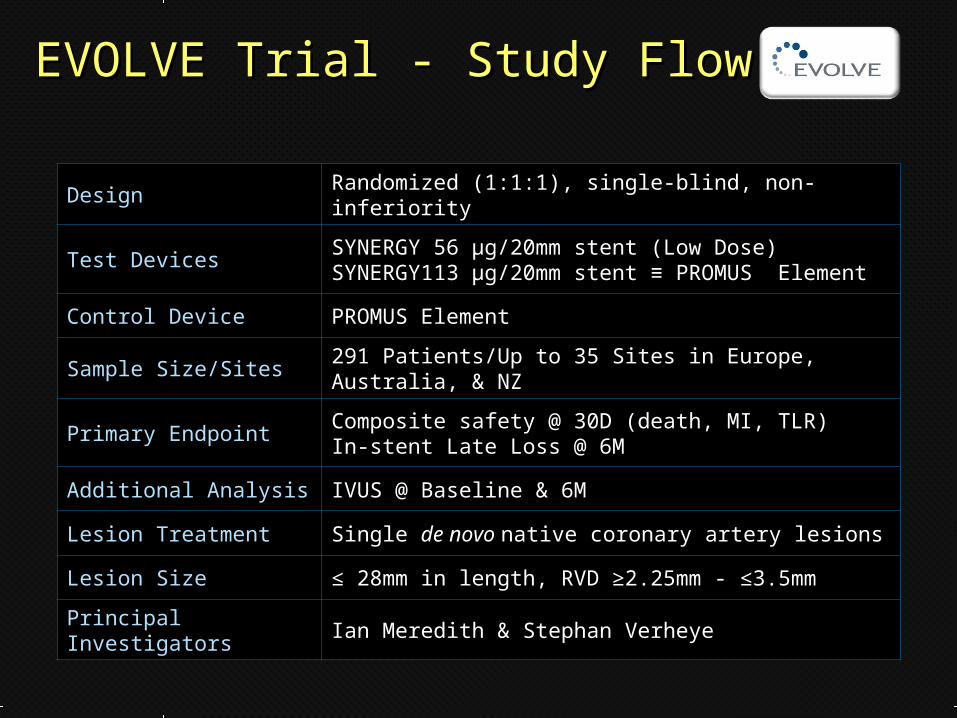
EVOLVE Trial - Study FlowEVOLVE Trial - Study Flow
Design Randomized (1:1:1), single-blind, non-inferiority
Test DevicesSYNERGY 56 µg/20mm stent (Low Dose)SYNERGY113 µg/20mm stent ≡ PROMUS Element
Control Device PROMUS Element
Sample Size/Sites291 Patients/Up to 35 Sites in Europe, Australia, & NZ
Primary EndpointComposite safety @ 30D (death, MI, TLR)In-stent Late Loss @ 6M
Additional Analysis IVUS @ Baseline & 6M
Lesion Treatment Single de novo native coronary artery lesions
Lesion Size ≤ 28mm in length, RVD ≥2.25mm - ≤3.5mm
Principal Investigators Ian Meredith & Stephan Verheye
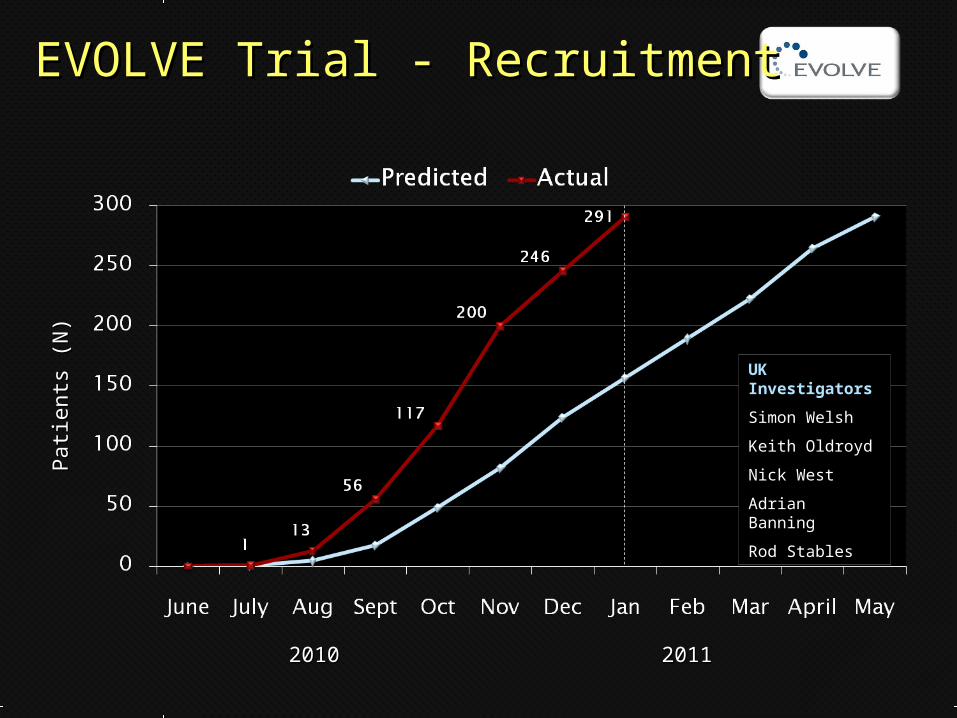
Pati
ents
(N
)Pati
ents
(N
)EVOLVE Trial - RecruitmentEVOLVE Trial - Recruitment
20102010 20112011
UK Investigators
Simon Welsh
Keith Oldroyd
Nick West
Adrian Banning
Rod Stables
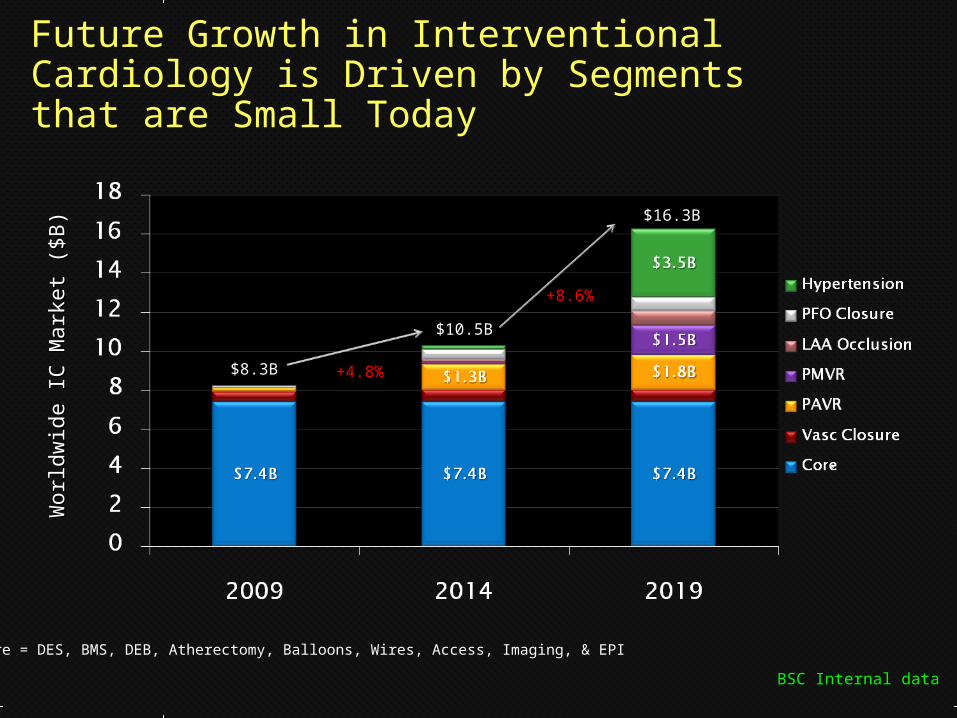
Future Growth in Interventional Cardiology is Driven by Segments that are Small Today
Worl
dw
ide IC
Mark
et
($B
)W
orl
dw
ide IC
Mark
et
($B
)
*
*Core = DES, BMS, DEB, Atherectomy, Balloons, Wires, Access, Imaging, & EPI
BSC Internal dataBSC Internal data
$8.3B$8.3B
$10.5B$10.5B
$16.3B$16.3B
+4.8+4.8%%
+8.6%+8.6%
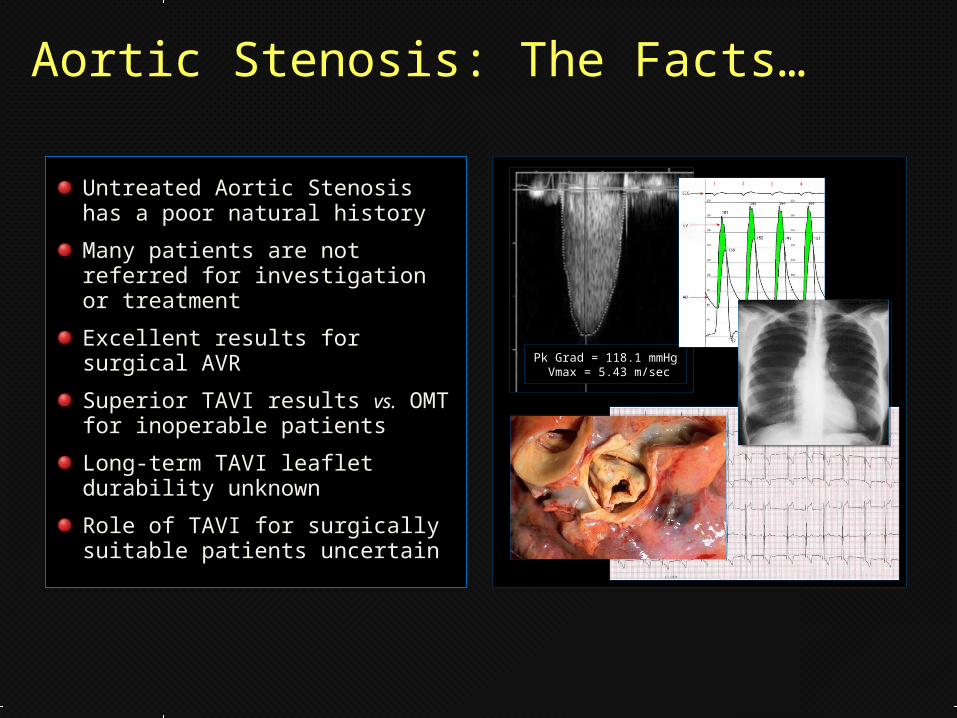
Aortic Stenosis: The Facts…
Untreated Aortic Stenosis has a poor natural history
Many patients are not referred for investigation or treatment
Excellent results for surgical AVR
Superior TAVI results vs. OMT for inoperable patients
Long-term TAVI leaflet durability unknown
Role of TAVI for surgically suitable patients uncertain
Pk Grad = 118.1 mmHg Vmax = 5.43 m/sec
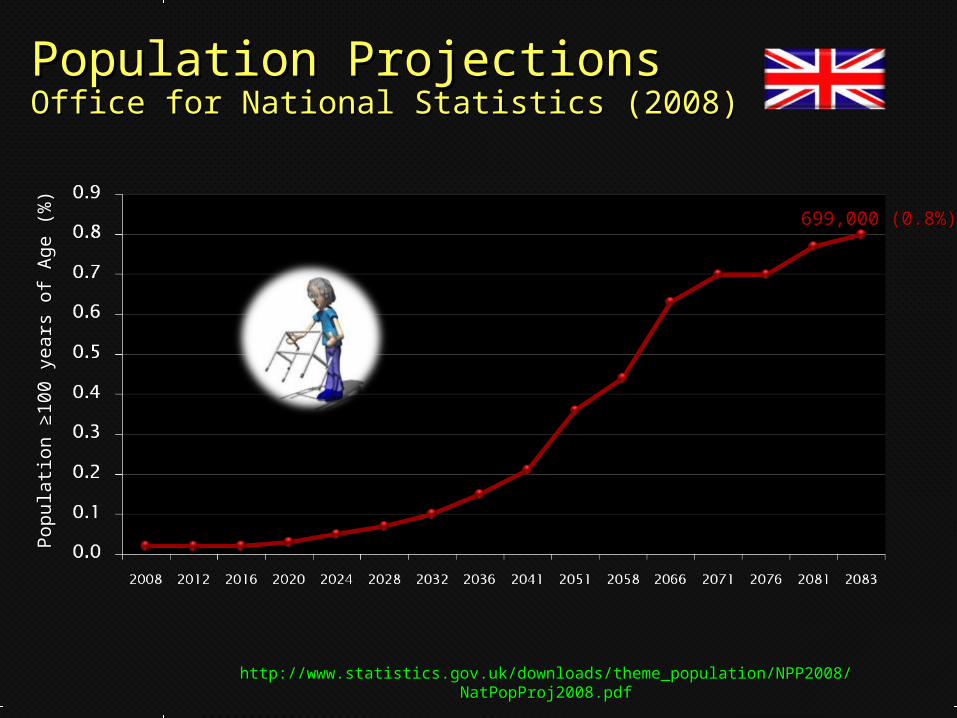
Population Projections Population Projections Office for National Statistics (2008) Office for National Statistics (2008)
Pop
ula
tion ≥
100 y
ears
of
Ag
e (
%)
Pop
ula
tion ≥
100 y
ears
of
Ag
e (
%)
http://www.statistics.gov.uk/downloads/theme_population/NPP2008/NatPopProj2008.pdfhttp://www.statistics.gov.uk/downloads/theme_population/NPP2008/NatPopProj2008.pdf
699,000 (0.8%)699,000 (0.8%)
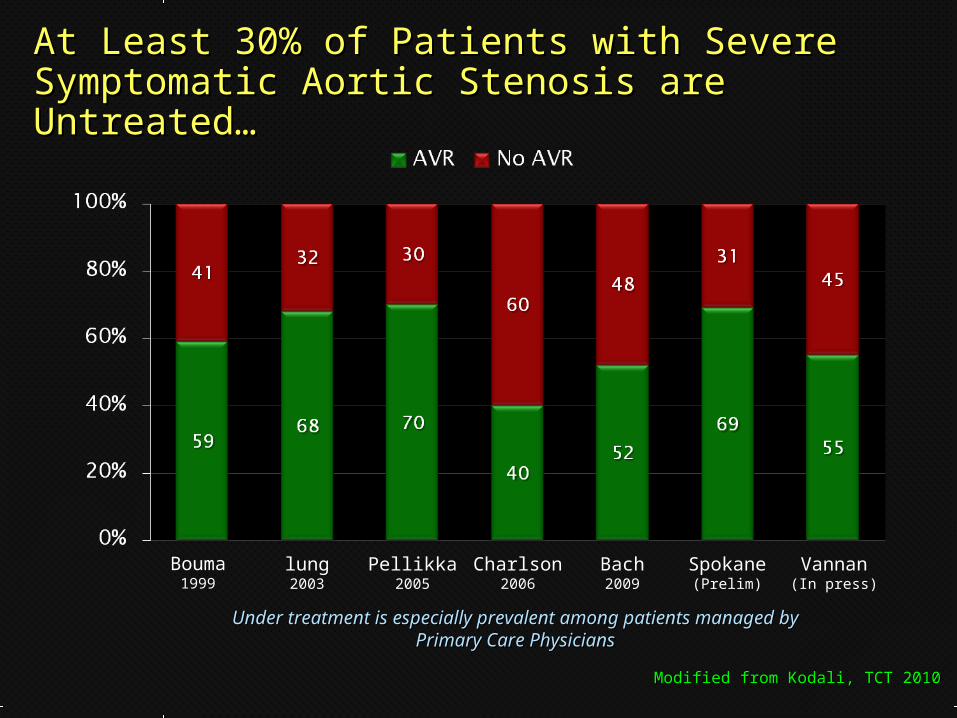
At Least 30% of Patients with Severe At Least 30% of Patients with Severe Symptomatic Aortic Stenosis are Untreated…Symptomatic Aortic Stenosis are Untreated…
Bouma1999
lung2003
Pellikka2005
Charlson2006
Bach2009
Spokane(Prelim)
Vannan(In press)
Under treatment is especially prevalent among patients Under treatment is especially prevalent among patients managed by Primary Care Physiciansmanaged by Primary Care Physicians
Modified from Kodali, TCT 2010Modified from Kodali, TCT 2010

Euro Heart SurveyEuro Heart SurveyFactors Associated with the Absence of Factors Associated with the Absence of Aortic Valve InterventionAortic Valve Intervention
Х2 p OR [95% CI]
Age >70 years 26.0 0.0001 3.4 [2.1-5.5]
LVEF <60% 14.1 0.0002 2.5 [1.6-4.2]
CHF on Admission 11.6 0.0007 2.8 [1.6-5.1]
NYHA Class 1-II vs. III-IV 6.4 0.01 2.2 [1.2-3.9]
>1 Co-morbidity 6.2 0.01 1.8 [1.1-3.0
Modified from Kodali, TCT 2010Modified from Kodali, TCT 2010Eur Heart J 2003;24:1231-1243Eur Heart J 2003;24:1231-1243

TAVI: Procedure SuccessTAVI: Procedure SuccessPerc
ent
(%)
Perc
ent
(%)
Meredith, TCT 2009; Avanzas Rev Esp Cardiol 2010;63:141-148Meredith, TCT 2009; Avanzas Rev Esp Cardiol 2010;63:141-148Eltchaninoff, EuroPCR 2010; Bosmans, EuroPCR 2010Eltchaninoff, EuroPCR 2010; Bosmans, EuroPCR 2010
Zahn, EuroPCR 2010; Ludman, EuroPCR 2010; Petronio, EuroPCR 2010Zahn, EuroPCR 2010; Ludman, EuroPCR 2010; Petronio, EuroPCR 2010Leon, N Engl J Med 2010;363:1597-1607Leon, N Engl J Med 2010;363:1597-1607
N=62N=62 N=108N=108 N= 66N= 66 N=119N=119 N=588N=588 N= 460N= 460 N= 772N= 772 N= 179N= 179
PA
RTN
ER
B

TAVI: 30-Day All-Cause MortalityTAVI: 30-Day All-Cause MortalityPerc
ent
(%)
Perc
ent
(%)
Meredith, TCT 2009; Avanzas Rev Esp Cardiol 2010;63:141-148Meredith, TCT 2009; Avanzas Rev Esp Cardiol 2010;63:141-148Eltchaninoff, EuroPCR 2010; Bosmans, EuroPCR 2010Eltchaninoff, EuroPCR 2010; Bosmans, EuroPCR 2010
Zahn, EuroPCR 2010; Ludman, EuroPCR 2010; Petronio, EuroPCR 2010Zahn, EuroPCR 2010; Ludman, EuroPCR 2010; Petronio, EuroPCR 2010Leon, N Engl J Med 2010;363:1597-1607Leon, N Engl J Med 2010;363:1597-1607
N=62N=62 N=108N=108 N= 66N= 66 N=119N=119 N=588N=588 N= 460N= 460 N= 772N= 772 N= 179N= 179
PA
RTN
ER
B

TAVI: 30-Day Stroke RateTAVI: 30-Day Stroke RatePerc
ent
(%)
Perc
ent
(%)
Eltchaninoff, EuroPCR 2010; Bosmans, EuroPCR 2010Eltchaninoff, EuroPCR 2010; Bosmans, EuroPCR 2010Zahn, EuroPCR 2010; Ludman, EuroPCR 2010; Petronio, EuroPCR 2010Zahn, EuroPCR 2010; Ludman, EuroPCR 2010; Petronio, EuroPCR 2010
Leon, N Engl J Med 2010;363:1597-1607Leon, N Engl J Med 2010;363:1597-1607
N= 66N= 66 N=119N=119 N=588N=588 N= 460N= 460 N= 772N= 772 N= 179N= 179
PA
RTN
ER
B

TAVI: Pooled Monitored StudiesTAVI: Pooled Monitored StudiesChanges in AR Grade with TimeChanges in AR Grade with Time
Modified from Kodali, TCT 2010Modified from Kodali, TCT 2010
25% of TAVI Recipients have ≥2+ AR at 24 months25% of TAVI Recipients have ≥2+ AR at 24 months
Pati
ents
(%
)Pati
ents
(%
)

TAVI Displacement (Dislocation)TAVI Displacement (Dislocation)30
-Day M
ort
alit
y (
%)
30
-Day M
ort
alit
y (
%)
p=0.024p=0.024
Circ Cardiovasc Interv 2010;3:531-536Circ Cardiovasc Interv 2010;3:531-536
21/212 191/212
In an experienced centre, CoreValve dislocation during TAVI occurred in10% of cases and significantly increased peri-procedural risk for severe complications and death
DisplacementDisplacement No Displacement

Sadra Medical Inc
Founded 2004. Start-up company
Headquarters: Los Gatos CA
Acquired by Boston Scientific (November 19, 2010)
FHU Feasibility Trial (EU) Completed 2010
First Lotus™ Valve: >3 year follow-up
CE-Mark Trial to commence 2011(Australia, Germany, UK)
http://www.sadramedical.comhttp://www.sadramedical.com

The Lotus™ Valve
Pre-loaded Valve
18F Delivery System
23mm & 27mm Diameter
Accurate Placement & Repositionable
True Retrievability
Negligible Aortic Regurgitation
Deploy RetrieveDeploy Retrieve
ReleaseRelease

AtritechAtritech
Founded in 2000. Early commercial company
Headquarters Minneapolis MN
Acquired by BSC ( January 19, 2011)
Watchman LAA Closure Device (CE-Mark 2005)
http://www.atritech.nethttp://www.atritech.net

NEJM 2009;360:2601-2602
LAA occlusion for patients intolerant or unsuitable for warfarin or newer anticoagulants (bleeding risk, poor control)
Watchman implant undertaken by electrophysiologists or interventional cardiologists
Implant as a stand-alone procedure or at the time of AF ablation

Conclusions
BSC has a robust product pipeline and is BSC has a robust product pipeline and is midway through a period of transformation midway through a period of transformation (restructuring, acquisitions and divestitures)(restructuring, acquisitions and divestitures)
The SYNERGY stent will build on the ELEMENT The SYNERGY stent will build on the ELEMENT stent platform, delivering abluminal stent platform, delivering abluminal everolimus via a bioerodable polymereverolimus via a bioerodable polymer
The LotusThe Lotus™™ valve and the Watchman valve and the Watchman device device offer significant diversification and growth offer significant diversification and growth opportunities within the BSC core cardiology opportunities within the BSC core cardiology portfolioportfolio


















